Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Balón de contrapulsación intra-aórtico (BCPI)
José Julián Arango Residente de anestesiología UdeA

2
Angina Inestable Refractaria Infarto Agudo del Miocardio (IAM)
Indicaciones shock cardiogénico Angina Inestable Refractaria Infarto Agudo del Miocardio (IAM) Falla Ventricular Refractaria Refractory Ventricular Failure In the already compromised heart, a decrease in arterial pressure can result in a reduction in myocardial oxygen supply and a loss of functional myocardial tissue. To prevent worsening failure and cardiogenic shock, any signs of hemodynamic instability must be treated promptly. Treatment is aimed at relieving left ventricular workload and restoring the balance between myocardial oxygen supply and demand, allowing the myocardium time to heal and recover maximal function. Intra-aortic balloon counterpulsation assists in this effort by decreasing left ventricular workload and increasing coronary artery perfusion. Cardiogenic Shock Left ventricular (LV) failure following an acute myocardial infarction may progress to cardiogenic shock. As with LV failure, treatment is aimed at decreasing cardiac work, increasing myocardial oxygen supply, and decreasing myocardial oxygen demands. The combined effects of IABP therapy - increased oxygen supply, decreased afterload, and improved systemic perfusion - allows the heart to rest and halt the subsequent vicious cycle that often occurs with an acute myocardial infarction. Unstable Refractory Angina Myocardial ischemia and chest pain associated with unstable angina may be effectively treated with IABP therapy. The IAB can be beneficial in maintaining adequate coronary artery perfusion, relieving myocardial ischemia, and decreasing myocardial oxygen demand. If cardiac catheterization and further interventions are indicated, the patient can undergo these procedures in a more hemodynamically stable condition.
 Falla Ventricular Refractaria. Refractory Ventricular Failure. In the already compromised heart, a decrease in arterial pressure can result in a reduction in myocardial oxygen supply and a loss of functional myocardial tissue. To prevent worsening failure and cardiogenic shock, any signs of hemodynamic instability must be treated promptly. Treatment is aimed at relieving left ventricular workload and restoring the balance between myocardial oxygen supply and demand, allowing the myocardium time to heal and recover maximal function. Intra-aortic balloon counterpulsation assists in this effort by decreasing left ventricular workload and increasing coronary artery perfusion. Cardiogenic Shock. Left ventricular (LV) failure following an acute myocardial infarction may progress to cardiogenic shock. As with LV failure, treatment is aimed at decreasing cardiac work, increasing myocardial oxygen supply, and decreasing myocardial oxygen demands. The combined effects of IABP therapy - increased oxygen supply, decreased afterload, and improved systemic perfusion - allows the heart to rest and halt the subsequent vicious cycle that often occurs with an acute myocardial infarction. Unstable Refractory Angina. Myocardial ischemia and chest pain associated with unstable angina may be effectively treated with IABP therapy. The IAB can be beneficial in maintaining adequate coronary artery perfusion, relieving myocardial ischemia, and decreasing myocardial oxygen demand. If cardiac catheterization and further interventions are indicated, the patient can undergo these procedures in a more hemodynamically stable condition.")
3
Indicaciones Complicaciones mecánicas del Infarto Agudo del Miocardio
Soporte para procedimientos percutáneos de revascularización o de diagnóstico Impending Infarction Patients experiencing severe chest pain accompanied by electrocardiogram changes and/or dysrhythmias, who do not obtain relief from drug therapy, are at great risk of developing a myocardial infarction. By improving coronary blood flow and reducing left ventricular work, chest pain and ECG changes associated with the myocardial ischemia can be minimized. If cardiac catheterization and further interventions are indicated, the patient can undergo these procedures in a more hemodynamically stable condition. Mechanical Complications due to Acute Myocardial Infarction Depending on the area of an acute myocardial infarction, mechanical complications can occur. Although these affect a small percentage of acute myocardial infarctions, the resulting hemodynamic compromise can have lethal consequences especially if not treated immediately. Ventricular septal defects, papillary muscle dysfunction or papillary muscle rupture usually require surgical intervention, often emergently. If the patient undergoes cardiac catheterization or surgical intervention in a hemodynamically compromised state, mortality and morbidity can be significantly increased. The IABP is utilized for temporary support to achieve hemodynamic stability until definitive measures are taken. Ischemia Related Intractable Ventricular Arrhythmias Ventricular irritability can be a frequent complication of acute MI, and may lead to severe dysrhythmias and further hemodynamic compromise. In most patients, conventional drug therapy and supportive measures are sufficient to reverse the irritability and dysrhythmias. However, patients refractory to conventional medical therapy are at high risk for further myocardial damage and death if this condition is not reversed. IABP therapy has proven effective in stabilizing the hemodynamic condition of these patients by increasing coronary artery perfusion, reducing ischemia and maintaining adequate peripheral perfusion.

