Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Insuficiencia cardíaca congestiva
Jorge Brenes, MD San José, Costa Rica

2
DEFINICIÓN “Situación en la cual el corazón es
incapaz de mantener un gasto cardiaco adecuado a los requerimientos metabólicos y al retorno venoso.” Definition of Heart Failure. There is no single definition of heart failure. Classically, heart failure is understood as the situation when the heart is incapable of maintaining a cardiac output adequate to accommodate the body’s metabolic requirements and the venous return. This concept is ambiguous and incomplete, however, because heart failure is a composite of clinical symptoms, physical signs, and abnormalities on the hemodynamic, neurohormonal, biochemical, anatomic and cellular levels. In addition, the actual cardiac output, venous return or absolute metabolic requirements are not usually measured in clinical practice. Heart failure is a syndrome characterized by symptoms and physical signs which are secondary to a change in function of the ventricles, valves or load conditions. Braunwald E.: Heart Diseases. W.B. Saunders Co E. Braunwald

3
“Síndrome clínico que se manifiesta por disnea y fatiga en reposo o ejercicio, con daño estructural y/o funcional miocárdico, con desarrollo de un proceso de remodelación y alteraciones neurohormonales.” Dr. Jorge Brenes

4
IC es una pandemia creciente, especialmente en la vejez, que determina gran impacto en economía, morbi y mortalidad. IC afecta 2-4 millones de residentes de USA y más de 15 millones en todo el mundo. NHLBI estima que el 75% de los pacientes con IC tienen antecedentes de HTA, 22% de hombres y 46% de mujeres víctimas de IMA desarrollarán IC en 6 años Es la mayor causa de hospitalización en USA en mayores de 65 años y la mitad de los pacientes son mayores de 65 años (prevalencia en Framinghan de 10/1000). El 40-50% tienen FE normales.
. El 40-50% tienen FE normales.")
5
Algunas estadísticas:
En USA hospitalizaciones como DX primario. 164% de aumento en hospitalizaciones en los últimos 15 años. 12-15 millones de visitas al médico/año. 6.5 millones de días hospital/año. Mortalidad hospitalaria: 5-8% Mortalidad anual para algunos pacientes: 40-60% 6 medicamentos promedio/paciente 78% con al menos 2 hospitalizaciones/año. 20% re-hospitalizados en 6 meses Diagnóstico de egreso más frecuente en mayores de 65 años. Costo: US$23.7 billones en 2004

7
Causas de aumento en la frecuencia
Envejecimiento de la población Mejoría en la sobrevida en infarto del miocardio (unidad coronaria y trombolisis) Reducción en la morbimortalidad en HTA debido a un mejor control Aumento en la prevalencia de cardiomiopatía idiopática
 Reducción en la morbimortalidad en HTA debido a un mejor control. Aumento en la prevalencia de cardiomiopatía idiopática.")
8
Estudio Framingham Mortalidad Muerte súbita
62 % en hombres a los 5 años 42% en mujeres a los 5 años 75% después de 9 años del inicio clínico Muerte súbita 25% en hombres, 13% en mujeres

9
Etiología Sobrecarga de volumen Sobrecarga de presión
Pérdida de miocardio Disminución en la contractilidad Restricción al llenado

11
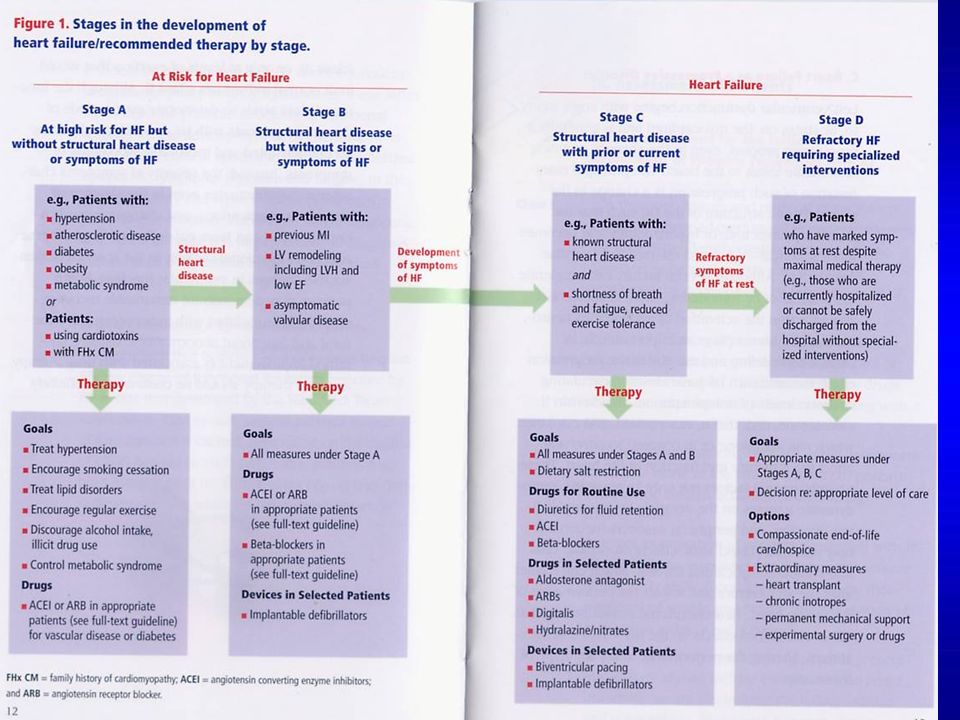
Las guías recientes establecen pacientes en riesgo de IC (ACC estadío A) y la prioridad es la TERAPIA PREVENTIVA. Pacientes ACC estadío D representan sólo el 10% de la población total en IC, tienen la mayor mortalidad a corto plazo y consumen el mayor porcentaje de recursos. Un análisis de 6 países reveló que el 1-2% del total de gastos en salud eran para IC, y el 70% de ellos por gastos de hospitalización. Una valoración de costos en Europa determinó US$ para trasplante, US$ para asistencia ventricular mecánica y US$ para desfibrilador implantable.

12
Varios factores de riesgo influyen en las tasas de mortalidad: edad, disfunción renal, DM y FA.
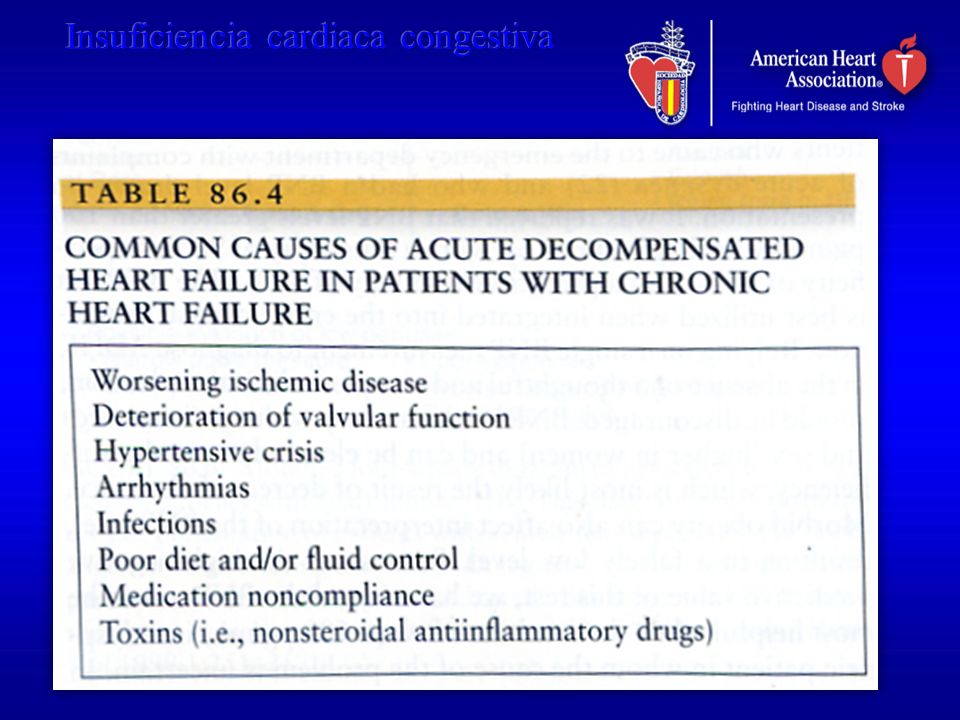
Un estudio canadiense demostró que la mayor mortalidad se puede establecer en minutos post-admisión y los factores de riesgo incluyen: mayor edad, TA sistólica, F. Resp, BUN e hiponatremia. Condiciones co-mórbidas: ECV, EBOC, cirrosis hepática, demencia y cáncer. En el estudio ADHERE (Acute Decompensated Heart Failure National Registry) los predictores fueron BUN > 43, TA ≤ 115, creat ≥ 2.75
 los predictores fueron BUN > 43, TA ≤ 115, creat ≥")
13
EVOLUCION DE ESTADIOS CLINICOS
Insuficiencia cardiaca congestiva EVOLUCION DE ESTADIOS CLINICOS NORMAL No síntomas Ejercicio normal Fx VI normal Disfunción VI asintomática No síntomas Ejercicio normal Fx VI alterada ICC compensada Important Concepts. Clinical stages in the evolution of heart failure Heart failure is a continuous spectrum of changes, from the subtle loss of normal function to the presence of symptoms refractory to medial therapy. The patient with cardiomyopathy may maintain overall normal ventricular function; the progression of dysfunction may be sudden or gradual. Asymptomatic ventricular dysfunction is characterized by the absence of symptoms or decline in functional capacity, even in the absence of treatment. It may be associated with different changes in cardiac physiology, including ventricular dilatation, regional wall motion abnormalities, and decreases in the LV ejection fraction and of other parameters of ventricular function. The absence of symptoms may be explained by the heart’s functional reserve capacity and by the activation of compensatory mechanisms opposing the deterioration of cardiac function. In compensated heart failure the symptoms are controlled by medical therapy. In decompensated heart failure, symptoms persist despite usual therapy and are refractory to adjustments in drugs and dosages. No síntomas ejercicio Fx VI alterada ICC descompensada Síntomas ejercicio Fx VI alterada ICC refractaria Síntomas no controlados con tratamiento

14
DETERMINANTES DE LA FUNCION VENTRICULAR
CONTRACTILIDAD PRECARGA POSTCARGA VOLUMEN LATIDO Pathophysiology of Congestive Heart Failure. Determinants of ventricular function. Ventricular function, and cardiac function in general, depends upon the interaction of four factors that regulate the volume of blood expelled by the heart (the cardiac output): contractility, preload, afterload, and heart rate. The first three determine the volume of blood expelled with each beat (the stroke or ejection volume), while the heart rate affects the cardiac output by varying the number of contractions per unit time. These four factors, which are intrinsic regulators of heart function, are all influenced by the nervous system. In the failing heart, especially in ischemic heart disease, it is also important to consider some purely mechanical factors, such as the synergy of ventricular contraction, the integrity of the septum, and the competence of the atrioventricular valves. - Contracción sinergística VI - Integridad pared VI - Competencia valvular FRECUENCIA CARDIACA GASTO CARDIACO
: contractility, preload, afterload, and heart rate. The first three determine the volume of blood expelled with each beat (the stroke or ejection volume), while the heart rate affects the cardiac output by varying the number of contractions per unit time. These four factors, which are intrinsic regulators of heart function, are all influenced by the nervous system. In the failing heart, especially in ischemic heart disease, it is also important to consider some purely mechanical factors, such as the synergy of ventricular contraction, the integrity of the septum, and the competence of the atrioventricular valves. - Contracción sinergística VI - Integridad pared VI - Competencia valvular. FRECUENCIA CARDIACA. GASTO CARDIACO.")
15
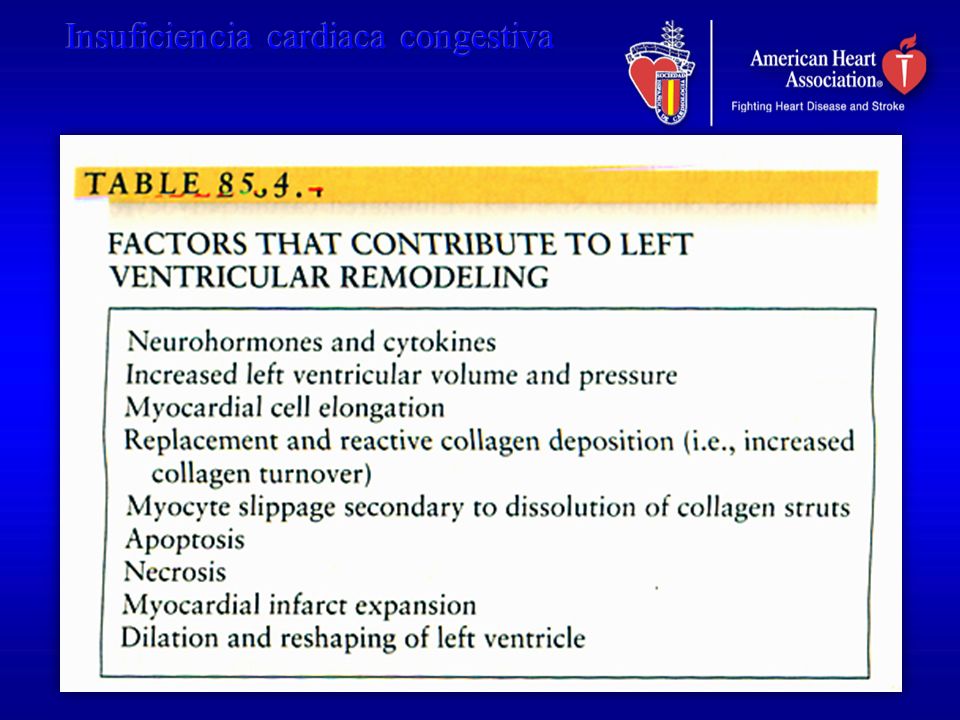
Remodelación SRAA y SS La remodelación ventricular es la que determina la historia natural de la IC en la mayoría de las circunstancias y es el principal objetivo de la terapia actualmente. Remodelación es el cambio en tamaño y forma del corazón, involucrando usualmente el VI. El distintivo de la IC sistólica es la remodelación progresiva. Contrario a la expansión del IMA, la remodelación progresiva del VI es un proceso más gradual que ocurre en meses o años posterior al evento. La distorsión en la arquitectura miocárdica predispone a arritmias artriales y ventriculares.

