Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Cáncer de Pulmón TABACO Y TRATAMIENTO
Dr. Claudio Martin Servicio de Oncologia “Hospital Maria Ferrer” Servicio de Oncologia Torácica “Instituto Alexander Fleming”

3
Metastasis to distant organs Contralateral lymph node
NSCLC stages Lymph nodes Invasion of chest wall Metastasis to distant organs Main bronchus Stage IV Stage 0 Stage IA Stage IIB Stage IIIB Lung cancer is staged according to three parameters: tumour (T), lymph nodes (N) and metastatic involvement (M).1 For each of these, x indicates that the value cannot be assessed and 0 indicates that no evidence of the parameter is found. Additional stages are outlined below. Tumour stages: TIS: carcinoma in situ (confined to airway lining) T1-T4: ranging from tumour <3 cm in greatest dimension through to tumour of any size that invades the mediastinum, heart, great vessels, trachea, oesophagus, vertebral body or carina. Lymph node stages: N1: metastasis to ipsilateral peribronchial and/or ipsilateral hilar lymph nodes and intrapulmonary nodes involved by direct extension of primary tumour N2: metastasis to ipsilateral mediastinal and/or subcarinal lymph node(s) N3: metastasis to contralateral mediastinal, contralateral hilar, ipsilateral or contralateral scalene, or supraclavicular lymph node(s). Distant metastasis stages: M1: distant metastasis present. The schematic diagram shows examples of some tumour stages: Early stage 0 (carcinoma in situ): tumour is confined to the airway lining stage IA (T1 N0 M0): tumour has spread to nearby lung tissue but has not reached the main bronchus Localised stage IIB (T2 N1 M0/T3 N0 M0): tumour has reached main bronchus and local lymph nodes or direct local invasion into chest wall, diaphragm, mediastinal pleura or parietal pericardium Advanced stage IIIB (T4 Any N M0/Any T N3 M0): tumour has invaded chest wall, trachea and the contralateral lymph nodes stage IV (Any T Any N M1): distant metastasis present in the brain. Fewer than 30% of patients present with stage I or II disease.2 References Mountain CF. Chest 1997; 111: Ihde DC. N Engl J Med 1992; 327: Contralateral lymph node
, lymph nodes (N) and metastatic involvement (M).1 For each of these, x indicates that the value cannot be assessed and 0 indicates that no evidence of the parameter is found. Additional stages are outlined below. Tumour stages: TIS: carcinoma in situ (confined to airway lining) T1-T4: ranging from tumour <3 cm in greatest dimension through to tumour of any size that invades the mediastinum, heart, great vessels, trachea, oesophagus, vertebral body or carina. Lymph node stages: N1: metastasis to ipsilateral peribronchial and/or ipsilateral hilar lymph nodes and intrapulmonary nodes involved by direct extension of primary tumour. N2: metastasis to ipsilateral mediastinal and/or subcarinal lymph node(s) N3: metastasis to contralateral mediastinal, contralateral hilar, ipsilateral or contralateral scalene, or supraclavicular lymph node(s). Distant metastasis stages: M1: distant metastasis present. The schematic diagram shows examples of some tumour stages: Early. stage 0 (carcinoma in situ): tumour is confined to the airway lining. stage IA (T1 N0 M0): tumour has spread to nearby lung tissue but has not reached the main bronchus. Localised. stage IIB (T2 N1 M0/T3 N0 M0): tumour has reached main bronchus and local lymph nodes or direct local invasion into chest wall, diaphragm, mediastinal pleura or parietal pericardium. Advanced. stage IIIB (T4 Any N M0/Any T N3 M0): tumour has invaded chest wall, trachea and the contralateral lymph nodes. stage IV (Any T Any N M1): distant metastasis present in the brain. Fewer than 30% of patients present with stage I or II disease.2. References. Mountain CF. Chest 1997; 111: Ihde DC. N Engl J Med 1992; 327: Contralateral lymph node.")
4
5-year survival by TNM status in NSCLC
Stage IA IB IIA IIB IIIA IIIB IV TNM classification T1N0M0 T2N0M0 T1N1M0 T2N1M0 or T3N0M0 T1-3N2M0 orT3N1M0 T4NanyM0 or TanyN3M0 TanyNanyM1 5-year survival (%) 61 38 34 24 13 5 1 Survival progressively declines as the stage of disease at presentation advances.1 Reference Mountain CF. Chest 1997; 111: Mountain 1997
 Survival progressively declines as the stage of disease at presentation advances.1. Reference. Mountain CF. Chest 1997; 111: Mountain")
5
NSCLC: treatment options overview
Stage I Lobectomy Curative radiotherapy if surgery is contraindicated Adjuvant chemotherapy Adjuvant radiotherapy Stage II Lobectomy. Curative radiotherapy if surgery contraindicated Adjuvant chemotherapy Adjuvant radiotherapy Stage IIIA Surgery alone Chemotherapy + radiotherapy/neoadjuvant therapy Post-operative radiotherapy Radiotherapy alone Stage IIIB Chemotherapy alone Chemotherapy + radiotherapy Stage IV Chemotherapy (platinum based), modest survival benefits New chemotherapy agents External beam radiotherapy (palliative relief) Endobronchial laser or brachytherapy for obstruction Stage I:1 surgery is the treatment of choice and curative radiotherapy may be used in patients with contraindications to surgery many patients resected for stage I NSCLC may later develop regional or distant