Descargar la presentación
La descarga está en progreso. Por favor, espere

1
ANESTESIA Y PERIOPERATORIO DEL GRAN OBESO
Leer el de paola y clincis 2006 morbida español y listo Ir viendo ppt 2005 españa.pdf (voy en premedicacion: slide 7/29)y barash manual pa Bajar todo este de best practice: Best Practice & Research Clinical Anaesthesiology, Volume 25, Issue 1, March 2011, Pages 11-25 Leer resume 2000: JORGE MÁRQUEZ UDEA
y barash manual pa. Bajar todo este de best practice: Best Practice & Research Clinical Anaesthesiology, Volume 25, Issue 1, March 2011, Pages Leer resume 2000: JORGE MÁRQUEZ. UDEA.")
2
Enfoque Introducción Preoperatorio Intraoperatorio Posoperatorio
Conclusión Introducción: Epidemiología, Comorbilidades leer mañana

3
DEFINICIÓN ≥ 70Kg/m2 : Ultraobeso Obes Rev 2007; 8(Suppl 1):13-17 .
Morbid obesity refers to those with a BMI >40, or >35 kg.m-2 in the presence of obesity-related comorbidity BMI 25–29.9 kg m2, overweight; BMI 30–39.9 kg m2, obese; BMI 40 kg m2, morbid obese; BMI > 50 kg m2, super-obese; and BMI > 60 kg m2, super-super-obese; BMI + 70 Ultra Obesoi ≥ 70Kg/m2 : Ultraobeso Obes Rev 2007; 8(Suppl 1):13-17 .
:")
4
Misma ref anterior Decir que es un problema Ompor: 7% + jovenes

5
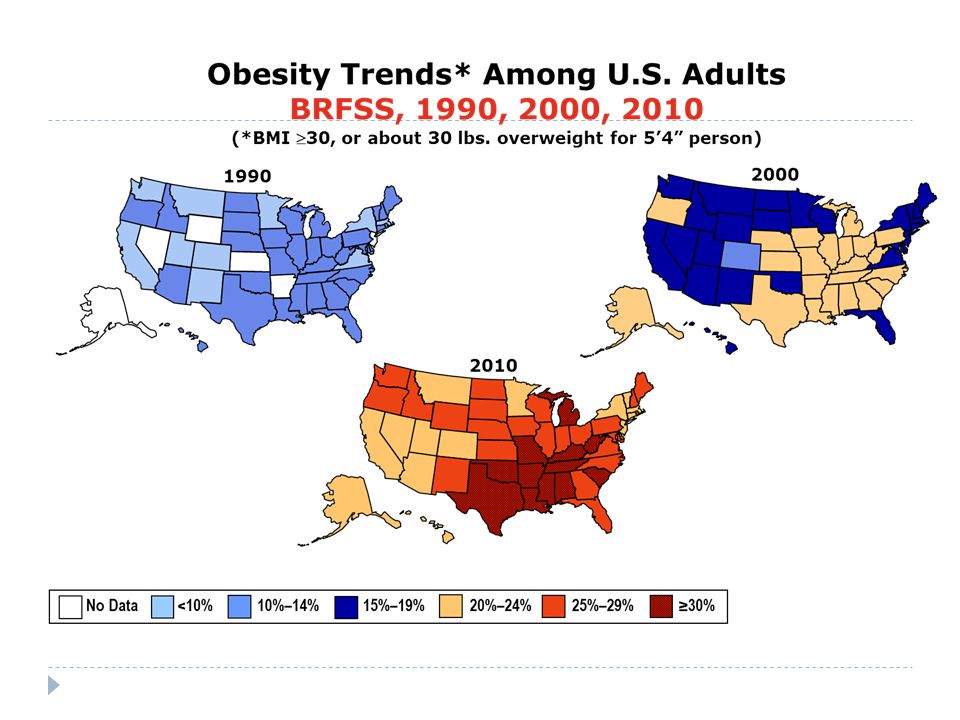
GLOBESIDAD Fig. 1. Past and projected overweight rates in selected countries. adapted from OECD website accessed 1/6/2011. Puntos praticos para intro chalao abrirla. Obesity is a problem faced by most medical providers in almost all medical specialities. The problem continues to worsen, and medical specialities have adapted and continue to adapt to this burden. Associated diseases, especially diabetes, osteoarthritis, hypertension, sleep apnoea and their sequelae are a significant financial burden to society. Obesity-related deaths are second only to smoking-related deaths, at least in the developed countries.

7
INTRODUCCIÓN 8% had a BMI over 40 kg/m2. The distribution indicated that 1.8% (349 patients) had a BMI over 50 kg/m2, and 50 patients were ultra-obese [BMI >70 kg/m2 or weight >200 kg (or >440 pounds)] (see Fig. 1). In other words, almost every day we have somebody in the operating room with a BMI of more than 50 kg/m2, and almost every week we anesthetize somebody who is ultra-obese, with a BMI of more than 70 kg/m2. We recently anesthetized a man with a BMI of 112 kg/m2 for an incision and drainage of the lower extremity for fasciitis, and a colleague recently intubated a 500-pound gravid woman for Cesarean section for twins due to failure of placement of an epidural. Some anesthetic aspects of morbid obesity Current Opinion in Anaesthesiology 2009, 22:442–446
 had a BMI over 50 kg/m2, and 50 patients were ultra-obese [BMI >70 kg/m2 or weight >200 kg (or >440 pounds)] (see Fig. 1). In other words, almost every day we have somebody in the operating room with a BMI of more than 50 kg/m2, and almost every week we anesthetize somebody who is ultra-obese, with a BMI of more than 70 kg/m2. We recently anesthetized a man. with a BMI of 112 kg/m2 for an incision and drainage of the lower extremity for fasciitis, and a colleague recently intubated a 500-pound gravid woman for Cesarean section for twins due to failure of placement of an epidural. Some anesthetic aspects of morbid obesity Current Opinion in Anaesthesiology 2009, 22:442–446.")
8
INTRODUCCIÓN Problemática en Colombia ENSIN 2005
Ver so hay datos mas recientes colombia ENSIN 2005

