Descargar la presentación
La descarga está en progreso. Por favor, espere

1
TRAQUESTOMÍA PERCUTÁNEA
Jorge márquez Universidad de Antioquia Motivaciòn Dudas en indicaciones y pq hacer en uci y PT

2
ENFOQUE POR QUÉ?? CUÁNDO?? CÓMO?? RIESGOS?? PQ. BENEFICI, INDICA
Cuando: precoa dìas Còmo: tècnica Procedimiento realizado con objeto de crear una abertura dentro de la tráquea a través de una incisión ejecutada en el cuello con la inserción de un tubo o cánula para facilitar el paso del aire a los pulmones.

3
INDICACIONES To relieve upper-airway obstruction due to tumor, surgery, trauma, foreign body, or infection • To prevent laryngeal and upper airway damage due to prolonged translaryngeal intubation • To allow easy or frequent access to the lower airway for suctioning and secretion removal • To provide a stable airway in a patient who requires prolonged mechanical ventilation or oxygenation support Obstrucción mecánica secundaria a: b) Tumores de la vía aérea digestiva superior. c) Cuerpos extraños que impiden la intubación o que existe el riesgo de desplazarlos hacia tráquea o bronquios. d) Secreciones. e) Parálisis laringea bilateral en aducción. f) Traumatismo laringeos o heridas de cuello complicadas. g) Malformaciones congénitas: membranas, hipoplasias. h) Infecciones: epiglotitis, laringotraqueobronquititis aguda, difteria laringea. i) Quemaduras de la vía aérea superior, cara o cuello. 2. Enfermedades pulmonares:a) Neumopatías extensas.b) EPOC con enfermedad pulmonar aguda oenfisema. c) Edema pulmonar agudo. 3. Enfermedades del sistema nervioso central (SNC): a) Accidente vascular encefálico. b) Coma. c) Craneotomía. 4. Profiláctica:a) Cirugía radical de cuello.b) Cirugía de cánceres mandibulares y de laboca. c) Resecciones pulmonares. 5. Mala eliminación de secreciones bronquiales: a) Dolor post operatorio. b) Senilidad. c) Escoliosis. d) Debilidad de la pared torácica. 6. Enfermedades neuromusculares:a) Poliomielitis.b) Tétanos.c) Miastenia gravis. d) Síndrome Guillan Barré. c) Polineuritis. 7. Depresión del centro respiratorio:a) TEC.b) Intoxicación por depresores del SNC ycentro respiratorio. c) Anestesia general. 8. Traumatismo torácico: a) Tórax volante; fracturas costales. 9. Uso de respiradores mecánicos.
 Tumores de la vía aérea digestiva superior. c) Cuerpos extraños que impiden la intubación. o que existe el riesgo de desplazarlos hacia. tráquea o bronquios. d) Secreciones. e) Parálisis laringea bilateral en aducción. f) Traumatismo laringeos o heridas de cuello. complicadas. g) Malformaciones congénitas: membranas, hipoplasias. h) Infecciones: epiglotitis, laringotraqueobronquititis aguda, difteria laringea. i) Quemaduras de la vía aérea superior, cara. o cuello. 2. Enfermedades pulmonares:a) Neumopatías extensas.b) EPOC con enfermedad pulmonar aguda oenfisema. c) Edema pulmonar agudo. 3. Enfermedades del sistema nervioso central (SNC): a) Accidente vascular encefálico. b) Coma. c) Craneotomía. 4. Profiláctica:a) Cirugía radical de cuello.b) Cirugía de cánceres mandibulares y de laboca. c) Resecciones pulmonares. 5. Mala eliminación de secreciones bronquiales: a) Dolor post operatorio. b) Senilidad. c) Escoliosis. d) Debilidad de la pared torácica. 6. Enfermedades neuromusculares:a) Poliomielitis.b) Tétanos.c) Miastenia gravis. d) Síndrome Guillan Barré. c) Polineuritis. 7. Depresión del centro respiratorio:a) TEC.b) Intoxicación por depresores del SNC ycentro respiratorio. c) Anestesia general. 8. Traumatismo torácico: a) Tórax volante; fracturas costales. 9. Uso de respiradores mecánicos.")
4
INDICACIONES Pacientes adultos intubados en UCI: Remover el TET.
Ayudar en el destete de la ventilación mecánica. Facilitar la limpieza pulmonar. Obstrucción de la vía aérea superior Protección de la Vía aérea. Prevenir complicaciones intubación prolongada Debilidad neuromuscular Alteración conciencia 2/3 partes de traqueso reali actal/: Al momento no existen criterios objetivos validados para la indicacion de una traqueostomi Tracheostomy is performed in about a quarter of ICU patients requiring prolonged mechanical ventilation, weaning from assisted ventilation, airway suction and airway protection. Tracheostomy improves patient comfort compared with standard intubation. Tracheostomy performed early upon ICU admission has not shown survival benefits. Percutaneous dilatational techniques are commonly used because the procedure can be performed at the bedside. Surgical tracheostomy is often reserved for cases with abnormal anatomy or failed percutaneous tracheostomy. It is not known which of the percutaneous techniques is safer in terms of perioperative complications. Ultrasound scanning of the neck and routine endoscopy during the procedure appear to reduce early complications. Decannulation is often delayed and an intensivist-led follow-up may facilitate timely removal of tracheostomy tubes in step down areas or wards.

