Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Ponente: Dr. Diego Arias Rodríguez
Anestesiología y Reanimación Moderador: Dr. Jesús Rico Feijoó

2
TODO UN RETO

3
MORTALIDAD: 1400 /día 40-60% INCIDENCIA: 50-95 casos/100000habit

4
EMERGENTE

5
Declaración de Barcelona (2002) Guidelines (2004)
Reducir la mortalidad de la sepsis severa un 25% en 5 años Declaración de Barcelona (2002) Guidelines (2004) Aplicación, valoración y aprendizaje
 Guidelines (2004) Aplicación, valoración y aprendizaje.")
6
DECLARACIÓN DE BARCELONA

7
GUIDELINES American Association of Critical Care Nurses
American College of Chest Physicians American College of Emergency Physicians American Thoracic Society Australian and New Zealand Intensive Care Society European Society of Clinical Microbiology and Infectious Diseases European Society of Intensive Care Medicine European Respiratory Society International Sepsis Forum Society of Critical Care Medicine Surgical Infection Society

9
APLICACIÓN VALORACIÓN APRENDIZAJE
3ª FASE APLICACIÓN VALORACIÓN APRENDIZAJE

11
Sepsis Sepsis severa Shock séptico
vs Sepsis severa Shock séptico

12
SIRS 1/3 Tª > 38 o < 36ºC Fc > 90 lpm
Fr > 20 rpm o paCO2 < 32 mmHg o VM Leucos > o < 4000 o >10% cayados 1/3 PROBABILIDAD 2 Criterios: 32% 3 Criterios: 36% 4 Criterios: 45%

13
SEPSIS Infección documentada o sospechada +
Tª > 38.3ºC o < 36ºC FcC > 90 lpm Taquipnea Alteración nivel de conciencia Edema importante o balance + Gluc > 120 mg/dl Leuc > o < 4000 Desv izqda Prot C react > 2 SD Procalcitonina > 2 SD SvcO2 > 70% IC > 3.5

14
SEPSIS SEVERA Sepsis FRACASO ORGÁNICO HIPOTENSIÓN HIPOPERFUSIÓN
PaO2 / FIO2 < 300 Oliguria aguda Creat > 2 mg/dl INR > 1.5 o TTPa > 60´´ Plaq < / ul BT > 2 mg/dl HIPOPERFUSIÓN Lactato > 2 mmol/l HIPOTENSIÓN SBP < 90 mmHg MAP < 70 mmHg SBP > 40 mmHg

15
A pesar de reposición de volumen
SHOCK SÉPTICO Fallo circulatorio agudo inexplicable por otras causas SBP < 90mmHg, MAP < 60 Descenso SBP > 40 mmHg A pesar de reposición de volumen

16
CORTICOTERAPIA SHOCK REFRACTARIO TAM > 60 mmHg pero:
Dopa > 0.15 mcg/kg/min Noradr > 0.25 mcg/kg/min CORTICOTERAPIA

17
SCREENING

18
Sepsis Sepsis severa Shock séptico
vs Sepsis severa Shock séptico

19
HERRAMIENTA DE DESPISTAJE

20
HERRAMIENTA DE DESPISTAJE

21
SCREENING LÁCTICO

22
ÁCIDO LÁCTICO (arterial)
Metabolismo anaerobio Hipoperfusión con o sin hipotensión >4 Shock séptico

23
SCREENING LÁCTICO FOCO DE INFECCIÓN HEMOCULTIVOS ANTIBIOTERAPIA

24
HEMOCULTIVOS Antes de AB Al menos 2 30-50% son + Protocolo Grado D
Uno de cada acceso vascular que lleve más de 48h y otro nuevo 30-50% son + Protocolo Grado D

25
ANTIBIOTERAPIA < 3 o 1 hora Susceptibilidad Amplio espectro
Grado E < 3 o 1 hora Susceptibilidad Amplio espectro Asociaciones Penetración Revisión cada horas Descalonamiento Grado B Grado E

26
SCREENING FOCO DE INFECCIÓN MEDIDAS ESPECÍFICAS MANEJO HEMODINÁMICO
LÁCTICO FOCO DE INFECCIÓN MEDIDAS ESPECÍFICAS HEMOCULTIVOS MANEJO HEMODINÁMICO ANTIBIOTERAPIA

