Descargar la presentación
La descarga está en progreso. Por favor, espere

1
VENTILACION NO INVASIVA EN NIÑOS
DRA CECILIA TABOADA PALOMINO MEDICO PEDIATRA – INTENSIVISTA UCIP HOSPITAL E. REBAGLIATI UCIP CLINICA RICARDO PALMA PEDIATRA CLINICA RICARDO PALMA

2
VENTILACION NO INVASIVA
ES LA ADMINISTRACION DE SOPORTE VENTILATORIO SIN LA COLOCACION DE UNA VIA AEREA ARTIFICIAL SEA INTUBACION TRAQUEAL O TRAQUEOSTOMIA, UTILIZA INTERFASES ( MASCARAS ) Respir Care. 2002;47(4):508-18
 Respir Care. 2002;47(4):")
3
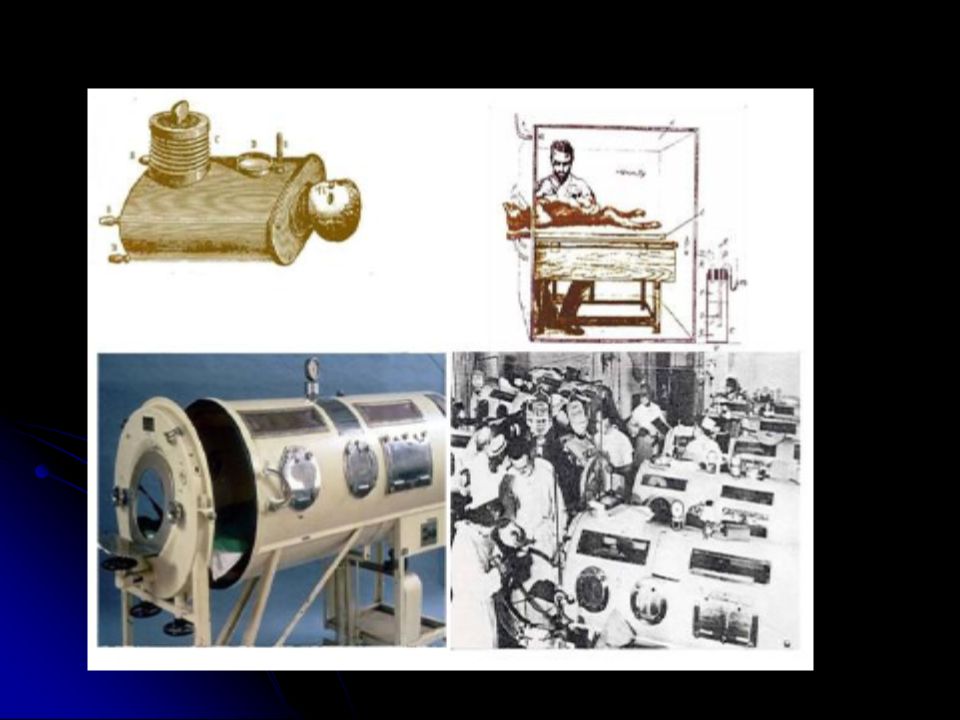
INICIO EN LOS AÑOS 60 : VENTILAR A LOS PACIENTES
H I S T O R I A INICIO EN LOS AÑOS 60 : VENTILAR A LOS PACIENTES CON PARALISIS RESPIRATORIA EN LA EPIDEMIA DE POLIO SE POPULARIZO EN LOS AÑOS 80 , EN SOPORTE DOMICILIARIO PARA ADULTOS , CON APNEA OBSTRUCTIVA ( CPAP ) USO SE EXTENDIO A PACIENTES CON ENFERMEDAD NEUROMUSCULAR AÑOS 90 : EMPIEZA A USAR EN PEDIATRIA INICIALMENTE EN NIÑOS CON ENFERMEDADES NEUROMUSCULARES, ACTUALMENTE EN INSUFICIENCIA RESPIRATORIA HIPERCAPNICA Y EN ALGUNAS HIPOXEMICAS
 USO SE EXTENDIO A PACIENTES CON ENFERMEDAD NEUROMUSCULAR. AÑOS 90 : EMPIEZA A USAR EN PEDIATRIA. INICIALMENTE EN NIÑOS CON ENFERMEDADES NEUROMUSCULARES, ACTUALMENTE EN INSUFICIENCIA RESPIRATORIA HIPERCAPNICA Y EN ALGUNAS HIPOXEMICAS.")
5
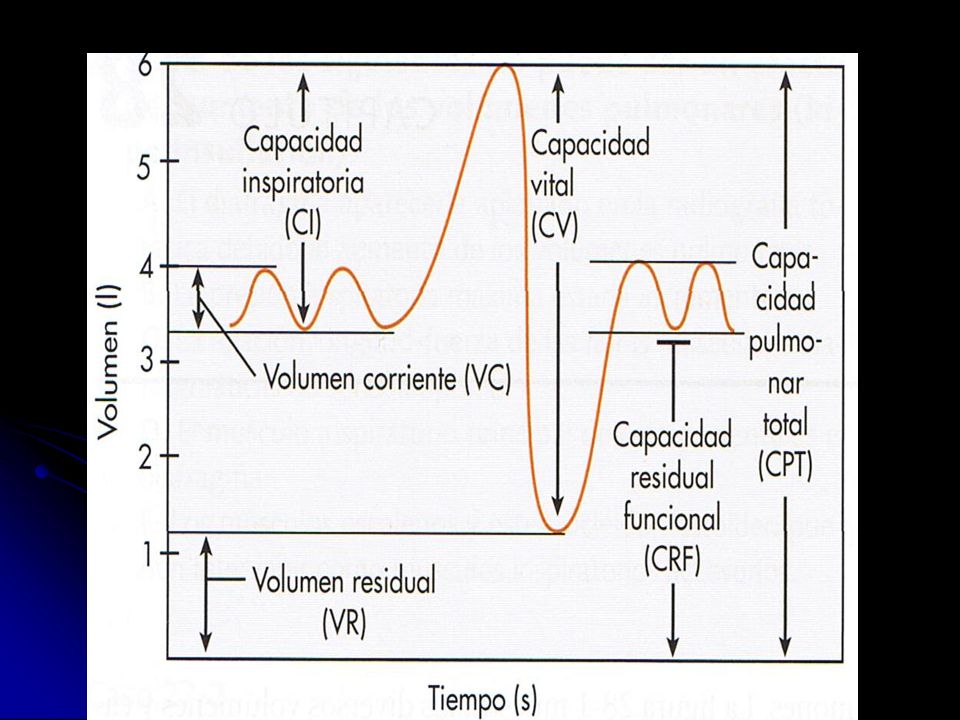
EFECTOS FISIOLOGICOS DE LA VNI
DISMINUIR EL TRABAJO VENTILATORIO -DISMINUIR LA FATIGA -AUMENTAR EL VOLUMEN MINUTO -AUMENTAR LA CAPACIDAD RESIDUAL FUNCIONAL -MEJORAR LA RELACION VENTILACION – PERFUSION -MEJORA EN LA OXIGENACION -OPTIMIZAR LA DIMANICA RESPIRATORIA -EVITA FORMACION ATELECTASIAS

