Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Hospital Universitario Virgen de la Victoria Málaga.
UPDATE EN CARDIOLOGIA Lo mejor de 2012 en Lípidos y Prevención Cardiovascular. Dr. JJ Gómez Doblas Hospital Universitario Virgen de la Victoria Málaga.

2
Dislipidemia. Inhibicion CETP
Cholesteryl ester transfer protein (CETP) is a plasma protein that catalyzes the transfer of CE from HDL to apoB-containing lipoproteins (VLDL and LDL-C) in exchange for Trig. LDL / VLDL LDL-R CE SR-B1 Liver X inhibition CETP FC Cholesteryl ester transfer protein (CETP) is a plasma protein that catalyzes the transfer of CE from HDL to apoB-containing lipoproteins (VLDL and LDL-C)in exchange for triglycerides that are transferred in the reverse direction. CETP inhibitors increase HDL-C and some also lower LDL-C, and therefore have the potential to reduce coronary events. HDL picks up free cholesterol (FC) from extrahepatic tissues. HDL FC is subsequently esterified by LCAT to form cholesteryl esters (CE) The HDL CE may then be delivered to the liver by either of two pathways: 1. A direct pathway following binding of HDL to hepatic SR-B1 2. An indirect pathway involving the CETP-mediated transfer of CE from HDL to VLDL and LDL with subsequent delivery to the liver following binding of LDL to the LDL receptor." After click: Inhibition of CETP prevents the transfer of CE from HDL to the VLDL/LDL fractions and results in an increase in concentration of HDL-C and a decrease in the cholesterol content of the VLDL/LDL. CE HDL LCAT Bile Free Cholesterol (FC) in Extrahepatic tissues FC 2
 is a plasma protein that catalyzes the transfer of CE from HDL to apoB-containing lipoproteins (VLDL and LDL-C) in exchange for Trig. LDL / VLDL. LDL-R. CE. SR-B1. Liver. X inhibition. CETP. FC. Cholesteryl ester transfer protein (CETP) is a plasma protein that catalyzes the transfer of CE from HDL to apoB-containing lipoproteins (VLDL and LDL-C)in exchange for triglycerides that are transferred in the reverse direction. CETP inhibitors increase HDL-C and some also lower LDL-C, and therefore have the potential to reduce coronary events. HDL picks up free cholesterol (FC) from extrahepatic tissues. HDL FC is subsequently esterified by LCAT to form cholesteryl esters (CE) The HDL CE may then be delivered to the liver by either of two pathways: 1. A direct pathway following binding of HDL to hepatic SR-B1. 2. An indirect pathway involving the CETP-mediated transfer of CE from HDL to VLDL and LDL with subsequent delivery to the liver following binding of LDL to the LDL receptor. After click: Inhibition of CETP prevents the transfer of CE from HDL to the VLDL/LDL fractions and results in an increase in concentration of HDL-C and a decrease in the cholesterol content of the VLDL/LDL. CE. HDL. LCAT. Bile. Free Cholesterol (FC) in Extrahepatic tissues. FC. 2.")
3
dal-VESSEL y dal-plaque
Characteristic Torcetrapib Anacetrapib Dalcetrapib Evacetrapib Clinical evidence of increased BP Yes1 No2 No3 No7 Preclinical evidence of increased aldosterone production* Yes3 No4 No8 Preclinical evidence of aldosterone synthase (CYP11B2) mRNA induction* ? Preclinical evidence of RAAS-associated gene induction* Yes5 No5 L-type Ca2+ channel activation* Yes6 No6 High-density lipoproteins (HDLs) participate in the process of cellular cholesterol efflux and may have additional protective effects against atherothrombosis.1 An inverse association between levels of HDL cholesterol and incident events of coronary heart disease has been shown in observational studies2,3 and persists in most post hoc analyses and meta-analyses of trials of statin therapy for patients with cardiovascular risk factors, chronic cardiovascular disease, or recent acute coronary syndrome.4-10 However, it remains uncertain whether pharmacologic intervention that raises HDL cholesterol levels results in decreased cardiovascular risk Moreover, changes in HDL cholesterol levels may not reflect changes in the physiologic functions of HDLs. Cholesteryl ester transfer protein (CETP) mediates the transfer of cholesteryl ester from HDLs to atherogenic lipoprotein particles containing apolipoprotein B, such as low-density lipoprotein (LDL). In most,18-20 but not all,21 analyses, genetic polymorphisms resulting in a lower mass or activity of CETP are associated with higher HDL cholesterol levels, lower LDL cholesterol levels, and a lower risk of coronary heart disease. These observations have led to the development of CETP inhibitors as drugs that might reduce cardiovascular risk. Torcetrapib, the first CETP inhibitor to be evaluated in a phase 3 clinical trial,22 increased HDL cholesterol levels by more than 70% and decreased LDL cholesterol levels by 25% but caused excess morbidity and mortality associated with elevation of aldosterone levels and blood pressure. Dalcetrapib is a CETP inhibitor that raised HDL cholesterol levels by approximately 30% in phase 2 studies, without significant effects on LDL cholesterol levels, blood pressure, or circulating neurohormones. 23,24 We designed a phase 3 trial, the dal-OUTCOMES study, to evaluate the effects of dalcetrapib on cardiovascular risk among patients with a recent acute coronary syndrome.
 mRNA induction* Preclinical evidence of RAAS-associated gene induction* Yes5. No5. L-type Ca2+ channel activation* Yes6. No6. High-density lipoproteins (HDLs) participate in the process of cellular cholesterol efflux and may have additional protective effects against atherothrombosis.1 An inverse association between levels of HDL cholesterol and incident events of coronary heart disease has been shown in observational studies2,3 and persists in most post hoc analyses and meta-analyses of trials of statin therapy for patients with cardiovascular risk factors, chronic cardiovascular disease, or recent acute coronary syndrome.4-10 However, it remains uncertain whether pharmacologic intervention that raises HDL cholesterol levels results in decreased cardiovascular risk Moreover, changes in HDL cholesterol levels may not reflect changes in the physiologic functions of HDLs. Cholesteryl ester transfer protein (CETP) mediates the transfer of cholesteryl ester from HDLs to atherogenic lipoprotein particles containing apolipoprotein B, such as low-density lipoprotein (LDL). In most,18-20 but not all,21 analyses, genetic polymorphisms resulting in a lower mass or activity of CETP are associated with higher HDL cholesterol levels, lower LDL cholesterol levels, and a lower risk of coronary heart disease. These observations have led to the development of CETP inhibitors as drugs that might reduce cardiovascular risk. Torcetrapib, the first CETP inhibitor to be evaluated in a phase 3 clinical trial,22 increased HDL cholesterol levels by more than 70% and decreased LDL cholesterol levels by 25% but caused excess morbidity and mortality associated with elevation of aldosterone levels and blood pressure. Dalcetrapib is a CETP inhibitor that raised HDL cholesterol levels by approximately 30% in phase 2 studies, without significant effects on LDL cholesterol levels, blood pressure, or circulating neurohormones. 23,24 We designed a phase 3 trial, the dal-OUTCOMES study, to evaluate the effects of dalcetrapib on cardiovascular risk among patients with a recent acute coronary syndrome.")
4
Efecto sobre HDL/LDL

