Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Hospital de Clínicas “José de San Martín”
GAMAPATÍAS MONOCLONALES División Hematología Hospital de Clínicas “José de San Martín”

2
MACROGLOBULINEMIA DE WALDENSTRÖM

3
GAMAPATÍA MONOCLONAL Ig M
ENTIDADES CLÍNICAS M.G.U.S.: Ig. M < 3 gr/dl. M.O.: sin infiltración Asintomática Desórdenes relacionados con la Ig.M: Neuropatías (síntomas por Ig.M Crioglobulinas M.O. no infiltrada) Crioaglutininas Amiloidosis Macroglobulinemia de Waldeström: Ig.M ↑ M.O. infiltrada Sintomática
 Crioaglutininas. Amiloidosis. Macroglobulinemia de Waldeström: Ig.M ↑ M.O. infiltrada. Sintomática.")
4
MACROGLOBULINEMIA DE WALDENSTRÖM
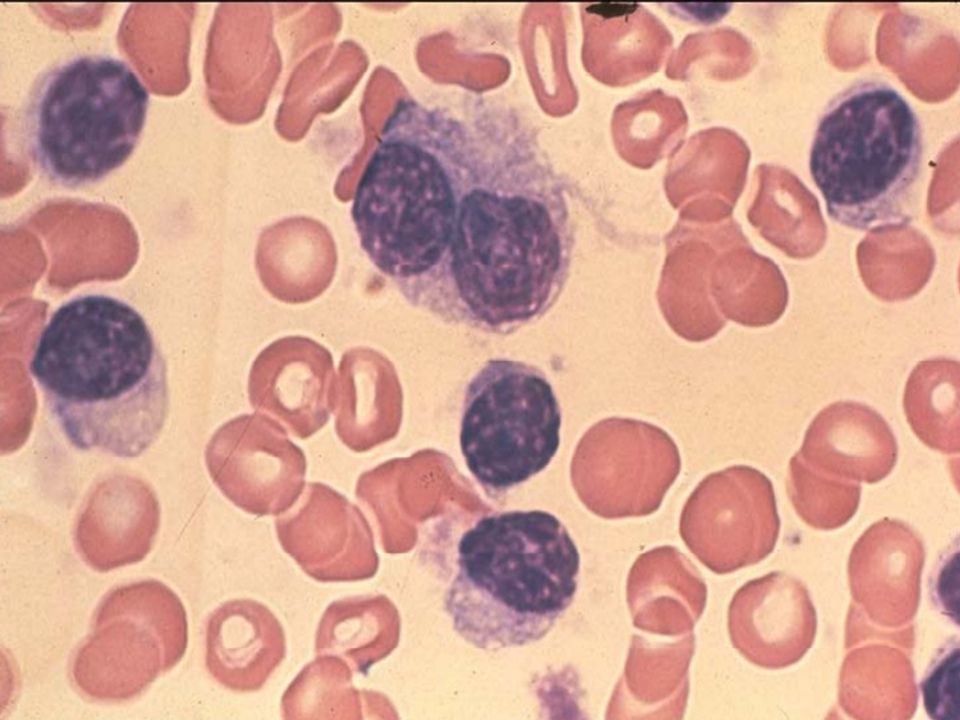
DEFINICIÓN Desorden linfoproliferativo poco común, caracterizado por una infiltración de médula ósea por linfocitos de aspecto maduro y / o linfoplasmocitos y plasmocitos y una gamapatía monoclonal Ig M. A.P. (W.H.O.): Linfoma linfoplasmocítico
: Linfoma linfoplasmocítico.")
5
Definición clínicopatológica de la MW
Diagnóstico histopatológico de Linfoma Linfoplasmocítico usando el criterio de la REAL/WHO Presencia de una proteina monoclonal Ig. M, sin importar su concentración REAL/WHO, Revised European-American Lymphoma / World Health Organization. I mentioned early on that Waldenström’s macroglobulinemia is a lymphoma and best classified under the pathological diagnosis of lymphoplasmacytic lymphoma using either the REAL or WHO criteria. Roughly 95% of the lymphoplasmacytic lymphomas make IgM and therefore are Waldenström’s, but a small percentage—5%—can make either IgG or IgA, or are what we call nonsecretory. The reason why I included “regardless of serum level” has to do with the study that we published in the journal Blood in the “How I Treat” series 2 years ago where we looked at the relationship of IgM to bone marrow involvement. Owen RG, et al. Semin Oncol. 2003;30: 5

