Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Electrolitos Sesión Magistral Dra. Adria Tinoco R1MI
Asesor: Dr. Ignacio Rangel Programa Multicéntrico de Residencias Médicas Enero de 2015

2
Abreviaturas ICF: Líquidos Intracelulares OsmU: Osmolaridad Urinaria
RK/CrU: Radio Potasio Creatinina Urinario ECF: Líquidos Extracelulares NaU: Sodio Urinario Ca: Calcio Osm.: Osmolaridad Na-K-ATPasa: Sodio-Potasio- ATPasa PO4: Fosforo Na+: Sodio UCI: Unidad de Cuidados Intensivos ATR: Acidosis Tubular Renal K+: Potasio PTH: Paratohormona Sx.: Síndrome S: sérico FA: Fosfatasa Alcalina Inf: Infundido Vit: Vitamina ACT: Agua corporal total Mg: Miligramos

3
Índice Introducción Trastornos del Sodio Hiponatremia Hipernatremia
Trastornos del Potasio Hipokalemia Hiperkalemia Trastornos del Calcio Trastornos del Fósforo

4
Objetivos Recordar la Fisiología de los Electrolitos
Recordar el Abordaje de los Trastornos Electrolíticos Conocer el manejo agudo de los trastornos Electrolíticos Nuevas tendencias en manejo

5
Sodio

6
Introducción Alteración electrolítica más frecuentemente
10% de los pacientes admitidos a urgencias sufre Hiponatremia y 2% Hipernatremia La mayoría de los síntomas secundarios a disnatremias son neurológicos, y en algunos casos devastadores Irregularities of sodium and water balance most often occur simultaneously and are some of the most common electrolyte abnormalities encountered by emergency medicine physicians. Approximately 10% of all patients admitted from the emergency department suffer from hyponatremia and 2% suffer from hypernatremia.1 Becauseof the close nature of sodium and water balance, and the relatively rigid limits placed on the central nervous system by the skull, it is not surprising that most symptoms related to disorders of sodium and water imbalance are neurologic and can, therefore, be devastating. Several important concepts are crucial to the understanding of these disorders, the least of which include body fluid compartments, regulation of osmolality, and the need for rapid identification and appropriate management The difference between a minor symptom and a life-threatening condition caused by a sodium imbalance is often a result of the rapidity of the change in sodium concentration, not necessarily the overall deficit; and how quickly the imbalance is recognized and then treated by clinicians. Because emergency physicians do not always have the most complete background information on their patients in acute settings, this article delineates the types of sodium and water imbalances, the symptoms and signs the clinician encounters, pitfalls and complications of correcting these imbalances too aggressively, and how to base initial management of these patients. Sodium and water disorders occur simultaneously and most commonly affect the neurologic system, potentially leading to devastating outcomes Sterns R. Disorders of Plasma Sodium –Causes, Consequences, and Correction. N Engl J M 2015; 372: 55-65 Harring T. Disorders of Sodium and Water Balance. Emerg Med Clin N Am 32 (2014);
;")
7
Fisiología El sodio representa el soluto más importante en el espacio extracelular Concentración normal: 140 mEq/L Peso Corporal Total Agua Corporal Total 60% Otros Tejidos 40% ICF ECF 20% Intersticial 15% Intra vascular 5% The primary solute of the ECF is sodium, with a normal concentration of 140 mEq/L. As the concentration of sodium changes, neurologic symptoms may begin to manifest because of the confining nature of the skull. These symptoms may be minor or they can lead to life-threatening conditions Adaptado de: Harring T. Disorders of Sodium and Water Balance. Emerg Med Clin N Am 32 (2014);
;")
8
Osmolaridad Plasmática mOsm/kgf
Fisiología Osmolaridad normal: mOsm/L H2O Sedf Osmolaridad Plasmática mOsm/kgf A D Hf Hipotálamo Hipófisis Riñón Nefrona Reguladores: 1.- Vasopresina 2.- Sed Plasma osmolality, with detected changes as small as 1% to 2%,5 is the most common stimulus for ADH release; however, other factors can stimulate ADH release, including decreased intravascular volume, decreased blood pressure, pain, anxiety, nausea, pregnancy, menstruation, hypoglycemia, severe hypoxemia, hypercapnia, third spacing of fluids (eg, burns, trauma, pancreatitis), and certain drugs Relation between plasma antidiuretic hormone (ADH) concentration and plasma osmolality in normal humans in whom the plasma osmolality was changed by varying the state of hydration. The osmotic threshold for thirst is a few mosmol/kg higher than that for ADH. Harring T. Disorders of Sodium and Water Balance. Emerg Med Clin N Am 32 (2014); Robertson GL, Aycinena P, Zerbe RL. Am J Med 1982; 72:339.
, and certain drugs. Relation between plasma antidiuretic hormone (ADH) concentration and plasma osmolality in normal humans in whom the plasma osmolality was changed by varying the state of hydration. The osmotic threshold for thirst is a few mosmol/kg higher than that for ADH. Harring T. Disorders of Sodium and Water Balance. Emerg Med Clin N Am 32 (2014); Robertson GL, Aycinena P, Zerbe RL. Am J Med 1982; 72:339.")
9
Hiponatremia Concentración de sodio sérico por debajo de 135 mEq/L
Prevalencia estimada entre 3-6 millones de personas en EUA Alteración primaria del balance corporal de agua The nature of underlying illness rather than the severity of hyponatremia best explains mortality associated with hyponatremia. Neurologic complications from hyponatremia are uncommon among patients who die with hyponatremia. Hyponatraemia is primarily a disorder of water balance, with a relative excess of body water compared to total body sodium and potassium content. It is usually associated with a disturbance in the hormone that governs water balance, vasopressin Harring T. Disorders of Sodium and Water Balance. Emerg Med Clin N Am 32 (2014); Waikar SS, Mount DB, Curhan GC. Mortality after hospitalization with mild, moderate, and severe hyponatremia. Am J Emerg Med 2009;122:857–65
; Waikar SS, Mount DB, Curhan GC. Mortality after hospitalization with mild, moderate, and severe hyponatremia. Am J Emerg Med 2009;122:857–65.")
10
Hiponatremia Riesgo de mortalidad 33% mayor que en pacientes con niveles de sodio normales ¿Contribución directa a mortalidad? La naturaleza de la enfermedad subyacente más que la hiponatremia explica la mortalidad asociada Harring T. Disorders of Sodium and Water Balance. Emerg Med Clin N Am 32 (2014); Waikar SS, Mount DB, Curhan GC. Mortality after hospitalization with mild, moderate, and severe hyponatremia. Am J Emerg Med 2009;122:857–65
; Waikar SS, Mount DB, Curhan GC. Mortality after hospitalization with mild, moderate, and severe hyponatremia. Am J Emerg Med 2009;122:857–65.")
11
Cuadro Clínico Cerebro Normal Estado Hipotónico Ganancia de Agua Rápida Adaptación Pérdida de Sodio, Potasio y Cloro Agua Adaptación Lenta Pérdida de Osmoles Orgánicos Mielinolisis Osmótica Corrección Rápida e Inapropiada Los síntomas se relacionan con el nivel y la rapidez en la instauración de la hiponatremia Edema Cerebral: Cefalea, nausea, vómito, debilidad, anorexia, letargia y confusión Symptoms of hyponatremia can range from mild to severe: some patients are asymptomatic, others present with seizures. The symptoms are typically related to the level and rapidity of sodium change and to the presence and degree of cerebral edema. As water moves into brain cells, the serum sodium level decreases; patients begin to have headache, nausea, vomiting, restlessness, anorexia, muscle cramps, lethargy, and confusion. The brain attempts to adapt quickly to hyponatremia by losing other intracellular solutes to decrease the chance of cerebral edema,12 which then becomes a factor in treatment. Most patients with symptomatic hyponatremia have some sort of neurologic complaint; however, some may present with a traumatic complaint, such as after a fall.1 If hyponatremia is not stabilized or corrected, patients can decompensate to seizures, coma, or even death. Adaptado de: Spasovski G et al. Clinical practice guideline on diagnosis and treatment of hyponatraemia. Clinical Practice Guideline. European Journal of Endocrinology (2014); 170, G1-G47.
; 170, G1-G47.")
12
Cuadro Clínico Severidad Síntoma Moderadamente Severa
Nausea sin vómito Confusión Cefalea Severa Vómito Distress Respiratorio Convulsiones Alteración estado mental Sterns R. Disorders of Plasma Sodium –Causes, Consequences, and Correction. N Engl J M 2015; 372: 55-65 Spasovski G et al. Clinical practice guideline on diagnosis and treatment of hyponatraemia. Clinical Practice Guideline. European Journal of Endocrinology (2014); 170, G1-G47.
; 170, G1-G47.")
13
Hiponatremia ¿Edema Cerebral? Tratamiento Urgente Osmolaridad Sérica
Osm. Plasmática: 2(Na) + (Glu/18) <275 mOsm/kg mOsm/kg >295 mOsm/kg Evaluación del Volumen Corporal Medición de Osmolaridad Urinaria Hiperproteinemia Hiperlipidemia Hiperglicemia Manitol Glicina (Sodio Sérico x 2) + (Glucosa/18) Singer GG. Fluid and electrolyte management. In: Carey CF, Lee HH, Woeltje KF, editors. The Washington manual of medical therapeutics. 29th ed. Philadelphia: Lippincott-Raven; 1998, p. 44
 + (Glu/18) <275 mOsm/kg mOsm/kg. >295 mOsm/kg. Evaluación del Volumen Corporal. Medición de Osmolaridad Urinaria. Hiperproteinemia. Hiperlipidemia. Hiperglicemia. Manitol. Glicina. (Sodio Sérico x 2) + (Glucosa/18) Singer GG. Fluid and electrolyte management. In: Carey CF, Lee HH, Woeltje KF, editors. The Washington manual of medical therapeutics. 29th ed. Philadelphia: Lippincott-Raven; 1998, p. 44.")
14
Hiponatremia Hipoosmolar
Osm Urinaria >100 mOsm/kg Hipovolémica Euvolémica Hipervolémica Osm. Urinaria <100 mOsm/kg Polidipsia Primaria Ingesta baja de Solutos Vómitos Diarrea Quemaduras Diuréticos SIAD Hipotiroidismo Déficit de Glucocorticoides Insuficiencia Cardiaca Cirrosis Nefrosis Singer GG. Fluid and electrolyte management. In: Carey CF, Lee HH, Woeltje KF, editors. The Washington manual of medical therapeutics. 29th ed. Philadelphia: Lippincott-Raven; 1998, p. 44

