Descargar la presentación
La descarga está en progreso. Por favor, espere

1
TIAZOLIDINEDIONAS GENERALIDADES

2
Objetivos Ubicar la resistencia a la Insulina como principal mecanismo fisiopatológico de la DM2. Describir el mecanismo de acción de las TZD’s (Tiazolidinedionas). Conocer las diferencias entre miembros de la familia de TZD’s. Identificar el vínculo entre DM2 y enfermedad cardiovascular. Definir e integrar el término “Memoria Metabólica” en el contexto del paciente con DM2.
. Conocer las diferencias entre miembros de la familia de TZD’s. Identificar el vínculo entre DM2 y enfermedad cardiovascular. Definir e integrar el término Memoria Metabólica en el contexto del paciente con DM2.")
3
Insulina y su receptor

4
Fisiopatología de la DM2
RESISTENCIA A LA INSULINA DEFICIENCIA DE INSULINA DEFICIENCIA DE INCRETINAS CONTRARREGULACIÓN PARADÓJICA

5
Concepto de “Resistencia” hormonal
Necesidad de mayores concentraciones de una hormona para lograr el mismo efecto. Existen bloqueos en uno o más puntos de la maquinaria metabólica que impiden que la hormona ejerza su efecto. Le “cuesta trabajo” llevar a cabo su acción.

6
Resistencia a la Insulina

7
Efecto de los AGL en Sensibilidad a la Insulina (Ciclo de Randle)
")
8
Efecto de los AGL en Sensibilidad a la Insulina (Ciclo de Randle)
")
9
Resistencia a la Insulina en el propio Islote
Lipotoxicidad / Glucotoxicidad

10
HISTORIA NATURAL DE LA DM2
abril de 2017 HISTORIA NATURAL DE LA DM2 Modificado de Groop L. Diabetes Obes Metab 1999

11
¿Qué recordar? La resistencia a la insulina es el principal mecanismo fisiopatológico de la DM2. La suma de factores genéticos y ambientales echa a andar mecanismos diversos que entorpecen la función metabólica. La resistencia a la insulina va de la mano de una depleción de la reserva pancreática de insulina. Existe RI también en el islote pancreático.

12
Familia de TZD’s Troglitazona fue voluntariamente retirada del mercado en Marzo de 2000 por toxicidad hepática.

13
Mecanismos de acción de TZD’s
RAPP RXR Transcripción génica COACTIVADORES LIGANDOS TZD TRANSACTIVACIÓN TRANSREPRESIÓN FN κB VÍAS INFLAMATORIAS VARIAS RAPP γ

14
Señalización insulina
Efectos de las TZD’s Masa de células β Proliferación de células β Apoptosis de células β Preservación insular Lipotoxicidad Glucotoxicidad Resistencia a la insulina: FNTα Captación de glucosa Adiponectina Señalización insulina Síntesis de Insulina Secreción de Insulina