6
Falta de relación entre el nivel de Ig. M y el compromiso de la M.O.
14,000 IgM (mg/dL) 12,000 10,000 8000 6000 What you can see here is that there’s absolutely no relationship between IgM and bone marrow involvement. You can have patients who have very little disease involvement but who make a lot of IgM. Many times, we have to treat these patients because they’re symptomatic from hyperviscosity because their IgM level is very high. At the other extreme, you can have patients who have a lot of disease involvement of their bone marrow but make very little IgM. For this reason, there’s no cutoff. It’s important to recognize this because you can have 2 patients that have the same IgM level but have vastly different underlying disease burden. 4000 2000 0% 20% 40% 60% 80% 100% BM Involvement Treon SP, Blood. 2009;114: 6
 12, , What you can see here is that there’s absolutely no relationship between IgM and bone marrow involvement. You can have patients who have very little disease involvement but who make a lot of IgM. Many times, we have to treat these patients because they’re symptomatic from hyperviscosity because their IgM level is very high. At the other extreme, you can have patients who have a lot of disease involvement of their bone marrow but make very little IgM. For this reason, there’s no cutoff. It’s important to recognize this because you can have 2 patients that have the same IgM level but have vastly different underlying disease burden % 20% 40% 60% 80% 100% BM Involvement. Treon SP, Blood. 2009;114:")
7
MACROGLOBULINEMIA DE WALDENSTRÖM
CARACTERISTICAS BAJA FRECUENCIA : 6% de todas las gamapatías monoclonales 2 a 5 casos / millón de habitantes / año EDAD AVANZADA : Media : 71 años – Hombre / mujer : 2:1 HISTORIA NATURAL : Enfermedad indolente 1/3 mueren por otras causas (no por W.M.)
")
8
MACROGLOBULINEMIA DE WALDENSTRÖM
ETIOLOGÍA Casos familiares : asociados a otros sindromes linfoproliferativos con o sin gamapatía monoclonal Estimulación antigénica crónica : Hepatitis C H.I.V Otras enfermedades autoinmunes

9
MACROGLOBULINEMIA DE WALDENSTRÖM
Biopsia de Médula Ósea: muy importante Infiltración por linfocitos de aspecto maduro,plasmocitos y linfoplasmocitos. Fenotipo: CD FMC 7 + CD CD 11c neg. CD CD 5 neg. CD CD 10 neg. Citogenética: del 6 q

11
MACROGLOBULINEMIA DE WALDENSTRÖM Clasificación clínica
ASINTOMÁTICA : supervivencia ≈ a población general SINTOMÁTICA : supervivencia 5 años más corta que población general

12
MACROGLOBULINEMIA DE WALDENSTRÖM
CUADRO CLÍNICO Motivo de consulta: Astenia progresiva – Anemia (38%) Hiperviscosidad (31%) Adenopatías (25%) Síntomas B (23%) Sangrado (23%) Síntomas neurológicos (22%) Características clínicas: Síntomas debidos al crecimiento tumoral Síntomas debidos a la paraproteina
 Hiperviscosidad (31%) Adenopatías (25%) Síntomas B (23%) Sangrado (23%) Síntomas neurológicos (22%) Características clínicas: Síntomas debidos al crecimiento tumoral. Síntomas debidos a la paraproteina.")
13
MACROGLOBULINEMIA DE WALDENSTRÖM
CUADRO CLÍNICO INFILTRACION TUMORAL Médula ósea Ganglios Bazo M.W. Ig. M CIRCULANTE Hiperviscosidad Crioglobulinas Crioaglutininas Ig. M TISULAR Neuropatía Depósito en glomérulo renal (Sindrome nefrótico) Amiloidosis
 Amiloidosis.")
14
MACROGLOBULINEMIA DE WALDENSTRÖM
CUADRO CLÍNICO Infiltración tumoral Médula ósea → anemia leucopenia plaquetopenia Ganglios linfáticos → Adenopatías (15 a 25%) Bazo → Esplenomegalia (15%) Otros órganos
 Bazo → Esplenomegalia (15%) Otros órganos.")
15
MACROGLOBULINEMIA DE WALDENSTRÖM
CUADRO CLÍNICO Hiperviscosidad Cefaleas Confusión mental Alteraciones de la visión Epistaxis Hipertensión arterial Insuficiencia cardíaca Coma

