Descargar la presentación
La descarga está en progreso. Por favor, espere

1
HISTIOCITOSIS DE CéLULas De langERHANS PULMONAR CON POLIDIPSIA, POLIURIA E HIPERNATREMIA
Dra. M. E. Vetrisano

2
26 años Ex Tabaquista (20 p/y) Neumotorax espontaneo
ANTECEDENTES PERSONALES Sexo 26 años Ex Tabaquista (20 p/y) Neumotorax espontaneo
 Neumotorax espontaneo.")
3
3/2008 3/2009 Repite neumotorax derecho Neumotorax izquierdo Disnea
Dolor hemitorax derecho 3/2008 Repite neumotorax derecho Neumotorax izquierdo 3/2009 NEUMOTORAX DERECHO En cuanto a la historia de los neumotorax Cuadro agudo de dolor en hemitorax dercho con disnea Se describe ntx derecho se coloca TAP que se retira alos 7 dias con expansion completa se describe en la rx torax aumento de la trama insterticial Dentro del mismo mes se repite el neumotorax decho Nuevo TAP y se realiza BX quirurgica Al año presenta neumotorax izquierdo del 50% TAP sin reexpansion completa a pesar de AC por lo que realizan pleurodesis izquierda Secondary spontaneous pneumothorax can be caused by many different diseases, including infectious processes (Pneumocystis jiroveci, Mycobacterium tuberculosis, and necrotizing pneumonia), interstitial lung disease, connective tissue disease, Langerhans cell histiocytosis, lymphangio leiomyomatosis, cystic fibrosis, and COPD. Cystic fibrosis and COPD are the most commonly reported associated conditions BIOPSIA QUIRÚRGICA PLEURODESIS
, interstitial lung disease, connective tissue disease, Langerhans cell histiocytosis, lymphangio leiomyomatosis, cystic fibrosis, and COPD. Cystic fibrosis and COPD are the most commonly reported associated conditions. BIOPSIA. QUIRÚRGICA. PLEURODESIS.")
4
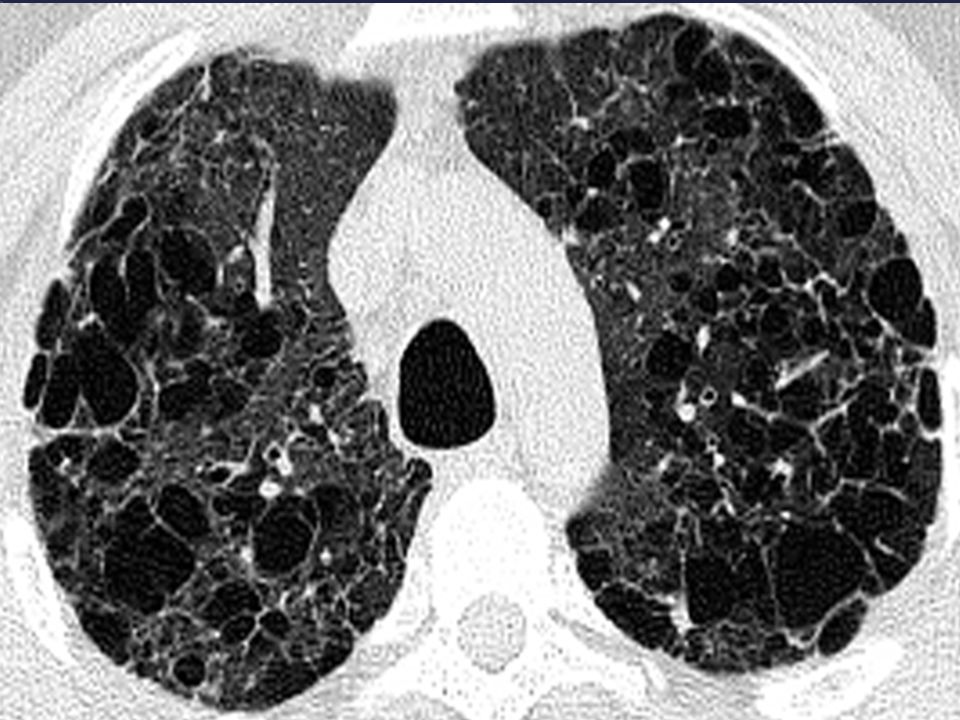
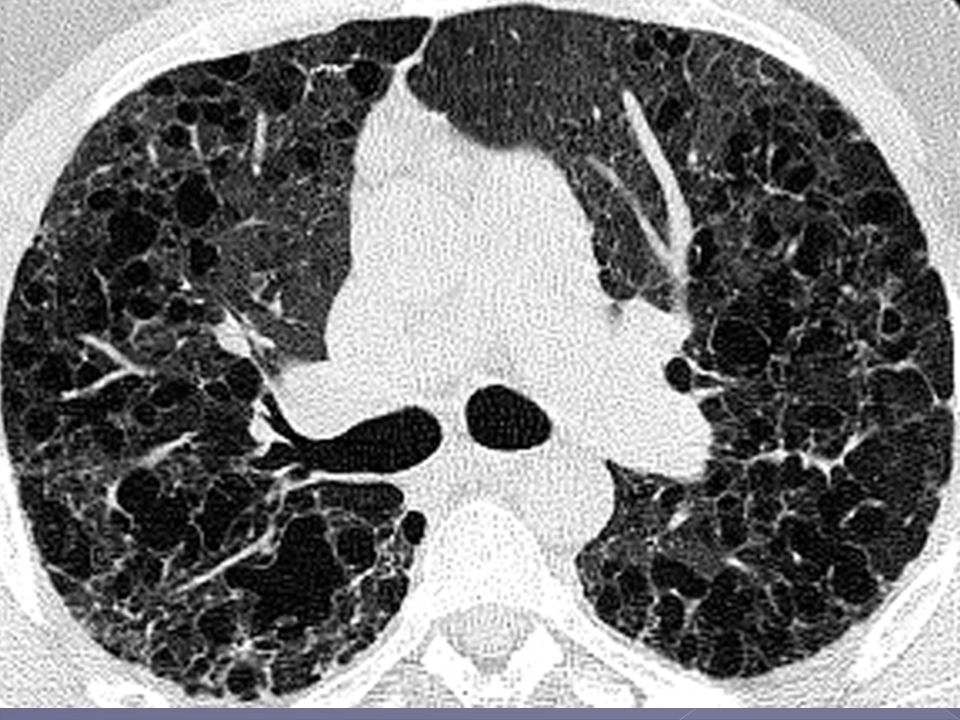
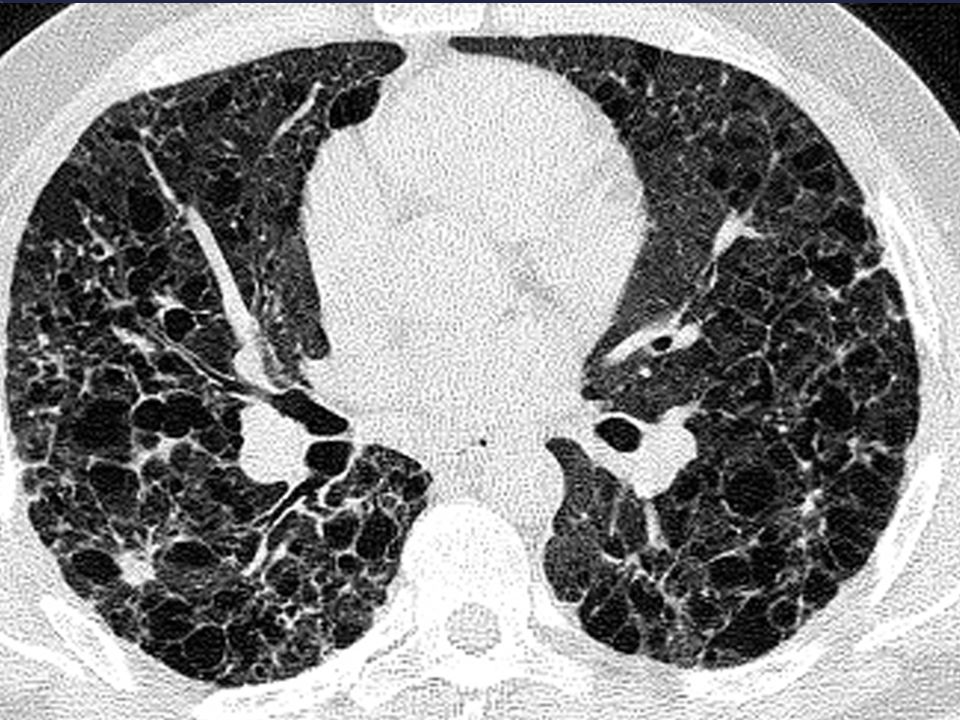
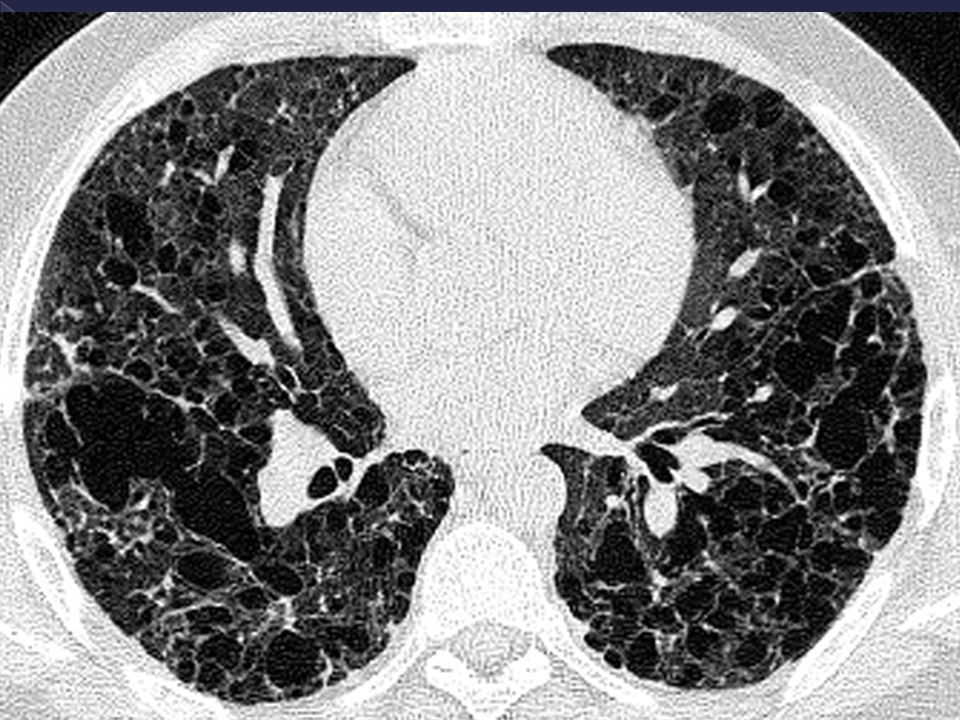