9
INTRODUCCIÓN Problemática en Colombia

10
INTRODUCCIÓN CC: suramerica +80 muj y 90 hombres El IMC es la herramienta mas usada para evaluar la severidad de la obesidad, pero no es el mejor predictor clínico de enfermedad. IMC falla en reconocer diferencias entre géneros, composición corporal, raza. La distribución del tejido adiposo más que el peso absoluto o IMC per se, tiene una mayor relevancia clínica. Obesidad androide o visceral. Relación cadera – cintura. Circunferencia Abdominal. Some anesthetic aspects of morbid obesity Current Opinion in Anaesthesiology 2009, 22:442–446

11
Síndrome Metabólico Obesidad central: ♂>102cm; ♀>88cm
↓HDL: ≤40 ♂; ≤50 ♀ ↑TG: ≥ 150 HTA: ≥130/85 Glucemia: ≥100 Estado proinflamatorio y protrombótico Riesgo cardiovascular: ↑ 50 – 60% Decir casitodos los morbido tienen SM Med Clin North Am Sep;95(5):855-73
:")
12
CIRUGÍA BARIÁTRICA Cardiovascular Evaluation and Management of Severely Obese Patients Undergoing Surgery Circulation. 2009;120:86-95.)
 .")
13
CIRUGÍA BARIÁTRICA Disminución del 80% en la tasa de mortalidad anual.
Resultados 6 – 12 meses perdida de peso mayor velocidad. 24 meses perdida de peso máxima. Falla de tratamiento Reducción del IMC < 35 kg/m². Perdida del exceso de peso < 40% Co-morbilidades DM 75% - 85% Dislipidemia 80% - 100% HTA 70% Cancer 80% OSA 80% Peso actual – peso ideal = exeso de peso Disminución del 80% en la tasa de mortalidad anual. Obesity and Bariatric Surgery Clin Chest Med 30 (2009)
")
14
An increase in BMI of 1 kg m2 is associated with an increased CO of 80 ml min1.11 Heart failure occurs most commonly in patients with a body weight 75% of ideal body weight (IBW) or with a BMI 40 kg m2. Most patients present with diastolic heart failure
 or with a BMI. 40 kg m2. Most patients present with diastolic heart failure.")
15
EVALUACIÓN PREOPERATORIA

16
EFECTOS FISIOPATOLÓGICOS
Pegar best practice 2011 Anaesthetic considerations and management of the obese patient. Current Anaesthesia & Critical Care 21 (2010) 16–23
 16–23.")
17
SISTEMA RESPIRATORIO ↑ VO2 y VCO2.
↑ del trabajo respiratorio, miopatía ↓ Distensibilidad torácica y pulmonar ↓ CRF, VRE, CPT, CVF. OM: patrón restrictivo Eucápnicos ↑ en la resistencia de la VA: PEEPi y ↓ Vol. pulmonar Hiperreactividad VA OHS / OSA La CRF puede disminuir al 50% en obesos comparada con 20% en no obesos, ocurre shunt intrapulmonar del 10-25% en obesos contra 2-5% en no obesos. La reducción de la CRF disminuye la capacidad del paciente obeso para tolerar la apnea, se desaturan rápidamente a pesar de la preoxigenación Diste pulmonar: volumen sanguíneo pulmonar aumentado. Estos cambios son más marcados en supino El incremento de la presión mecánica del abdomen, la disminución de la distensibilidad pulmonar y el incremento de las demandas metabólicas provocan ineficiencia de los músculos respiratorios y un incremento en el trabajo respiratorio. Ventilation and perfusion are also mismatched. The lung bases are well perfused, but they are hypoventilated up to 5% during spontaneous breathing due to airway closure and even alveolar collapse. Anesthesia for bariatric surgery. ASA refresher Vol 33 Chapter 5, 2005

18
SÍNDROME OBESIDAD-HIPOVENTILACIÓN
Desensibilización del centro respiratorio debido a la hipercapnia derivada de trastornos del sueño. Hipercapnicos, ↓ PaO2 Obesidad principal factor de riesgo. Somnolencia. Cardiomegalia. Policitemia. Hipoxemia e hipercapnia. Síndrome de Pickwick. Hipertensión pulmonar. Cor pulmonar. Patron ventilatorio de obeso + avanzaodo y agravado: fn resp peor Anesthesia for bariatric surgery. ASA refresher, 2008

19
APNEA OBSTRUCTIVA DEL SUEÑO
Episodios de apnea e hipopnea durante el sueño. Prevalencia del 70% en la población obesa (50% OM). Aumento de la morbi – mortalidad peri operatoria Aumento del riesgo de no ventilación/no intubación? Periodos de apnea Somnolencia diurna Ronquidos fuertes Cefalea matutina Despertar nocturnos frecuentes. el 50% de los pacientes morbidamente obesos tienen SAOS SAOS: FR indep pa HTA, morbimort CV y muerte subita Anesthetic Management of Patients with Obesity with and Without Sleep Apnea Clin Chest Med 30 (2009) 569–579
. Aumento de la morbi – mortalidad peri operatoria. Aumento del riesgo de no ventilación/no intubación Periodos de apnea. Somnolencia diurna. Ronquidos fuertes. Cefalea matutina. Despertar nocturnos frecuentes. el 50% de los pacientes morbidamente obesos tienen SAOS. SAOS: FR indep pa HTA, morbimort CV y muerte subita. Anesthetic Management of Patients with Obesity with and Without Sleep Apnea Clin Chest Med 30 (2009) 569–579.")
20
“STOP – BANG” Tamizaje para AOS. Snoring Ronquidos
Tiredness Cansancio durante el día Observed apnea Episodios presenciados de apnea Pressure Hipertensión BMI > 35 kg/m² Age Edad > 50 años Neck Circunferencia > 40cm Genere Masculino *Dos o más respuestas positivas, riesgo de SAOS Baja sensib, bueneo en SAOS severa STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology 2008; 108:812–821. An excellent study of a screening tool for sleep apnea. Rev Chil Anest 2010; 39:

21
APNEA OBSTRUCTIVA DEL SUEÑO
Pacientes con tamizaje positivo Polisomnografia. AHI > 5/Hr. CPAP BiPAP 6 – 12 semanas antes de la Cx. Gases arteriales pre y post tratamiento en OSA severa. Anesthetic Management of Patients with Obesity with and Without Sleep Apnea Clin Chest Med 30 (2009) 569–579
 569–579.")
22
SISTEMA CARDIOVASCULAR
Gasto cardiaco aumenta 0.1 L/min por cada Kg adicional ↑ VO2 absoluto ↑ del volumen sanguíneo y sistólico. Hipertensión sistémica. 3-4 mmHg PS y 2 mmHg PD por cada 10 kg. Hipertensión pulmonar. Falla cardiaca. Enfermedad isquémica cardiaca. Anesthesia for bariatric surgery. ASA refresher Vol 33 Chapter 5, 2005

23
SISTEMA CARDIOVASCULAR
Anaesthetic considerations and management of the obese patient. Current Anaesthesia & Critical Care 21 (2010) 16–23
 16–23.")
24
SISTEMA CARDIOVASCULAR
Examen Físico: RsCs alejados. Cuello grueso. Edema de MsIs. Hepatomegalia. Movilidad Limitada. Anaesthetic considerations and management of the obese patient. Current Anaesthesia & Critical Care 21 (2010) 16–23
 16–23.")
25
EXÁMENES PRE QUIRÚRGICOS
EKG A todos (+ 1 FRCV). Signos de HTP BRIHH Arritmias Rayos X de tórax A todos? (Hipoventilaciòn o complic pulmonares) Signos de falla cardiaca. Signos de HTP. Ecocardiografía basal. Pacientes con signos y síntomas de ICC HTP OHS/OSA Espirometría: EPOC SHO o Cx mayor? RX fondo: obese female patient, BMI 64.3 (165 cm, 175 kg body weight Hallazgos EKG obeso: Solo 4% bajo voltaje, deviacion eje(horizontalizacion), , ST, T, auricula Cx mayor: P. func pulmonar Cardiovascular Evaluation and Management of Severely Obese Patients Undergoing Surgery (Circulation. 2009;120:86-95.)
. Signos de HTP. BRIHH. Arritmias. Rayos X de tórax. A todos (Hipoventilaciòn o complic pulmonares) Signos de falla cardiaca. Signos de HTP. Ecocardiografía basal. Pacientes con signos y síntomas de ICC. HTP. OHS/OSA. Espirometría: EPOC. SHO o Cx mayor RX fondo: obese female patient, BMI 64.3 (165 cm, 175 kg body weight. Hallazgos EKG obeso: Solo 4% bajo voltaje, deviacion eje(horizontalizacion), , ST, T, auricula. Cx mayor: P. func pulmonar. Cardiovascular Evaluation and Management of Severely Obese Patients Undergoing Surgery (Circulation. 2009;120:86-95.)")
26
PRUEBAS DE STRESS Ecocardiografía con dobutamina
Imposibilidad de hacer ejercicio. Pacientes con ≥ 1 factor de riesgo. Pobre ventana ecocardiográfica. Pruebas de esfuerzo cardiopulmonar. Pacientes que puedan hacer ejercicio. SPECT – PET Uso limitado. Cardiovascular Evaluation and Management of Severely Obese Patients Undergoing Surgery (Circulation. 2009;120:86-95.)
")
27
Paso 1 Paso 2 Paso 3 Paso 4 Paso 5
Paciente de bajo riesgo Sí Proceder con la cirugía planeada Paso 2 Un factor de riesgo ECG si signos de RVH considerar HTP CVD estable si signos de BRIHH considerar CAD Placa de tórax si hipoventilación Considerar gases arteriales Paso 3 Buena clase funcional Sí Proceder con la cirugía No, o no evaluable Paso 4 Técnica de imagen de función cardiaca Paso 5 Función sistólica disminuída Considerar cardiomiopatía /obesidad Considerar angiografía Justificación placa de tórax: AP y lateral alta incidencia post operatoria de eventos respiratorios puede sugerir falla cardiaca no diagnosticada dilatación de cavidades cardiacas o vasculatura pulmoanr anormal con signo de HTP Cardiovascular Evaluation and Management of Severely Obese Patients Undergoing Surgery (Circulation. 2009;120:86-95.)
")
28
EXÁMENES PRE QUIRÚRGICOS
Hemograma completo. Electrolitos. Función renal. Función Hepática. Función tiroidea. Glicemia Perfil lipídico. Cortisol. Cardiovascular Evaluation and Management of Severely Obese Patients Undergoing Surgery (Circulation. 2009;120:86-95.)
")
29
OBESITY SURGERY MORTALITY RISK SCORE (OS – MRS)
Inicialmente para Cx. bariátrica. IMC ≥ 50 kg/m². Masculino. Hipertensión sistémica. Edad > 45 años. Factores de riesgo para TVP/TEP. Puntuación Riesgo Mortalidad 0 – 1 Bajo – Clase A 0.2% 2 – 3 Intermedio – Clase B 1.2% 4 – 5 Alto – Clase C 2.4% Pulmonary embolism (30%)was the most common cause of death, followed by cardiac causes (27%) and anastomosis leak (21%). Anaesthetic considerations and management of the obese patient. Current Anaesthesia & Critical Care 21 (2010) 16–23
was the most common cause. of death, followed by cardiac causes (27%) and anastomosis leak (21%). Anaesthetic considerations and management of the obese patient. Current Anaesthesia & Critical Care 21 (2010) 16–23.")
30
VÍA AÉREA Anatomía alterada Acúmulo de grasa en cara y pómulos.
Macroglosia Cuello corto y grueso. Limitación de movimientos. Exceso de tejido en paladar y faringe. Anesthesia for bariatric surgery. ASA refresher Vol 33 Chapter 5, 2005

32
Reduction of the BMI allows for an increased interincisor gap, thyromental distance, and reduction in neck circumference. Mallampati classification remains the same.