16
Fondo de ojo de un paciente con hipervicosidad
In this slide, we see a funduscopic examination of a patient with Waldenström’s with hyperviscosity syndrome, and you can see the dilated retinal blood vessels. In fact, you can see this kind of “sausage” appearance to these retinal vessels because you have periodic smooth muscle apertures that control the blood flow and, if you distend them out, you can see that the retinal vessels actually look like sausages. Reproduced with permission from Dr. Marvin Stone. 16

17
Fondo de ojo de pacientes con hipervicosidad
The patient’s funduscopic examination of his retina showed extensive hemorrhages in the periphery along with dilated blood vessels, which are shown on the right. You can see in the center that the patient had a sizeable hemorrhage. Graphic reproduced with permission. 17

18
MACROGLOBULINEMIA DE WALDENSTRÖM
CUADRO CLÍNICO Crioglobulinas → obstrucción de pequeños vasos en zonas expuestas al frío (10%) Crioaglutininas → anemia hemolítica por anticuerpos fríos (5%)
 Crioaglutininas → anemia hemolítica por. anticuerpos fríos. (5%)")
19
Paciente con crioglobulinemia
Pre-Pheresis This is an individual whose IgM would precipitate in the extremities, under cold conditions, and block peripheral blood vessels. The patient would then develop acrocyanosis leading to the cyanotic appearance that you see here. This is an individual that we then heated and plasma pheresed. By removing the cryoglobulins, we were able to restore his perfusion. Post-Pheresis Graphic used with permission. 19

20
MACROGLOBULINEMIA DE WALDENSTRÖM
CUADRO CLÍNICO Neuropatía 22% de los pacientes La Ig. M actúa como anticuerpo contra la mielina (MAG glicoproteina anti mielina) → Polineuropatía desmielinizante Se benefician con tratamiento precoz con Rituximab
 → Polineuropatía desmielinizante. Se benefician con tratamiento precoz con Rituximab.")
21
MACROGLOBULINEMIA DE WALDENSTRÖM
TRATAMIENTO ¿Cuando? ¿Cómo?:

22
MACROGLOBULINEMIA DE WALDENSTRÖM Clasificación clínica
ASINTOMÁTICA : supervivencia ≈ a población general SINTOMÁTICA : supervivencia 5 años más corta que población general

24
Panel de consenso para iniciar tratamiento
Hb ≤ 10 g/dL por la infiltración PLT < 100,000/mm3 por infiltración Hiperviscosidad sintomática (> 4.0 cp) Neuropatía moderada a severa Crioglobulinemia sintomática, crioaglutinina sintomática, amiloidosis, u otro evento relacionado con la enfermedad cp, centipoise. Not everybody that has Waldenström’s needs to be treated. If a patient has any of these factors, it’s fair game to treat based on consensus recommendations, but otherwise watch and wait is appropriate. Kyle RA, et al. Semin Oncol. 2003;30: 24
 Neuropatía moderada a severa. Crioglobulinemia sintomática, crioaglutinina sintomática, amiloidosis, u. otro evento relacionado con la enfermedad. cp, centipoise. Not everybody that has Waldenström’s needs to be treated. If a patient has any of these factors, it’s fair game to treat based on consensus recommendations, but otherwise watch and wait is appropriate. Kyle RA, et al. Semin Oncol. 2003;30:")
25
MACROGLOBULINEMIA DE WALDENSTRÖM
TRATAMIENTO ¿Cómo?: Plasmaféresis Rituximab (anti CD 20) Rituximab + Ciclofosfamida + DXM Clorambucil Bendamustine Talidomida o Lenalidomida Bortezomid Cladribine TAMO ( sólo Jóvenes ) Alotrasplante (sólo en ptes jóvenes y dentro de un ensayo clínico)
 Rituximab + Ciclofosfamida + DXM. Clorambucil. Bendamustine. Talidomida o Lenalidomida. Bortezomid. Cladribine. TAMO ( sólo Jóvenes ) Alotrasplante (sólo en ptes jóvenes y. dentro de un ensayo clínico)")
26
MACROGLOBULINEMIA DE WALDENSTRÖM
Casos clínicos Caso n° 1: Paciente de sexo femenino,82 años. Consulta por primera vez en el año 2000 por un Proteinograma:leve hiperproteinemia ; componente M en gama rápida→Ig M de baja concentración Proteinuria fisiológica Médula ósea: normal, sin infiltración Fondo de ojo normal .