5
VENTAJAS TRAQUEOSTOMÍA UCI
Confort del paciente Movilización temprana ↓ UCI y hospital Temprana: No ↑ mortalidad y puede mejorar: TEC y críticos ↓ Neumonía ventilador y mortalidad A poarte de benficios fisiolgios (VD) y operacionales (succión),…… Tracheostomy is one of the most frequent procedures performed in intensive care unit (ICU) patients. Of the many purported advantages of tracheostomy, only patient comfort, early movement from the ICU, and shorter ICU and hospital stay have significant supporting data. Even the belief of increased safety with tracheostomy may not be correct. Various techniques for tracheostomy have been developed; however, use of percutaneous dilation techniques with bronchoscopic control continue to expand in popularity throughout the world. Tracheostomy should occur as soon as the need for prolonged intubation (longer than 14 d) is identified. Accurate prediction of this duration by day 3 remains elusive. Mortality is not worse with tracheotomy and may be improved with earlier provision, especially in head-injured and critically ill medical patients. The timing of when to perform a tracheostomy continues to be individualized, should include daily weaning assessment, and can generally be made within 7 days of intubation. Bedside techniques are safe and efficient, allowing timely tracheostomy with low morbidity. TEC y críticos si taqieos precoz FOB though definitely advantageous over CPCT in terms of lesser complications and being highly useful in the obese, short necked, and those with scar marks, is not without drawbacks such as requirement of additional staff and increased expenditure. The main being inability to be used in patients with low respiratory reserve. Overall it would be complimentary for any ICU to have FOB facility and must be used in select group of patients Respir Care Aug;55(8):
 y operacionales (succión),…… Tracheostomy is one of the most frequent procedures performed in intensive care unit (ICU) patients. Of the many purported advantages of tracheostomy, only patient comfort, early movement from the ICU, and shorter ICU and hospital stay have significant supporting data. Even the belief of increased safety with tracheostomy may not be correct. Various techniques for tracheostomy have been developed; however, use of percutaneous dilation techniques with bronchoscopic control continue to expand in popularity throughout the world. Tracheostomy should occur as soon as the need for prolonged intubation (longer than 14 d) is identified. Accurate prediction of this duration by day 3 remains elusive. Mortality is not worse with tracheotomy and may be improved with earlier provision, especially in head-injured and critically ill medical patients. The timing of when to perform a tracheostomy continues to be individualized, should include daily weaning assessment, and can generally be made within 7 days of intubation. Bedside techniques are safe and efficient, allowing timely tracheostomy with low morbidity. TEC y críticos si taqieos precoz. FOB though definitely advantageous over CPCT in terms of lesser complications and being highly useful in the obese, short necked, and those with scar marks, is not without drawbacks such as requirement of additional staff and increased expenditure. The main being inability to be used in patients with low respiratory reserve. Overall it would be complimentary for any ICU to have FOB facility and must be used in select group of patients. Respir Care Aug;55(8):")
6
CONTRAINDICACIONES: Experiencia
Anatomía severa/ distorsionada: Masas, radiación, Cx mayor Anatomía no favorable : Obesos??. Masa en línea media del cuello. Arteria innominada alta. Coagulopatía no corregida?? Ear Nose Throat J Aug;89(8):387-95 Vía aérea no protegida. Niños PEEP > 20 cm H2O. Infección localizada Tiroides grande La 1a absoulta, las otras relativas: experiencia Coagulopathy is one of the relative contraindications to percutaneous dilational tracheostomy (PDT). We conducted a retrospective analysis of the records of 483 patients who had undergone PDT at Johns Hopkins Hospital from January 2000 through December 2007 to investigate the safety of PDT in those who were coagulopathic. The number of patients classified as coagulopathic varied greatly according to the particular diagnostic criteria used; 164 patients (33.95%) met one of the three diagnostic criteria (an abnormality in either prothrombin time, partial