Descargar la presentación
La descarga está en progreso. Por favor, espere

1
ARRITMIAS

2
TAQUIARRITMIAS BRADIARRITMIAS ASISTOLIA

3
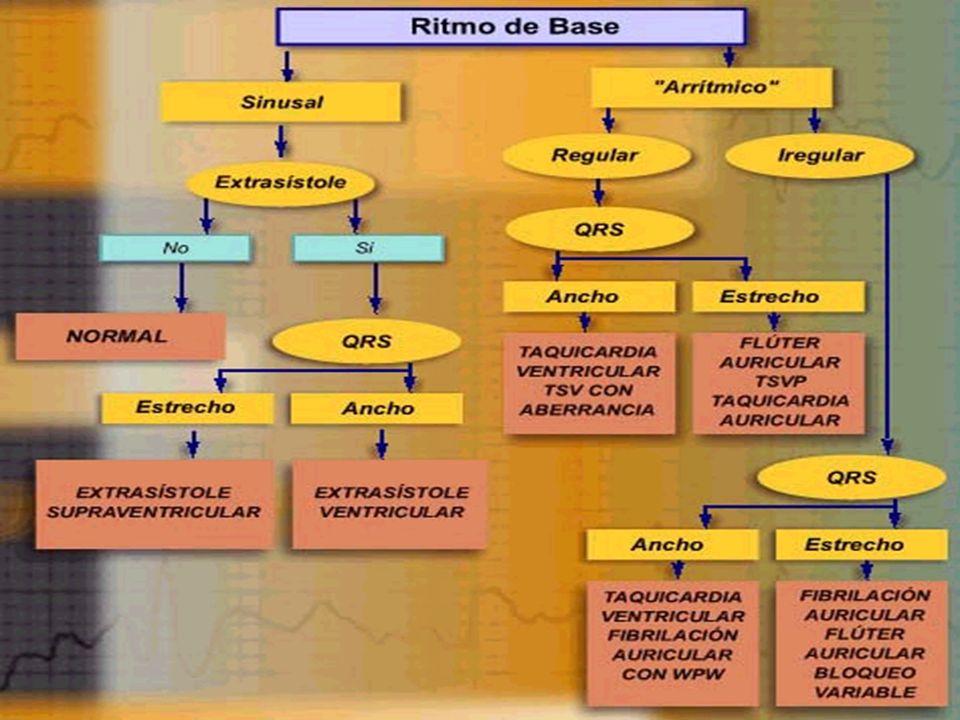
TAQUIARRITMIAS QRS ANGOSTO SINUSAL.-. FRECUENCIA > 100/MIN
SUPRAVENTRICULAR.->150/MIN (AUNQUE HAYA ONDA P ) ESTABLE O INESTABLE SIGNOS CLINICOS: HIPERTENSION CONGESTION PULMONAR (EDEMA) CONGESTION SISTEMICA
 ESTABLE O INESTABLE. SIGNOS CLINICOS: HIPERTENSION. CONGESTION PULMONAR (EDEMA) CONGESTION SISTEMICA.")
4
TAQUIARRITMIAS QRS ANGOSTO TAQUICARDIA SUPRAVENTRICULAR
POR REENTRADA FIBRILACION AURICULAR FLUTTER AURICULAR

5
TAQUICARDIA SINUSAL Emphasize the differences between PSVT and sinus tachycardia. It always makes for an interesting discussion with valuable teaching points to present a patient who is suffering from every possible sign of instability: SOB, low BP, poor mentation, chest pain, syncope on standing, rales heard in the chest. Tell the students that the above sinus tachycardia is the rhythm of the “unstable” patient. See how many people would elect to perform cardioversion for an “unstable tachycardia.” If you continue to increase the rate and continue to have the patient deteriorate, more and more students will raise their hand to indicate they would cardiovert. Of course, cardioversion is wrong—your goal with cardioversion is to convert the patient to a sinus rhythm. Cardioversion cannot make sinus tachycardia any better than it already is.

