Descargar la presentación
La descarga está en progreso. Por favor, espere

1
“DISLIPEMIAS: ENFOQUE ACTUAL DE UN FACTOR DE RIESGO CLASICO” Fernando Civeira Murillo Hospital Universitario Miguel Servet Zaragoza “Prevención Cardiovascular y Rehabilitación Cardiaca” CONGRESO SOCIEDAD VASCO-NAVARRA DE CARDIOLOGÍA Vitoria, 25 de noviembre de 2005

2
¿Qué cifra de colesterol es normal?
¿Cuál es el objetivo terapéutico? ¿Qué objetivos se alcanzan en la actualidad? ¿Qué fármacos son de elección?

3
¿Qué cifra de colesterol es normal?
¿Cuál es el objetivo terapéutico? ¿Qué objetivos se alcanzan en la actualidad? ¿Qué fármacos son de elección?

4
¿Qué cifra de colesterol es normal?
“Aquella asociada con menor morbimortalidad y mayor calidad de vida” Directa: Estudios epidemiológicos prospectivos Indirecta Metabolismo celular del colesterol Estudios comparativos entre poblaciones Hipobetalipoproteinemia familiar Comparación entre especies

5
COLESTEROL Y MORTALIDAD ESTUDIOS EPIDEMIOLÓGICOS PROSPECTIVOS
Estudio n Seguimiento Comienzo Framingham 1959/ Johns Kopkinps Chicago HAP Compañías Gas MRFIT

6
MORTALIDAD TOTAL FRAMINGHAM Varones 31-39 años al inicio

7
The Johns Hopkins Precursors Study
Klag MJ, et al. N Engl J Med 1993;328:

8
Multiple Risk Factor Intervention Trial (MRFIT)
Multiple Risk Factor Intervention Trial (MRFIT). Mortalidad tras 16 años de seguimiento de acuerdo a la concentración basal de colesterol ( varones) Stamler J, et al. JAMA 2000;284:
. Mortalidad tras 16 años de seguimiento de acuerdo a la concentración basal de colesterol ( varones) Stamler J, et al. JAMA 2000;284:")
9
¿Qué cifra de colesterol es normal?
En poblaciones occidentales los sujetos con medias de colesterol TOTAL de 150 mg/dl tiene una mayor esperanza de vida a largo plazo La menor mortalidad en MRFIF se asoció a varones con cifras de colesterol TOTAL de 122 mg/dl Respuesta: entre mg/dl

10
¿Qué cifra de colesterol es normal?
¿Cuál es el objetivo terapéutico? ¿Qué objetivos se alcanzan en la actualidad? ¿Qué fármacos son de elección?

11
SIMVASTATINA: EPISODIOS VASCULARES según NIVELES PREVIOS DE LIPIDOS
Baseline ESTATINA PLACEBO Risk ratio and 95% CI feature (10269) (10267) STATIN better STATIN worse LDL (mmol/l) < 3.0 (116 mg/dl) 602 761 c 3.0 < 3.5 483 655 2 Het = 3.0 2 3.5 (135 mg/dl) 957 1190 Total cholesterol (mmol/l) <5.0 (193 mg/dl) 361 476 c 5.0 < 6.0 746 965 Het 2 = 0.5 There were 6973 patients with LDL cholesterol below 3.0 mmol/l (116 mg/dl) at baseline. These results refute entirely the suggestion that there might be a threshold of LDL cholesterol at about this level below which lowering cholesterol does not reduce risk. In these high-risk populations, cholesterol- lowering therapy produced substantial benefits irrespective of the patient's pre- treatment cholesterol level. 2 6.0 (232 mg/dl) 935 1165 ALL PATIENTS 2042 2606 24% SE 2.6 (19.9%) (25.4%) reduction (2P< ) 0.4 0.6 0.8 1.0 1.2 1.4
 (10267) STATIN better. STATIN worse. LDL (mmol/l) < 3.0 (116 mg/dl) c. 3.0 < Het. = (135 mg/dl) Total cholesterol (mmol/l) <5.0 (193 mg/dl) c. 5.0 < Het. 2. = 0.5. There were 6973 patients with LDL cholesterol below 3.0 mmol/l (116 mg/dl) at baseline. These results refute entirely the suggestion that there might be a threshold of LDL cholesterol at about this level below which lowering cholesterol does not reduce risk. In these high-risk populations, cholesterol- lowering therapy produced substantial benefits irrespective of the patient s pre- treatment cholesterol level (232 mg/dl) ALL PATIENTS % SE 2.6. (19.9%) (25.4%) reduction. (2P< )")
13
95 mg/dl 62 mg/dl

