Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Calcificaciones extra-óseas en la IRC: diagnóstico y posibilidades terapéuticas
Walter Douthat Ateneo de Nefrologia Hospital Privado-Centro Médico de Córdoba Escuela de Posgrado, Universidad Católica de Córdoba

2
Calcificaciones vasculares
Tipos histopatologicos Diagnostico Epidemiologia Fisiopatogenia Actuales conocimientos en su manejo

3
Calcificaciones patológicas
METASTASICA: En tejido normal por alteraciones en el metabolismo del calcio y fósforo. DISTROFICA: En tejido dañado o necrótico en ausencia de alteraciones del metabolismo del calcio y fósforo.

4
Calcificaciones vasculares patológicas
INTIMA: proceso ateroesclerotico no afecta el musculo liso. Con o sin IRC. MEDIA ELASTICA: alrededor del musculo liso en ausencia de ateroesclerosis o inflamacion. Principalmente IRC o DBT. Esclerosis de Mockembec

5
Patron Vascular INTIMA: arterias de gran o mediano tamańo.
MEDIA ELASTICA: cualquier tamańo, incluyendo pequeńas arterias. *ARTERIOLOPATIA UREMICA CALCIFICANTE (calcifilaxis) afecta la media de arteriolas
 afecta la media de arteriolas.")
6
TEJIDOS AFECTADOS MORBILIDAD - MORTALIDAD CALCIFICACIONES
CARDIOVASCULARES Válvulas Mitral y Ao Miocardio Coronarias Grandes Arterias (Ao, Ilíacas y Carótidas) ICC Arritmias CALCIFICACIÓN TEJIDOS BLANDOS Infartos intestinales Pulmonares SNC Cornea y conjuntivas CALCIFILAXIS Necrosis de piel Peneana abdomen Extremidades Amputaciones MORBILIDAD - MORTALIDAD
 ICC. Arritmias. CALCIFICACIÓN TEJIDOS BLANDOS. Infartos intestinales. Pulmonares. SNC. Cornea y conjuntivas. CALCIFILAXIS. Necrosis de piel. Peneana abdomen. Extremidades Amputaciones. MORBILIDAD - MORTALIDAD.")
7
Calcificaciones vasculares
Tipos histopatologicos Diagnostico Epidemiologia Fisiopatogenia Actuales conocimientos en su manejo

8
A simple vascular Calcification score predicts cardiovascular risk in haemodialysis patients
Adragao, Neprol Dial Transp 2004

9
A simple vascular Calcification score predicts cardiovascular risk in haemodialysis patients
London et al. KI 2005

10
DIAGNOSTICO RADIOLOGICO

12
EVALUACION DE CALCIFICACIONES CORONARIAS
EBCT SCANNING EVALUACION DE CALCIFICACIONES CORONARIAS SCORE CORONARIO RIESGO 100 – 400 > 400 Muy Bajo Bajo Moderado Alto Rumberger et al. Mayo Clin Proc. 1999;74

13
CALCIFICACION DE TRES VASOS CORONARIOS

14
DIAGNOSTICO TOMOGRAFICO Calcificación cardíaca y aórtica
This slide shows myocardial calcification in a 29-year old woman on hemodialysis who had only intermittently poor control of Ca x P and PTH levels. Nevertheless, her entire ventricle is calcified.1 Approximately 2 years prior to this scan, this woman had a completely normal scan.1 1. Jing J, Kawashima A, Sickler K, Raval BK, Oldham AA. Metastatic cardiac calcification in a patient with chronic renal failure who was undergoing hemodialysis: radiographic and CT findings. Am J Roentgenol ;170: Jing J et al. Am J Roentgenol. 1998;170:

15
CALCIFILAXIS

16
Velocidad de la onda de pulso

17
Velocidad de la onda de pulso y supervivencia en diálisis

18
Calcificaciones vasculares
Tipos histopatologicos Diagnostico Epidemiologia Fisiopatogenia Actuales conocimientos en su manejo