6
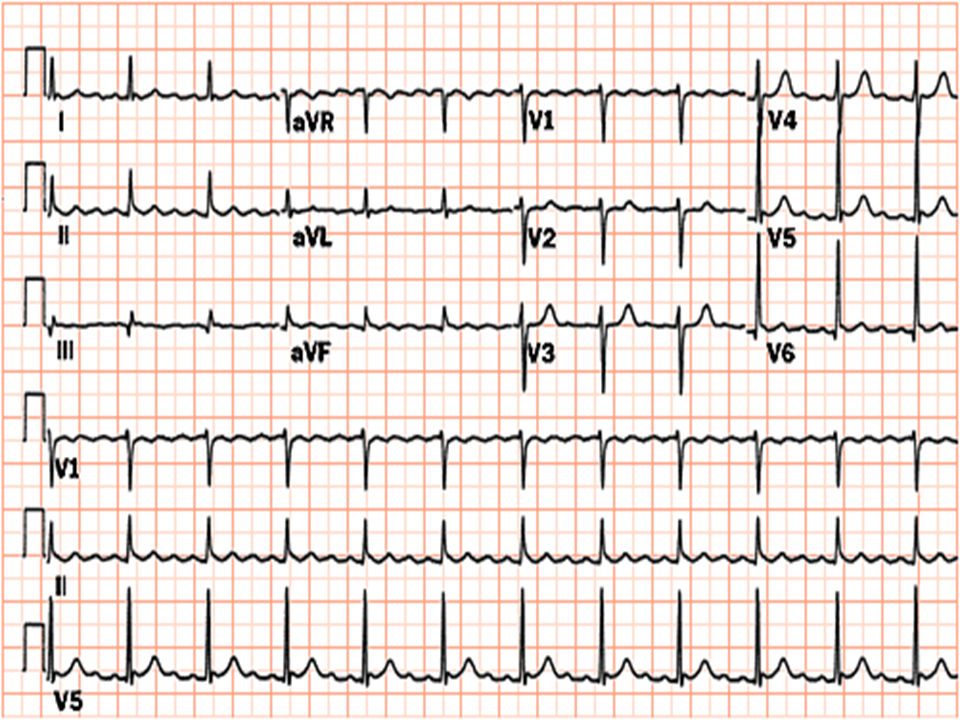
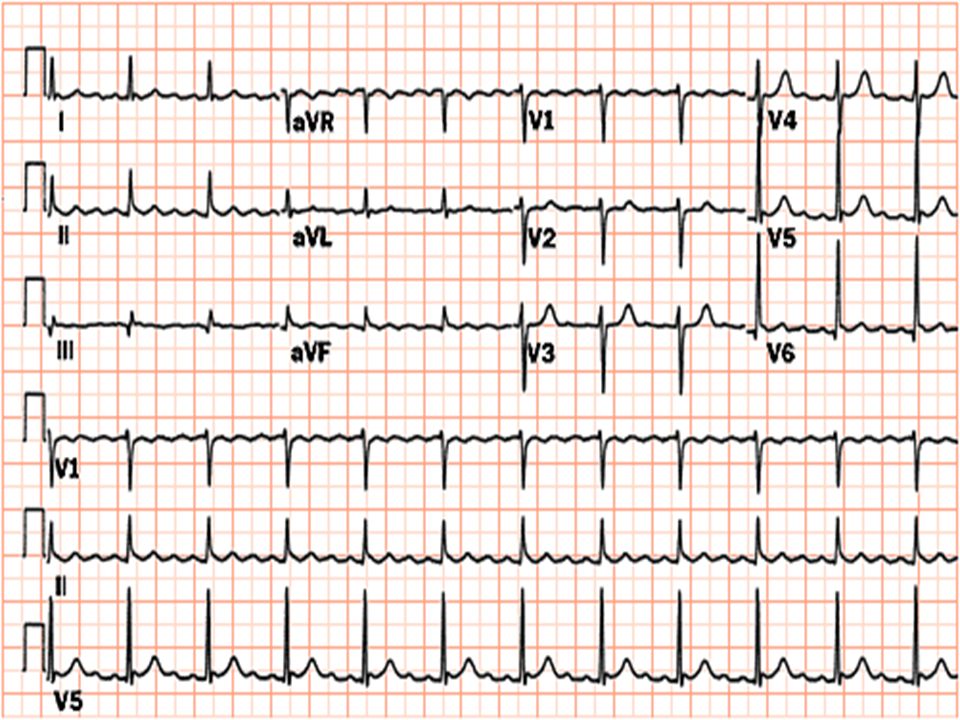
TAQUICARDIA SPV PAROXISTICA
Review the key characteristics of PSVT.