27
MACROGLOBULINEMIA DE WALDENSTRÖM
Casos clínicos Caso n° 1: 2005 → Asintomática , pero Ig M ↑ a 2,5 gr/l M.O. 25 % de infiltración 2009 → Fractura traumática de pelvis y costillas 2010 → Fractura traumática de cuello de fémur. 2011 → Leve anemia.Hematomas espontáneos. Componente M 3,5 gr/l

28
MACROGLOBULINEMIA DE WALDENSTRÖM
Casos clínicos Caso n° 2: Paciente de 48 años de sexo masculino Marzo de 2011: consulta por episodios de diarrea asociados a dolor lumbar y pérdida de 14 kg. de peso en un año Lab.: discreta anemia (hto 36 %) Eritro 93 Función renal normal LDH normal β 2 microglobulina ↑ Serologías virales negativas
 Eritro 93. Función renal normal. LDH normal. β 2 microglobulina ↑ Serologías virales negativas.")
29
MACROGLOBULINEMIA DE WALDENSTRÖM
Casos clínicos Caso n° 2: Julio 2011: continua con diarreas , dolor lumbar y se agregan edemas generalizados. > deterioro del estado general → se interna Anemia,Eritro ↑↑,> hipoalbuminemia β 2 microglobulina 17 No adenomegalias ni visceromegalia

30
MACROGLOBULINEMIA DE WALDENSTRÖM
Casos clínicos Caso n° 2: Médula Osea : PAMO y Biopsia:celularidad ┴ 25 % de infiltración por linfocitos, linfoplasmocitos y plasmocitos.Las células linfáticas son: CD 19 ++ CD CD 38 ++ las células plasmáticas son CD cadenas λ +

31
MACROGLOBULINEMIA DE WALDENSTRÖM
Casos clínicos Caso n° 2: Paciente con Componente monoclonal Ig. M Médula ósea infiltrada por linfoplasmocítos Diagnóstico: Macroglobulinemia de Waldenström

32
MACROGLOBULINEMIA DE WALDENSTRÖM
Casos clínicos Caso n° 2: Inició tratamiento con :Rituximab + Ciclofosfamida + Dexametasona Ciclos cada 21 días Cumplió 2 ciclos.Buena respuesta al tratamiento con mejoría del dolor,de las diarreas, disminución de los edemas y de la hipoalbuminemia

33
MACROGLOBULINEMIA DE WALDENSTRÖM
Casos clínicos Caso n° 2: Diarreas?→ Sindrome de mala absorción Linfoma? Amilodosis? Otra causa? VCC negativa EGC mucosa duodenal y yeyuno alteradas→Atrofia de las vellosidades,no infiltración por linfocitos patológicos,no linfangiectasias. No amiloide. Se descartó enfermedad celíaca

34
MACROGLOBULINEMIA DE WALDENSTRÖM
Casos clínicos Caso n° 2: Lumbalgia ? Rx neg RNM de columna : no lesiones osteolíticas espondiloartrosis moderada alteración de la señal de la médula ósea