16
La hipótesis neuroendocrina establece que la liberación temprana en IC antes de que aparezcan signos y síntomas, contribuye en forma importante a la remodelación progresiva del VI y la historia natural de la IC. En IC los sistemas RAA y S representan sistemas conservadores altamente eficientes para adaptarse a la depleción de volumen. En IC el SRRA está permanentemente activado. Hipokalemia y excesiva actividad simpática pueden también contribuir a muerte súbita en IC (20% de muertes en IC y mayor en NYHA II).
.")
17
Una anormalidad funcional sistólica se define como una disminución en la habilidad del corazón insuficiente para desarrollar fuerza y acortar a una determinada velocidad y condiciones de llenado establecidas. El límite de elongación de la sarcómera según Frank Starling es 2.2 µg.

20
Síntomas y signos Disnea Disnea de esfuerzo Ortopnea
Disnea paroxística nocturna Ritmo de galope Crépitos pulmonares o sibilancias Edema

25
OBJETIVOS DEL TRATAMIENTO
Sobrevida Morbilidad Capacidad ejercicio Calidad de vida Cambios neurohormonales Progresión de ICC Síntomas Treatment of Heart Failure. Objectives The objectives of treatment of the patient with heart failure are many, but they may be summarized in two principles: decrease symptoms and prolong life. In daily practice, the first priority is symptom control and the best plan is to adjust to the individual patient’s particular circumstances over the course of therapy. Nevertheless, the rest of the listed objectives should not be forgotten, as medical therapy now has the potential for decreasing morbidity (hospital admissions, embolism, etc.), increasing exercise capacity (all of the usually prescribed drugs), improve the quality of life, control neurohormonal changes (ACE-I, beta blockers), retard progression (ACEI) and prolong life.
, increasing exercise capacity (all of the usually prescribed drugs), improve the quality of life, control neurohormonal changes (ACE-I, beta blockers), retard progression (ACEI) and prolong life.")
26
Clasificación funcional New York Heart Association
Clase I. La actividad física acostumbrada no provoca síntomas (fatiga, palpitaciones, disnea, angor). Clase II. La actividad física acostumbrada provoca síntomas. Clase III. La actividad física menor que la acostumbrada provoca síntomas. Clase IV. Síntomas en reposo.
. Clase II. La actividad física acostumbrada provoca síntomas. Clase III. La actividad física menor que la acostumbrada provoca síntomas. Clase IV. Síntomas en reposo.")
27
Corrección de factores agravantes
TRATAMIENTO Corrección de factores agravantes Embarazo Arritmias (FA) Infecciones Hipertiroidismo Tromboembolismo Endocarditis Obesidad Hipertensión Actividad física Excesos en dieta Treatment of Heart Failure. Correction of aggravating factors Often a lack of response to conventional therapy for heart failure is due to the presence of uncorrected aggravating or precipitating factors. It is important to always consider the possibility of such factors, particularly in cases of refractory failure. AF: atrial fibrillation. MEDICACIONES
 Infecciones. Hipertiroidismo. Tromboembolismo. Endocarditis. Obesidad. Hipertensión. Actividad física. Excesos en dieta. Treatment of Heart Failure. Correction of aggravating factors. Often a lack of response to conventional therapy for heart failure is due to the presence of uncorrected aggravating or precipitating factors. It is important to always consider the possibility of such factors, particularly in cases of refractory failure. AF: atrial fibrillation. MEDICACIONES.")
28
TERAPIA FARMACOLOGICA
TRATAMIENTO TERAPIA FARMACOLOGICA DIURETICOS INOTROPICOS VASODILATORES ANTAGONISTAS NEUROHORMONALES OTROS (Anticoagulantes, antiarrítmicos, etc.) Treatment of Heart Failure. Drugs This is a simple and pragmatic classification of the vast numbers and types of medications in the pharmacopoeia for the treatment of heart failure.
 Treatment of Heart Failure. Drugs. This is a simple and pragmatic classification of the vast numbers and types of medications in the pharmacopoeia for the treatment of heart failure.")
29
EFECTOS HEMODINAMICOS Presión de llenado ventricular
DROGAS EFECTOS HEMODINAMICOS Normal A I Volumen latido A + V V Treatment of Heart Failure. Theoretical hemodynamic effects of different drugs for heart failure Effects of different treatments on the relationship between ventricular filling pressure (LVEDP) and stroke volume. Diuretics (D) and venous vasodilators (V) decrease the ventricular filling pressure in patients with heart failure and normal or elevated LVEDP, but except in patients with marked elevation of LVEDP, the stroke volume does not change. The pure arterial vasodilators (A) produce an increase in the stroke volume in patients with failure and an elevated LVEDP. Inotropic drugs (I) increase the stroke volume with a lesser effect of the ventricular filling pressure. ICC D Presión de llenado ventricular
 and stroke volume. Diuretics (D) and venous vasodilators (V) decrease the ventricular filling pressure in patients with heart failure and normal or elevated LVEDP, but except in patients with marked elevation of LVEDP, the stroke volume does not change. The pure arterial vasodilators (A) produce an increase in the stroke volume in patients with failure and an elevated LVEDP. Inotropic drugs (I) increase the stroke volume with a lesser effect of the ventricular filling pressure. ICC. D. Presión de llenado ventricular.")
30
Disminución mortalidad
TERAPIA FARMACOLOGICA Mejoría síntomas Disminución mortalidad Prevención de ICC Control neurohormonal DIURETICOS si ? ? NO DIGOXINA si = mínima si INOTROPICOS si mort. no ? Treatment of Heart Failure. Effect of the principle pharmacologic groups on the majority of symptoms, reduction in mortality, prevention of symptom development and control of neurohormonal abnormalities. The drugs which control neurohormonal abnormalities include ß-blockers, ACE inhibitors, dopaminergic receptor stimulants, and digoxin. si Vasodil.(Nitratos) si ? no I - Eca si SI si SI Otras drogas control neurohormonal si + / - ? SI
 si. no. I - Eca. si. SI. si. SI. Otras drogas control. neurohormonal. si. + / - SI.")
31
TRATAMIENTO Normal Disfunción VI Asintomática FE <40%
ICC Sintomática NYHA II I-ECA ICC Sintomática NYHA - III Diuréticos dosis baja Inhibidores neurohormonales Digoxina? ICC Sintomática NYHA - IV Diuréticos de asa Espironolactona Treatment of Heart Failure. Treatment scheme according to the degree of heart failure Patients with asymptomatic ventricular dysfunction should receive ACEI when the LVEF is significantly reduced, and clearly if it is less than 35%. In the presence of symptoms of heart failure, diuretics or neurohormonal inhibitors should be added. The use of digoxin remains controversial. In more advanced stages, in the presence of poorly controlled symptoms, newer drugs can be tried, reserving the inotropes for patients whose symptoms are uncontrollable with other medications. In any case, secondary prevention and assisting the patients in adapting to their limitations should remain in mind. Inotrópicos Terapia especializada Transplante Prevención secundaria Modificación de actividad física

32
DIURETICOS Cortex Médula Tiazidas Ahorradores de K Diuréticos de asa
Inhiben intercambio activo de Cl-Na en el segmento cortical diluyente del asa ascendente de Henle Cortex Ahorradores de K Inhiben reabsorción de Na en el túbulo distal convoluto y colector Treatment of heart failure. Diuretics: Classification and mechanisms of action Diuretics are drugs which eliminate Na and water by acting directly on the kidney. This category does not include other drugs with principle actions different from the diuretics, but which increase diuresis by improving heart failure or by mechanisms on the kidney which are incompletely understood. The diuretics are the primary line of therapy for the majority of patients with heart failure and pulmonary congestion. Diuretics (loop, thiazides and potassium-sparing) produce a net loss of Na and water acting directly on the kidney, decrease acute symptoms which result from fluid retention (dyspnea, edema). Diuretic drugs are classically divided into three groups: 1) thiazides, 2) loop diuretics and 3) potassium-sparing. Thiazide diuretics inhibit the active transport of Cl-Na in the cortical diluting segment of the ascending limb of the Loop of Henle. Loop diuretics inhibit the transport of Cl-Na-K in the thick portion of the ascending limb of the Loop of Henle. Potassium-sparing diuretics inhibit the reabsorption of Na in the distal convoluted and collecting tubules. Diuréticos de asa Inhiben intercambio de Cl-Na-K en el segmento grueso del asa ascendente de Henle Médula Asa de Henle Túbulo Colector
 produce a net loss of Na and water acting directly on the kidney, decrease acute symptoms which result from fluid retention (dyspnea, edema). Diuretic drugs are classically divided into three groups: 1) thiazides, 2) loop diuretics and 3) potassium-sparing. Thiazide diuretics inhibit the active transport of Cl-Na in the cortical diluting segment of the ascending limb of the Loop of Henle. Loop diuretics inhibit the transport of Cl-Na-K in the thick portion of the ascending limb of the Loop of Henle. Potassium-sparing diuretics inhibit the reabsorption of Na in the distal convoluted and collecting tubules. Diuréticos de asa. Inhiben intercambio de Cl-Na-K en. el segmento grueso del asa. ascendente de Henle. Médula. Asa de Henle. Túbulo Colector.")
33
TIAZIDAS MECANISMO DE ACCION
Excreta % del Na+ filtrado Eliminación de K Inhiben anhidrasa carbónica: incrementa eliminación de HCO3 Excreción de ácido úrico, Ca y Mg No relación dosis - efecto Treatment of heart failure. Diuretics: Mechanism of action of the thiazides The thiazides are diuretics of intermediate potency, excreting 5-10% of the filtered fraction of Na. The act from the luminal surface inhibiting the active transport of Cl and the subsequent diffusion of Na and water in the cortical diluting segment of the ascending portion of the loop of Henle. The also increase elimination of K by increasing the exchange of Na/K in the distal convoluted tubule and increase the urinary elimination of HCO3 by inhibiting carbonic anhydrase. In addition they increase tubular reabsorption of uric acid, Ca and Mg. There are important differences in the strength and duration of diuretic action depending on which thiazide is used.

34
DIURETICOS DE ASA MECANISMO DE ACCION
Excreta % del Na+ filtrado Eliminación de K+, Ca+ y Mg++ Resistencia de arteriolas aferentes Flujo cortical y TFG Libera PGs renales AINEs pueden antagonizar diuresis Treatment of heart failure. Diuretics Mechanism of action of loop diuretics Loop diuretics are the strongest, prompting the excretion of 15-20% of the filtered Na+. They act in the thick segment of the ascending loop of Henle, inhibiting the cotransport of Cl--Na+-K+ at the luminal surface. They also increase the elimination of K+, as the increase in Na that reaches the distal convoluted tubule stimulates its exchange for K+ and H+; in addition, they also stimulate the secretion of renin and the production of aldosterone which augments the elimination of K+. By inhibiting carbonic anhydrase, they increase the urinary elimination of HCO-3. They also increase elimination of Ca++ and Mg++. GFR: glomerular filtration rate; PGS: prostaglandins; NSAIDs: nonsteroidal anti-inflammatory drugs.

35
DIURETICOS AHORRADORES DE K MECANISMO DE ACCION
Elimina < 5% del Na+ filtrado Inhiben intercambio de Na+ por K+ o H+ Espironolactona = antagonista competitivo del receptor de aldosterona Amilorida y triamtereno bloquean los canales de Na+ controlados por aldosterona Treatment of heart failure. Diuretics: Mechanism of action of potassium-sparing diuretics Potassium-sparing diuretics inhibit reabsorption of Na+ at the level of the distal convoluted tubule and the collecting duct and its exchange for K+ or H+. Their diuretic strength is slight, as the fraction of Na eliminated is no more than 5%. Spironolactone is a competitive antagonist of aldosterone, interfering with its induction of synthesis of proteins which specifically facilitate Na reabsorption. As a result, its diuretic action depends on the role that aldosterone plays in the retention of water and Na. Triamterene and amiloride block the exchange of Na+-K+/H+, but their effect is independent of the levels of aldosterone. All of these drugs moderately increase the renal excretion of Na+, Cl- and HCO-3, at the same time that they diminish the excretion of K+, H +and ammonium, and may therefore cause hyperkalemia and hypochloremic acidosis.