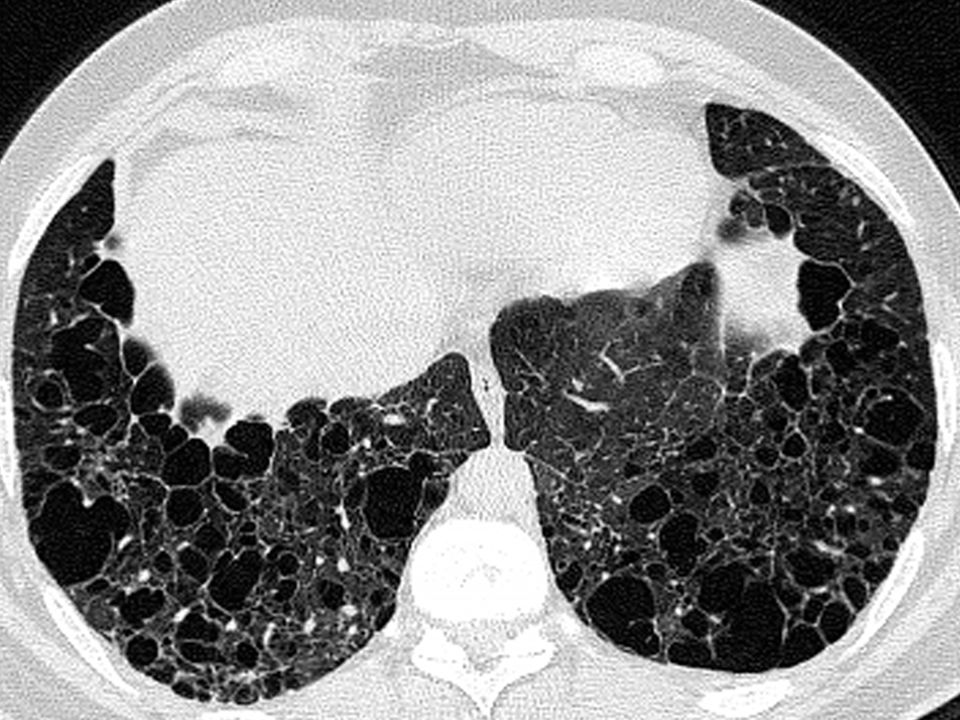
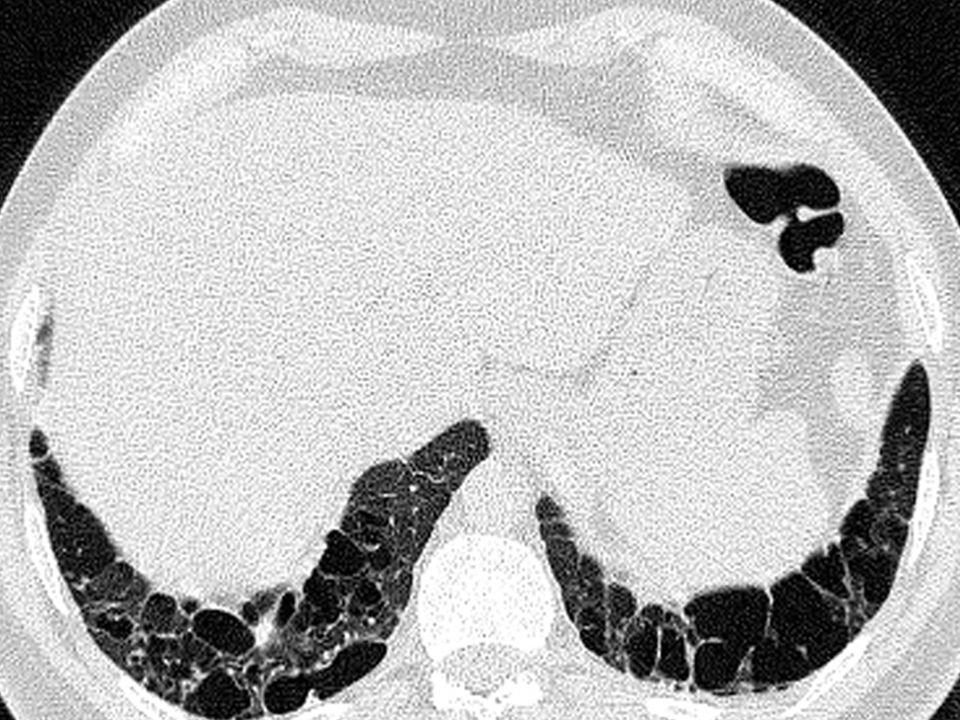
The frequency of cystic change reflects the timing ofimaging during the course of the disease. In the early stages, the most common finding is nodular change, whereas in the later stages, cystic change and fibrosis predominate. The combination of diffuse, irregularly shaped cystic spaces with small peribronchiolar nodular opacities, predominantly in the middle and upper lobe, is highly suggestive of pulmonary Langerhans’-cell histiocytosis. The presence of typical features on highresolution CT frequently allows the clinician to make a diagnosis of pulmonary Langerhans’-cell histiocytosis without lung biopsy (unless a definitive diagnosis is required). Although highly suggestive of pulmonary Langerhans’-cell histiocytosis, the typical pattern is not always present, and nonspecific patterns may be encountered.
