Descargar la presentación
La descarga está en progreso. Por favor, espere

1
PREVALENCIA Y CAUSALIDAD
Prevalencia en a. (criterios JNC VI) 50% estadío 1 ( /90-99 mmHg) 18% estadío 2 ( / mmHg) 6,5% estadío 3 (> 180/110 mmHg) 57-66% de los casos de HTA entre años es HSA (>160/>95 mmHg) La HTA es el principal factor de riesgo de morbimortalidad cardiovascular en ancianos Rigaud y Forette, J Gerontol Med Sci 2001
 50% estadío 1 ( /90-99 mmHg) 18% estadío 2 ( / mmHg) 6,5% estadío 3 (> 180/110 mmHg) 57-66% de los casos de HTA entre años es HSA (>160/>95 mmHg) La HTA es el principal factor de riesgo de morbimortalidad cardiovascular en ancianos. Rigaud y Forette, J Gerontol Med Sci")
2
Muestreo aleatorio (400puntos en España)
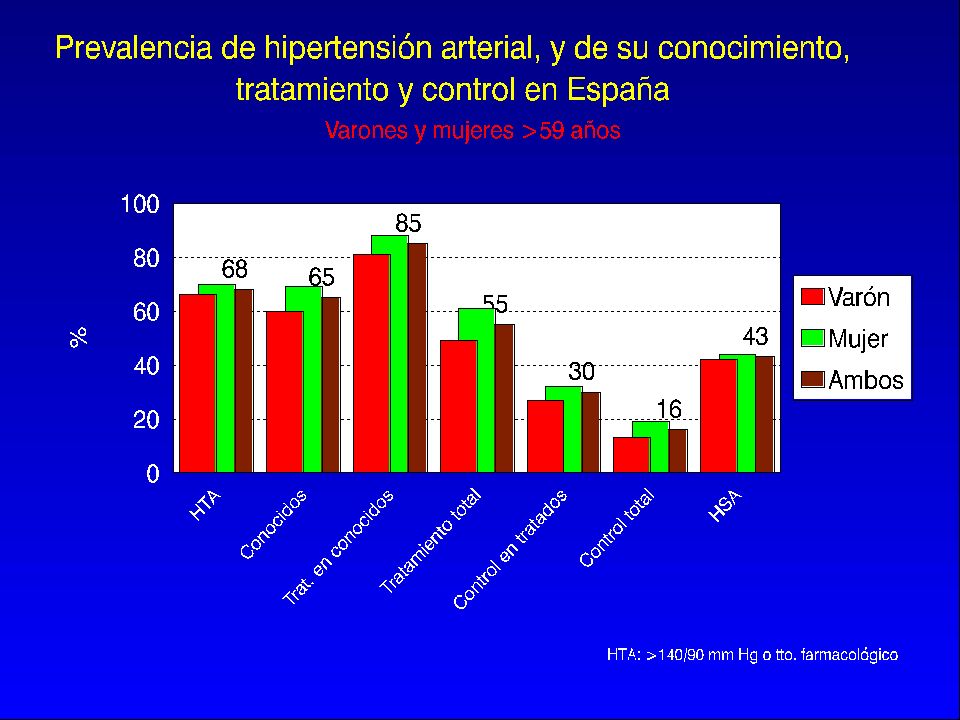
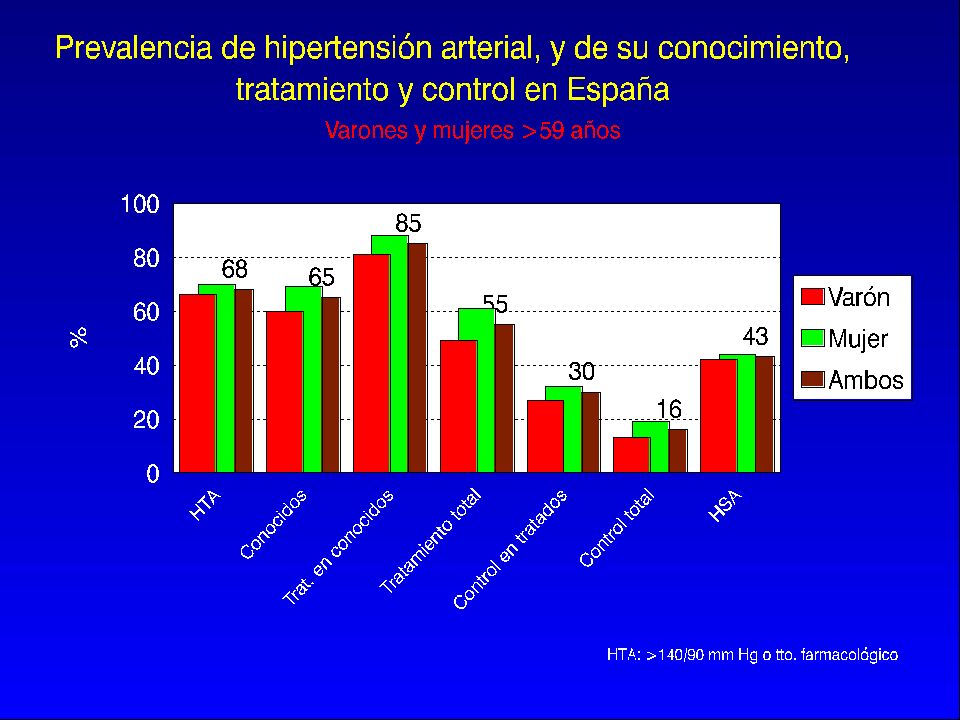
Epidemiología de la HTA en personas mayores de 60 años en España (HORA-España, 2001) Sujetos de estudio: 60 y más años Muestreo aleatorio (400puntos en España) Respuesta (76%) Tamaño (4100) JR Banegas, FR Artalejo, A Graciani, JJ Cruz, E López, L Díez, P Guallar, JLG Fisac, R Herruzo, J Rey-Calero Dpto. de Medicina Preventiva y Salud Pública (UAM)
 Sujetos de estudio: 60 y más años. Muestreo aleatorio (400puntos en España) Respuesta (76%) Tamaño (4100) JR Banegas, FR Artalejo, A Graciani, JJ Cruz, E López, L Díez, P Guallar, JLG Fisac, R Herruzo, J Rey-Calero. Dpto. de Medicina Preventiva y Salud Pública (UAM)")
4
Presión Arterial (mmHg)
por sexo y edad PAS PAD PP Total 143, , ,0 Varones 142, , ,3 60-69 años 140, , ,5 , , ,5 80 y más 146, , ,6 Mujeres 143, , ,6 60-69 años 140, , ,2 , , ,2 80 y más 145, , ,0 Medias de todas las mediciones disponibles (1-12).
.")
5
Condiciones HTA grado 1 HTA grado 2 HTA grado 3
Modificadoras PAS PAS PAS ≥ 180 ó PAD ó PAD ó PAD ≥ 110 I. Ausencia de otros Factores de riesgo (FR) II. Uno o dos FR III. Tres o más FR o LOD o diabetes IV. TCA BAJO MEDIO ALTO MEDIO MEDIO MUY ALTO ALTO ALTO MUY ALTO MUY ALTO MUY ALTO MUY ALTO OMS/ISH, 1999
 II. Uno o dos FR. III. Tres o más FR o. LOD o diabetes. IV. TCA. BAJO MEDIO ALTO. MEDIO MEDIO MUY ALTO. ALTO ALTO MUY ALTO. MUY ALTO MUY ALTO MUY ALTO. OMS/ISH,")
6
TASA DE EVENTOS CV (10 años)
Varones 8% % Mujeres 4% % Vasan y cols., N Engl J Med 2001