7
SPV

8
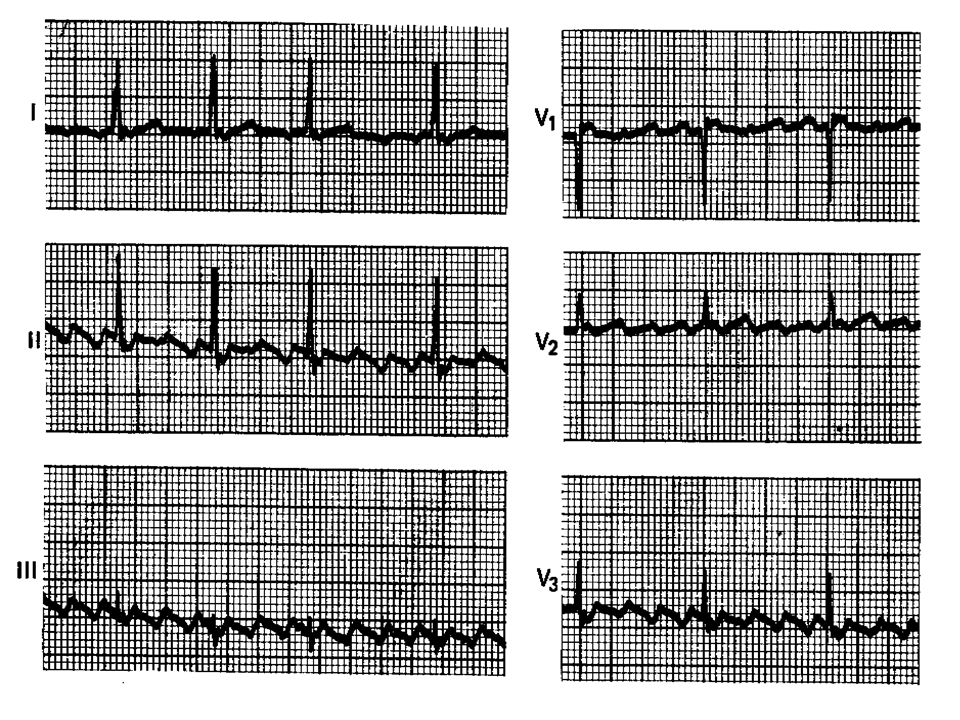
FIBRILACION AURICULAR

11
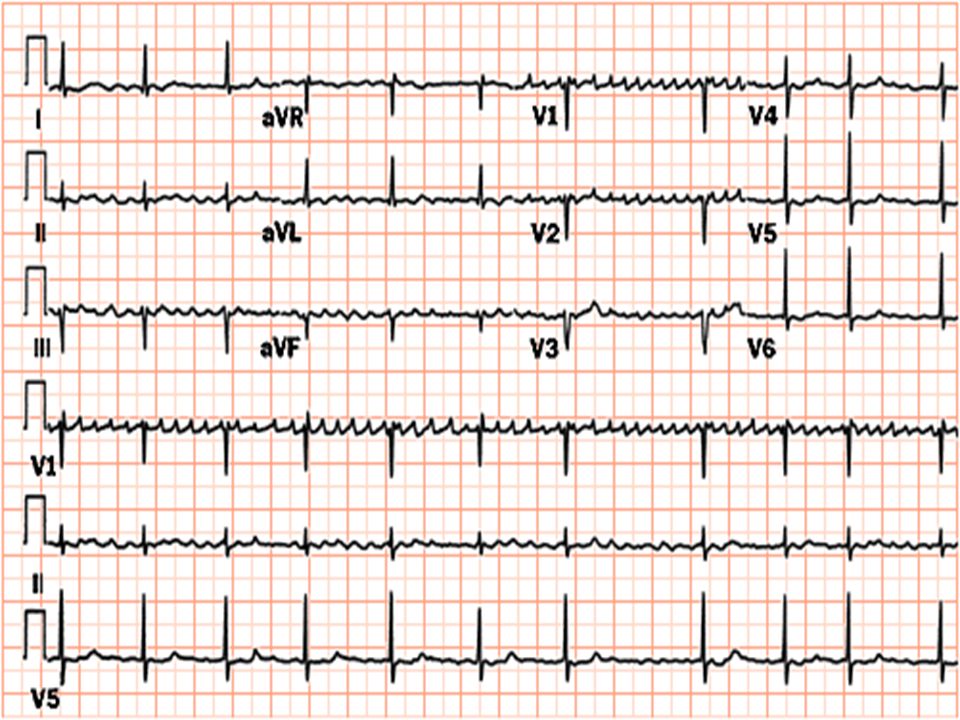
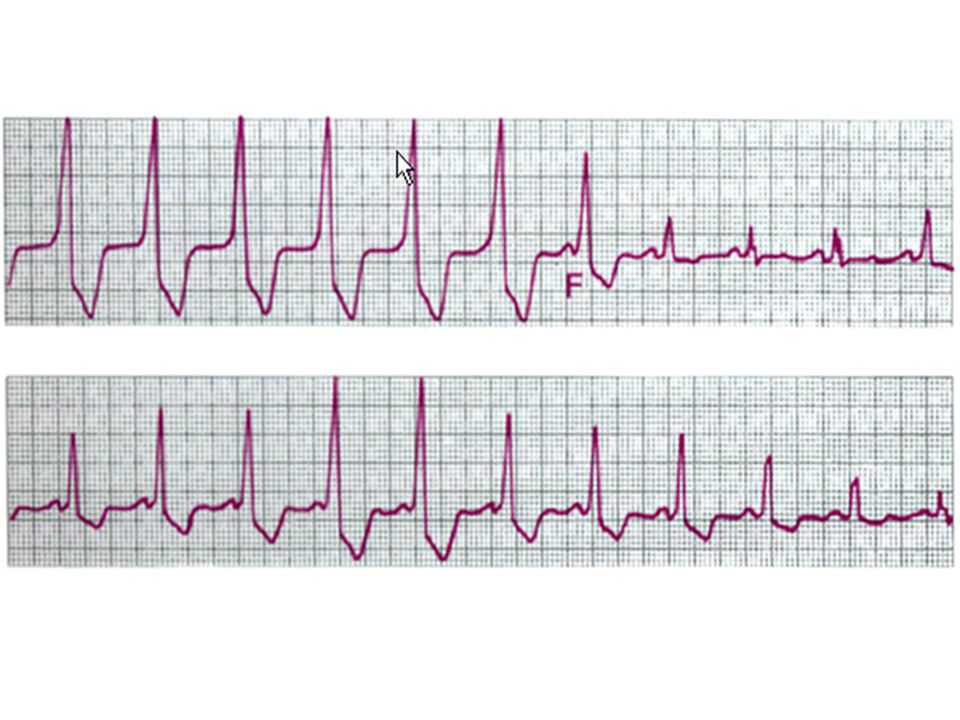
FLUTTER AURICULAR MEC.- REENTRADA INTRA AURICULAR
TIPO I ( ) P NEG II,III, VF TIPO II ( ) P POS II,DIII,VF PUEDE HABER BLOQUEO AV, VARIABLE TX CARDIOVERSION, CA- ANTAGO, ADENOSINA, PROPANOL, PROPAFENONA, FLECAINIDA
 P NEG II,III, VF. TIPO II ( ) P POS II,DIII,VF. PUEDE HABER BLOQUEO AV, VARIABLE. TX CARDIOVERSION, CA- ANTAGO, ADENOSINA, PROPANOL, PROPAFENONA, FLECAINIDA.")