thromboplastin time, or platelet count), and 32 patients (6.63%) met two or three of these criteria. Complications occurred in 16 patients (3.31%), none of whom met two or more diagnostic criteria; bleeding accounted for 5 of these complications (1.04%). No statistically significant difference was seen in complication rates between the coagulopathic patients and the controls (noncoagulopathic patients). We conclude that in the hands of an experienced surgeon, PDT can be safely performed in patients with abnormal coagulation factors provided that the surgical team strictly adheres to a standardized protocol Experiencia: Para que un operador haya superado su curva de aprendizaje y sea considerado un experto, debe haber realizado al menos 30 TP
: Vía aérea no protegida. Niños. PEEP > 20 cm H2O. Infección localizada Tiroides grande. La 1a absoulta, las otras relativas: experiencia. Coagulopathy is one of the relative contraindications to percutaneous dilational tracheostomy (PDT). We conducted a retrospective analysis of the records of 483 patients who had undergone PDT at Johns Hopkins Hospital from January 2000 through December 2007 to investigate the safety of PDT in those who were coagulopathic. The number of patients classified as coagulopathic varied greatly according to the particular diagnostic criteria used; 164 patients (33.95%) met one of the three diagnostic criteria (an abnormality in either prothrombin time, partial thromboplastin time, or platelet count), and 32 patients (6.63%) met two or three of these criteria. Complications occurred in 16 patients (3.31%), none of whom met two or more diagnostic criteria; bleeding accounted for 5 of these complications (1.04%). No statistically significant difference was seen in complication rates between the coagulopathic patients and the controls (noncoagulopathic patients). We conclude that in the hands of an experienced surgeon, PDT can be safely performed in patients with abnormal coagulation factors provided that the surgical team strictly adheres to a standardized protocol. Experiencia: Para que un operador haya superado. su curva de aprendizaje y sea considerado un experto, debe haber realizado al menos 30 TP.")
7
Momento Traqueostomía ??
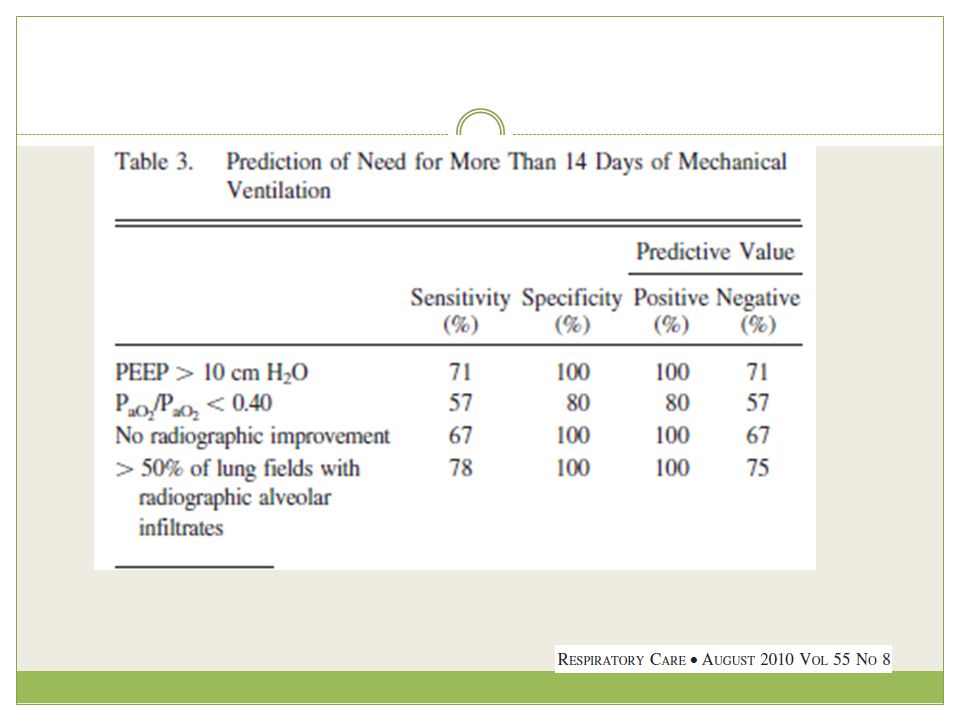
Individualizado: Evaluación diaria de weaning Primeros 7 días Identificación de intubación prolongada(+14 d) – predicción difícil Al lado del pte: Segura, eficiente, rápida , baja morbilidad Pacientes cuyo diagnostico anticipa la necesidad de ventilacion mecanica prolongada (> 10 - 14 dias), como por ejemplo, enfermos con sindrome de distres respitarorio agudo grave (indice de oxigenacion ≥ 15 y/o PaO2/FiO2 ≤ 100) pancratitis aguda grave complicada, lesion de medula cervical alta, sindrome de Gillain-Barre de variedad axonal. 1) Ausencia de criterios validados para identificar a aquellos pacientes que se beneficiaran de una traqueostomia temprana, 2) Carencia de una definicion consensuada sobre el periodo de tiempo considerado como temprano, y 3) La falta de estudios con un adecuado diseno metodologico y poder estadistico que respondan la interrogante. Predictores intub + 14 dìas(buena sensib y VPP:100%): PEEP +10, no mejorìa radiogràfica, infiltardos alveolares + de 50% CAMPO PULMONARES)
 – predicción difícil. Al lado del pte: Segura, eficiente, rápida , baja morbilidad. Pacientes cuyo diagnostico anticipa la necesidad. de ventilacion mecanica prolongada (> dias), como por ejemplo, enfermos con sindrome. de distres respitarorio agudo grave (indice. de oxigenacion ≥ 15 y/o PaO2/FiO2 ≤ 100) pancratitis aguda grave complicada, lesion de. medula cervical alta, sindrome de Gillain-Barre. de variedad axonal. 1) Ausencia de criterios validados. para identificar a aquellos pacientes que se beneficiaran. de una traqueostomia temprana, 2) Carencia. de una definicion consensuada sobre el periodo de. tiempo considerado como temprano, y 3) La falta. de estudios con un adecuado diseno metodologico y. poder estadistico que respondan la interrogante. Predictores intub + 14 dìas(buena sensib y VPP:100%): PEEP +10, no mejorìa radiogràfica, infiltardos alveolares + de 50% CAMPO PULMONARES)")
9
Hay metanalisis pero heterogenos: el Trachman: Beneficio a 30 dias en mortaidad(1º) 1-4 dìas vs pos 10 dìas: Parece que no diferencia
 1-4 dìas vs pos 10 dìas: Parece que no diferencia")
10
ARDS score: Dìa 4 y 7: PO2a/PO2A, PEEP, progresiòn RX