metastases. Investigations of adjuvant chemotherapy or radiotherapy following surgery are currently underway chemoprevention trials for second cancers in patients resected for stage I NSCLC are also underway. Stage II:1 many patients resected for stage II NSCLC may later develop regional or distant metastases. Investigations of adjuvant chemotherapy or radiotherapy following surgery are currently underway. Stage IIIA:1 surgery alone in highly selected cases chemotherapy combined with radiotherapy, chemotherapy plus radiotherapy followed by surgery, or chemotherapy after surgery (encouraging results for patients with good performance status). Optimal sequencing and scheduling have yet to be determined. Neoadjuvant chemotherapy could be considered for patients with good performance status surgery and post-operative radiotherapy (can improve local control but there is controversy over whether it improves survival) radiotherapy (long-term survival benefit in 5-10% of patients; patients with high performance status are most likely to benefit). Stage IIIB:1 radiotherapy alone (patients with advanced disease and high performance status are most likely to benefit) chemotherapy combined with radiotherapy (modest survival benefits compared with radiotherapy alone) chemotherapy and/or radiotherapy followed by surgery chemotherapy alone (for patients with malignant pleural effusion). Stage IV:1 cisplatin-containing combination regimens produce higher response rates than single-agent chemotherapy current treatments produce modest survival benefits compared with supportive care alone and there is no standard regimen new chemotherapy agents are being evaluated in clinical trials external radiotherapy may be used for palliation of symptoms such as compression of the trachea, oesophagus or bronchus; bone or brain metastases; local pain; vocal cord paralysis; haemoptysis; or superior vena cava syndrome endobronchial laser therapy or brachytherapy may be useful in treating lesions obstructing the proximal airways. Many patients do not receive any treatment, even first line; the proportion of patients receiving treatment reduces with the stage of the disease. Reference 1. PDQ Treatment Guidelines 2000. PDQ Guidelines 2000
, modest survival benefits. New chemotherapy agents. External beam radiotherapy (palliative relief) Endobronchial laser or brachytherapy for obstruction. Stage I:1. surgery is the treatment of choice and curative radiotherapy may be used in patients with contraindications to surgery. many patients resected for stage I NSCLC may later develop regional or distant metastases. Investigations of adjuvant chemotherapy or radiotherapy following surgery are currently underway. chemoprevention trials for second cancers in patients resected for stage I NSCLC are also underway. Stage II:1. many patients resected for stage II NSCLC may later develop regional or distant metastases. Investigations of adjuvant chemotherapy or radiotherapy following surgery are currently underway. Stage IIIA:1. surgery alone in highly selected cases. chemotherapy combined with radiotherapy, chemotherapy plus radiotherapy followed by surgery, or chemotherapy after surgery (encouraging results for patients with good performance status). Optimal sequencing and scheduling have yet to be determined. Neoadjuvant chemotherapy could be considered for patients with good performance status. surgery and post-operative radiotherapy (can improve local control but there is controversy over whether it improves survival) radiotherapy (long-term survival benefit in 5-10% of patients; patients with high performance status are most likely to benefit). Stage IIIB:1. radiotherapy alone (patients with advanced disease and high performance status are most likely to benefit) chemotherapy combined with radiotherapy (modest survival benefits compared with radiotherapy alone) chemotherapy and/or radiotherapy followed by surgery. chemotherapy alone (for patients with malignant pleural effusion). Stage IV:1. cisplatin-containing combination regimens produce higher response rates than single-agent chemotherapy. current treatments produce modest survival benefits compared with supportive care alone and there is no standard regimen. new chemotherapy agents are being evaluated in clinical trials. external radiotherapy may be used for palliation of symptoms such as compression of the trachea, oesophagus or bronchus; bone or brain metastases; local pain; vocal cord paralysis; haemoptysis; or superior vena cava syndrome. endobronchial laser therapy or brachytherapy may be useful in treating lesions obstructing the proximal airways. Many patients do not receive any treatment, even first line; the proportion of patients receiving treatment reduces with the stage of the disease. Reference. 1. PDQ Treatment Guidelines PDQ Guidelines")
6
Cáncer de Pulmón TABACO Y TRATAMIENTO
CONSIDERACIONES INCIALES I No búsqueda de datos en Clinical Trials . Solo registro al inicio de las Terapias Pocos datos de los efectos del tabaquismo y su relación con los tratamientos oncológicos. Relación tabaco QoL. Eg el retiro de nicotina puede cuasar distres emocional falsamente asociado al tratamiento.