15
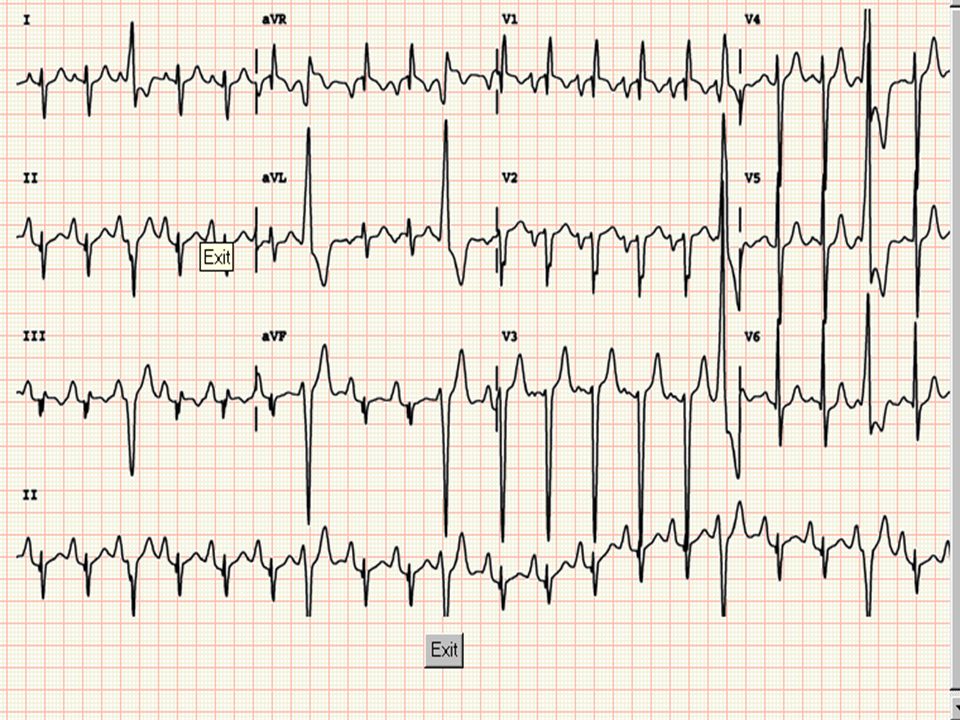
TAQUICARDIA POR VIA ANOMALA (SWPW)
7% DE LAS ARRITMIAS EN INC 90% MENORES DE 50 AÑOS (MASCULINO) 70-85% CORAZON ESTRUCTURALMENTE NORMAL ENOM. EBSTEIN.- MAS FRECUENTE MEC.- MACRORRENTRADA (MOV. CIRCULAR) PR CORTO, QRS ANCHO (ONDA DELTA)
 70-85% CORAZON ESTRUCTURALMENTE NORMAL. ENOM. EBSTEIN.- MAS FRECUENTE. MEC.- MACRORRENTRADA (MOV. CIRCULAR) PR CORTO, QRS ANCHO (ONDA DELTA)")
16
SWP-