11
CLASIFICACIÓN TRAQUESTOMÍA ABIERTA
TRAQUEOSTOMÍA PERCUTANEA: - Infx, cicatriz, Tpo, Hgia?? The most recent articles comparing surgical and percutaneous tracheostomies techniques are not able to demonstrate a superiority of one of them in terms of feasibility or safety. In other words, there should be a slight advantage for the percutaneous tracheostomy regarding to the late post-operative complications, as there should be a slight advantage for the surgical techniques regarding to the perioperative complications. The literature analysis point out firstly the learning curve for percutaneous dilational tracheostomy, with a significant decrease of complication incidence with the operator's experience and secondly the continuous endoscopic guidance seems to increase the safety of the percutaneous procedure Percutaneous dilatational techniques are commonly used because the procedure can be performed at the bedside. Surgical tracheostomy is often reserved for cases with abnormal anatomy or failed percutaneous tracheostomy. It is not known which of the percutaneous techniques is safer in terms of perioperative complications

13
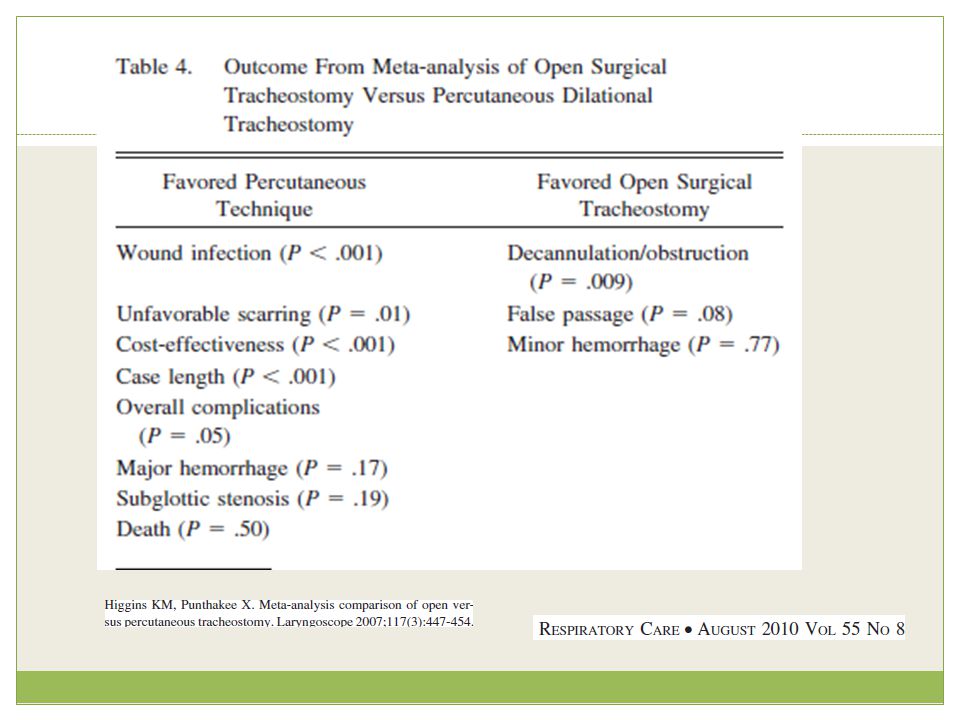
Menos estenosis traqueal: 20% vs 32,5%
CONTROVERSIA: Rata de complicaciones: 7 a favor de PT y 3 de Qx 572/ 576 ptes, 26% dificultades técnicas, 3% complicaciones tempranas, 0,7% compl tardías Colombia, menos estenosis y menos severa: +50% en abierta y no sign (10%) en percu) The choice between surgical (ST) and percutaneous tracheostomy (PT) is not often based on evidence. The aim is to evaluate the quality of evidence in published articles comparing the two methods. A MEDLINE search was done. From 298 articles found, 37 fulfilled the inclusion criteria and 35 were further analyzed. No study was based on type I evidence, 13 (37%) represented type II, in 1 (3%) a clear-cut definition between type II or III was not possible and 21 (60%) represented type III or IV evidence. Taking into account the complication rate of the 13 type II evidence studies, 7 are in favor of PT and 3 in favor of ST. The majority of studies comparing PT with ST are of type III or IV level of evidence. Even if only type II studies are analyzed, outcomes are controversial. Any claims by clinicians in favor of a particular treatment are still debatable. PDT was attempted in 576 patients and successfully completed in 572 PDT was abandoned in four patients due to bleeding, with three of these subsequently undergoing surgical tracheostomy (ST). A tracheostomy was performed on 589 patients during the study period. PDT was attempted in 576 patients and successfully completed in 572. PDT was abandoned in four patients due to bleeding, with three of these subsequently undergoing surgical tracheostomy (ST). ST was performed in 17 patients. Intraoperative technical difficulties were encountered in 149 (26%) cases. Sixteen (3%) procedures were deemed as having early complications. A further four (0.7%) cases had significant late complications including two tracheo-innominate fistulae (TIF). Both TIF patients died as a result of their complications giving a mortality directly attributable to PDT of 0.35%. There were no differences with respect to the occurrence of complications according to grade of operator