19
FRECUENCIA CRECIENTE DE REPORTE DE LAS CALCIFICACIONES CV
Registro de NZ y Aust

20
Total Score Coronary 2786 667 151 3000 2500 2000 1500 1000 500 N= 205
None (N=35) Mild to Moderate (N=56) Severe (N=55) Very Severe (N=59) N= 205 Raggi P et al. J Am Coll Cardiol 39, 2002
 Mild to Moderate. (N=56) Severe. (N=55) Very Severe. (N=59) N= 205. Raggi P et al. J Am Coll Cardiol 39,")
21
Coronary Artery Calcification by EBCT Coronary calcification score
2500 2000 1500 Coronary calcification score 1000 500 Age (yr) 28-39 40-49 50-59 60-69 No CAD CAD HD Braun, et al. Am J Kidney Dis 27, 1996
 No CAD. CAD. HD. Braun, et al. Am J Kidney Dis 27,")
22
Calcification score log
10000 1000 100 10 1 0.1 5 10 15 20 25 30 35 Age (yr) Goodman W et al. NEJM 2000, 342
 Goodman W et al. NEJM 2000, 342.")
23
Coronary Artery Calcification Score
700 500 300 100 60 40 20 First scan Second scan Goodman W et al. NEJM 2000, 342

24
History of Coronary Heart Disease by Baseline EBCT Score
90 80 70 60 50 Prevalence of CHD (%) 40 30 20 10 1-400 >1000 Categories of Coronary Calcium Score Raggi P et al. J Am Coll Cardiol 39, 2002
 >1000. Categories of Coronary Calcium Score. Raggi P et al. J Am Coll Cardiol 39,")
25
Mortalidad cardiovascular en la población general vs los pacientes con ERC estadío 5
100 10 Relacionados con ERC Hiperfosfatemia ⇧ Ca X P ⇧ PTH - ⇩ PTH Déficit 1,25 y/o 25 (OH) D Carga de Ca++ Inflamación Desnutrición Sobrecarga de volumen Anemia Albuminuria Uso infrecuente de ASS, β Bloqueantes Annual CVD mortality† (%) 1 Factores tradicionales Edad avanzada Sexo masculino HTA DBT Tabaquismo ↑ LDL, ↓ HDL ↑ Homocisteína ↑ PCR Inactividad física Historia fliar de ECV Menopausia Predisposición genética 0.1 0.01 0.001 25-34 35-44 45-54 55-64 65-74 75-84 >85 Age (years) Foley RN et al. Am J Kidney Dis. 1998;32:S112-S119
 D. Carga de Ca++ Inflamación. Desnutrición. Sobrecarga de volumen. Anemia. Albuminuria. Uso infrecuente de ASS, β Bloqueantes. Annual CVD mortality† (%) 1. Factores tradicionales. Edad avanzada. Sexo masculino. HTA. DBT. Tabaquismo. ↑ LDL, ↓ HDL. ↑ Homocisteína ↑ PCR. Inactividad física. Historia fliar de ECV. Menopausia. Predisposición genética >85. Age (years) Foley RN et al. Am J Kidney Dis. 1998;32:S112-S119.")
26
Calcificación coronaria y mortalidad
Block GA et al; Kidney Int 2007

27
Calcificaciones vasculares
Tipos histopatologicos Diagnostico Epidemiologia Fisiopatogenia Actuales conocimientos en su manejo

28
Calcificaciones vasculares
Fisiopatogenia Ateroesclerosis

30
Calcificaciones vasculares
Fisiopatogenia Condiciones locales del musculo liso vascular

31
Modelo del efecto del aumento del Ca-PO4 sobre la mineralización del VSMC

32
32

33
Calcificaciones vasculares
Fisiopatogenia Desequilibrio entre estimulantes e inhibidores de a calcificaciones

34
Calcificaciones vasculares
Fisiopatogenia Trastornos del metabolismo mineral hiperparatiroidismo hipoparatiroidismo hiperfosfatemia hipercalcemia Vitamina D