15
Tratamiento Demielinización Osmótica Edema Cerebral
Disminución Rápida del Sodio Sérico Hipernatremia Aguda Hiponatremia Aguda Corrección Rápida de Hiponatremia Crónica Corrección Rápida de Hipernatremia Crónica Aumento Rápido del Sodio Sérico Adaptado de: Sterns R. Disorders of Plasma Sodium –Causes, Consequences, and Correction. N Engl J M 2015; 372: 55-65

16
Tratamiento Tratamiento de Urgencia en pacientes Inestables
Edema Cerebral Solución Salina Hipertónica al 3% a 2 ml/kg en minutos Puede repetirse una o dos veces más si continúan los síntomas severos La corrección concomitante de Hipokalemia contribuirá al aumento del sodio sérico Monitoreo estrecho del sodio sérico cada 1-2 horas In a patient who is actively seizing, is neurologically compromised, or has respiratory arrest caused by hyponatremia, a bolus of hypertonic saline, given as 3% normal saline (NS) at a dose of 2 mL/kg (maximum 100 mL) should be given.2,7,70–72 The bolus should be given over 10 to 60 minutes and can be repeated once if severe symptoms are still evident. A bolus of 2 mL/kg increases the serum sodium level by approximately 2 mEq/L. This increase in serum sodium level should stop current symptoms and prevent other severe neurologic consequences. During infusion of hypertonic saline, the patient and the serum sodium levels much be monitored closely to look for any signs of deteriorating neurologic status or symptoms of fluid overload, which may dictate further management. Keep in mind that if hypokalaemia is present, correction of the hypokalaemia will contribute to an increase in serum sodium concentration. Sterns R. Disorders of Plasma Sodium –Causes, Consequences, and Correction. N Engl J M 2015; 372: 55-65 Spasovski G et al. Clinical practice guideline on diagnosis and treatment of hyponatraemia. Clinical Practice Guideline. European Journal of Endocrinology (2014); 170, G1-G47.
 at a dose of 2 mL/kg (maximum 100 mL) should be. given.2,7,70–72 The bolus should be given over 10 to 60 minutes and can be repeated. once if severe symptoms are still evident. A bolus of 2 mL/kg increases the serum sodium. level by approximately 2 mEq/L. This increase in serum sodium level should stop. current symptoms and prevent other severe neurologic consequences. During infusion. of hypertonic saline, the patient and the serum sodium levels much be monitored. closely to look for any signs of deteriorating neurologic status or symptoms of fluid. overload, which may dictate further management. Keep in mind that if hypokalaemia is present, correction. of the hypokalaemia will contribute to an increase in. serum sodium concentration. Sterns R. Disorders of Plasma Sodium –Causes, Consequences, and Correction. N Engl J M 2015; 372: Spasovski G et al. Clinical practice guideline on diagnosis and treatment of hyponatraemia. Clinical Practice Guideline. European Journal of Endocrinology (2014); 170, G1-G47.")
17
Δ[Na+]s={[Na++K+]inf-[Na+]S}/[ACT+1]
Tratamiento Hiponatremia Moderada/Severa Tratamiento orientado en la etiología Restringir la corrección a <10 mmol/l en las primeras 24 horas y <18 mmol/l en las primeras 48 horas. Adrogué Madiás: Δ[Na+]s={[Na++K+]inf-[Na+]S}/[ACT+1] Systematic review of the cases of osmotic demyelination syndrome published during the past 15 years generally supports restricting increases in serum sodium concentration !10 mmol/l in the first 24 h and !18 mmol/l in the first 48 h. It is very difficult, if not impossible, to set ‘safe’ rate limits for correcting hyponatraemia Hyponatremia. Adrogué HJ, Madias NE: N Engl J Med 342: 1581–1589, 2000 Spasovski G et al. Clinical practice guideline on diagnosis and treatment of hyponatraemia. Clinical Practice Guideline. European Journal of Endocrinology (2014); 170, G1-G47.
![Δ[Na+]s={[Na++K+]inf-[Na+]S}/[ACT+1]](http://slideplayer.es/slide/5771715/18/images/17/%CE%94%5BNa%2B%5Ds%3D%7B%5BNa%2B%2BK%2B%5Dinf-%5BNa%2B%5DS%7D%2F%5BACT%2B1%5D.jpg "Tratamiento. Hiponatremia Moderada/Severa. Tratamiento orientado en la etiología. Restringir la corrección a <10 mmol/l en las primeras 24 horas y <18 mmol/l en las primeras 48 horas. Adrogué Madiás: Δ[Na+]s={[Na++K+]inf-[Na+]S}/[ACT+1] Systematic review of the cases of osmotic demyelination. syndrome published during the past 15 years generally. supports restricting increases in serum sodium concentration. !10 mmol/l in the first 24 h and !18 mmol/l. in the first 48 h. It is very difficult, if not impossible, to. set ‘safe’ rate limits for correcting hyponatraemia. Hyponatremia. Adrogué HJ, Madias NE: N Engl J Med 342: 1581–1589, Spasovski G et al. Clinical practice guideline on diagnosis and treatment of hyponatraemia. Clinical Practice Guideline. European Journal of Endocrinology (2014); 170, G1-G47.")
18
Tratamiento Hiponatremia Hipervolémica Hiponatremia Hipovolémica
Restricción de Líquidos Diuréticos Mejorar el Volumen Arterial Efectivo ¿Vaptanes? Hiponatremia Hipovolémica Reposición de Volumen Peri A. The use of vaptans in clinical endocrinology. J Clin Endocrinol Metab 2013;98:1321–32. Spasovski G et al. Clinical practice guideline on diagnosis and treatment of hyponatraemia. Clinical Practice Guideline. European Journal of Endocrinology (2014); 170, G1-G47.
; 170, G1-G47.")
19
Tratamiento Hiponatremia Euvolémica Restricción de Líquidos
Manejo de la causa subyacente Vaptanes Urea Demeclociclina Peri A. The use of vaptans in clinical endocrinology. J Clin Endocrinol Metab 2013;98:1321–32. Spasovski G et al. Clinical practice guideline on diagnosis and treatment of hyponatraemia. Clinical Practice Guideline. European Journal of Endocrinology (2014); 170, G1-G47.
; 170, G1-G47.")
20
Vaptanes Urea Descanso Sodio Sérico Meses
Soupart A et al. Efficacy and Tolerance of Urea Compared with Vaptans for Long-Term Treatment of Patients with SIADH. Clin J Am Soc Nephrol 2012, 7:

21
Hipernatremia Concentración de Sodio Sérico >145 mEq/L
Deshidratación Intracelular secundaria a disminución del agua corporal total Disminución del consumo de agua libre Población en riesgo: ancianos, niños, pacientes en coma o en ventilación invasiva Lindner G, Funk GC. Hypernatremia in critically ill patients. J Crit Care 2013;28: 216.e11–20 Harring T. Disorders of Sodium and Water Balance. Emerg Med Clin N Am 32 (2014);
;")
22
Signos y Síntomas Letargo, rigidez de nuca, mioclonus, corea, convulsiones, hemorragia intracerebral Alteraciones en la contracción ventricular Rabdomiolisis Other consequences of hypernatremia include decreased left ventricular contractility, hyperventilation, impaired glucose use, muscle cramps, and rhabdomyolysis.99 Patients may present with lethargy, weakness, or restlessness; infants may present with irritability. Neurologic examination may show increased tone, nuchal rigidity, brisk reflexes, myoclonus, asterixis, chorea, or seizures.87 If not assessed and treated appropriately, the patient may progress to seizures, coma, or death.3,12,101 One study1 found that patients with hypernatremia are less likely to receive specific care for the dysnatremia, and have higher in-hospital mortality. Symptoms are again related not only to the absolute increase in serum sodium levels but also to the rapidity at which the increase occurs, because this correlates with the speed of brain cell dehydration.

23
Hipernatremia Status de Volumen Hipovolemia Euvolemia Hipervolemia
NaU>20 NaU<20 Soluciones Hipertónicas Ingestión de Sal Aldosteronismo OsmU>300 OsmU<300 Adipsia Pacientes críticos Pérdidas Extra renales 20 Pérdidas Renales 20 Diabetes Insípida20 Diuresis Osmótica DI Parcial Diuréticos Adrogue HJ, Madias NE: Hypernatremia. N Engl J Med 342:1493, 2000 Harring T. Disorders of Sodium and Water Balance. Emerg Med Clin N Am 32 (2014);
;")
24
Tratamiento Sustitución del déficit de agua libre y reducción de las pérdidas La Resucitación de volumen es siempre una prioridad, sin importar la gravedad de la hipernatremia Tratamiento Etiológico Los objetivos del tratamiento de la hipernatremia incluyen tanto la sustitución del déficit de agua libre y la prevención o reducción de la pérdida de agua permanente. La cantidad, la ruta, y la tasa de sustitución dependen de la gravedad de los síntomas, la frecuencia de aparición, las condiciones clínicas concurrentes, y el estado del volumen. Reanimación de volumen es siempre una prioridad, sin importar la gravedad de la hipernatremia. El agotamiento de líquido extracelular en el entorno de inestabilidad hemodinámica siempre debe ser corregido con solución salina normal antes de que se dirigió el déficit de agua. Es importante centrarse en el tratamiento de la hiponatremia, ya que con frecuencia las complicaciones de hipernatremia no son el resultado de la propia alteración electrolítica sino de corrección o tratamiento inadecuado. Gestión de la hipernatremia debe incluir la identificación de la causa subyacente, además de la corrección del estado hipertónico. El tratamiento de la hiponatremia puede, con mayor frecuencia, se desglosa en los siguientes siete pasos Lin M, Liu SJ, Lim IT. Disorders of water imbalance. Emerg Med Clin North Am 2005;23:749–70 Lindner G, Kneidinger N, Holzinger U, et al. Tonicity balance in patients with hypernatremia acquired in the intensive care unit. Am J Kidney Dis 2009;54:674–9.

25
Tratamiento en 7 pasos: Paso 1 Determine el estado de volumen Paso 2
Calcule el Déficit de Agua Libre Paso 3 Tipo de Solución a utilizar Paso 4 Determinar la velocidad de Infusión Paso 5 Estimar las Pérdidas Sensibles Paso 6 Estimar las Pérdidas Insensibles Paso 7 Determine la causa subyacente Solución Sodio Infundido (mEq/L) Distribución en EEC (%) Distribución intravascular (%) Sol. Glucosada 5% 33 (1/3) 8 0.225 NaCl en Sol. Glucosada 5% 38.5 50 12.5 0.45% NaCl 77 62.5 15.5 Ringer Lactato 130 100 25 0.9% NaCl 154 Step 4. Determine rate of repletion. The rate of correction of serum [Na+] is recommended to be approximately 0.5 mEq/L/hr, or a decrease of 10 to 12 mEq/L in a 24-hour period. There have not been any human studies performed to substantiate the appropriateness of this rate. However, based on animal studies, this reflects the observed rate of cerebral de-adaptation, or the rate at which the brain is able to shed electrolytes and idiogenic osmoles acquired in the adaptive response to cellular dehydration. An important exception to this recommended rate of correction occurs in acutelysymptomatic Tasa de Corrección: 0.5 mEq/L/hr o mEq/L en 24 horas Hiponatremia Aguda: 1-2 mEq/L/hr [Na]s: [Na]inf-[Na]s/ACT+1 Déficit de Agua: ACT (Sodio Sérico-140/140) ACT: (0.5 o 0.4)(Peso Corporal) Nguyen MK, Kurtz I: Analysis of current formulas used for treatment of the dysnatremias. Clin Exp Nephrol 8:12, 2004
 Distribución en EEC (%) Distribución intravascular (%) Sol. Glucosada 5% 33 (1/3) NaCl en Sol. Glucosada 5% % NaCl Ringer Lactato % NaCl Step 4. Determine rate of repletion. The rate of correction. of serum [Na+] is recommended to be approximately. 0.5 mEq/L/hr, or a decrease of 10 to 12 mEq/L in a 24-hour. period. There have not been any human studies performed to. substantiate the appropriateness of this rate. However, based. on animal studies, this reflects the observed rate of cerebral. de-adaptation, or the rate at which the brain is able to shed. electrolytes and idiogenic osmoles acquired in the adaptive response. to cellular dehydration. An important exception to this. recommended rate of correction occurs in acutelysymptomatic. Tasa de Corrección: 0.5 mEq/L/hr o mEq/L en 24 horas. Hiponatremia Aguda: 1-2 mEq/L/hr. [Na]s: [Na]inf-[Na]s/ACT+1. Déficit de Agua: ACT (Sodio Sérico-140/140) ACT: (0.5 o 0.4)(Peso Corporal) Nguyen MK, Kurtz I: Analysis of current formulas used for treatment of the dysnatremias. Clin Exp Nephrol 8:12,")
26
Potasio