17
MANEJO 1)ANTIARRITMICOS (PARA CONTROLAR
FRECUENCIA Y DISMUNIR CONSUMO O2 MIOCARDICO) 2)ESTUDIOS DE GABINETE PARA DESCARTAR PRESENCIA DE TROMBOS AURICULARES (ECO T. ESOF) 2)ANTICOAGULACION 3)CARDIOVERSION (PARA REVERTIR EL RITMO)
 2)ESTUDIOS DE GABINETE PARA DESCARTAR. PRESENCIA DE TROMBOS AURICULARES (ECO T. ESOF) 2)ANTICOAGULACION. 3)CARDIOVERSION (PARA REVERTIR EL RITMO)")
18
TAQUIARRITMIAS QRS ANCHO GENERALMENTE SON VENTRICULARES
NO SE PRECEDEN DE P MAS INESTABLES (SIND. BAJO GASTO) CON O SIN PULSO TIPO DE CARDIOVERSION
 CON O SIN PULSO. TIPO DE CARDIOVERSION.")
19
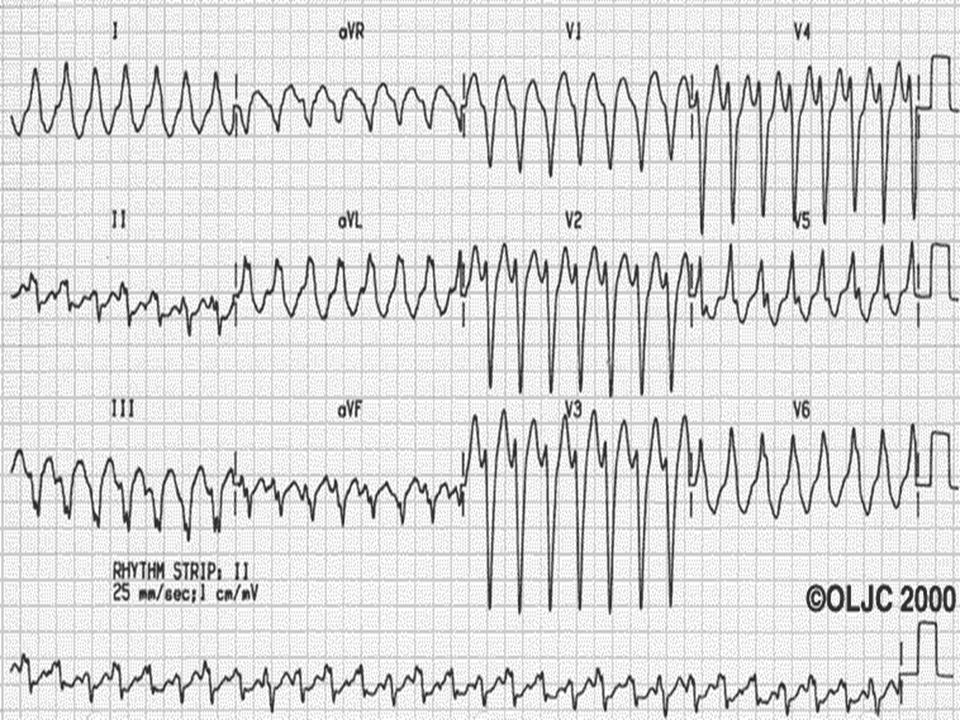
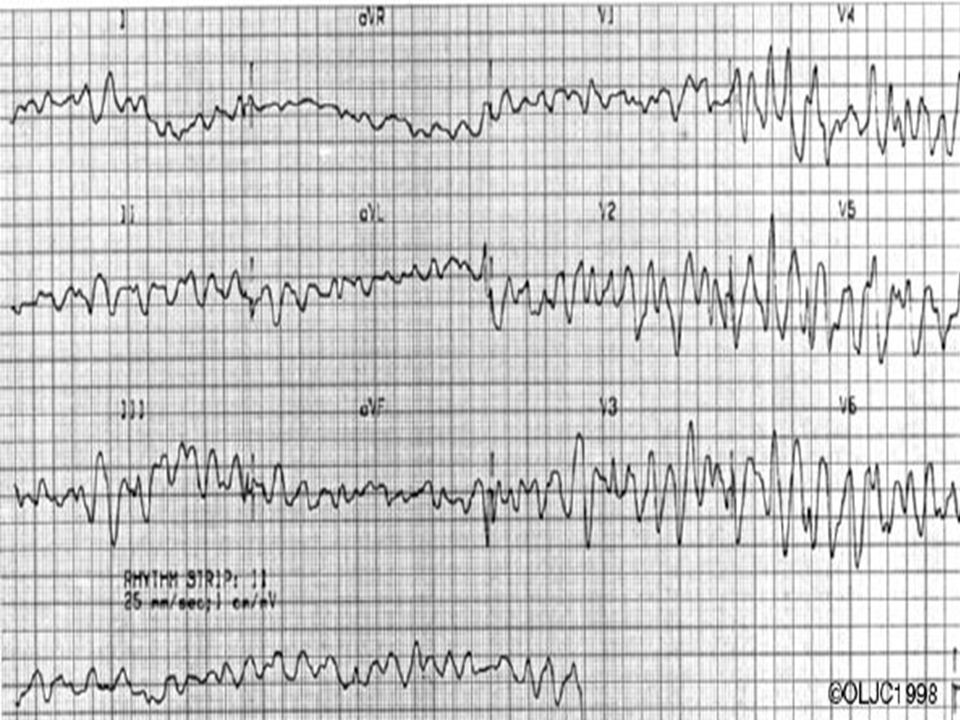
TAQUICARDIA QRS ANCHO TV vs TSPV CON COND. ABERRANTE
Note the obvious distinguishing feature of the tracing (ie, wide QRS complexes) and ask the participants for a diagnosis. Mention the possibilities of either ventricular tachycardia or supraventricular tachycardia with aberrant conduction.
 and ask the participants for a diagnosis. Mention the possibilities of either ventricular tachycardia or supraventricular tachycardia with aberrant conduction.")
20
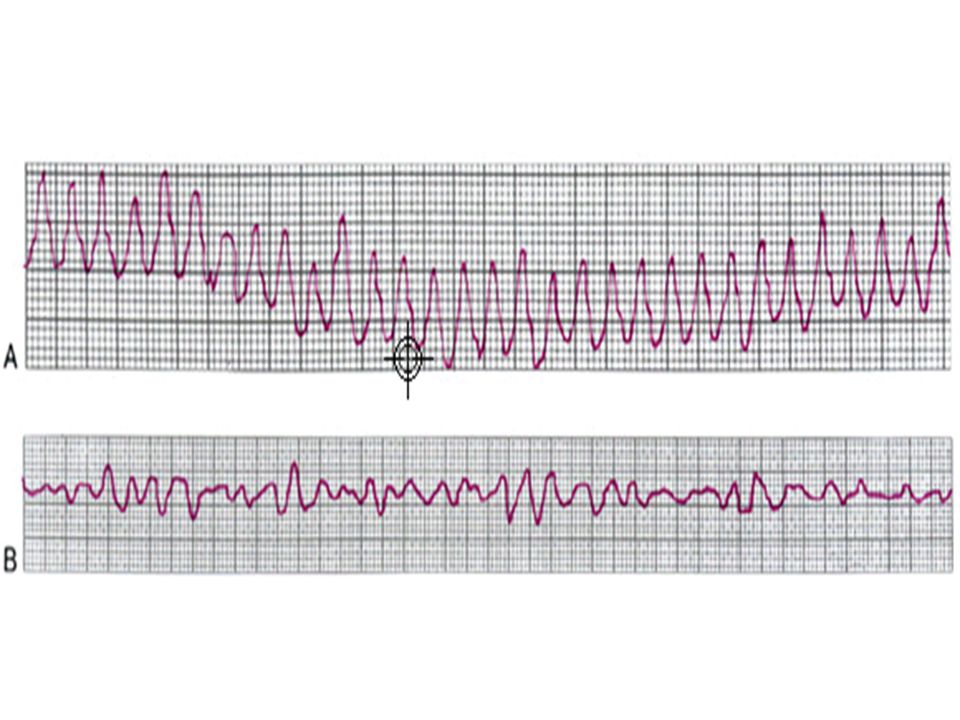
TAQUICARDIAS VENTRICULARES
MONOMORFICA POLIMORFICA SOSTENIDA NO SOSTENIDA TV CLASICA TV HELICOIDAL FLUTTER VENTRICULAR FIBRILACION VENTRICULAR