15
TZD’s: Mecanismo de acción

16
TZD’s inciden sobre los defectos centrales de la DM2
Función de la célula Hasta el Diabetes Tipo 2 92% Ha disminuido un 50% de los pacientes con DM2 tienen Al momento del diagnóstico Resistencia a la Insulina Reducción en la Resistencia a la Pioglitazona Mejoría en la función de la célula 5-9 Insulina5-9 1.Haffner SM, D’Agostino R, Jr., Mykkanen L, et al. Insulin sensitivity in subjects with type 2 diabetes. Relationship to cardiovascular risk factors: the Insulin Resistance Atherosclerosis Study. Diabetes Care. 1999;22(4): 2. Lebovitz HE. Insulin secretagogues: old and new. Diabetes Reviews. 1999;7: 3. UK Prospective Diabetes Study Group. UK prospective diabetes study 16. Overview of 6 years’ therapy of type 2 diabetes: a progressive disease. Diabetes. 1995;44(11): 4. Aronoff S, Rosenblatt S, Braithwaite S, Egan JW, Mathisen AL, Schneider RL. Pioglitazone hydrochloride monotherapy improves glycemic control in the treatment of patients with type 2 diabetes: a 6-month randomized placebo-controlled dose-response study. The Pioglitazone 001 Study Group. Diabetes Care. 2000;23(11): 5. Tan MH, Baksi A, Krahulec B, et al. Comparison of pioglitazone and gliclazide in sustaining glycemic control over 2 years in patients with type 2 diabetes. Diabetes Care. 2005;28(3): 6. ACTOS SmPC, Takeda Global Research and Development Centre (Europe) Ltd, 26 Jan 2007. 7. Wallace TM, Levy JC, Matthews DR. An increase in insulin sensitivity and basal beta-cell function in diabetic subjects treated with pioglitazone in a placebo-controlled randomized study. Diabet Med. 2004;21(6): 8. Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in manDiabetologia. 1985;28(7): (HOMA)* *HOMA está basado en el siguiente cálculo: HOMA–%S = 22.5/(insulina en ayuno x glucosa en ayuno); HOMA–BCF = (20 x insulina en ayuno)/(Glucosa en ayuno – 3.5). 1. Xiang AH et al. Diabetes 2006;55;517– Haffner SM, D’Agostino R, Jr., Mykkanen L, et al. Diabetes Care. 1999;22(4): Lebovitz HE. Diabetes Reviews. 1999;7: UK Prospective Diabetes Study Group. Diabetes. 1995;44(11): Aronoff S, Rosenblatt S, Braithwaite S, et al. Diabetes Care. 2000;23(11): Tan MH, Baksi A, Krahulec B, et al. Diabetes Care. 2005;28(3): ACTOS SmPC, Takeda Global Research and Development Centre (Europe) Ltd, 26 Jan Wallace TM, Levy JC, Matthews DR. Diabet Med. 2004;21(6): Matthews DR, Hosker JP, Rudenski AS, et al. Diabetologia. 1985;28(7):
: Lebovitz HE. Insulin secretagogues: old and new. Diabetes Reviews. 1999;7: UK Prospective Diabetes Study Group. UK prospective diabetes study 16. Overview of 6 years’ therapy of type 2 diabetes: a progressive disease. Diabetes. 1995;44(11): Aronoff S, Rosenblatt S, Braithwaite S, Egan JW, Mathisen AL, Schneider RL. Pioglitazone hydrochloride monotherapy improves glycemic control in the treatment of patients with type 2 diabetes: a 6-month randomized placebo-controlled dose-response study. The Pioglitazone 001 Study Group. Diabetes Care. 2000;23(11): Tan MH, Baksi A, Krahulec B, et al. Comparison of pioglitazone and gliclazide in sustaining glycemic control over 2 years in patients with type 2 diabetes. Diabetes Care. 2005;28(3): ACTOS SmPC, Takeda Global Research and Development Centre (Europe) Ltd, 26 Jan Wallace TM, Levy JC, Matthews DR. An increase in insulin sensitivity and basal beta-cell function in diabetic subjects treated with pioglitazone in a placebo-controlled randomized study. Diabet Med. 2004;21(6): Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in manDiabetologia. 1985;28(7): (HOMA)* *HOMA está basado en el siguiente cálculo: HOMA–%S = 22.5/(insulina en ayuno x glucosa en. ayuno); HOMA–BCF = (20 x insulina en ayuno)/(Glucosa en ayuno – 3.5). 1. Xiang AH et al. Diabetes 2006;55;517– Haffner SM, D’Agostino R, Jr., Mykkanen L, et al. Diabetes Care. 1999;22(4): Lebovitz HE. Diabetes Reviews. 1999;7: UK Prospective Diabetes Study Group. Diabetes. 1995;44(11): Aronoff S, Rosenblatt S, Braithwaite S, et al. Diabetes Care. 2000;23(11): Tan MH, Baksi A, Krahulec B, et al. Diabetes Care. 2005;28(3): ACTOS SmPC, Takeda Global Research and Development Centre (Europe) Ltd, 26 Jan Wallace TM, Levy JC, Matthews DR. Diabet Med. 2004;21(6): Matthews DR, Hosker JP, Rudenski AS, et al. Diabetologia. 1985;28(7):")
17
Al vencer resistencia a la Insulina debe haber reducción de HbA1c
Pioglitazona Placebo Por un periodo de 3 años *P<0.01 HbA1c promedio (%) PROspective pioglitAzone Clinical Trial In macroVascular Events (PROactive) Randomized, double-blind, add-on PBO-controlled outcome study Type 2 diabetes (35-75 years old) with a history of macrovascular disease Managed with diet and/or OHAs Insulin Randomized to receive pioglitazone (45 mg/day) vs. placebo in addition to existing therapy Primary end point is the time from randomization to occurrence of a new macrovascular event or death Mean follow-up: 34.5 months Primary outcome: All-cause mortality, nonfatal AMI, nonfatal CVA, coronary revascularization, acute coronary syndrome, leg amputation, leg revascularization Secondary outcome: All-cause mortality, nonfatal AMI, nonfatal CVA Tiempo (meses) Adaptado de la Presentación Metabolic Results by Professor Bernard Charbonnel. Accesada el 12 de Febrero, 2008. .
 PROspective pioglitAzone Clinical Trial In macroVascular Events (PROactive) Randomized, double-blind, add-on PBO-controlled outcome study. Type 2 diabetes (35-75 years old) with a history of macrovascular disease. Managed with diet and/or OHAs Insulin. Randomized to receive pioglitazone (45 mg/day) vs. placebo in addition to existing therapy. Primary end point is the time from randomization to occurrence of a new macrovascular event or death. Mean follow-up: 34.5 months. Primary outcome: All-cause mortality, nonfatal AMI, nonfatal CVA, coronary revascularization, acute coronary syndrome, leg amputation, leg revascularization. Secondary outcome: All-cause mortality, nonfatal AMI, nonfatal CVA. Tiempo (meses) Adaptado de la Presentación Metabolic Results by Professor Bernard Charbonnel. Accesada el 12 de Febrero,")
18
El efecto sobre HbA1c es SOSTENIDO