15
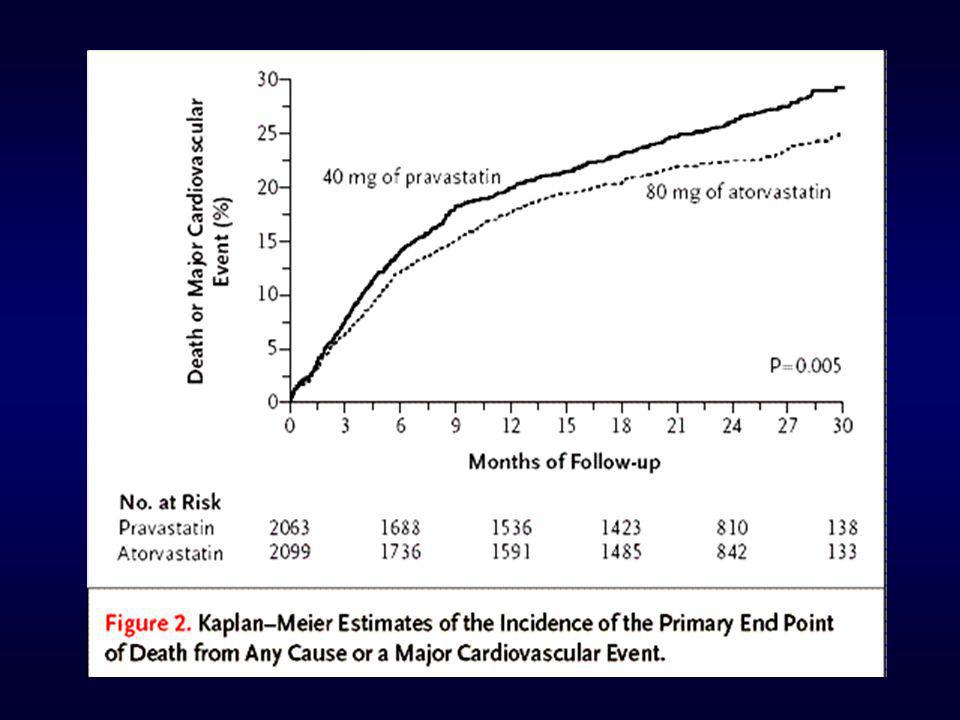
ESTUDIO TNT. EVENTOS CV MAYORES
Over the course of the study, there was a highly significant reduction in the composite efficacy outcome of major cardiovascular events (death from CHD, nonfatal non–procedure-related MI, resuscitated cardiac arrest, or fatal or nonfatal stroke) in the atorvastatin 80 mg group compared with the atorvastatin 10 mg group. The Kaplan-Meier analysis demonstrated a hazard ratio of 0.78 (95% CI 0.69, 0.89; P<0.001). This represented a 22% reduction in relative risk in the atorvastatin 80 mg group relative to the atorvastatin 10 mg group, over and above the low absolute event rate of 10.9% recorded in the atorvastatin 10 mg group. There was no statistical interaction for age or gender in the primary outcome measure. Reference 1. LaRosa JC, et al. N Engl J Med. 2005;352.
 in the atorvastatin 80 mg group compared with the atorvastatin 10 mg group. The Kaplan-Meier analysis demonstrated a hazard ratio of 0.78 (95% CI 0.69, 0.89; P<0.001). This represented a 22% reduction in relative risk in the atorvastatin 80 mg group relative to the atorvastatin 10 mg group, over and above the low absolute event rate of 10.9% recorded in the atorvastatin 10 mg group. There was no statistical interaction for age or gender in the primary outcome measure. Reference. 1. LaRosa JC, et al. N Engl J Med. 2005;352.")
16
ATORVASTATINA: ESTUDIO ASCOT
: CT: 160 mg/dl; c-LDL: 85,5 mg/dl : CT: 212 mg/dl; c-LDL: 133 mg/dl Sever PS, et al. Lancet :

