Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Dolor, Inflamación y Gota
TEMA 3

2
Prevalencia del Dolor Dos de cada tres personas acuden al médico por dolor Presente en 80% de pacientes oncológicos El 16% de la población >16 años sufre patología reumática (80% de evolución crónica) Vivencia determinada por Intensidad del daño físico Estado psicológico del paciente (ansiedad, miedo, depresión...) Elevada prevalencia media En Europa uno de cada cinco adultos tiene dolor crónico Una de cada tres familias se ve afectada por dolor crónico Breivik et al. Europ J Pain 2005: Epub
 Vivencia determinada por. Intensidad del daño físico. Estado psicológico del paciente (ansiedad, miedo, depresión...) Elevada prevalencia media. En Europa uno de cada cinco adultos tiene dolor crónico. Una de cada tres familias se ve afectada por dolor crónico. Breivik et al. Europ J Pain 2005: Epub.")
3
Escalera analgésica de la O.M.S.
Antidepresivos Imipramina, amitriptilina, mianserina, doxepina Neurolépticos Levopromacina, clorpromacina, haloperidol Ansiolíticos Clobazam, lorazepam, diazepam, clorazepato Anticonvulsivantes Carbamazepina, gabapentina, difenilhidantoína Otros OPIOIDE POTENTE (morfina) OPIOIDE DÉBIL (codeína) AINE (AAS, paracetamol, otros Aine) ± NO OPIOIDE ± ANALGÉSICO COADYUVANTE
 OPIOIDE DÉBIL. (codeína) AINE. (AAS, paracetamol, otros Aine) ± NO OPIOIDE. ± ANALGÉSICO COADYUVANTE.")
4
LESIÓN TISULAR INFLAMACIÓN LOCAL PERCEPCIÓN DEL DOLOR

5
Representan el 25% de toda la toxicidad por fármacos
Suponen mas del 15% del gasto total del S.N.S. Más del 20% de la población adulta ha tomado AINE durante al menos 1 mes. La mayoría son medicamentos OTC (3 formulaciones entre los 10 fármacos OTC más consumidos) Comparten las tres acciones que los definen (analgésica, antitérmica y antiinflamatoria) pero su eficacia relativa para cada una de ellas puede ser diferente. Su toxicidad puede coincidir con la del grupo o ser relativamente especifica. Pocas diferencia entre v. oral o parenteral Representan el 25% de toda la toxicidad por fármacos
 Comparten las tres acciones que los definen (analgésica, antitérmica y antiinflamatoria) pero su eficacia relativa para cada una de ellas puede ser diferente. Su toxicidad puede coincidir con la del grupo o ser relativamente especifica. Pocas diferencia entre v. oral o parenteral. Representan el 25% de toda la toxicidad por fármacos.")
6
Respuesta inflamatoria
FOSFOLÍPIDOS ACIDO ARAQUIDÓNICO CORTICOIDES AINES PLA2 LOX COX Inflamación + Sistema nervioso Células sanguíneas Sistema cardiovascular Sistema reproductor y endocrino Tracto gastrointestinal Riñón PROSTACICLINAS TROMBOXANOS PROSTAGLANDINAS LIPOXINAS LEUCOTRIENOS

7
Patofisiología Homeostasis Acido araquidónico AINE COX-1 COX-2
(constitutiva) COX-2 (inducible) Patofisiología Homeostasis Inflamación Dolor Fiebre Proliferación celular normal y patológica Estómago Intestino Riñón Plaquetas
 COX-2. (inducible) Patofisiología. Homeostasis. Inflamación. Dolor. Fiebre. Proliferación celular. normal y patológica. Estómago. Intestino. Riñón. Plaquetas.")
8
Patofisiología Homeostasis Acido araquidónico COXIB COX-1 COX-2
(constitutiva) COX-2 (inducible) Patofisiología Homeostasis Inflamación Dolor Fiebre Proliferación celular normal y patológica Estómago Intestino Riñón Plaquetas 8
 COX-2. (inducible) Patofisiología. Homeostasis. Inflamación. Dolor. Fiebre. Proliferación celular. normal y patológica. Estómago. Intestino. Riñón. Plaquetas. 8.")
9
Clasificación Derivados Acido Salicílico
ASPIRINA, SALICILATO DE LISINA, DIFLUNISAL, OLSALAZINA, SULFASALAZINA Derivados Paraaminofenol PARACETAMOL Derivados Pirazolona o pirazólicos METAMIZOL O DIPIRONA, PROPIFENAZONA Derivados Ácidoc. Propiónico IBUPROFENO, NAPROXENO, KETOPROFENO, FENOPROFENO, FLURBIPROFENO Derivados Ácido Acético INDOMETACINA, SULINDACO, KETOROLACO, DICLOFENACO, ACECLOFENACO Oxicams PIROXICAM, MELOXICAM Inhibidores selectivos COX-2 (Coxibs) CELECOXIB, ROFECOXIB
 CELECOXIB, ROFECOXIB.")
10
El paracetamol tiene poca o ninguna acción antiinflamatoria
Indometacina, ketorolaco y piroxican son los antiinflamatorios más potentes La aspirina tiene propiedades farmacológicas singulares Existen diferencias farmacocinéticas que justifican usos clínicos diferentes Diferencias importantes en toxicidad y tolerancia por el paciente

11
Actividad analgésica De intensidad moderada o media (inferior a opioides) pero sin alterar el sensorio o la percepción. Útiles en dolores asociados a inflamación o daño tisular Dosis normales: dismenorreas, dolores articulares, musculares, dentarios y cefaleas de diversa etiología Dosis más elevadas (o combinadas con opióides) eficaces en dolor postoperatorio y postraumático, ciertos cólicos y dolor cancerígeno en su primera etapa When employed as analgesic these drugs are effective only against pain of low-moderate intensity, such as dental pain. Although their maximal efficacy is generally much less than the opioids, NSAIDs lack the respiratory depression and the development of physical dependence. Chronic postoperative pain or pain arising from inflammation is controlled particularly well, whereas pain arising from the hollow viscera is usually no relieved. An exception to this is menstrual pain.
 eficaces en dolor postoperatorio y postraumático, ciertos cólicos y dolor cancerígeno en su primera etapa. When employed as analgesic these drugs are effective only against pain of low-moderate intensity, such as dental pain. Although their maximal efficacy is generally much less than the opioids, NSAIDs lack the respiratory depression and the development of physical dependence. Chronic postoperative pain or pain arising from inflammation is controlled particularly well, whereas pain arising from the hollow viscera is usually no relieved. An exception to this is menstrual pain.")
13
The 2007 Oxford league table of analgesic efficacy (at least 3 trials or 200 patients)Numbers needed to treat are calculated for the proportion of patients with at least 50% pain relief over 4-6 hours compared with placebo in randomised, double-blind, single-dose studies in patients with moderate to severe pain. Drugs were oral, unless specified, and doses are milligrams. Shaded rows are intramuscular administration. Understanding the league table Effective relief can be achieved with oral non-opioids and non-steroidal anti-inflammatory drugs. Analgesic efficacy is expressed as the NNT, the number of patients who need to receive the active drug for one to achieve at least 50% relief of pain compared with placebo over a 4-6 hour treatment period. The most effective drugs have a low NNT of just over 2. This means that for every two patients who receive the drug one patient will get at least 50% relief because of the treatment (the other patient may or may not obtain relief but it does not reach the 50% level). The NNT is treatment-specific, which is useful for comparison of relative efficacy. Because these NNT comparisons are against placebo, the best NNT of 2 means that 50 of 100 patients will get at least 50% relief specifically because of the treatment. Another twenty will have a placebo response giving them at least 50% relief. With ibuprofen 400 mg, therefore, about 70 of 100 in total will have effective pain relief. For comparison, with 10 mg intramuscular morphine about 53% of patients get more than 50% pain relief. Because the effect of placebo is added in, the comparisons between analgesics are not as stark as with NNT. It is clear that the oral NSAIDs do extremely well in this single-dose postoperative comparison. At these doses they all have NNT values of between 2 and 3, and the point estimate of the mean is below that of (i.e. better than) 10 mg of intramuscular morphine, even though the confidence intervals overlap. The simple analgesics, aspirin and paracetamol are significantly less effective than 10 mg intramuscular morphine. The point estimates of the NNT are higher, and there is no overlap of the confidence intervals. Weak opioids perform poorly in single doses on their own. Combining them with simple analgesics improves analgesic efficacy. Drawbacks of the league table The most important drawback is size. Small trials (or small data sets) cannot accurately estimate the magnitude of the analgesic effect. To know that the NNT of an analgesic is 3.0 with a confidence interval of 2.5 to 3.5 we need almost 1000 patients in a comparative trial. So as you contemplate the numbers, be conscious of the amount of information upon which NNTs and percent of patients with at least 50% pain relief are based. In practice any comparison with more than 250 or so patients is probably adequate. For instance, ibuprofen 800 mg is at the top of the league, with an NNT of 1.6 and with 100% of patients achieving at least 50% pain relief. But only 76 patients have ever been involved in comparative trials with placebo. This makes the apparent wonderful result less so, and you should treat it cautiously. The information is presented here, warts and all, so that professionals and public can make their own assessments. What is missing? Adverse effects from single-dose analgesic trials are rarely helpful with simple analgesics and NSAIDs, though they may be much more helpful with opioids. Work on adverse effects is being done, and a summary of this will appear on this site later in 1999. Some analgesics used commonly outside the UK may not be represented. Again work is ongoing to plug these gaps, but so often the randomised trials (placebo-controlled, randomised, double-blind and with proper outcome measures and entry criteria), have not been done. Finally cost information is not given here, because it can vary so much throughout the world.
. The NNT is treatment-specific, which is useful for comparison of relative efficacy. Because these NNT comparisons are against placebo, the best NNT of 2 means that 50 of 100 patients will get at least 50% relief specifically because of the treatment. Another twenty will have a placebo response giving them at least 50% relief. With ibuprofen 400 mg, therefore, about 70 of 100 in total will have effective pain relief. For comparison, with 10 mg intramuscular morphine about 53% of patients get more than 50% pain relief. Because the effect of placebo is added in, the comparisons between analgesics are not as stark as with NNT. It is clear that the oral NSAIDs do extremely well in this single-dose postoperative comparison. At these doses they all have NNT values of between 2 and 3, and the point estimate of the mean is below that of (i.e. better than) 10 mg of intramuscular morphine, even though the confidence intervals overlap. The simple analgesics, aspirin and paracetamol are significantly less effective than 10 mg intramuscular morphine. The point estimates of the NNT are higher, and there is no overlap of the confidence intervals. Weak opioids perform poorly in single doses on their own. Combining them with simple analgesics improves analgesic efficacy. Drawbacks of the league table. The most important drawback is size. Small trials (or small data sets) cannot accurately estimate the magnitude of the analgesic effect. To know that the NNT of an analgesic is 3.0 with a confidence interval of 2.5 to 3.5 we need almost 1000 patients in a comparative trial. So as you contemplate the numbers, be conscious of the amount of information upon which NNTs and percent of patients with at least 50% pain relief are based. In practice any comparison with more than 250 or so patients is probably adequate. For instance, ibuprofen 800 mg is at the top of the league, with an NNT of 1.6 and with 100% of patients achieving at least 50% pain relief. But only 76 patients have ever been involved in comparative trials with placebo. This makes the apparent wonderful result less so, and you should treat it cautiously. The information is presented here, warts and all, so that professionals and public can make their own assessments. What is missing Adverse effects from single-dose analgesic trials are rarely helpful with simple analgesics and NSAIDs, though they may be much more helpful with opioids. Work on adverse effects is being done, and a summary of this will appear on this site later in Some analgesics used commonly outside the UK may not be represented. Again work is ongoing to plug these gaps, but so often the randomised trials (placebo-controlled, randomised, double-blind and with proper outcome measures and entry criteria), have not been done. Finally cost information is not given here, because it can vary so much throughout the world.")
15
Ventas en España de AINE
Miles de Unidades en 2005 2 4 6 8 10 12 14 16 18 20 Ibup Diclo Aceclo Pirox Melox Naprox Keto Coxibs 15

16
Antiinflamatoria Se necesitan dosis más altas que las analgésicas (s/t en inflamación crónica) No hay tantas diferencias entre ellos como se piensa Mas eficaces en cuadros agudos que crónicos Important differences in adverse effects seem to exist between different NSAIDs. In contrast, their beneficial effects seem to be similar. The only metaanalysis that found one drug to be more effective than another was funded by the manufacturer; the studies it included were small and the result was not replicated in a large RCT. If the effect of one NSAID is not satisfactory, a switch to another NSAID cannot be expected to solve the problem. Likewise, doubling the dose of an NSAID leads to only a small increase in effect, which may not be clinically relevant. In acute musculoskeletal prob lems it is doubtful whether NSAIDs have any clinically relevant antiinflammatory effect; it is therefore unfor tunate that not one, large double blind RCT has com pared an NSAID with paracetamol. Paracetamol has been studied in osteoarthritis, where it had much the same effect as ibuprofen or naproxen.12 Clinical evidence. BMJ 2000, 320,