33
Lofateo izq, ramped derecha
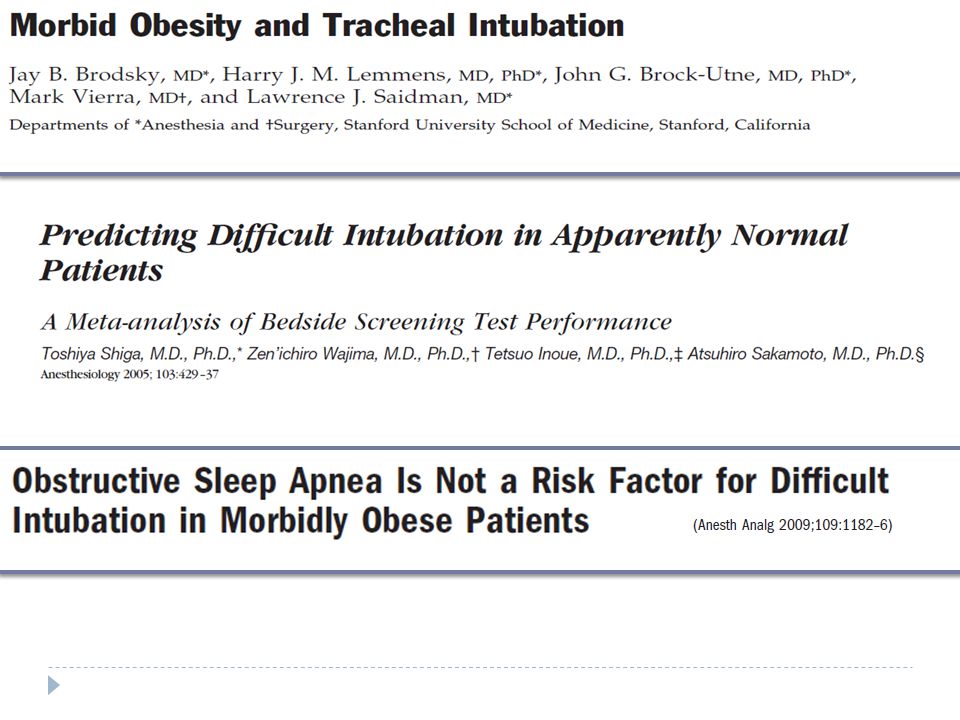
Colocar al paciente en “posición en rampa”, elevando la porción superior del tronco y la cabeza 20 a 30°, con objeto de alinear el meato auditivo externo y el hueco supraesternal, antes de la inducción e intubación traqueal La obesidad mórbida, reconocida históricamente como uno de los factores de riesgo de vía aérea difícil, hoy, a la luz de la experiencia en cirugía bariátrica, no constituye un factor de riesgo por sí misma, excepto en presencia de predictores de difi cultad reconocidos y de SAOS

34
Manejo de la vía aérea Dispositivos Anesth Analg 2003;96:1510–5.
Faltan estudios: Proseal: màs sobretodo ventilacion Anesth Analg 2003;96:1510–5. Clin Chest Med 30 (2009) 555–568
 555–568.")
35
Consideraciones Prácticas VA
Hay gran controversia Ventilación 3X difícil El IMC ni el AOS son predictores de VAD OSA severa?: Singapore Med J. 2011;52(2):94-9 Mallampati, CC y DTM mejor predicción Posición “ramped” parece ser la óptima Ayudas imagenológicas no validadas No se justifica intubación despierto en todos ALGUNOS: Despierto y en FOWLER NO ES LO MISMO!!! Dificultad Ventilación Mascarilla Facial Dificultad en la Laringoscopia Dificultad Intubación traqueal Pq: despierto: Resp espontanea, No dism de CRF, tono muscular, no need venmtilacion, , fowler: mejora intubacion y no dism mucho CRF, closing e intercambio Journal of Clinical Anesthesia (2011) 23, 575–586
:94-9. Mallampati, CC y DTM mejor predicción. Posición ramped parece ser la óptima. Ayudas imagenológicas no validadas. No se justifica intubación despierto en todos. ALGUNOS: Despierto y en FOWLER. NO ES LO MISMO!!! Dificultad Ventilación Mascarilla Facial. Dificultad en la Laringoscopia. Dificultad Intubación traqueal. Pq: despierto: Resp espontanea, No dism de CRF, tono muscular, no need venmtilacion, , fowler: mejora intubacion y no dism mucho CRF, closing e intercambio. Journal of Clinical Anesthesia (2011) 23, 575–586.")
36
OTRAS CONSIDERACIONES
Riesgo de aspiración. No diferencias en el volumen o pH gástrico en la población obesa. No premedicación rutinaria Sub-población de riesgo. Diabetes y gastroparesia. Signos y síntomas de reflujo gastro-esofágico. Hernia hiatal. Pacientes post cx. bariátrica. Endoscopia Digestiva Anesthesiology 2011;114: The risk of pulmonary aspiration in patients after weight loss due to bariatric surgery . Anesth Analg 2008;