5
End point primario Understanding why dalcetrapib failed
Dalcetrapib in patients with recent ACS with Dr Gregory Schwartz Dr Gregory Schwartz (University of Colorado School of Medicine, Denver), the lead investigator of dal-OUTCOMES, noted that there was no effect on LDL-cholesterol levels in the 15 871-patient trial. He added that the findings of the dal-OUTCOMES study highlight the importance of conducting large, phase 3 studies in order to detect small but clinically important safety signals. In the phase 2 studies with dalcetrapib, there was no evidence of an increase in blood pressure, but dal-OUTCOMES showed that blood pressure was increased 0.6 mm Hg with the CETP inhibitor. "The fact that anacetrapib and evacetrapib, in studies of about 1000 or 1500 patients, have not shown adverse effects on blood pressure doesn't mean that phase 3 trials might not end up showing something that we have seen here," said Schwartz. In addition to the adverse effect on blood pressure, Tall said that the modest 30% increase in HDL cholesterol might have been insufficient in patients optimally treated with statins and other cardioprotective medications. This hypothesis is supported by the AIM-HIGH study, where a small 15% increase in HDL cholesterol with niacin did not translate into a reduction in the clinical end point. Equally important, it's possible that CETP inhibition might produce a form of HDL cholesterol that is dysfunctional and incapable of reverse cholesterol transport. "It may be that when other risk factors are controlled as well as we currently can using many, if not all, of our evidence-based treatments, including statins, dual antiplatelet therapies, beta blockers, etc, that the risk that's modifiable by altering HDL-cholesterol levels may not be significant," said Schwartz. He pointed out that even among patients in dal-OUTCOMES who achieved the highest HDL-cholesterol levels, approximately 70 mg/dL in about 10% of patients, there was no apparent decrease in risk compared with other patients in the trial. Full results of the morbidity and mortality trials with anacetrapib and evacetrapib are not expected for a few years.
, the lead investigator of dal-OUTCOMES, noted that there was no effect on LDL-cholesterol levels in the patient trial. He added that the findings of the dal-OUTCOMES study highlight the importance of conducting large, phase 3 studies in order to detect small but clinically important safety signals. In the phase 2 studies with dalcetrapib, there was no evidence of an increase in blood pressure, but dal-OUTCOMES showed that blood pressure was increased 0.6 mm Hg with the CETP inhibitor. The fact that anacetrapib and evacetrapib, in studies of about 1000 or 1500 patients, have not shown adverse effects on blood pressure doesn t mean that phase 3 trials might not end up showing something that we have seen here, said Schwartz. In addition to the adverse effect on blood pressure, Tall said that the modest 30% increase in HDL cholesterol might have been insufficient in patients optimally treated with statins and other cardioprotective medications. This hypothesis is supported by the AIM-HIGH study, where a small 15% increase in HDL cholesterol with niacin did not translate into a reduction in the clinical end point. Equally important, it s possible that CETP inhibition might produce a form of HDL cholesterol that is dysfunctional and incapable of reverse cholesterol transport. It may be that when other risk factors are controlled as well as we currently can using many, if not all, of our evidence-based treatments, including statins, dual antiplatelet therapies, beta blockers, etc, that the risk that s modifiable by altering HDL-cholesterol levels may not be significant, said Schwartz. He pointed out that even among patients in dal-OUTCOMES who achieved the highest HDL-cholesterol levels, approximately 70 mg/dL in about 10% of patients, there was no apparent decrease in risk compared with other patients in the trial. Full results of the morbidity and mortality trials with anacetrapib and evacetrapib are not expected for a few years.")
6
Finalizacion de Dalcetrapib Clinical Trial 7/7/2012
“The dal-OUTCOMES trial evaluated the efficacy and safety profile of dalcetrapib when added to existing standard of care in patients with stable coronary heart disease following an acute coronary syndrome. Following the results of the second interim analysis of the dalcetrapib dal-OUTCOMES Phase III trial the Independent Data and Safety Monitoring Committee (DSMC) has recommended stopping the trial due to a lack of clinically meaningful efficacy. No safety signals relating to the dal-OUTCOMES trial were reported from the DSMC. As a result, Roche has decided to terminate the dal-OUTCOMES trial, as well as all other on-going studies in the dal-HEART program, including dal-PLAQUE 2 and dal-OUTCOMES 2. Additional information will be provided in due course as data become available.” Excerpt from letter to dal-OUTCOMES Investigators from Roche. Final results of the dal-OUTCOMES study, a phase 3 clinical trial testing the efficacy of the investigational cholesteryl ester transfer protein (CETP) inhibitor dalcetrapib (Hoffman-La Roche, Ltd), were presented today at the American Heart Association 2012 Scientific Sessions and published simultaneously in the New England Journal of Medicine, leaving investigators to wrestle with reasons that the drug failed to have an impact on clinical outcomes. Some experts believe the modest but clinically significant increase in blood pressure might have doomed the drug. As reported previously by