4
INTERVENCIONES CORONARIAS PERCUTANEAS DE ALTO RIESGO
FE baja, enf. multivaso, estenosis del tronco, inestabilidad hemodinámica, comorbilidades multiples 133 pacientes uso pre PCI eventos cardíacos mayores IAM, ACV, shock, muerte, CABG urgente 17% 0% pre PCI (p 0.001) Am Heart J 2003;145:700–707.
 Am Heart J 2003;145:700–707.")
5
Indicaciones Isquemia relacionada con arritmias ventriculares intratables Shock Séptico Generacion de flujo pulsátil intraoperatorio Destete del bypass (Puente Coronario) Cardiac Support for High Risk General Surgical Patients and Coronary Angiography/Angioplasty Patients Patients with existing impaired cardiac function are considered to be high-risk candidates for general surgery. Anesthetic agents and the procedure itself can place increased myocardial oxygen demands on the already impaired heart. Use of IABP provides hemodynamic stability by assisting in balancing myocardial oxygen supply and demand, preoperatively, intraoperatively, and during the critical post operative period when the demands on the heart are particularly high. Intra-aortic balloon counterpulsation may be used in conjunction with coronary angiography and angioplasty to support and stabilize high risk patients undergoing these procedures. Overall, intra-aortic balloon counterpulsation can provide increased coronary artery perfusion, and a decrease in cardiac work, thus reducing the risk of hemodynamic compromise due to reduced coronary flow during balloon inflation or acute coronary occlusion. Septic Shock Septic shock is caused by an overwhelming infection, affecting all the organ systems, increasing metabolic demands. It is characterized by low blood pressure, impaired neurologic function, decreased cardiac output, and high fever and can lead to cardiogenic shock. For patients unresponsive to maximal supportive therapy, intra-aortic balloon counterpulsation can increase coronary blood flow, reduce left ventricular work load by lowering systolic pressure, and improve tissue perfusion by maintaining adequate mean arterial pressure. Weaning from Cardiopulmonary Bypass Weaning a patient from cardiopulmonary bypass may be difficult in those cases in which aortic cross-clamping is prolonged, surgical revascularization is partially achieved, or pre-existing myocardial dysfunction is present. Termination of cardiopulmonary bypass may be marked by hypotension (low blood pressure) and a low cardiac index, despite administration of vasoactive drugs. The use of IABP in this setting decreases left ventricular resistance, increases cardiac output, and increases coronary artery and systemic perfusion pressures, facilitating the patient’s removal from cardiopulmonary bypass. Asistencia cardiaca a alto riesgo general del paciente quirúrgico, y la angiografía coronaria / pacientes con angioplastia Los pacientes con insuficiencia cardíaca existentes se consideran candidatos de alto riesgo para la cirugía general. Los agentes anestésicos y el procedimiento en sí puede colocar aumento de la demanda de oxígeno del miocardio en el corazón ya deteriorado. El uso de BCIA proporciona la estabilidad hemodinámica, ayudando a equilibrar la oferta y la demanda miocárdica de oxígeno, antes de la intervención, durante la operación, y durante el post operatorio crítico cuando las exigencias sobre el corazón son particularmente altas. Balón de contrapulsación aórtica puede ser usado en conjunción con la angiografía coronaria y la angioplastia para apoyar y estabilizar los pacientes de alto riesgo se someten a estos procedimientos. En general,-dentro de balón de contrapulsación aórtica puede proporcionar aumento de la perfusión coronaria, y una disminución en el trabajo cardíaco, reduciendo así el riesgo de compromiso hemodinámico debido a la reducción del flujo coronario durante el inflado del balón o la oclusión coronaria aguda. Shock séptico El shock séptico es causado por una infección masiva, que afecta a todos los órganos y sistemas, el aumento de las demandas metabólicas. Se caracteriza por presión arterial baja, deterioro de la función neurológica, disminución del gasto cardíaco, y fiebre alta y puede llevar a un shock cardiogénico. Para los pacientes que no responden a la terapia de apoyo máximo, dentro de balón de contrapulsación aórtica puede aumentar el flujo sanguíneo coronario, reducir la carga de trabajo del ventrículo izquierdo por reducción de la presión sistólica, y mejorar la perfusión tisular adecuada, manteniendo la presión arterial media. El destete de bypass cardiopulmonar El destete de un paciente de derivación cardiopulmonar puede ser difícil en aquellos casos en que el pinzamiento aórtico, se prolonga, la revascularización quirúrgica se logró parcialmente, o pre-existentes disfunción miocárdica está presente. La terminación de la circulación extracorpórea puede estar marcada por la hipotensión (presión arterial baja) y un índice cardíaco bajo, a pesar de la administración de drogas vasoactivas. El uso de BCIA en esta situación disminuye la resistencia del ventrículo izquierdo, aumenta el gasto cardíaco, y el aumento de la arteria coronaria y la presión de perfusión sistémica, facilitar la extracción del paciente de derivación cardiopulmonar.
 Cardiac Support for High Risk General Surgical Patients and Coronary Angiography/Angioplasty Patients. Patients with existing impaired cardiac function are considered to be high-risk candidates for general surgery. Anesthetic agents and the procedure itself can place increased myocardial oxygen demands on the already impaired heart. Use of IABP provides hemodynamic stability by assisting in balancing myocardial oxygen supply and demand, preoperatively, intraoperatively, and during the critical post operative period when the demands on the heart are particularly high. Intra-aortic balloon counterpulsation may be used in conjunction with coronary angiography and angioplasty to support and stabilize high risk patients undergoing these procedures. Overall, intra-aortic balloon counterpulsation can provide increased coronary artery perfusion, and a decrease in cardiac work, thus reducing the risk of hemodynamic compromise due to reduced coronary flow during balloon inflation or acute coronary occlusion. Septic Shock. Septic shock is caused by an overwhelming infection, affecting all the organ systems, increasing metabolic demands. It is characterized by low blood pressure, impaired neurologic function, decreased cardiac output, and high fever and can lead to cardiogenic shock. For patients unresponsive to maximal supportive therapy, intra-aortic balloon counterpulsation can increase coronary blood flow, reduce left ventricular work load by lowering systolic pressure, and improve tissue perfusion by maintaining adequate mean arterial pressure. Weaning from Cardiopulmonary Bypass. Weaning a patient from cardiopulmonary bypass may be difficult in those cases in which aortic cross-clamping is prolonged, surgical revascularization is partially achieved, or pre-existing myocardial dysfunction is present. Termination of cardiopulmonary bypass may be marked by hypotension (low blood pressure) and a low cardiac index, despite administration of vasoactive drugs. The use of IABP in this setting decreases left ventricular resistance, increases cardiac output, and increases coronary artery and systemic perfusion pressures, facilitating the patient’s removal from cardiopulmonary bypass. Asistencia cardiaca a alto riesgo general del paciente quirúrgico, y la angiografía coronaria / pacientes con angioplastia Los pacientes con insuficiencia cardíaca existentes se consideran candidatos de alto riesgo para la cirugía general. Los agentes anestésicos y el procedimiento en sí puede colocar aumento de la demanda de oxígeno del miocardio en el corazón ya deteriorado. El uso de BCIA proporciona la estabilidad hemodinámica, ayudando a equilibrar la oferta y la demanda miocárdica de oxígeno, antes de la intervención, durante la operación, y durante el post operatorio crítico cuando las exigencias sobre el corazón son particularmente altas. Balón de contrapulsación aórtica puede ser usado en conjunción con la angiografía coronaria y la angioplastia para apoyar y estabilizar los pacientes de alto riesgo se someten a estos procedimientos. En general,-dentro de balón de contrapulsación aórtica puede proporcionar aumento de la perfusión coronaria, y una disminución en el trabajo cardíaco, reduciendo así el riesgo de compromiso hemodinámico debido a la reducción del flujo coronario durante el inflado del balón o la oclusión coronaria aguda. Shock séptico El shock séptico es causado por una infección masiva, que afecta a todos los órganos y sistemas, el aumento de las demandas metabólicas. Se caracteriza por presión arterial baja, deterioro de la función neurológica, disminución del gasto cardíaco, y fiebre alta y puede llevar a un shock cardiogénico. Para los pacientes que no responden a la terapia de apoyo máximo, dentro de balón de contrapulsación aórtica puede aumentar el flujo sanguíneo coronario, reducir la carga de trabajo del ventrículo izquierdo por reducción de la presión sistólica, y mejorar la perfusión tisular adecuada, manteniendo la presión arterial media. El destete de bypass cardiopulmonar El destete de un paciente de derivación cardiopulmonar puede ser difícil en aquellos casos en que el pinzamiento aórtico, se prolonga, la revascularización quirúrgica se logró parcialmente, o pre-existentes disfunción miocárdica está presente. La terminación de la circulación extracorpórea puede estar marcada por la hipotensión (presión arterial baja) y un índice cardíaco bajo, a pesar de la administración de drogas vasoactivas. El uso de BCIA en esta situación disminuye la resistencia del ventrículo izquierdo, aumenta el gasto cardíaco, y el aumento de la arteria coronaria y la presión de perfusión sistémica, facilitar la extracción del paciente de derivación cardiopulmonar.")
6
Indicaciones Soporte cardíaco en cirugias no cardíacas
Uso preventivo en preparacion para la Cirugía Cardíaca Angioplastia fallida Disfunción miocárdica POP Support for Failed Angioplasty and Valvuloplasty Intra-aortic balloon counterpulsation may be used to support and stabilize patients with severe left ventricular failure due to failed angioplasty. Overall, the IAB may provide increased coronary artery perfusion, and decrease cardiac work, thus reducing the risk of hemodynamic compromise due to reduced coronary flow or acute coronary occlusion. Unsuccessful valvuloplasty may result in cardiac dysfunction. The IABP may be used to support cardiac function in these patients until valve repair or replacement can be performed. Intraoperative Pulsatile Flow Generation In the past, the IABP has been used in conjunction with cardio-pulmonary bypass to generate pulsatile flow. Currently, the IABP is often used intraoperatively, but the primary objectives are not only pulsatile flow generation, but improving coronary artery perfusion, decreasing cardiac work (afterload) and reestablishing a balance between myocardial oxygen supply and myocardial oxygen demands.
 and reestablishing a balance between myocardial oxygen supply and myocardial oxygen demands.")
7
Terapia de contrapulsación
El Contra pulsador es un dispositivo de asistencia cardíaca temporal La disponibilidad de este dispositivo mecánico de asistencia permite al paciente sobrevivir crisis agudas hasta que el tratamiento definitivo se realice