7
HTA EN EL ANCIANO “El incremento de la PA no es un fenómeno adaptativo
HTA EN EL ANCIANO “El incremento de la PA no es un fenómeno adaptativo. La HTA del anciano es un factor de riesgo CV mayor”

8
¿SISTÓLICA? ¿DIASTÓLICA?
Franklin y cols., Circulation 2001

9
¿Presión Sistólica, Diastólica o del Pulso?
1) A igualdad de PAD, el riesgo aumentaba con cada elevación de la PAS Circulation 1999; 100: 2) Cuando se consideró la PAS para estadiar a los pacientes, este criterio aislado clasificó correctamente al 91% de los sujetos, hecho que sucedió solo en el 22% de los casos en que se utilizó la PAD Hypertension 1999; 34: 3) “El paradigma se ha modificado hacia la Presión Arterial Sistólica” HR Black. Editorial de Hypertension 1999, vol. 34.
 A igualdad de PAD, el riesgo aumentaba con cada elevación de la PAS. Circulation 1999; 100: ) Cuando se consideró la PAS para estadiar a los pacientes, este criterio. aislado clasificó correctamente al 91% de los sujetos, hecho que sucedió. solo en el 22% de los casos en que se utilizó la PAD. Hypertension 1999; 34: ) El paradigma se ha modificado hacia la Presión Arterial Sistólica HR Black. Editorial de Hypertension 1999, vol. 34.")
10
ONDA DE PULSO, PP Y PAM

11
Riesgo cardiovascular según la PP
Estudio de Framingham Riesgo cardiovascular según la PP Franklin y cols. Circulation 1999;100:354