35
Factores de riesgo de enfermedad CV en pacientes con ERC
Factores tradicionales Edad avanzada Sexo masculino HTA DBT Tabaquismo ↑ LDL, ↓ HDL ↑ Homocisteína ↑ PCR Inactividad física Historia fliar de ECV HVI Menopausia Predisposición genética Relacionados con ERC Hiperfosfatemia ⇧ Ca X P ⇧ PTH - ⇩ PTH Déficit 1,25 (OH)2 D y/o 25 (OH) D Carga diaria de Ca++ Stress oxidativo/ Inflamación Desnutrición Sobrecarga de volumen Anemia crónica Albuminuria Uso infrecuente de ASS, β Bloqueantes e hipolipemiantes
2 D y/o. 25 (OH) D. Carga diaria de Ca++ Stress oxidativo/ Inflamación. Desnutrición. Sobrecarga de volumen. Anemia crónica. Albuminuria. Uso infrecuente de ASS, β Bloqueantes e hipolipemiantes.")
36
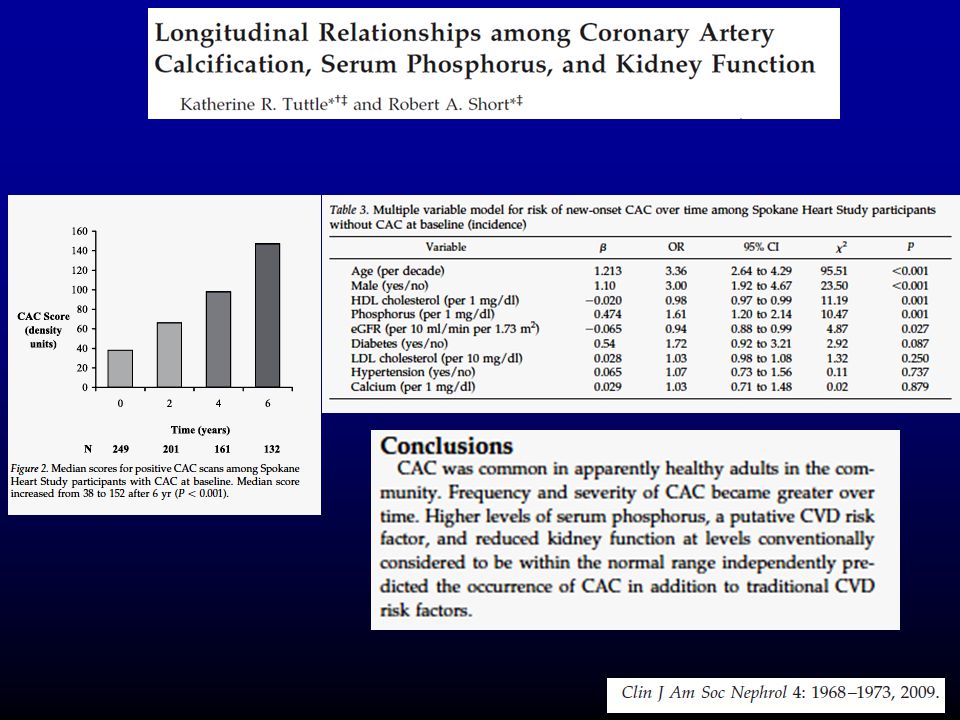
Spokane Heart Study Obj. Relacion longitudinal entre CAC, funcion renal y factores R. CV. 883 ptes con EBCT cada 2 anos y MDRD

38
VARIABLE VALOR P Edad Mujer Blancos DBT Tiempo HD Calcio Fósforo
FACTORES DE RIESGO ASOCIADO CON SCORE DE CALCIFICACION EN PACIENTES EN HD VARIABLE VALOR P Edad Mujer Blancos DBT Tiempo HD Calcio Fósforo 0.0003 0.007 0.05 0.01 0.001 0.004 Raggi P et al. J Am Coll Cardiol 39, 2002

39
Depósito en los Tejidos
Posible Efecto del Turnover Oseo sobre las Calcificaciones Extraesqueleticas PTH Bajo Turnover Oseo Alto Turnover Oseo Calcio Calcio Fósforo Fósforo Depósito en los Tejidos Calcificacion