8
Introducido a la práctica clínica al final de la década del 60
El Balón/Catéter Intra Aórtico (BIA) se coloca en la aorta torácica descendente, con la punta distal a la arteria subclavia izquierda El Balón se sincroniza para inflar y desinflar en sincronía con el ciclo cardíaco para aumentar la provisión de oxígeno y reducir la demanda de oxígeno por el miocárdico El sistema intra-aórtica con balón consiste en un globo en la punta del catéter que se conecta a una consola que controla el tiempo y el volumen de la inflación y desinflación del globo durante el ciclo cardíaco
 se coloca en la aorta torácica descendente, con la punta distal a la arteria subclavia izquierda. El Balón se sincroniza para inflar y desinflar en sincronía con el ciclo cardíaco para aumentar la provisión de oxígeno y reducir la demanda de oxígeno por el miocárdico. El sistema intra-aórtica con balón consiste en un globo en la punta del catéter que se conecta a una consola que controla el tiempo y el volumen de la inflación y desinflación del globo durante el ciclo cardíaco.")
9
Descripción Se trata de un balón de latex con una capacidad de cc Comandado por una consola que lo infla y desinfla sincrónicamente con el ciclo cardíaco. consola que controla el tiempo y el volumen de la inflación y desinflación del globo durante el ciclo cardíaco