Gliclazide 80 320 mg Pio 15 45 mg Por un periodo de 2 años HbA1c (%) P<0.01 Tan MH, Baksi A, Krahulec B, et al. Comparison of pioglitazone and gliclazide in sustaining glycemic control over 2 years in patients with type 2 diabetes. Diabetes Care. Mar 2005;28(3): Results from a 104-week, double-blind, randomised, double-dummy, multi-centre, parallel-group study using ACTOS 30 or 45 mg once-daily monotherapy. Completer analysis, n=147. Mean change at endpoint statistically significant vs baseline at P< Baseline HbA1c: 8.4%. OBJECTIVE— The hypothesis that pioglitazone treatment is superior to gliclazide treatment in sustaining glycemic control for up to 2 years in patients with type 2 diabetes was tested. RESEARCH DESIGN AND METHODS— This was a randomized, multicenter, double- blind, double-dummy, parallel-group, 2-year study. Approximately 600 patients from 98 centers participated. Eligible patients had completed a previous 12-month study and consented to continue treatment for a further year. To avoid selection bias, all patients from all centers were included in the primary analysis (a comparison of the time-to-failure distributions of the two groups by using a log-rank test) regardless of whether they continued treatment for a 2nd year. By using repeated-measures ANOVA, time course of least square means of HbA1c and homeostasis model of assessment (HOMA) indexes (HOMA-%S and HOMA-%B) were analyzed. RESULTS— A greater proportion of patients treated with pioglitazone maintained HbA1c 8% over the 2-year period than those treated with gliclazide. A difference between the Kaplan- Meier curves was apparent as early as week 32 and widened at each time point thereafter, becoming statistically significant from week 52 onward. At week 104, 129 (47.8%) of 270 pioglitazone-treated patients and 110 (37.0%) of 297 gliclazide-treated patients maintained HbA1c 8%. Compared with gliclazide treatment, pioglitazone treatment produced a larger decrease in HbA1c, a larger increase in HOMA-%S, and a smaller increase in HOMA-%B during the 2nd year of treatment. CONCLUSIONS— Pioglitazone is superior to gliclazide in sustaining glycemic control in patients with type 2 diabetes during the 2nd year of treatment. Años Adaptado de Tan MH, Baksi A, Krahulec B, et al. Diabetes Care. 2005;28(3):
 P<0.01. Tan MH, Baksi A, Krahulec B, et al. Comparison of pioglitazone and gliclazide in sustaining glycemic control over 2 years in patients with type 2 diabetes. Diabetes Care. Mar 2005;28(3): Results from a 104-week, double-blind, randomised, double-dummy, multi-centre, parallel-group study using ACTOS 30 or 45 mg once-daily monotherapy. Completer analysis, n=147. Mean change at endpoint statistically significant vs baseline at P< Baseline HbA1c: 8.4%. OBJECTIVE— The hypothesis that pioglitazone treatment is superior to gliclazide treatment. in sustaining glycemic control for up to 2 years in patients with type 2 diabetes was tested. RESEARCH DESIGN AND METHODS— This was a randomized, multicenter, double- blind, double-dummy, parallel-group, 2-year study. Approximately 600 patients from 98. centers participated. Eligible patients had completed a previous 12-month study and consented. to continue treatment for a further year. To avoid selection bias, all patients from all centers were. included in the primary analysis (a comparison of the time-to-failure distributions of the two. groups by using a log-rank test) regardless of whether they continued treatment for a 2nd year. By using repeated-measures ANOVA, time course of least square means of HbA1c and homeostasis. model of assessment (HOMA) indexes (HOMA-%S and HOMA-%B) were analyzed. RESULTS— A greater proportion of patients treated with pioglitazone maintained HbA1c. 8% over the 2-year period than those treated with gliclazide. A difference between the Kaplan- Meier curves was apparent as early as week 32 and widened at each time point thereafter, becoming statistically significant from week 52 onward. At week 104, 129 (47.8%) of 270. pioglitazone-treated patients and 110 (37.0%) of 297 gliclazide-treated patients maintained. HbA1c 8%. Compared with gliclazide treatment, pioglitazone treatment produced a larger. decrease in HbA1c, a larger increase in HOMA-%S, and a smaller increase in HOMA-%B during. the 2nd year of treatment. CONCLUSIONS— Pioglitazone is superior to gliclazide in sustaining glycemic control in. patients with type 2 diabetes during the 2nd year of treatment. Años. Adaptado de Tan MH, Baksi A, Krahulec B, et al. Diabetes Care. 2005;28(3):")
19
Algoritmo para la DM2 Sources: p. 8, Fig 2, including legend
a Sulfonylureas other than glybenclamide (glyburide) or chlorpropamide b Insufficient clinical use to be confident regarding safety Algorithm for the metabolic management of type 2 diabetes Reinforce Estilo de Vida interventions at every visit, check A1C every 3 months until A1C is <7% & then check A1C at least every 6 months If A1C is ≥7%, the interventions should be changed with rapid addition of medications, and transition to new regimens, when target glycemic goals not achieved or sustained (p. 7, 6th para) For Tier 2, if hypoglycemia is especially undesirable or if weight loss is a major consideration and A1C is <8.0%, exenatide is an option (p. 8, 3rd column, Tier 2) 19
 or chlorpropamide. b Insufficient clinical use to be confident regarding safety. Algorithm for the metabolic management of type 2 diabetes. Reinforce Estilo de Vida interventions at every visit, check A1C every 3 months until A1C is <7% & then check A1C at least every 6 months. If A1C is ≥7%, the interventions should be changed with rapid addition of medications, and transition to new regimens, when target glycemic goals not achieved or sustained (p. 7, 6th para) For Tier 2, if hypoglycemia is especially undesirable or if weight loss is a major consideration and A1C is <8.0%, exenatide is an option (p. 8, 3rd column, Tier 2) 19.")
20
Diferencias entre TZD´s
Diferencias bioquímicas Diferencias en expresión genética Diferencias clínicas Perfil lipídico Reduce recurrencia de IAM y EVC Prevención CV secundaria Perfil de seguridad Rev Clin Esp 2003;203(1):33-40
:")
21
Diferencias entre TZD’s
Expresión genética diferencial Rosiglitazona 17 23 19 Pioglitazona Adaptado de: Bioinformatics :3108