37
OTRAS CONSIDERACIONES
Riesgo de trombosis. Desbalance entre mecanismos pro coagulantes y anticoagulantes. Disfunción endotelial. Hiper-reactividad plaquetaria. Disminución en la movilidad Aumento presión venosa en MsIs. Trombosis venosa y/o arterial. OR 2.33 IC 95% (1.68 – 2.34) Pacientes de mayor riesgo para eventos trombóticos. IMC > 60, obesidad troncal OHS/OSA, hipercoagulabilidad Antecedente personal de TVP o TEP. Profilaxi TVP/TEP: Heparina no fracc: 5000UI/3d Enoxap: 40mg/2d: riesgo de sobrdosificaciòn por peso HBPM: peso ideal y elevar 25% la dosis Obesity, Metabolic Syndrome, and the Surgical Patient Anesthesiology Clin 27 (2009) 705–719 Cardiovascular risk factors and venous thromboembolism: a meta-analysis. Circulation 2008;117:93–102
 Pacientes de mayor riesgo para eventos trombóticos. IMC > 60, obesidad troncal. OHS/OSA, hipercoagulabilidad. Antecedente personal de TVP o TEP. Profilaxi TVP/TEP: Heparina no fracc: 5000UI/3d. Enoxap: 40mg/2d: riesgo de sobrdosificaciòn por peso. HBPM: peso ideal y elevar 25% la dosis. Obesity, Metabolic Syndrome, and the Surgical Patient Anesthesiology Clin 27 (2009) 705–719. Cardiovascular risk factors and venous thromboembolism: a meta-analysis. Circulation 2008;117:93–102.")
38
OTRAS CONSIDERACIONES
Riesgo peri operatorio TVP % TEP % Uso de profilaxis reduce el riesgo de eventos trombóticos en un 72%. ¿ Cuál heparina y momento?? National analysis of adverse patient safety for events in bariatric surgery. Am Surg 2005;71:406–13 Obesity, Metabolic Syndrome, and the Surgical Patient Anesthesiology Clin 27 (2009) 705–719
 705–719.")
39
OTRAS CONSIDERACIONES
Rabdomiólisis Incidencia 12.9 – 37.8% Cirugía prolongada ( > 240 min) IMC > 50 kg/m². Técnicas abiertas. Neuropatías Asociación de un 29% entre obesidad y neuropatía cubital. Lesión del plexo braquial. Lesión del N. ciático (15%) Evitar posición de litotomía. Anaesthetic considerations and management of the obese patient. Current Anaesthesia & Critical Care 21 (2010) 16–23
 IMC > 50 kg/m². Técnicas abiertas. Neuropatías. Asociación de un 29% entre obesidad y neuropatía cubital. Lesión del plexo braquial. Lesión del N. ciático (15%) Evitar posición de litotomía. Anaesthetic considerations and management of the obese patient. Current Anaesthesia & Critical Care 21 (2010) 16–23.")
40
Despite a higher incidence of perioperative complications, mortality is not increased in overweight
and obesity grade II patients. By contrast, there is excess mortality in underweight and morbidly obese patients (BMI > 40 kg m2). With respect to mortality, overweight and obese patients (up to BMI < 40 kg m2) had – despite the common co-morbidities and the higher complication rate – an even lower mortality compared with normal-weight controls
. With respect to mortality, overweight and obese patients (up to BMI < 40 kg m2) had – despite the. common co-morbidities and the higher complication rate – an even lower mortality compared with. normal-weight controls.")
41
MEDICAMENTOS Medicamento Implicaciones Anestésicas. Fluoxetina
Bradicardia, convulsiones, sangrado, hiponatremia, hepatotoxicidad. Metformina Acidosis láctica. Orlistat Diarrea, déficit de Vit liposolubles. Sibutramina Taquicardia, Hipertensión, arritmias. Fentermina Problemas cardio respiratorios. Fenilpropalamina ACV hemorrágico Cromo No efectos reportados Efedrina HTA, Trastornos psiquiátricos, disfunción autonómica. When prescribing a drug for premedication, meticulous care should be taken, as many patients suffer from OSA (see earlier) and are particularly susceptible to benzodiazepines. Prescribing sedative drugs the evening before surgery should be avoided, if possible. On patient’s request, a short-acting benzodiazepine (midazolam) or a a2-adrenoceptor-agonist (clonidin) may be given preoperatively. Continuous monitoring of the patient must then be ensured Anesthesia for bariatric surgery. ASA refresher Vol 33 Chapter 5, 2008
 and are particularly susceptible to benzodiazepines. Prescribing sedative drugs the evening before surgery should be avoided, if possible. On patient’s. request, a short-acting benzodiazepine (midazolam) or a a2-adrenoceptor-agonist (clonidin) may be. given preoperatively. Continuous monitoring of the patient must then be ensured. Anesthesia for bariatric surgery. ASA refresher Vol 33 Chapter 5,")
42
PREMEDICACIÓN Evitar sedación pre operatoria.
Antisialagogos si se planea intubación con FB. Considerar AntiH2 – Metoclopramida o Inhibidor de bomba de protones antes de una anestesia general. Profilaxis antibiótica y antitrombótica. Profilaxis PONV. No premedi rutina : 2011 Journal of Clinical Anesthesia (2011) 23, 575–586 Anesthesiology 2011;114: Anesthesia for bariatric surgery. ASA refresher Vol 33 Chapter 5, 2005
 23, 575–586 Anesthesiology 2011;114: Anesthesia for bariatric surgery. ASA refresher Vol 33 Chapter 5,")
43
Equipos y Logística Levantadores adecuados Sanitarios: Hasta 150 Kg
Camas y equipos de enfermería adecuados Mesa Qx: Hasta 150 kg. Disponer de 350 kg Camillas de transporte adaptadas Levantadores adecuados Personal entrenado Medias de compresión intermitente Protección postural Agujas para A. Regional Attention should be paid to protect compression points with soft foam or gel pads that must be available in different types in a sufficient number. The incidence of compression of the sciatic and ulnar nerves was reported to be higher in obese than in normal-weight patients.26,27 Lumbar compartment syndromes have been repeatedly reported, particularly after prolonged interventions

44
Operating table for patients up to 350 kg body weight

45
MANEJO INTRAOPERATORIO
+ tpo Qx qu epuede llevar a complica, sobretodo Rabdomiolisis en laparoscopias Too + conversiòn a cirufgia abierta: lo anterior son tendencias tendencias

46
POSICIÓN Mesa de cirugía adecuada.
Adecuada protección de zonas de presión. Fowler 25º mejor tolerada. En prono dejar abdomen libre. Trendelenburg y litotomía disminuyen los Vol. Pulmonares y aumenta el riesgo de neuropatías. Anaesthetic considerations and management of the obese patient. Current Anaesthesia & Critical Care 21 (2010) 16–23
 16–23.")
47
Poner esta foto de fondo en anterior