10
Equipo

11
balón en la Aorta descendente, se infla después del cierre valvular aórtico, permanece inflado durante la diástole y se colapsa antes del comienzo de la sístole Desinflado telediastólico La consola controla tiempo y volumen de inflado y desinflado del globo durante el ciclo cardíaco.

12
presión positiva durante la diástole
mejorar la circulación coronaria desinflado rápido del globo para retirar ese volumen durante la sístole ↓resistencia a la eyección sistólica fue P.413 concebido por Clauss en 1961 (1,2) y aplicar clínicamente por Kantrowitz en 1968 (3). Al principio, la práctica se limita a pacientes con shock cardiogénico (1,2), pero pronto fue seguido por el uso con éxito en pacientes con angina inestable refractaria médica (4). La inserción de un catéter con balón fue inicialmente realizada quirúrgicamente (los catéteres primera IAB mide 12 a 14 franceses de diámetro), pero la mayoría de las inserciones se realizan hoy por vía percutánea, gracias a un diámetro más pequeño (8 a 9 francés) over-the-wire catéteres (5, 6). La popularidad de BCIA se deriva de su facilidad de uso, la seguridad y la percepción de la eficacia clínica
 y aplicar clínicamente por Kantrowitz en 1968 (3). Al principio, la práctica se limita a pacientes con shock cardiogénico (1,2), pero pronto fue seguido por el uso con éxito en pacientes con angina inestable refractaria médica (4). La inserción de un catéter con balón fue inicialmente realizada quirúrgicamente (los catéteres primera IAB mide 12 a 14 franceses de diámetro), pero la mayoría de las inserciones se realizan hoy por vía percutánea, gracias a un diámetro más pequeño (8 a 9 francés) over-the-wire catéteres (5, 6). La popularidad de BCIA se deriva de su facilidad de uso, la seguridad y la percepción de la eficacia clínica.")
13
FALLA DEL VENTRICULO IZQUIERDO
Demanda Consumo de O2 por el miocardio If there is injury to the myocardium, a series of physiologic changes occur which will result in an imbalance between myocardial oxygen supply and demand. Oferta

14
Pérdida del Miocardio Ventricular
Falla del Ventrículo Izquierdo - Ciclo de eventos Cirugía Cardíaca Infarto del miocardio Trauma Cardíaco Pérdida del Miocardio Ventricular viable y contráctil Aumento Isquemia Miocárdica Aumento Isquemia Miocárdica Disminución Función Ventr. Izq. Disminución Provisión de Oxígeno Aumento Demanda de Oxígeno With cardiac failure, cardiac output falls which will reduce myocardial oxygen supply. In an attempt to compensate, preload, afterload, and heart rate increase. This will result in an increase in myocardial oxygen demands. As the failure progresses, a cycle develops whereby a greater imbalance between myocardial oxygen supply and demand results in a further failure of the pumping action of the heart. Myocardial oxygen supply will continue to decrease and myocardial oxygen demands will continue to rise. Disminución Perfusión Coronaria Aumento Frec. Cardíaca ↓ Gasto cardiaco Disminución Presión sanguínea Aumento poscarga y Resist. Vascular Sistémica