heartwire, dal-OUTCOMES was stopped after an interim analysis of the study showed the HDL-cholesterol-boosting drug was not significantly reducing cardiovascular adverse events despite increases in HDL cholesterol of approximately 30%. Dalcetrapib is the second CETP inhibitor to fall by the wayside, despite initial excitement that raising HDL-cholesterol levels would translate into a reduction in clinical events. In 2005, Pfizer halted the Investigation of Lipid Level Management to Understand its Impact in Atherosclerotic Events (ILLUMINATE) of torcetrapib when it was revealed the drug increased the risk of cardiovascular morbidity and mortality. Two other CETP inhibitors, evacetrapib (Lilly, Indianapolis, IN) and anacetrapib (Merck, Whitehouse Station, NJ) are currently being tested in large phase 3 morbidity and mortality trials. Dr Alan Tall (Columbia University, New York), who commented on the dal-OUTCOMES trial and CETP inhibition as a whole, said he does not believe the stopping of dal-OUTCOMES is a harbinger of more negative news to come about the drug class. "I wouldn't make that conclusion," Tall told the media during a formal presentation Sunday morning. "There is a concern the tiny blood-pressure signal could be a class effect, but in pretty big studies already done with anacetrapib and evacetrapib, there is no trace of that. It's important to note that the two remaining players in the field are really quite different. They lower LDL quite extensively, they lower vLDL cholesterol, and they really raise HDL cholesterol quite a lot, a lot more than dalcetrapib." In the DEFINE study, anacetrapib reduced LDL-cholesterol levels 36% and increased HDL-cholesterol levels by 138% in patients with coronary artery disease currently taking a statin. Evacetrapib was shown to have similar potency, reducing LDL cholesterol by as much as 52% when added to statin therapy and increasing HDL cholesterol by 129%.
 has recommended stopping the trial due to a lack of clinically meaningful efficacy. No safety signals relating to the dal-OUTCOMES trial were reported from the DSMC. As a result, Roche has decided to terminate the dal-OUTCOMES trial, as well as all other on-going studies in the dal-HEART program, including dal-PLAQUE 2 and dal-OUTCOMES 2. Additional information will be provided in due course as data become available. Excerpt from letter to dal-OUTCOMES Investigators from Roche. Final results of the dal-OUTCOMES study, a phase 3 clinical trial testing the efficacy of the investigational cholesteryl ester transfer protein (CETP) inhibitor dalcetrapib (Hoffman-La Roche, Ltd), were presented today at the American Heart Association 2012 Scientific Sessions and published simultaneously in the New England Journal of Medicine, leaving investigators to wrestle with reasons that the drug failed to have an impact on clinical outcomes. Some experts believe the modest but clinically significant increase in blood pressure might have doomed the drug. As reported previously by heartwire, dal-OUTCOMES was stopped after an interim analysis of the study showed the HDL-cholesterol-boosting drug was not significantly reducing cardiovascular adverse events despite increases in HDL cholesterol of approximately 30%. Dalcetrapib is the second CETP inhibitor to fall by the wayside, despite initial excitement that raising HDL-cholesterol levels would translate into a reduction in clinical events. In 2005, Pfizer halted the Investigation of Lipid Level Management to Understand its Impact in Atherosclerotic Events (ILLUMINATE) of torcetrapib when it was revealed the drug increased the risk of cardiovascular morbidity and mortality. Two other CETP inhibitors, evacetrapib (Lilly, Indianapolis, IN) and anacetrapib (Merck, Whitehouse Station, NJ) are currently being tested in large phase 3 morbidity and mortality trials. Dr Alan Tall (Columbia University, New York), who commented on the dal-OUTCOMES trial and CETP inhibition as a whole, said he does not believe the stopping of dal-OUTCOMES is a harbinger of more negative news to come about the drug class. I wouldn t make that conclusion, Tall told the media during a formal presentation Sunday morning. There is a concern the tiny blood-pressure signal could be a class effect, but in pretty big studies already done with anacetrapib and evacetrapib, there is no trace of that. It s important to note that the two remaining players in the field are really quite different. They lower LDL quite extensively, they lower vLDL cholesterol, and they really raise HDL cholesterol quite a lot, a lot more than dalcetrapib. In the DEFINE study, anacetrapib reduced LDL-cholesterol levels 36% and increased HDL-cholesterol levels by 138% in patients with coronary artery disease currently taking a statin. Evacetrapib was shown to have similar potency, reducing LDL cholesterol by as much as 52% when added to statin therapy and increasing HDL cholesterol by 129%.")
7
AMG 145 y REGN727/SAR (REGN727), anticuerpos monoclonales humanos que se unen PCSK9 (Proprotein convertase subtilisin/kexin type 9) El papel de PCSK9, una proteasa secretada que se ha relacionado con la regulación de la actividad del receptor LDL hepático está bien establecido a través de la genética humana y los modelos animales. Se ha visto que el bloqueo de la unión de PCSK9 al receptor LDL mediante anticuerpos monoclonales es efectivo en disminuir el C-LDL en humanos. Y el anticuerpo monoclonal de este estudio AMG145 ya había demostrado que al actuar sobre PCSK9 conseguía reducciones de un 81% frente a placebo en estudios de fases y el efecto se mantenía durante 28 días