22
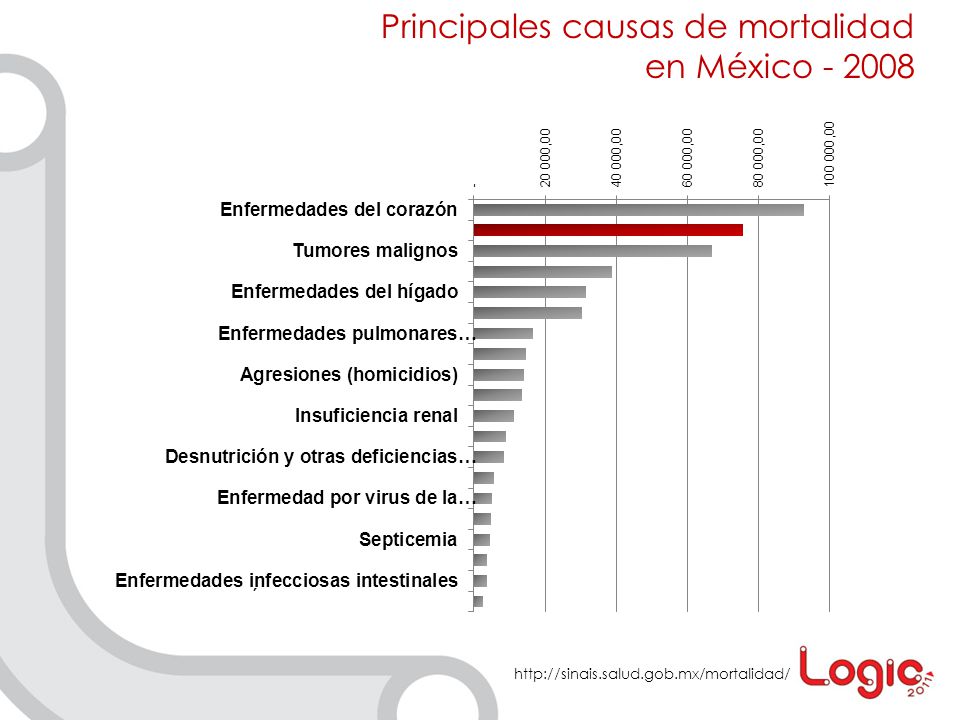
Enfermedad Cardiovascular PRINCIPAL CAUSA DE MORTALIDAD
EN DM2