15
Consumo de O2 por el miocardio
OBJETIVO DE LA TERAPIA = Oferta Demanda Consumo de O2 por el miocardio

16
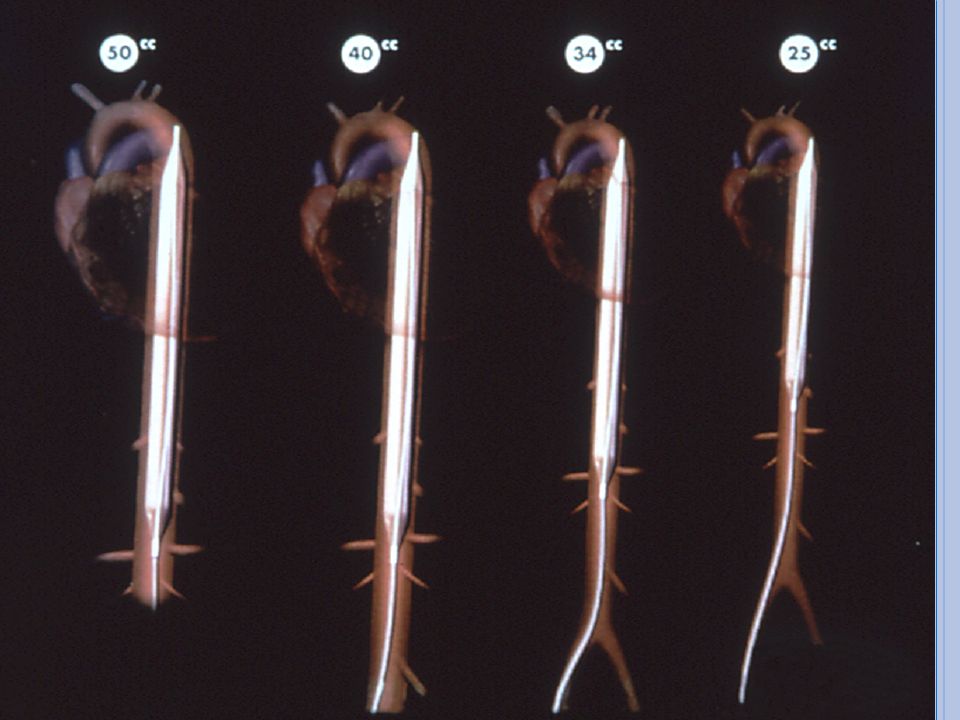
catéter/balón intra-aórtico
10 cm de longitud volumen de inflado 30 a 50 ml aorta torácica descendente a 1 a 2 cm del origen de la arteria subclavia izquierda. balón se infla con helio inmediatamente después del cierre de la válvula aórtica ↑ P diastólica aórtica. El inflado se mantiene hasta el comienzo de la sistóle apertura de la válvula aórtica desinflado produce una fuerte caída en la P sistólica aórtica con una ↓ postcarga. Se usa helio gas de bajo peso molecular que permite mas rapido inflado y desinflado

17
Sístole: Desinflado del BIA
• Disminuye el trabajo cardíaco Disminuye el consumo de oxígeno por el miocardio mejora el gasto cardíaco

18
Efectos primarios de la Contrapulsación
Desinflado telediastólico Disminuye postcarga Desinflado del BIA Oferta Demanda Consumo de O2 por el miocardio Inflado del BIA Inflación diastólica Mejora perfusión

19
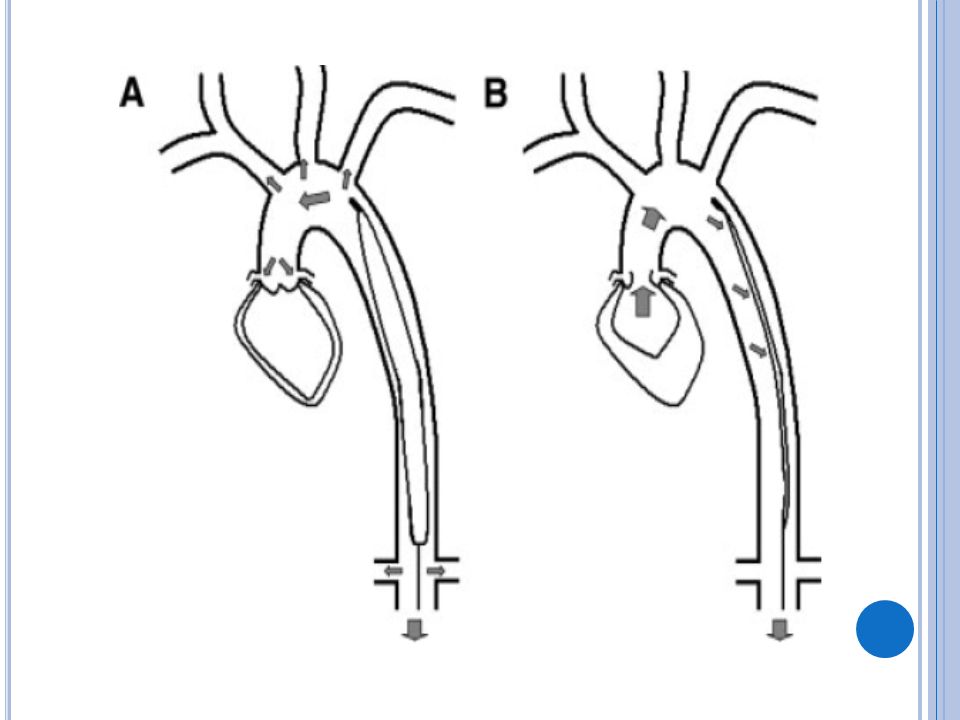
El balón inflado crea un flujo retrógrado resultando en:
PA diastólica en el arco aórtico perfusión coronaria perfusión sistémica oferta de O2