12
CONDICIONES MODIFICADORAS (I)
Factores de riesgo Lesión de órgano diana (FR) (LOD) HTA Varones de edad > 55a Mujeres de edad > 65a Tabaquismo Colesterol total elevado (> 6,5 mmol/l; 250 mg/dl) Diabetes AF de ECV prematura Hipertrofia ventrículo izqdo. (ECG, Eco o RX) Proteinuria y/o aumento leve de Cr. en plasma (1,2-2 mg/dl) Signos Eco o Rx de placa ate- rosclerótica (carótidas, aorta, femorales, ilíacas) Estenosis focal o generalizada de arterias retinianas
 (LOD) HTA. Varones de edad > 55a. Mujeres de edad > 65a. Tabaquismo. Colesterol total elevado. (> 6,5 mmol/l; 250 mg/dl) Diabetes. AF de ECV prematura. Hipertrofia ventrículo izqdo. (ECG, Eco o RX) Proteinuria y/o aumento leve. de Cr. en plasma (1,2-2 mg/dl) Signos Eco o Rx de placa ate- rosclerótica (carótidas, aorta, femorales, ilíacas) Estenosis focal o generalizada. de arterias retinianas.")
13
Trastornos Clínicos Asociados
CONDICIONES MODIFICADORAS (II) Trastornos Clínicos Asociados (TCA) ECV (ACVA, AIT) Cardiopatía (IAM, angor, revasc. coronaria, ICC) Enfermedad renal (nefropatía diabética) Insuficiencia Renal (Cr. en plasma > 2 mg/dl) Enfermedad Vascular (Aneurisma disecante, arteriopatía sintomática) Retinopatía hipertensiva avanzada (hemorragias, exudados o edema de papila)
 Trastornos Clínicos Asociados. (TCA) ECV (ACVA, AIT) Cardiopatía (IAM, angor, revasc. coronaria, ICC) Enfermedad renal (nefropatía diabética) Insuficiencia Renal (Cr. en plasma > 2 mg/dl) Enfermedad Vascular (Aneurisma disecante, arteriopatía sintomática) Retinopatía hipertensiva avanzada (hemorragias, exudados o edema de papila)")
14
Condiciones HTA grado 1 HTA grado 2 HTA grado 3
Modificadoras PAS PAS PAS ≥ 180 ó PAD ó PAD ó PAD ≥ 110 I. Ausencia de otros Factores de riesgo (FR) II. Uno o dos FR III. Tres o más FR o LOD o diabetes IV. TCA BAJO MEDIO ALTO MEDIO MEDIO MUY ALTO ALTO ALTO MUY ALTO MUY ALTO MUY ALTO MUY ALTO OMS/ISH, 1999
 II. Uno o dos FR. III. Tres o más FR o. LOD o diabetes. IV. TCA. BAJO MEDIO ALTO. MEDIO MEDIO MUY ALTO. ALTO ALTO MUY ALTO. MUY ALTO MUY ALTO MUY ALTO. OMS/ISH,")
15
Conforme la expectativa de vida se aproxima a los límites
biológicos de la longevidad, es el momento de reconocer que el objetivo primordial del cuidado médico es mejorar la función del paciente y reducir el grado de enfermedad. L.E. Cluff Chronic disease, function and quality of care J Chronic Dis 1981; 34:

16
OBJETIVOS DEL TRATAMIENTO DE LA HTA EN EL ANCIANO
Disminuir la mortalidad total y/o cardiovascular Disminuir la morbilidad cardiovascular Disminuir deterioro funcional, cognitivo o de la calidad de vida

18
BENEFICIOS DEL TRATAMIENTO DE LA HTA SISTÓLICA AISLADA EN ANCIANOS
AVC Eventos coronarios Mortalidad total Mortalidad CV Eventos CV 40 30 20 10 13 (P =0.02) Reducción eventos (%) 18 (P =0.01) 23 (P =0.001) A meta-analysis of eight trials involving older patients with ISH found active treatment reduced total mortality by 13%, cardiovascular mortality by 18%, all CVD complications by 26%, stroke by 30%, and coronary events by 23% A quantitative overview of eight trials sought to evaluate the risks associated with SBP in treated and untreated older patients with ISH. A total of 15,693 patients >60 years old with SBP >160 mm Hg and a DBP <95 mm Hg were followed for 3.8 years (median). After correction for regression dilution bias, sex, age, and DBP, the relative hazards rates associated with a 10 mm Hg higher initial SBP were significantly associated with total mortality (P =0.02) and stroke (P =0.0001). Active treatment reduced total mortality by 13%, cardiovascular mortality by 18%, all CVD complications by 26%, stroke by 30% and coronary events by 23%. In contrast to SBP, DBP was found to be inversely correlated with total mortality, further supporting the role of pulse pressure as a powerful risk factor. Staessen JA, et al. Risks of untreated and treated isolated systolic hypertension in the elderly: meta-analysis of outcome trials. Lancet. 2000;355: 26 (P <0.0001) 30 (P <0.0001) Meta-analysis of clinical trials (N=15,693) in ISH (SHEP/Syst-EUR/Syst-China/EWPHE/HEP/STOP/MRC1/MRC2). Staessen JA et al. Lancet. 2000;355:
 Reducción eventos (%) 18. (P =0.01) 23. (P =0.001) A meta-analysis of eight trials involving older patients with ISH found active treatment reduced total mortality by 13%, cardiovascular mortality by 18%, all CVD complications by 26%, stroke by 30%, and coronary events by 23% A quantitative overview of eight trials sought to evaluate the risks associated with SBP in treated and untreated older patients with ISH. A total of 15,693 patients >60 years old with SBP >160 mm Hg and a DBP <95 mm Hg were followed for 3.8 years (median). After correction for regression dilution bias, sex, age, and DBP, the relative hazards rates associated with a 10 mm Hg higher initial SBP were significantly associated with total mortality (P =0.02) and stroke (P =0.0001). Active treatment reduced total mortality by 13%, cardiovascular mortality by 18%, all CVD complications by 26%, stroke by 30% and coronary events by 23%. In contrast to SBP, DBP was found to be inversely correlated with total mortality, further supporting the role of pulse pressure as a powerful risk factor. Staessen JA, et al. Risks of untreated and treated isolated systolic hypertension in the elderly: meta-analysis of outcome trials. Lancet. 2000;355: (P <0.0001) 30. (P <0.0001) Meta-analysis of clinical trials (N=15,693) in ISH (SHEP/Syst-EUR/Syst-China/EWPHE/HEP/STOP/MRC1/MRC2). Staessen JA et al. Lancet. 2000;355:")
19
BENEFICIOS DEL TRATAMIENTO DE LA HTA
Estudio NNT* MRC / 1 año MRC-II / 5,8 años SHEP / 4,5 años STOP / 4 años Syst-Eur / 2 años (*) NNT: Nº de pacientes a tratar para evitar 1 AVCA
 NNT: Nº de pacientes a tratar para evitar 1 AVCA.")
20
OBJETIVOS DEL TRATAMIENTO DE LA HTA EN EL ANCIANO
Disminuir la mortalidad total y/o cardiovascular Disminuir la morbilidad cardiovascular Disminuir deterioro funcional, cognitivo o de la calidad de vida