24
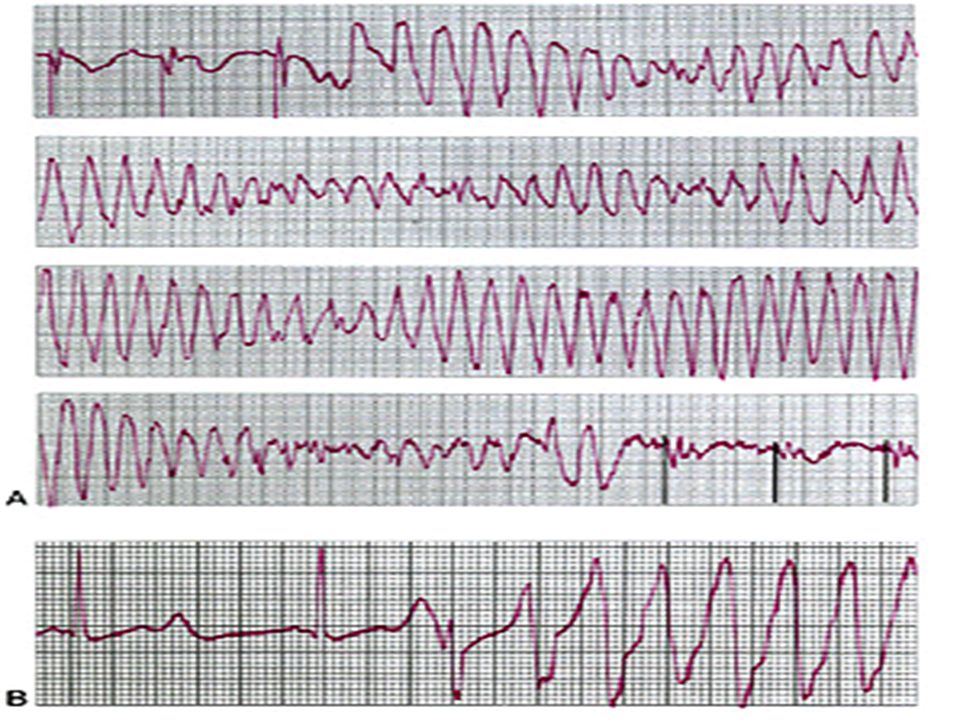
TAQUICARDIA VENTRICULAR HELICOIDAL (TORSADE POINTES)
")
28
PRINCIPALES CRITERIOS DX:
Una taquicardia regular con QRS ancho en un paciente con antecedente de infarto de miocardio es ventricular mientras no se demuestre lo contrario PRINCIPALES CRITERIOS DX: Presencia de DISOCIACIÓN AV Presencia de Capturas y/o Fusiones Criterios de anchura de QRS Criterios de morfología y eje