17
Reducción del riesgo relativo: 37% (IC del 95%: 17-52)
Efecto de atorvastatina sobre el parámetro principal de eficacia: Eventos cardiovasculares mayores, con ictus incluido Reducción del riesgo relativo: 37% (IC del 95%: 17-52) 15 P=0,001 Placebo 127 eventos 10 -37% Riesgo acumulado (%) 5 Atorvastatina 83 eventos El parámetro principal de eficacia comprendía los siguientes puntos: episodios de enfermedad coronaria aguda (IM con infarto silente, angina inestable, muerte por EC aguda, paro cardiaco con posterior reanimación), procedimientos de revascularización coronaria o ictus (mortal o no mortal). El tratamiento con atorvastatina 10 mg/día se asoció a una reducción altamente significativa del 37% en la incidencia del parámetro principal de eficacia de eventos cardiovasculares mayores e ictus (P=0,001). No todos los pacientes cumplieron completamente su tratamiento aleatorizado. Si todos los pacientes hubiesen seguido el tratamiento asignado, la reducción del riesgo del 37% podría considerarse una estimación conservadora. Podría decirse que con un cumplimiento perfecto, podría haberse esperado una reducción del riesgo de hasta un 46% en el parámetro principal de eficacia. La reducción de riesgo observada coincide con la descrita en HPS y ASCOT. La reducción del 37% de eventos cardiovasculares mayores de CARDS es la estimación puntual más importante del efecto del tratamiento observada en los tres estudios realizados con agentes hipolipemiantes para la prevención primaria en diabetes. En pacientes con diabetes y ECV clínicamente no evidente, el HPS demostró una reducción del riesgo del 33% durante 5 años (P=0,0003) y el ASCOT demostró una reducción del riesgo del 23% durante 3,3 años (P<0,001)2,3. 1. Colhoun HM, Betteridge DJ, Durrington PN, et al. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): A multicentre randomised placebo-controlled trial. Lancet. 2004;364: Collins R, Armitage J, Parish S, Sleigh P, Peto R. Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol-lowering with simvastatin in 5963 people with diabetes: a randomized placebo-controlled trial. Lancet. 2003;361: Sever PS, Dahlof B, Poulter N et al. ASCOT-LLA: questions about the benefits of atorvastatin. Lancet. 2003;361: 1 2 3 4 4,75 Años Placebo 1410 1351 1306 1022 651 305 Atorva 1428 1392 1361 1074 694 328 Colhoun HM, Betteridge DJ, Durrington PN, et al. Lancet. 2004;364:
 15. P=0,001. Placebo. 127 eventos % Riesgo acumulado (%) 5. Atorvastatina. 83 eventos. El parámetro principal de eficacia comprendía los siguientes puntos: episodios de enfermedad coronaria aguda (IM con infarto silente, angina inestable, muerte por EC aguda, paro cardiaco con posterior reanimación), procedimientos de revascularización coronaria o ictus (mortal o no mortal). El tratamiento con atorvastatina 10 mg/día se asoció a una reducción altamente significativa del 37% en la incidencia del parámetro principal de eficacia de eventos cardiovasculares mayores e ictus (P=0,001). No todos los pacientes cumplieron completamente su tratamiento aleatorizado. Si todos los pacientes hubiesen seguido el tratamiento asignado, la reducción del riesgo del 37% podría considerarse una estimación conservadora. Podría decirse que con un cumplimiento perfecto, podría haberse esperado una reducción del riesgo de hasta un 46% en el parámetro principal de eficacia. La reducción de riesgo observada coincide con la descrita en HPS y ASCOT. La reducción del 37% de eventos cardiovasculares mayores de CARDS es la estimación puntual más importante del efecto del tratamiento observada en los tres estudios realizados con agentes hipolipemiantes para la prevención primaria en diabetes. En pacientes con diabetes y ECV clínicamente no evidente, el HPS demostró una reducción del riesgo del 33% durante 5 años (P=0,0003) y el ASCOT demostró una reducción del riesgo del 23% durante 3,3 años (P<0,001)2,3. 1. Colhoun HM, Betteridge DJ, Durrington PN, et al. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): A multicentre randomised placebo-controlled trial. Lancet. 2004;364: Collins R, Armitage J, Parish S, Sleigh P, Peto R. Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol-lowering with simvastatin in 5963 people with diabetes: a randomized placebo-controlled trial. Lancet. 2003;361: Sever PS, Dahlof B, Poulter N et al. ASCOT-LLA: questions about the benefits of atorvastatin. Lancet. 2003;361: ,75. Años. Placebo Atorva Colhoun HM, Betteridge DJ, Durrington PN, et al. Lancet. 2004;364:")
18
Major Statin Trials: Historical Perspectives
Secondary Prevention 25 20 15 10 5 4S-P Primary Prevention 4S-S Simvastatin Pravastatin Lovastatin LIPID-P Percent with CHD event CARE-P PROSPER-S HPS-P TNT 10 LIPID-S PROSPER-P WOSCOPS-P Atorvastatin TNT 80 CARE-S WOSCOPS-S The link between elevated LDL-C levels and increased risk of CHD events is no longer disputed. Indeed, for both primary and secondary prevention trials, the relationship between on-treatment LDL-C levels and CHD event rates appears to be approximately linear. It is anticipated that data from TNT and IDEAL will show that this linear trend is maintained even at LDL-C levels below 100 mg/dL. HPS-S ASCOT-P* S = statin treated P = placebo treated *Extrapolated to 5 years ASCOT-S* AFCAPS-P AFCAPS-S 90 110 130 150 170 190 210 LDL-C (mg/dL)
")
20
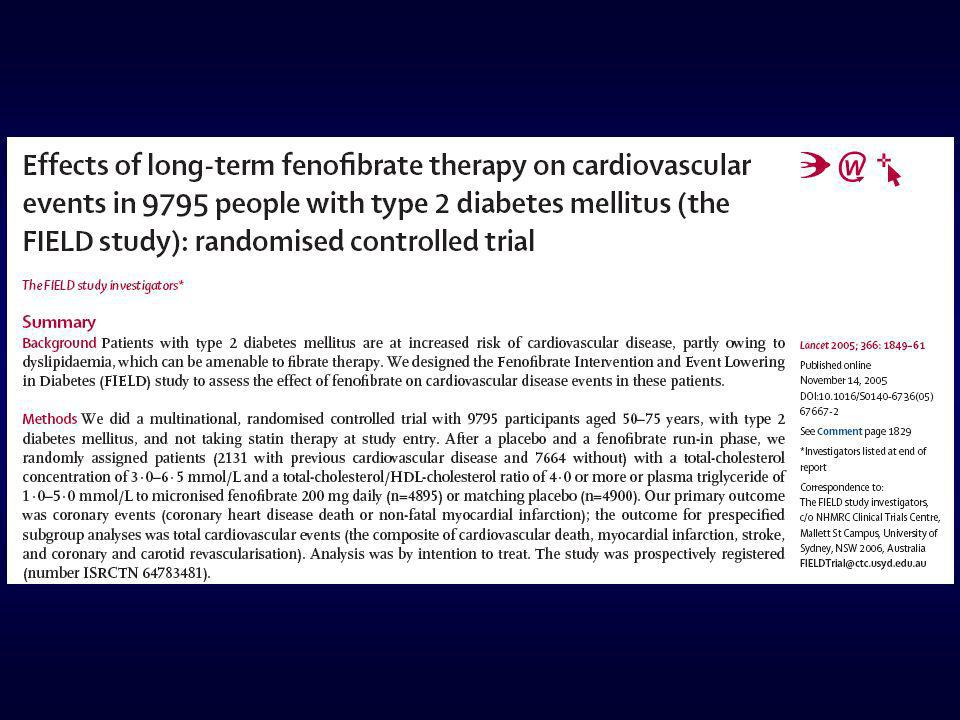
ESTUDIO FIELD. CURVAS DE EVENTOS
The FIELD study investigators. Lancet 2005;366:1849