48
MONITORIZACIÓN ASA básico. Monitoreo de nervio periférico.
Agujas / electrodos convencionales. Línea arterial. Procedimientos de alto riesgo. No hay adecuada medición de PANI. Ultra obesos (IMC > 60 kg/m²) Catéter venoso central Imposibilidad de accesos periféricos. Lecturas alteradas de PVC ¿Métodos no invasivos? Volumetric variables of preload, such as the global end-diastolic volume index (GEDVI), may be advantageous in this patient population. Dynamic variables of fluid responsiveness, such as stroke volume variation (SVV) and pulse pressure variation (PPV), may also be reliable in obese patients. The threshold values indicating fluid responsiveness, however, may be altered in these patients due to increased intra-abdominal pressure Anaesthetic considerations and management of the obese patient. Current Anaesthesia & Critical Care 21 (2010) 16–23
 Catéter venoso central. Imposibilidad de accesos periféricos. Lecturas alteradas de PVC. ¿Métodos no invasivos Volumetric variables of preload, such as the global end-diastolic volume index (GEDVI), may be advantageous in this patient population. Dynamic variables of fluid responsiveness, such as. stroke volume variation (SVV) and pulse pressure variation (PPV), may also be reliable in obese. patients. The threshold values indicating fluid responsiveness, however, may be altered in these. patients due to increased intra-abdominal pressure. Anaesthetic considerations and management of the obese patient. Current Anaesthesia & Critical Care 21 (2010) 16–23.")
49
CONSIDERACIONES FARMACOLÓGICAS
Los cambios fisiológicos en la población obesa afecta la distribución, unión a proteínas y la eliminación de varios agentes anestésicos. Medida Hombres Mujeres Peso Ideal Altura (cm) – 100 Altura (cm) – 105 50kg (150 cm) kg x cada 2.5 cm adicionales 45 kg (150 cm) kg x cada 2.5 cm adicionales Peso magro 80 % del peso total 75 % peso total Peso ideal + el 30% Peso ideal + el 20% Por peso magro: se infraestima, por real: se sobreestima dosis exc blo musculares Lean body weight (LBW) is highly correlated with the increased cardiac output, more so than fat mass or other variables. For most drugs, clearance increases nonlinearly with total body weight but linearly with LBW. Morbid obesity has no clinically significant impact on the uptake of the inhalation anesthetics isoflurane, sevoflurane, and desflurane when used in routine clinical practice. Total body weight dosing of neuromuscular blocking agents will result in a prolonged effect For the induction dose of hypnotics and the initial dose of other drugs that have a fast onset of effect, cardiac output or LBW are relevant dosing scalars. For maintenance dosing, LBW seems to be a more appropriate dosing scalar than total body weight Peso ideal. Talla (cm) Hombres=49.9kg+0.89(talla-152.4) Mujeres= (talla-152.4) O Talla – 100 hombres Talla – 105 mujeres Anaesthetic considerations and management of the obese patient. Current Anaesthesia & Critical Care 21 (2010) 16–23
 – 100. Altura (cm) – kg (150 cm) kg x cada 2.5 cm adicionales. 45 kg (150 cm) kg x cada 2.5 cm adicionales. Peso magro. 80 % del peso total. 75 % peso total. Peso ideal + el 30% Peso ideal + el 20% Por peso magro: se infraestima, por real: se sobreestima dosis exc blo musculares. Lean body weight (LBW) is highly correlated with the increased cardiac output, more so than fat mass or other variables. For most drugs, clearance increases nonlinearly with total body weight but linearly with LBW. Morbid obesity has no clinically significant impact on the uptake of the inhalation anesthetics isoflurane, sevoflurane, and desflurane when used in routine clinical practice. Total body weight dosing of neuromuscular blocking agents will result in a prolonged effect. For the induction dose of hypnotics and the initial dose of other drugs that have a fast onset of effect, cardiac output or LBW are relevant dosing scalars. For maintenance dosing, LBW seems to be a more appropriate dosing scalar than total body weight. Peso ideal. Talla (cm) Hombres=49.9kg+0.89(talla-152.4) Mujeres= (talla-152.4) O. Talla – 100 hombres. Talla – 105 mujeres. Anaesthetic considerations and management of the obese patient. Current Anaesthesia & Critical Care 21 (2010) 16–23.")
50
CONSIDERACIONES: Peso magro (- relajantes)
Agente Dosis Propofol Inducción Peso Ideal Mantenimiento Peso Magro Tiopental Inducción Peso Magro Midazolam Peso Total Succinilcolina Rocuronio Peso Ideal Cis – Atracurio Vecuronio Fentanyl Peso Total/Ideal Remifentanyl Peso ideal Dexmedetomidina Peso Magro Succinilcolina: mas dosis por +pseudocolinesterasas y LEC Anaesthetic considerations and management of the obese patient. Current Anaesthesia & Critical Care 21 (2010) 16–23
 16–23.")
51
TÉCNICA ANESTÉSICA Si la cirugía y el paciente lo permiten se debe considerar la anestesia regional (Neuroaxial o Bloqueo N. periférico) Control del dolor POP ↓ necesidad de opiodes. Evita sedación residual y preserva respiración Anestesia general balanceada cuando sea estrictamente necesario, en pacientes súper obesos o con OSA Opinion expertos Perioperative Considerations for the Morbidly Obese Patient. Advances in Anesthesia 25 (2007) 59–77
 59–77.")
52
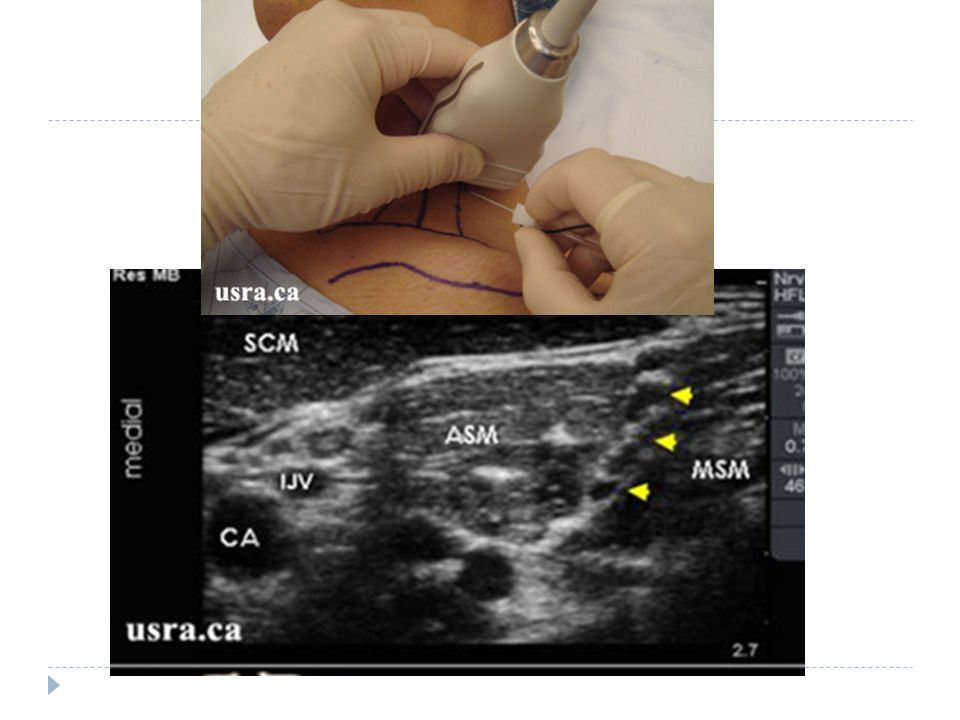
Riesgo de bloqueos fallidos es 1.62 veces mayor.
Existe mayor probabilidad de complicaciones asociados a la anestesia regional. Precaución con neuropatías periféricas post – cx. Idealmente deben ser colocados por anestesiólogos entrenados y bajo guía ecográfica. Requerimientos de AL se disminuyen en un 20% - 30% en técnicas neuroaxiales. Us pa bloqeuos y epidural: imagen Journal of Clinical Anesthesia (2011) 23, 575–586;
 23, 575–586;")
54
ANESTESIA GENERAL Oxigenación preinducción. 5 min O2 al 100%
20 – 25º Fowler Vs posición de rampa. Pre oxigenación con PEEP de 10 cm de H2O x 5 min seguida en la inducción de la anestesia con ventilación mecánica por medio de una máscara facial con PEEP de 10 cm de H2O aumentó la duración de la apnea no hipóxica un 50%. O CPAP pòr 5 min: menos desatuiracion PEEP during induction of general anesthesia increases duration of nonhypoxic apnea in morbidly obese patients. Anesth Analg 2005;100:580–4. Perioperative Considerations for the Morbidly Obese Patient. Advances in Anesthesia 25 (2007) 59–77 Journal of Clinical Anesthesia (2011) 23, 575–586
 59–77 Journal of Clinical Anesthesia (2011) 23, 575–586.")
55
Preoxygenation via a close-fitting face mask
Beach-chair position for endoscopic gastric resection. This position is also suitable for induction of anaesthesia