7
VENTAJAS ADICIONALES EVITAR COMPLICACIONES ASOCIADAS A IOT SIMPLE
MEJORAR CONFORT PACIENTE PRESERVA LOS MECANISMOS DE DEFENSA DE LA VIA AEREA PRESERVA LA COMUNICACIÓN PRESERVA LA DEGLUCION FACIL DE INICIAR , FACIL DE TERMINAR

8
VENTAJAS ADICIONALES MENOR USO DE SEDANTES
DISMINUYE INCIDENCIA ATROFIA MUSCULOS VENTILATORIOS, INDUCIDO POR LA VMI ELIMINA TRABAJO IMPUESTO POR TET MENORES COMPLICACIONES

9
CONSIDERACIONES BASICAS
NECESIDAD DE USAR UNA INTERFASE CONFORTABLE SELECCIÓN ADECUADA DE PARAMETROS DE VENTILACION MONITORIZACION APROPIADA PRINCIPALMENTE : ATENCION DE UN EQUIPO ENTRENADO

10
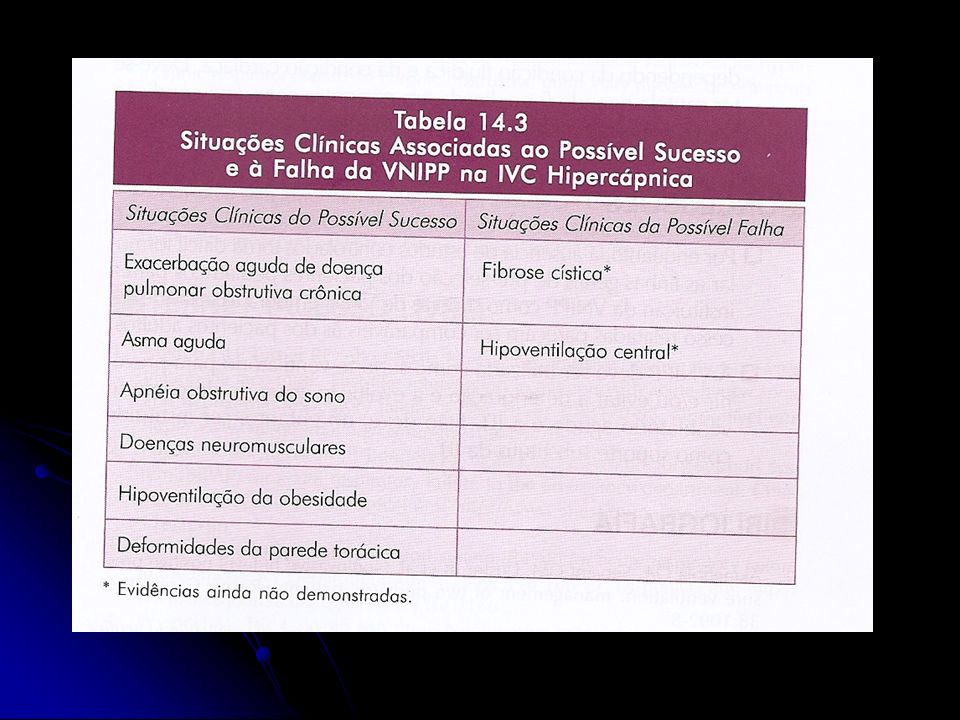
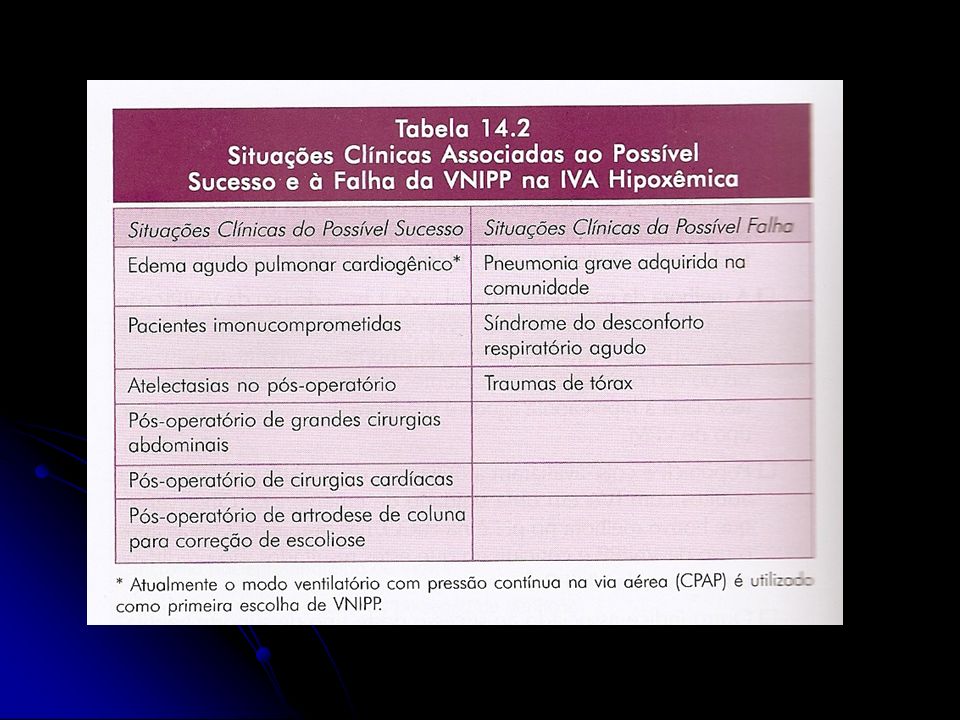
INDICACIONES Insuficiencia respiratoria crónica agudizada ( neumonia ,
Atelectasias , postoperatoria ) Enfermedades neuromusculares: atrofia espinal, enfermedad de Duchebnne Fibrosis quística: fase pretrasplante SAOS, cifoescoliosis Insuficiencia respiratoria aguda hipoxémica Neumonía (Pneumocystis, Legionella) Insuficiencia respiratoria postextubación Edema agudo de pulmón Insuficiencia respiratoria en paciente oncológico
 Enfermedades neuromusculares: atrofia espinal, enfermedad. de Duchebnne. Fibrosis quística: fase pretrasplante. SAOS, cifoescoliosis. Insuficiencia respiratoria aguda hipoxémica. Neumonía (Pneumocystis, Legionella) Insuficiencia respiratoria postextubación. Edema agudo de pulmón. Insuficiencia respiratoria en paciente oncológico.")