17
Antitérmica Disminuyen la temperatura elevada sin afectar la normal.
Reducen la producción de PGs (s/t PGE2) en el hipotálamo al inhibir la COX-2 ¿otros mecanismos responsables? (¿COX-3?; ¿existencia de otros mediadores?) La fiebre como mecanismo de alerta y defensa cumple una función adaptativa fisiológica y no debería ser siempre objeto de tratamiento
 en el hipotálamo al inhibir la COX-2. ¿otros mecanismos responsables (¿COX-3 ; ¿existencia de otros mediadores ) La fiebre como mecanismo de alerta y defensa cumple una función adaptativa fisiológica y no debería ser siempre objeto de tratamiento.")
18
Uricosúrica Inhiben el transporte del ácido úrico desde la luz del túbulo renal hasta el espacio intersticial Solo es apreciable con algunos AINES (dosis elevadas de salicilato, fenilbutazona y sulfinpirazona) Además útiles en el tratamiento del ataque de gota por su acción analgésica y antiinflamatoria.
 Además útiles en el tratamiento del ataque de gota por su acción analgésica y antiinflamatoria.")
19
Aspirina y salicilatos (5-asa)
También empleado como antiagregante plaquetario, prevención del cancer de colon, enfermedad de Alzheimer, reducción de la diarrea por radiación Inhibe la COX de forma irreversible Efectos adversos (s/t en niños o con dosis altas) Salicilismo (vértigo, disminución de la audición, vómitos y nauseas) Acidosis metabólica y respiratoria Dosis bajas interfieren con la eliminación de acd. úrico y pueden interaccionar con la medicación de la gota Evitar consumo durante el ultimo trimestre del embarazo
 Salicilismo (vértigo, disminución de la audición, vómitos y nauseas) Acidosis metabólica y respiratoria. Dosis bajas interfieren con la eliminación de acd. úrico y pueden interaccionar con la medicación de la gota. Evitar consumo durante el ultimo trimestre del embarazo.")
20
The 2007 Oxford league table of analgesic efficacy (at least 3 trials or 200 patients)Numbers needed to treat are calculated for the proportion of patients with at least 50% pain relief over 4-6 hours compared with placebo in randomised, double-blind, single-dose studies in patients with moderate to severe pain. Drugs were oral, unless specified, and doses are milligrams. Shaded rows are intramuscular administration. Understanding the league table Effective relief can be achieved with oral non-opioids and non-steroidal anti-inflammatory drugs. Analgesic efficacy is expressed as the NNT, the number of patients who need to receive the active drug for one to achieve at least 50% relief of pain compared with placebo over a 4-6 hour treatment period. The most effective drugs have a low NNT of just over 2. This means that for every two patients who receive the drug one patient will get at least 50% relief because of the treatment (the other patient may or may not obtain relief but it does not reach the 50% level). The NNT is treatment-specific, which is useful for comparison of relative efficacy. Because these NNT comparisons are against placebo, the best NNT of 2 means that 50 of 100 patients will get at least 50% relief specifically because of the treatment. Another twenty will have a placebo response giving them at least 50% relief. With ibuprofen 400 mg, therefore, about 70 of 100 in total will have effective pain relief. For comparison, with 10 mg intramuscular morphine about 53% of patients get more than 50% pain relief. Because the effect of placebo is added in, the comparisons between analgesics are not as stark as with NNT. It is clear that the oral NSAIDs do extremely well in this single-dose postoperative comparison. At these doses they all have NNT values of between 2 and 3, and the point estimate of the mean is below that of (i.e. better than) 10 mg of intramuscular morphine, even though the confidence intervals overlap. The simple analgesics, aspirin and paracetamol are significantly less effective than 10 mg intramuscular morphine. The point estimates of the NNT are higher, and there is no overlap of the confidence intervals. Weak opioids perform poorly in single doses on their own. Combining them with simple analgesics improves analgesic efficacy. Drawbacks of the league table The most important drawback is size. Small trials (or small data sets) cannot accurately estimate the magnitude of the analgesic effect. To know that the NNT of an analgesic is 3.0 with a confidence interval of 2.5 to 3.5 we need almost 1000 patients in a comparative trial. So as you contemplate the numbers, be conscious of the amount of information upon which NNTs and percent of patients with at least 50% pain relief are based. In practice any comparison with more than 250 or so patients is probably adequate. For instance, ibuprofen 800 mg is at the top of the league, with an NNT of 1.6 and with 100% of patients achieving at least 50% pain relief. But only 76 patients have ever been involved in comparative trials with placebo. This makes the apparent wonderful result less so, and you should treat it cautiously. The information is presented here, warts and all, so that professionals and public can make their own assessments. What is missing? Adverse effects from single-dose analgesic trials are rarely helpful with simple analgesics and NSAIDs, though they may be much more helpful with opioids. Work on adverse effects is being done, and a summary of this will appear on this site later in 1999. Some analgesics used commonly outside the UK may not be represented. Again work is ongoing to plug these gaps, but so often the randomised trials (placebo-controlled, randomised, double-blind and with proper outcome measures and entry criteria), have not been done. Finally cost information is not given here, because it can vary so much throughout the world.
. The NNT is treatment-specific, which is useful for comparison of relative efficacy. Because these NNT comparisons are against placebo, the best NNT of 2 means that 50 of 100 patients will get at least 50% relief specifically because of the treatment. Another twenty will have a placebo response giving them at least 50% relief. With ibuprofen 400 mg, therefore, about 70 of 100 in total will have effective pain relief. For comparison, with 10 mg intramuscular morphine about 53% of patients get more than 50% pain relief. Because the effect of placebo is added in, the comparisons between analgesics are not as stark as with NNT. It is clear that the oral NSAIDs do extremely well in this single-dose postoperative comparison. At these doses they all have NNT values of between 2 and 3, and the point estimate of the mean is below that of (i.e. better than) 10 mg of intramuscular morphine, even though the confidence intervals overlap. The simple analgesics, aspirin and paracetamol are significantly less effective than 10 mg intramuscular morphine. The point estimates of the NNT are higher, and there is no overlap of the confidence intervals. Weak opioids perform poorly in single doses on their own. Combining them with simple analgesics improves analgesic efficacy. Drawbacks of the league table. The most important drawback is size. Small trials (or small data sets) cannot accurately estimate the magnitude of the analgesic effect. To know that the NNT of an analgesic is 3.0 with a confidence interval of 2.5 to 3.5 we need almost 1000 patients in a comparative trial. So as you contemplate the numbers, be conscious of the amount of information upon which NNTs and percent of patients with at least 50% pain relief are based. In practice any comparison with more than 250 or so patients is probably adequate. For instance, ibuprofen 800 mg is at the top of the league, with an NNT of 1.6 and with 100% of patients achieving at least 50% pain relief. But only 76 patients have ever been involved in comparative trials with placebo. This makes the apparent wonderful result less so, and you should treat it cautiously. The information is presented here, warts and all, so that professionals and public can make their own assessments. What is missing Adverse effects from single-dose analgesic trials are rarely helpful with simple analgesics and NSAIDs, though they may be much more helpful with opioids. Work on adverse effects is being done, and a summary of this will appear on this site later in Some analgesics used commonly outside the UK may not be represented. Again work is ongoing to plug these gaps, but so often the randomised trials (placebo-controlled, randomised, double-blind and with proper outcome measures and entry criteria), have not been done. Finally cost information is not given here, because it can vary so much throughout the world.")
21
Paracetamol (acetaminofeno)
Equiparable a los otros AINEs como analgésico y antipirético, pero no tiene casi efecto antiinflamatorio y es menos eficaz en dolores de tipo inflamatorio ¿Inhibidor de COX-3?- ¿inactivado en tejido inflamado? De elección en niños (Síndrome de Reye) Farmacocinética Vida media de 2-4 h pero con dosis tóxicas puede aumentar a 4-8 h por suturar los mecanismos de metabolización Efectos adversos (s/t en niños o con dosis altas) A dosis terapéuticas uno de los AINES más seguros Dosis altas mantenidas relacionadas con daño renal Dosis tóxica (2-3 veces la terapéutica) hepatotoxicidad seria
 Farmacocinética. Vida media de 2-4 h pero con dosis tóxicas puede aumentar a 4-8 h por suturar los mecanismos de metabolización. Efectos adversos (s/t en niños o con dosis altas) A dosis terapéuticas uno de los AINES más seguros. Dosis altas mantenidas relacionadas con daño renal. Dosis tóxica (2-3 veces la terapéutica) hepatotoxicidad seria.")
22
The 2007 Oxford league table of analgesic efficacy (at least 3 trials or 200 patients)Numbers needed to treat are calculated for the proportion of patients with at least 50% pain relief over 4-6 hours compared with placebo in randomised, double-blind, single-dose studies in patients with moderate to severe pain. Drugs were oral, unless specified, and doses are milligrams. Shaded rows are intramuscular administration. Understanding the league table Effective relief can be achieved with oral non-opioids and non-steroidal anti-inflammatory drugs. Analgesic efficacy is expressed as the NNT, the number of patients who need to receive the active drug for one to achieve at least 50% relief of pain compared with placebo over a 4-6 hour treatment period. The most effective drugs have a low NNT of just over 2. This means that for every two patients who receive the drug one patient will get at least 50% relief because of the treatment (the other patient may or may not obtain relief but it does not reach the 50% level). The NNT is treatment-specific, which is useful for comparison of relative efficacy. Because these NNT comparisons are against placebo, the best NNT of 2 means that 50 of 100 patients will get at least 50% relief specifically because of the treatment. Another twenty will have a placebo response giving them at least 50% relief. With ibuprofen 400 mg, therefore, about 70 of 100 in total will have effective pain relief. For comparison, with 10 mg intramuscular morphine about 53% of patients get more than 50% pain relief. Because the effect of placebo is added in, the comparisons between analgesics are not as stark as with NNT. It is clear that the oral NSAIDs do extremely well in this single-dose postoperative comparison. At these doses they all have NNT values of between 2 and 3, and the point estimate of the mean is below that of (i.e. better than) 10 mg of intramuscular morphine, even though the confidence intervals overlap. The simple analgesics, aspirin and paracetamol are significantly less effective than 10 mg intramuscular morphine. The point estimates of the NNT are higher, and there is no overlap of the confidence intervals. Weak opioids perform poorly in single doses on their own. Combining them with simple analgesics improves analgesic efficacy. Drawbacks of the league table The most important drawback is size. Small trials (or small data sets) cannot accurately estimate the magnitude of the analgesic effect. To know that the NNT of an analgesic is 3.0 with a confidence interval of 2.5 to 3.5 we need almost 1000 patients in a comparative trial. So as you contemplate the numbers, be conscious of the amount of information upon which NNTs and percent of patients with at least 50% pain relief are based. In practice any comparison with more than 250 or so patients is probably adequate. For instance, ibuprofen 800 mg is at the top of the league, with an NNT of 1.6 and with 100% of patients achieving at least 50% pain relief. But only 76 patients have ever been involved in comparative trials with placebo. This makes the apparent wonderful result less so, and you should treat it cautiously. The information is presented here, warts and all, so that professionals and public can make their own assessments. What is missing? Adverse effects from single-dose analgesic trials are rarely helpful with simple analgesics and NSAIDs, though they may be much more helpful with opioids. Work on adverse effects is being done, and a summary of this will appear on this site later in 1999. Some analgesics used commonly outside the UK may not be represented. Again work is ongoing to plug these gaps, but so often the randomised trials (placebo-controlled, randomised, double-blind and with proper outcome measures and entry criteria), have not been done. Finally cost information is not given here, because it can vary so much throughout the world.
. The NNT is treatment-specific, which is useful for comparison of relative efficacy. Because these NNT comparisons are against placebo, the best NNT of 2 means that 50 of 100 patients will get at least 50% relief specifically because of the treatment. Another twenty will have a placebo response giving them at least 50% relief. With ibuprofen 400 mg, therefore, about 70 of 100 in total will have effective pain relief. For comparison, with 10 mg intramuscular morphine about 53% of patients get more than 50% pain relief. Because the effect of placebo is added in, the comparisons between analgesics are not as stark as with NNT. It is clear that the oral NSAIDs do extremely well in this single-dose postoperative comparison. At these doses they all have NNT values of between 2 and 3, and the point estimate of the mean is below that of (i.e. better than) 10 mg of intramuscular morphine, even though the confidence intervals overlap. The simple analgesics, aspirin and paracetamol are significantly less effective than 10 mg intramuscular morphine. The point estimates of the NNT are higher, and there is no overlap of the confidence intervals. Weak opioids perform poorly in single doses on their own. Combining them with simple analgesics improves analgesic efficacy. Drawbacks of the league table. The most important drawback is size. Small trials (or small data sets) cannot accurately estimate the magnitude of the analgesic effect. To know that the NNT of an analgesic is 3.0 with a confidence interval of 2.5 to 3.5 we need almost 1000 patients in a comparative trial. So as you contemplate the numbers, be conscious of the amount of information upon which NNTs and percent of patients with at least 50% pain relief are based. In practice any comparison with more than 250 or so patients is probably adequate. For instance, ibuprofen 800 mg is at the top of the league, with an NNT of 1.6 and with 100% of patients achieving at least 50% pain relief. But only 76 patients have ever been involved in comparative trials with placebo. This makes the apparent wonderful result less so, and you should treat it cautiously. The information is presented here, warts and all, so that professionals and public can make their own assessments. What is missing Adverse effects from single-dose analgesic trials are rarely helpful with simple analgesics and NSAIDs, though they may be much more helpful with opioids. Work on adverse effects is being done, and a summary of this will appear on this site later in Some analgesics used commonly outside the UK may not be represented. Again work is ongoing to plug these gaps, but so often the randomised trials (placebo-controlled, randomised, double-blind and with proper outcome measures and entry criteria), have not been done. Finally cost information is not given here, because it can vary so much throughout the world.")
23
Derivados Pirazolona o pirazólicos
S/T analgésicos y antitérmicos. Eficacia similar a AAS y morfina a dosis bajas. Relaja algo la fibra lisa por lo que se emplea en dolores de tipo cólico solo o asociado a espasmolíticos o anticolinérgicos. Menos gastrolesivo y riesgo de agranulocitosis bajo (aunque superior al de cualquier otros AINE). Riesgo mayor en mujer y con la edad. Muy utilizados en asociación con otros fármacos METAMIZOL, PROPIFENAZONA
. Riesgo mayor en mujer y con la edad. Muy utilizados en asociación con otros fármacos. METAMIZOL, PROPIFENAZONA.")
24
Derivados Ac. Propiónico
Eficacia moderada con poca incidencia de efectos adversos (s/t gastrointestinales). Interfieren con la acción antiagregante del AAS. Se eliminan poco por leche (~ 1%), de elección para madres lactando Dispares químicamente y en su farmacocinética, pero con una actuación farmacológica homogénea y un perfil similar de efectos adversos IBUPROFENO, NAPROXENO, KETOPROFENO, FENOPROFENO, FLURBIPROFENO
. Interfieren con la acción antiagregante del AAS. Se eliminan poco por leche (~ 1%), de elección para madres lactando. Dispares químicamente y en su farmacocinética, pero con una actuación farmacológica homogénea y un perfil similar de efectos adversos. IBUPROFENO, NAPROXENO, KETOPROFENO, FENOPROFENO, FLURBIPROFENO.")
25
The 2007 Oxford league table of analgesic efficacy (at least 3 trials or 200 patients)Numbers needed to treat are calculated for the proportion of patients with at least 50% pain relief over 4-6 hours compared with placebo in randomised, double-blind, single-dose studies in patients with moderate to severe pain. Drugs were oral, unless specified, and doses are milligrams. Shaded rows are intramuscular administration. Understanding the league table Effective relief can be achieved with oral non-opioids and non-steroidal anti-inflammatory drugs. Analgesic efficacy is expressed as the NNT, the number of patients who need to receive the active drug for one to achieve at least 50% relief of pain compared with placebo over a 4-6 hour treatment period. The most effective drugs have a low NNT of just over 2. This means that for every two patients who receive the drug one patient will get at least 50% relief because of the treatment (the other patient may or may not obtain relief but it does not reach the 50% level). The NNT is treatment-specific, which is useful for comparison of relative efficacy. Because these NNT comparisons are against placebo, the best NNT of 2 means that 50 of 100 patients will get at least 50% relief specifically because of the treatment. Another twenty will have a placebo response giving them at least 50% relief. With ibuprofen 400 mg, therefore, about 70 of 100 in total will have effective pain relief. For comparison, with 10 mg intramuscular morphine about 53% of patients get more than 50% pain relief. Because the effect of placebo is added in, the comparisons between analgesics are not as stark as with NNT. It is clear that the oral NSAIDs do extremely well in this single-dose postoperative comparison. At these doses they all have NNT values of between 2 and 3, and the point estimate of the mean is below that of (i.e. better than) 10 mg of intramuscular morphine, even though the confidence intervals overlap. The simple analgesics, aspirin and paracetamol are significantly less effective than 10 mg intramuscular morphine. The point estimates of the NNT are higher, and there is no overlap of the confidence intervals. Weak opioids perform poorly in single doses on their own. Combining them with simple analgesics improves analgesic efficacy. Drawbacks of the league table The most important drawback is size. Small trials (or small data sets) cannot accurately estimate the magnitude of the analgesic effect. To know that the NNT of an analgesic is 3.0 with a confidence interval of 2.5 to 3.5 we need almost 1000 patients in a comparative trial. So as you contemplate the numbers, be conscious of the amount of information upon which NNTs and percent of patients with at least 50% pain relief are based. In practice any comparison with more than 250 or so patients is probably adequate. For instance, ibuprofen 800 mg is at the top of the league, with an NNT of 1.6 and with 100% of patients achieving at least 50% pain relief. But only 76 patients have ever been involved in comparative trials with placebo. This makes the apparent wonderful result less so, and you should treat it cautiously. The information is presented here, warts and all, so that professionals and public can make their own assessments. What is missing? Adverse effects from single-dose analgesic trials are rarely helpful with simple analgesics and NSAIDs, though they may be much more helpful with opioids. Work on adverse effects is being done, and a summary of this will appear on this site later in 1999. Some analgesics used commonly outside the UK may not be represented. Again work is ongoing to plug these gaps, but so often the randomised trials (placebo-controlled, randomised, double-blind and with proper outcome measures and entry criteria), have not been done. Finally cost information is not given here, because it can vary so much throughout the world.
. The NNT is treatment-specific, which is useful for comparison of relative efficacy. Because these NNT comparisons are against placebo, the best NNT of 2 means that 50 of 100 patients will get at least 50% relief specifically because of the treatment. Another twenty will have a placebo response giving them at least 50% relief. With ibuprofen 400 mg, therefore, about 70 of 100 in total will have effective pain relief. For comparison, with 10 mg intramuscular morphine about 53% of patients get more than 50% pain relief. Because the effect of placebo is added in, the comparisons between analgesics are not as stark as with NNT. It is clear that the oral NSAIDs do extremely well in this single-dose postoperative comparison. At these doses they all have NNT values of between 2 and 3, and the point estimate of the mean is below that of (i.e. better than) 10 mg of intramuscular morphine, even though the confidence intervals overlap. The simple analgesics, aspirin and paracetamol are significantly less effective than 10 mg intramuscular morphine. The point estimates of the NNT are higher, and there is no overlap of the confidence intervals. Weak opioids perform poorly in single doses on their own. Combining them with simple analgesics improves analgesic efficacy. Drawbacks of the league table. The most important drawback is size. Small trials (or small data sets) cannot accurately estimate the magnitude of the analgesic effect. To know that the NNT of an analgesic is 3.0 with a confidence interval of 2.5 to 3.5 we need almost 1000 patients in a comparative trial. So as you contemplate the numbers, be conscious of the amount of information upon which NNTs and percent of patients with at least 50% pain relief are based. In practice any comparison with more than 250 or so patients is probably adequate. For instance, ibuprofen 800 mg is at the top of the league, with an NNT of 1.6 and with 100% of patients achieving at least 50% pain relief. But only 76 patients have ever been involved in comparative trials with placebo. This makes the apparent wonderful result less so, and you should treat it cautiously. The information is presented here, warts and all, so that professionals and public can make their own assessments. What is missing Adverse effects from single-dose analgesic trials are rarely helpful with simple analgesics and NSAIDs, though they may be much more helpful with opioids. Work on adverse effects is being done, and a summary of this will appear on this site later in Some analgesics used commonly outside the UK may not be represented. Again work is ongoing to plug these gaps, but so often the randomised trials (placebo-controlled, randomised, double-blind and with proper outcome measures and entry criteria), have not been done. Finally cost information is not given here, because it can vary so much throughout the world.")
26
Derivados Acido Acético (I)
Fármacos con actividad analgésica, antitérmica y antiinflamatoria potente Indometacina Muy potente (>20 veces aspirina) Especial tratamiento de procesos artríticos por su gran eficacia, pero muchos efectos adversos (30-35%, dosis -dependientes): digestivos, SNC Sulindaco Potencia 50% de la Indometacina Menor toxicidad La indo inhibe mas la COX que la aspirina pero tiene alto nivel de intolerancia. Es aroximadamente 20 veces mas potente que asprina para tratar alteraciones de la artritis reumatoide
 Especial tratamiento de procesos artríticos por su gran eficacia, pero muchos efectos adversos (30-35%, dosis -dependientes): digestivos, SNC. Sulindaco. Potencia 50% de la Indometacina. Menor toxicidad. La indo inhibe mas la COX que la aspirina pero tiene alto nivel de intolerancia. Es aroximadamente 20 veces mas potente que asprina para tratar alteraciones de la artritis reumatoide.")
27
Derivados Acido Acético (II)
Ketorolaco Gran componente analgésico además de antiinflamatorio 30 mg (i.m.) eficacia comparable a 10 mg de morfina, pero a diferencia de esta la acción analgésica apenas aumenta a dosis superiores No se debe utilizar de rutina como analgésico, solo cuando exista un gran dolor (cólico nefrítico) y/o tenga un importante componente inflamatorio, y siempre durante pocos días El más gastrolesivo Uno de los pocos AINE adecuados para administración parenteral y con vida media larga 27
 eficacia comparable a 10 mg de morfina, pero a diferencia de esta la acción analgésica apenas aumenta a dosis superiores. No se debe utilizar de rutina como analgésico, solo cuando exista un gran dolor (cólico nefrítico) y/o tenga un importante componente inflamatorio, y siempre durante pocos días. El más gastrolesivo. Uno de los pocos AINE adecuados para administración parenteral y con vida media larga. 27.")
28
Derivados Acido Acético (III)
Diclofenaco y aceclofenaco Es un COXIB El diclofenaco a dosis habituales interfiere menos en la agregación plaquetaria que la mayoría de los AINES y es uricosúrico Se acumula en el liquido sinovial Interfiere menos con la acción antiagregante de la aspirina Amplio espectro: desde tratamiento agudo de la artritis reumatoide y artrosis hasta dolor agudo por procesos inflamatorios no reumáticos o la dismenorrea primaria Reacciones adversas similares a los derivados del ácido Propiónico 28