8
En tres ensayos fase I, tratamiento con con REGN727 redujo de forma significativa el LDL en voluntarios sanos y pacientes con hipercolesterolemia familiar o no. No se aprecio ninguna suspensión de tratamiento por efectos adversos.

9
Dosis respuesta con AMG 145 SC cada 2 semanas
Dosis respuesta con AMG 145 SC cada 2 semanas. % reducción LDL en 12 semanas

10
Diseño del estudio 78 centers 5 countries 934 screened 631 random.
Day 1 Visits: Week 2 Week 8 Week 12 Week 6 Week 4 Week 10 Week 14 70 mg AMG 145 SC Q2W 79 Subjects 105 mg AMG 145 SC Q2W 79 Subjects 140 mg AMG 145 SC Q2W 78 Subjects Placebo SC Q2W 78 Subjects Q2W: Screening and Placebo Run-in Period Subcutaneous injection of 6 mL placebo Fasting LDL-C 5-10 days before randomization Randomization (n=631) : : : 1 End of Study: 4 weeks after last dose Optional Enrollment in Extension Study Primary Endpoint Assessed 280 mg AMG 145 SC Q4W 79 Subjects 350 mg AMG 145 SC Q4W 79 Subjects 420 mg AMG 145 SC Q4W 80 Subjects Placebo SC Q4W 77 Subjects Q4W: 1 : : 1 : 1 Maximum 6 weeks 934 screened 631 random. 629 treated ( *2 subjects assigned placebo Q4W received no study drug) Kohli P, et al. Clin Cardiol. 2012;35:
 1 : 1 : 1 : 1. End of Study: 4 weeks after last dose. Optional Enrollment in Extension Study. Primary Endpoint. Assessed. 280 mg AMG 145 SC Q4W 79 Subjects. 350 mg AMG 145 SC Q4W 79 Subjects. 420 mg AMG 145 SC Q4W 80 Subjects. Placebo SC Q4W 77 Subjects. Q4W: 1 : 1 : 1 : 1. Maximum 6 weeks. 934 screened. 631 random. 629 treated. ( *2 subjects assigned placebo Q4W received no study drug) Kohli P, et al. Clin Cardiol. 2012;35:")
12
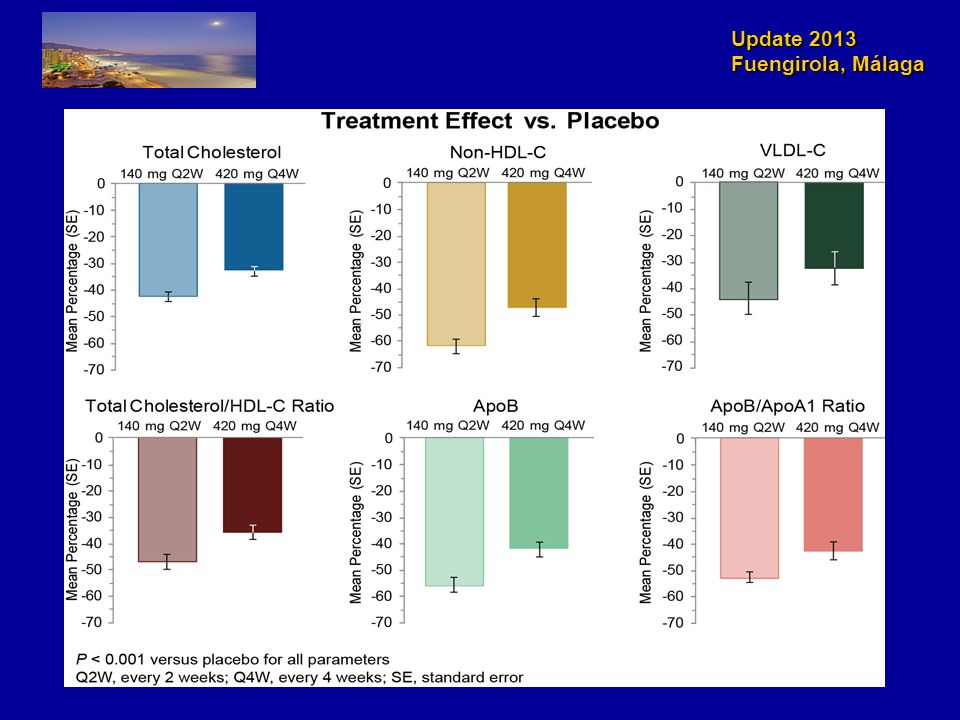
En LAPLACE-TIMI 57, 631 pacientes estables con estatinas (y 10% con ezetimibe) se randomizaron a 6 brazos de AMG-145 o placebo. LDL basal medio fue 120 mg/dL. Tras 12 sem de tratamiento los niveles de LDL cayeron hasta LDL un 66% con AMG-145. No eventos adversos ni anticuerpos En un análisis de 284 pacientes con alto riesgo cardiovascular, 90% con la dosis mas alta de AMG-145 alcanzaron los niveles de LDL <70 mg/dL.

13
Hipercolesterolemia LDL > 100
MENDEL study Figure 2 Percentage change in LDL-C concentration from baseline to week 12 in AMG 145 every 2 weeks, placebo every 2 weeks, and daily ezetimibe groups (A) and AMG 145 every 4 weeks, placebo every 4 weeks, and daily ezetimibe groups (B) Data are ... Efficacy, safety, and tolerability of a monoclonal antibody to proprotein convertase subtilisin/kexin type 9 as monotherapy in patients with hypercholesterolaemia (MENDEL): a randomised, double-blind, placebo-controlled, phase 2 study. The Lancet Volume 380, Issue
 and AMG 145 every 4 weeks, placebo every 4 weeks, and daily ezetimibe groups (B) Data are ... Efficacy, safety, and tolerability of a monoclonal antibody to proprotein convertase subtilisin/kexin type 9 as monotherapy in patients with hypercholesterolaemia (MENDEL): a randomised, double-blind, placebo-controlled, phase 2 study. The Lancet Volume 380, Issue")
14
Intolerantes a estatinas.
GAUSS Trial LDL-C values at baseline and week 12 were measured using preparative ultracentrifugation. Q4W, every 4 weeks; QD, daily; SE, standard error JAMA. 2012;308(23):
:")
15
Hipercolesterolemia familiar.
RUTHEFORD study Percentage change from baseline in calculated low-density lipoprotein cholesterol (LDL-C) to week 12. Circulation. 126(20): , November 13, 2012.
 to week 12. Circulation. 126(20): , November 13,")
16
Hipercolesterolemia familiar.
REGN727/SAR236553 Percentage change from baseline in calculated low-density lipoprotein cholesterol (LDL-C) to week 12. Lancet 2012; 380: 29–36
 to week 12. Lancet 2012; 380: 29–36.")
17
Que esperamos… Fuente: Clinicaltrials.gov
The ODYSSEY Outcomes incluira pacientes con un SCA y LDL fuera de objetivos valorara la eficacia de SAR236553/REGN727 (inyeccion SC de 75 mg SC cada 2 semanas) añadido a dosis maximas de estatinas y evaluara reducción de eventos CV.5 años de seguimiento. Marzo Fase 3 Durable Effect of PCSK9 Antibody CompARed wiTh placEbo Study - DESCARTES; Fase 2 con AMG 145 que evalúa efectos a las 52 semanas en pacientes con hipercolesterolemia. Abril 2014. Further Cardiovascular Outcomes Research With PCSK9 Inhibition in Subjects With Elevated Risk -FOURIER que evalúa efectos sobre muerte cardiovascular, infarto de miocardio, hospitalización por angina inestable, ictus o revascularización coronaria con un seguimiento de unos 5 años pacientes . Mayo Fase 3 Fuente: Clinicaltrials.gov
 añadido a dosis maximas de estatinas y evaluara reducción de eventos CV.5 años de seguimiento. Marzo Fase 3. Durable Effect of PCSK9 Antibody CompARed wiTh placEbo Study - DESCARTES; Fase 2 con AMG 145 que evalúa efectos a las 52 semanas en pacientes con hipercolesterolemia. Abril Further Cardiovascular Outcomes Research With PCSK9 Inhibition in Subjects With Elevated Risk -FOURIER que evalúa efectos sobre muerte cardiovascular, infarto de miocardio, hospitalización por angina inestable, ictus o revascularización coronaria con un seguimiento de unos 5 años pacientes . Mayo Fase 3. Fuente: Clinicaltrials.gov.")
18
25,673 high-risk patients with occlusive arterial disease from China, Scandinavia and UK
Randomized comparison: ER niacin/laropiprant (ERN/LRPT) 2g daily versus placebo Primary end point: Major vascular events after median follow-up of 4 years Pre-specified safety analyses: Median follow-up of 3.4 years (to January 2012) Background LDL-lowering therapy with: Simvastatin 40mg (+/- ezetimibe 10mg) daily
 2g daily versus placebo Primary end point: Major vascular events after median follow-up of 4 years Pre-specified safety analyses: Median follow-up of 3.4 years (to January 2012) Background LDL-lowering therapy with: Simvastatin 40mg (+/- ezetimibe 10mg) daily")
19
HPS2-THRIVE: Diseño y randomizacion