21
ESTUDIOS DE INTERVENCION RESULTADOS FUNCIONALES
H E P M R C P P C E W P H E S T O P S Y S T - E U R A B V D ? ? ? ? ? ? A I V D ? ? ? ? ? ? C O G N I H U M R = ? ? ? ? M e j o r í a * C A L I D E V ? ? ? ? ? ? * Forette F et al., Lancet 1998; 352:

22
TRATAMIENTO FARMACOLOGICO
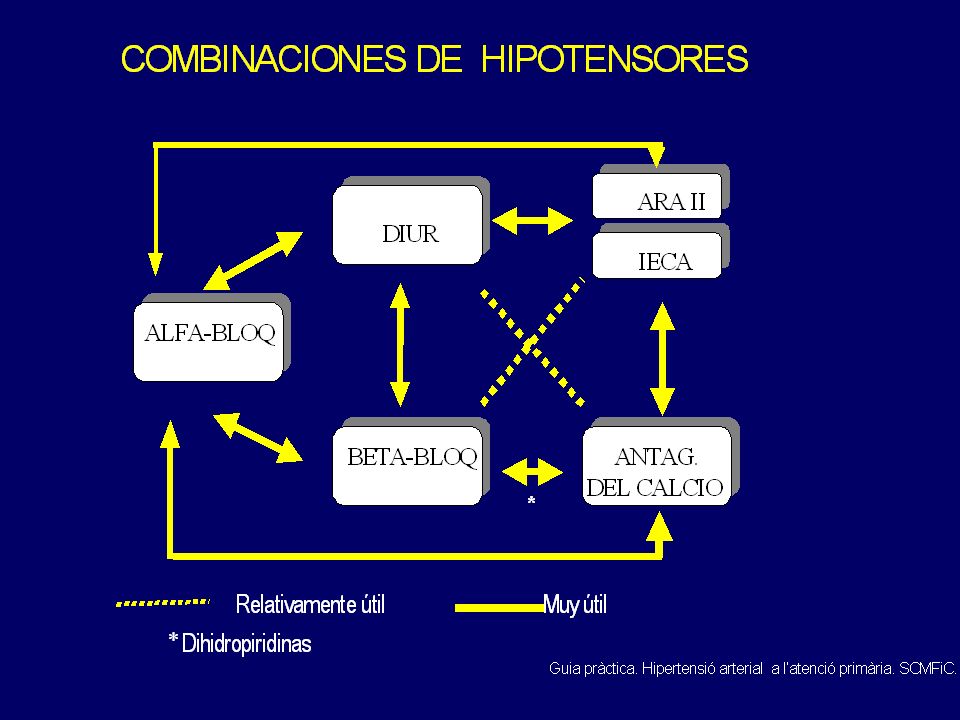
Como terapéutica inicial debe elegirse un diurético y/o un -bloqueante, a menos que existan indicaciones específicas para otro fármaco. En personas ancianas, los diuréticos son de elección y puede considerarse el uso de los calcio-antagonistas dihidropiridínicos de duración larga. Sexto informe del JNC. Arch Intern Med, 1997