29
The 2007 Oxford league table of analgesic efficacy (at least 3 trials or 200 patients)Numbers needed to treat are calculated for the proportion of patients with at least 50% pain relief over 4-6 hours compared with placebo in randomised, double-blind, single-dose studies in patients with moderate to severe pain. Drugs were oral, unless specified, and doses are milligrams. Shaded rows are intramuscular administration. Understanding the league table Effective relief can be achieved with oral non-opioids and non-steroidal anti-inflammatory drugs. Analgesic efficacy is expressed as the NNT, the number of patients who need to receive the active drug for one to achieve at least 50% relief of pain compared with placebo over a 4-6 hour treatment period. The most effective drugs have a low NNT of just over 2. This means that for every two patients who receive the drug one patient will get at least 50% relief because of the treatment (the other patient may or may not obtain relief but it does not reach the 50% level). The NNT is treatment-specific, which is useful for comparison of relative efficacy. Because these NNT comparisons are against placebo, the best NNT of 2 means that 50 of 100 patients will get at least 50% relief specifically because of the treatment. Another twenty will have a placebo response giving them at least 50% relief. With ibuprofen 400 mg, therefore, about 70 of 100 in total will have effective pain relief. For comparison, with 10 mg intramuscular morphine about 53% of patients get more than 50% pain relief. Because the effect of placebo is added in, the comparisons between analgesics are not as stark as with NNT. It is clear that the oral NSAIDs do extremely well in this single-dose postoperative comparison. At these doses they all have NNT values of between 2 and 3, and the point estimate of the mean is below that of (i.e. better than) 10 mg of intramuscular morphine, even though the confidence intervals overlap. The simple analgesics, aspirin and paracetamol are significantly less effective than 10 mg intramuscular morphine. The point estimates of the NNT are higher, and there is no overlap of the confidence intervals. Weak opioids perform poorly in single doses on their own. Combining them with simple analgesics improves analgesic efficacy. Drawbacks of the league table The most important drawback is size. Small trials (or small data sets) cannot accurately estimate the magnitude of the analgesic effect. To know that the NNT of an analgesic is 3.0 with a confidence interval of 2.5 to 3.5 we need almost 1000 patients in a comparative trial. So as you contemplate the numbers, be conscious of the amount of information upon which NNTs and percent of patients with at least 50% pain relief are based. In practice any comparison with more than 250 or so patients is probably adequate. For instance, ibuprofen 800 mg is at the top of the league, with an NNT of 1.6 and with 100% of patients achieving at least 50% pain relief. But only 76 patients have ever been involved in comparative trials with placebo. This makes the apparent wonderful result less so, and you should treat it cautiously. The information is presented here, warts and all, so that professionals and public can make their own assessments. What is missing? Adverse effects from single-dose analgesic trials are rarely helpful with simple analgesics and NSAIDs, though they may be much more helpful with opioids. Work on adverse effects is being done, and a summary of this will appear on this site later in 1999. Some analgesics used commonly outside the UK may not be represented. Again work is ongoing to plug these gaps, but so often the randomised trials (placebo-controlled, randomised, double-blind and with proper outcome measures and entry criteria), have not been done. Finally cost information is not given here, because it can vary so much throughout the world.
. The NNT is treatment-specific, which is useful for comparison of relative efficacy. Because these NNT comparisons are against placebo, the best NNT of 2 means that 50 of 100 patients will get at least 50% relief specifically because of the treatment. Another twenty will have a placebo response giving them at least 50% relief. With ibuprofen 400 mg, therefore, about 70 of 100 in total will have effective pain relief. For comparison, with 10 mg intramuscular morphine about 53% of patients get more than 50% pain relief. Because the effect of placebo is added in, the comparisons between analgesics are not as stark as with NNT. It is clear that the oral NSAIDs do extremely well in this single-dose postoperative comparison. At these doses they all have NNT values of between 2 and 3, and the point estimate of the mean is below that of (i.e. better than) 10 mg of intramuscular morphine, even though the confidence intervals overlap. The simple analgesics, aspirin and paracetamol are significantly less effective than 10 mg intramuscular morphine. The point estimates of the NNT are higher, and there is no overlap of the confidence intervals. Weak opioids perform poorly in single doses on their own. Combining them with simple analgesics improves analgesic efficacy. Drawbacks of the league table. The most important drawback is size. Small trials (or small data sets) cannot accurately estimate the magnitude of the analgesic effect. To know that the NNT of an analgesic is 3.0 with a confidence interval of 2.5 to 3.5 we need almost 1000 patients in a comparative trial. So as you contemplate the numbers, be conscious of the amount of information upon which NNTs and percent of patients with at least 50% pain relief are based. In practice any comparison with more than 250 or so patients is probably adequate. For instance, ibuprofen 800 mg is at the top of the league, with an NNT of 1.6 and with 100% of patients achieving at least 50% pain relief. But only 76 patients have ever been involved in comparative trials with placebo. This makes the apparent wonderful result less so, and you should treat it cautiously. The information is presented here, warts and all, so that professionals and public can make their own assessments. What is missing Adverse effects from single-dose analgesic trials are rarely helpful with simple analgesics and NSAIDs, though they may be much more helpful with opioids. Work on adverse effects is being done, and a summary of this will appear on this site later in Some analgesics used commonly outside the UK may not be represented. Again work is ongoing to plug these gaps, but so often the randomised trials (placebo-controlled, randomised, double-blind and with proper outcome measures and entry criteria), have not been done. Finally cost information is not given here, because it can vary so much throughout the world.")
30
Inhibidores de la COX-2 Efectivos como antiartríticos y en el control del dolor de la dismenorrea, o el posquirúrgico o dental Menos toxicidad gastrointestinal (50-60% reducción), SÍ dispepsia No antiagregante plaquetario ni uricosúrico, pero disminuyen (como los demás AINES) la filtración glomerular en ancianos Aumentan el riesgo de problemas cardiovasculares e incrementan la presión arterial cuando hay una función renal comprometida Ni por eficacia ni por precio esta justificado su uso en situaciones banales, en pacientes jóvenes o en los que no tengan riesgo de desarrollar complicaciones gastrointestinales
, SÍ dispepsia. No antiagregante plaquetario ni uricosúrico, pero disminuyen (como los demás AINES) la filtración glomerular en ancianos. Aumentan el riesgo de problemas cardiovasculares e incrementan la presión arterial cuando hay una función renal comprometida. Ni por eficacia ni por precio esta justificado su uso en situaciones banales, en pacientes jóvenes o en los que no tengan riesgo de desarrollar complicaciones gastrointestinales.")
31
The 2007 Oxford league table of analgesic efficacy (at least 3 trials or 200 patients)Numbers needed to treat are calculated for the proportion of patients with at least 50% pain relief over 4-6 hours compared with placebo in randomised, double-blind, single-dose studies in patients with moderate to severe pain. Drugs were oral, unless specified, and doses are milligrams. Shaded rows are intramuscular administration. Understanding the league table Effective relief can be achieved with oral non-opioids and non-steroidal anti-inflammatory drugs. Analgesic efficacy is expressed as the NNT, the number of patients who need to receive the active drug for one to achieve at least 50% relief of pain compared with placebo over a 4-6 hour treatment period. The most effective drugs have a low NNT of just over 2. This means that for every two patients who receive the drug one patient will get at least 50% relief because of the treatment (the other patient may or may not obtain relief but it does not reach the 50% level). The NNT is treatment-specific, which is useful for comparison of relative efficacy. Because these NNT comparisons are against placebo, the best NNT of 2 means that 50 of 100 patients will get at least 50% relief specifically because of the treatment. Another twenty will have a placebo response giving them at least 50% relief. With ibuprofen 400 mg, therefore, about 70 of 100 in total will have effective pain relief. For comparison, with 10 mg intramuscular morphine about 53% of patients get more than 50% pain relief. Because the effect of placebo is added in, the comparisons between analgesics are not as stark as with NNT. It is clear that the oral NSAIDs do extremely well in this single-dose postoperative comparison. At these doses they all have NNT values of between 2 and 3, and the point estimate of the mean is below that of (i.e. better than) 10 mg of intramuscular morphine, even though the confidence intervals overlap. The simple analgesics, aspirin and paracetamol are significantly less effective than 10 mg intramuscular morphine. The point estimates of the NNT are higher, and there is no overlap of the confidence intervals. Weak opioids perform poorly in single doses on their own. Combining them with simple analgesics improves analgesic efficacy. Drawbacks of the league table The most important drawback is size. Small trials (or small data sets) cannot accurately estimate the magnitude of the analgesic effect. To know that the NNT of an analgesic is 3.0 with a confidence interval of 2.5 to 3.5 we need almost 1000 patients in a comparative trial. So as you contemplate the numbers, be conscious of the amount of information upon which NNTs and percent of patients with at least 50% pain relief are based. In practice any comparison with more than 250 or so patients is probably adequate. For instance, ibuprofen 800 mg is at the top of the league, with an NNT of 1.6 and with 100% of patients achieving at least 50% pain relief. But only 76 patients have ever been involved in comparative trials with placebo. This makes the apparent wonderful result less so, and you should treat it cautiously. The information is presented here, warts and all, so that professionals and public can make their own assessments. What is missing? Adverse effects from single-dose analgesic trials are rarely helpful with simple analgesics and NSAIDs, though they may be much more helpful with opioids. Work on adverse effects is being done, and a summary of this will appear on this site later in 1999. Some analgesics used commonly outside the UK may not be represented. Again work is ongoing to plug these gaps, but so often the randomised trials (placebo-controlled, randomised, double-blind and with proper outcome measures and entry criteria), have not been done. Finally cost information is not given here, because it can vary so much throughout the world.
. The NNT is treatment-specific, which is useful for comparison of relative efficacy. Because these NNT comparisons are against placebo, the best NNT of 2 means that 50 of 100 patients will get at least 50% relief specifically because of the treatment. Another twenty will have a placebo response giving them at least 50% relief. With ibuprofen 400 mg, therefore, about 70 of 100 in total will have effective pain relief. For comparison, with 10 mg intramuscular morphine about 53% of patients get more than 50% pain relief. Because the effect of placebo is added in, the comparisons between analgesics are not as stark as with NNT. It is clear that the oral NSAIDs do extremely well in this single-dose postoperative comparison. At these doses they all have NNT values of between 2 and 3, and the point estimate of the mean is below that of (i.e. better than) 10 mg of intramuscular morphine, even though the confidence intervals overlap. The simple analgesics, aspirin and paracetamol are significantly less effective than 10 mg intramuscular morphine. The point estimates of the NNT are higher, and there is no overlap of the confidence intervals. Weak opioids perform poorly in single doses on their own. Combining them with simple analgesics improves analgesic efficacy. Drawbacks of the league table. The most important drawback is size. Small trials (or small data sets) cannot accurately estimate the magnitude of the analgesic effect. To know that the NNT of an analgesic is 3.0 with a confidence interval of 2.5 to 3.5 we need almost 1000 patients in a comparative trial. So as you contemplate the numbers, be conscious of the amount of information upon which NNTs and percent of patients with at least 50% pain relief are based. In practice any comparison with more than 250 or so patients is probably adequate. For instance, ibuprofen 800 mg is at the top of the league, with an NNT of 1.6 and with 100% of patients achieving at least 50% pain relief. But only 76 patients have ever been involved in comparative trials with placebo. This makes the apparent wonderful result less so, and you should treat it cautiously. The information is presented here, warts and all, so that professionals and public can make their own assessments. What is missing Adverse effects from single-dose analgesic trials are rarely helpful with simple analgesics and NSAIDs, though they may be much more helpful with opioids. Work on adverse effects is being done, and a summary of this will appear on this site later in Some analgesics used commonly outside the UK may not be represented. Again work is ongoing to plug these gaps, but so often the randomised trials (placebo-controlled, randomised, double-blind and with proper outcome measures and entry criteria), have not been done. Finally cost information is not given here, because it can vary so much throughout the world.")
32
Ventas en España de AINE
Miles de Unidades en 2005 2 4 6 8 10 12 14 16 18 20 Ibup Diclo Aceclo Pirox Melox Naprox Keto Coxibs 32