27
OBJETIVOS 1ª 6 h PVC 8-12 mmHg PAM > 65mmHg
Diuresis > 0.5 ml/Kg/h SvcO2 > 70% Grado B

28
In-hospital mortality (all patients)
The Importance of Early Goal-Directed Therapy for Sepsis Induced Hypoperfusion NNT to prevent 1 event (death) = 6-8 60 Standard therapy EGDT 50 40 Mortality (%) 30 20 10 In-hospital mortality (all patients) 28-day mortality 60-day mortality Adapted from Table 3, page 1374, with permission from Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med 2001; 345:
 = Standard therapy. EGDT Mortality (%) In-hospital mortality (all patients) 28-day mortality. 60-day mortality. Adapted from Table 3, page 1374, with permission from Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med 2001; 345:")
29
FLUIDOTERAPIA HIPOPERFUSIÓN No esperar HIPOTENSIÓN
Lactato > 4 mmol/l HIPOTENSIÓN SBP < 90 mmHg MAP < 70 mmHg SBP > 40 mmHg No esperar

30
Cristaloides: 500-1000ml/30min >Vol de disribución
FLUIDOTERAPIA Grado E FLUID CHALLENGE: Cristaloides: ml/30min Coloide: ml/30min Mínimo: 20 ml/kg de cristaloide o su coloide correspondiente ( g/kg). Edema agudo de pulmón >Vol de disribución >Cantidad >Edema Más baratos OBJETIVO PVC: 8-12 mmHg
. Edema agudo de pulmón. >Vol de disribución. >Cantidad. >Edema. Más baratos. OBJETIVO. PVC: 8-12 mmHg.")
31
VASOPRESORES Dopamina: Noradr:
Si PAM < 65 mmHg a pesar de fluidoterapia Dopamina: Fc y VS TAM y GC Mejora función sistólica Más taquicardia y más arritmias Noradr: TAM por vasoconstricción directa Más potente Grado D

32
Si no hay respuesta pensar en :
Vasopresina: Vasoconstrictor directo uds/min No afecta al crono ni inotropismo GC y Flujo hepatoesplénico Si no hay respuesta pensar en : Depresión de la función miocárdica Insuficiencia adrenal Neumotórax a tensión Taponamiento cardiaco

33
SCREENING FOCO DE INFECCIÓN MEDIDAS ESPECÍFICAS MANEJO HEMODINÁMICO
LÁCTICO FOCO DE INFECCIÓN MEDIDAS ESPECÍFICAS HEMOCULTIVOS MANEJO HEMODINÁMICO ANTIBIOTERAPIA HIPOTENSIÓN y/o LACTATO>4 FLUIDOTERAPIA PAM<65 VASOPRESORES

34
SHOCK SÉPTICO y/o LÁCTICO>4
PVC = 8 – 12 mmHg SvO2 > 70% Si HTO< 30% : C de Hm Dobutamina (máximo 20 g/kg/min) Si TAM baja: añadir vasopresores (hasta TAM > 65) Grado B
 Si TAM baja: añadir vasopresores (hasta TAM > 65) Grado B.")
35
CATÉTER VENOSO CENTRAL
ScVO2 Consumo de oxígeno Baja: Aumento demandas Incapacidad del GC para las demandas PVC: Reposición de fluidos Aumenta en VM con PEEP

36
SCREENING FOCO DE INFECCIÓN MEDIDAS ESPECÍFICAS MANEJO HEMODINÁMICO
LÁCTICO FOCO DE INFECCIÓN MEDIDAS ESPECÍFICAS HEMOCULTIVOS MANEJO HEMODINÁMICO ANTIBIOTERAPIA HIPOTENSIÓN y/o LACTATO>4 SHOCK y/o LACTATO>4 FLUIDOTERAPIA SvcO>70% PAM<65 PVC: 8-12 C de Hm DOBUTAMINA VASOPRESORES

37
OBJETIVOS 1ª 6 h PVC 8-12 mmHg PAM > 65mmHg
Diuresis > 0.5 ml/Kg/h SvcO2 > 70% Grado B

38
SCREENING FOCO DE INFECCIÓN MEDIDAS ESPECÍFICAS MANEJO HEMODINÁMICO
LÁCTICO FOCO DE INFECCIÓN MEDIDAS ESPECÍFICAS HEMOCULTIVOS MANEJO HEMODINÁMICO ANTIBIOTERAPIA HIPOTENSIÓN y/o LACTATO>4 SHOCK y/o LACTATO>4 FLUIDOTERAPIA SvcO>70% PAM<65 PVC: 8-12 C de Hm DOBUTAMINA VASOPRESORES