40
Calcium-phosphate metabolism and bone histomorphometry as a function of arterial calcification
Serum PTH (pg/ml) Osteoclast Resoprtion (%) p<0.0001 p<0.001 600 3,5 500 3 2,5 400 2 300 1,5 200 1 100 0,5 1 2 3 4 1 2 3 4 CaCO3 (g Ca/d) Osteoblast Surface (%) p<0.0001 p<0.0001 2,5 14 12 2 10 1,5 8 6 1 4 0,5 2 1 2 3 4 1 2 3 4 London L et al, JASN 15, 2004
 Osteoclast Resoprtion (%) p< p< , , , , CaCO3 (g Ca/d) Osteoblast Surface (%) p< p< , , , London L et al, JASN 15,")
41
Calcificaciones vasculares
Fisiopatogenia Trastornos del metabolismo mineral FGF23 y Klotho

42
FGF23 (-) (-) (-) (-) HIPERFOSFATEMIA PARATIROIDES INTESTINO NaPiIIb
HUESO 1aOHasa TCP RENAL

43
ALTERACIONES DEL METABOLISMO DEL FOSFATO

44
Nephrol Dial Transplant (2009) 24: 2618–2620
The time course of serum FGF23 levels, serum phosphate (P) levels and fractional P excretion (FeP) from normal renal function towards end-stage kidney disease is illustrated. The association between P and FGF23 levels and mortality/morbidity in CKD stage 5D may be 3-fold: (a) P is a direct mortality factor causing cardiovascular damage; (b) FGF23 is a direct mortality factor causing cardiovascular damage; or (c) through their regulatory interaction, FGF23 is a biomarker of the cardiovascualr damage potential of phosphate loads (partly independent of the magnitude of phosphate levels). Nephrol Dial Transplant (2009) 24: 2618–2620 44
 levels and fractional P excretion (FeP) from normal renal function towards end-stage kidney disease is illustrated. The association between P and. FGF23 levels and mortality/morbidity in CKD stage 5D may be 3-fold: (a) P is a direct mortality factor causing cardiovascular damage; (b) FGF23 is a direct mortality factor causing cardiovascular damage; or (c) through their regulatory interaction, FGF23 is a biomarker of the cardiovascualr damage potential of phosphate loads (partly independent of the magnitude of phosphate levels). Nephrol Dial Transplant (2009) 24: 2618–")
45
NEJM, 2008;359: 45

46
N Engl J Med 2008;359: 46

47
N Engl J Med 2008;359: 47

48
Mirza et al. / Atherosclerosis 2009
48

49
Calcificaciones vasculares
Tipos histopatologicos Diagnostico Epidemiologia Fisiopatogenia Actuales conocimientos en su manejo

50
TRATAMIENTO Prevencion o reversion ? Hidroxiapatita - insoluble
Whitockita - insoluble Fosfato de calcio amorfo - semi soluble

51
TRATAMIENTO Prevencion o reversion ?
Trastornos del metabolismo mineral Hiperparatiroidismo Hipoparatiroidismo Hiperfosfatemia Hipocalcemia Hipovitaminosis D

52
TRATAMIENTO Hiperfosfatemia Captores orales del fosfato

53
Mean Change of score calcification at 52 weeks
Coronary Aorta 175 125 75 25 -25 -75 300 100 -100 -300 -500 -700 151 ± 56 * 185 ± 370 * - 523 ± 217 Score change (SE) Score change (SE) - 46 ± 88 Calcium (N=70) Sevelamer (N=62) Calcium (N=70) Sevelamer (N=62) * p<0.001 * p<0.001 Chertow G et al, Kidney Int 62, 2002
 Score change (SE) - 46 ± 88. Calcium. (N=70) Sevelamer. (N=62) Calcium. (N=70) Sevelamer. (N=62) * p< * p< Chertow G et al, Kidney Int 62,")
54
Effects of sevelamer and calcium on coronary artery calcification in patients new to hemodialysis
Block G, Kidney Int 68, 2005

55
CAUSAS DE MENOR CALCIFICACION VASCULAR CON SEVELAMER
Menor hipercalcemia. Menor LDL. Sobresupresión de Paratiroides con Ca. Menor carga de Calcio.