33
Lesiones digestivas por los Aine
Los AINE clásicos representan el 20-25% de todos los efectos adversos reportados por fármacos Hazleman 1989; Wolfe et al 1986 Lesiones digestivas por los Aine

34
Reducción de la función renal (no en sujeto normal)
Retención hidrosalina (hiperpotasemía, hiperuricemia) Empeoramiento función renal en pacientes renales, cardíacos o cirróticos Disminución efectividad antihipertensivos y diuréticos Consumo crónico: nefropatía analgésica HIPERSENSIBILIDAD Cruzada Reacciones de hipersensibilidad (1-2%, rinitis, edema angioneurótico, urticaria y asma (10%) Alteraciones cutaneas (rash, fotosensivilidad, urticaria,...) son las segundas mas frecuentes s/t con ac. mefenámico y sulindaco nefropatía analgésica:fallo renal progresivo asociado a un consumo de dosis altas de AINEs e infecciones urinarias reiteradas. Si se diagnostica pronto y se retiran los AINE la función renal puede normalizarse 34
 Empeoramiento función renal en pacientes renales, cardíacos o cirróticos. Disminución efectividad antihipertensivos y diuréticos. Consumo crónico: nefropatía analgésica. HIPERSENSIBILIDAD. Cruzada. Reacciones de hipersensibilidad (1-2%, rinitis, edema angioneurótico, urticaria y asma (10%) Alteraciones cutaneas (rash, fotosensivilidad, urticaria,...) son las segundas mas frecuentes s/t con ac. mefenámico y sulindaco. nefropatía analgésica:fallo renal progresivo asociado a un consumo de dosis altas de AINEs e infecciones urinarias reiteradas. Si se diagnostica pronto y se retiran los AINE la función renal puede normalizarse. 34.")
35
Elevación transaminasas (15%)
HEPÁTICO Elevación transaminasas (15%) Insuficiencia hepática fulminante (s/t coincidente con insf. Renal) OTROS Exacerbación de la HTA (26-50%), angina e insuficiencia cardíaca congestiva. (Disminución efectividad antihipertensivos y diuréticos) Reacciones hematológicas (raras pero graves) Hemorragias e interacción con anticoagulantes (actuación sobre las plaquetas) SNC: cefalea, umbral convulsiones Hiperventilación Cierre ductus arterioso 35
 Insuficiencia hepática fulminante (s/t coincidente con insf. Renal) OTROS. Exacerbación de la HTA (26-50%), angina e insuficiencia cardíaca congestiva. (Disminución efectividad antihipertensivos y diuréticos) Reacciones hematológicas (raras pero graves) Hemorragias e interacción con anticoagulantes (actuación sobre las plaquetas) SNC: cefalea, umbral convulsiones. Hiperventilación. Cierre ductus arterioso. 35.")
36
Sindrome de Reye Cuadro de aparición rápida asociada al uso de aspirina en menores de 20 años con fiebre de origen viral. Cursa con encefalopatía, disfunción hepática e infiltración grasa del hígado y otros órganos. Origen y mecanismo desconocido pero aociado al uso de aspirina. Se debe utilizar paracetamol

37
Aumento de riesgo cardiovascular con los COXIBS

38
Embarazo y lactancia No recomendados
Los niveles de Pg aumentan durante el embarazo pero los AINE no son recomendados como tocolíticos por cerrar el ductus arterioso y dificultar la circulación uterina, sobre todo a partir de las 32 semanas. Pueden aumentar el riesgo de sangrados postparto.