. Although highly suggestive of pulmonary Langerhans’-cell histiocytosis, the typical pattern is not always present, and nonspecific patterns may be encountered.")
14
Biopsia quirurgica HISTIocitosis de CélulaS de langerhans PULMONAR
NO SON fotos del paciente.. Tengo que poner las citas de donde la saque????????????????? A Very Early Lesion of Pulmonary Langerhans’-Cell Histiocytosis along an Alveolar Duct with a Slight Increase in the Cellularity of the Walls of the Alveolar Duct and Associated Alveoli. Panel A shows an increase in pigmented alveolar macrophages typical of that seen in smokers (i.e., an accompanying respiratory bronchiolitis) (hematoxylin and eosin, ¬100). Panel B shows a detail of one of the alveolar duct walls. In the center, three or four Langerhans’ cells are recognizable (arrow); these cells were positive for S-100 protein (hematoxylin and eosin, ¬400). FIGURE 4. Immunostaining (haematoxylin and eosin) of an early lesion of pulmonary Langerhans’ cell histiocytosis with an antibody directed against CD1a. The bronchiole wall is infiltrated and partially destroyed by numerous Langerhans’ cells. Scale bar525 mm.
 (hematoxylin and eosin, ¬100). Panel B shows. a detail of one of the alveolar duct walls. In the center, three or. four Langerhans’ cells are recognizable (arrow); these cells were positive for S-100 protein (hematoxylin and eosin, ¬400). FIGURE 4. Immunostaining (haematoxylin and eosin) of an early lesion of. pulmonary Langerhans’ cell histiocytosis with an antibody directed against CD1a. The bronchiole wall is infiltrated and partially destroyed by numerous Langerhans’ cells. Scale bar525 mm.")
15
La Histiocitosis de Células de Langerhans (LCH) incluye un grupo de trastornos de causa desconocida con una gran variedad de presentaciones clínicas que se caracteriza por la infiltración de los tejidos afectados por células de Langerhans que se organizan en granulomas .
 incluye un grupo de trastornos de causa desconocida con una gran variedad de presentaciones clínicas que se caracteriza por la infiltración de los tejidos afectados por células de Langerhans que se organizan en granulomas .")
16
Clasificación de la Histiocitosis de células de langerhans
LETTERER SIWE MULTISISTÉMICA NIÑOS PEOR PRONÓSTICO 1)EXOFTALMOS 2)DIABETES INSÍPIDA 3)LESIONES LÍTICAS EN CRANEO HAND SCHÜLER CHRISTIAN MULTIFOCAL NIÑOS MAYORES/ADOLESCENTES PRONÓSTICO MÁS FAVORABLE The classification of LCH clinical patterns developed by the Histiocyte Society is based chiefly on the number of organs involved . Acute disseminated LCH (Letterer–Siwe disease) is a severe multisystemic disease that predominantly affects young children and less commonly older adults and carries a poor Multifocal LCH is seen mainly in older children and adolescents (Hand–Schu¨ ller–Christian syndrome or multifocal eosinophilic granuloma The classical triad of HSC disease – exophthalmos, diabetes insipidus, and calvarial lytic lesions – is seen only in one-third of patients. ) and runs a variable but usually more favourable course Single-system disease (eosinophilic granuloma and primary pulmonary histiocytosis) is characterised by the involvement of a single organ (bone, lungs or skin) and usually follows a benign course and can regress spontaneously [3– Pulmonary involvement in patients with multisystemic disease is rarely at the forefront of the clinical picture, yet may be of adverse prognostic significance Therefore, PLCH may occur as an isolated disorder or as a component of a multisystem illness. In the latter setting, the pulmonary disease does not usually dominate the clinical picture at presentation, but can contribute to morbidity and mortality Adults with LCH are more likely to have isolated PLCH; HUESO PULMÓN PIEL GRANULOMA EOSINOFILO/ HISTIOCITOSIS PULMONAR PRIMARIA UNO/ DOS ÓRGANOS ADULTOS PRONÓSTICO BENIGNO
EXOFTALMOS. 2)DIABETES INSÍPIDA. 3)LESIONES LÍTICAS EN CRANEO. HAND. SCHÜLER. CHRISTIAN. MULTIFOCAL. NIÑOS MAYORES/ADOLESCENTES. PRONÓSTICO MÁS FAVORABLE. The classification of LCH clinical patterns developed by the Histiocyte Society is based chiefly on the number of organs involved . Acute disseminated LCH (Letterer–Siwe disease) is a severe multisystemic disease that predominantly affects young children and less commonly older adults and carries a poor. Multifocal LCH is seen mainly in older children and adolescents (Hand–Schu¨ ller–Christian syndrome or multifocal eosinophilic granuloma The classical triad of HSC disease – exophthalmos, diabetes insipidus, and calvarial lytic lesions – is seen only in one-third of patients. ) and. runs a variable but usually more favourable course. Single-system disease (eosinophilic granuloma and primary pulmonary histiocytosis) is characterised by the involvement of a single. organ (bone, lungs or skin) and usually follows a benign course and can regress spontaneously [3– Pulmonary involvement in patients with multisystemic disease is rarely at the forefront. of the clinical picture, yet may be of adverse prognostic significance. Therefore, PLCH may occur as an isolated disorder or as a component of a multisystem illness. In the latter setting, the. pulmonary disease does not usually dominate the clinical picture at presentation, but can contribute to morbidity and mortality. Adults with LCH are more likely to have isolated PLCH; HUESO. PULMÓN. PIEL. GRANULOMA EOSINOFILO/ HISTIOCITOSIS PULMONAR PRIMARIA. UNO/ DOS ÓRGANOS. ADULTOS. PRONÓSTICO BENIGNO.")