7
Cáncer de Pulmón TABACO Y TRATAMIENTO CONSIDERACIONES INCIALES II
EL DAÑO YA ESTA HECHO CONSIDERACIONES INCIALES II Causan cáncer ¿¿¿Y después ? “Es demasiado tarde” “Ya no importa“ “El daño ya esta echo“ “Ya tiene demasiado stress con la Quimio“ ES sabido que causan cancer y lo dice claramente en la caja

8
Cáncer de Pulmón TABACO Y TRATAMIENTO
Sobrevida Global Segundos Primarios Cirugía Quimioterapia Radioterapia Nuevas Moléculas

9
Cáncer de Pulmón TABACO Y TRATAMIENTO
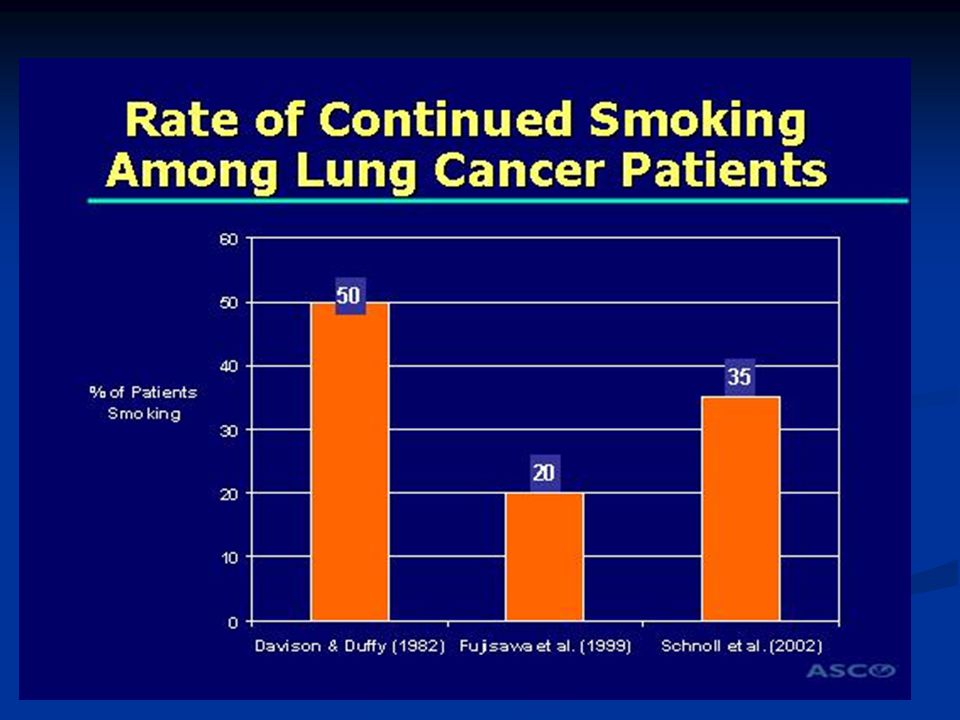
¿ Cuantos Pacientes siguen fumando luego del Diagnostico de Cáncer de Pulmón ?