23
Principales causas de mortalidad en México - 2008
24
DM2 y Enfermedad Cardiovascular
ECV DM2 HAS LÍPIDOS TABACO OBESIDAD INFLAMACIÓN

25
Factores de riesgo CV sobre los que inciden las TZD’s
ECV DM2 HAS LÍPIDOS TABACO OBESIDAD INFLAMACIÓN

26
TZD´s: Triglicéridos *p<0.001 entre grupos de tratamiento
Rosiglitazona Triglicéridos Medios (mg/dL)) Pioglitazona *p<0.001 entre grupos de tratamiento Goldberg et al., Diabetes Care; 28:1547, 2005
) Pioglitazona. *p<0.001 entre grupos de tratamiento. Goldberg et al., Diabetes Care; 28:1547,")
27
TZD´s: HDL-C *p<0.001 entre grupos de tratamiento Pioglitazona
Rosiglitazona *p<0.001 entre grupos de tratamiento Goldberg et al., Diabetes Care; 28:1547, 2005

28
Pioglitazona: efecto en TA
Estudio observacional, 4866 pacientes, 16 semanas. Pacientes previamente tratados con metformina. Edad 61 años, duración DM 6.7 años, A1c basal 7.8%. Basal A las 16 semanas TA sistólica (mmHg) 140±15 134±12 P<0.001 TA diastólica (mmHg) 83±9 80.5±7.5 DIABETES TECHNOLOGY & THERAPEUTICS (6):
 140± ±12. P< TA diastólica (mmHg) 83± ±7.5. DIABETES TECHNOLOGY & THERAPEUTICS (6):")
29
Riesgo de EVC o IAM recurrente en pacientes con DM2
↓47% J Am Col Cardiol 2007;49:1772 Stroke 2007;38:865 ↓28%

30
Seguridad CV – Rosiglitazona vs. Pioglitazona
Diabetes, Obesity and Metabolism 12: 1023–1035, 2010.

31
Rosiglitazone Revisited
An Updated Meta-analysis of Risk for Myocardial Infarction and Cardiovascular Mortality Steven E. Nissen, MD; Kathy Wolski, MPH Conclusions: Eleven years after the introduction of rosiglitazone, the totality of randomized clinical trials continue to demonstrate increased risk for MI although not for CV or all-cause mortality. The current findings suggest an unfavorable benefit to risk ratio for rosiglitazone. Arch Intern Med. Published online June 28, 2010. doi: /archinternmed

32
Risk of Acute Myocardial Infarction, Stroke, Heart Failure, and Death in Elderly Medicare Patients Treated With Rosiglitazone or Pioglitazone David J. Graham, MD, MPH TASA DE RIESGO 31% EVC 27% ICC 17% Mortalidad Rita Ouellet-Hellstrom, PhD Thomas E. MaCurdy, PhD Farzana Ali, BA Christopher Sholley, BS Christopher Worral, BS Jeffrey A. Kelman, MD, MMSc Conclusion Compared with prescription of pioglitazone, prescription of rosiglitazone was associated with an increades risk of stroke, hearth failure, and all-cause mortality and an increased risk of the composite of AMI, stroke, heart failure, of all-cause mortality in patients 65 years or older.

33
EMA: SUSPENSIÓN DEL MEDICAMENTO FDA: Programa de acceso restringido
Pioglitazona vs. Rosiglitazona 2010 EMA: SUSPENSIÓN DEL MEDICAMENTO FDA: Programa de acceso restringido

34
Candidatos al uso de Pioglitazona
Resistencia a la Insulina. HbA1c ≤ 8.5%. Hipertrigliceridemia con HDL bajo. Preocupación por el riesgo de hipoglucemia. Preocupación por el riesgo de complicaciones micro y macrovasculares. Requieren de prevención secundaria cardiovascular.

35
¿Qué recordar? Las TZD’s actúan en el núcleo de las células estimulando o bloqueando la expresión de genes . TZD’s vencen resistencia a la insulina (principal mecanismo fisiopatológico de la DM2). La enfermedad cardiovascular es la principal causa de mortalidad entre los diabéticos. Pioglitazona posee un perfil de protección cardiovascular global.
. La enfermedad cardiovascular es la principal causa de mortalidad entre los diabéticos. Pioglitazona posee un perfil de protección cardiovascular global.")
36
Es imprescindible dejar de considerar a la glucosa como elemento principal de la DM2.
ROMPER EL PARADIGMA GLUCOCÉNTRICO Durante el tiempo que invertimos en reducir la glucosa de ayuno de nuestros pacientes, la enfermedad cardiovascular va consumiendo a la mayoría, y a pesar de nuestros esfuerzos, nuevos medicamentos, etc., los pacientes siguen falleciendo en forma incrementada.