17
•Rara enfermedad insterticial de causa desconocida
•Rara enfermedad insterticial de causa desconocida. •Compromiso pulmonar generalmente único. •Formación de granulomas de células de Langerhans que infiltran y destruyen los bronquiolos distales. •4-5% de las enfermedades insterticiales (biopsia quirúrgica). •20-40 años de edad. • = •Tabaquistas jovenes (90%). la histicitosis de celulas de langerhans pulmonar pulmonary involvement with Langerhans’ cell histiocytosis usually occurs as a single-system disease and is characterised by focal Langerhans’ cell granulomas infiltrating and destroying distal bronchioles PLCH predominantly affects young adults, with a frequency peak at 20–40 yrs of age . Female patients may be slightly older, particularly in the USA [15]. A marked male predominance was initially reported , but, in more recent studies, a similar proportion of males and females, or even a slight predominance of females, was observed, particularly in series from the USA These differences probably reflect smoking habit changes over time. en cuanto a la prevalencia Precise data regarding prevalence are not available, but a large series of hundreds of patients undergoing surgical lung biopsies for diffuse lung disease reported PLCH in 4-5% of all diffuse lung disease biopsies [9]. This is probably an under estimation as many patients may never undergo surgical lung biopsy for diagnosis. Hay paciente asintomaticos, no siempre es necesaria la obtencion de mustra para el diaagnostico y aunque tuvieramos tejido en estadios avanzados las celulas de langerhans pueden estar ausentes y no por eso excluiremos el diagnostico Indeed, the most striking epidemiological characteristic of adult PLCH is that 90–100% of patients are smokers (often smoking .20 cigarettes/dia) The prevalence of PLCH is, however, probably underestimated because some patients exhibit no symptoms or experience spontaneous remission,
. •20-40 años de edad. • = . •Tabaquistas jovenes (90%). la histicitosis de celulas de langerhans pulmonar pulmonary involvement with Langerhans’ cell histiocytosis usually occurs as a single-system disease and is characterised by focal Langerhans’ cell granulomas infiltrating and destroying distal bronchioles. PLCH predominantly affects young adults, with a frequency peak at 20–40 yrs of age . Female patients may. be slightly older, particularly in the USA [15]. A marked male predominance was initially reported , but, in more recent. studies, a similar proportion of males and females, or even a slight predominance of females, was observed, particularly in series from the USA These differences probably reflect smoking habit changes over time. en cuanto a la prevalencia Precise data regarding prevalence are not available, but a large series of hundreds of patients undergoing surgical lung biopsies. for diffuse lung disease reported PLCH in 4-5% of all diffuse lung disease biopsies [9]. This is probably an under estimation as many patients may never undergo. surgical lung biopsy for diagnosis. Hay paciente asintomaticos, no siempre es necesaria la obtencion de mustra para el diaagnostico y aunque tuvieramos tejido en estadios avanzados las celulas de langerhans pueden estar ausentes y no por eso excluiremos el diagnostico. Indeed, the most striking epidemiological characteristic of adult PLCH is. that 90–100% of patients are smokers (often smoking .20 cigarettes/dia) The prevalence of PLCH is, however, probably underestimated. because some patients exhibit no symptoms or experience. spontaneous remission,")
18
FORMAS DE PRESENTACIÓN
ASINTOMÁTICA PLCH is pleomorphic in its presentation Despite diffuse lung involvement, symptoms can be relatively minor or absent, and patients often initially attribute their symptoms to smoking.]. The diagnosis is usually made in one of the following three circumstances. 1) In ,25% of cases, the disease causes no symptoms and is detected on a routinechest radiograph. 2) Respiratory symptoms, mainly a dry cough and, somewhat less frequently, dyspnoea on exertion, are present in approximately two-thirds of cases and can be associated with constitutional manifestations (asthenia, fever, night sweats and weight loss). 