20
REDUCCION DE LA POST CARGA
El flujo de la sangre con el balón desinflado resultando en: el volumen y presión del arco volumen sistólico levemente la PAS el tiempo de la eyección sistólica perfusión coronaria

21
Mejora gasto cardiaco 20-40%
Cuando el balón se infla , aumenta la presión diastólica y esto contribuye a mejorar el flujo sanguíneo coronario cerebral y sistémico. El desinflado pre-sistólico disminuye la resistencia a la eyección sistólica del ventrículo izquierdo ( ↓ postcarga ) con lo que el trabajo miocárdico y la demanda de oxígeno del mismo se ↓ Mejora gasto cardiaco 20-40% Esta rápida disminución en el volumen aórtico hace que la presión aórtica caiga justo antes del inicio de la eyección del ventrículo izquierdo, o sea que éste al expeler la sangre lo hará contra una carga o presión menor, con lo que su trabajo disminuye Tan pronto como la válvula aórtica se cierra, el volumen que se había retirado durante la sístole por desinflado del balón, se repone por inflado en la diástole. Este volumen aórtico ahora expandido en 30 o 40 cc, aumenta la presión aórtica y por lo tanto mejorará el flujo y la perfusión coronaria Básicamente al desinflar el balón dentro de la aorta se produce un efecto similar al vacío reduciendo la resistencia vascular y mejorando la propulsión de la sangre a través de la aorta. Es como si se produjera un espacio virtual en el lugar que ocupa el balón dentro de la aorta generando casi una presión negativa en ese sector
 con lo que el trabajo miocárdico y la demanda de oxígeno del mismo se ↓ Mejora gasto cardiaco 20-40% Esta rápida disminución en el volumen aórtico hace que la presión aórtica caiga justo antes del inicio de la eyección del ventrículo izquierdo, o sea que éste al expeler la sangre lo hará contra una carga o presión menor, con lo que su trabajo disminuye. Tan pronto como la válvula aórtica se cierra, el volumen que se había retirado durante la sístole por desinflado del balón, se repone por inflado en la diástole. Este volumen aórtico ahora expandido en 30 o 40 cc, aumenta la presión aórtica y por lo tanto mejorará el flujo y la perfusión coronaria. Básicamente al desinflar el balón dentro de la aorta se produce un efecto similar al vacío reduciendo la resistencia vascular y mejorando la propulsión de la sangre a través de la aorta. Es como si se produjera un espacio virtual en el lugar que ocupa el balón dentro de la aorta generando casi una presión negativa en ese sector.")
22
Efectos Hemodinámicos
Poscarga Disminuye Gasto cardiaco Aumenta Frecuencia Presiones centrales Tensión pared

23
El uso de la Contrapulsación
Selección del Balón/Catéter Tamaño del Catéter Volumen del Balón Métodos de inserción percutánea Sin vaina Con vaina Vaina de inserción Aunque la inserción a través de una vaina es muy fácil, la mayoría de los globos actuales tienen una nariz afilada para permitir que se inserta directamente sobre un alambre guía (es decir, sin el uso de una vaina). Debido a que el eje del globo es de aproximadamente 1.5F (0,5 mm) más pequeño que el diámetro exterior de la vaina correspondiente, los resultados de inserción sin vaina < trauma arterial femoral y menos obstrucción a la circulación de las extremidades en pacientes con arterias pequeñas o aterosclerosis
. Debido a que el eje del globo es de aproximadamente 1.5F (0,5 mm) más pequeño que el diámetro exterior de la vaina correspondiente, los resultados de inserción sin vaina < trauma arterial femoral y menos obstrucción a la circulación de las extremidades en pacientes con arterias pequeñas o aterosclerosis.")
25
TECNICA DE INSERCION Vía arteria femoral - técnica percutánea
Vía aorta torácica – quirúrgica arteria femoral 8F es el tamaño mas usado Parámetros de coagulación evaluación clínica vascular periférica

26
Colocación del BIA: Idealmente se debe usar fluoroscopio
La punta del BIA debe estar 1 o 2 cms. distal a la arteria subclavia izquierda Si no hay fluoroscopio mida : colocando la punta del BIA en el ángulo de Louis hasta el obligo y oblicuamente de allí al punto de inserción femoral. Marque el catéter y al colocar el BIA aváncelo hasta esa marca. Rayos X verificar la correcta colocación del BIA Presión Arterial

28
La punta del BIA debe posicionarse entre el segundo y tercer espacio intercostal
Correcta Incorrecta

29
• Puesta en marcha • Ayuda en pantalla • Transportable Automático:
El Contrapulsador Fácil de usar: • Puesta en marcha • Ayuda en pantalla • Transportable Automático: • Sincronización • Llenado del Balón The pump uses a safety disk patient isolation system. Vacuum and pressure are alternately applied to shuttle helium into and out of the IAB catheter. Ease of use: Start up: Automica puesta en marcha permite la iniciación rápida de la terapia. Help Screen: One button access to help screen for initial step-by-step set up guide and probable cause & corrective action for alarms and alerts. User Preferences: Allows for customization of display and audio features without interrupting pumping. Transportable: 4 + horas de tiempo de batería Automated: Timing: CardiosyncTM software accurately anticipates balloon timing by actually classifying specific cardiac beat patterns. The system analyzes the emerging rhythm, rapidly adapts to arrhythmias and ectopic beats, and controls timing in a manner which maximizes trigger reliability and augmentation Helium fill procedure:The system automatically purges and refills the balloon catheter circuit with helium every two hours to maintain optimal helium concentration and balloon inflation [when augmentation set at maximum] Condensate removal: During balloon pumping condensed water vapor may be observed in the catheter extension tubing. The condensate removal module will automatically collect and remove the condensate without operator intervention or interruption of pumping.