36
EFECTOS DE LOS DIURETICOS
Volumen y precarga Mejoría síntomas de congestión No efecto directo en GC, pero una reducción excesiva precarga puede Mejoría distensibilidad arterial Activación neurohormonal Niveles de NA, Ang II y ARP Excepción: con espironolactona Treatment of heart failure. Diuretics: Mechanisms of action Diuretics decrease volume and preload, and as a result are very effective at improving the signs of pulmonary and systemic venous congestion. They do not change the cardiac output (CO), but CO may fall if an excessive decrease in preload occurs. They slightly improve arterial distensibility, but this effect is of no clinical relevance. The main drawback to diuretics use is their effect on the neurohormonal milieu, increasing the plasma levels of noradrenaline (NA), angiotensin II (Ang II) and aldosterone, and the plasma renin activity (PRA).
, but CO may fall if an excessive decrease in preload occurs. They slightly improve arterial distensibility, but this effect is of no clinical relevance. The main drawback to diuretics use is their effect on the neurohormonal milieu, increasing the plasma levels of noradrenaline (NA), angiotensin II (Ang II) and aldosterone, and the plasma renin activity (PRA).")
37
DIURETICOS REACCIONES ADVERSAS Tiazidas y diuréticos de asa
Cambios en electrolitos: Volumen Na+, K+, Ca++, Mg++ alcalosis metabólica Cambios metabólicos: glicemia, uremia, gota LDL-C y TG Reacciones cutáneas alérgicas Treatment of heart failure. Diuretics: Adverse effects of thiazide and loop diuretics Thiazide and loop diuretics create electrolyte imbalances: hypovolemia, hyponatremia, hypokalemia, hypomagnesemia, hypercalcemia and metabolic alkalosis. They also create metabolic changes (hyperglycemia, hyperuricemia, gout, increase in LDL-cholesterol and triglycerides), impotence and menstrual cramps. Hypokalemia can be treated with K+ supplements or with the simultaneous use of potassium-sparing diuretics. Cutaneous allergic reactions (rash, pruritis) are frequent. In addition, these are cross-reactions between the various thiazides (except chlorthalidone) and because of their chemical resemblance, with furosemide and bumetanide. Thiazides can aggravate myopia in pregnant women.
, impotence and menstrual cramps. Hypokalemia can be treated with K+ supplements or with the simultaneous use of potassium-sparing diuretics. Cutaneous allergic reactions (rash, pruritis) are frequent. In addition, these are cross-reactions between the various thiazides (except chlorthalidone) and because of their chemical resemblance, with furosemide and bumetanide. Thiazides can aggravate myopia in pregnant women.")
38
DIURETICOS REACCIONES ADVERSAS Tiazidas y diuréticos de asa
Efectos idiosincráticos: Discrasia sanguínea, ictericia colestática y pancreatitis aguda Efectos gastrointestinales Efectos genitourinarios: Impotencia y cólicos menstruales Sordera, nefrotoxicidad (diuréticos de asa) Treatment of heart failure. Diuretics: Adverse effects of thiazide and loop diuretics Known adverse reactions include parenchymal (pancreatitis, cholestatic jaundice, hemolytic anemia, thrombocytopenia), gastrointestinal effects (ethacrynic acid), myalgias (bumetanide, piretanide) and muscle cramps related to electrolyte disorders. Loop diuretics are associated with ototoxicity with loss of hearing and balance and these are more frequent in patients with renal insufficiency or with concomitant use of aminoglycoside antibiotics. They may also cause interstitial nephritis.
 Treatment of heart failure. Diuretics: Adverse effects of thiazide and loop diuretics. Known adverse reactions include parenchymal (pancreatitis, cholestatic jaundice, hemolytic anemia, thrombocytopenia), gastrointestinal effects (ethacrynic acid), myalgias (bumetanide, piretanide) and muscle cramps related to electrolyte disorders. Loop diuretics are associated with ototoxicity with loss of hearing and balance and these are more frequent in patients with renal insufficiency or with concomitant use of aminoglycoside antibiotics. They may also cause interstitial nephritis.")
39
DIURETICOS AHORRADORES DE K
REACCIONES Cambios en electrolitos: Na+, K+, acidosis Músculo-esquelética: Calambres, debilidad Reacciones cutáneas alérgicas: Rash, prurito Treatment of heart failure. Diuretics: Adverse reactions to potassium-sparing agents The main adverse reaction to these agents is hyperkalemia, which occurs mostly in patients with renal failure, particularly if they are also receiving ACE inhibitors. They may also create metabolic acidosis, muscle cramps and weakness, and cutaneous allergic reactions.