23
D I U R E T I C O S B E T A B L O Q . A C V , 6 1 ( , 5 1 - , 7 2 ) ,
, 6 1 ( , 5 1 - , 7 2 ) , 7 4 ( , 5 7 - , 9 8 ) M o r t . A C V I s q a d i v c l , 6 7 ( , 4 9 - , 9 ) , 7 6 ( , 4 8 - 1 , 2 2 ) , 7 4 ( , 6 4 - , 8 5 ) 1 , 1 ( , 8 - 1 , 2 9 ) , 7 5 ( , 6 4 - , 8 7 ) , 9 8 ( , 7 8 - 1 , 2 3 ) , 8 6 ( , 7 7 - , 9 6 ) 1 , 5 ( , 8 8 - 1 , 2 5 ) Messerli FH et al., JAMA 1998; 279:
 , ( , , ) M. o. r. t. . A. C. V. I. s. q. a. d. i. v. c. l. , ( , , 9. ) , ( , , ) , ( , , ) 1. , 1. ( , , ) , ( , , ) , ( , , ) , ( , , ) 1. , 5. ( , , ) Messerli FH et al., JAMA 1998; 279:")
24
Tratamiento con clortalidona (bajas dosis)
Estudio SHEP Tratamiento con clortalidona (bajas dosis) Riesgo Relativo respecto a placebo DIABETICOS NO DIABETICOS Eventos CV mayores 0, ,66 Ictus ,78 0,62 IAM y C. Isq. 0,46 0,77 C. isq. Mayor 0,44 0,81 Mortalidad Total 0,74 0,85 Curb y cols., JAMA 1996
 Riesgo Relativo respecto a placebo. DIABETICOS NO DIABETICOS. Eventos CV mayores 0,66 0,66. Ictus 0,78 0,62. IAM y C. Isq. 0,46 0,77. C. isq. Mayor 0,44 0,81. Mortalidad. Total 0,74 0,85. Curb y cols., JAMA")
25
EFICACIA DEL TRATAMIENTO EN ANCIANOS DIABÉTICOS
Estudio SYST-EUR EFICACIA DEL TRATAMIENTO EN ANCIANOS DIABÉTICOS The New England Journal of Medicine; 1999: Vol. 340:

26
Efecto de tratamientos sobre la Presión del Pulso
Estudio de la Administración de Veteranos Cushman y cols., Hypertension 2001

27
Efecto de asociaciones sobre la Presión del Pulso
Estudio de la Administración de Veteranos Cushman y cols., Hypertension 2001