30
E.K.G : insufla en la cúspide onda T desinfla al comienzo Q.R.S El desinflado se desencadena en relación con la onda R del ECG de superficie. P.A : insufla en la incisura dicrota desinfla antes del comienzo de la sístole arterial

31
Aumento de la Perfusión
Evaluación de la sincronización Aumento de la Perfusión a la arteria coronaria mm Hg C D A B E F 120 100 80 Inflation and deflation of the IAB change the configuration of the arterial pressure waveform. A properly timed balloon will inflate at the dicrotic notch, which will appear as a sharp “V” configuration between the systolic pressure and the diastolic augmentation. The peak diastolic augmentation represents the maximum pressure in the aorta with balloon inflation during diastole. Deflation of the balloon at the end of diastole is reflected in an assisted aortic end-diastolic pressure lower than the unassisted aortic end-diastolic pressure. Proper deflation will also reduce the systolic pressure that follows balloon deflation. The next systolic beat is called the assisted systole. A = Un ciclo cardíaco completo B = Presión diastólica final sin asistencia C = Presión sistólica sin asistencia D = Aumento diastólico E = Presión diastólica aórtica final reducida F = Presión sistólica reducida

32
Sincronización Convencional (Predictiva)
The QRS is used to signify the beginning of the cardiac cycle and the onset of inflation during diastole. Deflation of the balloon is timed to occur most usually prior to the PEP or the beginning of systole If the R wave is premature, the balloon automatically deflates - similar to R wave deflation timing La sincronización convencional se basa en la duración del inflado durante la diástole

33
Sincronización - Desinflado en la Onda R
The QRS is used to trigger and immediately deflate the IAB during early systole or the pre-ejection period [PEP]. R wave deflation timing is based on the constancy of the systolic time interval. The systolic time interval consists of the pre-ejection period and the ejection time. Due to the variability of diastolic time intervals with frequent ectopy or in Atrial Fibrillation, the Clinician may find that R-wave deflation works the best. La sincronización con desinflado en la onda R está basada en el desinflado durante la sístole

34
Aumento diastólico sub-óptimo
120 mm Hg 100 80 Sístole Diástole

35
Factores que afectan el Aumento Diastólico
BIA dentro de la vaina Apertura inadecuada Posición del BIA Acodamiento del BIA Fuga/rotura del BIA Baja concentración del Helio IAB in sheath: If the balloon membrane has not entirely existed the introducer sheath, it will not inflate and deflate properly. [refer to instructions for use on guidelines for sheath placement]. IAB not unfolded: If after a few cycles of counterpulsation, it appears that the balloon membrane is not fully open, perform a manual inflation of the balloon [refer to instructions for use for manual inflation]. IAB position: Clinical experience has demonstrated that that optimal balloon placement is to position the IAB tip 1 to 2 cms distal to the left subclavian artery. A catheter that is placed too low may be unable to inflate fully due to the narrowing of the abdominal aorta. Conversely, a catheter placed too high may cause the balloon and catheter to bend around the arch or encourage catheter restraint. Either circumstance may prevent optimal balloon inflation and affect diastolic augmentation. Kink in IAB catheter: Any kink in the catheter or catheter extender tubing may obstruct the flow of gas through the system, thus influencing diastolic augmentation. IAB leak: A sudden change in the diastolic augmentation pressure may also indicate the presence of blood in the balloon membrane or tubing. This will affect gas shuttling and ultimately diastolic augmentation. Low Helium concentration: It is normal for small molecules of Helium to diffuse across the balloon membrane over time. With patients that are tachycardic and/or hyperthermic the rate of Helium diffusion will increase, resulting in a reduction in augmented diastolic pressure.

36
Factores que afectan el Aumento Diastólico
IABP Sincronización Posición del control de Aumento Diastólico Timing: Proper timing is essential to ensure displacement of the available stroke volume is maximized and optimal diastolic augmentation is achieved. Late Inflation and/or Early Deflation are incorrect timing and will result in sub optimal augmentation. Position of IAB augmentation control: For optimal augmentation the IAB augmentation control should be set a maximum. If set below maximum the balloon will not inflate to it’s full volume and diastolic augmentation pressure will be affected.