 en percu) The choice between surgical (ST) and percutaneous tracheostomy (PT) is not often based on evidence. The aim is to evaluate the quality of evidence in published articles comparing the two methods. A MEDLINE search was done. From 298 articles found, 37 fulfilled the inclusion criteria and 35 were further analyzed. No study was based on type I evidence, 13 (37%) represented type II, in 1 (3%) a clear-cut definition between type II or III was not possible and 21 (60%) represented type III or IV evidence. Taking into account the complication rate of the 13 type II evidence studies, 7 are in favor of PT and 3 in favor of ST. The majority of studies comparing PT with ST are of type III or IV level of evidence. Even if only type II studies are analyzed, outcomes are controversial. Any claims by clinicians in favor of a particular treatment are still debatable. PDT was attempted in 576 patients and successfully completed in 572. PDT was abandoned in four patients due to bleeding, with three of these subsequently undergoing surgical tracheostomy (ST). A tracheostomy was performed on 589 patients during the study period. PDT was attempted in 576 patients and successfully completed in 572. PDT was abandoned in four patients due to bleeding, with three of these subsequently undergoing surgical tracheostomy (ST). ST was performed in 17 patients. Intraoperative technical difficulties were encountered in 149 (26%) cases. Sixteen (3%) procedures were deemed as having early complications. A further four (0.7%) cases had significant late complications including two tracheo-innominate fistulae (TIF). Both TIF patients died as a result of their complications giving a mortality directly attributable to PDT of 0.35%. There were no differences with respect to the occurrence of complications according to grade of operator.")
15
TRAQUESTOMÍA PERCUTANEA
EVALUACIÓN PREOPERATORIA H.C Y E.F EVALUAR ANATOMÍA CERVICAL: (horquilla y cricoides) PARACLÍNICOS Rx de Tórax Hb TP – INR – TPT - Plaquetas CARRO DE VÍA AÉREA PERSONAL 4 personas: 2 médicos, 1 terapista respiratoria, 1 enfermera. Requisitos previos Consentimiento informado firmado por familiares Pruebas de coagulación adecuadas (Plaq > , TP > 70%, TTPA N) Checklist de insumos y equipos 1 procedimiento (derecha) 1 fibroscopio (cabezera) 1 técnico respiratorio (parámetros y tubo), a la izquierda 1 enfermera (medicación, signos, instrum
 PARACLÍNICOS. Rx de Tórax. Hb. TP – INR – TPT - Plaquetas. CARRO DE VÍA AÉREA. PERSONAL. 4 personas: 2 médicos, 1 terapista respiratoria, 1 enfermera. Requisitos previos. Consentimiento informado firmado por familiares Pruebas de coagulación adecuadas (Plaq > , TP > 70%, TTPA N) Checklist de insumos y equipos. 1 procedimiento (derecha) 1 fibroscopio (cabezera) 1 técnico respiratorio (parámetros y tubo), a la izquierda. 1 enfermera (medicación, signos, instrum.")
16
TÉCNICAS SHELDEN SCHACHNER TÉCNICA DE CIAGLIA TÉCNICA DE FANTONI
TÉCNICA DE GRIGGS