22
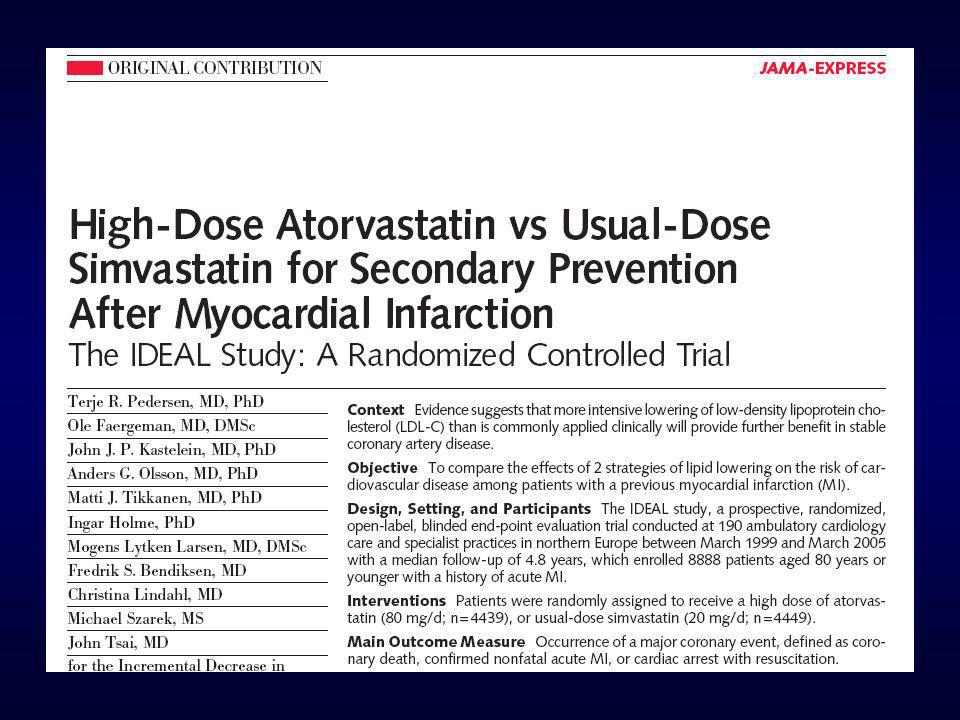
ESTUDIO IDEAL LDLc 105 mg/dl LDLc 78 mg/dl