11
domiciliaria en pacientes neuromusculares
Indicaciones de ventilación no invasiva domiciliaria en pacientes neuromusculares Atelectasias/neumonías de repetición Capacidad vital < 40% Disminución del 25 % de la capacidad vital en decúbito SatHb < 95 % diurna sin patología respiratoria aguda Registro pulsioximétrico nocturno patológico SatHb inferior a 90% > a 1 h Episodios de bradicardia secundarios a desaturación

12
To assess the effect of institution of noninvasive ventilation (NIV) on clinical outcome and quality of life (QOL) in a cohort of children with severe neuromuscular disorders. Conclusion: Treatment of respiratory failure, in children with neuromuscular disease, with noninvasive ventilation results in a reduction in symptoms, hospitalizations, and health care costs without adverse effects on quality of life.

13
USO PRECOZ EN ENFERMEDADES NEUROMUSCULARES

14
CONTRAINDICACIONES AUSENCIA DE ESTIMULO RESPIRATORIO
AUSENCIA DE REFLEJO DE TOS SECRECIONES RESPIRATORIAS ABUNDANTES NEUMOPATIA BULOSA NEUMOTORAX INESTABILIDAD HEMODINAMICA ANSIEDAD O FALTA DE COLABORACION DEL PACIENTE INFECCION SINUSAL , OTICA HEMORRAGIA DIGESTIVA ALTA, VOMITOS , DISTENSION ABDOMINAL CIRUGIA DE CARA , TEC, CIRUGIA DE SENOS PARANASALES