3) Spontaneous pneumothorax responsible for chest pain leads to the diagnosis in ,10–20% of cases. The occurrence of pneumothorax seems more common in young males, may occur at any time during the course of the disease and may be bilateral and/or recurrent, Haemoptysis is uncommon and should not be attributed to PLCH until other causes (particularly lung cancer aspergiloma en cavida quistima in these smoking patients) have been ruled out PLCH in adults is usually a single-system disease. In the large majority of patients, there is no evidence for the involvement of other tissues. Bone lesions (,20% of patients), diabetesinsipidus with polyuria and polydipsia, resulting from infiltration of the posterior pituitary (5% of patients), and skinlesions are the most common extrapulmonary manifestations DISNEA / TOS SECA NEUMOTORAX ESPONTANEO MANIFESTACIONES EXTRAPULMONARES
 In ,25% of cases, the disease causes no symptoms and is detected on a routinechest radiograph. 2) Respiratory symptoms, mainly a dry cough and, somewhat less frequently, dyspnoea on exertion, are present in approximately two-thirds of cases and can be associated with constitutional manifestations (asthenia, fever, night sweats and weight loss). 3) Spontaneous pneumothorax responsible for chest pain leads to the diagnosis in ,10–20% of cases. The occurrence of pneumothorax seems more common in young males, may occur at any time during the course of the disease and may be bilateral and/or recurrent, Haemoptysis is uncommon and should not be attributed to PLCH until other. causes (particularly lung cancer aspergiloma en cavida quistima in these smoking patients) have been ruled out PLCH in adults is usually a single-system disease. In the large majority of patients, there is no evidence for the involvement of other tissues. Bone lesions (,20% of patients), diabetesinsipidus with polyuria and polydipsia, resulting from infiltration of the posterior pituitary (5% of patients), and skinlesions are the most common extrapulmonary manifestations. DISNEA / TOS SECA. NEUMOTORAX ESPONTANEO. MANIFESTACIONES EXTRAPULMONARES.")
19
T6MC (2014) 490 mts Borg0 2 Sat 96% % Obstrucc muy severa sin respuesta bd significativa con capacidad pulmonar normal atrapamiento aereo y dlco moderadamente disminuidaThe degree and extent of abnormalities on pulmonary- function testing depend on the extent of pulmonary involvement and the stage of disease. At the time of presentation, the results of pulmonaryfunction tests either are normal or demonstrate mild obstructive, restrictive, or mixed abnormalities. The most consistent abnormality is a reduction in the carbon monoxide diffusing capacity, which is present in 60 to 90 percent of patients. The degree of impairment in diffusing capacity appears to correlate with limitation in exercise performance. Mild obstructive physiologic findings were the most frequent lung-function abnormality reported in two series. In contrast, a recent study found mild restriction or normal spirometric results in the majority of patients. Evidence of obstructive changes on pulmonaryfunction testing may be due to cigarette smoking and concomitant chronic obstructive pulmonary disease, although this abnormality may also be due to the bronchiolar obstruction that results from the peribronchiolar distribution of the inflammatory and fibrotic lesions. In later stages of the disease, restriction may represent the physiologic correlate of extensive lung fibrosis. In some patients, predominantly cystic and bullous disease may develop later, resulting in increased lung volumes with variable degrees of obstruction.

20
EFR 2009 2012 2013 2014 FVC FEV1 FEV1/FVC DLCO T6MC MTS 3,63 (73%)
3,23 (62%) 3,18 (61%) 3,53 (68%) FEV1 2,06 (48%) 1,60 (32%) 1,98 (44%) 1,94 (45%) FEV1/FVC 56% 49% 60% 55% DLCO 31% 43% 45% T6MC MTS 400 330 317 490 %Sat inicial/final 100/97 94/77 93/79 96/76 No se si ponerla
 3,18 (61%) 3,53 (68%) FEV1. 2,06 (48%) 1,60 (32%) 1,98 (44%) 1,94 (45%) FEV1/FVC. 56% 49% 60% 55% DLCO. 31% 43% 45% T6MC. MTS %Sat inicial/final. 100/97. 94/77. 93/79. 96/76. No se si ponerla.")
21
Ecocardiograma con doppler
Dilatación severa de cavidades derechas Espesor parietal conservado FS VI conservada FS VD conservada IT leve que permite estimar PSAP 59mmhg (hipertensión pulmonar moderada a severa) No entiendo el informe del cateterismo
 No entiendo el informe del cateterismo.")