20
HPS2-THRIVE: Suspension del estudio
“In the study, adding the combination of extended-release niacin and laropiprant to statin therapy did not significantly further reduce the risk of the combination of coronary deaths, non-fatal heart attacks, strokes or revascularizations compared to statin therapy. In addition, there was a statistically significant increase in the incidence of some types of non-fatal serious adverse events in the group that received extended-release niacin/laropiprant. “

21
DIABETES. ESTUDIO ORIGIN

22
El control intensivo tardío no mejora los eventos CV
ACCORD ADVANCE VADT Características de los pacientes n 10.251 11.140 1.791 Edad media (años) 62 66 60 Duración de la diabetes (años) 10 8 11,5 Historia de ECV (%) 35 32 40 Mediana de HbA1c basal (%) 8,1 7,2 9,4 Tratamiento con insulina en el basal (%) 1,5 52 Características del protocolo del estudio Objetivos de HbA1c (%) (l vs. E) < 6,0 vs. 7,0 - 7,9 < 6,0 vs. “recomendacion local” <6 (cambio si > 6,5) vs dif -1,5 Protocolo de control glucémico (l vs. E) Múltiples fármacos + gliclizida vs - gliclizida Manejo de otros factores de riesgo presión arterial y lípidos presión arterial Protocolo tratamiento intensivo ambos grupos Resultados del estudio Mediana de HbA1c alcanzada (%) (l vs. E) 6,4 vs. 7,5 6,3 vs. 7,0 6,9 vs. 8,5 Insulina al final del estudio (%) (l vs. E) 77 vs. 55* 40 vs. 24 89 vs. 0,74 Cambios en el peso (kg) (l vs. E) + 3,5 vs +0,4 - 0,1 vs -1,0 + 7,8 vs +3,4 Hipoglucemias severa (pac con >1 episodios durante el estudio) (l vs. E) 16,2 vs 5,1 2,7 vs 1,5 21,2 vs 9,9 Variables Definición variable principal Macrovascular ^ Microvascular más macrovascular (IM no fatal, ictus no fatal, muerte ECV) Macrovascular ^, hospitalización por IC, revascularización HR para variable principal (IC 95%) 0,90 (0,78 - 1,04) 0,90 (0,82 - 0,98); Macro 0,94 (0,84 - 1,06) 0,88 (0,74 - 1,05) HR para resultados mortalidad (IC 95%) 1,22 (1,01 - 1,46) 0,93 (0,83 - 1,06) 1,07 (0,81 - 1,42) Los beneficios del control glucémico intensivo sobre las complicaciones microvasculares y neuropáticas están bien establecidos. Los estudios ADVANCE y VADT aumentan la evidencia al demostrar una reducción significativa del riesgo de sufrir o empeorar la albuminuria con el control glucémico intensivo. La falta de reducción significativa de los eventos cardiovasculares con el control glucémico intensivo en el ACCORD, ADVANCE y VADT no deberia llevar a los clínicos a abandonar el objetivo general de HbA1c<7% eliminando el beneficio del buen control sobre las complicaciones microvasculares, que son bebilitantes y graves. Un meta-analisis de los 3 estudios sugiere que la reducción de la glucemia tiene una modesta reducción (9%) pero estadisticamente significativa en los eventos CV graves (IM no fatal) sin aumento significativo de la mortalidad. Un subanálisis sugiere que la mayor reducción de eventos CV ocurre en los pacientes sin ECV conocida (HR 0.84(IC95% ). Por el contrario, la mortalidad del ACCORD y subanálisis del VADT sugieren que el riesgo potencial del control glucémico muy intensivo puede soprepasar los beneficios en algunos pacientes, con duración muy larga de la diabetes, historial conocido de hipoglucemias gravesl atersoclerosis avanzada y edad avanzada/fraglidad. Hay que prevenir las hipoglucemias graves en pacientes con enfermedad avanzada y no deberia conseguirse de forma agresiva HbA1c casi-normal en pacientes en los que este objetivo no se pueda conseguir razonable y facilmente. (ADA2011) Reducción evento microvascular (macroalbuminuria) Aumento de la mortalidad con tto intensivo Aumento de mortalidad CV pero NS * Las tasas de insulinización en el estudio ACCORD fueron para cualquier uso durante el estudio. I: control glucémico intensivo; E: control glucémico estándar. ^Macrovascular: IM no fatal, ictus no fatal, muerte ECV American Diabetes Association. Diabetes Care 2010.
 Duración de la diabetes (años) ,5. Historia de ECV (%) Mediana de HbA1c basal (%) 8,1. 7,2. 9,4. Tratamiento con insulina en el basal (%) 1, Características del protocolo del estudio. Objetivos de HbA1c (%) (l vs. E) < 6,0 vs. 7,0 - 7,9. < 6,0 vs. recomendacion local <6 (cambio si > 6,5) vs dif -1,5. Protocolo de control glucémico (l vs. E) Múltiples fármacos. + gliclizida vs - gliclizida. Manejo de otros factores de riesgo. presión arterial y lípidos. presión arterial. Protocolo tratamiento intensivo ambos grupos. Resultados del estudio. Mediana de HbA1c alcanzada (%) (l vs. E) 6,4 vs. 7,5. 6,3 vs. 7,0. 6,9 vs. 8,5. Insulina al final del estudio (%) (l vs. E) 77 vs. 55* 40 vs vs. 0,74. Cambios en el peso (kg) (l vs. E) + 3,5 vs +0,4. - 0,1 vs -1,0. + 7,8 vs +3,4. Hipoglucemias severa (pac con >1 episodios durante el estudio) (l vs. E) 16,2 vs 5,1. 2,7 vs 1,5. 21,2 vs 9,9. Variables. Definición variable principal. Macrovascular ^ Microvascular más macrovascular (IM no fatal, ictus no fatal, muerte ECV) Macrovascular ^, hospitalización por IC, revascularización. HR para variable principal (IC 95%) 0,90 (0,78 - 1,04) 0,90 (0,82 - 0,98); Macro 0,94 (0,84 - 1,06) 0,88 (0,74 - 1,05) HR para resultados mortalidad (IC 95%) 1,22 (1,01 - 1,46) 0,93 (0,83 - 1,06) 1,07 (0,81 - 1,42) Los beneficios del control glucémico intensivo sobre las complicaciones microvasculares y neuropáticas están bien establecidos. Los estudios ADVANCE y VADT aumentan la evidencia al demostrar una reducción significativa del riesgo de sufrir o empeorar la albuminuria con el control glucémico intensivo. La falta de reducción significativa de los eventos cardiovasculares con el control glucémico intensivo en el ACCORD, ADVANCE y VADT no deberia llevar a los clínicos a abandonar el objetivo general de HbA1c<7% eliminando el beneficio del buen control sobre las complicaciones microvasculares, que son bebilitantes y graves. Un meta-analisis de los 3 estudios sugiere que la reducción de la glucemia tiene una modesta reducción (9%) pero estadisticamente significativa en los eventos CV graves (IM no fatal) sin aumento significativo de la mortalidad. Un subanálisis sugiere que la mayor reducción de eventos CV ocurre en los pacientes sin ECV conocida (HR 0.84(IC95% ). Por el contrario, la mortalidad del ACCORD y subanálisis del VADT sugieren que el riesgo potencial del control glucémico muy intensivo puede soprepasar los beneficios en algunos pacientes, con duración muy larga de la diabetes, historial conocido de hipoglucemias gravesl atersoclerosis avanzada y edad avanzada/fraglidad. Hay que prevenir las hipoglucemias graves en pacientes con enfermedad avanzada y no deberia conseguirse de forma agresiva HbA1c casi-normal en pacientes en los que este objetivo no se pueda conseguir razonable y facilmente. (ADA2011) Reducción evento microvascular (macroalbuminuria) Aumento de la mortalidad con tto intensivo. Aumento de mortalidad CV pero NS. * Las tasas de insulinización en el estudio ACCORD fueron para cualquier uso durante el estudio. I: control glucémico intensivo; E: control glucémico estándar. ^Macrovascular: IM no fatal, ictus no fatal, muerte ECV. American Diabetes Association. Diabetes Care")
23
Meta-analisis de los estudios que comparan control intensivo vs estandard (ACCORD, ADVANCE, UKPDS*, VADT): pacientes ↓9% riesgo eventos coronarios mayores, ↓15% riesgo Infarto de miocardio. No efecto en la incidencia de ICTUS, insuficiencia cardiaca, mortalidad cualquier causa, muerte CV ↑ 2-5 veces riesgo de hipoglucemias en tto intensivo vs menos intensivo * Seguimiento hasta 5 años para el metaanalisis. † Fatal o non-fatal IM. Turnbull FM et al. Diabetologia 2009;52:

24
ORIGIN abarca eventos CV asi como prevención de diabetes
Tiempo desde el diagnóstico de la diabetes -15a -10a -5a 0a +5a +10a +15a NAVIGATOR ADVANCE STOP-NIDDM PROactive DREAM ACCORD DPP VADT STENO-2 UKPDS ORIGIN GAA/IOG Diabetes Mellitus tipo 2 Retinopatia, Nefropatia, Neuropatia Enfermedad CV 24

25
Cuestiones planteadas en el Estudio ORIGIN
¿Proporcionar insulina basal suficiente (glargina) para conseguir de una manera segura (normoglucemia en ayunas) reduce la incidencia de eventos CV más que el tratamiento estándar en personas con elevación moderada de la glucemia y alto riesgo CV? ¿Los ácidos insaturados (ω-3-acid ethyl esteres 90) reducen la mortalidad CV comparados con placebo? Proporcionar insulina basal, glargina titulada para conseguir GPA normal durante más de 6 años: ¿Reduce la ECV, complicaciones ojos/riñones, otros eventos? ¿Retrasa la diabetes en personas con alteraciones de la glucemia? ¿La hipoglucemia producida por insulina causa daños?
 para conseguir de una manera segura (normoglucemia en ayunas) reduce la incidencia de eventos CV más que el tratamiento estándar en personas con elevación moderada de la glucemia y alto riesgo CV ¿Los ácidos insaturados (ω-3-acid ethyl esteres 90) reducen la mortalidad CV comparados con placebo Proporcionar insulina basal, glargina titulada para conseguir GPA normal durante más de 6 años: ¿Reduce la ECV, complicaciones ojos/riñones, otros eventos ¿Retrasa la diabetes en personas con alteraciones de la glucemia ¿La hipoglucemia producida por insulina causa daños")
26
Basal Insulin and Cardiovascular and Other Outcomes in Dysglycemia
Figure 2. Proportion of Participants with Events over Time. The ORIGIN Trial Investigators. N Engl J Med 2012;367:

27
n–3 Fatty Acids and Cardiovascular Outcomes in Patients with Dysglycemia
The ORIGIN Trial Investigators. N Engl J Med 2012;367:

29
Novedades respecto a las guías 2007
Nueva escala de recomendación. 4 niveles de riesgo CV. Se etiquetan mas países de bajo riesgo. Concepto de edad-riesgo y tablas de riesgo relativo Importancia de los factores psicosociales Papel limitado de los nuevos biomarcadores de riesgo Tabaquismo pasivo Objetivos en HTA, DM y Lípidos

30
Recomendaciones: Nueva escala de recomendación
Método convencional: Niveles de evidencia: A, B y C Recomendación: I, IIa, IIb o III Escala GRADE: Strong o Fuerte: Uno debería recomendar este tratamiento Weak o débil : Uno podría considerar tras opciones El grado de reco- mendación se basa en el nivel de evidencia, el cociente riesgo/benefi- cio, las preferencias de los pacientes y los recursos disponibles. Una recomendación GRADE strong o fuerte implica que la mayoría de los pacientes bien informados elegirían la intervención, la mayoría de los médicos la aplicarían y es asumible por el sistema sanitario, mientras que una recomendación GRADE weak o débil es aquella que sólo algu- nos pacientes elegirían, los médicos la indicarían individualizada- mente y su aplicabilidad sociosanitaria es debatible