39
Ibuprofeno y otros AINE
FDA.- Seguridad de los AINE para el feto Riesgo aumentado con AAS y AINE tomados en período cercano a gestación o durante más de una semana No con paracetamol Clasificación: A.- Ningún riesgo fetal B.- No riesgo fetal en experimentación animal, no en humanos pero con pocos estudios C.- Alguna evidencia de riesgo fetal en experimientación animal D.- Alguna evidencia de riesgo fetal en humanos X.- Contraindicación por evidencias suficientes de riesgo fetal en humanos Fármaco Embarazo Aspirina D 80. Because Nexium® has an advantageous metabolism compared with omeprazole, more compound is available to inhibit gastric proton pumps As a result of stereoselective metabolism that favours Nexium®, it has an advantageous metabolism compared with omeprazole, first-pass metabolism is decreased and systemic clearance is decreased. Thus, following absorption, more Nexium® passes through the liver without being metabolised, and more compound remains in the bloodstream. Delivery of Nexium® to the proton pumps of the gastric parietal cell is thus enhanced compared with omeprazole. Aspirina infantil A Indometacina A (1T), evitar después Ibuprofeno y otros AINE C COX2 C Paracetamol B Codeina A 39
, evitar después. Ibuprofeno y otros AINE. C. COX2. C. Paracetamol. B. Codeina. A. 39.")
40
Lesiones gastrointestinales por AINE
NSAIDs can cause gastroduodenal lesions NSAIDs provide a range of benefits, but they also carry significant risks for the patient through injury of the gastroduodenal mucosa. When the mucosa is visualised by scanning electron microscopy only 16 minutes after administration of aspirin, there is evidence of significant localised foci and damaged cells, compared with the normal mucosa.26 Indeed, endoscopic studies have shown that approximately half of those taking classical NSAIDs regularly have gastric erosions and 10–30% have gastric ulcers.24 Although the COX-2 selective NSAIDs may reduce the overall incidence of peptic ulcers and ulcer complications, patients taking these agents are not free of the risk of gastroduodenal injury.21,27 This is particularly the case among sub-categories of patients with additional risk factors (e.g. elderly patients, those with a history of upper GI clinical events or infected with H. pylori)1 or those taking low-dose aspirin for cardiovascular protection.21 In addition to causing peptic ulcer formation, classical NSAIDs are known to delay the healing of pre-existing ulcers.28 Recent studies indicate that COX-2 plays an important role in gastric mucosal defence and healing,29 and that COX-2 selective NSAIDs also inhibit peptic ulcer healing.30 16 min tras AAS Normal Baskin et al, 1976
1 or those taking low-dose aspirin for cardiovascular protection.21. In addition to causing peptic ulcer formation, classical NSAIDs are known to delay the healing of pre-existing ulcers.28 Recent studies indicate that COX-2 plays an important role in gastric mucosal defence and healing,29 and that COX-2 selective NSAIDs also inhibit peptic ulcer healing min tras AAS. Normal. Baskin et al,")
41
Mortalidad asociada a AINEs “La epidemia silente”
25.000 20.000 15.000 10.000 NSAID-associated deaths: the ‘silent epidemic’ Conservative estimates suggest that each year NSAIDs are responsible for about 16,500 deaths among patients with rheumatoid arthritis or osteoarthritis in the USA.37 This is comparable with the number of deaths from acquired immunodeficiency syndrome (AIDS), and considerably greater than the number of deaths from conditions such as multiple myeloma, asthma, cervical cancer or Hodgkin’s disease. If deaths resulting from NSAID-related upper GI complications were tabulated separately, they would represent the 15th most common cause of death in the USA. Despite this high mortality, NSAID gastrotoxicity remains a ‘silent epidemic’: many physicians and most patients are unaware of the scale of the problem. In one survey, for example, nearly 75% of patients who used NSAIDs regularly were unaware of or unconcerned about possible upper GI complications.42 The increased use of COX-2 selective NSAIDs may move NSAID-associated deaths slightly further down the list of causes of death. However, as many patients will continue to be treated with classical NSAIDs, and COX-2 selective NSAIDs are not totally free of GI toxicity (see later slides), this ‘silent epidemic’ will not disappear. 5.000 SIDA Astma Leucemia Mieloma AINEs Cáncer cérvix Enf. Hodgkin *USA 1997 data Wolfe et al 1999
, and considerably greater than the number of deaths from conditions such as multiple myeloma, asthma, cervical cancer or Hodgkin’s disease. If deaths resulting from NSAID-related upper GI complications were tabulated separately, they would represent the 15th most common cause of death in the USA. Despite this high mortality, NSAID gastrotoxicity remains a ‘silent epidemic’: many physicians and most patients are unaware of the scale of the problem. In one survey, for example, nearly 75% of patients who used NSAIDs regularly were unaware of or unconcerned about possible upper GI complications.42. The increased use of COX-2 selective NSAIDs may move NSAID-associated deaths slightly further down the list of causes of death. However, as many patients will continue to be treated with classical NSAIDs, and COX-2 selective NSAIDs are not totally free of GI toxicity (see later slides), this ‘silent epidemic’ will not disappear SIDA. Astma. Leucemia. Mieloma. AINEs. Cáncer cérvix. Enf. Hodgkin. *USA 1997 data. Wolfe et al")
42
Mortalidad asociada a AINEs “La epidemia silente”
25.000 20.000 15.000 10.000 NSAID-associated deaths: the ‘silent epidemic’ Conservative estimates suggest that each year NSAIDs are responsible for about 16,500 deaths among patients with rheumatoid arthritis or osteoarthritis in the USA.37 This is comparable with the number of deaths from acquired immunodeficiency syndrome (AIDS), and considerably greater than the number of deaths from conditions such as multiple myeloma, asthma, cervical cancer or Hodgkin’s disease. If deaths resulting from NSAID-related upper GI complications were tabulated separately, they would represent the 15th most common cause of death in the USA. Despite this high mortality, NSAID gastrotoxicity remains a ‘silent epidemic’: many physicians and most patients are unaware of the scale of the problem. In one survey, for example, nearly 75% of patients who used NSAIDs regularly were unaware of or unconcerned about possible upper GI complications.42 The increased use of COX-2 selective NSAIDs may move NSAID-associated deaths slightly further down the list of causes of death. However, as many patients will continue to be treated with classical NSAIDs, and COX-2 selective NSAIDs are not totally free of GI toxicity (see later slides), this ‘silent epidemic’ will not disappear. 5.000 SIDA Astma Leucemia Mieloma AINE Cáncer cérvix Enf. Hodgkin *USA 1997 data Wolfe et al 1999
, and considerably greater than the number of deaths from conditions such as multiple myeloma, asthma, cervical cancer or Hodgkin’s disease. If deaths resulting from NSAID-related upper GI complications were tabulated separately, they would represent the 15th most common cause of death in the USA. Despite this high mortality, NSAID gastrotoxicity remains a ‘silent epidemic’: many physicians and most patients are unaware of the scale of the problem. In one survey, for example, nearly 75% of patients who used NSAIDs regularly were unaware of or unconcerned about possible upper GI complications.42. The increased use of COX-2 selective NSAIDs may move NSAID-associated deaths slightly further down the list of causes of death. However, as many patients will continue to be treated with classical NSAIDs, and COX-2 selective NSAIDs are not totally free of GI toxicity (see later slides), this ‘silent epidemic’ will not disappear SIDA. Astma. Leucemia. Mieloma. AINE. Cáncer cérvix. Enf. Hodgkin. *USA 1997 data. Wolfe et al")
43
Lesiones digestivas por los Aine

44
¿A quién gastroproteger?
El coste de gastroproteger a todos los tratados con AINE oscila entre € por episodio de hemorragia digestiva prevenido

45
Factores de riesgo de complicaciones gastroduodenales tras AINE
Edad (+ 65 años), severidad patología de base 5.6 (>70 años) Antecedentes de enfermedad ulcerosa 13.5 (complicada) 6.1 (No complicada) Combinación de varios AINE (AAS) 9 Tipo de Aine 2.6 – 33* Dosis altas de Aine 7 Combinación con corticoides, ISRS o antiacoagulantes 2.2, 3.6, 6.4 H. pylori La erradicación reduce el riesgo en paciente que comienzan tratamiento pero no en los que ya son consumidores crónicos DDW 2006
, severidad patología de base. 5.6 (>70 años) Antecedentes de enfermedad ulcerosa (complicada) 6.1 (No complicada) Combinación de varios AINE (AAS) 9. Tipo de Aine. 2.6 – 33* Dosis altas de Aine. 7. Combinación con corticoides, ISRS o antiacoagulantes. 2.2, 3.6, 6.4. H. pylori. La erradicación reduce el riesgo en paciente que comienzan tratamiento pero no en los que ya son consumidores crónicos. DDW")
46
GASTROPROTEGER DESDE EL PRIMER DÍA
Chan FKL, Nature Clin Pract. 2006, 3, DDW 2006 GASTROPROTEGER DESDE EL PRIMER DÍA Edad (+ 65 años), severidad patología de base 5.6 (>70 años) Antecedentes de enfermedad ulcerosa 13.5 (complicada) 6.1 (No complicada) Combinación de varios AINE (AAS) 9 Tipo de Aine 2.6 – 33* Dosis altas de Aine 7 Combinación con corticoides, ISRS o antiacoagulantes 2.2, 3.6, 6.4 H. pylori 1.79 (solo) 6.13 (+AINE) Incidencia anual de complicaciones por acumulación de riesgos 40% >4 factores 18% - 4 factores 8% - 3 factores 2% - 1 factor 0.8% - ningún factor
, severidad patología de base. 5.6 (>70 años) Antecedentes de enfermedad ulcerosa (complicada) 6.1 (No complicada) Combinación de varios AINE (AAS) 9. Tipo de Aine. 2.6 – 33* Dosis altas de Aine. 7. Combinación con corticoides, ISRS o antiacoagulantes. 2.2, 3.6, 6.4. H. pylori (solo) 6.13 (+AINE) Incidencia anual de complicaciones por acumulación de riesgos. 40% >4 factores. 18% - 4 factores. 8% - 3 factores. 2% - 1 factor. 0.8% - ningún factor.")
47
¿Cómo Prevenir en el paciente de riesgo?
- Reducir uso de AINE - Dosis mínima necesaria - AINE menos lesivos: - Diclofenaco Ibuprofeno Coxibs,..... - Tratamiento concomitante con IBP