23
PROPORCION DEL EFECTO DEL TRATAMIENTO (PET) EXPLICADO POR LOS CAMBIOS LIPIDICOS. ESTUDIO LIPID
ESTUDIO LIPID: Simes RJ, et al. Circulation 2002;105:

24
¿CUÁL ES EL OBJETIVO TERAPÉUTICO?
El objetivo es reducir LDL colesterol La reducción debe ser proporcional al riesgo Reducciones hasta 70 mg/dl de LDL colesterol mejoran morbimortalidad cardiovascular Reducciones hasta 100 mg/dl son coste-efectivas en prevención secundaria

25
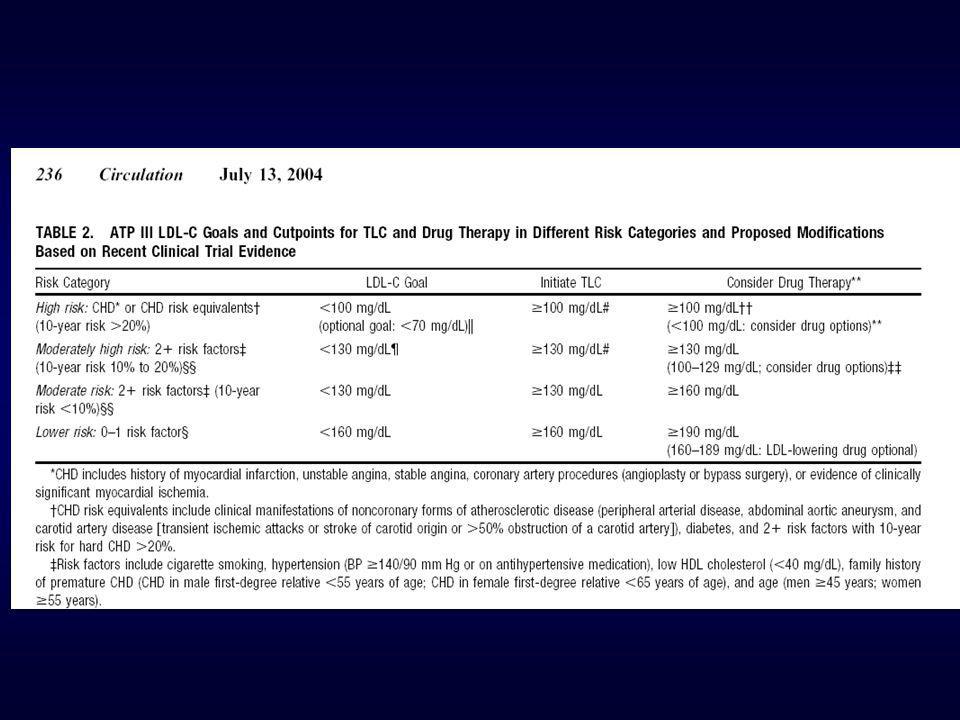
OBJETIVOS DE LDL-C Y NO-HDL-C EN LAS TRES CATEGORIAS DE RIESGO
National Cholesterol Education Program Adult Treatment Panel III (ATP III) Guidelines OBJETIVOS DE LDL-C Y NO-HDL-C EN LAS TRES CATEGORIAS DE RIESGO Risk Category LDL-C Goal (mg/dL) Non-HDL-C Goal (mg/dL) CHD and CHD Risk Equivalent (10-year risk for CHD >20% <100 <130 Multiple (2+) Risk Factors and 10-year risk <20% <130 <160 0–1 Risk Factor <160 <190
 Guidelines. OBJETIVOS DE LDL-C Y NO-HDL-C EN LAS TRES CATEGORIAS DE RIESGO. Risk Category. LDL-C Goal. (mg/dL) Non-HDL-C Goal (mg/dL) CHD and CHD Risk Equivalent. (10-year risk for CHD >20% <100. <130. Multiple (2+) Risk Factors and. 10-year risk <20% <130. <160. 0–1 Risk Factor. <160. <190.")
28
CANDIDATOS PARA LDLc < 70 mg/dl