17
TRAQUESTOMÍA PERCUTANEA
EQUIPOS KIT COOK (ORIGINAL): 7 DILATADORES CURVOS DESDE 12 – 36 FR KIT COOK ÚNICO DILATADOR FIBROBRONCOSCOPIO ??: Complicaciones: 8,3% vs 16,8% ECOGRAFIA ?? Metaanalisi fibro: 8,3%...
: 7 DILATADORES CURVOS DESDE 12 – 36 FR. KIT COOK ÚNICO DILATADOR. FIBROBRONCOSCOPIO : Complicaciones: 8,3% vs 16,8% ECOGRAFIA Metaanalisi fibro: 8,3%...")
22
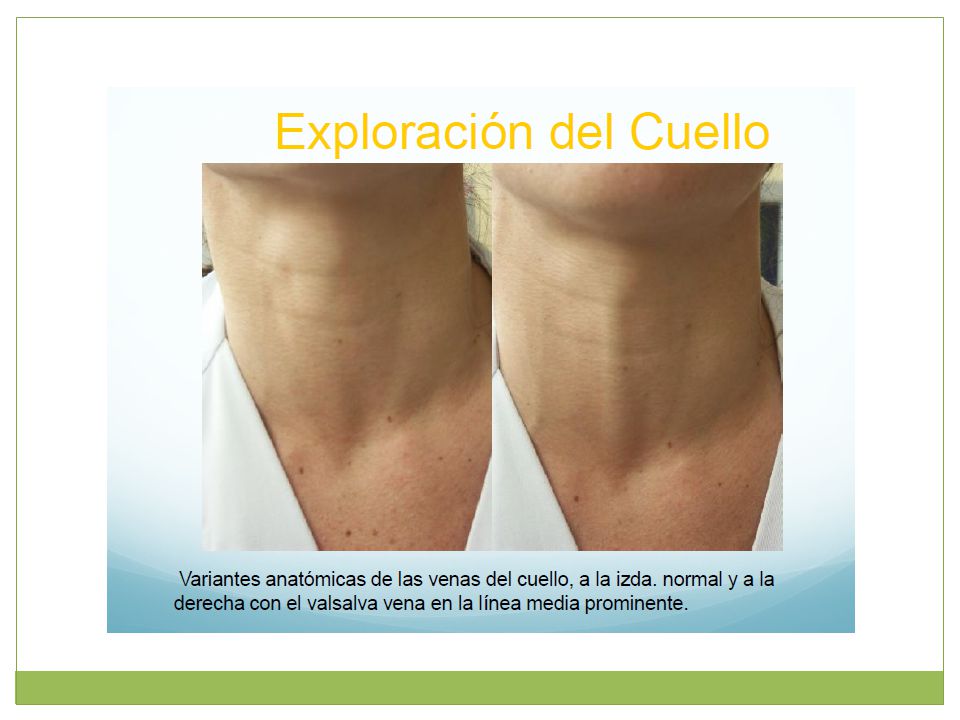
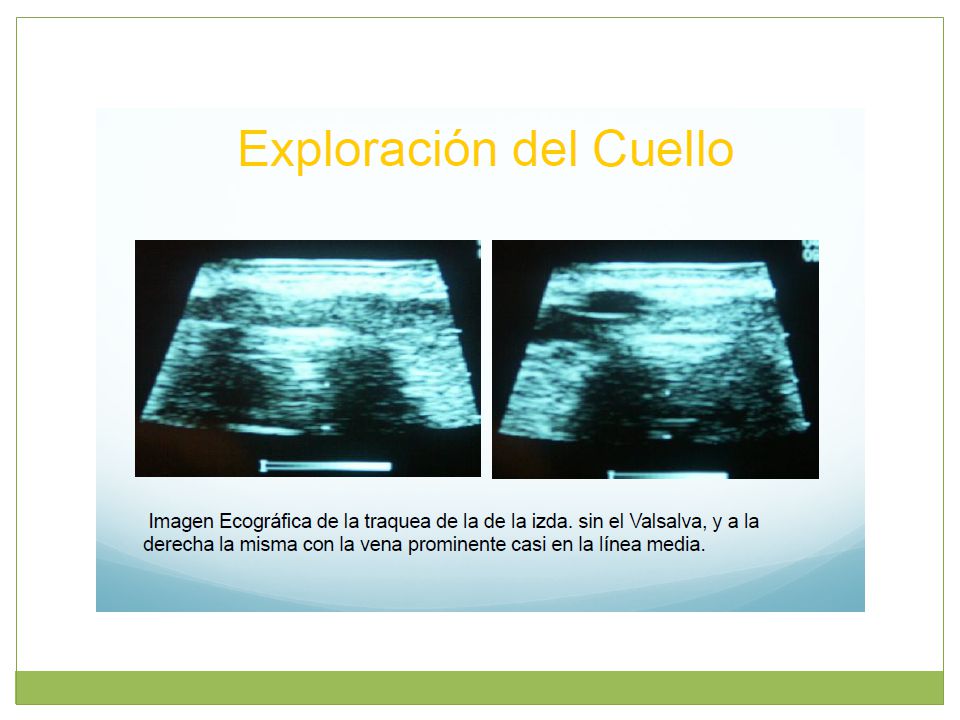
Ecografía Obesidad mórbida y prevención cervical
Percutaneous tracheostomy has become a routine procedure in most intensive care units, and point of care ultrasound is becoming used with greater frequency to augment diagnosis and therapy for critically ill patients. The case series from Rajajee and colleagues incorporates 'real-time' ultrasound in an effort to improve the safety of percutaneous tracheostomy. While their report does not prove that ultrasound should be used prior to or during all percutaneous tracheostomies, it does reinforce several important safety considerations concerning the anatomy of the neck, and in particular the potential to encounter bleeding complications during these procedures. * Ultrasound (US) performed prior to percutaneous tracheostomy (PT) may be useful in avoiding injury to pretracheal vascular structures and in avoiding high placement of the tube: Mechanically ventilated patients with acute brain injury requiring tracheostomy underwent US guided PT. The orotracheal tube was withdrawn using direct laryngoscopy. The trachea was punctured under real-time US guidance (with visualization of the needle path) while using the acoustic shadows of the cricoid and the tracheal rings to identify the level of puncture. After guidewire passage the site and level of entry was verified using the bronchoscope, which was then withdrawn. Following dilatation and tube placement, placement in the airway was confirmed using auscultation and the "lung sliding" sign on US. Bronchoscopy and chest X-ray were then performed to identify any complications: Thirteen patients successfully underwent US guided PT. Three patients were morbidly obese, two were in cervical spine precautions and one had a previous tracheostomy. In all 13 patients bronchoscopy confirmed that guidewire entry was through the anterior wall and between the first and fifth tracheal rings. There was no case of tube misplacement, pneumothorax, posterior wall injury, significant bleeding or other complication during the procedure. CONCLUSIONS: Percutaneous tracheostomy performed under real-time ultrasound guidance is feasible and appears accurate and safe, including in patients with morbid obesity and cervical spine precautions. Larger studies are required to further define the safety and relative benefits of this technique