27
Fisiología 2% 3-5 mmol/L 98% 150 mmol/L Concentración: 50 mEq/L
K 2% 3-5 mmol/L Na 98% 150 mmol/L K Concentración: 50 mEq/L Gradiente de voltaje importante para el Potencial en Reposo Transmembrana Na-K-ATPasa Na K Theisen-Thoupal J. Hypokalemia and Hyperkalemia. Hosp Med Clin 4 (2015) 34–50 Schaefer T. Disorders of Potassium. Emerg Med Clin N Am 23 (2005) 723–747
 34–50. Schaefer T. Disorders of Potassium. Emerg Med Clin N Am 23 (2005) 723–747.")
28
Fisiología Desplazamiento Transcelular Alteración en la Ingesta
Integridad de la Membrana Na-K-ATPasa Concentración de Potasio Status Ácido-Base Osmolaridad Plasmática Desplazamiento Transcelular Alteración en la Ingesta Pérdidas Gastrointestinales Pérdidas Renales Alteración en la Excreción Schaefer T. Disorders of Potassium. Emerg Med Clin N Am 23 (2005) 723–747
 723–747.")
29
Excreción Renal El Riñón elimina más del 90% del potasio corporal
Capaces de disminuir la excreción urinaria de potasio hasta 5 mEq/L La Excreción Renal depende de: 1.- Aldosterona Plasmática 2.- Potasio Plasmático 3.- Concentración de Sodio y Agua que llega al túbulo colector distal Theisen-Thoupal J. Hypokalemia and Hyperkalemia. Hosp Med Clin 4 (2015) 34–50 Schaefer T. Disorders of Potassium. Emerg Med Clin N Am 23 (2005) 723–747
 34–50. Schaefer T. Disorders of Potassium. Emerg Med Clin N Am 23 (2005) 723–747.")
30
Hipokalemia Concentración Sérica de Potasio menor a 3.5 mEq/L
Se encuentra en más del 20% de los pacientes hospitalizados Mayor riesgo de complicaciones cardiovasculares y reingresos hospitalarios La hipopotasemia (generalmente definida como el potasio sérico inferior a 3,6 mEq por litro) es una anomalía electrolítica excepcionalmente común en la práctica clínica. Más del 20% de los pacientes hospitalizados se han notificado a tener cierto grado de hipopotasemia. Los pacientes que toman diuréticos, especialmente tiazidas, corren especial riesgo de hipopotasemia. La hipopotasemia también se observa con frecuencia en pacientes de trauma, con algunos centros de reportar una incidencia de 45% a 68% en la entrada Medford-Davis L, Rafique Z. Derangements of Potasium. Emerg Med Clin N Am 32 (2014) 329–347 Theisen-Thoupal J. Hypokalemia and Hyperkalemia. Hosp Med Clin 4 (2015) 34–50
 es una anomalía electrolítica excepcionalmente común en la práctica clínica. Más del 20% de los pacientes hospitalizados se han notificado a tener cierto grado de hipopotasemia. Los pacientes que toman diuréticos, especialmente tiazidas, corren especial riesgo de hipopotasemia. La hipopotasemia también se observa con frecuencia en pacientes de trauma, con algunos centros de reportar una incidencia de 45% a 68% en la entrada. Medford-Davis L, Rafique Z. Derangements of Potasium. Emerg Med Clin N Am 32 (2014) 329–347. Theisen-Thoupal J. Hypokalemia and Hyperkalemia. Hosp Med Clin 4 (2015) 34–50.")
31
Manifestaciones Clínicas
Cardiaco Digestivo Renal Músculo Arritmias Defectos en la Conducción Mayor riesgo de Arritmias con Digitálicos Cambios EKGs Íleo Metabólico Diabetes Insípida Nefrogénica Nefropatía Hipokalémica Alcalosis Metabólica Amoniogénesis Skeletal muscle Weakness Paralysis Rhabdomyolysis Fasiculations and tetany Debilidad Muscular Parálisis Rabdomiólisis Fasciculaciones y Tetania Medford-Davis L, Rafique Z. Derangements of Potasium. Emerg Med Clin N Am 32 (2014) 329–347
 329–347.")
32
Manifestaciones Clínicas
Hipokalemia Leve Debilidad Muscular Mínima Asintomáticos Hipokalemia Moderada Constipación Debilidad Muscular Proximal Hipokalemia Severa Parálisis Simétrica Ascendente Mioglobinuria Rabdomiólisis reported. Severely hypokalemic patients (serum potassium levels below 2.5 mEq per liter) may develop rhabdomyolysis, myoglobinuria, an ascending symmetric paralysis with a clear sensorium, and even respiratory arrest [2]. Central nervous system symptoms, although reported, are more likely the result of acid-base changes or other coexisting abnormalities [22]. Symptoms are not only associated with the degree of hypokalemia found, but also the rapidity with which it developed Medford-Davis L, Rafique Z. Derangements of Potasium. Emerg Med Clin N Am 32 (2014) 329–347
 may develop rhabdomyolysis, myoglobinuria, an ascending symmetric paralysis with a clear sensorium, and even respiratory arrest [2]. Central nervous system symptoms, although reported, are more likely the result of acid-base changes or other coexisting abnormalities [22]. Symptoms are not only associated with the degree of hypokalemia found, but also the rapidity with which it developed. Medford-Davis L, Rafique Z. Derangements of Potasium. Emerg Med Clin N Am 32 (2014) 329–347.")
33
Electrocardiograma Aumento del potencial de reposo de membrana y el periodo refractario La presencia o ausencia de estos hallazgos no es predictivo de hipokalemia o su severidad Aumento en la amplitud de la onda P Reducción e Inversión de la onda T Depresión del Segmento ST y aparición de la onda U Aparente Prolongación del Intérvalo QT Prolonged PR interval Reduction in T-wave amplitude T-wave inversion Webster A, Brady W, Morris F. Recognising signs of danger: ECG changes resulting from an abnormal serum potassium concentration. Emerg Med J 2002;19:74–7.