56
. 70 pacientes con IMC > 35 kg/m²
Pre-oxigenación con O2 100% 5 min, fentanyl ( mcg), Precurarización con rocuronio (5 mg), propofol (2 mg/kg). Succinilcolina (1.5 mg/kg) Mantenimiento con Sevofluorane (2%) Vs. Desfluorane (6%), mezcla de O2 y aire al 50%. No diferencias en la emergencia de la anestesia. Similares características de recuperación 50 pacientes con IMC > 35 kg/m² No diferencias relevantes en la recuperación en PACU entre los pacientes anestesiados con sevofluorane o desfluorane. Ambos agentes son seguros y proporcionan una adecuada recuperación en pacientes con obesidad mórbida. Incidencia de PONV fue menor en el grupo de sevofluorane Mejor perfil hemodinámico en el grupo de sevofluorane VS ISORANE
, Precurarización con rocuronio (5 mg), propofol (2 mg/kg). Succinilcolina (1.5 mg/kg) Mantenimiento con Sevofluorane (2%) Vs. Desfluorane (6%), mezcla de O2 y aire al 50%. No diferencias en la emergencia de la anestesia. Similares características de recuperación. 50 pacientes con IMC > 35 kg/m². No diferencias relevantes en la recuperación en PACU entre los pacientes anestesiados con sevofluorane o desfluorane. Ambos agentes son seguros y proporcionan una adecuada recuperación en pacientes con obesidad mórbida. Incidencia de PONV fue menor en el grupo de sevofluorane. Mejor perfil hemodinámico en el grupo de sevofluorane VS ISORANE.")
57
VENTILACIÓN Reclutamiento
Volúmenes corrientes > 20 ml/kg (PCI) Aumento de las presiones en la VA sin obtener mejoría en la saturación arterial de O2. Hipocapnia excesiva. Ventilación mecánica protectora. Volumen corriente 6-10 ml/kg FIO %. Frecuencia 14 – 16 x minuto. PEEP 5 – 10 cm H2O. Monitorice Pplateua y PEEPi Ventilación controlada por presión. Laparoscopia o en Trendelenburg extremo. Br J Anaesth May;100(5):709-16 Ventilación espontánea. Adición de presión soporte y mantener el PEEP disminuye atelectasias. Laparoscopia: Mejor por presiòn: mejor Pafi, sat O2 y gases MencionarManionras reclutamniento: 35-55cmH2O por 6s seguidos de PEEP 10)ver los abstract que pegue por ahí en la ppt Journal of Clinical Anesthesia (2011) 23, 575–586 Some anesthetic aspects of morbid obesity Current Opinion in Anaesthesiology 2009, 22:442–446 . Advances in Anesthesia 25 (2007) 59–77
 Aumento de las presiones en la VA sin obtener mejoría en la saturación arterial de O2. Hipocapnia excesiva. Ventilación mecánica protectora. Volumen corriente 6-10 ml/kg FIO %. Frecuencia 14 – 16 x minuto. PEEP 5 – 10 cm H2O. Monitorice Pplateua y PEEPi. Ventilación controlada por presión. Laparoscopia o en Trendelenburg extremo. Br J Anaesth May;100(5): Ventilación espontánea. Adición de presión soporte y mantener el PEEP disminuye atelectasias. Laparoscopia: Mejor por presiòn: mejor Pafi, sat O2 y gases. MencionarManionras reclutamniento: 35-55cmH2O por 6s seguidos de PEEP 10)ver los abstract que pegue por ahí en la ppt. Journal of Clinical Anesthesia (2011) 23, 575–586. Some anesthetic aspects of morbid obesity Current Opinion in Anaesthesiology 2009, 22:442– Advances in Anesthesia 25 (2007) 59–77.")
58
CIRCULACIÓN Neumoperitoneo Manejo de líquidos.
Aumento resistencias vasculares. Reducción del GC y la TFG. Presión ideal 15 mmHg – Máximo 20 mmHg. Efectos exacerbados por Trendelenburg y PEEP. Manejo de líquidos. Liberal (12ml/kg/hr) Vs Restrictiva (4ml/kg/hr) Cristaloides o coloides hasta Hto > 25% Transfusión sanguínea Hto < 25% BACKGROUND: Respiratory function is impaired in obese patients undergoing laparoscopic surgery. This study was performed to determine whether repeated lung recruitment combined with PEEP improves respiratory compliance and arterial partial pressure of oxygen (Pa(O2)) in obese patients undergoing laparoscopic gastric banding. METHODS: Sixty patients with BMI >30 kg m(-2) were randomized, after induction of pneumoperitoneum, to receive either PEEP of 10 cm H2O (Group P), inspiratory pressure of 40 cm H2O for 15 s once (Group R), Group R recruitment followed by PEEP 10 cm H2O (Group RP), or Group RP recruitment but with the inspiratory manoeuvre repeated every 10 min (Group RRP). Static respiratory compliance and Pa(O2) were determined after intubation, 10 min after pneumoperitoneum (before lung recruitment), and every 10 min thereafter (after recruitment). Results are presented as mean (SD). RESULTS: Pneumoperitoneum decreased respiratory compliance from 48 (3) to 30 (1) ml cm H2O(-1) and decreased Pa(O2) from 12.4 (0.3) to 8.8 (0.3) kPa in all groups (P<0.01). Immediately after recruitment, compliance was 32 (1), 32 (2), 40 (2), and 40 (1) ml cm H2O(-1) and Pa(O2) was 9.1 (0.3), 9.1 (0.1), 11.9 (0.1), and 11.9 (0.1) kPa in Groups P, R, RP, and RRP, respectively (P<0.01). Ten and 20 min later, Pa(O2) in Group R decreased to 9.2 (0.1) kPa and compliance in Group PR decreased to 33 (2) ml cm H2O(-1), respectively (P<0.01). CONCLUSIONS: Group RRP recruitment strategy was associated with the best intraoperative respiratory compliance and Pa(O2) in obese patients undergoing laparoscopic gastric Some anesthetic aspects of morbid obesity Current Opinion in Anaesthesiology 2009, 22:442–446 Perioperative Considerations for the Morbidly Obese Patient. Advances in Anesthesia 25 (2007) 59–77
 Vs Restrictiva (4ml/kg/hr) Cristaloides o coloides hasta Hto > 25% Transfusión sanguínea Hto < 25% BACKGROUND: Respiratory function is impaired in obese patients undergoing laparoscopic surgery. This study was performed to determine whether repeated lung recruitment combined with PEEP improves respiratory compliance and arterial partial pressure of oxygen (Pa(O2)) in obese patients undergoing laparoscopic gastric banding. METHODS: Sixty patients with BMI >30 kg m(-2) were randomized, after induction of pneumoperitoneum, to receive either PEEP of 10 cm H2O (Group P), inspiratory pressure of 40 cm H2O for 15 s once (Group R), Group R recruitment followed by PEEP 10 cm H2O (Group RP), or Group RP recruitment but with the inspiratory manoeuvre repeated every 10 min (Group RRP). Static respiratory compliance and Pa(O2) were determined after intubation, 10 min after pneumoperitoneum (before lung recruitment), and every 10 min thereafter (after recruitment). Results are presented as mean (SD). RESULTS: Pneumoperitoneum decreased respiratory compliance from 48 (3) to 30 (1) ml cm H2O(-1) and decreased Pa(O2) from 12.4 (0.3) to 8.8 (0.3) kPa in all groups (P<0.01). Immediately after recruitment, compliance was 32 (1), 32 (2), 40 (2), and 40 (1) ml cm H2O(-1) and Pa(O2) was 9.1 (0.3), 9.1 (0.1), 11.9 (0.1), and 11.9 (0.1) kPa in Groups P, R, RP, and RRP, respectively (P<0.01). Ten and 20 min later, Pa(O2) in Group R decreased to 9.2 (0.1) kPa and compliance in Group PR decreased to 33 (2) ml cm H2O(-1), respectively (P<0.01). CONCLUSIONS: Group RRP recruitment strategy was associated with the best intraoperative respiratory compliance and Pa(O2) in obese patients undergoing laparoscopic gastric. Some anesthetic aspects of morbid obesity Current Opinion in Anaesthesiology 2009, 22:442–446. Perioperative Considerations for the Morbidly Obese Patient. Advances in Anesthesia 25 (2007) 59–77.")
59
Diez minutos antes de Extubación
1. Mantener Fowler 2. ↓ FIO2 a 40% 3. Succión VA 4. Reclutamiento: cmH2O por 6 seg luego PEEP 10 5. No succionar tubo durante extubación