29
¿Qué cifra de colesterol es normal?
¿Cuál es el objetivo terapéutico? ¿Qué objetivos se alcanzan en la actualidad? ¿Qué fármacos son de elección?

30
ESTUDIO HISPALIPID Control Dislipemia en Consultas No control Control
100 84,9 90 80 71,0 67,1 70 58,3 60 % Control 50 43,4 40 32,9 29,0 30 15,1 20 10 Total R. Alto R. Medio R. Bajo Categoría de riesgo NCEP-ATP III

31
PACIENTES DISLIPEMICOS Y OBJETIVOS TERAPÉUTICOS: ESTUDIO REALITY
Tratamiento y logro de objetivos en España En total, un 27% de los pacientes alcanza los objetivos c-LDL 12,92% de pacientes en objetivo (n=80) 619 pacientes 48,8% de pacientes no cambian de potencia de dosis (n=263) 31,5% de pacientes en objetivo (n=87) 87,08% de pacientes no en objetivo (n=539) 51,2% de pacientes cambian de potencia (n=276) Diapositiva 11 PACIENTES DISLIPEMICOS Y OBJETIVOS TERAPÉUTICOS: ESTUDIO REALITY TRATAMIENTO Y LOGRO DE OBJETIVOS EN c-LDL EN ESPAÑA. Se evaluaron en el estudio REALITY 619 pacientes, de los cuales sólo el 13% (n=80) alcanzaron el objetivo de c-LDL con el tratamiento hipolipemiante inicial mientras que el 87% restante no alcanzaron el objetivo de c-LDL.13 Al 51,2% de los pacientes se les modificó el tratamiento hipolipemiante y tras esa modificación el 31,5% lograron el objetivo lipídico, es decir, el 14% del total de pacientes evaluados, lograron objetivos de c-LDL tras modificar el tratamiento inicial. Al 48,8% de los pacientes no se les cambió de potencia la dosis de tratamiento hipolipemiante, no llegando así a objetivos. Por otro lado, el 68,5% de los pacientes a quienes se modificó la dosis inicial, tampoco lograron los objetivos. Por tanto, en total, solamente un 27% de los pacientes alcanzaron objetivos de c-LDL.13 68,5% de pacientes no en objetivo (n=189) Tomado de García Ruiz FJ et al. [Poster & Abstract No. 304]. Presentados en: The 3rd World Congress on Heart Disease - New Trends in Research, Diagnosis and Treatment. Washington, D.C.,USA, July 12-15, The Journal of Heart Disease 2003;3(1): 76.
 619 pacientes. 48,8% de pacientes no cambian de potencia de dosis (n=263) 31,5% de pacientes en objetivo (n=87) 87,08% de pacientes no en objetivo (n=539) 51,2% de pacientes cambian de potencia (n=276) Diapositiva 11. PACIENTES DISLIPEMICOS Y OBJETIVOS TERAPÉUTICOS: ESTUDIO REALITY. TRATAMIENTO Y LOGRO DE OBJETIVOS EN c-LDL EN ESPAÑA. Se evaluaron en el estudio REALITY 619 pacientes, de los cuales sólo el 13% (n=80) alcanzaron el objetivo de c-LDL con el tratamiento hipolipemiante inicial mientras que el 87% restante no alcanzaron el objetivo de c-LDL.13. Al 51,2% de los pacientes se les modificó el tratamiento hipolipemiante y tras esa modificación el 31,5% lograron el objetivo lipídico, es decir, el 14% del total de pacientes evaluados, lograron objetivos de c-LDL tras modificar el tratamiento inicial. Al 48,8% de los pacientes no se les cambió de potencia la dosis de tratamiento hipolipemiante, no llegando así a objetivos. Por otro lado, el 68,5% de los pacientes a quienes se modificó la dosis inicial, tampoco lograron los objetivos. Por tanto, en total, solamente un 27% de los pacientes alcanzaron objetivos de c-LDL ,5% de pacientes no en objetivo (n=189) Tomado de García Ruiz FJ et al. [Poster & Abstract No. 304]. Presentados en: The 3rd World Congress on Heart Disease - New Trends in Research, Diagnosis and Treatment. Washington, D.C.,USA, July 12-15, The Journal of Heart Disease 2003;3(1):")
32
PACIENTES DISLIPEMICOS Y OBJETIVOS TERAPÉUTICOS: ESTUDIO REALITY
% de pacientes en cifras objetivo de c-LDL 40% 27% 20,21% % de pacientes 20% Diapositiva 12: PACIENTES DISLIPEMICOS Y OBJETIVOS TERAPÉUTICOS: ESTUDIO REALITY % de pacientes en cifras objetivo de c-LDL Se evaluaron 619 pacientes, sólo el 13% de los pacientes alcanzaron el objetivo de c-LDL con el tratamiento hipolipemiante inicial, y un 14% adicional lo alcanzó tras modificar el tratamiento inicial, para lograr un total de 27% al final del periodo de seguimiento. Sin embargo de los pacientes con enfermedad cardiovascular (coronaria y equivalentes) alcanzaron el objetivo de c-LDL (<100 mg/dl), tan solo el 20,21%.13 0% TOTAL (n=619) ENF. CORONARIA Y EQUIVALENTES* (n=282) * Objetivo de c-LDL < 100 mg/dl, según NCEP ATP III.8 Tomado de García Ruiz FJ et al. [Poster & Abstract No. 304]. Presentados en: The 3rd World Congress on Heart Disease - New Trends in Research, Diagnosis and Treatment. Washington, D.C.,USA, July 12-15, The Journal of Heart Disease 2003;3(1): 76.
 alcanzaron el objetivo de c-LDL (<100 mg/dl), tan solo el 20,21%.13. 0% TOTAL (n=619) ENF. CORONARIA Y EQUIVALENTES* (n=282) * Objetivo de c-LDL < 100 mg/dl, según NCEP ATP III.8. Tomado de García Ruiz FJ et al. [Poster & Abstract No. 304]. Presentados en: The 3rd World Congress on Heart Disease - New Trends in Research, Diagnosis and Treatment. Washington, D.C.,USA, July 12-15, The Journal of Heart Disease 2003;3(1):")
33
¿Qué cifra de colesterol es normal?
¿Cuál es el objetivo terapéutico? ¿Qué objetivos se alcanzan en la actualidad? ¿Qué fármacos son de elección?

34
Eficacia comparada de estatinas
Civeira F, et al. Atherosclerosis 2004;173:55-68

35
EZETIMIBA COADMINISTRADA CON ESTATINAS: CONSISTENCIA EN LOS RESULTADOS DE LOS ESTUDIOS
Estatina sola Estatina + ezetimiba 0.5 1.5 2.5 3.0 3.5 1.0 2.0 0.5 1.5 2.5 3.0 3.5 1.0 2.0 3.5 20% 3.5 3.4 20% 21% 2.9 21% 2.8 2.8 2.7 22% 2.7 C-LDL medio (mmol/l) al final del estudio 2.3 2.1 Atorvastatina Simvastatina Pravastatina Lovastatina Tratamiento en curso con estatinas Datos del dossier de registro desarrollados por la compañía, disponibles mediante petición a MSD1
 al final del estudio Atorvastatina. Simvastatina. Pravastatina. Lovastatina. Tratamiento en curso. con estatinas. Datos del dossier de registro desarrollados por la compañía, disponibles mediante petición a MSD1.")
36
RESUMEN La cifra de colesterol “normal” es mucho más baja de las que hemos venido considerando El objetivo del tratamiento hipolipemiante es reducir el LDL colesterol La reducción debe ser proporcional al riesgo Las estatinas, solas o en combinación con ezetimiba, son los fármacos de elección

Presentaciones similares