39
SCREENING FOCO DE INFECCIÓN MEDIDAS ESPECÍFICAS MANEJO HEMODINÁMICO
LÁCTICO FOCO DE INFECCIÓN MEDIDAS ESPECÍFICAS HEMOCULTIVOS MANEJO HEMODINÁMICO MEDIDAS GENERALES ANTIBIOTERAPIA CORTICOIDES HIPOTENSIÓN y/o LACTATO>4 SHOCK y/o LACTATO>4 GLUCEMIA rhAPC FLUIDOTERAPIA VENTILACIÓN SvcO>70% PAM<65 PVC: 8-12 C de Hm DOBUTAMINA VASOPRESORES

40
¿ CORTICOTERAPIA ? Insuficiencia adrenal relativa (50-75%)
Resistencia periférica a los corticoides Efectos sobre el tono vascular Efecto sobre la respuesta inflamatoria Aumenta la supervivencia

41
CORTICOTERAPIA Si requiere vasopresores HIDROCORTISONA
mg/día (7días) No usar dosis mayores Test ACTH?? Cuando y como retirarlos??? Sin miedo a la inmunosupresión Grado C Grado A
 No usar dosis mayores. Test ACTH Cuando y como retirarlos Sin miedo a la inmunosupresión. Grado C. Grado A.")
42
CORTICOTERAPIA SHOCK REFRACTARIO TAM > 60 mmHg pero:
Dopa > 0.15 mcg/kg/min Noradr > 0.25 mcg/kg/min CORTICOTERAPIA

43
CORTICOTERAPIA Si requiere vasopresores HIDROCORTISONA
mg/día (7días) No usar dosis mayores Test ACTH?? Cuando y como retirarlos??? Sin miedo a la inmunosupresión
 No usar dosis mayores. Test ACTH Cuando y como retirarlos Sin miedo a la inmunosupresión.")
44
DROTRECOGIN ALFA (ACTIVADO)
Anticoagulante endógeno con propiedades antinflamatorias Indicaciones: APACHE > 25 y/o Shock séptico Fracaso multiorgánico SDRA-Sepsis Contraindicaciones: Sangrado activo ACV hace menos de 3m TCE severo, Cx SNC menos de 2m Tx con riesgo de hemorragia Cateter epidural Tumor cerebral Grado B

45
Results: 28-Day All-Cause Mortality
Primary analysis results 2-sided p-value Adjusted relative risk reduction 19.4% Increase in odds of survival 38.1% 35 30.8% Placebo (n-840) 30 6.1% absolute reduction in mortality 24.7% Drotrecogin alfa (activated) (n=850) 25 20 Mortality (%) Activated protein C when administered in a blinded, randomized fashion to over 1600 patients with severe sepsis and septic shock produced a 6.1% absolute reduction in mortality. 15 10 5 Adapted from Table 4, page 704, with permission from Bernard GR, Vincent JL, Laterre PF, et al. Efficacy and safety of recombinant human activated protein C for severe sepsis. N Engl J Med 2001; 344:
 % absolute reduction in mortality. 24.7% Drotrecogin alfa (activated) (n=850) Mortality (%) Activated protein C when administered in a blinded, randomized fashion to over 1600 patients with severe sepsis and septic shock produced a 6.1% absolute reduction in mortality Adapted from Table 4, page 704, with permission from Bernard GR, Vincent JL, Laterre PF, et al. Efficacy and safety of recombinant human activated protein C for severe sepsis. N Engl J Med 2001; 344:")
46
Mortality and Numbers of Organs Failing
Percent Mortality 10 20 30 40 50 60 1 2 3 4 5 Placebo Drotrecogin Number of Organs Failing at Entry The European regulatory authority lists multiple organ failure as the indication for rhAPC therapy in severe sepsis. This is based on subset analysis indicating that patients with multiple organ failure are most likely to benefit. Adapted from Figure 4, page S91, with permission from Bernard GR. Drotrecogin alfa (activated) (recombinant human activated protein C) for the treatment of severe sepsis. Crit Care Med 2003; 31[Suppl.]:S85-S90
 (recombinant human activated protein C) for the treatment of severe sepsis. Crit Care Med 2003; 31[Suppl.]:S85-S90.")
47
CONTROL DE GLUCEMIA Reduce la mitad la prevalencia de: Bacteriemias
Inflamación prolongada IRA con hemodiálisis o ultrafiltración Polineuropatía del crítico Necesidades transfusionales