28
El prescriptor prudente que, sobre la base de los resultados
de los ensayos del SHEP, el STOP y el MRC hubiera decidido que los diuréticos tiazídicos deben ser el tratamiento de primera línea para los ancianos hipertensos, verá reforzada su postura por estos resultados del STOP-2. Kendall MJ. Editorial del Lancet que comenta el STOP-2 (1999)
")
29
Variable Primaria Tiempo hasta duplicación de creatinina sérica,
enfermedad renal terminal o muerte Variable Primaria Neil A, Hawkins M, Potok M, et al. A prospective population-based study of microalbuminaria as a predictor of mortality in NIDDM. Diabet Care 1993;16: Nielsen FS, Rossing P, Gall M-A, et al. Long-term effect of lisinopril and atenolol on kidney function in hypertensive NIDDM subjects with diabetic nephropathy. Diabetes 1997;46: O'Donnell MP, Crary GS, Oda H, Kasiske BL, Powell JR, Keane WF. Irbesartan lowers blood pressure and ameliorates renal injury in experimental non-insulin-dependent diabetes mellitus. Kidney Int 1997;52(suppl 63):S218-S220. Parving H-H, Smidt UM, Hommel E, et al. Effective antihypertensive treatment postpones renal insufficiency in diabetic nephropathy. Am J Kid Dis 1993;22: Parving H-H, Tarnow L, Rossing P. Renal protection in diabetes: An emerging role for calcium antagonists. J Hypertens 1996;14(suppl 4):S21-S25. Perico N, Remuzzi A, Sangalli F, et al. The antiproteinuric effect of angiotensin antagonism in human IgA nephropathy is potentiated by indomethacin. J Am Soc Nephrol 1998;9: Pohl M, Cooper M, Ulrey J, Pauls J, Rohde R. Safety and efficacy of irbesartan in hypertensive patients with type II diabetes and proteinuria. Am J Hypertens 1997;10:105A. Abstract. Pugh JA, Medina R, Ramirez, M. Comparison of the course to end-stage renal disease of type 1 (insulin-dependent) and type 2 (non-insulin-dependent) diabetic nephropathy. Diabetologia 1993;36: Pylypchuk GB. ACE inhibitor- versus angiotensin II blocker-induced cough and angioedema. Ann Pharmacother 1998;32: Ravid M, Savin H, Jutrin I, et al. Long-term stabilizing effect of angiotensin-converting enzyme inhibition on plasma creatinine and on proteinuria in normotensive type II diabetic patients. Ann Intern Med 1993;118: Ravid M, Savin H, Lang R, Jutrin I, Shoshana L, Lishner M. Proteinuria, renal impairment, metabolic control, and blood pressure in type 2 diabetes mellitus. Arch Intern Med 1992;152: Reeves RA, Lin C-S, Kassler-Taub K, Pouleur H. Dose-related efficacy of irbesartan for hypertension: an integrated analysis. Hypertension 1998;31: Rodby RA, Rohde RD, Clarke WR, et al. The irbesartan type II diabetic nephropathy trial: study design and baseline patient characteristics. Nephrol Dial, in press. Rossing P, Hommel E, Smidt UM, et al. Reduction in albuminuria predicts diminished progresion in diabetic nephropathy. Kidney Int 1994;45(suppl.):S145-S149. SHEP Cooperative Research Group. Prevention of stroke by antihypertensive drug treatment in older persons with isolated systolic hypertension: final results of the systolic hypertension in the elderly program (SHEP). JAMA 1991;265: Sica DA, Marino MR, Hammett JL, Ferreira I, Gehr TWB, Ford NF. The pharmacokinetics of irbesartan in renal failure and maintenance hemodialysis. Clin Pharmacol Ther 1997;62: Simon TA, Gelarden T, Freitag SA, Kassler-Taub KB, Davies R. Safety of irbesartan in the treatment of mild to moderate systemic hypertension. Am J Cardiol 1998;82: Staessen JA, Fagard R, Thijs L, et al. Randomized double-blind comparison of placebo and active treatment for older patients with isolated systolic hypertension. Lancet 1997;350: Stamler J, Vaccaro O, Neaton JD, et al. Diabetes, other risk factors, and 12-yr cardiovascular mortality for men screened in multiple risk factor intervention trial. Diabetes Care 1993;16: Stone PH, Muller JE, Hartwell T, et al. The effect of diabetes mellitus on pronosis and serial left ventricular function after acute myocardial infarction: contribution of both coronary disease and diastolic left ventricular dysfunction to the adverse prognosis. The MILIS Study Group. J Am Cardiol 1989;14:49-57. Tarnow L, Rossing P, Gall M-A, et al. Prevalence of arterial hypertension in diabetic patients before and after the JNC-V. Diabet Care 1994;17: Tatti P, Pahor M, Byington RP, et al. Outcome results of the fosinopril versus amlodipine cardiovascular events randomized trial (FACET) in patients with hypertension and NIDDM. Diabetes Care 1998;21: Tuomilehto J, Rastenyte D, Birkenhäger WH, et al. Effects of calcium-channel blockade in older patients with diabetes and systolic hypertension. N Engl J Med 1999;340: RRR=Reducción del Riesgo Relativo Irbesartán Amlodipino 60 RRR 23% P=0.006 RRR 20% P=0.024 Placebo Amlodipino 50 RRR -4% P=NS Sujetos que alcanzan la variable primaria (%) Placebo 40 Irbesartán 30 20 10 6 12 18 24 30 36 42 48 Seguimiento (meses) NEJM 2001;345:851-60
:S218-S220. Parving H-H, Smidt UM, Hommel E, et al. Effective antihypertensive treatment postpones renal insufficiency in diabetic nephropathy. Am J Kid Dis 1993;22: Parving H-H, Tarnow L, Rossing P. Renal protection in diabetes: An emerging role for calcium antagonists. J Hypertens 1996;14(suppl 4):S21-S25. Perico N, Remuzzi A, Sangalli F, et al. The antiproteinuric effect of angiotensin antagonism in human IgA nephropathy is potentiated by indomethacin. J Am Soc Nephrol 1998;9: Pohl M, Cooper M, Ulrey J, Pauls J, Rohde R. Safety and efficacy of irbesartan in hypertensive patients with type II diabetes and proteinuria. Am J Hypertens 1997;10:105A. Abstract. Pugh JA, Medina R, Ramirez, M. Comparison of the course to end-stage renal disease of type 1 (insulin-dependent) and type 2 (non-insulin-dependent) diabetic nephropathy. Diabetologia 1993;36: Pylypchuk GB. ACE inhibitor- versus angiotensin II blocker-induced cough and angioedema. Ann Pharmacother 1998;32: Ravid M, Savin H, Jutrin I, et al. Long-term stabilizing effect of angiotensin-converting enzyme inhibition on plasma creatinine and on proteinuria in normotensive type II diabetic patients. Ann Intern Med 1993;118: Ravid M, Savin H, Lang R, Jutrin I, Shoshana L, Lishner M. Proteinuria, renal impairment, metabolic control, and blood pressure in type 2 diabetes mellitus. Arch Intern Med 1992;152: Reeves RA, Lin C-S, Kassler-Taub K, Pouleur H. Dose-related efficacy of irbesartan for hypertension: an integrated analysis. Hypertension 1998;31: Rodby RA, Rohde RD, Clarke WR, et al. The irbesartan type II diabetic nephropathy trial: study design and baseline patient characteristics. Nephrol Dial, in press. Rossing P, Hommel E, Smidt UM, et al. Reduction in albuminuria predicts diminished progresion in diabetic nephropathy. Kidney Int 1994;45(suppl.):S145-S149. SHEP Cooperative Research Group. Prevention of stroke by antihypertensive drug treatment in older persons with isolated systolic hypertension: final results of the systolic hypertension in the elderly program (SHEP). JAMA 1991;265: Sica DA, Marino MR, Hammett JL, Ferreira I, Gehr TWB, Ford NF. The pharmacokinetics of irbesartan in renal failure and maintenance hemodialysis. Clin Pharmacol Ther 1997;62: Simon TA, Gelarden T, Freitag SA, Kassler-Taub KB, Davies R. Safety of irbesartan in the treatment of mild to moderate systemic hypertension. Am J Cardiol 1998;82: Staessen JA, Fagard R, Thijs L, et al. Randomized double-blind comparison of placebo and active treatment for older patients with isolated systolic hypertension. Lancet 1997;350: Stamler J, Vaccaro O, Neaton JD, et al. Diabetes, other risk factors, and 12-yr cardiovascular mortality for men screened in multiple risk factor intervention trial. Diabetes Care 1993;16: Stone PH, Muller JE, Hartwell T, et al. The effect of diabetes mellitus on pronosis and serial left ventricular function after acute myocardial infarction: contribution of both coronary disease and diastolic left ventricular dysfunction to the adverse prognosis. The MILIS Study Group. J Am Cardiol 1989;14: Tarnow L, Rossing P, Gall M-A, et al. Prevalence of arterial hypertension in diabetic patients before and after the JNC-V. Diabet Care 1994;17: Tatti P, Pahor M, Byington RP, et al. Outcome results of the fosinopril versus amlodipine cardiovascular events randomized trial (FACET) in patients with hypertension and NIDDM. Diabetes Care 1998;21: Tuomilehto J, Rastenyte D, Birkenhäger WH, et al. Effects of calcium-channel blockade in older patients with diabetes and systolic hypertension. N Engl J Med 1999;340: RRR=Reducción del Riesgo Relativo. Irbesartán. Amlodipino. 60. RRR 23% P= RRR 20% P= Placebo. Amlodipino. 50. RRR -4% P=NS. Sujetos que alcanzan la variable primaria. (%) Placebo. 40. Irbesartán Seguimiento (meses) NEJM 2001;345:")
30
ESTUDIO PROGRESS Lancet, 2001