15
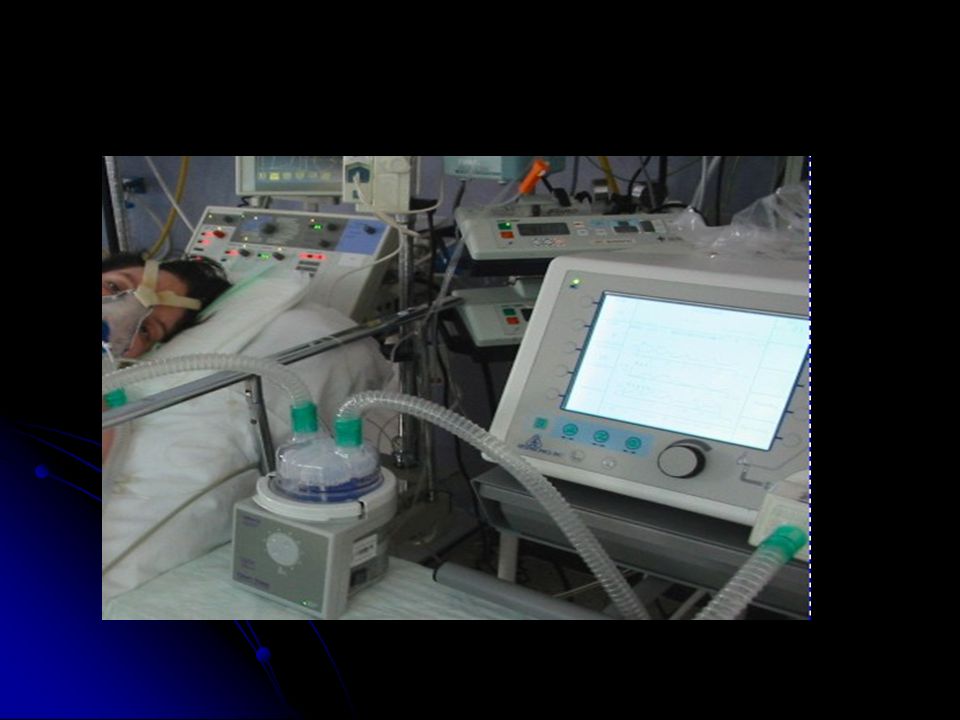
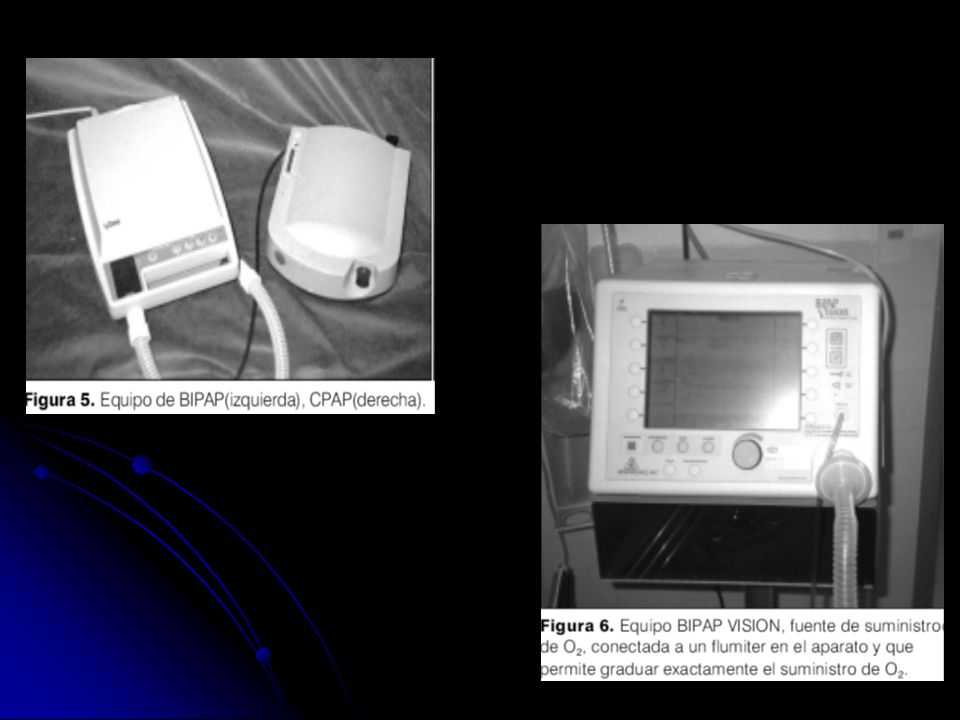
MATERIAL NECESARIO INTERFASES O MASCARAS VENTILADORES MECANICOS
EQUIPO MULTIDISCIPLINARIO ENTRENADO