48
CONTROL DE GLUCEMIA <150 mg/dl Bomba de infusión de Insulina
Glucosa o dieta (evitar hipogluc) Monitorización: Inicial: min Estabilizado: 4 horas Grado D Grado E
 Monitorización: Inicial: min. Estabilizado: 4 horas. Grado D. Grado E.")
49
VENTILACIÓN DE PROTECCIÓN
Grado B P plateau <30cmH2O Vt bajos (6ml/kg) Hipercapnia permitida No si HIC o acidosis láctica PEEP Según FiO2 Decúbito prono SDRA con FiO2 o PEEP elevadas Semiincorporado a 45º Grado C Grado E Grado E Grado C
 Hipercapnia permitida. No si HIC o acidosis láctica. PEEP. Según FiO2. Decúbito prono. SDRA con FiO2 o PEEP elevadas. Semiincorporado a 45º. Grado C. Grado E. Grado E. Grado C.")
50
ARDSnet Mechanical Ventilation Protocol
Results: Mortality 40 35 30 25 6 ml/kg 20 % Mortality 12 ml/kg The ARDSnet trial compared 6 ml/kg ideal body weight vs. 12 ml/kg ideal body weight (low tidal volume/high tidal volume comparison). The low tidal volume group demonstrated a significant decrease in mortality. 15 10 5 Adapted from Figure 1, page 1306, with permission from The Acute Respiratory Distress Syndrome Network. N Engl J Med 2000;342:
. The low tidal volume group demonstrated a significant decrease in mortality Adapted from Figure 1, page 1306, with permission from The Acute Respiratory Distress Syndrome Network. N Engl J Med 2000;342:")
51
BUNDLE RESUCITACIÓN Láctico Hemocultivos previos a la antibióterapia
Antibioterapia de amplio espectro (3-1hora) Si hipotensión y/o lactato >4 Fluid challenge Si no responde vasopresores (TAM>65 mmHg) Shock séptico y/o lactato >4 (objetivos: PVC >8mmHg y SvO2>70%) Concentrados de Hm si HTO <30% Dobutamina
 Si hipotensión y/o lactato >4. Fluid challenge. Si no responde vasopresores (TAM>65 mmHg) Shock séptico y/o lactato >4. (objetivos: PVC >8mmHg y SvO2>70%) Concentrados de Hm si HTO <30% Dobutamina.")
52
SCREENING FOCO DE INFECCIÓN MEDIDAS ESPECÍFICAS MANEJO HEMODINÁMICO
LÁCTICO FOCO DE INFECCIÓN MEDIDAS ESPECÍFICAS HEMOCULTIVOS MANEJO HEMODINÁMICO MEDIDAS GENERALES ANTIBIOTERAPIA CORTICOIDES HIPOTENSIÓN y/o LACTATO>4 SHOCK y/o LACTATO>4 GLUCEMIA rhAPC FLUIDOTERAPIA VENTILACIÓN SvcO>70% PAM<65 PVC: 8-12 C de Hm DOBUTAMINA VASOPRESORES

53
BUNDLE MANEJO Corticoides a bajas dosis Drotrecogin alfa activado
Glucemias <150mg/dl Ventilación protectora

54
SCREENING FOCO DE INFECCIÓN MEDIDAS ESPECÍFICAS MANEJO HEMODINÁMICO
LÁCTICO FOCO DE INFECCIÓN MEDIDAS ESPECÍFICAS HEMOCULTIVOS MANEJO HEMODINÁMICO MEDIDAS GENERALES ANTIBIOTERAPIA CORTICOIDES HIPOTENSIÓN y/o LACTATO>4 SHOCK y/o LACTATO>4 GLUCEMIA rhAPC FLUIDOTERAPIA VENTILACIÓN SvcO>70% PAM<65 PVC: 8-12 C de Hm DOBUTAMINA VASOPRESORES