40
DIGOXINA Na-K ATPasa Intercambiador Na-Ca
Treatment of heart failure. Digoxin: Mechanism of action Digoxin attaches to specific receptors which form a part of the enzyme, Na+/K+-dependent ATP-ase (sodium pump), inhibiting it. This blockade produces a progressive increase in the intracellular concentration of Na, which in turn activates the exchange of Na+-Ca++ and increases the influx of Ca++ and its intracellular concentration, [Ca++]i. This increase in the [Ca++]i at the level of the contractile proteins explains the resultant increase in cardiac contractility. Miofilamentos Ca++ K+ Na+ CONTRACTILIDAD
, inhibiting it. This blockade produces a progressive increase in the intracellular concentration of Na, which in turn activates the exchange of Na+-Ca++ and increases the influx of Ca++ and its intracellular concentration, [Ca++]i. This increase in the [Ca++]i at the level of the contractile proteins explains the resultant increase in cardiac contractility. Miofilamentos. Ca++ K+ Na+ CONTRACTILIDAD.")
41
DIGOXINA PROPIEDADES FARMACOCINETICAS
Absorción oral (%) Unión a proteínas (%) Volumen de distribución (l/Kg) Vida media Eliminación Inicio (min) i.v. oral Efecto máximo (h) Duración Nivel terapéutico (ng/ml) 25 6 (3-9) 36 (26-46) h Renal 5 - 30 2 - 4 3 - 6 2 - 6 días Treatment of heart failure. Digoxin: Pharmacokinetics Oral absorption is 60-75% of the administered dose; when given by this route, maximal levels are reached after minutes and its action is maximal after 3-6 h. When given i.v., onset of action is at 5-30 min and this reaches its maximum at 2-4 h. It is approximately 25% bound to plasma proteins and is widely distributed through the body, crossing the blood brain barrier and the placenta. It accumulates in skeletal muscle, liver and heart, where it may reach concentrations that are 10 to 50 times higher than serum levels. This explains why hemodialysis eliminates little of the digoxin load in digoxin toxicity. Cardiac uptake of digoxin increases in patients with hypokalemia and decreases in the presence of hyperkalemia, hypercalcemia or hypomagnesemia. Digoxin undergoes very little biotransformation, and is mainly eliminated through glomerular filtration and somewhat by tubular secretion. In patients with renal insufficiency, the half life of digoxin increases 2-4 times, so that the maintenance dose must be determined according to the creatinine clearance, generally requiring half of the usual dose and, in severe cases, intermittent dosing.
 Unión a proteínas (%) Volumen de distribución (l/Kg) Vida media. Eliminación. Inicio (min) i.v. oral. Efecto máximo (h) Duración. Nivel terapéutico (ng/ml) (3-9) 36 (26-46) h. Renal días Treatment of heart failure. Digoxin: Pharmacokinetics. Oral absorption is 60-75% of the administered dose; when given by this route, maximal levels are reached after minutes and its action is maximal after 3-6 h. When given i.v., onset of action is at 5-30 min and this reaches its maximum at 2-4 h. It is approximately 25% bound to plasma proteins and is widely distributed through the body, crossing the blood brain barrier and the placenta. It accumulates in skeletal muscle, liver and heart, where it may reach concentrations that are 10 to 50 times higher than serum levels. This explains why hemodialysis eliminates little of the digoxin load in digoxin toxicity. Cardiac uptake of digoxin increases in patients with hypokalemia and decreases in the presence of hyperkalemia, hypercalcemia or hypomagnesemia. Digoxin undergoes very little biotransformation, and is mainly eliminated through glomerular filtration and somewhat by tubular secretion. In patients with renal insufficiency, the half life of digoxin increases 2-4 times, so that the maintenance dose must be determined according to the creatinine clearance, generally requiring half of the usual dose and, in severe cases, intermittent dosing.")
42
DIGOXINA ESTRATEGIAS DE DIGITALIZACION
Dosis de mantenimiento Dosis de carga (mg) i.v / 4 h ILD: oral h / 6 h oral 2-5 d 0.25 / 6-12 h (mg) / d 0.25 / d Treatment of heart failure. Digoxin: Digitalization strategies The dose of digoxin should be individualized according to age, renal function, severity of the circumstances and the existence of factors which modify the patients’ sensitivity to digoxin, and the dose then adjusted according to clinical response. The time required to reach stable serum levels is 5 half-lives, that is, 7 days. Loading can be accomplished: a) Rapidly, by i.v. (12-24 hours). This is not advisable except in cases of emergency, as it does not allow individualization of the treatment and increases the risk of cardiac toxicity. b) Slowly, via the oral route (5 days for digoxin), which carries less risk. Once loading is accomplished, the maintenance dose must be determined, and should correspond to the amount of digoxin which is eliminated daily (30% of the initial digoxin dose). In the majority of adults, the maintenance dose of digoxin is 0.25 mg/day; in patients with atrial fibrillation the dose may be increased to mg/day, while in the elderly and in patients with renal failure it may need to be reduced to mg/day and with anuria to mg every 48 h. ILD = Dosis INICIAL promedio requirida para impregnación
 i.v / 4 h. ILD: oral h / 6 h oral 2-5 d / 6-12 h (mg) / d / d. Treatment of heart failure. Digoxin: Digitalization strategies. The dose of digoxin should be individualized according to age, renal function, severity of the circumstances and the existence of factors which modify the patients’ sensitivity to digoxin, and the dose then adjusted according to clinical response. The time required to reach stable serum levels is 5 half-lives, that is, 7 days. Loading can be accomplished: a) Rapidly, by i.v. (12-24 hours). This is not advisable except in cases of emergency, as it does not allow individualization of the treatment and increases the risk of cardiac toxicity. b) Slowly, via the oral route (5 days for digoxin), which carries less risk. Once loading is accomplished, the maintenance dose must be determined, and should correspond to the amount of digoxin which is eliminated daily (30% of the initial digoxin dose). In the majority of adults, the maintenance dose of digoxin is 0.25 mg/day; in patients with atrial fibrillation the dose may be increased to mg/day, while in the elderly and in patients with renal failure it may need to be reduced to mg/day and with anuria to mg every 48 h. ILD = Dosis INICIAL promedio requirida para impregnación.")
43
DIGOXINA EFECTOS HEMODINAMICOS
Gasto cardiaco Fracción de eyección del VI PTDVI Tolerancia al ejercicio Natriuresis Activación neurohormonal Treatment of heart failure. Digoxin: Hemodynamic effects Digoxin increases contractile force, maximal shortening velocity (dp/dt max) and the cardiac output, decreases the LV filling pressure and volume, the pulmonary capillary wedge pressure, wall stress and the cardiothoracic ratio. Digoxin displaced the ventricular function curve up and to the left, meaning that it increases the cardiac output at any filling pressure. All of these effects explain when digoxin decreases the signs of congestion and peripheral hypoperfusion in the patient with heart failure. The increase in cardiac output reduces the heart rate, the peripheral vascular resistance, and offsets the increased myocardial demand for oxygen that the increase in contractility might create.
 and the cardiac output, decreases the LV filling pressure and volume, the pulmonary capillary wedge pressure, wall stress and the cardiothoracic ratio. Digoxin displaced the ventricular function curve up and to the left, meaning that it increases the cardiac output at any filling pressure. All of these effects explain when digoxin decreases the signs of congestion and peripheral hypoperfusion in the patient with heart failure. The increase in cardiac output reduces the heart rate, the peripheral vascular resistance, and offsets the increased myocardial demand for oxygen that the increase in contractility might create.")
44
DIGOXINA EFECTOS NEUROHORMONALES
Norepinefrina plasmática Actividad sistema nervioso periférico Actividad SRAA Tono vagal Normaliza baroreceptores arteriales Treatment of heart failure. Digoxin: Neurohormonal effects Digoxin, at the doses which augment cardiac contractility, restores the inhibitory effect of the arterial baroreceptors and markedly inhibits the activity of the sympathetic nervous system, which can be seen in the reduction of plasma levels of noradrenaline, the activity of peripheral sympathetic system, and the activity of the renin-angiotensin- aldosterone system (RAAS). This neurohormonal inhibition reduces the heart rate, the peripheral vascular resistance and the signs of congestion and peripheral hypoperfusion in the patient with heart failure. This creates the question to what point do the beneficial effects of digoxin reflect its positive inotropic quality. Digoxin also decreases the reabsorption of Na and water; this natriuretic action, secondary to the increase in cardiac output, increases renal perfusion and the glomerular filtration rate, decreasing renal vasoconstriction and the activation of the RAAS.
. This neurohormonal inhibition reduces the heart rate, the peripheral vascular resistance and the signs of congestion and peripheral hypoperfusion in the patient with heart failure. This creates the question to what point do the beneficial effects of digoxin reflect its positive inotropic quality. Digoxin also decreases the reabsorption of Na and water; this natriuretic action, secondary to the increase in cardiac output, increases renal perfusion and the glomerular filtration rate, decreasing renal vasoconstriction and the activation of the RAAS.")
45
DIGOXINA EFECTO EN PROGRESION ICC
30 Placebo n=93 DIGOXINA Suspensión % EMPEORAMIENTO DE ICC 20 DIGOXINA: mg /d ( ng/ml) EF < 35% Clase I-III (digoxina+diurético+IECA) También disminución significativa en tiempo ejercicio y FEVI. p = 0.001 10 Treatment of heart failure. Digoxin: Effect on morbidity The RADIANCE trial (multicenter, randomized, double-blind on the efficacy and safety of stopping digoxin in patients with heart failure who were receiving treatment with ACEI) analyzed clinical evolution in 178 patients with heart failure of functional classes II-III and LVEF < 35% treated with digoxin and diuretics and ACEI. Patients either maintained their dose of digoxin between mg/d with serum levels of ng/ml or were given placebo instead. After 100 days of treatment, digoxin withdrawal produced a significant worsening in heart failure which was greater than that observed in the group of patients in whom digoxin was maintained. Packer M et al (RADIANCE). N Engl J Med 1993;329:1 DIGOXINA n=85 RADIANCE N Engl J Med 1993;329:1 20 40 60 80 100 Días
 EF < 35% Clase I-III (digoxina+diurético+IECA) También disminución significativa. en tiempo ejercicio y FEVI. p = Treatment of heart failure. Digoxin: Effect on morbidity. The RADIANCE trial (multicenter, randomized, double-blind on the efficacy and safety of stopping digoxin in patients with heart failure who were receiving treatment with ACEI) analyzed clinical evolution in 178 patients with heart failure of functional classes II-III and LVEF < 35% treated with digoxin and diuretics and ACEI. Patients either maintained their dose of digoxin between mg/d with serum levels of ng/ml or were given placebo instead. After 100 days of treatment, digoxin withdrawal produced a significant worsening in heart failure which was greater than that observed in the group of patients in whom digoxin was maintained. Packer M et al (RADIANCE). N Engl J Med 1993;329:1. DIGOXINA n=85. RADIANCE. N Engl J Med 1993;329: Días.")
46
MORTALIDAD TOTAL % 50 40 30 20 10 Placebo n=3403 DIGOXINA n=3397 12 24
% Placebo n=3403 p = 0.8 Treatment of heart failure. Digoxin: Effect on survival The results obtained from 3 controlled studies which included patients at low risk (The German and Austrian Xamoterol Study Group, 1988; The Captopril-Digoxin Multicenter Research Group, 1988; DiBianco et al., 1989) indicate that the mortality was similar in the group of patients with placebo. The results of the Digitalis Investigator Group-DIG study, which included 7788 patients with heart failure in sinus rhythm, functional class II-III and LVEF < 45%. The patients were treated with digoxin or placebo, in addition to conventional therapy over a mean of 37 months ( months). No differences in mortality were observed between the two treatment groups. Am Coll Cardiol 1996 DIGOXINA n=3397 12 24 36 48 DIG N Engl J Med 1997;336:525 Meses
 indicate that the mortality was similar in the group of patients with placebo. The results of the Digitalis Investigator Group-DIG study, which included 7788 patients with heart failure in sinus rhythm, functional class II-III and LVEF < 45%. The patients were treated with digoxin or placebo, in addition to conventional therapy over a mean of 37 months ( months). No differences in mortality were observed between the two treatment groups. Am Coll Cardiol DIGOXINA. n= DIG. N Engl J Med 1997;336:525. Meses.")
47
DIGOXINA EFECTOS A LARGO PLAZO
Sobrevida similar a placebo Menos admisiones hospitalarias Arritmias más serias Más infartos del miocardio Treatment of heart failure. Digoxin: Effect on long term course The results obtained in 3 controlled studies that included patients at low risk (The German and Austrian Xamoterol Study Group, 1988; The Captopril-Digoxin Multicenter Research Group, 1988; DiBianco et al., 1989) indicate that the mortality were similar in both treatment groups. In the DIG study (Digitalis Investigator Group), the survival of 7788 patients with heart failure classes II-III and LVEF < 45% and sinus rhythm treated over 37 months ( ) with digoxin, to determine if it increased or decreased the mortality of patients with symptoms of heart failure. There was no observed effect on survival, but it decreased slightly the number of admissions for cardiovascular causes and also increased the incidence of serious arrhythmias and episodes of acute myocardial infarction. The results of this study probably demand redefinition of the indication for the use of digoxin in patients with heart failure.
 indicate that the mortality were similar in both treatment groups. In the DIG study (Digitalis Investigator Group), the survival of 7788 patients with heart failure classes II-III and LVEF < 45% and sinus rhythm treated over 37 months ( ) with digoxin, to determine if it increased or decreased the mortality of patients with symptoms of heart failure. There was no observed effect on survival, but it decreased slightly the number of admissions for cardiovascular causes and also increased the incidence of serious arrhythmias and episodes of acute myocardial infarction. The results of this study probably demand redefinition of the indication for the use of digoxin in patients with heart failure.")
48
DIGOXINA USOS CLINICOS