48
Riesgo individual de los AINE
Lanas et al. 2005, 2006 Fármaco O.R. (95% CI) Celecoxib 1.2 Ibuprofeno ( ) Diclofenaco ( ) Aspirina ( ) Naproxen ( ) Meloxicam ( )) Piroxicam (11-3.6) Ketorolaco ( )
 Celecoxib 1.2. Ibuprofeno 2.6 ( ) Diclofenaco 5.1 ( ) Aspirina 6 ( ) Naproxen 6.5 ( ) Meloxicam 4.4 ( )) Piroxicam 20.4 (11-3.6) Ketorolaco 33 ( )")
49
Riesgos de IM y uso reciente de AINE y coxib
Riesgo Relativo Ajustado (95% IC) Tipo de Uso Celecoxib Rofecoxib AINE Ibuprofeno Diclofenaco Naproxeno 0.5 1 2 3 4 5 6 1,21 1,32 1,21 1,24 1,55 1,27 Hipisley J, Coupland C. BMJ 2005
 Tipo de Uso. Celecoxib. Rofecoxib. AINE. Ibuprofeno. Diclofenaco. Naproxeno ,21. 1,32. 1,21. 1,24. 1,55. 1,27. Hipisley J, Coupland C. BMJ")
50
Todos los AINE aumentan el riesgo cardiovascular
RR eventos cardiovasculares Baiget et al, en prensa (Laine, DDW 2006)
")
51
Utilización AINE Aspirina Riesgo GI No / bajo Moderado Alto NO Sí AINE
COX2 ó AINE + IBP Considerar terapia alternativa sin AINE COX2 + IBP Sí (Riesgo CV) AINE (Diclofenac) + IBP Naproxeno + IBP Considerar Terapia alternativa sin AINE AINE no recomendado Continuar ASA + IBP Scheiman JM, et al Aliment. Pharmacol. Ther Chan FKL nature Clin Pract 2006, 3,
 AINE (Diclofenac) + IBP. Naproxeno + IBP. Considerar Terapia alternativa sin AINE. AINE no recomendado. Continuar ASA + IBP. Scheiman JM, et al Aliment. Pharmacol. Ther Chan FKL nature Clin Pract 2006, 3,")
52
Efectos Secundarios Gastrointestinales Altos por AINE
Ulceras 15-30% Debutan sin dispepsia Complicaciones por úlceras 1.5% Dispepsia > 25% No ulceras Lanas 1999

53
Proporción (%) acumulada de pacientes con alivio de síntomas
AINE no-selectivos COX-2 selectivos 10 20 30 40 50 60 70 80 2 4 6 8 12 14 16 18 22 24 10 20 30 40 50 60 70 80 2 4 6 8 12 14 16 18 22 24 esomeprazol 40 mg (n=134) esomeprazol 40 mg (n=240) esomeprazol 20 mg (n=118) esomeprazol 20 mg (n=257) placebo (n=133) placebo (n=257) Días Días AINES selectivos para COX-2 Log-rank test E40 vs pl p<0.001 E20 vs pl p=0.003 AINEs no selectivos Log-rank test E40 vs pl p=0.002 E20 vs pl p<0.001 Yeomans et al. DDW 2003
 esomeprazol 40 mg (n=240) esomeprazol 20 mg (n=118) esomeprazol 20 mg (n=257) placebo (n=133) placebo (n=257) Días. Días. AINES selectivos para COX-2. Log-rank test E40 vs pl p<0.001 E20 vs pl p= AINEs no selectivos. Log-rank test E40 vs pl p=0.002 E20 vs pl p< Yeomans et al. DDW")
54
ANTICOAGULANTES ORALES
INTERACCIONES CORTICOIDES Incremento incidencia de gastropatías ANTICOAGULANTES ORALES Incremento riesgo de hemorragias ANTIHIPERTENSIVOS (IECA y -BLOQUEANTE) Reducción del efecto y posibilidad de bradicardia severa (s/t en ancianos, hipertensos, diabéticos, insuficiencia cardiaca,…) Retención de sodio DIURÉTICOS Reducción efecto diurético y natriurético DIGOXINA Riesgo de intoxicación digitálica
 Reducción del efecto y posibilidad de bradicardia severa (s/t en ancianos, hipertensos, diabéticos, insuficiencia cardiaca,…) Retención de sodio. DIURÉTICOS. Reducción efecto diurético y natriurético. DIGOXINA. Riesgo de intoxicación digitálica.")
55
Uso racional de los Aine
Utilizar los de seguridad y eficacia demostradas Con dosis adecuadas el 60% de los pacientes responden a cualquier AINE. Gran variabilidad en la respuesta individual Recomendable una semana de prueba para analgesia y tres semanas para acción antiinflamatoria. Si se cambia un AINE por fracaso terapéutico, escogerlo de otra familia (no siempre funciona). Doblar dosis solo induce ligera mejoría terapéutica pero incrementa mucho la toxicidad NO COMBINAR NUNCA DOS O MÁS AINE. No en supositorios: absorción impredecible
. Doblar dosis solo induce ligera mejoría terapéutica pero incrementa mucho la toxicidad. NO COMBINAR NUNCA DOS O MÁS AINE. No en supositorios: absorción impredecible.")
57
Corticoides Los antiinflamatorios máss eficaces, pero necesitamos dosis farmacológicas (hasta 1000 veces superiores a las fisiológicas) Por comodidad y coste la prednisona oral (se convierte en prednisolona) es la referencia, pero cualquier otro corticoide puede sustituirla teniendo en cuenta la presentación galénica y las correspondencias farmacológicas Indicaciones terapéuticas Antiinflamatorio Inmunosupresor Terapia de sustitución Preferible terapia local a sistémica y, si se puede, mejor asociarlo a otros agentes para reducir dosis y toxicidad Las dosis aisladas (o únicas) son relativamente inocuas
 es la referencia, pero cualquier otro corticoide puede sustituirla teniendo en cuenta la presentación galénica y las correspondencias farmacológicas. Indicaciones terapéuticas. Antiinflamatorio. Inmunosupresor. Terapia de sustitución. Preferible terapia local a sistémica y, si se puede, mejor asociarlo a otros agentes para reducir dosis y toxicidad. Las dosis aisladas (o únicas) son relativamente inocuas.")
58
Corticoide Proteína Núcleo Receptor para glucocorticoides ARNm
Los agonistas β2-tienen un efecto positivo sobre la activación de los receptores para glucocorticoides (RG) Los agonistas β2 potencian la acción de los corticoides. Este efecto es más marcado con los LABA que con los SABA. Los LABA aumentan la translocación de los RG en las células del músculo liso de las vías aéreas y aumentan la activación de un factor de transcripción (CCAAT enhancer binding protein-α) que regula diversos genes incluidos aquellos implicados en la proliferación del músculo liso. Las células de músculo liso de las vías aéreas son una fuente importante de mediadores inflamatorios por medio de la expresión de múltiples genes proinflamatorios implicados en el reclutamiento de neutrófilos y eosinófilos en las vías aéreas. La interacción positiva entre los LABA y los corticoides en la EPOC podría potenciar el efecto antiinflamatorio de los corticoides en las células del músculo liso de las vías aéreas, inhibiendo así la inflamación aguda. Esta podría ser la base molecular de la interacción sinérgica entre el formoterol y la budesónida que podría explicar la reducción de las exacerbaciones observada cuando se administran estos componentes juntos. 1. Barnes PJ. Eur Respir J 2002;19:182–191. 2. Barnes PJ. Eur Respir J 2007;29:587–595. ARNm Núcleo Gen sensible a los esteroides Barnes PJ. Eur Respir J 2002;19:
 Los agonistas β2 potencian la acción de los corticoides. Este efecto es más marcado con los LABA que con los SABA. Los LABA aumentan la translocación de los RG en las células del músculo liso de las vías aéreas y aumentan la activación de un factor de transcripción (CCAAT enhancer binding protein-α) que regula diversos genes incluidos aquellos implicados en la proliferación del músculo liso. Las células de músculo liso de las vías aéreas son una fuente importante de mediadores inflamatorios por medio de la expresión de múltiples genes proinflamatorios implicados en el reclutamiento de neutrófilos y eosinófilos en las vías aéreas. La interacción positiva entre los LABA y los corticoides en la EPOC podría potenciar el efecto antiinflamatorio de los corticoides en las células del músculo liso de las vías aéreas, inhibiendo así la inflamación aguda. Esta podría ser la base molecular de la interacción sinérgica entre el formoterol y la budesónida que podría explicar la reducción de las exacerbaciones observada cuando se administran estos componentes juntos. 1. Barnes PJ. Eur Respir J 2002;19:182– Barnes PJ. Eur Respir J 2007;29:587–595. ARNm. Núcleo. Gen sensible a los esteroides. Barnes PJ. Eur Respir J 2002;19:")
59
Respuesta inflamatoria
FOSFOLÍPIDOS ACIDO ARAQUIDÓNICO CORTICOIDES AINES PLA2 LOX COX PROSTACICLINAS TROMBOXANOS PROSTAGLANDINAS LIPOXINAS LEUCOTRIENOS 59

61
Efectos corticoides Metabólicos
Carbohidratos: tendencia a hiperglucemia Disminuye captación y utilización glucosa Incremento gluconeogénesis Proteinas: Aumento catabolismo y disminuye anabolismo Lípidos: favorece acción hormonas lipolíticas y redistribución grasa

62
Efectos corticoides (II)
Regulatorias Hipotalamo y pituitaria anterior: feed-back con ACTH Vasculares Vasodilatación y permeabilidad reducida Inflamatoria Reducción inflamación crónica y respuestas autoinmunes, disminución cicatrización y aspectos protectores de la respuesta inflamatoria

63
Farmacocinética Corticoides
Buena absorción (varía con la sal empleada): oral, rectal, inhalatoria, conjuntival, intraarticular, i.m., tópica Semivida plasmática 1.5-5h. Duración del efecto 8-50h Metabolismo principalmente hepático, originando metabolitos menos activos (ojo beclometasona) y de eliminación renal Ojo con la depresion es muy fercuente y los psoquiatras los retiran
: oral, rectal, inhalatoria, conjuntival, intraarticular, i.m., tópica. Semivida plasmática 1.5-5h. Duración del efecto 8-50h. Metabolismo principalmente hepático, originando metabolitos menos activos (ojo beclometasona) y de eliminación renal. Ojo con la depresion es muy fercuente y los psoquiatras los retiran.")
64
Depresión Retraso crecimiento

65
Criterios de selección
La potencia no es determinante: a dosis terapéuticas todos se consideran equivalentes por vía sistémica La duración de la acción: Acción corta o intermedia: Tratamientos de urgencia o casos agudos (varias tomas al día) Terapias en días alternos (evitan atrofia eje HHA) Acción larga: Cuando no responde a la terapia alternada (artritis reumatoide, colitis ulcerosa) o si se desea acción inmunosupresora La acción mineralcorticoide: Lo ideal es baja acción o media (en tratamientos de corta duración) Tras tratamientos desde 2 semanas: suspensión gradual para evitar insuficiencia suprarrenal aguda
 Terapias en días alternos (evitan atrofia eje HHA) Acción larga: Cuando no responde a la terapia alternada (artritis reumatoide, colitis ulcerosa) o si se desea acción inmunosupresora. La acción mineralcorticoide: Lo ideal es baja acción o media (en tratamientos de corta duración) Tras tratamientos desde 2 semanas: suspensión gradual para evitar insuficiencia suprarrenal aguda.")
66
Fármacos antiartríticos
AINE: en solitario (al inicio) o en combinación, proporcionan alivio sintomático (Dolor e inflamación) pero no modifican el desarrollo de la enfermedad ni previenen la lesión estructural A largo plazo no utilizar aisladamente: con modificadores del desarrollo de la enfermedad No hay diferencias en eficacia, y la elección se debe basar en otros factores (dosificación, tolerancia, costo, tratamientos o enfermedades concurrentes, respuesta individual,..)
 o en combinación, proporcionan alivio sintomático (Dolor e inflamación) pero no modifican el desarrollo de la enfermedad ni previenen la lesión estructural. A largo plazo no utilizar aisladamente: con modificadores del desarrollo de la enfermedad. No hay diferencias en eficacia, y la elección se debe basar en otros factores (dosificación, tolerancia, costo, tratamientos o enfermedades concurrentes, respuesta individual,..)")
67
Fármacos antiartríticos (II)
Modificadores del desarrollo de la enfermedad reumática: reducen la lesión articular, al menos temporalmente. Su efecto es lento, 1-6 meses hasta repuesta clínica clara. Eficacia impredecible en un paciente dado, aunque 2/3 pueden responder bien. La toxicidad, singular para cada uno, debe ser muy vigilada. Tratamiento precoz y agresivo. Mas efectivos combinados que en solitario 1ª linea: Metotrexato, sulfasalacina, antimalaricos (cloroquina e hidroxicloroquina), leflunomina. 2ª linea: ciclosporina, minociclina, azatioprina, ciclofosfamida.
, leflunomina. 2ª linea: ciclosporina, minociclina, azatioprina, ciclofosfamida.")
68
Fármacos antiartríticos (III)
Modificadores de las respuestas biológicas al TNF-α e IL-1: etanercept, infliximab, anakinra. Corticoides: Tratamiento manifestaciones extraarticulares graves (vasculitis reumatoidea o neumonitis reumatoidea), a dosis elevadas (1 mg/kg/día de prednisona o equivalente). Tratamiento puente para el control de la sinovitis, mientras se consolida el efecto de los modificadores del desarrollo de la enfermedad, a dosis bajas o moderadas Crónicamente (30-60% pacientes), a dosis bajas (≤7.5 mg día de prednisona) para controlar sinovitis y retardar erosión ósea
, a dosis elevadas (1 mg/kg/día de prednisona o equivalente). Tratamiento puente para el control de la sinovitis, mientras se consolida el efecto de los modificadores del desarrollo de la enfermedad, a dosis bajas o moderadas. Crónicamente (30-60% pacientes), a dosis bajas (≤7.5 mg día de prednisona) para controlar sinovitis y retardar erosión ósea.")
69
Metotrexato Antagonista del ácido fólico
Dosis menores que en cáncer (hasta mg/semana), con acción antiinflamatoria y poco inmunosupresora De elección en tratamiento inicial de formas moderadas y graves de la AR, tanto en monoterapia como combinada. Mejora rápido (3-6 semanas) signos y síntomas inflamatorios. Mejores efectos con enfermedad poco avanzada. Frecuentes efectos adversos pero manejables sin suspender tratamiento (acd. fólico 1-3 mg/día; folínico tras MTX). Alopecia, estomatitis e intolerancia gastrointestinal tratadas con ácido fólico. Leucopenia moderada, mielosupresión, incremento transaminasas,.. Neumonitis (3.5% incidencia, 17% mortalidad) s/t al principio tratamiento El efecto terapéutico puede mantenerse años y la retirada del fármaco conlleva empeoramiento de la artritis en 3-6 semanas. Efecto teratógeno
, con acción antiinflamatoria y poco inmunosupresora. De elección en tratamiento inicial de formas moderadas y graves de la AR, tanto en monoterapia como combinada. Mejora rápido (3-6 semanas) signos y síntomas inflamatorios. Mejores efectos con enfermedad poco avanzada. Frecuentes efectos adversos pero manejables sin suspender tratamiento (acd. fólico 1-3 mg/día; folínico tras MTX). Alopecia, estomatitis e intolerancia gastrointestinal tratadas con ácido fólico. Leucopenia moderada, mielosupresión, incremento transaminasas,.. Neumonitis (3.5% incidencia, 17% mortalidad) s/t al principio tratamiento. El efecto terapéutico puede mantenerse años y la retirada del fármaco conlleva empeoramiento de la artritis en 3-6 semanas. Efecto teratógeno.")
70
DMART: disease –modifying antirheumatic drugs