60
CUIDADOS POST OPERATORIOS

61
POST OPERATORIO Extubación UCI/UCE CPAP / BiPAP
Completamente despierto. Capaz de seguir órdenes. Analgesia adecuada Relajación residual. Normotermia UCI/UCE Cardiópatas. OSA/OHS. Cx Prolongada. CPAP / BiPAP Reiniciar lo antes posible. Antes de extubar: Hipoxemia y dism CRF hasta 3-7 dias POP Anesthesia for bariatric surgery. ASA refresher Vol 33 Chapter 5, 2005 Anaesthetic considerations and management of the obese patient. Current Anaesthesia & Critical Care 21 (2010) 16–23
 16–23.")
62
Obeso Mórbido Atelectasias Neumonìa TVP / TEP
Depresión respiratoria por opioides Agravar AOS Recuperar sentado Espirometría incentiva, Presión positiva intermitente Equipo de CPAP o NPPV 1as 24 horas POP Seguir profilaxis TVP + riesgo de: Equipo CPAP=: si utilizaba en casa para AOS

63
POST OPERATORIO Profilaxis anti-trombótica. Analgesia
Deambulación precoz Analgesia Multimodal Evitar uso excesivo de opiodes. PCA calculadas según peso ideal. Anestesia regional: ↓ opioides Dolor Osteomuscular por mesa Anesthesia for bariatric surgery. ASA refresher Vol 33 Chapter 5, 2005 Anaesthetic considerations and management of the obese patient. Current Anaesthesia & Critical Care 21 (2010) 16–23
 16–23.")
64
CONCLUSIÓN El manejo perioperatorio del gran obeso por sus múltiples comorbilidades y particularidades implica múltiples retos y no sólo la “temida” vía aérea Obesity is a worldwide epidemic with increasing importance in both industrialised and developing countries. Anaesthesiologists will be increasingly challenged by the care for morbidly and super-obese patients. Prerequisites for an optimal perioperative care are a suitable environment on the ward, the timely and comprehensive preoperative evaluation focussed on co-morbidities, such as diabetes, coronary artery disease and OSA syndrome and appropriate equipment for positioning, anaesthesia and surgery. To deliver an adequate standard of care, anaesthesiologists must consider the pharmacokinetic characteristics and pathophysiological sequelae of obesity

Presentaciones similares