34
Hipokalemia ¿Historia de Diuréticos? ¿Hipertensión?
Hipokalemia asociada a Diuréticos ¿Hipertensión? No Si Medición de Renina y Aldosterona No ¿Redistribución Celular? Si Alcalosis B2 Agonistas Insulina Vit B12 Drogas Parálisis Periódica Hipokalémica No Medición de la excreción urinaria de Potasio Unwin RJ, Luft FC, Shirley DG. Pathophysiology and management of hypokalemia: a clinical perspective. Nat Rev Nephrol. 2011;7(2):75-84
:")
35
Excreción Urinaria de Potasio
Disminuida K orina de 24 hrs <20 mEq/d Radio K-Cr urinario >15 mEq/g Aumentada K orina de 24 hrs >30 mEq/d Radio K-Cr urinario >20 mEq/g Pobre Ingesta Pérdidas Extrarenales Uso remoto de Diuréticos Estatus Ácido-Base Acidosis Metabólica Normal Alcalosis Metabólica ATR Tolueno Anfotericina Cetoacidosis Diabética Lysozymuria Polidipsia Primaria Sobredosis de Acetaminofén Diuréticos Sx. de Bartter Sx. de Gitelman Aminoglucósidos Hipomagenesemia Unwin RJ, Luft FC, Shirley DG. Pathophysiology and management of hypokalemia: a clinical perspective. Nat Rev Nephrol. 2011;7(2):75-84
:")
36
Medición de Renina y Aldosterona
Renina y Aldosterona Elevadas Aldosterona Elevada Renina Baja Renina y Aldosterona Disminuídas Hipertensión Renovascular Tumor Secretor de Renina Hipertensión Maligna Coartación Aórtica Hiperaldosteronismo Primario Exceso aparente de Mineralocorticoides Tumor productor de DOC Síndrome de Cushing Deficiencia de 11-B-HSD Sx. De Liddle Hiperplasia adrenal congénita Unwin RJ, Luft FC, Shirley DG. Pathophysiology and management of hypokalemia: a clinical perspective. Nat Rev Nephrol. 2011;7(2):75-84
:")
37
Diagnóstico Electrocardiograma Gasometría Medición sérica de Magnesio Cuantificación de Potasio en orina de 24 horas Kim GH, Han JS. Therapeutic Approach to Hypokalemia. Nephron 2002;92(Supp. 1):28–32.
:28–32.")
38
Tratamiento La decisión de corregir la hipokalemia debe estar centrada en el estado clínico del paciente Hipokalemia Leve Hipokalemia Moderada/Severa Situaciones Espaciales No requiere tratamiento urgente Dieta Rica en Potasio Reposición Urgente de Potasio Shift Intracelular SICA However, patients with acute myocardial infarction are an exception, due to the increased risk of ventricular dysrhythmias in the presence of even mild hypokalemia. It is recommended that the serum potassium be maintained above 4.5 mEq per liter in this population Patients with moderate to severe hypokalemia (!3.0 mEq/L) or those who are symptomatic with significant electrocardiogram changes, dysrhythmias, severe weakness, or paralysis require more urgent potassium replacement. The choice of route and formulation is dependent on the severity of the symptoms and underlying conditions Special care must be taken in the treatment of patients with low serum potassium due to transcellular potassium shifts. These patients may not have significant total body potassium deficits. Rebound hyperkalemia can occur as the cause of the transcellular shift is corrected and if aggressive potassium replacement has been given No requiere Tratamiento Urgente Dieta rica en Potasio Theisen-Thoupal J. Hypokalemia and Hyperkalemia. Hosp Med Clin 4 (2015) 34–50 Kim GH, Han JS. Therapeutic Approach to Hypokalemia. Nephron 2002;92(Supp. 1):28–32.
 or those. who are symptomatic with significant electrocardiogram changes, dysrhythmias, severe weakness, or paralysis require more urgent potassium. replacement. The choice of route and formulation is dependent on the. severity of the symptoms and underlying conditions. Special care must be taken in the treatment of patients with low serum. potassium due to transcellular potassium shifts. These patients may not. have significant total body potassium deficits. Rebound hyperkalemia can. occur as the cause of the transcellular shift is corrected and if aggressive. potassium replacement has been given. No requiere Tratamiento Urgente. Dieta rica en Potasio. Theisen-Thoupal J. Hypokalemia and Hyperkalemia. Hosp Med Clin 4 (2015) 34–50. Kim GH, Han JS. Therapeutic Approach to Hypokalemia. Nephron 2002;92(Supp. 1):28–32.")
39
Tratamiento Formulación Dosis Indicación KCL Oral 20-80 mEq/día
Corrección no urgente Potasio Oral Líquido 40-60 mEq/dosis Rápida elevación para pacientes que requieren correcciones urgentes KCL Intravenoso 20-40 mEq/h Pacientes con síntomas severos o incapaces de tolerar la vía oral Kim GH, Han JS. Therapeutic Approach to Hypokalemia. Nephron 2002;92(Supp. 1):28–32. Theisen-Thoupal J. Hypokalemia and Hyperkalemia. Hosp Med Clin 4 (2015) 34–50
:28–32. Theisen-Thoupal J. Hypokalemia and Hyperkalemia. Hosp Med Clin 4 (2015) 34–50.")
40
Hiperkalemia Trastorno electrolítico muy frecuente
Los trastornos renales representan la principal causa de hiperkalemia, seguidos de las patologías que se acompañan de lisis celular con liberación de gran cantidad de potasio intracelular Renal disorders are the most common cause of hyperkalemia, followed by cell lysis, which releases large intracellular K1 stores Medford-Davis L, Rafique Z. Derangements of Potasium. Emerg Med Clin N Am 32 (2014) 329–347
 329–347.")
41
Alteración en la Excreción Redistribución Celular
Etiología Pseudohiperkalemia Disminución en la filtración glomerular Insuficiencia Cardiaca Uropatía Obstructiva Hipoaldosteronismo Acidosis Tubular Renal tipo lV Alteración en la Excreción Transcellular shifts (Na-K ATPase pump) Hemolysis Rhabdomyolysis Tumor lysis syndrome Hematoma reabsorption Medications that inhibit Na-K ATPase pump (see Box 1) Insulin deficiency Diabetes mellitus Prolonged fasting Hypertonicity Hyperglycemia Hypernatremia Acidosis Hyperkalemic periodic paralysis (mutation of skeletal muscle Na-K pump) Fasting Intense exercise High-K1 meal Hemolisis Medicamentos Deficiencia de Insulina Hipertonicidad Acidosis Redistribución Celular Medford-Davis L, Rafique Z. Derangements of Potasium. Emerg Med Clin N Am 32 (2014) 329–347
 Hemolysis. Rhabdomyolysis. Tumor lysis syndrome. Hematoma reabsorption. Medications that inhibit Na-K ATPase pump (see Box 1) Insulin deficiency. Diabetes mellitus. Prolonged fasting. Hypertonicity. Hyperglycemia. Hypernatremia. Acidosis. Hyperkalemic periodic paralysis (mutation of skeletal muscle Na-K pump) Fasting. Intense exercise. High-K1 meal. Hemolisis. Medicamentos. Deficiencia de Insulina. Hipertonicidad. Acidosis. Redistribución Celular. Medford-Davis L, Rafique Z. Derangements of Potasium. Emerg Med Clin N Am 32 (2014) 329–347.")
42
Manifestaciones Clínicas
Palpitaciones, bradicardia, arritmias, contracciones ventriculares prematuras Calambres musculares, parestesias, debilidad, disminución en los reflejos tendinosos Náusea, vómito, diarrea Neurologic examination may reveal decreased deep tendon reflexes and decreased strength with intact sensation. Weisberg LS. Management of severe hyperkalemia. Crit Care Med 2008;36(12):3246–51 Medford-Davis L, Rafique Z. Derangements of Potasium. Emerg Med Clin N Am 32 (2014) 329–347
:3246–51. Medford-Davis L, Rafique Z. Derangements of Potasium. Emerg Med Clin N Am 32 (2014) 329–347.")
43
Electrocardiograma El EKG representa el estudio inicial de elección
1.- Ondas T picudas de base ancha 2.- Alargamiento del PR 3.- QRS ensanchado 4.- Disminución en la amplitud de ondas P. “Ritmo Nodal” 5.- Onda Sinusoidal 6.- Fibrilación Ventricular 1.- Aurículas 2.- Ventrículos 3.- Ramas de His 4.- Nodo Sinoauricular 5.- Tractos Interauriculares Therefore, the ECG progresses through several phases that are loosely correlated with absolute serum K1 levels and with the rate of increase in serum K1 levels. The first and most common sign is tall, “peaked” T waves with a narrow base (Fig. 1). These occur most frequently in the precordial leads V2-V4. A sensitive sign is if the amplitude of the T exceeds the amplitude of the R.7 As the atria are affected the PR interval lengthens, and as the ventricles are affected the QRS widens. When hyperkalemia affects the conduction system, the P waves decrease in amplitude until the ECG develops a “nodal” rhythm with absent P waves (Fig. 2). The QRS continues to widen until the S and T waves merge into a “sine wave” pattern (Fig. 3). The sine wave pattern usually shortly precedes ventricular fibrillation (VFib) and cardiac arrest. Montague B, Ouellette JR, Buller GK. Retrospective review of the frequency of ECG changes in hyperkalemia. Clin J Am Soc Nephrol 2008;3:324–30. Slovis C, Jenkns R. ABC of clinical electrocardiography: conditions not primarily affecting the heart. BMJ 2002;324:1320–3.
. These occur most frequently in the precordial leads V2-V4. A sensitive sign is if the amplitude of the T exceeds the amplitude of the R.7 As the atria are affected the PR interval lengthens, and as the ventricles are affected the QRS widens. When hyperkalemia affects the conduction system, the P waves decrease in amplitude until the ECG develops a nodal rhythm with absent P waves (Fig. 2). The QRS continues to widen until the S and T waves merge into a sine wave pattern (Fig. 3). The sine wave pattern usually shortly precedes ventricular fibrillation (VFib) and cardiac arrest. Montague B, Ouellette JR, Buller GK. Retrospective review of the frequency of ECG changes in hyperkalemia. Clin J Am Soc Nephrol 2008;3:324–30. Slovis C, Jenkns R. ABC of clinical electrocardiography: conditions not primarily affecting the heart. BMJ 2002;324:1320–3.")
44
52% exhibía algún cambio electrocardiográfico
Estudio retrospectivo que valoró la frecuencia de cambios electrocardiográficos en 90 pacientes con niveles de potasio sérico superiores a 6 mEq/L Sólo 18% de los participantes cumplía criterios estrictos de Hiperkalemia en el electrocardiograma 52% exhibía algún cambio electrocardiográfico Herramienta poco sensible para el diagnóstico de Hiperkalemia Of the 90 cases reviewed, 16 patients met strict criteria for ECG changes and 47 showed some ECG change. Twenty-nine patients had peaked T waves, and 28 patients were noted to have symmetric T waves. Sensitivities for all criteria were low ranging from 0.18 for strict criteria to 0.52 for the presence of any ECG change. The likelihood of meeting strict criteria for ECG changes increased with increasing concentrations of serum potassium (P = ), and there was a trend toward increased likelihood of new or resolving symmetric T waves (P = 0.052). The presence of new or resolving peaking of T waves was not significantly associated with serum potassium concentration (P = 0.095); neither was the presence of any T-wave change (P = 0.18). Montague B, Ouellette JR, Buller GK. Retrospective review of the frequency of ECG changes in hyperkalemia. Clin J Am Soc Nephrol 2008;3:324–30.
, and there was a trend toward increased likelihood of new or resolving symmetric T waves (P = 0.052). The presence of new or resolving peaking of T waves was not significantly associated with serum potassium concentration (P = 0.095); neither was the presence of any T-wave change (P = 0.18). Montague B, Ouellette JR, Buller GK. Retrospective review of the frequency of ECG changes in hyperkalemia. Clin J Am Soc Nephrol 2008;3:324–30.")
45
Tratamiento Estabilización de la Membrana Cardíaca
Gluconato de Calcio Cloruro de Calcio Disminución de los niveles de potasio Aumento del Shift Intracelular: Insulina, Beta Agonistas, Bicarbonato Disminución neta de potasio: Diuréticos de Asa, Kayexalate, Diálisis