22
en esta publicacion se estudiaron 21 pacientes con histiocitosis de celulas de langrhans se estudio el fincional respiratorio y parametros hemodinamicos se obtuvo muestra histologica en mas del 50% de elllos y se observo que la hipertension pulmonar asociada a la histioctitosis x se debe al compromiso vascular intrinsico de la enfermedad (Intimal fibrosis of muscular pulmonary artery within Langerhans’ granuloma. may be observed histopathologically as intimal fibrosis and remodeling of both venous and arterial systems) mas alla del compromiso parenquimatoso y de la pequeña via aérea. Tambien se vio que comparado con otras enfermedades respiratorias cronicas los pacientes con histio desarrollan htp severa en este estudio la media de PSAP 59,,, el fev1 era mas bajo en EPOC y FP ..estaban peor funcionalmente y no presentaban HTP Progressive vascular involvement may occur in a minority of patients despite relative stability of pulmonary parenchymal lesions. Due to prognostic and potential therapeutic implications (personal observations), it is important to screen all patients for pulmonary hypertension. Although there is no universally accepted screening test for pulmonary hypertension, echocardiography is very useful in this context and provides a noninvasive approach to screen patients [99]. Our practice is to screen all patients at the time of diagnosis, particularly patients with dyspnea that seems to be out of proportion to degree of pulmonary function impairment. In patients with echocardiographic signs of possible pulmonary hypertension (elevated estimated right ventricular systolic pressure > 40 mmHg, or reduced right-sided cardiac function) it is prudent to consider cardiac catheterization with the goal of confirming the presence, defining the severity of pulmonary hypertension, and objectively determining the hemodynamic response to a vasodilator trial. When pulmonary hypertension is present, therapy with vasodilators including phosphodiesterase inhibitors or endothelin receptor antagonists may be of substantial benefit, and may result in objective reduction in pulmonary artery pressure and improved exercise capacity (unpublished observations). Epoprostenol (prostacyclin) can cause severe pulmonary edema and should be used very cautiously in this patient population given the prominent venous involvement and higher incidence of veno-occlusive disease
, it is. important to screen all patients for pulmonary hypertension. Although there is no universally accepted screening. test for pulmonary hypertension, echocardiography is very useful in this context and provides a noninvasive. approach to screen patients [99]. Our practice is to screen all patients at the time of diagnosis, particularly. patients with dyspnea that seems to be out of proportion to degree of pulmonary function impairment. In patients with echocardiographic signs of possible pulmonary hypertension (elevated estimated right ventricular systolic pressure > 40 mmHg, or reduced right-sided cardiac function) it is prudent to consider cardiac catheterization with the goal of confirming the presence, defining the severity of pulmonary hypertension, and objectively determining the hemodynamic response to a vasodilator trial. When pulmonary hypertension is present, therapy with vasodilators including phosphodiesterase inhibitors or endothelin receptor antagonists may. be of substantial benefit, and may result in objective reduction in pulmonary artery pressure and improved. exercise capacity (unpublished observations). Epoprostenol (prostacyclin) can cause severe pulmonary edema. and should be used very cautiously in this patient population given the prominent venous involvement and. higher incidence of veno-occlusive disease.")
23
PREDICTORES DE MAL PRONÓSTICO
* Lesiones quísticas extensas * Edad avanzada * FEV1/FVC * VR/TLC * DLCO * Hipertensión pulmonar En rojo los FR de mal pronostico de mi paCIENTE

24
*Diuresis inmensurable
ENFERMEDAD ACTUAL INTERROGATORIO *Polidipsia *Boca seca *Diuresis inmensurable Episodio de obnubilación, seguido de pérdida de conocimiento que motiva su hospitalización En marzo de 2014 presentó episodio súbito de obnubilación seguido de pérdida del conocimiento por lo cual fue hospitalizado

25
DIABETES INSÍPIDA Sodio plasmático Osmolaridad plasmática
Diuresis 12 litros/24 hs Sodio urinario Osmolaridad urinaria Densidad urinaria Glucosa en orina negativa D La bioquímica sanguinea mostró hipernatremia con osmolaridad plasmática aumentada, volumen urinario de 12 litros/24 hs con Sodio, Potasio y Cloro disminuidos, Densidad 0, cortisol libre urinario (CLU) y hormonas tiroideas dentro de valor normal. En TAC de cerebro no se observan áreas sugestivas de sangrado agudo y se complementa con RNM de cerebro en la que no se observan cambios significativos en la intensidad de señal a nivel del eje hipotálamo-hipofisiario. Se interpretó el cuadro como Diabetes Insípida secundaria al compromiso de la neurohipofisis por la enfermedad de base y se inició terapia de reemplazo hormonal con desmopresina via oral luego de la cual el paciente presentó mejoría sintomática y normalización de las pruebas de laboratorio. Cortisol libre urinario y hormonas tiroideas normales
 y hormonas tiroideas dentro de valor normal. En TAC de cerebro no se observan áreas sugestivas de sangrado agudo y se complementa con RNM de cerebro en la que no se observan cambios significativos en la intensidad de señal a nivel del eje hipotálamo-hipofisiario. Se interpretó el cuadro como Diabetes Insípida secundaria al compromiso de la neurohipofisis por la enfermedad de base y se inició terapia de reemplazo hormonal con desmopresina via oral luego de la cual el paciente presentó mejoría sintomática y normalización de las pruebas de laboratorio. Cortisol libre urinario y hormonas tiroideas normales.")
26
La Diabetes Insípida (DI) es un síndrome clínico que se caracteriza por la excresión de grandes volumenes de orina diluída asociada a una ingesta hídrica aumentada. Existen dos formas de DI: •CENTRAL (deficiencia de ADH) •NEFROGENICA (resistencia a ADH). DI of central origin most often results from lesions in the hypothalamic-neurohypophyseal axis. The differential diagnosis of central DI should include the pathologic processes (e.g. traumatic, infectious or inflammatory, and neoplastic) that involve the structures normally found in the pituitary gland or contiguous structures. However, idiopathic central DI is diagnosed when central DI occurs in the absence of any alteration that is known to be responsible for DI Sagittal T1-weighted MR image shows the normal anatomy of the sella turcica and juxtasellar region. The anterior lobe (thick arrow), posterior lobe (open arrow), pituitary stalk (thick arrowhead), optic chiasm (open arrowhead), mamillary body (M), and clivus (C) are indicated. In most healthy individuals, a normal posterior lobe appears hyperintense on T1 weighted MR images, due to phospholipid or secretory granules contained in pituicytes In longstanding DI, this high signal intensity of the posterior lobe is absent as a result of failure to synthesize, transport or store neurosecretory granules. After the administration of contrast material, the pituitary gland and pituitary stalk enhance homogeneously.