29
SINDROME TAQUI-BRADI Use this rhythm as a summary and review of the important elements of caring for tachycardias. See how many students would shout out a treatment just after seeing only this rhythm. Several pieces of information are critical to managing this rhythm. Plan on a brief history to present along with this rhythm as the students begin to ask clinical questions. They should ask: 1. Is this patient stable or unstable? (Hint: make the rhythm unstable in that it keeps reverting to the wide-complex tachycardia. Each time the patient stays in the wide-complex tachycardia for longer periods and begins to clinically deteriorate. 2. Does this patient have a normal cardiac function or is the function impaired? Look at the algorithms and state what differences the heart condition would make in treatment. 3. What medications are already on board? (Either chronically or given within the last hour or so.) 4. Play out the scenario where this rhythm is occurring (going back and forth between wide-complex tachycardia and second-degree heart block.) See how many students will notice that between the tachycardia episodes the patient has type II second-degree heart block, which if symptomatic is an indication for other drugs as well as pacing. Direct them to the Bradycardia Algorithm (page 14) and state the drugs that could possibly be used there (atropine, epinephrine, isoproteronol). What would be the effect if one of those agents was started to treat the heart block and the patient returned to the tachycardia? 5. Should further therapy be guided by the Narrow-Complex Tachycardia Algorithm on page 18; the algorithm for wide-complex tachycardia of unknown type on page 15; or the Stable Ventricular Tachycardia Algorithm on page 19?
 4. Play out the scenario where this rhythm is occurring (going back and forth between wide-complex tachycardia and second-degree heart block.) See how many students will notice that between the tachycardia episodes the patient has type II second-degree heart block, which if symptomatic is an indication for other drugs as well as pacing. Direct them to the Bradycardia Algorithm (page 14) and state the drugs that could possibly be used there (atropine, epinephrine, isoproteronol). What would be the effect if one of those agents was started to treat the heart block and the patient returned to the tachycardia 5. Should further therapy be guided by the Narrow-Complex Tachycardia Algorithm on page 18; the algorithm for wide-complex tachycardia of unknown type on page 15; or the Stable Ventricular Tachycardia Algorithm on page 19")
30
CONOCIMIENTOS BASICOS DE TODO MEDICO
-CONOCER Y MANEJAR UN DESFIBRILADOR/MONITOR -SABER COMO COLOCAR LOS ELECTRODOS PARA MONITORIZAR RA LA LA LL C -DIFERENCIAR CARDIOVERSION /DEFIBRILACION