71
DMART: disease –modifying antirheumatic drugs

72
LESIÓN TISULAR INFLAMACIÓN LOCAL PERCEPCIÓN DEL DOLOR

73
Opioides Agonistas puros mayores Morfina, metadona, fentanilo
Agonistas puros menores Codeína (oxicodona), petidina, dihidrocodeína, dextropropoxifeno, tramadol Agonistas parciales Buprenorfina Agonistas-Antagonistas mixtos Nalorfina, pentazocina, butorfanol, nalbufina Antagonistas puros Naloxona, naltrexona
, petidina, dihidrocodeína, dextropropoxifeno, tramadol. Agonistas parciales Buprenorfina. Agonistas-Antagonistas mixtos Nalorfina, pentazocina, butorfanol, nalbufina. Antagonistas puros Naloxona, naltrexona.")
74
Opioides Agonistas puros mayores: Elevada capacidad de producir analgesia, euforia y dependencia Agonistas puros menores: menor potencia y menor toxicidad Agonistas parciales: Analgesia no aprovechable, acción euforizante y depresora respiratoria Agonistas-Antagonistas mixtos: A dosis bajas, similares a morfina Antagonistas puros: Sin actividad farmacológica propia. Uso en casos de sobredosis o deshabituación

75
Efectos farmacológicos
SNC: Analgesia, depresión respiratoria, antitusígena, náuseas y vómitos, miosis, euforia y disforia. TD: Vómitos, estreñimiento, retraso del vaciado gástrico Urinario: Espasmos de vejiga. Retención urinaria Respiratorio: Broncoconstricción Cardiovascular: Hipotensión y bradicardia a dosis superiores a las analgésicas Metabolismo: Disminución de la temperatura corporal, hiperglucemia, disminución del metabolismo basal y del consumo de O2

76
FARMACOCINÉTICA Biodisponibilidad oral variable. Alternativas eficaces i.m. y s.c. Las vías más rápidas son i.v., epidural e intratecal Parches, preparaciones absorción oral retardada, intranasal Buena distribución y alto metabolismo hepático de primer paso. Excreción renal (90% en 24 h) Márgenes terapéuticos amplios. Las funciones cognitivas, conducir vehículos y manejar maquinaria, preservada con dosis moderadas (10 mg/4h??) y estables de opioides para control dolor crónico. La mayoría 180 mg/día de morfina, (se puede subir hasta 1g, empleadas durante meses-años). La administración prolongada tiene un perfil adverso singular (cambios hormonales, inmunológicos,…)
 Márgenes terapéuticos amplios. Las funciones cognitivas, conducir vehículos y manejar maquinaria, preservada con dosis moderadas (10 mg/4h ) y estables de opioides para control dolor crónico. La mayoría 180 mg/día de morfina, (se puede subir hasta 1g, empleadas durante meses-años). La administración prolongada tiene un perfil adverso singular (cambios hormonales, inmunológicos,…)")
77
Efectos adversos Estreñimiento (70%) Náuseas (60%)
Somnolencia y sedación (60%) Depresión respiratoria (1-10%) Confusión y alucinaciones (5%) Efectos neurológicos: mareos, alteraciones visuales, eufória, disfória, convulsiones Retención urinaria, oliguria TOLERANCIA Y DEPENDENCIA
 Depresión respiratoria (1-10%) Confusión y alucinaciones (5%) Efectos neurológicos: mareos, alteraciones visuales, eufória, disfória, convulsiones. Retención urinaria, oliguria. TOLERANCIA Y DEPENDENCIA.")
78
CONTRAINDICACIONES Asma bronquial y EPOC
Lesiones intracraneales e hipertensión craneal Insuficiencia hepática Estados convulsivos Insuficiencia renal Hipotiroidismo Cólico biliar Niños, ancianos

79
INTERACCIONES Si se administra por vía oral::retrasa la absorción de otros fármacos. Derivadas de las interferencias con el metabolismo hepático de otros medicamentos: INDUCTORES e INHIBIDORES enzimáticos Derivadas de su actividad depresora del SNC potencia y es potenciada: fenotiazidas, antidepresivos tricíclicos, BZD, anestésicos gaseosos, alcohol,…

80
Indicaciones DOLOR: Agudo en infarto, cólico nefrítico, pleurítico, traumático. Crónico oncológico. No indicados en dolor neuropático, aunque responde Administración continuada del opioide…NO en respuesta a crisis Se recomienda combinar con AINE o paracetamol

81
The 2007 Oxford league table of analgesic efficacy (at least 3 trials or 200 patients)Numbers needed to treat are calculated for the proportion of patients with at least 50% pain relief over 4-6 hours compared with placebo in randomised, double-blind, single-dose studies in patients with moderate to severe pain. Drugs were oral, unless specified, and doses are milligrams. Shaded rows are intramuscular administration. Understanding the league table Effective relief can be achieved with oral non-opioids and non-steroidal anti-inflammatory drugs. Analgesic efficacy is expressed as the NNT, the number of patients who need to receive the active drug for one to achieve at least 50% relief of pain compared with placebo over a 4-6 hour treatment period. The most effective drugs have a low NNT of just over 2. This means that for every two patients who receive the drug one patient will get at least 50% relief because of the treatment (the other patient may or may not obtain relief but it does not reach the 50% level). The NNT is treatment-specific, which is useful for comparison of relative efficacy. Because these NNT comparisons are against placebo, the best NNT of 2 means that 50 of 100 patients will get at least 50% relief specifically because of the treatment. Another twenty will have a placebo response giving them at least 50% relief. With ibuprofen 400 mg, therefore, about 70 of 100 in total will have effective pain relief. For comparison, with 10 mg intramuscular morphine about 53% of patients get more than 50% pain relief. Because the effect of placebo is added in, the comparisons between analgesics are not as stark as with NNT. It is clear that the oral NSAIDs do extremely well in this single-dose postoperative comparison. At these doses they all have NNT values of between 2 and 3, and the point estimate of the mean is below that of (i.e. better than) 10 mg of intramuscular morphine, even though the confidence intervals overlap. The simple analgesics, aspirin and paracetamol are significantly less effective than 10 mg intramuscular morphine. The point estimates of the NNT are higher, and there is no overlap of the confidence intervals. Weak opioids perform poorly in single doses on their own. Combining them with simple analgesics improves analgesic efficacy. Drawbacks of the league table The most important drawback is size. Small trials (or small data sets) cannot accurately estimate the magnitude of the analgesic effect. To know that the NNT of an analgesic is 3.0 with a confidence interval of 2.5 to 3.5 we need almost 1000 patients in a comparative trial. So as you contemplate the numbers, be conscious of the amount of information upon which NNTs and percent of patients with at least 50% pain relief are based. In practice any comparison with more than 250 or so patients is probably adequate. For instance, ibuprofen 800 mg is at the top of the league, with an NNT of 1.6 and with 100% of patients achieving at least 50% pain relief. But only 76 patients have ever been involved in comparative trials with placebo. This makes the apparent wonderful result less so, and you should treat it cautiously. The information is presented here, warts and all, so that professionals and public can make their own assessments. What is missing? Adverse effects from single-dose analgesic trials are rarely helpful with simple analgesics and NSAIDs, though they may be much more helpful with opioids. Work on adverse effects is being done, and a summary of this will appear on this site later in 1999. Some analgesics used commonly outside the UK may not be represented. Again work is ongoing to plug these gaps, but so often the randomised trials (placebo-controlled, randomised, double-blind and with proper outcome measures and entry criteria), have not been done. Finally cost information is not given here, because it can vary so much throughout the world.
. The NNT is treatment-specific, which is useful for comparison of relative efficacy. Because these NNT comparisons are against placebo, the best NNT of 2 means that 50 of 100 patients will get at least 50% relief specifically because of the treatment. Another twenty will have a placebo response giving them at least 50% relief. With ibuprofen 400 mg, therefore, about 70 of 100 in total will have effective pain relief. For comparison, with 10 mg intramuscular morphine about 53% of patients get more than 50% pain relief. Because the effect of placebo is added in, the comparisons between analgesics are not as stark as with NNT. It is clear that the oral NSAIDs do extremely well in this single-dose postoperative comparison. At these doses they all have NNT values of between 2 and 3, and the point estimate of the mean is below that of (i.e. better than) 10 mg of intramuscular morphine, even though the confidence intervals overlap. The simple analgesics, aspirin and paracetamol are significantly less effective than 10 mg intramuscular morphine. The point estimates of the NNT are higher, and there is no overlap of the confidence intervals. Weak opioids perform poorly in single doses on their own. Combining them with simple analgesics improves analgesic efficacy. Drawbacks of the league table. The most important drawback is size. Small trials (or small data sets) cannot accurately estimate the magnitude of the analgesic effect. To know that the NNT of an analgesic is 3.0 with a confidence interval of 2.5 to 3.5 we need almost 1000 patients in a comparative trial. So as you contemplate the numbers, be conscious of the amount of information upon which NNTs and percent of patients with at least 50% pain relief are based. In practice any comparison with more than 250 or so patients is probably adequate. For instance, ibuprofen 800 mg is at the top of the league, with an NNT of 1.6 and with 100% of patients achieving at least 50% pain relief. But only 76 patients have ever been involved in comparative trials with placebo. This makes the apparent wonderful result less so, and you should treat it cautiously. The information is presented here, warts and all, so that professionals and public can make their own assessments. What is missing Adverse effects from single-dose analgesic trials are rarely helpful with simple analgesics and NSAIDs, though they may be much more helpful with opioids. Work on adverse effects is being done, and a summary of this will appear on this site later in Some analgesics used commonly outside the UK may not be represented. Again work is ongoing to plug these gaps, but so often the randomised trials (placebo-controlled, randomised, double-blind and with proper outcome measures and entry criteria), have not been done. Finally cost information is not given here, because it can vary so much throughout the world.")
82
Indicaciones DIARREA que no cede
TOS seca DIARREA que no cede Insuficiencia cardíaca izquierda: reduce la precarga por venodilatación DISNEA acompañada de IC, en edema agudo de pulmón quita la ansiedad y mejora la sintomatología.