56
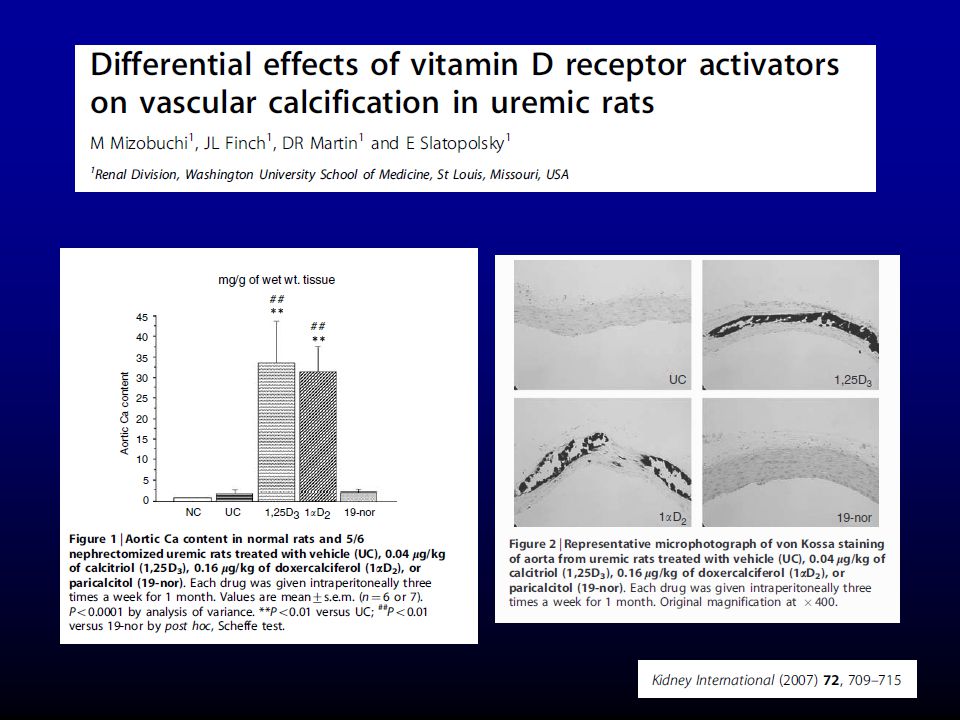
TRATAMIENTO Trastornos del Metabolismo Mineral Calcitriol
Derivados de la vitamina D