31
4 CATEGORIAS DE RIESGO ECV documentada
MUY ALTO RIESGO ECV documentada DM I o II con uno o más factores de riesgo CV o lesión de órgano diana. IRC grave (TFG < 30 ml/min/1,73 m2). Riesgo SCORE ≥ 10%. ALTO RIESGO Factores de riesgo específicos marcadamente elevados, como dislipemia familiar e hipertensión grave. DM I o II sin factores de riesgo CV o lesión de órgano diana. IRC moderada (TFG ml/min/1,73 m2). Riesgo SCORE ≥ 5 % y < 10%. MODERADO RIESGO Se considera que un individuo tiene un riesgo moderado cuando su estimación SCORE de riesgo a 10 años es ≥ 1% y < 5%. BAJO RIESGO La categoría de bajo riesgo se aplica a individuos con una estimación SCORE < 1% y en ausencia de otros calificadores que indicaran un riesgo moderado.
. Riesgo SCORE ≥ 10%. ALTO RIESGO. Factores de riesgo específicos marcadamente elevados, como dislipemia familiar e hipertensión grave. DM I o II sin factores de riesgo CV o lesión de órgano diana. IRC moderada (TFG ml/min/1,73 m2). Riesgo SCORE ≥ 5 % y < 10%. MODERADO RIESGO. Se considera que un individuo tiene un riesgo moderado cuando su estimación SCORE de riesgo a 10 años es ≥ 1% y < 5%. BAJO RIESGO. La categoría de bajo riesgo se aplica a individuos con una estimación SCORE < 1% y en ausencia de otros calificadores que indicaran un riesgo moderado.")
32
Paises de alto y bajo riesgo
• Punto de corte: mortalidad CV y por DM en 2008 para personas de edades comprendidas entre los 45 y los 74 años (220/ varones y 160/ mujeres) • Low risk: Andorra, Austria, Belgium, Cyprus, Denmark, Finland, France, Germany, Greece, Iceland, Ireland, Israel, Italy, Luxembourg, Malta, Monaco, The Netherlands, Norway, Portugal, San Marino, Slovenia, Spain, Sweden, Switzerland, United Kingdom Que la mortalidad CV haya descendido en muchos países europeos implica que más países entren en la categoría de bajo riesgo. Si bien cualquier punto de corte es arbitrario y susceptible de debate, en esta guía los puntos de corte se basan en la mortalidad CV y por DM en 2008 para personas de edades comprendidas entre los 45 y los 74 años (220/ varones y 160/ mujeres)69. Esto define a 21 países y marca un punto en el cual hay una gran diferencia con el país número 22 (República Checa). • High risk: All others • Very high risk: (>500/100,000 for men and >250/100/000 for women): Armenia, Azerbaijan, Belarus, Bulgaria, Georgia, Kazakhstan, Kyrgyzstan, Latvia, Lithuania, Macedonia FYR, Moldova, Russia, Ukraine, Uzbekistan
 • Low risk: Andorra, Austria, Belgium, Cyprus, Denmark, Finland, France, Germany, Greece, Iceland, Ireland, Israel, Italy, Luxembourg, Malta, Monaco, The Netherlands, Norway, Portugal, San Marino, Slovenia, Spain, Sweden, Switzerland, United Kingdom. Que la mortalidad CV haya descendido en muchos países europeos implica que más países entren en la categoría de bajo riesgo. Si bien cualquier punto de corte es arbitrario y susceptible de debate, en esta guía los puntos de corte se basan en la mortalidad CV y por DM en 2008 para personas de edades comprendidas entre los 45 y los 74 años (220/ varones y 160/ mujeres)69. Esto define a 21 países y marca un punto en el cual hay una gran diferencia con el país número 22 (República Checa). • High risk: All others. • Very high risk: (>500/100,000 for men and. >250/100/000 for women): Armenia, Azerbaijan, Belarus, Bulgaria, Georgia, Kazakhstan, Kyrgyzstan, Latvia, Lithuania, Macedonia FYR, Moldova, Russia, Ukraine, Uzbekistan.")
33
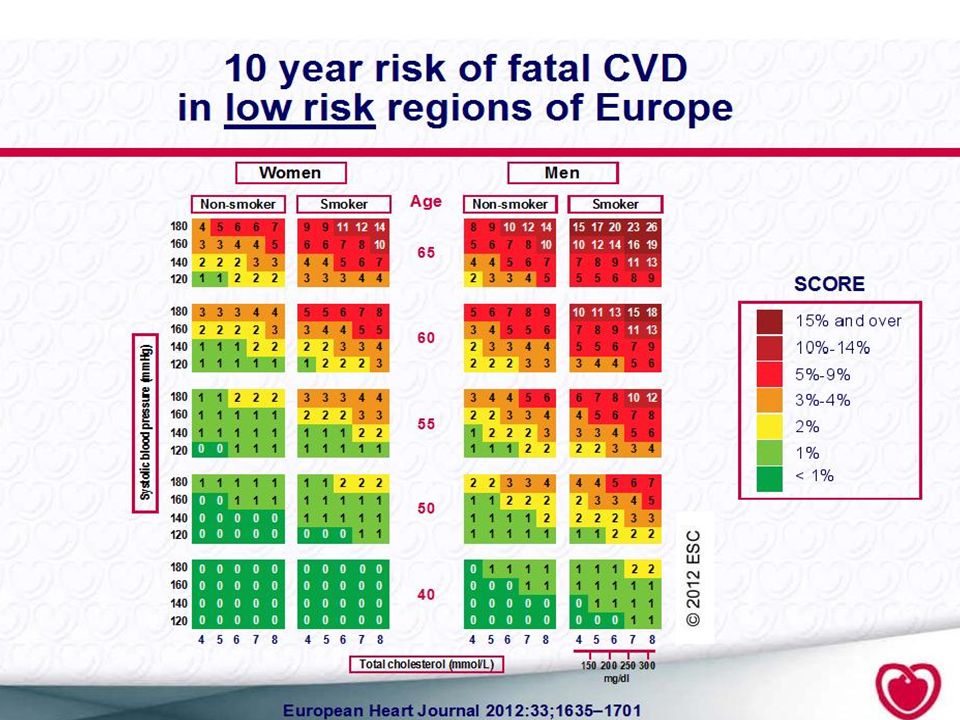
Age standardised CHD mortality rates (under 65) in men & women No data
< 30 30-50 50-70 70-100 > 200 Age standardised CHD mortality rates (under 65) in men & women
 in men & women.")
35
Tabla de riesgo relativo
En personas jóvenes, un riesgo absoluto bajo puede encubrir un riesgo relativo muy alto; el uso de las tablas de riesgo relativo o la estimación de su edad de riesgo son útiles en estas personas y permiten asesorarles sobre la necesidad de cambios en el estilo de vida VARON 55 AÑOS 120/80 CT 270 mg/dl FUMADOR 4 % Riesgo moderado Pero 3 veces mas que otro Varón de la misma edad sin FRC