10
Tabaquismo luego del Diagnostico de NSCLC Estadio I (Gritz): Cancer Causes and Control 1991 105
Estadios I NSCLC FU 4 años 60% Fumadores a baseline

11
Tabaquismo luego del Diagnostico de NSCLC Estadio I (Gritz): Cancer Causes and Control 1991 105
Restrospectivo de 3 Trials del LCSG en NSCLC I Los mas de un año de exfumadore son los que mas probalbemente se encuentren abstinentes

13
Predictores de tabaquismo luego del Cáncer (Ostroff
Predictores de tabaquismo luego del Cáncer (Ostroff.J Cancer Jan 1995 :569) 144 pacientes Carcinoma epidermoide Cabeza y Cuello Cirugía ± Radioterapia ± Quimioterapia PREDICTORES Radioterapia Postoperatoria Estadio Sitio Nivel de Escolaridad Pacientes head and neck Menos avanzadao el tumor el pacieten puede seguir fumando y n o percibe tantola gravedad de la lesion
 144 pacientes. Carcinoma epidermoide Cabeza y Cuello. Cirugía ± Radioterapia ± Quimioterapia. PREDICTORES. Radioterapia Postoperatoria. Estadio. Sitio. Nivel de Escolaridad. Pacientes head and neck. Menos avanzadao el tumor el pacieten puede seguir fumando y n o percibe tantola gravedad de la lesion.")
14
Tabaco Cáncer de Pulmón y Sobrevida (Fox : Lung Cancer 2004 44 287)
NSCLC que recibieron RT o QT /RT N 237 p Retrospectivo Estadio I II IIIa / III b

15
Tabaco Cáncer de Pulmón y Sobrevida (Fox : Lung Cancer 2004 44 287)
")
16
Tabaco Cáncer de Pulmón y Sobrevida (Fox : Lung Cancer 2004 44 287)
Pobre pronostico en estadio III puede overlapear el efecto del tabaco. Similar mortalidad cancer especifica

17
Tabaco Cáncer de Pulmón y Sobrevida Tammemagi Chest 2004 123 27
Retrospectivo N Cáncer de Pulmón Todos los estadios EX fumadores > 4 semanas Rol de la Comorbilidades

18
Tabaco Cáncer de Pulmón y Sobrevida Tammemagi Chest 2004 123 27

19
Tabaco Cáncer de Pulmón y Sobrevida Tammemagi Chest 2004 123 27
Ajustafdo con otras variavble ( co morbilidades edad sexo estadio hsitologia ) smoking al diagnostico fue el mas robusto predictor de sobrevida Los fumadorre s tiene mas riesgo de recibir menos tratameinto
 smoking al diagnostico fue el mas robusto predictor de sobrevida. Los fumadorre s tiene mas riesgo de recibir menos tratameinto.")
20
Tabaco Cáncer de Pulmón y Sobrevida Videtic JCO 21 1544
215 ptes en LSCLC Dana Farber Retrospectivo TTO QT / RT

21
Fig 1. Actuarial overall survival according to smoking status during chemoradiotherapy (P = .0017)
Rwvisoinde 10 años uniinstitucional Videtic, G. M.M. et al. J Clin Oncol; 21:

22
Fig 3. Actuarial overall survival according to smoking status and requirement for toxicity-related treatment breaks (delay) during chemoradiotherapy (P = .0014) Videtic, G. M.M. et al. J Clin Oncol; 21:

23
Tabaco Cáncer de Pulmón y Sobrevida Fujisawas T JCO 1999 2086
NSCLC Estadios I N 375 ptes Operados entre to 1993

24
Fig 2. Overall survival curves in patients with primary, resected stage I NSCLC, evaluated by pack-years

25
Tabaco Cáncer de Pulmón y Sobrevida Fujisawas T JCO 1999 2086
Paques año fumados antes de la cirugia

26
Molecular abnormalities in lung cancer
Atypical alveolar hyperplasia Premalignant adenomas Commonly observed genetic changes Inappropriate response to external signals Loss of cell cycle control Loss of apoptosis pathway Loss of contact inhibition Ability to metastasise Angiogenesis Immortality Autocrine growth loops Tobacco carcinogen Normal epithelium Lung cancer Bronchial metaplasia Carcinoma in situ Dysplasia

27
CONCLUSIONES I Tabaquismo es un factor pronostico independiente de sobrevida en pacientes con cáncer de pulmón. Historial Tabaquico / Status Diagnostico / Habito post Tratamiento Comorbilidades / Tabaquismo Per Se

28
Tabaco y Segundos Primarios Do: Cancer 2004 101 2837
Pacientes con estadios iniciales tumores de Cabeza y Cuello enrolados trial de prevención con 13 Cis retinoico N 1190

29
Tabaco y Segundos Primarios Do: Cancer 2004 101 2837
En fumadores > dek 50 % de los STP fueron en pulmon mientora no fue asi en los no fumadores. En no fumadores el 80 % de los tobaco cancers fueron diagnosticados fueron tumores de la cavidad oral

30
Tabaco y Segundos Primarios Do: Cancer 2004 101 2837

31
Tabaco y Complicaciones Operatorias (Barrera Chest 2005 1977)
N 300 toracotomias por cáncer Prospectivo - No fumadores - EX fumadores alejados (> de 2 meses) - EX fumadores recientes (≤ de 2 meses > 1 semana) - Fumadores
 - EX fumadores recientes (≤ de 2 meses > 1 semana) - Fumadores.")
32
Tabaco y Complicaciones Operatorias (Barrera Chest 2005 1977)
")
33
Tabaco y Complicaciones Operatorias
(Barrera Chest )
")
34
Tabaco y Complicaciones Operatorias (Barrera Chest 2005 1977)
")
35
Tabaco y Complicaciones Operatorias (Varpociyan Annals Surg 2002 : 420)
Retrospectivo 261 neumonectomias Incidencia de Eventos Pulmonares Mayores - Neumonía - SDRA

36
Tabaco y Complicaciones Operatorias (Varpociyan Annals Surg 2002 : 420)
El factor predictivo más consistente TIEMPO DE CESACION DE FUMAR Las causa predominantes de muerte luego de una neumonectomia son distress respiratorio y neumonia

37
TABACO Y QoL Garces (Chest 2004 1733)
N 1019 Diagnostico de Cáncer de Pulmón LCSS (Lung Cancer Symptom Scale) Enviado x correo
 Enviado x correo.")
38
TABACO Y QoL Garces (Chest 2004 1733)
N ( % ) No Fumadores 180 ( 18 % ) Ex Fumadores 562 ( 55 % ) Ex Fumadores Recaidos 29 ( 3 % ) Fumadores Abstinentes 173 ( 17 % ) Fumadores Persistentes 75 ( 7 % )
 No Fumadores. 180 ( 18 % ) Ex Fumadores. 562 ( 55 % ) Ex Fumadores Recaidos. 29 ( 3 % ) Fumadores Abstinentes. 173 ( 17 % ) Fumadores Persistentes. 75 ( 7 % )")
39
TABACO Y QoL Garces (Chest 2004 1733)
7 de los 9 items fueron clinica y estadisticamnete significante Apetito

40
Tabaco y Radioterapia (Browman NEJM Vol 328 159)
N 115 Ca Cabeza y Cuello tratados con RT ± 5 FU. Conducta tabaquica al Baseline y luego semanalmente Fumadores No Fumadores Respuestas Completas 45 % 74 % P = 0.008