37
Memoria Metabólica Periodo de mal control Periodo de control intensivo
“Mala” memoria metabólica Tiempo desde el diagnosis (años) Diabetología (2009) 52:1219–1226
 Diabetología (2009) 52:1219–1226.")
38
Diabetes tipo 2, una enfermedad progresiva
UKPDS Diabetes tipo 2, una enfermedad progresiva Convencional Intensivo Límite superior del rango normal Años LANCET 1998; 572:

39
UKPDS a 10 años SU / Insulina – terapia inicial
Holman RR N Engl J Med 2008; 359:1577

40
LA MEMORIA METABÓLICA NOS OBLIGA A CONTROLAR AGRESIVAMENTE LA DIABETES DESDE ETAPAS TEMPRANAS.

41
¿Qué porcentaje de pacientes están alcanzando las metas de control?
China (CODIC-2)1 HbA1c < 7.5% 68% 32% EUA (NHANES)4 HbA1c < 7% 37% 63% 20% 80% México (ENSANUT2006) HbA1c < 7% Europa (CODE-2)5 HbA1c < 6.5% 43% 57% 31% 69% Latinoamérica (DEAL)3 HbA1c < 7% 1Xingbao C. Chinese Health Economics 2003; Ling T. China Diabetic Journal Harris SB, et al. Diabetes Res Clin Pract 2005; 70:90–97. 3Lopez Stewart G, et al. Rev Panam Salud Pública 2007; 22:12–20. 4Saydah SH, et al. JAMA 2004; 291:335–342. 5Liebl A, et al. Diabetología 2002; 45:S23–S28.
1. HbA1c < 7.5% 68% 32% EUA. (NHANES)4. HbA1c < 7% 37% 63% 20% 80% México. (ENSANUT2006) HbA1c < 7% Europa. (CODE-2)5. HbA1c < 6.5% 43% 57% 31% 69% Latinoamérica. (DEAL)3. HbA1c < 7% 1Xingbao C. Chinese Health Economics 2003; Ling T. China Diabetic Journal Harris SB, et al. Diabetes Res Clin Pract 2005; 70:90–97. 3Lopez Stewart G, et al. Rev Panam Salud Pública 2007; 22:12–20. 4Saydah SH, et al. JAMA 2004; 291:335–342. 5Liebl A, et al. Diabetología 2002; 45:S23–S28.")
42
Diabetes Technology & Therapeutics. June 2009, 11(6): 379-383
Nuevas Tendencias Competact, a Fixed Combination of Pioglitazone and Metformin, Improves Metabolic Markers in Type 2 Diabetes Patients with Insufficient Glycemic Control by Metformin Alone—Results from a Post-Marketing Surveillance Trial Under Daily Routine Conditions Thomas Schöndorf, Efstrathios Karagiannis, Richard E.K. Posseldt, Thomas Forst, Andreas Pfützner. Diabetes Technology & Therapeutics. June 2009, 11(6):
:")
43
PIOGLITAZONA + METFORMINA: MECANISMOS DE ACCIÓN DIFERENTES Y ADITIVOS
Mejora la resistencia a la insulina directamente. Incrementa la utilización de glucosa por el músculo. Efecto antiinflamatorio. Metformin Disminuye la producción hepática de glucosa. Sensibilizador central a la insulina. Se ha asociado a pérdida de peso en algunos pacientes. Improved blood glucose control Inzucchi SE. JAMA 2002; 287:360–372.