36
Edad de riesgo o edad vascular
Cuende JL et al European Heart Journal (2010) 31, 2351–2358
 31, 2351–2358.")
37
FACTORES PSICOSOCIALES
• Se reconocen los factores psicosociales como factores de riesgo que contribuyen a un aumento del riesgo CV y peor pronostico. Estos factores impiden la adherencia al tratamiento y estilo de vida saludable Estos factores deberian ser evaluados de forma sistematica para mejorar el pronostico y calidad de vida de estos pacientes

38
FACTORES PSICOSOCIALES
Arch Intern Med. 2012;172(22):
:")
39
BIOMARCADORES DE RIESGO
LIMITACIONES NUEVOS BIOMARCADORES DE RIESGO El uso de estos biomarcadores queda reducido a pacientes con riesgo moderado para reclasificarlos a un riesgo superior con una recomendación débil (IIb B, GRADE débil).
.")
40
BIOMARCADORES DE RIESGO
LIMITACIONES NUEVOS BIOMARCADORES DE RIESGO Según las guías actuales, la evaluación de la PCR o fibrinógeno en personas de riesgo intermedio para un evento CV prevendría un único evento adicional sobre un periodo de 10 años por cada personas bajo screening. Emerging Risk Factors Collaboration investigated the predictive value of adding C-reactive protein or fibrinogen levels to conventional risk factors.6 In a meta-analysis of 52 prospective studies of participants without a history of CV disease, the assessment of C-reactive protein or fibrinogen levels yielded only a modest reclassification improvement for those at intermediate risk compared with models which included only age, sex smoking status, blood pressure, history of diabetes, and total cholesterol levels.6 It was estimated that participants at intermediate risk who did not meet recommendations for the initiation of statin therapy by ATPIII guidelines would become eligible after an additional assessment of C-reactive protein and this might result in prevention of 30 additional CV events over a 10-year period.6 These results, however, have been challenged by the ASCOT investigators.7 In this large study of hypertensive patients, there was no improvement in CV event prediction when C-reactive protein was added to the Framingham risk score. Importantly, reduction in C-reactive protein associated with statin therapy was not a predictor of CV benefit.7 N Engl J Med 2012;367: Evaluation of C-reactive protein prior to and on-treatment as a predictor of benefit from atorvastatin: observations from the Anglo-Scandinavian Cardiac Outcomes Trial. Eur Heart J 2012;33:486–494.

41
TABAQUISMO Como novedad, se resalta la importancia del tabaquismo pasivo y de las leyes que restringen el consumo de tabaco en lugares públicos.

42
Rev Esp Cardiol. 2012;65(10):937.e1-e66
:937.e1-e66")
43
DIABETES Información nueva importante: • El objetivo terapéutico de HbA1c ha aumentado de < 6,5% a < 7,0%. • Actualmente la aspirina no se recomienda para la prevención primaria en pacientes diabéticos Rev Esp Cardiol. 2012;65(10):937.e1-e66
:937.e1-e66.")
44
DISLIPEMIA Objetivos Rev Esp Cardiol. 2012;65(10):937.e1-e66
Riesgo Bajo o Moderado: LDL < 115 Riesgo elevado: LDL < 100 Riesgo muy alto: LDL < 70 Rev Esp Cardiol. 2012;65(10):937.e1-e66
:937.e1-e66.")
45
OTROS TRENDING TOPIC DEL AÑO
Use of a Multidrug Pill In Reducing cardiovascular Events (UMPIRE): rationale and design of a randomised controlled trial of a cardiovascular preventive polypill-based strategy in India and Europe. Eur J Prev Cardiol Oct 4. Presentado AHA 2012 Physical activity levels, ownership of goods promoting sedentary behaviour and risk of myocardial infarction: results of the INTERHEART study. Eur Heart J 2012;33:452–466. Sugar-sweetened beverages and genetic risk of obesity. N Engl J Med 2012;367:1387–1396. A trial of sugar-free or sugar-sweetened beverages and body weight in children. N Engl J Med 2012;367:1397–1406. A randomized trial of sugar-sweetened beverages and adolescent body weight. N Engl J Med 2012;367:1407–1416. 1. Thom et al.37 reported the preliminary results of the UMPIRE Trial, where a fixed-dose combination pill containing aspirin, a statin, and two antihypertensives was administered to patients with or at high risk for CV disease. The use of a single pill (polypill) resulted in 21% increase in the number of patients adherent to medications.37 This was associated with significantly lower systolic blood pressure and LDL cholesterol recorded in the polypill group compared with patients who received usual care.
: rationale and design of a randomised controlled trial of a cardiovascular preventive polypill-based strategy in India and Europe. Eur J Prev Cardiol Oct 4. Presentado AHA Physical activity levels, ownership of goods promoting sedentary behaviour and risk of myocardial infarction: results of the INTERHEART study. Eur Heart J 2012;33:452–466. Sugar-sweetened beverages and genetic risk of obesity. N Engl J Med 2012;367:1387–1396. A trial of sugar-free or sugar-sweetened beverages and body weight in children. N Engl J Med 2012;367:1397–1406. A randomized trial of sugar-sweetened beverages and adolescent body weight. N Engl J Med 2012;367:1407– Thom et al.37. reported the preliminary results of the UMPIRE Trial, where a. fixed-dose combination pill containing aspirin, a statin, and two. antihypertensives was administered to patients with or at high. risk for CV disease. The use of a single pill (polypill) resulted in. 21% increase in the number of patients adherent to medications.37. This was associated with significantly lower systolic blood pressure. and LDL cholesterol recorded in the polypill group compared with. patients who received usual care.")
Presentaciones similares














en Ateroesclerosis. Seguridad y Eficacia Presentado en el.>")