83
Los pacientes con dolor crónico no asociado a enfermedad terminal pueden obtener una analgesia satisfactoria mediante el uso de dosis estables (no incrementadas) de opioides, sin riesgo de adicción. Este tratamiento puede durar varios años Rotación de opiodes

84
En el control del dolor crónico los incrementos de dosis se deben realizar en las primeras semanas, las dosis deben ser moderadas y los incrementos cuidadosos: lograr equilibrio ANALGESIA/ EFECTOS ADVERSOS Muchos médicos utilizan dosis muy altas (hasta 1 g o más de morfina /día) que, aunque no parecen comprometer la vida del paciente, tampoco parecen añadir nada en potencia analgésica
 que, aunque no parecen comprometer la vida del paciente, tampoco parecen añadir nada en potencia analgésica.")
85
ANTIDEPRESIVOS TRICÍCLICOS
Mejores que los ISRS S/t en el neuropático Efecto antidepresivo y ansiolítico. Mejoran el sueño. Potenciación de la analgesia Efecto analgésico per se, previo y a dosis menores (Dosis bajas, al acostarse) que el antidepresivo NEUROLÉPTICOS Potencian la analgesia y sedación de antidepresivos (LEVOPROMACINA) Antieméticos, asociados a opioides (HALOPERIDOL)
 que el antidepresivo. NEUROLÉPTICOS. Potencian la analgesia y sedación de antidepresivos (LEVOPROMACINA) Antieméticos, asociados a opioides (HALOPERIDOL)")
86
BENZODIAZEPINAS Efecto relajante muscular Si ansiedad y/o insomnio persistentes Solo en crisis agudas y nunca más de días ANTICONVULSIVANTES Analgésicos en cuadros de dolor neuropático GABAPENTINA, CARBAMACEPINA, FENITOINA SÓDICA Muy eficaces en la profilaxis de crisis de migraña

87
OTROS CALCITONINA: Mecanismo desconocido. Beneficiosa en dolor por metástasis óseas CORTICOIDES: Efecto antiinflamatorio beneficioso en el dolor oncológico y osteoarticular de origen inflamatorio

88
¿Inflamación neurogénica como etiología?
11% prevalencia año (6% hombres, 15-18% mujer) 1.5 episodios/año 10% episodio semanal Duración media 24h Raramente controlada por un profesional Importante respuesta a placebo Importancia de hábitos regulares ¿Inflamación neurogénica como etiología?
 1.5 episodios/año. 10% episodio semanal. Duración media 24h. Raramente controlada por un profesional. Importante respuesta a placebo. Importancia de hábitos regulares. ¿Inflamación neurogénica como etiología")
89
Complicaciones fibróticas
Mecanismo de acción poco claro, pero modifica la sensibilidad del cerebro a la migraña Eficacia moderada y efectos adversos De elección en: Pacientes que no responden a terapia aguda Ataques muy invalidantes o con frecuencia en aumento Mas de 3-4 episodios/mes 2/3 pacientes reducción 50% frecuencia Comenzar con dosis bajas y subir, explicar efectos adversos

90
Farmacología Migraña No específicos Específicos para Mg. neurovascular
AAS, paracetamol, AINE. Específicos para Mg. neurovascular Alcaloides cornezuelo de centeno: Ergotamina, dihidroergotamina,… Triptanes (agonistas 5-HT1B/1D) No existe tratamiento específico para Mg. tensional o dolor facial atípico Antieméticos administrados concomitantemente facilitan la absorción de los fármacos y potencian.
 No existe tratamiento específico para Mg. tensional o dolor facial atípico. Antieméticos administrados concomitantemente facilitan la absorción de los fármacos y potencian.")
91
Alcaloides del cornezuelo
Mecanismo de acción Receptores 5-HT1 y 5HT2 Receptores dopaminérgicos Receptores adrenérgicos Sus efectos son consecuencia de una actuación particular para cada uno de ellos como agonista, agonista parcial y antagonista

92
Alcaloides del cornezuelo
Ergotamina y dihidroergotamina: migraña Ergometrina: prevención hemorragia postparto Metisergida: profilaxis migraña, síndrome carcinoide Bromocriptina: parkinson y trastornos endocrinos Farmacocinetica errática Muy baratos Nauseas, vómitos, vasoconstricción y efecto rebote son los principales efectos adversos

93
Tratamiento agudo de la migraña
Comenzar cuanto antes y con los mas sencillos Grupo significativo no responde a administración oral Aines, Ergotamina,.. Dosis adecuadas pero no más de 2-3 x semanas Triptanes: agonistas 5-HT1B/1D Mecanismo de acción difuso: control de las aferentes nociceptivas del trigémino por vasoconstricción, inhibición neuronas periféricas, inhibición transmisión neuronal. Constricción coronarias: síntomas de angina (poco importante si se previene al paciente) Contraindicados en cardíacos e hipertensos Caros
 Contraindicados en cardíacos e hipertensos. Caros.")
94
No son siempre efectivos
Sumatriptan, Naratriptan, Rizatriptan Zolmitriptan, Almotriptan Eletriptan Vías de administración Formulas orales (80%), spray nasal, inhaladores, supositorios, parenteral No son siempre efectivos
, spray nasal, inhaladores, supositorios, parenteral. No son siempre efectivos.")
96
DOLOR POSTOPERATORIO Suele ser de duración corta (2-5 días) y localizado. La máxima intensidad es a las 48-72h. Si no se controla acarrea complicaciones TRATAMIENTO: Premedicación con opiodes y bloqueo analgésico con anestésicos locales: disminuye el tiempo de analgesia requerido en el postoperatorio AINES vía parenteral (salicilato de lisina, indometacina, ketorolaco, metamizol) Opioides via parenteral (morfina, metadona, tramadol, buprenorfina), y epidural A partir del 5º día “a demanda”
 y localizado. La máxima intensidad es a las 48-72h. Si no se controla acarrea complicaciones. TRATAMIENTO: Premedicación con opiodes y bloqueo analgésico con anestésicos locales: disminuye el tiempo de analgesia requerido en el postoperatorio. AINES vía parenteral (salicilato de lisina, indometacina, ketorolaco, metamizol) Opioides via parenteral (morfina, metadona, tramadol, buprenorfina), y epidural. A partir del 5º día a demanda")
97
DOLOR MUSCULOESQUELÉTICO
Puede ser espontáneo o postraumático TRATAMIENTO: Inicialmente, frío Relajantes musculares de acción central (baclofeno, diazepan) AINES Infiltración local con anestésicos locales (lidocaína) Rehabilitación
 AINES. Infiltración local con anestésicos locales (lidocaína) Rehabilitación.")
98
CÓLICO NEFRÍTICO TRATAMIENTO:
AINES (diclofenaco, indometacina, ketorolaco, metamizol) vía parenteral inicialmente, luego v.o. Analgésicos opioides (petidina) Antiespasmódicos Bloqueo con anestésicos locales Calor, reposo y forzar la diuresis Antibióticos en profilaxis
 vía parenteral inicialmente, luego v.o. Analgésicos opioides (petidina) Antiespasmódicos. Bloqueo con anestésicos locales. Calor, reposo y forzar la diuresis. Antibióticos en profilaxis.")
99
NEURALGIA POSTHERPÉTICA
TRATAMIENTO: Valaciclovir v.o. En las 48h siguientes al inicio Dolor leve: AINES v.o. (paracetamol) Dolor moderado: Paracetamol + amitriptilina/ desipramina, + gabapentina/carbamazepina + corticoides Terapia tópica (capsaicina, parches de lidocaína)
 Dolor moderado: Paracetamol + amitriptilina/ desipramina, + gabapentina/carbamazepina + corticoides. Terapia tópica (capsaicina, parches de lidocaína)")
100
DOLOR ONCOLÓGICO Dolor agudo y crónico
Mucha importancia el estado general del paciente TRATAMIENTO: Escalera analgésica de la O.M.S. De elección: morfina, metadona, parches de fentanilo Terapia adyuvante: Antidepresivos tricíclicos y anticonvulsivantes (40% de casos con componente neuropático) Neurolépticos (Levopromacina) Corticoides (dexametasona) Nunca utilizar placebos En la medida de lo posible: paciente ambulatorio y vía oral No hay dependencia psicológica
 Neurolépticos (Levopromacina) Corticoides (dexametasona) Nunca utilizar placebos. En la medida de lo posible: paciente ambulatorio y vía oral. No hay dependencia psicológica.")
Presentaciones similares
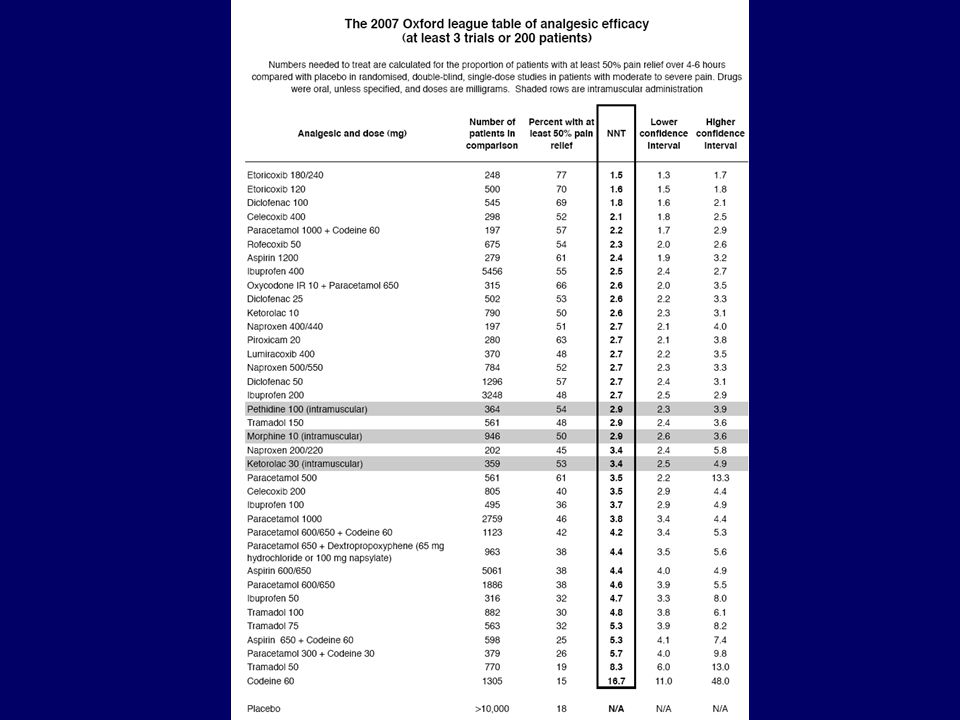

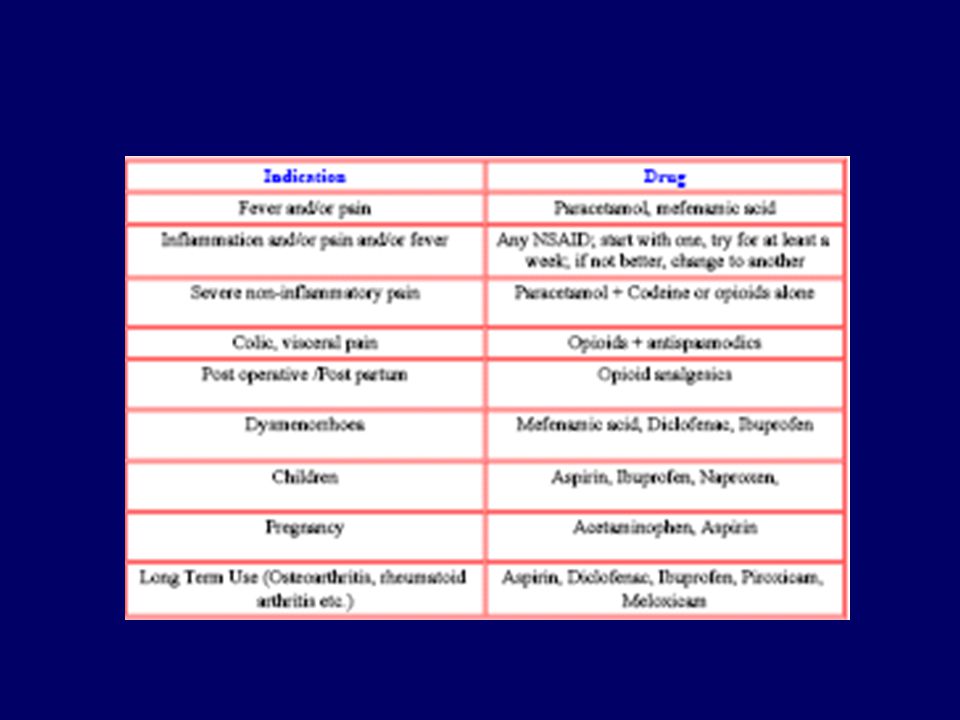


















.>")