FA con respuesta ventricular rápida ICC refractaria a otras drogas ¿Otras indicaciones? Puede ser combinada con otras drogas Treatment of heart failure. Digoxin: Clinical uses Digoxin is the drug of choice for patients with heart failure associated with atrial fibrillation/flutter with rapid ventricular response. Accompanied by diuretics and ACEI it is also useful in patients in sinus rhythm with systolic heart failure. The best results are obtained when cardiomegaly (cardiothoracic index > 60%) and important systolic dysfunction (LVEF < 40%, symptoms at rest, third heart sound) are present. It is also useful in patients who do not respond to diuretics and vasodilators and in severe heart failure associated with hypotension when vasodilators are contraindicated. Digoxin is more effective in heart failure with low cardiac output associated with cardiomyopathies, ischemic cardiomyopathy, arterial hypertension or rheumatic valvular disease with left ventricular failure. It is relatively inefficacious in heart failure with high cardiac output (associated with hyperthyroidism, anemia, arteriovenous fistulas, glomerulonephritis or Paget’s disease) and in heart failure secondary to hypertrophic cardiomyopathy. The results of the study of survival with digoxin require a reassessment of the indications for digoxin use in patients with heart failure. Probably digoxin will become a second-line drug, and its use may be restricted to patients with refractory symptoms, except in patient with rapid atrial fibrillation.
 and important systolic dysfunction (LVEF < 40%, symptoms at rest, third heart sound) are present. It is also useful in patients who do not respond to diuretics and vasodilators and in severe heart failure associated with hypotension when vasodilators are contraindicated. Digoxin is more effective in heart failure with low cardiac output associated with cardiomyopathies, ischemic cardiomyopathy, arterial hypertension or rheumatic valvular disease with left ventricular failure. It is relatively inefficacious in heart failure with high cardiac output (associated with hyperthyroidism, anemia, arteriovenous fistulas, glomerulonephritis or Paget’s disease) and in heart failure secondary to hypertrophic cardiomyopathy. The results of the study of survival with digoxin require a reassessment of the indications for digoxin use in patients with heart failure. Probably digoxin will become a second-line drug, and its use may be restricted to patients with refractory symptoms, except in patient with rapid atrial fibrillation.")
49
DIGOXINA CONTRAINDICACIONES
ABSOLUTA: Toxicidad a digoxina RELATIVAS: Bloqueo AV avanzado sin marcapaso Bradicardia o seno enfermo sin MP CVP’s y TV Hipokalemia marcada W-P-W con fibrilación atrial Treatment of heart failure Digoxin: Contraindications The only absolute contraindication for digoxin use is the presence of digoxin toxicity. Relative contraindications include: a) presence of advanced A-V blocks without pacemaker, as incremental blockade of conduction through the A-V node increases the risk of complete A-V block; b) ventricular extrasystoles and tachycardias, as these may be aggravated; nevertheless, digoxin may be given if the patient’s extrasystoles are secondary to heart failure; c) marked bradycardia or sinus node disease without pacemaker; d) marked, uncontrolled hypokalemia, and e) patients with Wolff-Parkinson-White syndrome and atrial fibrillation.
 presence of advanced A-V blocks without pacemaker, as incremental blockade of conduction through the A-V node increases the risk of complete A-V block; b) ventricular extrasystoles and tachycardias, as these may be aggravated; nevertheless, digoxin may be given if the patient’s extrasystoles are secondary to heart failure; c) marked bradycardia or sinus node disease without pacemaker; d) marked, uncontrolled hypokalemia, and e) patients with Wolff-Parkinson-White syndrome and atrial fibrillation.")
50
TOXICIDAD POR DIGOXINA MANIFESTACIONES CARDIACAS
ARRITMIAS : Ventricular (CVPs, TV, FV) Supraventricular (CAPs, TSV) BLOQUEOS: BLOQUEOS S-A Y A-V EXACERBACION ICC Treatment of heart failure. Digoxin toxicity Digoxin has a narrow therapeutic margin, and digoxin intoxication remains relatively frequent although it has diminished somewhat as it has become better recognized and lower doses are being prescribed. Cardiac manifestations. Digoxin may cause any type of cardiac arrhythmia, although at times the ECG may be nonspecific. At the ventricular level, isolated or multifocal PVC’s, bigeminy, tachycardia and ventricular fibrillation may occur; at the supraventricular level, digoxin may induce extrasystoles and paroxysmal tachycardias which may result in atrial flutter or fibrillation. In addition, depression of sinoatrial node function may produce bradycardia and even complete sinoatrial block. It prolongs the refractory period and depresses conduction velocity across the A-V node (lengthens the PR interval on the ECG), thereby creating different grade of conduction block, which may precede the appearance of reentrant nodal tachycardias and nodal rhythms. Exacerbation of heart failure in patients treated with digoxin should raise the question of digoxin toxicity.
 Supraventricular (CAPs, TSV) BLOQUEOS: BLOQUEOS S-A Y A-V. EXACERBACION ICC. Treatment of heart failure. Digoxin toxicity. Digoxin has a narrow therapeutic margin, and digoxin intoxication remains relatively frequent although it has diminished somewhat as it has become better recognized and lower doses are being prescribed. Cardiac manifestations. Digoxin may cause any type of cardiac arrhythmia, although at times the ECG may be nonspecific. At the ventricular level, isolated or multifocal PVC’s, bigeminy, tachycardia and ventricular fibrillation may occur; at the supraventricular level, digoxin may induce extrasystoles and paroxysmal tachycardias which may result in atrial flutter or fibrillation. In addition, depression of sinoatrial node function may produce bradycardia and even complete sinoatrial block. It prolongs the refractory period and depresses conduction velocity across the A-V node (lengthens the PR interval on the ECG), thereby creating different grade of conduction block, which may precede the appearance of reentrant nodal tachycardias and nodal rhythms. Exacerbation of heart failure in patients treated with digoxin should raise the question of digoxin toxicity.")
51
TOXICIDAD POR DIGOXINA MANIFESTACIONES EXTRACARDIACAS
GASTROINTESTINALES: Náusea, vómito, diarrea NERVIOSAS: Depresión, desorientación, parestesias VISUALES: Visión borrosa, escotomas y visión amarilla HIPERESTROGENISMO: Ginecomastia, galactorrea Treatment of heart failure. Digoxin intoxication Extracardiac adverse reactions: a) Gastrointestinal: anorexia, nausea, vomiting, diarrhea, weight loss. b) Nervous: depression, disorientation, confusion, delirium, neuritis and paresthesias. c) Visual changes: blurry vision, scotomas, yellow-green vision. d) Digoxin inhibits the metabolism of ß-estradiol and can produce signs of hyperestrogenism: gynecomastia and galactorrhea or vaginal plaques which may be confused with carcinoma in postmenopausal women.
 Gastrointestinal: anorexia, nausea, vomiting, diarrhea, weight loss. b) Nervous: depression, disorientation, confusion, delirium, neuritis and paresthesias. c) Visual changes: blurry vision, scotomas, yellow-green vision. d) Digoxin inhibits the metabolism of ß-estradiol and can produce signs of hyperestrogenism: gynecomastia and galactorrhea or vaginal plaques which may be confused with carcinoma in postmenopausal women.")
52
INOTROPICOS POSITIVOS
GLICOSIDOS CARDIACOS SIMPATICOMIMETICOS Catecolaminas Agonistas ß-adrenérgicos INHIBIDORES FOSFODIESTERASA Amrinona Enoximona Otros Treatment of heart failure. Positive inotropic agents The use of inotropic agents in heart failure is intended to increase contractility and cardiac output to meet the metabolic needs of the body. Theoretically, their use should be greatest in heart failure associated with a decrease in systolic function and marked cardiomegaly, depression of ejection fraction and elevated left ventricular filling pressure. In addition to the cardiac glycosides, other positive inotropic agents include: a) the sympathomimetics, represented by the ß1 agonists (which stimulate cardiac contractility) and ß2-adrenergics (vasodilators). Both groups increase the intracellular concentration of cAMP by stimulating the activity of adenylate cyclase which converts ATP to cAMP; b) Phosphodiesterase inhibitors, which inhibit the enzyme that breaks down cAMP, increase cardiac contractility and have arteriovenous vasodilatory effect; c) other ionotropic drugs including glucagon and Na+ channels agonists. Milrinone Piroximone
 the sympathomimetics, represented by the ß1 agonists (which stimulate cardiac contractility) and ß2-adrenergics (vasodilators). Both groups increase the intracellular concentration of cAMP by stimulating the activity of adenylate cyclase which converts ATP to cAMP; b) Phosphodiesterase inhibitors, which inhibit the enzyme that breaks down cAMP, increase cardiac contractility and have arteriovenous vasodilatory effect; c) other ionotropic drugs including glucagon and Na+ channels agonists. Milrinone. Piroximone.")
53
Estimulantes B1 Estimulantes B2 Mixto
ESTIMULANTES ß-ADRENERGICOS CLASIFICACION Estimulantes B1 Aumentan la contractilidad Dobutamina Doxaminol Xamoterol Butopamina Prenalterol Tazolol Estimulantes B2 Producen vasodilatación arterial y reducen RVS Pirbuterol Carbuterol Rimiterol Fenoterol Tretoquinol Salbutamol Terbutalina Salmefamol Soterenol Quinterenol Treatment of heart failure. ß-adrenergic agonists: Classification In an attempt to find options to digoxin, in the 1980’s different positive inotropic drugs became available, among them ß-adrenergic agonists and phosphodiesterase III inhibitors. Both groups of drugs increase the intracellular concentration of cAMP; ß-adrenergic agonists by stimulating the activity of adenylate cyclase which converts ATP into cAMP, and the phosphodiesterase III inhibitors by inhibiting the breakdown of cAMP. The ß-adrenergic agonists can be classified according to the capacity for stimulating the cardiac ß1 receptors (increasing contractility and heart rate), ß2-vasodilatory receptors or both (mixed). SVR = Systemic vascular resistance Mixto Dopamina
, ß2-vasodilatory receptors or both (mixed). SVR = Systemic vascular resistance. Mixto. Dopamina.")
54
DOPAMINA Y DOBUTAMINA EFECTOS
DA (µg / Kg / min) Dobutamina < 2 2 - 5 > 5 Receptores DA1 / DA2 ß1 ß1 + a ß1 Contractilidad ++ ++ ++ Treatment of heart failure Dopamine (DA) and dobutamine: Hemodynamic effects The hemodynamic effects vary, depending on the dose used: At low doses (0.2-2 µg/kg/min), DA stimulates DA1 and DA2 receptors, producing renal, mesenteric, cerebral and coronary vasodilatation. Renal vasodilatation increases glomerular filtration rate, urine production and renal excretion of Na; the majority of Na excretion seems to be due to a direct tubular action of DA and stimulation of DA2 receptors that inhibit the liberation of aldosterone. Inhibition of sympathetic tone produced by the stimulation of DA2 receptors explains why at these doses the arterial pressure decreases slightly and the heart rate remains the same or even falls. These doses are used for induction of diuresis, particularly in patients who do not respond to furosemide. At intermediate doses (2-5 µg/kg/min) DA also stimulates cardiac ß1 and ß2 receptors, increasing contractility, heart rate and cardiac output at the same time as it decreases peripheral resistance (stimulation of DA1 and ß2 receptors). These doses are used in the treatment of heart failure without hypotension. At high doses (> 5 µg/kg/min) DA also stimulates a-adrenergic receptors, increasing peripheral resistance and blood pressure. In addition, the marked stimulation of the cardiac ß1 receptors increases the heart rate and contractility, the myocardial O2 demand, and may produce arrhythmias. These doses are only used in patients with severe hypotension and/or cardiogenic shock. Frec. Cardiaca + ++ Presión arterial + ++ ++ Perfusión renal ++ + + Arritmias - ++
 Dobutamina. < > 5. Receptores. DA1 / DA2. ß1. ß1 + a. ß1. Contractilidad Treatment of heart failure. Dopamine (DA) and dobutamine: Hemodynamic effects. The hemodynamic effects vary, depending on the dose used: At low doses (0.2-2 µg/kg/min), DA stimulates DA1 and DA2 receptors, producing renal, mesenteric, cerebral and coronary vasodilatation. Renal vasodilatation increases glomerular filtration rate, urine production and renal excretion of Na; the majority of Na excretion seems to be due to a direct tubular action of DA and stimulation of DA2 receptors that inhibit the liberation of aldosterone. Inhibition of sympathetic tone produced by the stimulation of DA2 receptors explains why at these doses the arterial pressure decreases slightly and the heart rate remains the same or even falls. These doses are used for induction of diuresis, particularly in patients who do not respond to furosemide. At intermediate doses (2-5 µg/kg/min) DA also stimulates cardiac ß1 and ß2 receptors, increasing contractility, heart rate and cardiac output at the same time as it decreases peripheral resistance (stimulation of DA1 and ß2 receptors). These doses are used in the treatment of heart failure without hypotension. At high doses (> 5 µg/kg/min) DA also stimulates a-adrenergic receptors, increasing peripheral resistance and blood pressure. In addition, the marked stimulation of the cardiac ß1 receptors increases the heart rate and contractility, the myocardial O2 demand, and may produce arrhythmias. These doses are only used in patients with severe hypotension and/or cardiogenic shock. Frec. Cardiaca Presión arterial Perfusión renal Arritmias")
55
INOTROPICOS POSITIVOS CONCLUSIONES
Pueden aumentar mortalidad Seguros en dosis bajas Uso únicamente en ICC refractaria NO para uso como terapia crónica Treatment of heart failure. Inotropes: General problems Positive inotropic drugs which increase cellular levels of cAMP have important proarrhythmic effects and seem to accelerate the progression of heart failure. Their hemodynamic effects decreased with prolonged treatment which suggests that they should not be used for chronic treatment. Safety and efficacy increases when they are used in low doses, with which the increase in contractility is slight. This points out that their beneficial effects probably do not depend on their positive inotropic action. The reduction in neurohumoral activation produced by digoxin and ibopamine, the antiarrhythmic action of Vesnarinone or the vasodilatory effects of dopamine, dobutamine or PDE III inhibitors may be more important than the increase in contractility that until recently was though to be their utility in the treatment of heart failure. With the exception of digoxin, chronic administration of these drugs increases mortality, so their use, in low doses, should be restricted to patients with refractory heart failure, with persistent symptoms despite treatment with combinations of other drugs. As it is precisely the sickest patients who manifest the increase in mortality, treatment with inotropic drugs is not likely to prolong the survival of these patients.