 that involve the structures normally found in the pituitary gland or contiguous structures. However, idiopathic central DI is diagnosed when central DI occurs in the absence of any alteration that is known to be responsible for DI. Sagittal T1-weighted MR image shows the normal anatomy of the sella turcica and juxtasellar region. The anterior lobe (thick arrow), posterior lobe (open arrow), pituitary stalk (thick arrowhead), optic chiasm (open arrowhead), mamillary body (M), and clivus (C) are indicated. In most healthy individuals, a normal posterior lobe appears hyperintense on T1 weighted MR images, due to. phospholipid or secretory granules contained in pituicytes In longstanding DI, this high signal intensity of. the posterior lobe is absent as a result of failure to synthesize, transport or store neurosecretory granules. After the. administration of contrast material, the pituitary gland and pituitary stalk enhance homogeneously.")
27
Lesiones óseas (20%) Diabetes Insípida (5%) Lesiones cutáneas
Manifestaciones extrapulmonares de la Histiocitosis de Células de Langerhans Pulmonar Lesiones óseas (20%) Diabetes Insípida (5%) Lesiones cutáneas PLCH in adults is usually a single-system disease. In the large majority of patients, there is no evidence for the involvement of other tissues. Bone lesions (,20% of patients), diabetes insipidus with polyuria and polydipsia, resulting from infiltration of the posterior pituitary (5% of patients), and skin lesions are the most common extrapulmonary manifestations
 Diabetes Insípida (5%) Lesiones cutáneas. PLCH in adults is usually a single-system disease. In the large. majority of patients, there is no evidence for the involvement of. other tissues. Bone lesions (,20% of patients), diabetes. insipidus with polyuria and polydipsia, resulting from. infiltration of the posterior pituitary (5% of patients), and skin. lesions are the most common extrapulmonary manifestations.")
28
Este es un trabajo con un n importante de pacientes con histiocitosis de cel de langerhans en los se se los siguio durante un poquito mas de 3 años y medio ,,, pero son pediatricos.. Y en elllos la forma mas frecuente es la multisistemica.. A diferencia de lo que ocurre en el adulto De poco mas de 1700 ptes con histiocitosis incluidos.. Completaron el estudio poco menos de 1200 pte (1183) De ellos 520 con enfemedad multisistemica 663 con enfermedad limitada a un organo o sistemica Ellos encontraron que de los 1700 iniciales 212 (”%) pte presentaron DI central.. 1o2 inicialmente y otros 110 a lo largo del seguimiento Ademas observaron que el padecer enfermedad multisistemica aumenta 4,7 mas la posibilidad de padecer DI Y el compromiso craneofacial oido ,ojo boca casi duplica 1,7 la posibilidad de tener DI independientemente de la extension dela enfermedad
 De ellos 520 con enfemedad multisistemica. 663 con enfermedad limitada a un organo o sistemica. Ellos encontraron que de los 1700 iniciales 212 ( %) pte presentaron DI central.. 1o2 inicialmente y otros 110 a lo largo del seguimiento. Ademas observaron que el padecer enfermedad multisistemica aumenta 4,7 mas la posibilidad de padecer DI. Y el compromiso craneofacial oido ,ojo boca casi duplica 1,7 la posibilidad de tener DI independientemente de la extension dela enfermedad.")
29
CONCLUSIONES Si bien la Histiocitosis de Células de Langerhans Pulmonar es una enfermedad que compromete en la mayoría de los pacientes el pulmón, un 15% de ellos pueden presentar compromiso extrapulmonar. Y esto tiene implicancias.. en el tratamiento.. Basicamente.. De la manifestación extrapulmonar Mala calidad de vida…TRH.. Pero En la revisión bibliográfica no encontré bibliografía que justifique el tratamiento de la histio por tener manifestaciones extrapulomonar El tratamiento en si con corticoides,, is se indica en las formas sistémicas (del pediatrico) y de los corticoides no existe evidencia (ECRC)a favor que modifique el efr,,, es todo opinión de expertos en ptes muy sintomáticos o con enfermedad progresiva.. Si en algunos trabajos se comenta que de los pacientes con histio que se trasplantaron la recurrencia de la enfermedad se asocio a la persistencia del habito tabáquico y en otros describen como fr de recaída la existencia de lesiones extrapulmonares en el momento del diagnostico.
 y de los corticoides no existe evidencia (ECRC)a favor que modifique el efr,,, es todo opinión de expertos en ptes muy sintomáticos o con enfermedad progresiva.. Si en algunos trabajos se comenta que de los pacientes con histio que se trasplantaron la recurrencia de la enfermedad se asocio a la persistencia del habito tabáquico y en otros describen como fr de recaída la existencia de lesiones extrapulmonares en el momento del diagnostico.")
30
cias Muchas gracias

Presentaciones similares



>")











>")