55
SCREENING FOCO DE INFECCIÓN MEDIDAS ESPECÍFICAS MANEJO HEMODINÁMICO
LÁCTICO FOCO DE INFECCIÓN MEDIDAS ESPECÍFICAS HEMOCULTIVOS MANEJO HEMODINÁMICO ANTIBIOTERAPIA HIPOTENSIÓN y/o LACTATO>4 SHOCK y/o LACTATO>4 FLUIDOTERAPIA SvcO>70% PAM<65 PVC: 8-12 C de Hm DOBUTAMINA VASOPRESORES

57
SCREENING FOCO DE INFECCIÓN MEDIDAS ESPECÍFICAS MANEJO HEMODINÁMICO
LÁCTICO FOCO DE INFECCIÓN MEDIDAS ESPECÍFICAS HEMOCULTIVOS MANEJO HEMODINÁMICO MEDIDAS GENERALES ANTIBIOTERAPIA CORTICOIDES HIPOTENSIÓN y/o LACTATO>4 SHOCK y/o LACTATO>4 GLUCEMIA rhAPC FLUIDOTERAPIA VENTILACIÓN SvcO>70% PAM<65 PVC: 8-12 C de Hm DOBUTAMINA VASOPRESORES

58
OTRAS

59
ESTADÍOS SIRS SEPSIS SEPSIS GRAVE SEPSIS GRAVE DE ALTO RIESGO
SHOCK SÉPTICO

60
SEPSIS Tª > 38 o < 36ºC Fc > 90 lpm
Fr > 20 rpm o paCO2 < 32 mmHg o Vm Leucos > o < 4000 o >10% cayados SIRS + Infección documentada clínica y/o microbiológicamente

61
Grados de la evidencia:
Grados de las recomendaciones: A: Basada en al menos dos estudios de nivel I B: Basada en un solo estudio de nivel I C: Basada en estudios de nivel II D: Basada en estudios de nivel III E: Basada en estudios de nivel IV o V Grados de la evidencia: I: Ensayos aleatorizados de tamaño grande con resultados concluyentes II: Ensayos aleatorizados de tamaño pequeño con resultados inciertos III: Estudios no aleatorizados con controles concurrentes IV: Estudios no aleatorizados con controles históricos, y opinión de expertos V: Series de casos, estudios no controlados, y opinión de expertos