31
¿SE TRATA LA HTA EN MAYORES DE 80?
Meta-análisis Gueyffier y cols.. Lancet 1999; 353: Efecto sobre morbilidad: Disminuye ACVA en un 36% Disminuye eventos cardiovasculares mayores en un 23% Disminuye ICC en un 42% Efecto sobre mortalidad: Aumenta la mortalidad total en un 14% (p=0,05) 1) La supervivencia debe ajustarse por la calidad de vida. 2) Estos hallazgos no sugieren la existencia de un umbral de edad por encima del cual la HTA no debiera ser tratada.
 1) La supervivencia debe ajustarse por la calidad de vida. 2) Estos hallazgos no sugieren la existencia de un umbral de edad. por encima del cual la HTA no debiera ser tratada.")
32
HIPOTENSORES EN EL ANCIANO
DIURÉTICOS (si no hay contraindicaciones o indicaciones específicas del resto de grupos) BETA-BLOQUEADORES (Cardiopatía isquémica) CALCIOANTAGONISTAS (HTA sistólica) I-ECA/ARA.II (Insuf.Cardiaca, Nefropatía diabética)
 BETA-BLOQUEADORES (Cardiopatía isquémica) CALCIOANTAGONISTAS (HTA sistólica) I-ECA/ARA.II (Insuf.Cardiaca, Nefropatía diabética)")
33
La menor incidencia de eventos cardiovasculares mayores
ocurrieron cuando se alcanzó una PAD de 82,6 mmHg. (Estudio HOT, Lancet 1998; 351: ). El estudio HOT aporta una poderosa evidencia sobre el efecto beneficioso de la terapia intensiva antihipertensiva, con una máxima protección conseguida alrededor de 140/85 mmHg. (Kaplan N, Lancet 1998; 351: ). El regimen de diurético o diurético+betabloqueante produjo la media más baja de presiones (140,6/82,3mmHg). (Perry HM et al, Hypertension 1998; 31: ).
. El estudio HOT aporta una poderosa evidencia sobre el efecto. beneficioso de la terapia intensiva antihipertensiva, con una. máxima protección conseguida alrededor de 140/85 mmHg. (Kaplan N, Lancet 1998; 351: ). El regimen de diurético o diurético+betabloqueante produjo. la media más baja de presiones (140,6/82,3mmHg). (Perry HM et al, Hypertension 1998; 31: ).")
34
“.......¡no reducir la PAD < 65 mmHg!”
Y en ancianos con HTA sistólica “ ¡no reducir la PAD < 65 mmHg!” Staessen J.Lancet 2000;355;865 Vokó Z. Hypertension 1999;34:1181 Somes G, Arch Intern Med 1999;159:2004 Kaplan NM. Arch Intern Med 2001;161:1480