41
Tabaco y Radioterapia (Browman NEJM Vol 328 159)
OS a 2 años 66 % no fumadores Vs 39 % fumadores P= 0.005

42
Tabaco y Radioterapia (Browman NEJM Vol 328 159)
Seguir fumando junto con la RT Disminuye las Respuestas Empeora la Sobrevida

43
Tabaco y Quimioterapia (Gritz 2005) Cancer Epidemiol Biomarkers Prev Pag 2287
 Cancer Epidemiol Biomarkers Prev Pag 2287")
44
Tabaco y Quimioterapia (Gritz 2005) Cancer Epidemiol Biomarkers Prev Pag 2287
TOPICOS NO EXPLORADOS: Relación tabaco eficacia Historia tabaquica y genero Relación tabaco y Qol Estrategias de cesación luego del Diagnostico Relación entre el fumador pasivo y eficacia

45
Tabaco y quimioterapia
Efectos del tabaco y Qumioterapia: - Inhibición de la apoptosis - Estimular la angiogenesis - Incrementa carboxihemoglobina - Alteran la inmunidad celular y Natural Killer - Afecta la disponibilidad de drogas a nivel tisular - Disminuye la producción de radicales libres - Estimulo de la ciclooxigenasa 2 - Aumento del Monoxido de Carbono

46
Tabaco y quimioterapia Jongh (BJM 2003 1199)
N 400 p con Cisplatino semanal analisis de factores pronosticos Nefrotoxidad

47
Tabaco y Nuevas Moléculas

48
û û û Mode of action of EGFR inhibitors DNA ERLOTINIB GEFITINIB
EGF/TGFα R R Antibody Extracellular Membrane û û Intracellular ERLOTINIB GEFITINIB EGFR-TKI K K EGFR-TKI û Cell survival (anti-apoptosis) Proliferation Signalling EGFR is activated by the binding of a variety of ligands [eg EGF, transforming growth factor-α (TGFα)] to the extracellular domain. This results in receptor dimerisation, leading to activation of the receptor’s tyrosine kinase and subsequent intracellular signalling. EGFR activation has been implicated in the control of cell proliferation, survival and metastasis.1 There is increasing evidence that EGFR is expressed in a range of human tumours, including NSCLC, and high-level expression has been correlated in many cases with poor prognosis.2,3 Inhibitors of the EGFR in clinical development include the small molecule EGFR tyrosine kinase inhibitors gefitinib and OSI-774, and the monoclonal antibody C A lack of EGFR positivity has been observed in SCLC.7 References Woodburn J. Pharmacol Ther 1999; 82: Salomon D, et al. Crit Rev Oncol Hematol 1995; 19: Wells A. Int J Biochem Cell Biol 1999; 31: Baselga J, Averbuch S. Drugs 2000; 60 (Suppl 1): Hidalgo M, et al. J Clin Oncol 2001; 19: Baselga J, et al. J Clin Oncol 2000; 18: Cerny T, et al. Br J Cancer 1986; 54: DNA Growth factors Angiogenesis Chemotherapy/ radiotherapy sensitivity Metastasis R, epidermal growth factor receptor
 Proliferation. Signalling. EGFR is activated by the binding of a variety of ligands [eg EGF, transforming growth factor-α (TGFα)] to the extracellular domain. This results in receptor dimerisation, leading to activation of the receptor’s tyrosine kinase and subsequent intracellular signalling. EGFR activation has been implicated in the control of cell proliferation, survival and metastasis.1. There is increasing evidence that EGFR is expressed in a range of human tumours, including NSCLC, and high-level expression has been correlated in many cases with poor prognosis.2,3. Inhibitors of the EGFR in clinical development include the small molecule EGFR tyrosine kinase inhibitors gefitinib and OSI-774, and the monoclonal antibody C A lack of EGFR positivity has been observed in SCLC.7. References. Woodburn J. Pharmacol Ther 1999; 82: Salomon D, et al. Crit Rev Oncol Hematol 1995; 19: Wells A. Int J Biochem Cell Biol 1999; 31: Baselga J, Averbuch S. Drugs 2000; 60 (Suppl 1): Hidalgo M, et al. J Clin Oncol 2001; 19: Baselga J, et al. J Clin Oncol 2000; 18: Cerny T, et al. Br J Cancer 1986; 54: DNA. Growth factors. Angiogenesis. Chemotherapy/ radiotherapy sensitivity. Metastasis. R, epidermal growth factor receptor.")
49
Tabaco y Nuevas Moléculas
Estudio Pivotal ( NEJM 2005 : ) TARCEVA 150 mg / d PLACEBO R A N D O M I Z s NSCLC Pacientes Progresados 1 ó 2 líneas de QT
 TARCEVA 150 mg / d. PLACEBO. R. A. N. D. O. M. I. Z. s. NSCLC. Pacientes. Progresados. 1 ó 2 líneas de QT.")
50
BR.21: improvement in overall survival with Tarceva
1.00 0.75 0.50 0.25 42.5% improvement in median survival Tarceva Placebo (n=488) (n= 243 ) Median survival (months) 6.7 4.7 1 - year survival (%) 31 21 Survival distribution function HR=0.73, p<0.001* Tarceva Placebo Survival time (months) *HR and p value adjusted for stratification factors at randomisation and HER1/EGFR status Shepherd F, et al. N Engl J Med 2005;353:123–32
 (n= 243. ) Median survival (months) year survival (%) Survival distribution function. HR=0.73, p<0.001* Tarceva. Placebo Survival time (months) *HR and p value adjusted for stratification factors at randomisation and HER1/EGFR status. Shepherd F, et al. N Engl J Med 2005;353:123–32.")
51
Subgrupos de Riesgo Relativo erlotinib vs Placebo