16
I N T E R F A S E S

17
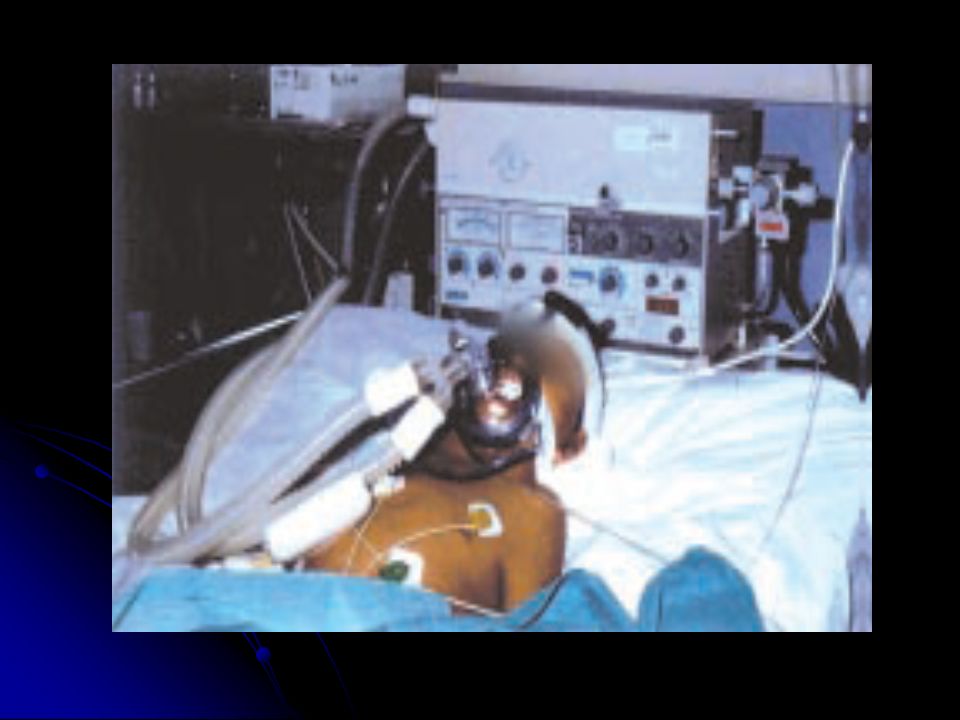
MASCARILLAS O INTERFASES
SON LOS ELEMENTOS QUE PERMITEN LA ADECUADA ADAPTACION ENTRE VENTILADOR Y PACIENTE SELLAN LA VIA AEREA DEL PACIENTE LA ADECUADA ADAPTACION DE LA INTERFASE A LA ANATOMIA DEL PACIENTE ES UN FACTOR PRINCIPAL QUE DETERMINA EL ÉXITO O FRACASO DE LA TECNICA. MATERIAL DE LA MASCARILLA ES VARIABLE , LA SILICONA ES VARIABLE , PERMITE SER MODELABLE Y UN MEJOR ACOPLAMIENTO AL PACIENTE.

18
SISTEMAS DE SUJECION GORROS O CINCHAS LOGRAR UN AJUSTE ADECUADO

22
MASCARILLA NASOBUCAL SELLA NARIZ Y BOCA. SE CONSIGUE MEJOR CONTROL SOBRE LAS PRESIONES ES MAS CLAUSTROFOBICA MAYOR RIESGO DE ASPIRACION EN CASO D E VOMITO MENOS COMODA PARA SU USO A LARGO PLAZO

24
MASCARILLA NASAL MAS COMODA
NECESARIO QUE PAC. MANTENGA BOCA CERRADA .EN CASO CONTRARIO LA COMPENSACION D E FUGAS HARA INTOLE RABLE LA MASCARA SELLA LA PARTE SUPERIOR DEL TRIANGULO NASOGENIANO, DEJA LIBRE LA BOCA EXISTE UNA VARIACION : INTERFASE TIPO ADAMS, QUE SE ACOPLA EN LAS FOSASNASALES Y SE APOYA EN EL VERTICE CRANEAL, EVITANDO APOYARSE EN EL PUENTE NASAL.

26
MASCARILLA FACIAL COMPLETA
MINIMIZA POSIBILIDAD D E FUGAS NORMALMENTE D E MATERIAL RIGIDO, MEDIANTE UNA FINA LAMINA DE SILICONA SE ADAPTA A LA CARA, LA CUAL QUEDA ENTERA INCLUIDA EN SU INTERIOR. PROPORCIONA PUNTOS DE APOYO DIFERENTES A LAS OTRAS INTERFASES, LO QUE PERMITE PERIODOS DE DESCANSO O RECUPERAC. DE LESIONES . IMPIDE LA ALIMENTACION MAYOR RIESGO D E ASPIRACION POR VOMITOS GRAN CANTIDAD DE ESPACIO MUERTO SENSACION DE SOFOCO Y CALOR