37
Sincronización Sincronización Optima

38
Errores de Sincronización
Inflado prematuro Características del Trazado: - ↑ Diastólico se mezcla con la Sístole Efectos Fisiológicos: - Posibilidad de cierre prematuro V Aórtica - ↑ potencial del volumen y P final del ventrículo - ↑ postcarga - Regurgitación Aórtica - ↑ de la demanda de Oxígeno por el miocardio Waveform Characteristics: • Inflation of IAB prior to dicrotic notch • Diastolic augmentation encroaches onto systole [may be unable to distinguish] Physiologic Effects: • Potential premature closure of the aortic valve • Potential increase in LVEDV and LVEDP or PCWP • Increased left ventricular wall stress or afterload • Aortic regurgitation • Increased MVO2 demand

39
Errores de Sincronizacióon
Características del Trazado - Inflado del Balón después del nudo dicrótico - Aumento diastólico pobre Efectos Fisiológicos - Poca perfusión coronaria adicional Waveform Characteristics: • Inflation of the IAB after the dicrotic notch • Absence of a sharp V • Sub-optimal diastolic augmentation Physiologic Effects: • Sub-optimal coronary artery perfusion Inflado tardío

40
Desinflado prematuro Errores de Sincronización
Características del trazado: - El desinflado se ve como una caída súbita después del aumento diastólico - Un aumento diastólico pobre Efectos fisiológicos: - Poca perfusión coronaria extra - - La reducción de la postcarga no es óptima - Aumento en la demanda de O2 Waveform Characteristics: • Deflation of IAB is seen as a sharp drop following diastolic augmentation • Sub-optimal diastolic augmentation • Assisted aortic end-diastolic pressure may be equal to or less than the unassisted aortic end-diastolic pressure • Assisted systolic pressure may rise Physiologic Effects: • Sub-optimal coronary perfusion • Potential for retrograde coronary and carotid blood flow • Angina may occur as a result of retrograde coronary blood flow • Sub-optimal afterload reduction • Increased MVO2 demand Desinflado prematuro

41
Errores de Sincronización
Trazado: - La sístole asistida es lenta El aumento diastólico es más ancho Efectos Fisiológicos: - Mínima ↓ de la postcarga ↑ del consumo de oxígeno ventrículo eyecta contra una resistencia > El balón puede impedir la eyección ventricular Waveform Characteristics: • Assisted aortic end-diastolic pressure may be equal to the unassisted aortic end-diastolic pressure • Rate of rise of assisted systole is prolonged • Diastolic augmentation may appear widened Physiologic Effects: • Afterload reduction is essentially absent • Increased MVO2 consumption due to the left ventricle ejecting against a greater resistance and a prolonged isovolumetric contraction phase • IAB may impede left ventricular ejection and increase the afterload Desinflado tardío

42
Contraindicaciones Insuficiencia Aórtica Severa
Aneurisma abdominal o aórtico Severas calcificaciones en la aorta-iliacas o severa enfermedad periférica vascular Inserción sin vaina en pacientes severamente obesos o con cicatrices en las ingles Contraindications Severe Aortic Insufficiency Intra-aortic balloon counterpulsation is contraindicated in patients with severe aortic valve insufficiency. If an intra-aortic balloon was used, as the balloon inflated, blood in the aorta could be forced across the valve into the ventricle. Aortic regurgitation could possibly overloading the ventricle with additional blood volume and increase cardiac work. Abdominal or Aortic Aneurysm If the patient has an abdominal or thoracic aortic aneurysm, the use of an intra-aortic balloon is contraindicated since the increased pressure generated with counterpulsation can worsen the aneurysm. Severe Calcific Aorta-Iliac Disease or Peripheral Vascular Disease Severe arterial calcific disease or peripheral vascular disease is a contraindication for IABP therapy although it is viewed by some as a relative contraindication. If the benefits of IABP therapy outweigh the risk of further compromised arterial blood flow, the clinician must decide if the use of the IABP is appropriate. Peripheral vascular disease may limit the physicians ability to advance the catheter through the atherosclerotic vessel. Sheathless Insertion with Severe Obesity, Scarring of the Groin Sheathless insertion is not recommended if the patient has a lot of fatty tissue, scar tissue at the site of the common femoral artery, or other contraindications to percutaneous insertion.

43
Posibles efectos colaterales y complicaciones
Isquemia en las extremidades Sangrado en el punto de inserción Trombocitopenia Trombosis Inmobilidad del Balón Catéter Fuga/Rotura del BIA Infección Disección Aórtica Sindrome compartimental Reduccion del flujo capilar Prevention: Limb Ischemia: • Use smallest catheter/sheath sizes indicated. • Risk factors: female,diabetics,peripheral vascular disease • Select limb with best pulse Excessive bleeding from insertion site: • Careful insertion technique • Monitor anticoagulation therapy • Prevent catheter movement at insertion site Thrombocytopenia: • Avoid excessive heparin Thrombosis: • May occur during counterpulsation. The symptoms associated with thrombosis formation and treatment will depend on the organ system involved. Immobility of balloon catheter: • Maintain adequate trigger • Observe movement of IAB status indicator • If unable to inflate the IAB with the IABP, inflate and deflate the IAB by hand, using a syringe and stopcock once every 3-5 min. Balloon leak: • Do not remove the IAB from its tray until it is ready to be inserted • Ensure proper balloon size used to patient size • Ensure proper balloon placement Infection: • Sterile technique during insertion and dressing changes as per infection control policy Aortic dissection: • Insertion of IAB over guidewire with fluoroscopic control Compartment syndrome: [may develop after balloon removal] • Use the smallest catheter/sheath size indicated • Maintain adequate colloid osmotic pressure

Presentaciones similares