44
Pioglitazona + Metformina vs monoterapia
Current Medical Research & Opinion, (12):2915–2923
:2915–2923.")
45
Pioglitazona + Metformina: efectos adversos
MTF PIO/MTF Edema 4.2% 1.4% 3% Diarrea 2.6% 15% 9% Peso +1.6 Kg -1.3 Kg +0.7 Kg Hipoglucemia 0.5% 1.0% Current Medical Research & Opinion, (12):2915–2923
:2915–2923.")
46
BMC Endocr Disord. 2009 Jul 29;9:17
Act Now for the prevention of diabetes (ACT NOW) study Defronzo RA, Banerji M, Bray GA, Buchanan TA, Clement S, Henry RR, Kitabchi AE, Mudaliar S, Musi N, Ratner R, Reaven PD, Schwenke D, Stentz FB, Tripathy D Texas Diabetes Institute and University of Texas Health Science Center, San Antonio, TX, USA. BMC Endocr Disord Jul 29;9:17 Es necesario frenar un Mecanismo presente y bien identificado
 study. Defronzo RA, Banerji M, Bray GA, Buchanan TA, Clement S, Henry RR, Kitabchi AE, Mudaliar S, Musi N, Ratner R, Reaven PD, Schwenke D, Stentz FB, Tripathy D. Texas Diabetes Institute and University of Texas Health Science Center, San Antonio, TX, USA. BMC Endocr Disord Jul 29;9:17. Es necesario frenar un. Mecanismo presente y bien identificado.")
47
Pioglitazona vs iDPP IV
Pioglitazona 45mg. Sitagliptina100mg.2 Pacientes en metformina, HbA1c basal= 8.5%. Pioglitazona 30mg. Vildagliptina 100mg.1 Pacientes vírgenes al tratamiento, HbA1c basal = 8.7%. Rosenstock J, Baron MA, Camisasca RP, Cressier F, Couturier A, Dejager S. Efficacy and tolerability of initial combination therapy with vildagliptin and pioglitazone compared with component monotherapy in patients with type 2 diabetes. Diabetes Obes Metab. Mar 2007;9(2): Aim: The aim of this study was to compare efficacy and tolerability of initial combination therapy with vildagliptin/pioglitazone to component monotherapy. Methods: This 24-week, multicentre, randomized, double-blind, active-controlled study assessed the effects of the dipeptidyl peptidase-4 inhibitor vildagliptin (100 mg q.d.), pioglitazone (30 mg q.d.) and vildagliptin combined with pioglitazone (100/30 mg q.d. or 50/15 mg q.d.) in 607 drug-naive patients with type 2 diabetes (T2DM). The primary outcome measure was change from baseline in HbA1c in patients receiving initial combination therapy compared with pioglitazone monotherapy. Results: After 24-week treatment, adjusted mean changes in HbA1c from baseline (approximately 8.7%) in patients receiving pioglitazone monotherapy, 50/15 mg combination, 100/30 mg combination and vildagliptin monotherapy were −1.4 ± 0.1%, −1.7 ± 0.1%, −1.9 ± 0.1% and −1.1 ± 0.1% respectively. Both low-dose and high-dose combinations were significantly more efficacious than pioglitazone alone (p = and p < respectively). Adjusted mean changes in fasting plasma glucose were −1.9 ± 0.2, −2.4 ± 0.2, −2.8 ± 0.2 and −1.3 ± 0.2 mmol/l respectively, and both combination groups were significantly more effective than pioglitazone monotherapy (p = and p < respectively). The overall incidence of adverse events ranged from 45.8% in the low-dose combination to 51.6% in the pioglitazone monotherapy group. The incidence of peripheral oedema was highest in patients receiving pioglitazone monotherapy (9.3%) and lowest in those receiving low-dose combination (3.5%). One mild hypoglycaemic event was reported by one patient receiving high-dose combination and one patient receiving vildagliptin monotherapy. Conclusions: First-line treatment with vildagliptin/pioglitazone combination in patients with T2DM provides better glycaemic control than either monotherapy component yet has minimal risk of hypoglycaemia and a tolerability profile comparable with component monotherapy. Bolli G, Dotta F, Rochotte E, Cohen SE. Efficacy and tolerability of vildagliptin vs. pioglitazone when added to metformin: a 24-week, randomized, double-blind study. Diabetes Obes Metab. Jan 2008;10(1):82-90. Aim: The aim of this study was to compare the efficacy and tolerability of vildagliptin vs. pioglitazone as add-on therapy in patients with type 2 diabetes inadequately controlled with metformin monotherapy. Methods: This 24-week, multicentre, double-blind, randomized, active-controlled study compared vildagliptin (100 mg daily, given as equally divided doses, n = 295) and pioglitazone (30 mg daily, given as a single q.d. dose, n = 281) in patients with inadequate glycaemic control (A1C 7.5–11%) while receiving a stable metformin dose (≥1500 mg daily). The adjusted mean changes from baseline to study endpoint (AMΔ) in A1C, fasting plasma glucose (FPG), fasting lipids and body weight were compared by analysis of covariance. Results: When added to a stable dose of metformin (mean dose at baseline >2000 mg/day), both vildagliptin and pioglitazone decreased A1C (AMΔ = −0.9 ± 0.1% and −1.0 ± 0.1%, respectively) from identical baseline values (8.4 ± 0.1%). The between-group difference in AMΔ A1C was 0.1 ± 0.1%, and non-inferiority of vildagliptin to pioglitazone was established at both 0.4 and 0.3% margins for upper limit of the 95% confidence intervals. Pioglitazone decreased FPG (AMΔ = −2.1 ± 0.1 mmol/l) to a greater extent than vildagliptin (AMΔ = −1.4 ± 0.1 mmol/l), but only pioglitazone increased body weight (AMΔ = +1.9 ± 0.2 kg: between-group difference = −1.6 ± 0.3 kg, p < 0.001). Adverse events (AEs) were reported by 60% of vildagliptin-treated patients and by 56.4% of pioglitazone-treated patients; serious AEs were reported by 2.0 and 4.6% of patients receiving vildagliptin and pioglitazone respectively. Mild hypoglycaemia was reported by one patient (0.3%) in the vildagliptin group and by no patients receiving pioglitazone. Conclusions: When added to metformin, the efficacy of vildagliptin is non-inferior to that of pioglitazone. The treatments were similarly well tolerated, but only pioglitazone increased body weight. Diferencia media ponderada 0.3 (95% CI )3 1. Rosenstock J,. Diabetes Obes Metab. 2007;9(2): 2. ADA 69th Scientific Sessions, 6-LB 3. JAMA. 2007;298(2):