52
BR.21: change in QoL domains (EORTC QLQ-C30)
Improved* (%) Stable (%) Worse (%) Variable Tarceva Placebo Global QoL† 35 26 16 28 49 46 Physical function† 31 19 18 24 51 57 Role function 39 32 14 20 47 Cognitive function 29 23 Emotional function† 30 36 37 Social function 21 44 *³10 point change from baseline at any time (clinically significant) †p0.01 Bezjak A, et al. J Clin Oncol 2006;24:3831–7
 Stable (%) Worse (%) Variable. Tarceva. Placebo. Global QoL† Physical function† Role function Cognitive function Emotional function† Social function *³10 point change from baseline at any time (clinically significant) †p0.01. Bezjak A, et al. J Clin Oncol 2006;24:3831–7.")
53
BR.21: adverse events (%) Tarceva (n=485) Placebo (n=242) Any
Grade 3, 4 Any Grade 3, 4 Rash 75 9 17 Diarrhoea 54 6 18 <1 Nausea 33 3 24 2 Stomatitis 17 <1 3 Ocular (all) 27 1 9 <1 Shepherd F, et al. N Engl J Med 2005;353:123–32
 <1. Shepherd F, et al. N Engl J Med 2005;353:123–32.")
54
Predictores de Respuesta a ITK(%)
No Fumadores 27 Fumadores 5 Mujeres 15 Hombres Adenocarcinoma 33 No Adenocarcinoma 8 Japoneses Caucásicos 11

55
El tabaquismo resultó predictivo en el BR.21

56
Tarceva Tabaco y farmacocinetica Hamilton Clin Cancer Res 2006 2166

57
Tarceva Tabaco y Farmacocinetica Hamilton Clin Cancer Res 2006 2166

58
Gefitinib y Mutaciones del receptor TaronClin Cancer Res 2005

59
Fig 2. Kaplan-Meier plots of (A) time to progression and (B) overall survival according to epidermal growth factor receptor mutational status
 time to progression and (B) overall survival according to epidermal growth factor receptor mutational status.")
60
Tabaco y Probabilidad de Mutaciones
EGFR Pham JCO

61
Tabaquismo Luego del Diagnostico de Cáncer
- Aumenta las complicaciones posoperatorias - Disminuye la efectividad del tratamiento radiante/ quimioterapia aumentando la toxicidad - Disminuye la Sobrevida - Deteriora La calidad de vida - Condiciona la Utilidad de nuevas moléculas

63
DEJAR DE FUMAR NUNCA ES DEMASIADO TARDE

64
GRACIAS

Presentaciones similares






 1.>")