28
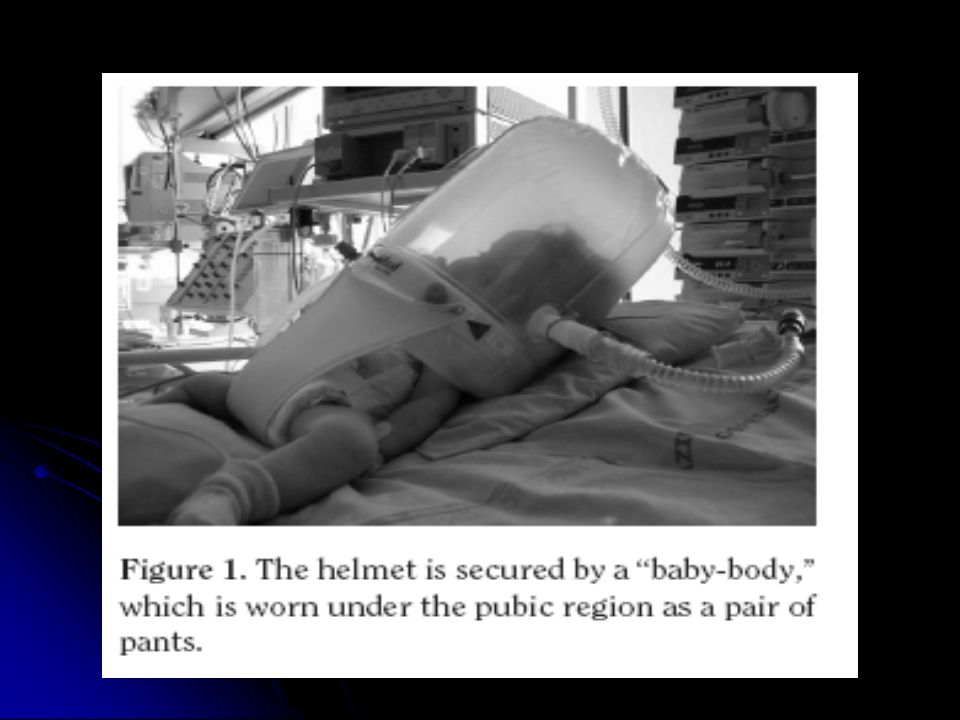
Interfase tipo Helmet.

30
RESPIRADORES RESPIRADORES DE VNI COMPENSAN FUGAS FACILES DE USAR
TRANSPORTABLES PERMITEN USO DOMICILIARIO NO TODOS TIENEN OXIGENO INCORPORADO SOLO ALGUNOS PERMITEN MONITORIZACION

36
RESPIRADORES CONVENCIONALES
NO COMPENSAN FUGAS NO SINCRONIZAN BIEN CON EL PACIENTE NO USO DOMICILIARIO POSIBLIDAD DE MONITORIZACION

38
PASOS PARA APLICAR LA VNI
A ) Determinar si el paciente necesita asistencia ventilatoria: clínicos , laboratoriales Determinar basado en las indicaciones y contraindicaciones si el niño es candidato a la instalación de la VNI o a IOT Si el niño es candidato a la VNI, escoger la interfase y elegir los parámetros ventilatorios iniciales. D ) Monitorizar desde el inicio, la tolerancia, confort y la sincronía con el aparato. E ) Monitorizar las variables para evaluar éxito o fracaso de la VNI, despues de una o dos horas de iniciada.
 Determinar si el paciente necesita asistencia ventilatoria: clínicos , laboratoriales. Determinar basado en las indicaciones y contraindicaciones. si el niño es candidato a la instalación de la VNI o a IOT. Si el niño es candidato a la VNI, escoger la interfase y elegir. los parámetros ventilatorios iniciales. D ) Monitorizar desde el inicio, la tolerancia, confort y la sincronía con. el aparato. E ) Monitorizar las variables para evaluar éxito o fracaso de la VNI, despues de una o dos horas de iniciada.")
39
PROTOCOLO PARA EL INICIO DE LA VNI
Monitorización apropiada De cubito elevado, 30 – 45 grados Seleccionar y adaptar la interfase Seleccionar los parámetros ventilatorios Protección de cara , evitando tensión excesiva de la máscara Conectar la interfase al circuito del ventilador Iniciar con presiones o volumenes bajos: limite de presión inspiratoria 8 a 12 cm presión espiratoria a 5 cm límite de volumen : 10 ml /kg frecuencia baja, modo espontaneo, asistido Aumentar la presión gradualmente, o el volumen Iniciar suplementación de O2 si necesita Evaluar extravasamiento de aire, reajustar la máscara si es necesario

41
MONITORIZACION Y VIGILANCIA
RESPUESTA CLINICA SCORE DE DIFICULTAD RESPIRATORIA , FRECUENCIA RESPIRATORIA EVALUACION DEL CONFORT Y ANSIEDAD FUGAS PRESENCIA DE DISTENSION ABDOMINAL PULSIOXIMETRIA CONTROL GASOMETRICO

42
CAUSAS DE FRACASO DE LA VNIP
EMPEORA DEL PROCESO PATOLOGICO NO COOPERACION DEL PACIENTE APARATOS INADECUADOS ASIMETRIA DE FASE ESCAPES NO COMPENSADOS POR EL VENTILADOR TOS INADECUADA , RETENCION DE SECRECIONES GRAN ALTERACION DEL INTERCAMBIO GASEOSO