59
TRATAMIENTO Trastornos del Metabolismo Mineral Calcitriol
Derivados de la vitamina D Calcimimeticos Paratiroidectomia

60
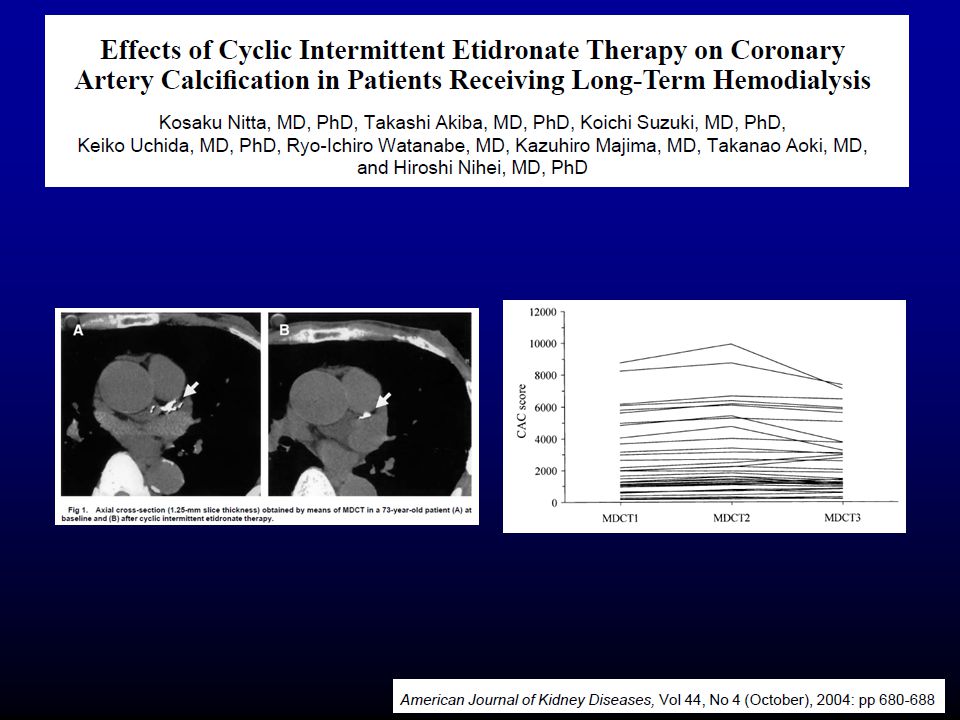