56
DROGAS VASODILATORAS PRINCIPIOS
Contractilidad Normal Contractilidad Normal GC VV AV Contractilidad Disminuida Contractilidad Disminuida PRECARGA POSCARGA

57
VASODILATORES CLASIFICACION
Vasodilatación Venosa VENOSOS Nitratos Molsidomina MIXTOS Calcioantagonistas Bloqueadores a-adrenérgicos IECA Antagonistas Angiotensina II Activadores canales K+ Nitroprusiato Vasodilatación Arterial ARTERIAL Minoxidil Hidralazina

58
NITRATOS EFECTOS HEMODINAMICOS
1- VASODILATACION VENOSA Precarga 2- Vasodilatación coronaria Perfusión miocárdica 3- Vasodilatación arterial Postcarga 4- Otros Congestión pulmonar Tamaño ventricular Stress pared ventricular MVO2 Treatment of Heart Failure. Nitrates: Hemodynamic effects At therapeutic doses, nitrates produce venodilatation that reduces systemic and pulmonary venous resistances. As a consequence, right atrial pressure, pulmonary capillary pressure, and LVEDP decrease. The preload reduction improves the signs of pulmonary congestion and decreases myocardial wall tension and ventricular size, which in turn reduce oxygen consumption. With higher doses, nitrates produce arterial vasodilatation that decreases peripheral vascular resistance and mean arterial pressure, leading to a decrease in afterload, and thereby reduce oxygen consumption. This arterial vasodilatation increases cardiac output, counteracting the possible reduction caused by the reduction in preload caused by venodilatation. The overall effect on cardiac output depends on the LVEDP; when LVEDP is high, nitrates increase cardiac output, while when it is normal nitrates can decrease cardiac output. Nitrates can also produce coronary vasodilatation, as much through reducing preload as through a direct effect on the vascular endothelium. This vasodilatation can decrease the mechanical compression of subendocardial vessels and increases blood flow at this level. Additionally, nitrates reduce coronary vascular tone, overcoming vasospasm. • Gasto cardiaco • Presión arterial

59
NITRATOS CAPACIDAD FUNCIONAL ISOSORBIDE 5 - MONONITRATO
100 200 300 400 n=24 392 384 ** ** TIEMPO EJERCICIO, 267 segundos Treatment of Heart Failure. Nitrates: Functional capacity Effect of isosorbide 5-mononitrate on functional capacity (maximal exercise time) in chronic heart failure patients. TID dosing of 20mg is effective both short-term and overall compared to pre-treatment control. Jansen W et al. Med Welt 1982;33:1756 Control 1 dosis 4 semanas ISOSORBIDE 5 - MONONITRATO Jansen W et al Med Welt 1982;33:1756 20 mg / 8h
 in chronic heart failure patients. TID dosing of 20mg is effective both short-term and overall compared to pre-treatment control. Jansen W et al. Med Welt 1982;33:1756. Control. 1. dosis. 4. semanas. ISOSORBIDE 5 - MONONITRATO. Jansen W et al Med Welt 1982;33: mg / 8h.")
60
NITRATOS SOBREVIDA MESES PROBABILIDAD DE MUERTE 0.7 0.6 0.5 0.4 0.3
Placebo (273) Prazosin (183) Hz + ISDN (186) 0.6 0.5 PROBABILIDAD DE MUERTE 0.4 0.3 Treatment of Heart Failure. Nitrates: Survival Mortality curves of heart failure patients. In men with class II-III heart failure, the VHeFT-I study showed that for patients already treated with digoxin and diuretics, the combination of hydralazine (300mg/day) and isosorbide dinitrate (160mg/day) improved symptoms and functional status. More importantly, combination therapy was associated with a 23% reduction in mortality at 3 years; this effect was not seen in patients treated with prazosin (30mg/day). Selection of the treatment arms in this study was based on certain suppositions. The placebo group received digitalis and diuretics, and subsequent to this study the combination has been administered obligatorily in control groups. The combined administration of hydralazine (arterial vasodilator) and a nitrate (venodilator) was designed to provide equilibrated vasodilatation. Prazosin combined both arterial and venous vasodilatory capacities in one medication, and was initially assumed to be better than combination therapy. The lack of effect of prazosin was probably due to development of tolerance. Perhaps the most relevant finding of the study was that, in practice, the effects of a medicine on symptoms or hemodynamic effects do not correlate well with effects on overall survival. Veterans Administration Cooperative Study (VHefT-1). N Engl J Med 1986;314:1547 0.2 0.1 VHefT-1 N Engl J Med 1986;314:1547 6 12 18 24 30 36 42 MESES
 Prazosin (183) Hz + ISDN (186) PROBABILIDAD DE MUERTE Treatment of Heart Failure. Nitrates: Survival. Mortality curves of heart failure patients. In men with class II-III heart failure, the VHeFT-I study showed that for patients already treated with digoxin and diuretics, the combination of hydralazine (300mg/day) and isosorbide dinitrate (160mg/day) improved symptoms and functional status. More importantly, combination therapy was associated with a 23% reduction in mortality at 3 years; this effect was not seen in patients treated with prazosin (30mg/day). Selection of the treatment arms in this study was based on certain suppositions. The placebo group received digitalis and diuretics, and subsequent to this study the combination has been administered obligatorily in control groups. The combined administration of hydralazine (arterial vasodilator) and a nitrate (venodilator) was designed to provide equilibrated vasodilatation. Prazosin combined both arterial and venous vasodilatory capacities in one medication, and was initially assumed to be better than combination therapy. The lack of effect of prazosin was probably due to development of tolerance. Perhaps the most relevant finding of the study was that, in practice, the effects of a medicine on symptoms or hemodynamic effects do not correlate well with effects on overall survival. Veterans Administration Cooperative Study (VHefT-1). N Engl J Med. 1986;314: VHefT-1. N Engl J Med 1986;314: MESES.")
61
NITRATOS TOLERANCIA " Disminución en el efecto de una droga
cuando se administra en una forma prolongada" Se presenta con todos los nitratos Es dosis-dependiente Desaparece en 24 h. después de parar la droga Tolerancia puede ser evitada Usando la menor dosis efectiva Creando niveles plasmáticos discontinuos Treatment of Heart Failure. Nitrates: Tolerance Repetitive administration of nitrates over days is accompanied by a reduction in intensity and duration of its effects (tolerance), that obligates sequential increases in dose to obtain the desired effect. Nitrate tolerance appears with all nitrates, crosses over from one nitrate preparation to another (explaining the poor effect that IV NTG can have in patients on oral nitrate therapy), and is not dose dependent. Additionally, tolerance appears within 8-24 hours of administration of preparations that allow for maintenance of stable plasma nitrate levels (i.v., patch), but disappears rapidly (<48hrs) after stopping treatment. Increasing dosage does not overcome the tolerance effect. Tolerance can be avoided, however, by using the lowest effective dose, and by avoiding continuous plasma levels (drug-free periods).
, that obligates sequential increases in dose to obtain the desired effect. Nitrate tolerance appears with all nitrates, crosses over from one nitrate preparation to another (explaining the poor effect that IV NTG can have in patients on oral nitrate therapy), and is not dose dependent. Additionally, tolerance appears within 8-24 hours of administration of preparations that allow for maintenance of stable plasma nitrate levels (i.v., patch), but disappears rapidly (<48hrs) after stopping treatment. Increasing dosage does not overcome the tolerance effect. Tolerance can be avoided, however, by using the lowest effective dose, and by avoiding continuous plasma levels (drug-free periods).")
62
NITRATOS TOLERANCIA Puede ser evitada o minimizada
Administración intermitente Usar la dosis más baja posible Interponer intervalos libres de nitratos Buscar picos y valles en niveles plasmáticos Recuperar la sensibilidad a los nitratos del músculo liso vascular durante los nadires Parches: remover después de 8-10 h Treatment of Heart Failure. Nitrates: Tolerance Tolerance can be minimized through intermittent dosing, using the lowest possible dose, and allowing for “drug-free periods”. Peaks and valleys of drug levels occur; during valleys the plasma concentration is less than the minimal effective concentration, which allows the vascular smooth muscle to recover its nitrate-sensitivity. For this reason it is recommended to use oral nitrates 2-3 times during the day and to remove the nitrate patches for a 12 hour period.

63
NITRATOS TOLERANCIA NTG s.l. ISDN I 5-MN NTG percutánea
V I D A M E NTG s.l. ISDN I 5-MN NTG percutánea Treatment of Heart Failure. Nitrates: Tolerance Tolerance is related to the duration of the nitrate effects, such that the longer the half-life, the higher the risk that tolerance will occur.