62
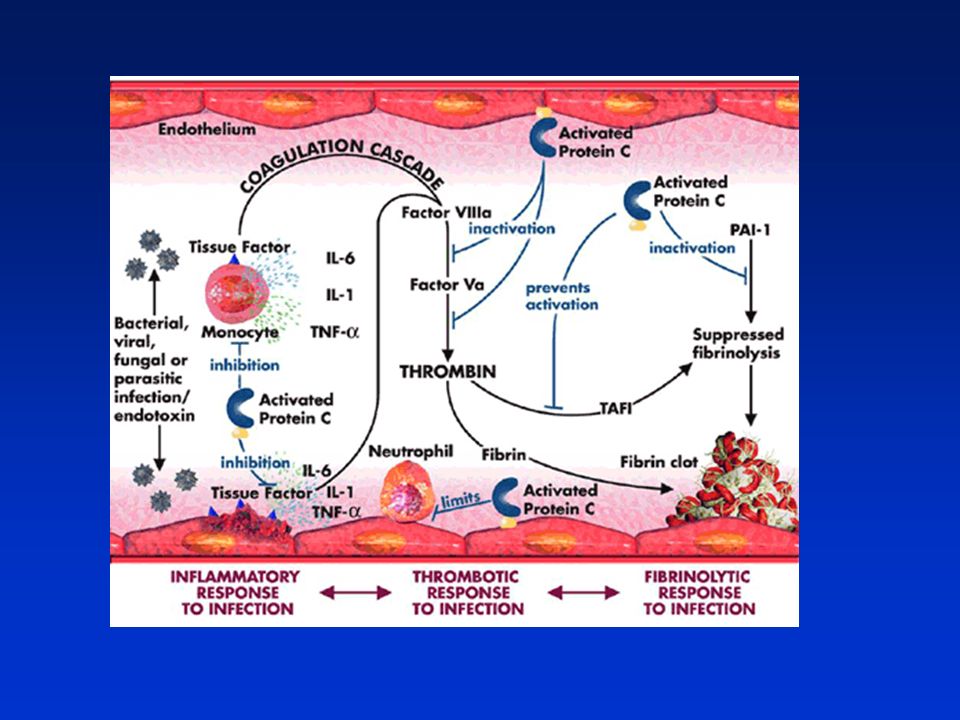
FISIOPATOLOGÍA SEPSIS Reacción inflamatoria (IL-6, TNF-α,...)
HIPOPERFUSIÓN Descenso de la P de perfusión por hipotensión Redistrib vascular del GC (puede estar n o ) Alteración celular SHOCK DISTRIBUTIVO
 Alteración celular. SHOCK DISTRIBUTIVO.")
63
Capillary blood flow (mL/min/100 g) 6.0 + 1.6 5.8 + 11 5.3 + 0.9
MAP Urinary output (mL) 49 +18 43 +13 .60/.71 Capillary blood flow (mL/min/100 g) .59/.55 Red Cell Velocity (au) .74/.97 Pico2 (mm Hg) 41 + 2 47 + 2 46 + 2 .11/.12 Pa-Pico2 (mm Hg) 13 + 3 17 + 3 16 + 3 .27/.40 75 mm Hg 65 mm Hg 85 mm Hg F/LT Adapted from Table 4, page 2731, with permission from LeDoux, Astiz ME, Carpati CM, Rackow ED. Effects of perfusion pressure on tissue perfusion in septic shock. Crit Care Med 2000; 28:
 /.71. Capillary blood flow (mL/min/100 g) /.55. Red Cell. Velocity (au) /.97. Pico2 (mm Hg) /.12. Pa-Pico2 (mm Hg) / mm Hg. 65 mm Hg. 85 mm Hg. F/LT. Adapted from Table 4, page 2731, with permission from LeDoux, Astiz ME, Carpati CM, Rackow ED. Effects of perfusion pressure on tissue perfusion in septic shock. Crit Care Med 2000; 28:")
65
Mortality and APACHE II Quartile
118:80 50 Placebo 45 Drotrecogin 40 58:48 35 57:49 30 Mortality (percent) 25 20 26:33 15 10 The FDA labeling for rhAPC indicates use for patients with sepsis induced organ dysfunction associated with a high risk of death, such as APACHE II of 25 or greater. This is based on subset analysis of the four APACHE II quartiles in the rhAPC clinical trial showing that most of the benefit occurred in patients with APACHE II of 25 or greater. 5 1st (3-19) 2nd (20-24) 3rd (25-29) 4th (30-53) APACHE II Quartile *Numbers above bars indicate total deaths Adapted from Figure 2, page S90, with permission from Bernard GR. Drotrecogin alfa (activated) (recombinant human activated protein C) for the treatment of severe sepsis. Crit Care Med 2003; 31[Suppl.]:S85-S90
 : The FDA labeling for rhAPC indicates use for patients with sepsis induced organ dysfunction associated with a high risk of death, such as APACHE II of 25 or greater. This is based on subset analysis of the four APACHE II quartiles in the rhAPC clinical trial showing that most of the benefit occurred in patients with APACHE II of 25 or greater. 5. 1st (3-19) 2nd (20-24) 3rd (25-29) 4th (30-53) APACHE II Quartile. *Numbers above bars indicate total deaths. Adapted from Figure 2, page S90, with permission from Bernard GR. Drotrecogin alfa (activated) (recombinant human activated protein C) for the treatment of severe sepsis. Crit Care Med 2003; 31[Suppl.]:S85-S90.")
66
Previo al intento de destete:
Estar despierto Hemodinámicamente estable (sin vasopresores) Sin nuevas complicaciones Baja ventilación y bajas PEEP Requerir uno niveles de FiO2 fácilmente alcanzables con gafas o ventimask
 Sin nuevas complicaciones. Baja ventilación y bajas PEEP. Requerir uno niveles de FiO2 fácilmente alcanzables con gafas o ventimask.")
67
SUSTITUCIÓN RENAL BICARBONATO
Hemodinámicamente estable: HVVC = Hemodiálisis intermitente Inestable: HVVC Grado B BICARBONATO No si pH > 7.15 Grado C

68
Changing pH Has Limited Value
Treatment Before After NaHCO3 (2 mEq/kg) pH PAOP 15 17 Cardiac output 0.9% NaCl pH PAOP 14 17 Cardiac output Cooper DJ, et al. Ann Intern Med 1990; 112:
 pH PAOP Cardiac output % NaCl. pH PAOP Cardiac output Cooper DJ, et al. Ann Intern Med 1990; 112:")
69
PROFILAXIS TVP ÚLCERAS DE ESTRÉS
Grado A Heparinas no fraccionadas o de bajo Pm Si contraindicación Medios físicos Alto riesgo: Heparina + Medios Físicos ÚLCERAS DE ESTRÉS Anti H2 Grado C