45
CAUSAS DE FRACASO DE LA VNIPP
A small prospective study of infants and children in the ICU undergoing NIPPV for respiratory failure demonstrated that inspired oxygen (FIO2) after 1 hour of NIPPV may be a predictor for outcome, with a requirement for an FIO2 greater than 80% being associated with NIPPV failure
 after 1 hour of NIPPV may be a predictor for outcome, with a requirement for an FIO2 greater than 80% being associated with NIPPV failure.")
46
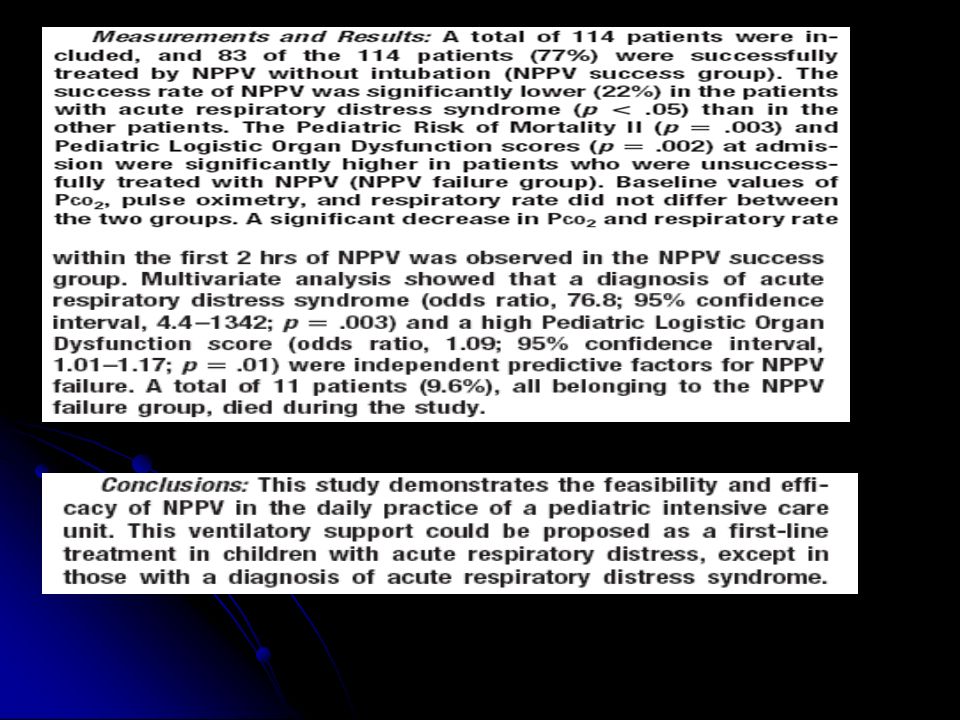
Essouri S, Chevret L, Durand P, et al
Essouri S, Chevret L, Durand P, et al. Noninvasive positive pressure ventilation: five years of experience in a pediatric intensive care unit. Pediatr Crit Care Med 2006;7: A larger study of NIPPV in PICUs found that acute respiratory distress syndrome and a high pediatric logistic organ dysfunction (PELOD) score were independent predictive variables of NIPPV failure – This study noted that there was improvement in breathing pattern and in gas exchange in some patients on NIPPV in the first few hours. Most of the patients who failed did so within the first 48 hours. These findings support the need for close monitoring of patients on NIPPV and the need to consider discontinuation if improvement is not noted in the short term.
 score were independent predictive variables of NIPPV failure – This study noted that there was improvement in breathing pattern and in gas exchange in some patients on NIPPV in the first few hours. Most of the patients who failed did so within the first 48 hours. These. findings support the need for close monitoring of patients on NIPPV and the need to consider discontinuation if improvement is not noted in the short term.")
47
ERITEMA O ULCERACION DE LA BASE DE LA NARIZ
COMPLICACIONES DISCONFORT CLAUSTROFOBIA ERITEMA O ULCERACION DE LA BASE DE LA NARIZ IRRITACIONES O ULCERAS DE PIEL EPISTAXIS NECROSIS FACIAL DOLOR DE OIDO O CAVIDADES SINUSALES

48
DISTENSION ABDOMINA L CON INSUFLACION GASTRICA ( RARO) VOMITOS
CONJUNTIVITIS IRRITATIVA SINUSITIS DISTENSION ABDOMINA L CON INSUFLACION GASTRICA ( RARO) VOMITOS REMOCION INADVERTIDA DE MASCARA HIPERINSUFLACION PULMONAR RESECAMIENTO ORAL RESECAMIENTO NASAL
 VOMITOS. REMOCION INADVERTIDA DE MASCARA. HIPERINSUFLACION PULMONAR. RESECAMIENTO ORAL. RESECAMIENTO NASAL.")
51
Supervisar y mantener el correcto funcionamiento del ventilador
CUIDADOS DE ENFERMERIA Asegurar permeabilidad de las vias aereas aspirando y humidificando las secreciones Supervisar y mantener el correcto funcionamiento del ventilador Ajustar frecuentemente la mascarilla para evitar fugas excesivas Controlar las zonas de roce y de presión para evitar aparición de úlceras Controlar el efecto sobre los ojos de las fugas de la interfase y prevenir la aparición de conjuntivitis