64
NITRATOS CONTRAINDICACIONES
Hipersensibilidad previa Hipotensión ( < 80 mmHg) IAM con presión de llenado ventricular baja 1er trimestre del embarazo Treatment of Heart Failure. Nitrates: Contraindications Nitrates are contraindicated in patients with histories of nitrate hypersensitivity, marked hypertension or shock, acute infarction with low filling pressures, and first-trimester pregnancy. They should also not be given to patients with anemia, increased intracranial pressure, severe aortic or mitral stenosis, cardiac tamponade, constrictive pericarditis or coronary thrombosis. Nitrates can aggravate angina in the setting of hypertrophic cardiomyopathy. CON PRECAUCION: Pericarditis constrictiva Hipertensión intracraneana Cardiomiopatía hipertrófica
 IAM con presión de llenado ventricular baja. 1er trimestre del embarazo. Treatment of Heart Failure. Nitrates: Contraindications. Nitrates are contraindicated in patients with histories of nitrate hypersensitivity, marked hypertension or shock, acute infarction with low filling pressures, and first-trimester pregnancy. They should also not be given to patients with anemia, increased intracranial pressure, severe aortic or mitral stenosis, cardiac tamponade, constrictive pericarditis or coronary thrombosis. Nitrates can aggravate angina in the setting of hypertrophic cardiomyopathy. CON PRECAUCION: Pericarditis constrictiva. Hipertensión intracraneana. Cardiomiopatía hipertrófica.")
65
NITRATOS USOS CLINICOS
Congestión pulmonar Disnea paroxística nocturna y ortopnea Isquemia miocárdica con ICC En ICC aguda y en edema pulmonar: NTG s.l. o i.v. Treatment of Heart Failure. Nitrates: Use in Heart Failure Through venodilation, nitrates reduce LVEDP, PAD, and PCWP, thereby improving pulmonary congestion and exercise tolerance. The reduction in end-diastolic pressure and volume decrease wall tension and oxygen consumption. Cardiac output and arterial pressure are not significantly changed, although a decrease in the LVEDP of 12 mmHg can decrease cardiac output. Nitrates are particularly useful in patients with signs of pulmonary congestion (PCWP > 18 mm Hg) and normal cardiac outputs, or in patients with orthopnea and PND. Recommended doses are well tolerated and rarely cause reflex tachycardia or hypotension. In patients with acute heart failure accompanied by pulmonary edema nitroglycerine can be given sublingually or i.v. I.V. administration allows for immediate onset of action, and rapid disappearance of effect within minutes of stopping the infusion. Patients receiving I.V. nitroglycerin should be monitored. In patients with low cardiac output, nitrates can be used in conjunction with arterial vasodilators, dopamine, or dobutamine. In the treatment of chronic heart failure preparations with long half-lives are used. Topical nitroglycerine and other nitrates administered qHS are effective in patients with orthopnea and PND.
 and normal cardiac outputs, or in patients with orthopnea and PND. Recommended doses are well tolerated and rarely cause reflex tachycardia or hypotension. In patients with acute heart failure accompanied by pulmonary edema nitroglycerine can be given sublingually or i.v. I.V. administration allows for immediate onset of action, and rapid disappearance of effect within minutes of stopping the infusion. Patients receiving I.V. nitroglycerin should be monitored. In patients with low cardiac output, nitrates can be used in conjunction with arterial vasodilators, dopamine, or dobutamine. In the treatment of chronic heart failure preparations with long half-lives are used. Topical nitroglycerine and other nitrates administered qHS are effective in patients with orthopnea and PND.")
66
IECA MECANISMO DE ACCION E.C.A. Kininasa II
VASOCONSTRICCION VASODILATACION ALDOSTERONA PROSTAGLANDINAS VASOPRESINA Kininógeno tPA SNS Kalikreina Angiotensinógeno RENINA BRADIKININA Treatment of Heart Failure Angiotensin Converting-Enzyme Inhibitors (ACEI) :Mechanisms of action ACE-inhibitors competitively block the converting enzyme that transforms angiotensin I into angiotensin II. The reduction in angiotensin II levels explains its arteriovenous vasodilatory actions, as angiotensin II is a potent vasoconstrictor that augments sympathetic tone in the arteriovenous system. Additionally, angiotensin causes vasopressin release and produces sodium and water retention, both through a direct renal effect and through the liberation of aldosterone. Since converting enzyme has a similar structure to kinase II that degrades bradykinin, ACE-inhibitors increase kinin levels that are potent vasodilators (E2 and F2) and increase release of fibrinolytic substances such as tPA. Angiotensina I E.C.A. Inhibidor Kininasa II ANGIOTENSINA II Fragmentos inactivos
 :Mechanisms of action. ACE-inhibitors competitively block the converting enzyme that transforms angiotensin I into angiotensin II. The reduction in angiotensin II levels explains its arteriovenous vasodilatory actions, as angiotensin II is a potent vasoconstrictor that augments sympathetic tone in the arteriovenous system. Additionally, angiotensin causes vasopressin release and produces sodium and water retention, both through a direct renal effect and through the liberation of aldosterone. Since converting enzyme has a similar structure to kinase II that degrades bradykinin, ACE-inhibitors increase kinin levels that are potent vasodilators (E2 and F2) and increase release of fibrinolytic substances such as tPA. Angiotensina I. E.C.A. Inhibidor. Kininasa II. ANGIOTENSINA II. Fragmentos inactivos.")
67
EFECTOS HEMODINAMICOS
IECA EFECTOS HEMODINAMICOS Vasodilatación arterial PAD, PCP y PTDVI RVS y PA GC y tolerancia al ejercicio No cambio en FC / contractilidad MVO2 Flujo renal, coronario y cerebral Diuresis y natriuresis Treatment of Heart Failure. Angiotensin Converting-Enzyme Inhibitors (ACEI): Mechanisms of action ACE-inhibitors cause arteriovenous vasodilatation. Venodilation is accompanied by reduction in PAD, PCWP, and LVEDP. Arterial vasodilatation decreases SVR and MAP and increases cardiac output, ejection fraction, and exercise tolerance. Heart rate and contractility do not change, and, thus, double product and myocardial oxygen demand are decreased. These effects are more noticeable in patients with low sodium levels, in whom there is an increased plasma renin activity. Vasodilatation is seen in various vascular territories: renal, coronary, cerebral, and musculoskeletal (increasing exercise capacity). Additionally, ACE-inhibitors cause diuretic and natriuretic effects that are a consequence of the inhibition of angiotensin II and aldosterone synthesis, as well as the increase in cardiac output and renal perfusion. It is now known that the magnitude and duration of blood pressure reduction correlates better with the activity of ACE in certain tissues (heart, vessels, kidney, adrenal, etc.) than with its plasma levels, which indicates that ACE-inhibitors act by inhibiting local tissue production of angiotensin II. Plasma levels of ACE are not good predictors of the magnitude of hemodynamic effects of ACE-inhibition.
: Mechanisms of action. ACE-inhibitors cause arteriovenous vasodilatation. Venodilation is accompanied by reduction in PAD, PCWP, and LVEDP. Arterial vasodilatation decreases SVR and MAP and increases cardiac output, ejection fraction, and exercise tolerance. Heart rate and contractility do not change, and, thus, double product and myocardial oxygen demand are decreased. These effects are more noticeable in patients with low sodium levels, in whom there is an increased plasma renin activity. Vasodilatation is seen in various vascular territories: renal, coronary, cerebral, and musculoskeletal (increasing exercise capacity). Additionally, ACE-inhibitors cause diuretic and natriuretic effects that are a consequence of the inhibition of angiotensin II and aldosterone synthesis, as well as the increase in cardiac output and renal perfusion. It is now known that the magnitude and duration of blood pressure reduction correlates better with the activity of ACE in certain tissues (heart, vessels, kidney, adrenal, etc.) than with its plasma levels, which indicates that ACE-inhibitors act by inhibiting local tissue production of angiotensin II. Plasma levels of ACE are not good predictors of the magnitude of hemodynamic effects of ACE-inhibition.")
68
IECA CAPACIDAD FUNCIONAL
100 No Tratamiento Adicional Necesario (%) 95 Quinapril Continución n=114 90 p<0.001 85 Treatment of Heart Failure Angiotensin Converting-Enzyme Inhibitors: Effect on Mortality The effect of discontinuation of quinapril therapy on patients with class II-III heart failure in the Quinapril Heart Failure Trial is shown. At 20 weeks of treatment the group whose quinapril treatment was terminated had increased symptoms compared to the group who continued to receive quinapril therapy. The latter group maintained a stable functional status. This study, whose design was similar to PROVD and RADIANCE, again demonstrates the efficacy of ACE-inhibitors in the treatment of heart failure. Pflugfelder PW et al. J Am Coll Cardiol 1993;22:1557. Quinapril detenido Placebo n=110 80 Clase II-III 75 12 6 2 10 4 8 18 20 14 16 Quinapril Heart Failure Trial JACC 1993;22:1557 Semanas
 95. Quinapril. Continución. n= p< Treatment of Heart Failure. Angiotensin Converting-Enzyme Inhibitors: Effect on Mortality. The effect of discontinuation of quinapril therapy on patients with class II-III heart failure in the Quinapril Heart Failure Trial is shown. At 20 weeks of treatment the group whose quinapril treatment was terminated had increased symptoms compared to the group who continued to receive quinapril therapy. The latter group maintained a stable functional status. This study, whose design was similar to PROVD and RADIANCE, again demonstrates the efficacy of ACE-inhibitors in the treatment of heart failure. Pflugfelder PW et al. J Am Coll Cardiol 1993;22:1557. Quinapril. detenido. Placebo. n= Clase II-III Quinapril Heart Failure Trial. JACC 1993;22:1557. Semanas.")
69
IECA VENTAJAS Inhiben remodelamiento VI post-IM
Modifican la progresión de la ICC crónica Sobrevida Hospitalizaciones Mejoría de la calidad de vida En contraste con otros vasodilatores, no producen activación neurohormonal o taquicardia refleja No se desarrolla tolerancia a sus efectos Treatment of Heart Failure. Angiotensin Converting-Enzyme Inhibitors (ACEI) : Advantages In class II-IV heart failure patients treated with diuretics and digitalis, ACE-inhibitors decrease symptoms, improve hemodynamics and functional class, and increase exercise tolerance. Additionally, they reduce left ventricular dimensions, improve the cardiothoracic index, improve renal function, and improve hyponatremia. More importantly, ACE-inhibitors are the best drugs to date for preventing expansion and dilatation of the left ventricle post infarction, thereby decreasing the number and duration of hospitalizations, and improving symptoms and survival. They also retard progression to heart failure in patients with asymptomatic ventricular dysfunction. ACE-inhibitors differ from other vasodilators in that they do not produce neurohormonal activation or reflex tachycardia, and tolerance to these agents does not seem to develop over time. ACE-inhibitors increase plasma renin, bradykinin, and angiotensin I activities, and reduce plasma and tissue levels of angiotensin II, and plasma levels of aldosterone and cortisol. ACE-inhibitors can also decrease plasma norepinephrine levels, especially after long-term therapy, which has been attributed to the suppression of the stimulating effect angiotensin II has on the synthesis and release of norepinephrine. ACE-inhibitors also reduce arginine-vasopressin levels.
 : Advantages. In class II-IV heart failure patients treated with diuretics and digitalis, ACE-inhibitors decrease symptoms, improve hemodynamics and functional class, and increase exercise tolerance. Additionally, they reduce left ventricular dimensions, improve the cardiothoracic index, improve renal function, and improve hyponatremia. More importantly, ACE-inhibitors are the best drugs to date for preventing expansion and dilatation of the left ventricle post infarction, thereby decreasing the number and duration of hospitalizations, and improving symptoms and survival. They also retard progression to heart failure in patients with asymptomatic ventricular dysfunction. ACE-inhibitors differ from other vasodilators in that they do not produce neurohormonal activation or reflex tachycardia, and tolerance to these agents does not seem to develop over time. ACE-inhibitors increase plasma renin, bradykinin, and angiotensin I activities, and reduce plasma and tissue levels of angiotensin II, and plasma levels of aldosterone and cortisol. ACE-inhibitors can also decrease plasma norepinephrine levels, especially after long-term therapy, which has been attributed to the suppression of the stimulating effect angiotensin II has on the synthesis and release of norepinephrine. ACE-inhibitors also reduce arginine-vasopressin levels.")
70
IECA SOBREVIDA Placebo Enalapril PROBABILIDAD DE MUERTE CONSENSUS
0.8 0.7 Placebo 0.6 PROBABILIDAD DE MUERTE p< 0.001 0.5 0.4 p< 0.002 0.3 Enalapril Treatment of Heart Failure. Angiotensin Converting-Enzyme Inhibitors (ACEI): Survival CONSENSUS. Prolonged administration of ACE-inhibitors reduces mortality in symptomatic heart failure. The first study to demonstrate this effect was CONSENSUS I. This graph shows the cumulative mortality curves of the treatment and placebo group in this randomized, double-blind trial. The study analyzed the effect of enalapril on prognosis of 253 patients with class IV heart failure, who also received digitalis, diuretics, and conventional vasodilators. At the end of 6 months of treatment, there was a clear-cut improvement in functional class, a reduction in the need for medications, and a 40% reduction in mortality (p<0.002). After 12 months the mortality reduction was 31% (p<0.001). Nonetheless, there were no differences in the incidence of sudden death between the two groups, or in the sub-group that received other conventional vasodilators. Another characteristic of this study was variability of the dose that was used for each patient (adjusted for tolerance and symptoms): mg/day. This aspect shows the importance of individualized treatment for heart failure patients. The CONSENSUS Trial Study Group. N Engl J Med 1987;316:1429. 0.2 0.1 CONSENSUS N Engl J Med 1987;316:1429 1 2 3 4 5 6 7 8 9 10 11 12 MESES
: Survival. CONSENSUS. Prolonged administration of ACE-inhibitors reduces mortality in symptomatic heart failure. The first study to demonstrate this effect was CONSENSUS I. This graph shows the cumulative mortality curves of the treatment and placebo group in this randomized, double-blind trial. The study analyzed the effect of enalapril on prognosis of 253 patients with class IV heart failure, who also received digitalis, diuretics, and conventional vasodilators. At the end of 6 months of treatment, there was a clear-cut improvement in functional class, a reduction in the need for medications, and a 40% reduction in mortality (p<0.002). After 12 months the mortality reduction was 31% (p<0.001). Nonetheless, there were no differences in the incidence of sudden death between the two groups, or in the sub-group that received other conventional vasodilators. Another characteristic of this study was variability of the dose that was used for each patient (adjusted for tolerance and symptoms): mg/day. This aspect shows the importance of individualized treatment for heart failure patients. The CONSENSUS Trial Study Group. N Engl J Med 1987;316: CONSENSUS. N Engl J Med 1987;316: MESES.")
71
IECA SOBREVIDA Placebo n=2117 % MORTALIDAD Enalapril n=2111 50 40 30
20 Enalapril n=2111 Treatment of Heart Failure. Angiotensin Converting-Enzyme Inhibitors (ACEI): Survival Mortality curves in patients with asymptomatic ventricular dysfunction in the SOLVD study. This study compared the effect of enalapril versus placebo in 4228 asymptomatic patients with EF < 35% who were previously untreated. Overall mortality was similar in both groups (15.8% vs. 14.8%, NS), but in the enalapril arm a reduction in development of clinical symptoms of heart failure or need for hospitalization was seen. Once again, patients with the lowest EF’s were those who benefited the most from therapy. The SOLVD Investigators. N Engl J Med1992;327:685 n = 4228 No síntomas ICC FE < 35 10 6 12 18 24 30 36 42 48 SOLVD (Prevención) N Engl J Med 1992;327:685 Meses
: Survival. Mortality curves in patients with asymptomatic ventricular dysfunction in the SOLVD study. This study compared the effect of enalapril versus placebo in 4228 asymptomatic patients with EF < 35% who were previously untreated. Overall mortality was similar in both groups (15.8% vs. 14.8%, NS), but in the enalapril arm a reduction in development of clinical symptoms of heart failure or need for hospitalization was seen. Once again, patients with the lowest EF’s were those who benefited the most from therapy. The SOLVD Investigators. N Engl J Med1992;327:685. n = No síntomas ICC. FE < SOLVD (Prevención) N Engl J Med 1992;327:685. Meses.")
72
IECA SOBREVIDA Mortalidad % Placebo Enalapril 50 40 30 20 10 48 6 12
p = Placebo n=1284 Mortalidad % Enalapril n=1285 Treatment of Heart Failure Angiotensin Converting-Enzyme Inhibitors (ACEI) : Survival SOLVD study-symptomatic heart failure. Mortality curves in patients with clinical heart failure in the SOLVD treatment study. In this study, 2589 symptomatic heart failure patients with EFs<35% (90% in functional class II – III) were randomized to receive enalapril or placebo. Mortality over a 41 month follow-up period was 39.7% in the enalapril arm and 35.2% in the placebo arm (p<0.004). The mortality reduction was chiefly mediated through less progression of heart failure; deaths due to arrhythmia were not reduced. Additionally, the enalapril group required fewer hospitalizations for heart failure. The SOLVD Investigators. N Engl J Med 1991;325:293 n = 2589 ICC - NYHA II-III - FE < 35 48 6 12 18 24 30 36 42 SOLVD (Tratamiento) N Engl J M 1991;325:293 Meses
 : Survival. SOLVD study-symptomatic heart failure. Mortality curves in patients with clinical heart failure in the SOLVD treatment study. In this study, 2589 symptomatic heart failure patients with EFs<35% (90% in functional class II – III) were randomized to receive enalapril or placebo. Mortality over a 41 month follow-up period was 39.7% in the enalapril arm and 35.2% in the placebo arm (p<0.004). The mortality reduction was chiefly mediated through less progression of heart failure; deaths due to arrhythmia were not reduced. Additionally, the enalapril group required fewer hospitalizations for heart failure. The SOLVD Investigators. N Engl J Med 1991;325:293. n = ICC. - NYHA II-III. - FE < SOLVD (Tratamiento) N Engl J M 1991;325:293. Meses.")
73
IECA SOBREVIDA Mortalidad % Años 30 Placebo 20 Captopril 10 1 2 3 4
Disfunción ventricular post IM asintomática Placebo n=1116 Mortalidad % 20 Captopril n=1115 Treatment of Heart Failure Angiotensin Converting-Enzyme Inhibitors (ACEI): Survival SAVE (Survival and Ventricular Enlargement). Mortality curves in the SAVE study in patients with varying degrees of post-infarct ventricular dysfunction. In this study, 2231 patients with EF < 40% were randomized to receive captopril or placebo between 3 to 16 days after experiencing a transmural infarct. After 42 months, the captopril group had a significant reduction in overall mortality (-19%), number of reinfarctions (-25%), hospitalizations (-22%), and in the number of patients who developed clinical congestive heart failure. The mortality reduction appeared after 1 year of treatment. Pfeffer MA et al. Survival and Ventricular Enlargement (SAVE) Study. NEngl J Med 1992;327:669. 10 n = 2231 días post IAM FE < 40 mg / day ² -19% p=0.019 SAVE N Engl J Med 1992;327:669 1 2 3 4 Años
: Survival. SAVE (Survival and Ventricular Enlargement). Mortality curves in the SAVE study in patients with varying degrees of post-infarct ventricular dysfunction. In this study, 2231 patients with EF < 40% were randomized to receive captopril or placebo between 3 to 16 days after experiencing a transmural infarct. After 42 months, the captopril group had a significant reduction in overall mortality (-19%), number of reinfarctions (-25%), hospitalizations (-22%), and in the number of patients who developed clinical congestive heart failure. The mortality reduction appeared after 1 year of treatment. Pfeffer MA et al. Survival and Ventricular Enlargement (SAVE) Study. NEngl J Med 1992;327: n = días post IAM. FE < mg / day. ² -19% p= SAVE. N Engl J Med 1992;327: Años.")
74
IECA SOBREVIDA POST IM IECA Beneficio Selección pt ISIS-4 Captopril
0.5 / 5 sem Todos con IAM GISSI-3 Lisinopril 0.8 / 6 sem Todos con IAM SAVE Captopril 4.2 / 3.5 a FE < 40 Asintomático Treatment of Heart Failure. Angiotensin Converting-Enzyme Inhibitors (ACEI) : Survival Post-infarction studies. The results of the various studies that have compared ACE-inhibitors with placebo in the post-MI setting have differing results. Nonetheless, the benefit obtained in each study correlates with the degree of ventricular dysfunction of the selected patients. In this graph, the difference in mortality over time is seen in absolute terms (lives saved per 100 patients treated = % mortality in placebo group - % mortality in ACEI group/ follow-up time). Even though the studies demonstrated statistically significant differences between placebo and ACE-inhibitor therapy, the benefit of treatment is minimal in low-risk patients, probably not justifying its routine use in every post-MI patient (ISIS-4 and GISSI-3). Benefits are moderate in patients with higher risk (asymptomatic ventricular dysfunction) (SAVE and SMILE), and maximal in patients with sever ventricular dysfunction or clinical heart failure (TRACE and AIRE). ISIS-4: Lancet 1995; 345:669 GISSI-3: Lancet 1994;343:1115 SAVE: N Engl J Med 1992;327:669. SMILE: N Engl J Med 1992;332:80. TRACE: N Engl J Med. 1995; 333:1670. AIRE: Lancet 1993; 342: 821. SMILE Zofenopril 4.1 / 1 a IAM ant., no TRL TRACE Trandolapril 7.6 / 3 a Disf Vent / ICC clínica FE < 35 AIRE Ramipril 6 / 1 a ICC clínica
 : Survival. Post-infarction studies. The results of the various studies that have compared ACE-inhibitors with placebo in the post-MI setting have differing results. Nonetheless, the benefit obtained in each study correlates with the degree of ventricular dysfunction of the selected patients. In this graph, the difference in mortality over time is seen in absolute terms (lives saved per 100 patients treated = % mortality in placebo group - % mortality in ACEI group/ follow-up time). Even though the studies demonstrated statistically significant differences between placebo and ACE-inhibitor therapy, the benefit of treatment is minimal in low-risk patients, probably not justifying its routine use in every post-MI patient (ISIS-4 and GISSI-3). Benefits are moderate in patients with higher risk (asymptomatic ventricular dysfunction) (SAVE and SMILE), and maximal in patients with sever ventricular dysfunction or clinical heart failure (TRACE and AIRE). ISIS-4: Lancet 1995; 345:669. GISSI-3: Lancet 1994;343:1115. SAVE: N Engl J Med 1992;327:669. SMILE: N Engl J Med 1992;332:80. TRACE: N Engl J Med. 1995; 333:1670. AIRE: Lancet 1993; 342: 821. SMILE. Zofenopril. 4.1 / 1 a. IAM ant., no TRL. TRACE. Trandolapril. 7.6 / 3 a. Disf Vent / ICC clínica. FE < 35. AIRE. Ramipril. 6 / 1 a. ICC clínica.")
75
IECA INDICACIONES Insuficiencia cardiaca clínica
Todos los pacientes Disfunción ventricular asintomática FEVI < 35 % Treatment of Heart Failure Angiotensin Converting-Enzyme Inhibits (ACEI) Indications. ACE-inhibitors probably constitute the cornerstone of drug therapy for heart failure, in that administration over time leads to amelioration of symptoms, beneficial hemodynamic changes, increased functional capacity, regression of structural changes, and, unequivocally, prolongation of survival. Thus, ACE-inhibitors are first-line therapy, not only in symptomatic heart failure patients, but also in patients with asymptomatic left ventricular dysfunction. The exact degree of ventricular dysfunction below which it is advisable to begin therapy with an ACE-inhibitor has not been defined; however, in general terms they can be helpful in patients with ejection fractions less than 35%.
 Indications. ACE-inhibitors probably constitute the cornerstone of drug therapy for heart failure, in that administration over time leads to amelioration of symptoms, beneficial hemodynamic changes, increased functional capacity, regression of structural changes, and, unequivocally, prolongation of survival. Thus, ACE-inhibitors are first-line therapy, not only in symptomatic heart failure patients, but also in patients with asymptomatic left ventricular dysfunction. The exact degree of ventricular dysfunction below which it is advisable to begin therapy with an ACE-inhibitor has not been defined; however, in general terms they can be helpful in patients with ejection fractions less than 35%.")
76
IECA EFECTOS INDESEABLES
Inherentes en su mecanismo de acción Hipotensión Hiperkalemia Edema angioneurótico Debidos a su estructura química Erupciones cutáneas Neutropenia, trombocitopenia Malestar digestivo Tos seca Insuf. renal Treatment of Heart Failure. Angiotensin Converting-Enzyme Inhibitors (ACEI) : Undesirable Effects These can be classified into two groups. One group includes those effects that are inherent to its mechanism of action, and therefore are common to all ACE-inhibitors. The other includes those effects that are related to the specific chemical structure of the drug. In this case, substitution of one ACE-inhibitor for another could possibly reduce the intensity of the adverse reaction (e.g. choosing an ACE-inhibitor without a sulfhydryl moiety). Disgeusia Proteinuria
 : Undesirable Effects. These can be classified into two groups. One group includes those effects that are inherent to its mechanism of action, and therefore are common to all ACE-inhibitors. The other includes those effects that are related to the specific chemical structure of the drug. In this case, substitution of one ACE-inhibitor for another could possibly reduce the intensity of the adverse reaction (e.g. choosing an ACE-inhibitor without a sulfhydryl moiety). Disgeusia. Proteinuria.")
77
IECA CONTRAINDICACIONES
Estenosis de la arteria renal Insuficiencia renal Hiperkalemia Hipotensión arterial Intolerancia (debido a efectos adversos) Treatment of Heart Failure Angiotensin Converting-Enzyme Inhibitors (ACEI) Contraindications. There are few absolute contraindications for the use of ACE-inhibitors. The most important one is the presence of renal artery stenosis. The most frequent contraindication is intolerance of the drug. Hypotension, the presence of renal insufficiency, or hyperkalemia limits their use, or the ability to administer adequate doses, in up to 20% of patients.
 Treatment of Heart Failure. Angiotensin Converting-Enzyme Inhibitors (ACEI) Contraindications. There are few absolute contraindications for the use of ACE-inhibitors. The most important one is the presence of renal artery stenosis. The most frequent contraindication is intolerance of the drug. Hypotension, the presence of renal insufficiency, or hyperkalemia limits their use, or the ability to administer adequate doses, in up to 20% of patients.")
78
ANTAGONISTAS ANGIOTENSINA II Angiotensina I ANGIOTENSINA II
MECANISMO DE ACCION RENINA Angiotensinógeno Angiotensina I ANGIOTENSINA II ECA Otras vías BLOQUEADORES RECEPTOR AT1 Treatment of congestive heart failure. Angiotensin II inhibitors Angiotensin II has different effects mediated via specific receptors. There are two types of tissue receptors for angiotensin: AT1 and AT2. Stimulation of AT1 receptors has a proliferative and vasoconstrictor effect, while stimulation of AT2 receptors has the opposite effects, that is, vasodilatory and antiproliferative. In the treatment of heart failure, specific blockade of the AT1 receptors is desirable. Drugs which create a selective and competitive block of the AT1 receptors include:losartan, valsartan, irbersartan and candersartan. RECEPTORES AT1 AT2 Vasoconstricción Acción proliferativa Vasodilatación Acción Antiproliferativa