 performed prior to percutaneous tracheostomy (PT) may be useful in avoiding injury to pretracheal vascular structures and in avoiding high placement of the tube: Mechanically ventilated patients with acute brain injury requiring tracheostomy underwent US guided PT. The orotracheal tube was withdrawn using direct laryngoscopy. The trachea was punctured under real-time US guidance (with visualization of the needle path) while using the acoustic shadows of the cricoid and the tracheal rings to identify the level of puncture. After guidewire passage the site and level of entry was verified using the bronchoscope, which was then withdrawn. Following dilatation and tube placement, placement in the airway was confirmed using auscultation and the lung sliding sign on US. Bronchoscopy and chest X-ray were then performed to identify any complications: Thirteen patients successfully underwent US guided PT. Three patients were morbidly obese, two were in cervical spine precautions and one had a previous tracheostomy. In all 13 patients bronchoscopy confirmed that guidewire entry was through the anterior wall and between the first and fifth tracheal rings. There was no case of tube misplacement, pneumothorax, posterior wall injury, significant bleeding or other complication during the procedure. CONCLUSIONS: Percutaneous tracheostomy performed under real-time ultrasound guidance is feasible and appears accurate and safe, including in patients with morbid obesity and cervical spine precautions. Larger studies are required to further define the safety and relative benefits of this technique.")
23
Ultrasound scanning of the neck and routine endoscopy during the procedure appear to reduce early complications A FAVOR: Facilita el procedimiento. Mayor seguridad, eliminando el riesgo de falsas rutas. EN CONTRA: Prolonga la duración del procedimiento. Aumenta los costos. Puede dificultar la ventilación del paciente. Percutánea + fibroscopio: Obesos, cuello corto, cicatrices - J Anaesthesiol Clin Pharmacol Oct;26(4):514-6.
:")
24
TRAQUESTOMÍA PERCUTANEA
ANESTESIA Procedimiento altamente estimulante: Anestesia local: Lidocaína + epinefrina (infiltración) Anestesia local: Lidocaína (Intratraqueal) Sedación: Midazolam Fentanyl Propofol Morfina Relajación: Adyuvante Rocuronio
 Anestesia local: Lidocaína (Intratraqueal) Sedación: Midazolam. Fentanyl. Propofol. Morfina. Relajación: Adyuvante. Rocuronio.")
25
AGUJA DILATADOR CORTO DILATADOR ESTABILIZADOR GUÍA DE ALAMBRE EN J BISTURÍ