31
CONOCIMIENTOS BASICOS DE TODO MEDICO
-SABER CARDIOVERTIR Y/O DESFIBRILAR -SABER CUANDO CARDIOVERTIR EN MODO SINCRONIZADO / NO SINCRONIZADO -RECONOCER LOS CUIDADOS MAS IMPORTANTES POSTCARDIOVERSION (O2, IV,MONITOREO, ANTIARRITMICOS)
")
32
DEBE SER PREMEDICADA A)CARDIOVERSION SINCRONIZADA
TAQUICARDIAS ESTABLES DESCARGA PORCION DESCENDENTE DE LA ONDA T DEBE SER PREMEDICADA

33
PERIODOS REFRACTARIOS
ABSOLUTO RELATIVO

34
Cardioversion Sincronizada
Niveles de descarga: TSPVP: 50 J, 100 J, 200 J, 300 J, 360 J TV: 100 J, 200 J, 300 J, 360 J TV Polimorfica (como FV): 200 J, 200 to 300 J, 360 J Fibril. auric: 100 J, 200 J, 300 J, 360 J Flutter auric: 100 J, 200 J, 300 J, 360 J Solicit participant responses. Complications may include deterioration to VF, embolization of a thrombus, etc. If the rhythm deteriorates to VF, instruct the participants to rapidly assess cardiovascular status and proceed to immediate defibrillation.
: 200 J, 200 to 300 J, 360 J. Fibril. auric: 100 J, 200 J, 300 J, 360 J. Flutter auric: 100 J, 200 J, 300 J, 360 J. Solicit participant responses. Complications may include deterioration to VF, embolization of a thrombus, etc. If the rhythm deteriorates to VF, instruct the participants to rapidly assess cardiovascular status and proceed to immediate defibrillation.")
35
Cardioversion Sincronizada
Valorar Premedición : Diazepam Midazolam Barbiturates Etomidate Ketamine Methohexital Analgesics Fentanyl Morphine Meperidine Sedatives may be used for the awake, hemodynamically unstable patient. Some facilities prefer to use anesthesia for elective synchronized cardioversion attempts. The hemodynamic status of the patient and the potential for further deterioration should be considered. Watch for apnea or hypoventilation after sedation. Frequent monitoring of vital signs after cardioversion is essential until stabilization occurs.

36
B)CARDIOVERSION ASINCRONICA (DESFIBRILACION)
DESPOLARIZACION COMPLETA DE LA CELULA PARA QUE GENERE UN POT. DE ACCION NORMAL Y UNA CONTRACTILIDAD COORDINADA (RESET) TAQUIC. SPV INESTABLES (DESCARGAS BAJAS CON AUMENTO PROGRESIVO) TV,FV, SIN PULSO ( 360 J) + RCP
 TAQUIC. SPV INESTABLES (DESCARGAS. BAJAS CON AUMENTO PROGRESIVO) TV,FV, SIN PULSO. ( 360 J) + RCP.")
38
RECOMENDACIONES GENERALES
No ponerse más sintomático que el paciente Valorar inicialmente la tolerancia hemodinámica de la arritmia Si la tolerancia es aceptable : ECG de 12 derivaciones, registros a diferentes ampliaciones y velocidades. Intenta ver ondas P, especialmente en I y V1 Una vez finalizada la taquicardia observar con detenimiento el ECG en ritmo sinusal, puede aclarar el diagnóstico. (p.ej. si en ritmo sinusal aparece conducción por vía accesoria una taquicardia con QRS ancho en este contexto probablemente sea supraventricular)
")
39
PRINCIPALES CRITERIOS DX:
Una taquicardia regular con QRS ancho en un paciente con antecedente de infarto de miocardio es ventricular mientras no se demuestre lo contrario PRINCIPALES CRITERIOS DX: Presencia de DISOCIACIÓN AV Presencia de Capturas y/o Fusiones Criterios de anchura de QRS Criterios de morfología y eje

Presentaciones similares






>")