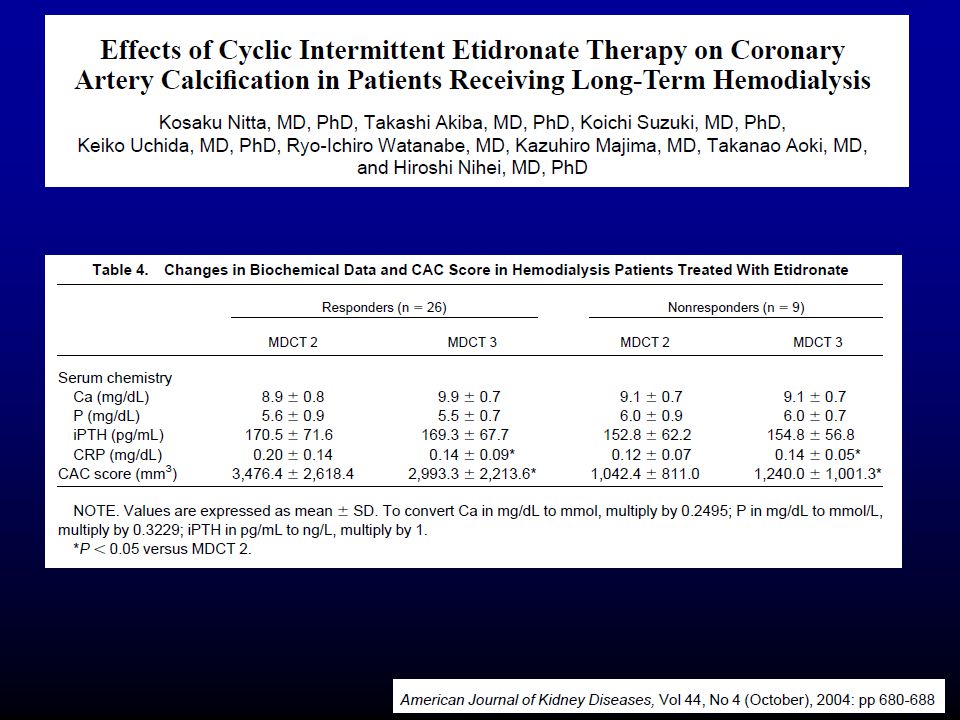
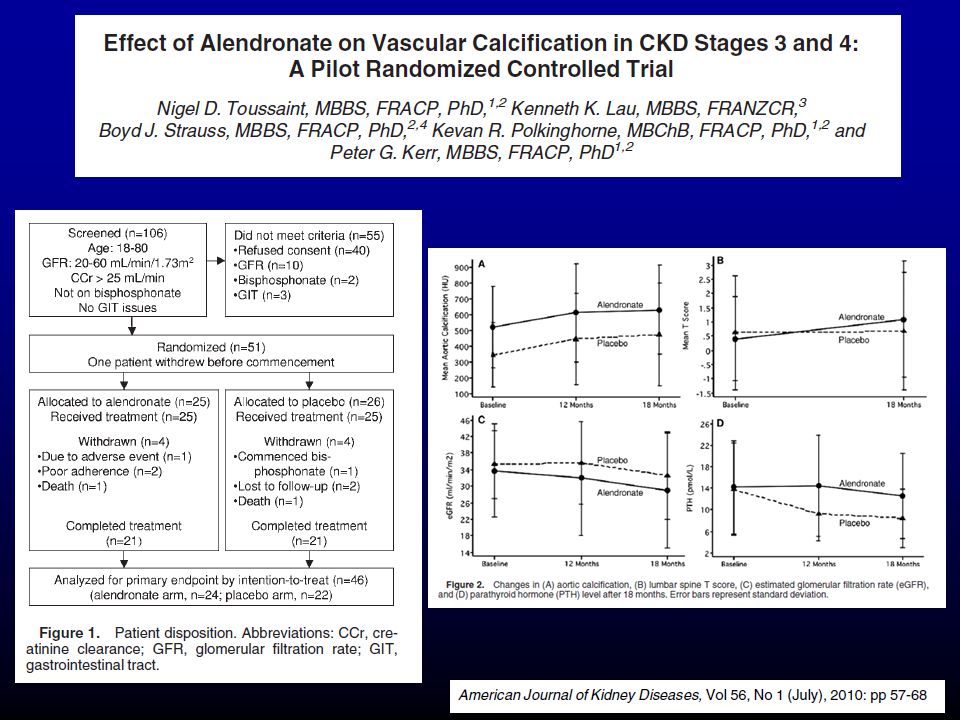
TRATAMIENTO Otras medidas terapeuticas Pirofosfato Bifosfonatos
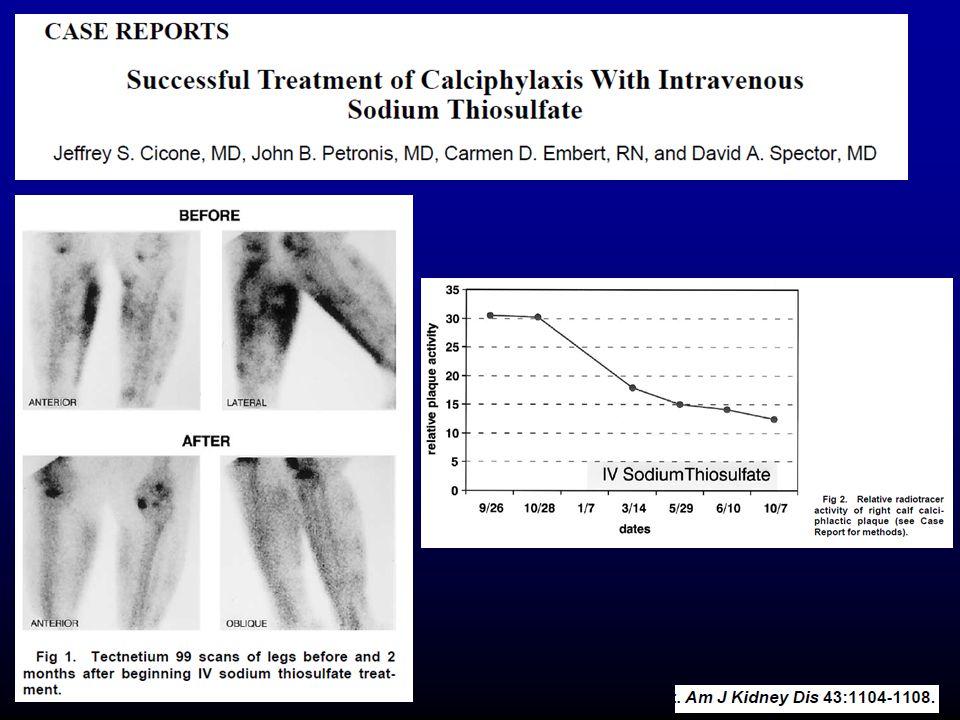
Tiosulfato