46
Kayexalate Resina de Intercambio Iónico Inicio de acción en 2-6 horas
Asociada a Constipación por lo que se administra generalmente con ablandadores de heces Asociado a Necrosis Colónica However, subsequent research has not replicated the 1961 results, instead showing .5 A dangerous side effect of Kayexalate is intestinal necrosis, and the US Food and Drug Administration has issued a warning against administering it in combination with the stool softener sorbitol, which is thought to increase the incidence of intestinal necrosis.4,5 In light of its delayed onset of action, uncertain efficacy, and high-risk side-effect profile, Kayexalate is not recommended in the treatment of hyperkalemia Resin potassium binders One study (Gruy-Kapral 1998) addressed the effects of sodium polystyrene sulfonate on serum potassium in chronic renal failure patients. No differences in serum potassium were observed at four hours when resin was compared with placebo. No useful information on later time points could be extracted from this study, because oral potassium was administered at four hours Thirty reports describing 58 cases (41 preparations containing sorbitol and 17 preparations without sorbitol) of adverse events were identified. The colon was the most common site of injury (n44;76%), and transmural necrosis (n36; 62%) was the most common histopathologic lesion reported. Mortality was reported in 33% of these cases due to gastrointestinal injury. CONCLUSIONS: Sodium polystyrene sulfonate use, both with and without sorbitol, may be associated with fatal gastrointestinal injury. Physicians must be cognizant of the risk of these adverse events when prescribing this therapy for the management of hyperkalemia. Harel Z et al. Gastrointestinal Adverse Events With Sodium Polystyrene Sulfonate (Kayexalate) Use: A Sistematic Review. The American Journal of Medicine (2013) 126, 9-24
 addressed the effects of sodium polystyrene sulfonate on serum potassium in chronic renal failure patients. No differences in serum potassium were observed at four hours when resin was compared with placebo. No useful information on later time points could be extracted from this study, because oral potassium was administered at four hours. Thirty reports describing 58 cases (41 preparations containing sorbitol and 17 preparations without sorbitol) of adverse events were identified. The colon was the most common site of injury (n44;76%), and transmural necrosis (n36; 62%) was the most common histopathologic lesion reported. Mortality was reported in 33% of these cases due to gastrointestinal injury. CONCLUSIONS: Sodium polystyrene sulfonate use, both with and without sorbitol, may be associated with fatal gastrointestinal injury. Physicians must be cognizant of the risk of these adverse events when prescribing this therapy for the management of hyperkalemia. Harel Z et al. Gastrointestinal Adverse Events With Sodium Polystyrene Sulfonate (Kayexalate) Use: A Sistematic Review. The American Journal of Medicine (2013) 126,")
47
Punto Final Primario Tasa de Cambio en el Potasio Sérico a las 48 horas Punto Final Secundario Tasa de Cambio en el Potasio Sérico a los 12 días Pacientes con Normocalemia en el día 3 pasan a la 2 fase Fase Inicial Fase de Mantenimiento Seguimiento 2 Días 12 Días 7 Días Día del Estudio ZS9 Medición de Potasio 3 Dosis Diarias 1 Dosis Diaria Ensayo Clínico de fase 3. 753 pacientes asignados al azar a recibir ZS-9 tres veces al día durante 48 horas Punto Final Primario: Tasa Exponencial de cambio en el potasio sérico a las 48 horas Packham D. Sodium Zirconium Cyclosilicate in Hyperkalemia. N Engl J Med 2015; 372:

48
Reducciones de los niveles de potasio sérico en todos los grupos que recibieron ZS-9 (p<0.001)
Reducción significativa en los niveles de potasio en 48 horas, con niveles de potasio normales durante los 12 días de terapia de mantenimiento Packham D. Sodium Zirconium Cyclosilicate in Hyperkalemia. N Engl J Med 2015; 372:

49
Calcio

50
Receptor Sensor de calcio
Calcio Ionizado Túbulo Renal Receptor Sensor de calcio Célula Paratiroidea Receptor de PTH Hueso PTHrP Duodeno 1,25(OH)2D Mecanismo Parácrino-Autócrino Cartílago y Células Blanco Endocrine and metabolic emergencies: Hypocalcaemia. Ther Adv Endocrinol Metab (2010) 1(1) 29-33
2D. Mecanismo Parácrino-Autócrino. Cartílago y Células Blanco. Endocrine and metabolic emergencies: Hypocalcaemia. Ther Adv Endocrinol Metab (2010) 1(1)")
51
Hipocalcemia 26% de los pacientes admitidos a un hospital
88% de los pacientes en UCI 50% de lo casos secundaria a deficiencia de Vitamina D Endocrine and metabolic emergencies: Hypocalcaemia. Ther Adv Endocrinol Metab (2010) 1(1) 29-33
 1(1)")
52
Concentraciones bajas de Vitamina D
Causa principal de Hipocalcemia a nivel mundial Algunas poblaciones con riesgo aumentado Baja exposición al Sol Dietas mal balanceadas Ingesta de Medicamentos Embarazo Enfermedades del Intestino Delgado Enfermedades Renales o Hepáticas Cooper, M.S. and Gittoes, N.J.L. (2008) Diagnosis and management of hypocalcaemia. BMJ 336:
 Diagnosis and management of hypocalcaemia. BMJ 336:")
53
Pseudohipoparatiroidismo Deficiencia Vitamina D
Hipocalcemia Hormona Paratiroidea Baja Alta Magnesio Función Renal Deficiencia Mg Hipopituitarismo Baja Enf. Renal 25 OH Vitamina D Alta Pseudohipoparatiroidismo Deficiencia de Calcio Deficiencia Vitamina D Baja Normal Adaptado de: Cooper, M.S. and Gittoes, N.J.L. (2008) Diagnosis and management of hypocalcaemia. BMJ 336:
 Diagnosis and management of hypocalcaemia. BMJ 336:")
54
Deficiencia de Vitamina D
Hipocalcemia Causa PTH FA Fosfato 25(OH) Vit D3 Deficiencia de Vitamina D Elevada Normal Bajo Hipoparatiroidismo Alto ERC Normal o Alta Normal o Bajo Hipomagenesemia Normal o Baja Tohme JF, Bilezekian JP. Hypocalcemic emergencies. Endocrinol Metab Clin North Am. 22: 1993; Endocrine and metabolic emergencies: Hypocalcaemia. Ther Adv Endocrinol Metab (2010) 1(1) 29-33 Hall, L. and Gallacher, S.J. (2006) Primary Hypoparathyroidism Resistant to Conventional Therapy. Scott Med J 51: 54.
 Vit D3. Deficiencia de Vitamina D. Elevada. Normal. Bajo. Hipoparatiroidismo. Alto. ERC. Normal o Alta. Normal o Bajo. Hipomagenesemia. Normal o Baja. Tohme JF, Bilezekian JP. Hypocalcemic emergencies. Endocrinol Metab Clin North Am. 22: 1993; Endocrine and metabolic emergencies: Hypocalcaemia. Ther Adv Endocrinol Metab (2010) 1(1) Hall, L. and Gallacher, S.J. (2006) Primary Hypoparathyroidism Resistant to Conventional Therapy. Scott Med J 51: 54.")
55
Manifestaciones Clínicas
Excitabilidad Neuromuscular Presentación en relación a concentración absoluta y velocidad de disminución Signos de Chvostek y Trousseau espasmo carpopedal, espasmos musculares, espasmos, hormigueo y entumecimiento Tohme JF, Bilezekian JP. Hypocalcemic emergencies. Endocrinol Metab Clin North Am. 22: 1993; Endocrine and metabolic emergencies: Hypocalcaemia. Ther Adv Endocrinol Metab (2010) 1(1) 29-33
 1(1)")
56
Manifestaciones Clínicas
Asociada a Trastornos Psiquiátricos La Hipocalcemia crónica incluso sin síntomas neuromusculares está asociada al desarrollo de síntomas neuropsiquiátricos The most common picture is one of delirium. Cognitive impairment, psychosis, depression, or anxiety is also frequently observed Denko JD, Kaelbling R. The Psychiatric Aspects of Hypoparathyroidism. Acta Psychiatr Scand Suppl. 2962; 38(164):1-70
:1-70.")
57
Intervención Aguda Pacientes Sintomáticos
Asintomáticos con hipocalcemias severas (<8 mg/dl) Gluconato de Calcio al 10% Inicio concomitante de suplementación oral con Calcio y Vitamina D Endocrine and metabolic emergencies: Hypocalcaemia. Ther Adv Endocrinol Metab (2010) 1(1) 29-33
 Gluconato de Calcio al 10% Inicio concomitante de suplementación oral con Calcio y Vitamina D. Endocrine and metabolic emergencies: Hypocalcaemia. Ther Adv Endocrinol Metab (2010) 1(1)")
58
Tetania, Convulsiones, Laringoespasmo, Disfunción Cardíaca
Tratamiento Inmediato con Alta Sospecha, de los contrario, Medición de Calcio Sérico 10-20 ml Gluconato de Calcio en ml SF0.9% o SG5% para min Repetir hasta la desaparición de los síntomas Iniciar Carbonato de Calcio + Vitamina D Oral 100 ml Gluconato de Calcio en 1000 ml SF0.9% o SG5% a ml/hr Adaptado de: Cooper, M.S. and Gittoes, N.J.L. (2008) Diagnosis and management of hypocalcaemia. BMJ 336:
 Diagnosis and management of hypocalcaemia. BMJ 336:")
59
Teriparatide Análogo de PTH Incrementa la densidad y arquitectura ósea
Actualmente sólo aprobado su uso para Osteoporosis Estudios demuestran beneficio en Hipoparatiroidismo 2 ug/kg/día Análogo de PTH. Incrementa la densidad y arquitectura ósea. Actualmente sólo aprobado su uso para Osteoporosis. Estudios demuestran beneficio en Hipoparatiroidismo. 2 ug/kg/día Winer, K.K., Ko, C.W., Reynolds, J.C., Dowdy, K., Keil, M., Peterson, D. et al. (2003) Long-term treatment of hypoparathyroidism: a randomized controlled study comparing parathyroid hormone versus calcitriol and calcium. J Clin Endocrinol Metab 88:
 Long-term treatment of hypoparathyroidism: a randomized controlled study comparing parathyroid hormone versus calcitriol and calcium. J Clin Endocrinol Metab 88:")
60
Estudio Aleatorio Controlado Doble Ciego
428 participantes recibiendo glucocorticoides 214 recibieron 20ug de Teriparatide y 210 recibieron 10 mg de Alendronato End Points: Cambio en la densidad ósea a nivel lumbar, cambios en la densidad mineral ósea de la cadera y cambios en los marcadores óseos In an 18-month randomized, double-blind, controlled trial, we compared teriparatide with alendronate in 428 women and men with osteoporosis (ages, 22 to 89 years) who had received glucocorticoids for at least 3 months (prednisone equivalent, 5 mg daily or more). A total of 214 patients received 20 μg of teriparatide once daily, and 214 received 10 mg of alendronate once daily. The primary outcome was the change in bone mineral density at the lumbar spine. Secondary outcomes included changes in bone mineral density at the total hip and in markers of bone turnover, the time to changes in bone mineral density, the incidence of fractures, and safety. Saag K et al. Teriparatide or Alendronate in Glucocorticoid-Induced Osteoporosis. N Engl J Med 2007; 357:
 who had received glucocorticoids for at least 3 months (prednisone equivalent, 5 mg daily or more). A total of 214 patients received 20 μg of teriparatide once daily, and 214 received 10 mg of alendronate once daily. The primary outcome was the change in bone mineral density at the lumbar spine. Secondary outcomes included changes in bone mineral density at the total hip and in markers of bone turnover, the time to changes in bone mineral density, the incidence of fractures, and safety. Saag K et al. Teriparatide or Alendronate in Glucocorticoid-Induced Osteoporosis. N Engl J Med 2007; 357:")
61
Riesgo de fracturas similar en los dos grupos
Incremento en la Densidad Mineral Ósea a nivel lumbar mayor en el grupo de Teriparátide (p<0.001) Incremento en la Densidad Mineral Ósea de la cadera en el grupo de Teriparátide (p=0.004) Riesgo de fracturas similar en los dos grupos Elevación de Calcio sérico en grupo de Teriparátide (p<0.001) Saag K et al. Teriparatide or Alendronate in Glucocorticoid-Induced Osteoporosis. N Engl J Med 2007; 357:
 Incremento en la Densidad Mineral Ósea de la cadera en el grupo de Teriparátide (p=0.004) Riesgo de fracturas similar en los dos grupos. Elevación de Calcio sérico en grupo de Teriparátide (p<0.001) Saag K et al. Teriparatide or Alendronate in Glucocorticoid-Induced Osteoporosis. N Engl J Med 2007; 357:")
62
Terapias Emergentes Calcilíticos NPSP558
Antagonistas del Receptor Sensor de Calcio en las Paratiroides Actualmente en estudio para su uso en Osteoporosis e Hipoparatirodismo NPSP558 Análogo de PTH Fase 3 de Ensayo Clínico para su uso en Hipoparatiroidismo The only bone anabolic agents currently available on the market are based on the parathyroid hormone (PTH). Secretion of endogenous PTH is controlled by a calcium-sensing receptor at the surface of the parathyroid glands. Antagonists of this receptor (calcilytics) induce the release of the hormone. Provided the effect of the calcilytic is of short duration, a bone anabolic effect should also result. Although the first calcilytic series became known approximately 10 years ago, the number of different structural types is still small today. This article outlines the quest from hits to potent development candidates of all relevant calcilytic series currently known. Even after the front-runners unexpectedly failed in the clinic, the approach for an oral alternative to parenteral PTH remains highly attractive.
. Secretion of endogenous PTH is controlled by a calcium-sensing receptor at the surface of the parathyroid glands. Antagonists of this receptor (calcilytics) induce the release of the hormone. Provided the effect of the calcilytic is of short duration, a bone anabolic effect should also result. Although the first calcilytic series became known approximately 10 years ago, the number of different structural types is still small today. This article outlines the quest from hits to potent development candidates of all relevant calcilytic series currently known. Even after the front-runners unexpectedly failed in the clinic, the approach for an oral alternative to parenteral PTH remains highly attractive.")
63
¿Suplementos de Calcio para Todos?