26
PROCEDIMIENTO (Video**)
PALPAR ESTRUCTURAS ANATÓMICAS

27
PROCEDIMIENTO INCISIÓN PREVIA INFILTRACIÓN

28
PROCEDIMIENTO DISECCIÓN DE TEJIDOS

29
PROCEDIMIENTO RETIRO DEL TET

30
PROCEDIMIENTO PUNCIÓN TRAQUEAL

31
PROCEDIMIENTO REMOVER AGUJA E INTRODUCIR DE LA GUÍA

32
PROCEDIMIENTO DILATADOR CORTO

33
PROCEDIMIENTO ESTABILIZADOR Y DILATADOR

34
PROCEDIMIENTO ENSAMBLAJE Y PASO DEL TUBO DE TRAQUEOSTOMÍA

35
PROCEDIMIENTO ENSAMBLAJE Y PASO DEL TUBO DE TRAQUEOSTOMÍA

36
PROCEDIMIENTO FIJACIÓN DEL TUBO DE TRAQUEOSTOMÍA

37
CONSIDERACIONES POSTOPERATORIAS
Evaluar posibles complicaciones. Monitorización de signos vitales. Rx de Tórax de control ??. Decanulación accidental: reintubar, no intentar pasar cánula. 9. Indicaciones posop RxTx post-procedimiento: Cánula y complicaciones Reiniciar heparina, aspirina y similares 12 horas post-procedimiento Control semanal del paciente (hasta su decanulación). Llenar ficha de protocolo. Cabecera 35º x 1h Ungüento antibiótico c/8h x 3 días
. Llenar ficha de protocolo. Cabecera 35º x 1h. Ungüento antibiótico c/8h x 3 días.")
38
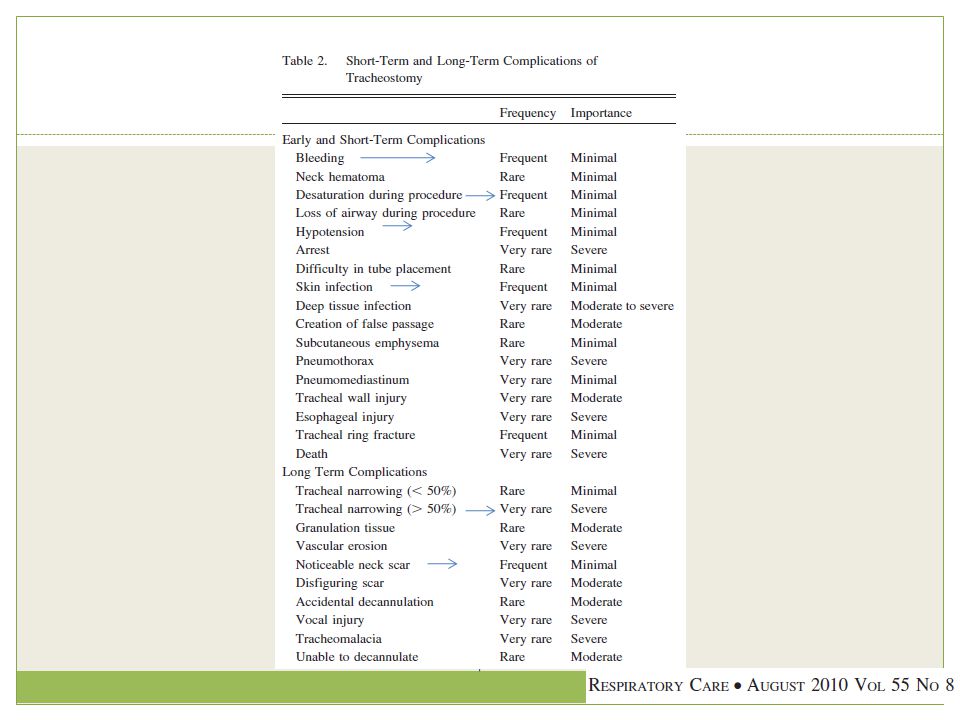
COMPLICACIONES INTRAOPERATORIAS POSTOPERATORIAS SANGRADO FISTULA T-E
NEUMOTORAX NEUMOMEDIASTINO LESIÓN DEL NLR LESIÓN DEL CRICOIDES PARO CARDIORESPIRATORIO POSTOPERATORIAS SANGRADO INFECCIÓN ENFISEMA SC PROBLEMAS DE DEGLUCIÓN OBSTRUCCIÓN DEL TUBO DESPLAZAMIENTO DEL TUBO GRANULOMA FÍSTULAS ESTENOSIS L-T Decannulation is often delayed and an intensivist-led follow-up may facilitate timely removal of tracheostomy tubes in step down areas or wards. insercion paratraqueal de la canula de traqueostomia o laceracion de la pared posterolateral de la traquea Intraoperatorias – Hemorragia: Venas yugulares anteriores – Paro cardiorespiratorio: reflejo vasovagal – Neumotórax o neumomediastino: Lesión de la pleura • Postoperatorias inmediatas – Hemorragia – Infección de la herida – Enfisema subcutáneo: escape de aire de la VM a tejidos blandos – Obstrucción del tubo – Desplazamiento del tubo – Broncoaspiración: disminución de reflejos laringeos Postoperatorio tardío – Fístula de la arteria innominada: Lesión directa de la Art. Inominada. – Estenosis traqueal: por la TQT o balón Formación de granulomas – Fístula traqueo – esofágica: Presión de la pared posterior. – Fístula traqueo – cutánea: por epitelización del estoma en ptes con TQT permanentes

39
COMPLICACIONES Las complicaciones perioperatorias (hasta 24 horas después del procedimiento) fluctúan ente el 2 a 6% ocurriendo falsa vía, muerte, hemorragia, extubación, neumotórax, enfisema, hipotensión e imposibilidad de realizar la técnica.15,17,18 Las complicaciones (percutanea) postoperatorias (después de 24 horas del procedimiento) se presentan entre el 9 a 17% pudiendo presentarse neumotórax, infección, hemorragias, desplazamiento del tubo, e incluso muerte.14-17
 fluctúan ente el 2 a 6% ocurriendo falsa vía, muerte, hemorragia, extubación, neumotórax, enfisema, hipotensión e imposibilidad de realizar la. técnica.15,17,18. Las complicaciones (percutanea) postoperatorias (después de 24 horas del procedimiento) se presentan entre el 9 a 17% pudiendo presentarse neumotórax, infección, hemorragias, desplazamiento del tubo, e incluso muerte")
41
CONCLUSIONES TPC (Ciaglia Blue Rhino) es una alternativa segura y simple técnicamente a la traqueostomía qx. Necesidad de consenso para momento de TPC Elimina la necesidad de traslado del paciente a la UCI. Uso de fibroscopio y US en algunos pacientes Traqueostomía temprana puede ↓ días ventilación y UCI CONCLUSION: Since there has been a great deal of percutaneous tracheostomy in the intensive care units, the incidence of tracheostomy have increased in those services. There is a trend to replace the surgical procedure by the percutaneous one. However, according to the potentially jeopardizing complications, percutaneous tracheostomy should be done by an experienced operator with the help of a continuous endoscopic guidance.

Presentaciones similares