67
TRATAMIENTO Otras medidas terapeuticas Vitamina K Acidosis Fetuina A

68
Calcified Tissue International
Efecto de la warfarina y vitamina K Does prolonged warfarin exposure potentiate coronary calcification in human? Results of the Warfarin and Coronary Calcification Study T Villines, O Malley and A Taylor Warfarin inhibition of the vitamin K–dependent protein matrix gla protein, a potent inhibitor of tissue calcification. Cross-sectional analysis of the extent of coronary artery calcification (CAC) in patients without coronary heart disease, currently taking or referred for warfarin therapy. The primary end point was severity of CAC measured by EBCT. 70 ptes from three groups of warfarin use duration: (1) <6 months (n = 31, mean duration 1 ± 1 months), (2) 6–24 months (n = 11), and (3) >24 months (n = 28, mean 67 ± 40 months). In univariate analysis, there was a nonsignificant trend to increased CAC with increasing warfarin exposure (P = 0.18). Bivariate analysis revealed no correlation between warfarin duration and CAC score (r = 0.075, P = 0.537). Among patients without known coronary heart disease, duration of warfarin exposure was not associated with extent of coronary calcification. Calcified Tissue International Volume 1 / Volume 88 / 2011
 in patients without coronary heart disease, currently taking or referred for warfarin therapy. The primary end point was severity of CAC measured by EBCT. 70 ptes from three groups of warfarin use duration: (1) <6 months (n = 31, mean duration 1 ± 1 months), (2) 6–24 months (n = 11), and (3) >24 months (n = 28, mean 67 ± 40 months). In univariate analysis, there was a nonsignificant trend to increased CAC with increasing warfarin exposure (P = 0.18). Bivariate analysis revealed no correlation between warfarin duration and CAC score (r = 0.075, P = 0.537). Among patients without known coronary heart disease, duration of warfarin exposure was not associated with extent of coronary calcification. Calcified Tissue International. Volume 1 / Volume 88 /")
71
RESUMEN DE MEDIDAS GENERALES DE MANEJO

72
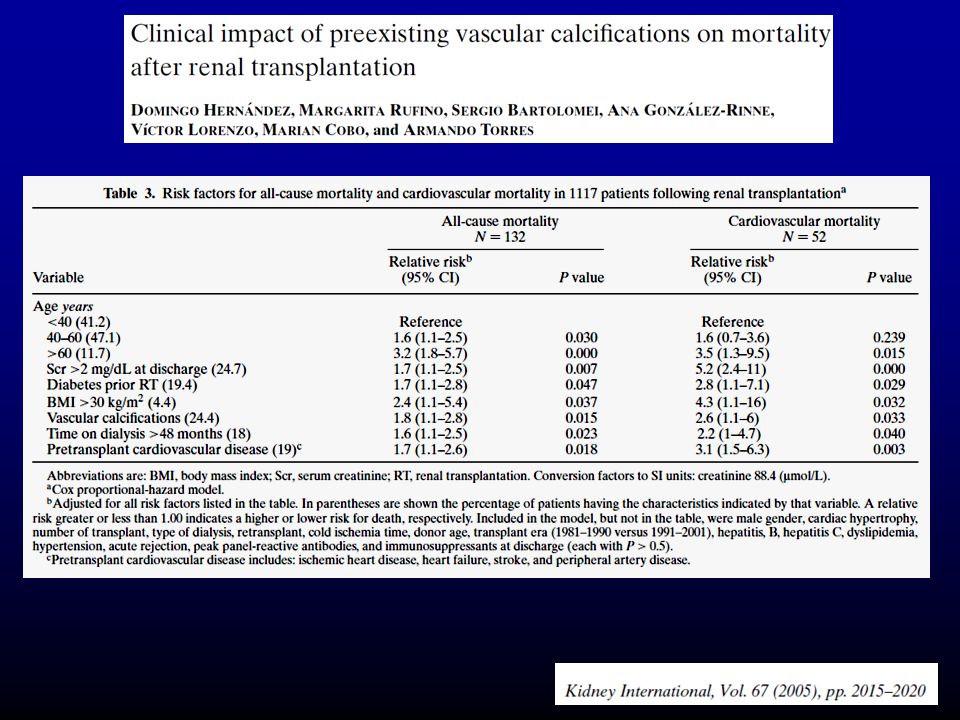
CALCIFICACIONES VASCULARES EN POS-TRASPLANTE RENAL

76
FINAL

Presentaciones similares