64
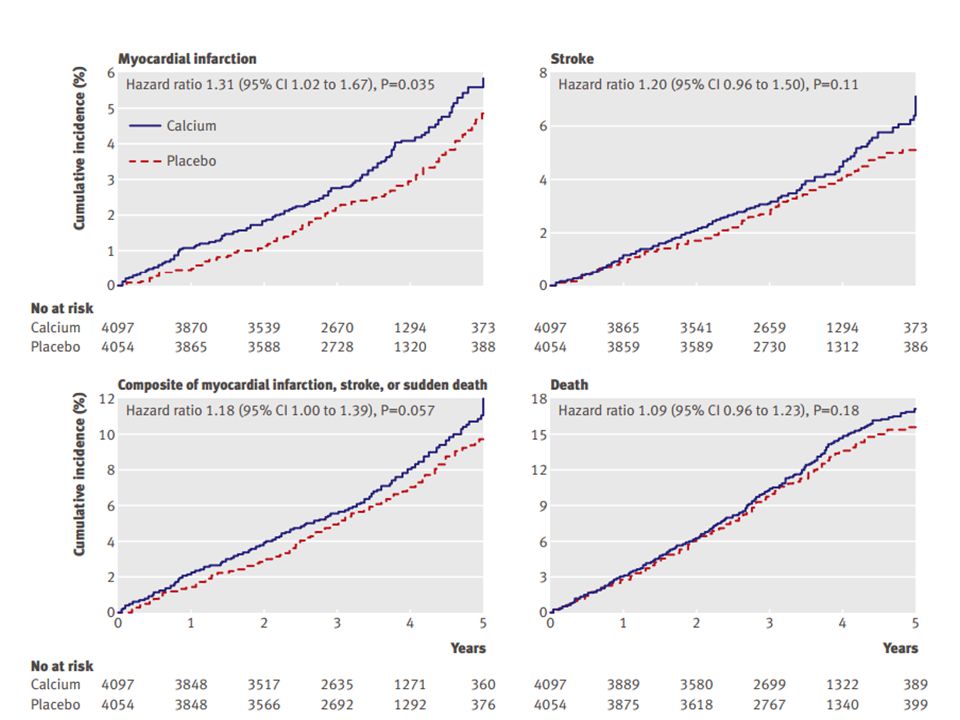
Vascular Events in Healthy Older Women Receiving Calcium Supplementation: Randomised Controlled Trial

65
Ataque Isquémico Transitorio
Eventos Vasculares Calcio N=732 Placebo N=739 Valor de P RR (95%CI) Angina 50 (88) 71 (99) 0.058 ) IAM 31 (45) 14 (19) 0.0099 2.24 ( ) Ataque Isquémico Transitorio 33 (42) 21 (27) 0.10 1.59 ( ) EVC 40 (52) 0.14 1.44 ( ) Muerte Súbita 4 1 0.22 4.04 ( ) AIM, EVC o Muerte Súbita 69 (101) 42 (54) 0.0075 1.66 ( )
 Angina. 50 (88) 71 (99) ) IAM. 31 (45) 14 (19) ( ) Ataque Isquémico Transitorio. 33 (42) 21 (27) ( ) EVC. 40 (52) ( ) Muerte Súbita ( ) AIM, EVC o Muerte Súbita. 69 (101) 42 (54) ( )")
66
Effect of Calcium Supplements on Risk Of Myocardial Infarction and Cardiovascular Events: Meta-analysis

68
Hipercalcemia Incremento en la Absorción Intestinal Incremento en la resorción osea Alteraciones a nivel Renal Carroll R, Matfin G. Endocrine and metabolic emergencies: hypercalcaemia. Ther Adv Endocrinol Metab (2010) 1 (5)
 1 (5)")
69
Consideraciones Diagnósticas
En estados con fluctuaciones en la concentración de albúmina sérica medir el calcio ionizado La medición de PTH se considera el primer paso Azoados, Vitamina D3, Función tiroidea, proteínas de Bence-Jones, Marcadores oseos Carroll R, Matfin G. Endocrine and metabolic emergencies: hypercalcaemia. Ther Adv Endocrinol Metab (2010) 1 (5)
 1 (5)")
70
Hipercalcemia PTH Elevada PTH Suprimida
1.- Hiperparatiroidismo Primario 2.- Hiperparatiroidismo Terciario ERC Avanzada Deficiencia de Vit D Malabsorción de Calcio 1.- Malignidad 2.- Inducida por Fármacos 3.- Endocrinopatías 4.- Inmovilización 5.- Enfermedades Granulomatosas Adaptado de: Carroll R, Matfin G. Endocrine and metabolic emergencies: hypercalcaemia. Ther Adv Endocrinol Metab (2010) 1 (5)
 1 (5)")
71
Manejo El manejo agudo de la Hipercalcemia dependerá de una gran variedad de factores Resucitación Hídrica se considera la piedra angular Diuréticos de ASA Movilización Precoz Bifosfonatos Calcitonina Carroll R, Matfin G. Endocrine and metabolic emergencies: hypercalcaemia. Ther Adv Endocrinol Metab (2010) 1 (5)
 1 (5)")
72
Fosforo

73
Introducción Componente vital del ser humano
Anión Intracelular principal Concentración normal: mg/dl Hipofosfatemia Alcalosis Respiratoria Hiperfosfatemia Enfermedad Renal Crónica IMAGEN SOBRE FISIOLOGÍA DEL FOSFATO PARA EXPLICAR

74
Población en Riesgo Hiperfosfatemia Hipofosfatemia
Lesión Renal Aguda o Crónica, Hipoparatiroidismo, Hemolisis, Síndrome de Lisis Tumoral, Uso crónico de Antiácidos EPOC, Neoplasias, Nutrición Parenteral, Alcoholismo, Enfermedad Inflamatoria Intestinal 30% mayor mortalidad en Hipofosfatemia Severa Hipofosfatemia Adaptado de: Cooper, M.S. and Gittoes, N.J.L. (2008) Diagnosis and management of hypocalcaemia. BMJ 336:
 Diagnosis and management of hypocalcaemia. BMJ 336:")
75
Manifestaciones Clínicas
Hipofosfatemia Convulsiones Arritmias Prolongación del QT Debilidad Tetania Depósitos subdérmicos Parestesias Convulsiones Insuficiencia Cardíaca Arritmias Falla Respiratoria Rabdomiólisis Hemólisis Hiperfosfatemia Adaptado de: Cooper, M.S. and Gittoes, N.J.L. (2008) Diagnosis and management of hypocalcaemia. BMJ 336:
 Diagnosis and management of hypocalcaemia. BMJ 336:")
76
Tratamiento Hipofosfatemia
Se prefiere la vía oral sobre la intravenosa Por cada 1 mg de fosforo que administremos el fosfato sérico incrementará aproximadamente 1 mg/dl Administrar al menos 1 mg de Fósforo al día Controles seriados de Fosfato, Calcio y Magnesio si utilizamos la vía Intravenosa Adaptado de: Cooper, M.S. and Gittoes, N.J.L. (2008) Diagnosis and management of hypocalcaemia. BMJ 336:
 Diagnosis and management of hypocalcaemia. BMJ 336:")
77
Tratamiento Hiperfosfatemia
Tratamiento etiológico de la Hiperfosfatemia Enfermedad Renal Crónica: Restricción en la Ingesta de Fosfatos Quelantes del Fósforo Diálisis Adaptado de: Cooper, M.S. and Gittoes, N.J.L. (2008) Diagnosis and management of hypocalcaemia. BMJ 336:
 Diagnosis and management of hypocalcaemia. BMJ 336:")
78
Hiperfosfatemia en ERC
Asociada a progresión de la enfermedad renal, enfermedad cardiovascular y mortalidad Desarrollo de Hiperparatiroidismo Secundario, Anormalidades óseas y calcificaciones No existe evidencia directa que demuestre que el control del fósforo mejora la morbimortalidad Adaptado de: Cooper, M.S. and Gittoes, N.J.L. (2008) Diagnosis and management of hypocalcaemia. BMJ 336:
 Diagnosis and management of hypocalcaemia. BMJ 336:")
79
Clorhidrato de Sevelamer Carbonato de Sevelamer
Quelante Contenido Mineral Ventajas Desventajas Hidróxido de Aluminio mg por tableta Económicos Toxicidad por Aluminio Acetato de Calcio 250 mg de Calcio por gramo Hipercalcemia Supresión de PTH Carbonato de Calcio 400 mg de Calcio por gramo Carbonato de Magnesio 250 mg de Magnesio por gramo Hipermagnesemia e Hiperkalemia Clorhidrato de Sevelamer Ninguno Menos riesgo de Hipercalcemia No Absorbibles Disminución de LDL Precio Elevado Carbonato de Sevelamer Carbonato de Lantano mg de Lantano por tableta Efectivo Adaptado de: Cooper, M.S. and Gittoes, N.J.L. (2008) Diagnosis and management of hypocalcaemia. BMJ 336:
 Diagnosis and management of hypocalcaemia. BMJ 336:")
Presentaciones similares