79
ANTAGONISTAS RECEPTOR AT1 Bloqueo competitivo y selectivo
DROGAS Losartan Valsartan Irbersartan Candersartan Treatment of congestive heart failure. Angiotensin II inhibitors Drugs which create a selective and competitive block of the AT1 receptors include: losartan, valsartan, irbersartan and candersartan. Bloqueo competitivo y selectivo de los receptores AT1

80
Antagonistas receptor AT 1
Resolvd. Candesartan vs enalapril vs candesartan/enalapril. No diferencias. Menos dilatación en el grupo combinado. Elite. Losartan mejor que captopril. Elite II. Losartan igual que captopril. ValHeft. Valsartan vs placebo. Por publicarse.

81
Antagonistas receptor AT 1
En pacientes con disfunción sistólica, los inhibidores ECA permanecen como la droga de primera escogencia. Los bloqueadores del receptor de Angiotensina pueden ser considerados como una alternativa si el inhibidor de la ECA no fue tolerado Poole-Wilson PA, Pitt B. Presented at 72nd Scientific Sessions of American Heart Association, November 10, Atlanta, Georgia.

82
INHIBIDORES ALDOSTERONA
Espironolactona ALDOSTERONA Antagonista competitivo del receptor de aldosterona (miocardio, pared arterial, riñón) Retención Na+ Retención H2O Excreción K+ Excreción Mg2+ Depósito de colágeno Fibrosis - miocardio - vasos Edema Treatment of congestive heart failure. Aldosterone inhibitors: Mechanism of action Aldosterone acts directly on specific receptors. At the renal level it produces retention of sodium and water, resulting in an increase in preload and afterload, edema formation and the appearance of symptoms of pulmonary and systemic venous congestion. In addition, it increases the elimination of potassium and magnesium, creating an electrolyte imbalance which may be responsible in part for cardiac arrhythmias. At the tissue level, aldosterone stimulates the production of collagen, being in large part responsible for the fibrosis that is found in hypertrophied myocardium and in the arterial walls of patients with heart failure. The beneficial effects of spironolactone derive from the direct and competitive blockade of specific aldosterone receptors. Aldosterone inhibitors therefore have three types of effects: - Diuretic effect, which is most noticeable when fluid retention and increased levels of aldosterone are present. - Antiarrhythmic effect, mediated by the correction of hypokalemia and hypomagnesemia. - Antifibrotic effect. This effect, demonstrated in animal models, can contribute to a decrease in the progression of structural changes in patients with heart failure. Arritmias
 Retención Na+ Retención H2O. Excreción K+ Excreción Mg2+ Depósito de. colágeno. Fibrosis. - miocardio. - vasos. Edema. Treatment of congestive heart failure. Aldosterone inhibitors: Mechanism of action. Aldosterone acts directly on specific receptors. At the renal level it produces retention of sodium and water, resulting in an increase in preload and afterload, edema formation and the appearance of symptoms of pulmonary and systemic venous congestion. In addition, it increases the elimination of potassium and magnesium, creating an electrolyte imbalance which may be responsible in part for cardiac arrhythmias. At the tissue level, aldosterone stimulates the production of collagen, being in large part responsible for the fibrosis that is found in hypertrophied myocardium and in the arterial walls of patients with heart failure. The beneficial effects of spironolactone derive from the direct and competitive blockade of specific aldosterone receptors. Aldosterone inhibitors therefore have three types of effects: - Diuretic effect, which is most noticeable when fluid retention and increased levels of aldosterone are present. - Antiarrhythmic effect, mediated by the correction of hypokalemia and hypomagnesemia. - Antifibrotic effect. This effect, demonstrated in animal models, can contribute to a decrease in the progression of structural changes in patients with heart failure. Arritmias.")
83
INHIBIDORES ALDOSTERONA INDICACIONES
EFECTO DIURETICO Congestión pulmonar (disnea) Congestión sistémica (edema) EFECTOS ELECTROLITICOS Hipo K+, Hipo Mg+ Arritmias Mejor que suplementos K+ EFECTOS NEUROHORMONALES RALES Treatment of congestive heart failure. Aldosterone inhibitors: Indications Spironolactone has been used for several decades for its diuretic effect in heart failure. It is currently considered a second line diuretic, to be considered when more potent diuretics, such as the loop diuretics, are inadequate. Retention of K+ and Mg+ prompted by spironolactone has an antiarrhythmic effect which may be helpful in patients with low serum levels of those electrolytes. One indication is when potassium supplementation is required; in these cases, spironolactone administration is preferable. Finally, spironolactone, by virtue of its neurohormonal effects, probably influences the progression and prognosis of patients with heart failure. Its effect on survival is being assessed in a prospective study, compared to placebo (Randomized ALdactone Evaluation Study) in 1400 patients with chronic severe heart failure. The results of this will allow better definition of the indications for spironolactone in patients with chronic congestive heart failure.
 Congestión sistémica (edema) EFECTOS ELECTROLITICOS. Hipo K+, Hipo Mg+ Arritmias. Mejor que suplementos K+ EFECTOS NEUROHORMONALES. RALES. Treatment of congestive heart failure. Aldosterone inhibitors: Indications. Spironolactone has been used for several decades for its diuretic effect in heart failure. It is currently considered a second line diuretic, to be considered when more potent diuretics, such as the loop diuretics, are inadequate. Retention of K+ and Mg+ prompted by spironolactone has an antiarrhythmic effect which may be helpful in patients with low serum levels of those electrolytes. One indication is when potassium supplementation is required; in these cases, spironolactone. administration is preferable. Finally, spironolactone, by virtue of its neurohormonal effects, probably influences the progression and prognosis of patients with heart failure. Its effect on survival is being assessed in a prospective study, compared to placebo (Randomized ALdactone Evaluation Study) in 1400 patients with chronic severe heart failure. The results of this will allow better definition of the indications for spironolactone in patients with chronic congestive heart failure.")
84
Insuficiencia renal severa Acidosis metabólica
INHIBIDORES ALDOSTERONA CONTRAINDICACIONES Hiperkalemia Insuficiencia renal severa Acidosis metabólica Treatment of congestive heart failure. Aldosterone inhibitors: Contraindications The contraindications for spironolactone use include hyperkalemia and chronic renal insufficiency.

85
Densidad de receptores ß1
BLOQUEADORES ß-ADRENERGICOS POSIBLES EFECTOS BENEFICIOSOS Densidad de receptores ß1 Inhiben cardiotoxicidad de catecolaminas Activación neurohormonal FC Antihipertensivos y antianginosos Antiarrítmicos Antioxidante Antiproliferativo Treatment of congestive heart failure. Possible benefits of beta adrenergic blockers The use of ß-blockers in patients with heart failure is controversial. Nevertheless, this slide lists some of the potentially beneficial effects of these drugs for patients in heart failure.

86
FRACCION DE EYECCION VI
ß BLOQUEADORES SOBREVIDA 50 ß Bloqueador 40 Placebo 30 % 20 Treatment of Heart Failure. Possible Benefits of Beta-Blockers In the Beta-Blocker Heart Attack Trial the decrease in mortality associated with propranolol use was found to be inversely related to the pre-treatment ejection fraction. Beta Blocker Heart Attack Trial (BHAT). JACC 1990;16:1327 10 < 30% 30-40% > 40% BHAT JACC 1990;16:1327 FRACCION DE EYECCION VI
. JACC 1990;16: < 30% 30-40% > 40% BHAT. JACC 1990;16:1327. FRACCION DE EYECCION VI.")
87
ß BLOQUEADORES Mortalidad SI No Si 13.3% 24.3% No 19.5% 27.7%
Treatment of Heart Failure. Possible Benefits of Beta-Blockers Other indirect data that suggest a beneficial effect of beta-blocker use in heart failure or LV dysfunction can be found in the SAVE trial. In this study, 2231 patients with EF < 40% post-AMI were included. A retrospective analysis of overall mortality (at median 42 months of follow-up) showed the results that are on this slide. Mortality was lower in patients who received beta-blockers, regardless of randomization to placebo or ACE-inhibitor therapy. Mortality was lowest when beta-blocker therapy was combined with ACE-inhibitors, and maximal when neither drug was used. SAVE. Circulation 1995;92:3132 IECA No 19.5% 27.7% SAVE Circulation 1995;92:3132
 showed the results that are on this slide. Mortality was lower in patients who received beta-blockers, regardless of randomization to placebo or ACE-inhibitor therapy. Mortality was lowest when beta-blocker therapy was combined with ACE-inhibitors, and maximal when neither drug was used. SAVE. Circulation 1995;92:3132. IECA. No. 19.5% 27.7% SAVE. Circulation 1995;92:3132.")
88
BLOQUEADORES ß-ADRENERGICOS INDICACIONES y UTILIZACION
No claramente establecida Empezar con dosis muy bajas Lento aumento de la dosis ¿Suspensión lenta? Treatment of Heart Failure. Indications for Beta-Blocker Therapy In spite of more than 20 years of clinical investigation, the indication for beta-blockers in patients with heart failure has not yet been precisely established. Nonetheless, it is suggested that treatment be started with doses much lower than those used for the treatment of angina, and the dose should be increased slowly.

89
BLOQUEADORES ß-ADRENERGICOS
CANDIDATO IDEAL ? Sospecha de activación adrenérgica Arritmias Hipertensión Angina Treatment of Heart Failure. Possible Benefits of Beta-Blockers The ideal candidate for beta-blocker therapy has not yet been established. Nonetheless, having other indications for beta-blocker therapy could be an initial criterion for selection. Examples of these indications include sinus tachycardia, ventricular arrhythmia, hypertension, or angina in a heart failure patient.

90
BLOQUEADORES ß-ADRENERGICOS
CONTRAINDICACIONES Hipotensión: PA < 100 mmHg Bradicardia: FC < 50 bpm Inestabilidad clínica Bronquitis crónica, ASMA Insuficiencia renal crónica severa Treatment of Heart Failure. Beta-Blockers: Contraindications Contraindications to beta-blocker therapy in heart failure patients are the same as those for the general population.

91
CALCIOANTAGONISTAS EFECTOS POTENCIALES
Antiisquémicos Vasodilatación periférica Inotropismo Treatment of Heart Failure. Possible Benefits of Calcium-channel Blockers Calcium-channel blockers are theoretically useful in heart failure for a number of reasons, including their vasodilatory action and their anti-ischemic effect, but some have a negative inotropic effect that could be detrimental, and preclude their use.

92
CALCIOANTAGONISTAS POSIBLE UTILIDAD
Diltiazem contraindicado Verapamil y Nifedipina no recomendados Vasoselectivos (amlodipina, nisoldipina), pueden ser útiles en isquemia + ICC Amlodipina puede ser útil en ICC no isquémica Treatment of Heart Failure. Utility of Calcium-channel Blockers Use of calcium-channel blockers in patients with heart failure is still a subject of heated debate. Diltiazem is contraindicated, as are verapamil and nifedipine. It is likely that the newer dihydropyridines that have selective effects on vascular smooth muscle will be useful in treatment of heart failure. Amlodipine can be used to control myocardial ischemia in heart failure patients. In the PRAISE-2 trial, a trend towards a survival benefit was noted in the amlodipine-treated group.
, pueden ser útiles en isquemia + ICC. Amlodipina puede ser útil en ICC no isquémica. Treatment of Heart Failure. Utility of Calcium-channel Blockers. Use of calcium-channel blockers in patients with heart failure is still a subject of heated debate. Diltiazem is contraindicated, as are verapamil and nifedipine. It is likely that the newer dihydropyridines that have selective effects on vascular smooth muscle will be useful in treatment of heart failure. Amlodipine can be used to control myocardial ischemia in heart failure patients. In the PRAISE-2 trial, a trend towards a survival benefit was noted in the amlodipine-treated group.")
93
ANTICOAGULANTES EPISODIO EMBOLICO PREVIO FIBRILACION ATRIAL
Trombo identificado Aneurisma VI (3-6 m post IM) Clase III-IV en la presencia de: FE < 30 Aneurisma o un VI muy dilatado Flebitis Reposo en cama prolongado Treatment of Heart Failure. Anticoagulants The goal of using anticoagulants in heart failure patients is to reduce the risk of systemic and pulmonary embolism. Anticoagulation should be reserved for patients with highest risk of embolization, who are indicated in this graph. Of the possible noted indications, the only ones that are NOT controversial at present are history of previous embolism and the presence of atrial fibrillation.
 Clase III-IV en la presencia de: FE < 30. Aneurisma o un VI muy dilatado. Flebitis. Reposo en cama prolongado. Treatment of Heart Failure. Anticoagulants. The goal of using anticoagulants in heart failure patients is to reduce the risk of systemic and pulmonary embolism. Anticoagulation should be reserved for patients with highest risk of embolization, who are indicated in this graph. Of the possible noted indications, the only ones that are NOT controversial at present are history of previous embolism and the presence of atrial fibrillation.")
94
ANTIARRITMICOS TV sostenida, con/sin síntomas ß Bloqueadores
Amiodarona Muerte súbita por FV Considerar desfibrilador implantable Treatment of Heart Failure. Antiarrhythmics Approximately half of deaths in heart failure patients are attributable to arrhythmia. Nonetheless, the use of antiarrhythmics is controversial. No trial to date has shown that these agents should be used in heart failure patients as a group. Only beta-blockers and amiodarone can be considered safe, and should be used in patients with malignant ventricular arrhythmias. Consideration of AICD implantation should be given in cases of sudden death related to VF, as long as ischemic arrhythmia or another reversible cause (electrolyte imbalance, for example).
.")
95
ANTIARRITMICOS MORTALIDAD
5 10 15 13.6 13.7 ns MORTALIDAD A 2 AÑOS % n=1486 5-21d post IM Amiodarona 200 mg/d Seguimiento años Treatment of Heart Failure. Antiarrhythmics The use of antiarrhythmics in heart failure is controversial. In some studies, such as SWORD (post-infarction ventricular dysfunction), the administration of sotalol had to be suspended because of the finding of increased mortality in the treatment arm. Amiodarone is considered to be the most effective agent in the prevention of sudden death in patients with heart failure or ventricular dysfunction. This effect, however, has never been demonstrated unequivocally. In one of the most important studies, EMIAT, the administration of amiodarone did not provide an overall improvement in prognosis. Am Coll Cardiol 1996 101 / 743 102 / 743 EMIAT Am Coll Cardiol 1996 Placebo Amiodarona
, the administration of sotalol had to be suspended because of the finding of increased mortality in the treatment arm. Amiodarone is considered to be the most effective agent in the prevention of sudden death in patients with heart failure or ventricular dysfunction. This effect, however, has never been demonstrated unequivocally. In one of the most important studies, EMIAT, the administration of amiodarone did not provide an overall improvement in prognosis. Am Coll Cardiol / / 743. EMIAT. Am Coll Cardiol Placebo. Amiodarona.")
98
Terapia no farmacológica
Ultrafiltración Asistencia ventricular mecánica Resincronizadores Defibriladores implantables Cirugía (infartectomía, aneurismectomía, etc.) Células madre Inmunomodulación Trasplante
 Células madre. Inmunomodulación. Trasplante.")
99
¡Nos estamos quedando cortos!
Futuro ¡Nos estamos quedando cortos! El estudio ADHERE demostró el uso de IECA sólo en 74%, ß Bloq en 73%, instrucciones post egreso en 47% y estrategias para dejar de fumar en 64%. El uso de dopamina en pacientes externos aumentó la mortalidad a pesar de mejorar clase funcional. Los resincronizadores mejoraron calidad de vida y disminuyeron mortalidad. Los defibriladores no tienen aprobación total actualmente. NESIRETIDE aprobado en 2001 por FDA , en estudios recientes, han demostrado aumento en mortalidad y empeoramiento de la función renal.

100
Estudios recientes para bloquear endotelina y TNF-α fallaron en demostrar aumento de sobrevida en IC. La solución de la IC es la PREVENCIÓN. Estatinas, IECA, ARA II junto con la modificación de estilos de vida que disminuyan el fumado, obesidad y aumenten actividad física, son objetivos alcanzables. El mejor entendimiento de la fisiopatología, la manipulación genética, la modulación metabólica y farmacológica, así como el mejoramiento en los dispositivos electromecánicos y en la cirugía, determinan el Norte de esta pandemia.

Presentaciones similares