70
HEMODERIVADOS I Sin hipoperfusión ni circunstancias estenuantes, como acidosis láctica, enfermedad coronaria, hemorragia aguda. Transfundir si Hb < 7g/dl Objetivo 7-9 g/dl Plasma fresco congelado: Sangrado Cx próxima Grado B Grado E

71
Transfusion Strategy in the Critically Ill
Figure 2A, page 414, reproduced with permission from Hebert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. N Engl J Med 1999; 340:

72
HEMODERIVADOS II No EPO No AT-III Plaquetas: < 5000: Transfundir
: Si riesgo de sangrado <50000: Si sangrado o Cx próxima Grado E

73
A clinician, armed with the sepsis bundles, attacks the three heads of severe sepsis: hypotension, hypoperfusion and organ dysfunction. Crit Care Med 2004; 320(Suppl):S595-S597
:S595-S597.")
74
Actual title of painting is “Hercules Kills Cerberus,” by Renato Pettinato, Painting hangs in Zuccaro Place in Agira, Sicily, Italy. Used with permission of artist and the Rubolotto family.

75
Surviving Sepsis Phase 1 Barcelona declaration
Phase 2 Evidence based guidelines Paediatric issues Phase 3 Implementation and education Although there is limited data available from prospective clinical trials in pediatric septic patients, there are considerable differences in the pathophysiology of pediatric sepsis that warrants comment.

76
Fluid Resuscitation Aggressive fluid resuscitation with boluses of 20 ml/kg over 5-10 min Blood pressure by itself is not a reliable endpoint for resuscitation Initial resuscitation usually requires ml/kg, but more may be required Fluid resuscitation of pediatric patients is weight based and aggressive, with initial resuscitation of 20ml/kg and often up to 40–60ml/kg required during the initial resuscitation. Blood pressure itself is not a reliable endpoint for resuscitation. Physical exam, urine output, and pulse response are the primary response monitors.

77
Hemodynamic Support Hemodynamic profile may be variable
Dopamine for hypotension Epinephrine or norepinephrine for dopamine-refractory shock Dobutamine for low cardiac output state Inhaled NO useful in neonates with post-partum pulmonary hypertension and sepsis The hemodynamic profile of pediatric sepsis is quite variable. Dopamine with its combined inotrope and vasopressor characteristics is recommended for pediatric hypotension because of the tendency for a lower cardiac output in this patient population. Epinephrine or norepinephrine are then added for dopamine refractory shock. When cardiac output is measured, dobutamine is recommended for low cardiac output states. Inhaled nitric oxide may be useful in neonates who are septic with post-partum pulmonary hypertension.

78
Therapeutic Endpoints
Capillary refill < 2 sec Warm extremities Urine output > 1 ml/kg/hr Normal mental status Decreased lactate Central venous O2 saturation > 70% Physical exam findings indicating successful resuscitation include a capillary refill < 2sec, warm extremities, and normal mental status. Other objective targets include urine output > 1ml/kg/hr and normalization of lactate, and as in the adult, central venous O2 sat 70%.

79
Other Therapies Steroids: recommended for children with catecholamine resistance and suspected or proven adrenal insufficiency. Activated protein C not studied adequately in children yet. GM-CSF shown to be of benefit in neonates with sepsis and neutropenia. Extracorporeal membrane oxygenation (ECMO) may be considered in children with refractory shock or respiratory failure. As in adults, steroids are recommended for children with catecholamine resistance and suspected or proven adrenal insufficiency. Activated protein C has not been studied in pediatric severe sepsis. Unlike adults GM-CSF has been shown to be of benefit in neonates in circumstances of neutropenia and sepsis. ECMO, not recommended in adults, may be useful in children with refractory shock or respiratory failure.
 may be considered in children with refractory shock or respiratory failure. As in adults, steroids are recommended for children with catecholamine resistance and suspected or proven adrenal insufficiency. Activated protein C has not been studied in pediatric severe sepsis. Unlike adults GM-CSF has been shown to be of benefit in neonates in circumstances of neutropenia and sepsis. ECMO, not recommended in adults, may be useful in children with refractory shock or respiratory failure.")
Presentaciones similares