: Aim: The aim of this study was to compare efficacy and tolerability of initial combination therapy with vildagliptin/pioglitazone to component monotherapy. Methods: This 24-week, multicentre, randomized, double-blind, active-controlled study assessed the effects of the dipeptidyl peptidase-4 inhibitor vildagliptin (100 mg q.d.), pioglitazone (30 mg q.d.) and vildagliptin combined with pioglitazone (100/30 mg q.d. or 50/15 mg q.d.) in 607 drug-naive patients with type 2 diabetes (T2DM). The primary outcome measure was change from baseline in HbA1c in patients receiving initial combination therapy compared with pioglitazone monotherapy. Results: After 24-week treatment, adjusted mean changes in HbA1c from baseline (approximately 8.7%) in patients receiving pioglitazone monotherapy, 50/15 mg combination, 100/30 mg combination and vildagliptin monotherapy were −1.4 ± 0.1%, −1.7 ± 0.1%, −1.9 ± 0.1% and −1.1 ± 0.1% respectively. Both low-dose and high-dose combinations were significantly more efficacious than pioglitazone alone (p = and p < respectively). Adjusted mean changes in fasting plasma glucose were −1.9 ± 0.2, −2.4 ± 0.2, −2.8 ± 0.2 and −1.3 ± 0.2 mmol/l respectively, and both combination groups were significantly more effective than pioglitazone monotherapy (p = and p < respectively). The overall incidence of adverse events ranged from 45.8% in the low-dose combination to 51.6% in the pioglitazone monotherapy group. The incidence of peripheral oedema was highest in patients receiving pioglitazone monotherapy (9.3%) and lowest in those receiving low-dose combination (3.5%). One mild hypoglycaemic event was reported by one patient receiving high-dose combination and one patient receiving vildagliptin monotherapy. Conclusions: First-line treatment with vildagliptin/pioglitazone combination in patients with T2DM provides better glycaemic control than either monotherapy component yet has minimal risk of hypoglycaemia and a tolerability profile comparable with component monotherapy. Bolli G, Dotta F, Rochotte E, Cohen SE. Efficacy and tolerability of vildagliptin vs. pioglitazone when added to metformin: a 24-week, randomized, double-blind study. Diabetes Obes Metab. Jan 2008;10(1): Aim: The aim of this study was to compare the efficacy and tolerability of vildagliptin vs. pioglitazone as add-on therapy in patients with type 2 diabetes inadequately controlled with metformin monotherapy. Methods: This 24-week, multicentre, double-blind, randomized, active-controlled study compared vildagliptin (100 mg daily, given as equally divided doses, n = 295) and pioglitazone (30 mg daily, given as a single q.d. dose, n = 281) in patients with inadequate glycaemic control (A1C 7.5–11%) while receiving a stable metformin dose (≥1500 mg daily). The adjusted mean changes from baseline to study endpoint (AMΔ) in A1C, fasting plasma glucose (FPG), fasting lipids and body weight were compared by analysis of covariance. Results: When added to a stable dose of metformin (mean dose at baseline >2000 mg/day), both vildagliptin and pioglitazone decreased A1C (AMΔ = −0.9 ± 0.1% and −1.0 ± 0.1%, respectively) from identical baseline values (8.4 ± 0.1%). The between-group difference in AMΔ A1C was 0.1 ± 0.1%, and non-inferiority of vildagliptin to pioglitazone was established at both 0.4 and 0.3% margins for upper limit of the 95% confidence intervals. Pioglitazone decreased FPG (AMΔ = −2.1 ± 0.1 mmol/l) to a greater extent than vildagliptin (AMΔ = −1.4 ± 0.1 mmol/l), but only pioglitazone increased body weight (AMΔ = +1.9 ± 0.2 kg: between-group difference = −1.6 ± 0.3 kg, p < 0.001). Adverse events (AEs) were reported by 60% of vildagliptin-treated patients and by 56.4% of pioglitazone-treated patients; serious AEs were reported by 2.0 and 4.6% of patients receiving vildagliptin and pioglitazone respectively. Mild hypoglycaemia was reported by one patient (0.3%) in the vildagliptin group and by no patients receiving pioglitazone. Conclusions: When added to metformin, the efficacy of vildagliptin is non-inferior to that of pioglitazone. The treatments were similarly well tolerated, but only pioglitazone increased body weight. Diferencia media ponderada 0.3. (95% CI )3. 1. Rosenstock J,. Diabetes Obes Metab. 2007;9(2): ADA 69th Scientific Sessions, 6-LB. 3. JAMA. 2007;298(2):")
48
Sitagliptina vs Pioglitazona en combinación con Metformina
Adaptado de Lancet 2010;376:431

49
¿Qué recordar? La “Memoria Metabólica” nos obliga a tomar el control de la DM2 en forma estricta desde etapas tempranas. La mezcla Pioglitazona + Metformina es ideal para frenar un proceso que no sólo lleva al paciente a desarrollar DM2, sino que prevalece durante toda su historia. Pioglitazona tiene mecanismos de acción muy distintos a los iDPP IV y no son sustituibles.

Presentaciones similares



