35
DISTRIBUCION DE LA POBLACIÓN HIPERTENSA EN EEUU DE AMÉRICA
50 100 150 200 250 PAS (mm Hg) 140 More than twice as many hypertensives in the United States are above the treatment goal of SBP 140 mm Hg than the goal of DBP 90 mm Hg [1] Patients with systolic hypertension are less likely to be aware of their condition and more likely to be treatment failures [1] The maxim that DBP is the primary predicator of cardiovascular disease (CVD) has been revised in the face of substantial evidence strongly indicating that SBP and pulse pressure (PP) are more potent predictors of CVD risk [2-6]. To identify the prevalence and characteristics of hypertension subtypes in the United States, and to determine where treatment and control efforts are most needed, the National Health and Nutrition Examination Survey III (NHANES III) hypertensive population data was distributed by systolic and diastolic hypertension. From this extrapolated NHANES III data, 42.7 million adults (mean age 43.3 years) were identified as hypertensive, representing 24% of the adjusted adult U.S. population. More than twice as many hypertensives (over 28 million, 66%, represented in upper two quadrants of this slide) are above the SBP goal of 140 mm Hg than the DBP goal of 90 mm Hg (11.4 million, 27%, represented in right hand quadrants of this slide) [1]. Differences were also found in the percentage of subjects who were aware of their disease when patients with systolic and diastolic hypertension were compared. Among untreated hypertensives in the United States, 42% of the population with DBP 90 mm Hg were aware of their condition, but only 29% of patients with SBP 140 mm Hg knew of their hypertensive status. Further, the population with elevated SBP were more likely than those with elevated DBP to be categorized as treatment failures [1]. (CONTINUED ON NEXT SLIDE) 50 100 150 90 PAD (mm Hg) Lapuerta P et al. Am J Hypertens. 1999;12(part2):92A.
 140. More than twice as many hypertensives in the United States are above the treatment goal of SBP 140 mm Hg than the goal of DBP 90 mm Hg [1] Patients with systolic hypertension are less likely to be aware of their condition and more likely to be treatment failures [1] The maxim that DBP is the primary predicator of cardiovascular disease (CVD) has been revised in the face of substantial evidence strongly indicating that SBP and pulse pressure (PP) are more potent predictors of CVD risk [2-6]. To identify the prevalence and characteristics of hypertension subtypes in the United States, and to determine where treatment and control efforts are most needed, the National Health and Nutrition Examination Survey III (NHANES III) hypertensive population data was distributed by systolic and diastolic hypertension. From this extrapolated NHANES III data, 42.7 million adults (mean age 43.3 years) were identified as hypertensive, representing 24% of the adjusted adult U.S. population. More than twice as many hypertensives (over 28 million, 66%, represented in upper two quadrants of this slide) are above the SBP goal of 140 mm Hg than the DBP goal of 90 mm Hg (11.4 million, 27%, represented in right hand quadrants of this slide) [1]. Differences were also found in the percentage of subjects who were aware of their disease when patients with systolic and diastolic hypertension were compared. Among untreated hypertensives in the United States, 42% of the population with DBP 90 mm Hg were aware of their condition, but only 29% of patients with SBP 140 mm Hg knew of their hypertensive status. Further, the population with elevated SBP were more likely than those with elevated DBP to be categorized as treatment failures [1]. (CONTINUED ON NEXT SLIDE) PAD (mm Hg) Lapuerta P et al. Am J Hypertens. 1999;12(part2):92A.")
37
La dificultad para controlar la PAS
Estudio STOP-2 140 95 190 PA (mmHg) 54 meses Hansson et al, Lancet 1999; 354:
 54 meses. Hansson et al, Lancet 1999; 354:")
38
Seguimiento de indicación higiénico-dietética y fármacos (%) en Hipertensos Conocidos
Sujetos de 60 y más años

39
PA diastólica PA sistólica 105 100 95 90 185 180 175 170 165 160 155 150 T D < > 65 < > 65 EDAD DEL PACIENTE BMJ, 1995

40
ACTITUD ANTE EL TRATAMIENTO INSTAURADO (No control)
18,8% 1,2% 10,4% 69,6% Mantener tto Disminución dosis Aumento dosis Cambio tto

41
PORCENTAJE DE PACIENTES EN TERAPIA COMBINADA
* * * * * * * Ancianos

43
CONCLUSIONES (I) La identificación y el tratamiento de los pacientes hipertensos sigue siendo la mejor forma comprobada de prevención primaria de la enfermedad cardiovascular, especialmente en los ancianos con HTA sistólica. El tratamiento de la hipertensión en los ancianos produce efectos beneficiosos sobre la morbimortalidad.

44
CONCLUSIONES (II) El efecto del tratamiento de la hipertensión depende de las cifras de PA que se obtengan. El efecto que el tratamiento de la hipertensión produce sobre la función y la calidad de vida es casi desconocido.

Presentaciones similares









 15,000 Mexicanos 43.2% HAS (Salud Publica de México 2010) EUA 1999-2000 29-31% >18 años 58-65.>")