52
ÉXITO : TRABAJO EN EQUIPO

55
NON INVASIVE VENTILATION IN A PEDIATRIC INTENSIVE CARE UNIT
Pedro NUNES et al, Ventilação não invasiva numa unidade de cuidados intensivos pediátricos, Acta Med Port. 2010; 23(3): Objectivo: Determinar a eficácia da VNI em crianças com insuficiência respiratória aguda ou crónica agudizada Métodos: Estudo prospectivo de todas as crianças submetidas a VNI (Novembro 2005 a Abril 2008). Foram analisados dados demográficos e avaliados os seguintes parâmetros: frequência respiratória, frequência cardíaca, SatO2 e gasimetrias capilares antes e 1, 2, 6, 12 e 24 horas após o inicio de VNI
: Objectivo: Determinar a eficácia da VNI em crianças com insuficiência respiratória aguda ou crónica agudizada. Métodos: Estudo prospectivo de todas as crianças submetidas a VNI (Novembro 2005 a Abril 2008). Foram analisados dados demográficos e avaliados os seguintes parâmetros: frequência respiratória, frequência cardíaca, SatO2 e gasimetrias capilares antes e 1, 2, 6, 12 e 24 horas após o inicio de VNI.")
56
Resultados: Incluídos 113 doentes (116 episódios VNI)
Resultados: Incluídos 113 doentes (116 episódios VNI). Idade média 9,4 ± 26,2 meses (mediana: 1,5 meses). CPAP usado em 63 e BiPAP em 53 episódios. Diagnóstico principal: bronquiolite em 61 (52,6%), pneumonia em 36 (31,0%). Indicações para VNI: insuficiência respiratória aguda hipoxémica e/ou hipercapnica em 109 (94%), ocorrência de apneia (13), agudização de doença pulmonar crónica (três), obstrução parcial via aérea superior (quatro). Verificou-se melhoria significativa nas frequências respiratória e cardíaca, pH e pCO2 às 1,2,4, 6, 12, 24 e 48h horas após início VNI (p < 0,05) (tabela). Duração média de VNI 47,7 ± 35,6 horas. Sedação com hidrato de cloral necessária em 58 (50,0%). Vinte e oito (24,1%) crianças necessitaram de ventilação mecânica convencional (VMC), sendo o principal motivo a presença de apneia com bradicardia (8). Não houve complicações major Relacionadas com a VNI. Conclusões: Nesta amostra, a VNI foi eficaz em lactentes e crianças com insuficiência respiratória aguda, prevenindo alguns doentes de agravamento e/ou de necessitarem de VMC
. Idade média 9,4 ± 26,2 meses (mediana: 1,5 meses). CPAP usado em 63 e BiPAP em 53. episódios. Diagnóstico principal: bronquiolite em 61 (52,6%), pneumonia em. 36 (31,0%). Indicações para VNI: insuficiência respiratória aguda hipoxémica. e/ou hipercapnica em 109 (94%), ocorrência de apneia (13), agudização de. doença pulmonar crónica (três), obstrução parcial via aérea superior (quatro). Verificou-se melhoria significativa nas frequências respiratória e cardíaca, pH e pCO2 às 1,2,4, 6, 12, 24 e 48h horas após início VNI (p < 0,05) (tabela). Duração média de VNI 47,7 ± 35,6 horas. Sedação com hidrato de cloral. necessária em 58 (50,0%). Vinte e oito (24,1%) crianças necessitaram de. ventilação mecânica convencional (VMC), sendo o principal motivo a. presença de apneia com bradicardia (8). Não houve complicações major. Relacionadas com a VNI. Conclusões: Nesta amostra, a VNI foi eficaz em lactentes e crianças com insuficiência respiratória aguda, prevenindo alguns doentes de agravamento e/ou de necessitarem de VMC.")
57
Ventilación no invasiva en cuidado Intensivo
Pediátrico, cuatro años de experiencia Arch Argent Pediatr 2011;109(2): Objetivo. Describir la experiencia en la aplicación de VNI en una unidad de cuidados intensivos pediátricos y analizar las características asociadas al éxito del procedimiento. Población y método. Se revisaron las historias clínicas de pacientes que ingresaron a VNI entre 2006 y Se establecieron 3 grupos, según el contexto clínico de aplicación: VNI electiva (1); VNI de rescate (2); VNI preventiva (3). Para cada grupo se recolectaron edad, gravedad (puntaje PIM 2), días de VNI y evolución. Se consideró fracaso de VNI a la necesidad de intubación (grupo 1) o de reintubación (grupo 2 y 3) en las 72 h posteriores a la aplicación de VNI
: Objetivo. Describir la experiencia en la aplicación de VNI en una unidad de cuidados intensivos pediátricos y analizar las características asociadas al éxito del procedimiento. Población y método. Se revisaron las historias clínicas de pacientes que ingresaron a VNI entre 2006 y Se establecieron 3 grupos, según el contexto clínico de aplicación: VNI electiva (1); VNI de rescate (2); VNI preventiva (3). Para cada grupo se recolectaron edad, gravedad (puntaje PIM 2), días de VNI y evolución. Se consideró fracaso de VNI a la necesidad de intubación (grupo 1) o de reintubación (grupo 2 y 3) en las 72 h posteriores a la aplicación de VNI.")
58
Resultados . Ingresaron a VNI 313 niños en quienes se utilizó VNI en 332 ocasiones: 154 correspondieron al grupo electivo, 60 al de rescate y 118 al preventivo; la tasa de éxitos fue del 52%, 63% y 77% respectivamente; en el grupo 1 el éxito se asoció a menor gravedad de los niños y en todos los casos los pacientes que fracasaron tuvieron mayor tiempo de internación y peor evolución. Conclusión. La VNI evitó el ingreso a ventilación mecánica invasiva en un alto porcentaje de niños. Su uso preventivo requiere aún estudios para definir las indicaciones de su aplicación

Presentaciones similares




























 : INTERFASES>")