35
MACROGLOBULINEMIA DE WALDENSTRÖM
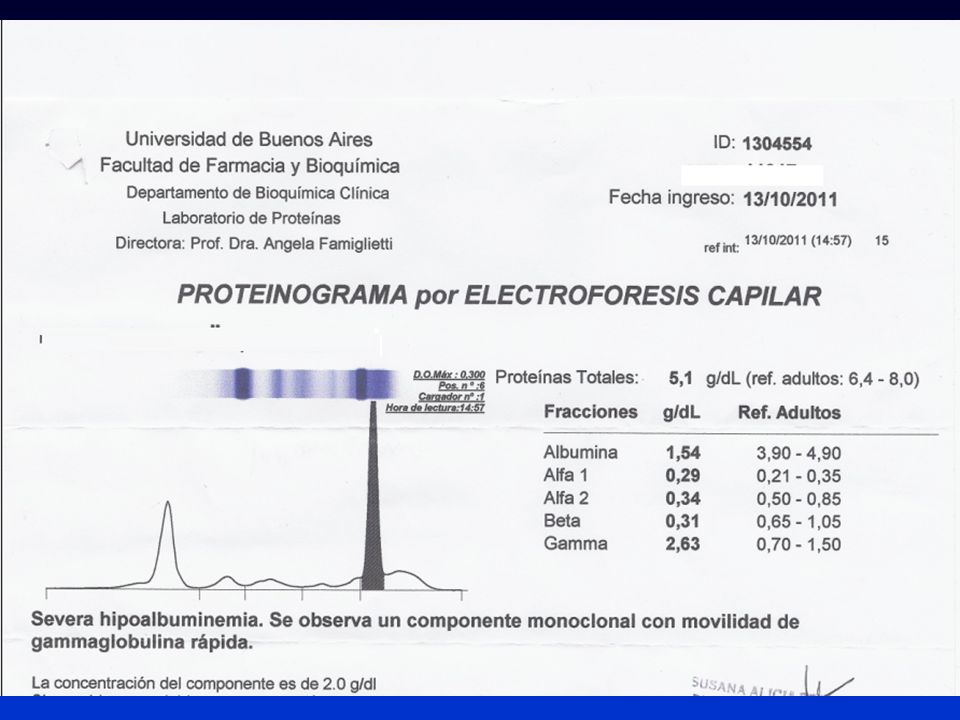
Casos clínicos Caso n° 2: Proteinograma : P.T. 7,8 gr /l Albúmina 2,8 γ glob. 3,34 comp M 2,35 Ig.M 2500 Ig A 155 Ig.G 1162 Proteinuria : 0,65 gr/ 24 hs Bence Jones + cadenas lambda

37
AMILOIDOSIS

38
AMILOIDOSIS Desorden poco frecuente que se produce por el depósito de proteína amiloide en los tejidos La proteína amiloide se caracteriza por su configuración tridimensional como estructura plegada Es resistente a la proteólisis y tiene afinidad por el rojo congo

39
AMILOIDOSIS Proteína precursora Abreviatura Clínica
Cadenas livianas de inmunoglobulinas AL Amiloidosis primaria o asociada a: Mieloma multiple Macroglobulemia secundaria Proteina A AA Procesos inflamatorios o infecciones de evolución crónica Transtiretina ATTR Senil Familiares Fibrinógeno Aα A Fib Familiar Compromiso Renal APO Lipoproteina A Aapo I Compromiso cardíaco y neuropático β2 microglobulina A β2M Diálisis Depósito osteo articular

40
AMILOIDOSIS PRIMARIA Es una neoplasia de células plasmáticas que segregan una inmunoglobulina anormal, (cadena liviana) que se deposita en varios órganos en forma de estructura β plegada y causa la disfunción de los mismos Incidencia anual: 8 casos / de habitantes Edad media: 55 años Predominio ♂ 2:1
 que se deposita en varios órganos en forma de estructura β plegada y causa la disfunción de los mismos. Incidencia anual: 8 casos / de habitantes. Edad media: 55 años. Predominio ♂ 2:1.")
41
AMILOIDOSIS PRIMARIA Cuadro clínico
Fatiga – dificultad para subir escaleras Macroglosia 10% Púrpura (periorbital) 15% Depósitos periarticulares y en estructuras submandibulares Síndrome del túnel carpiano (25%) Hipoesplenia Amiloidomas
 15% Depósitos periarticulares y en estructuras submandibulares. Síndrome del túnel carpiano (25%) Hipoesplenia. Amiloidomas.")
42
Diagnóstico diferencial
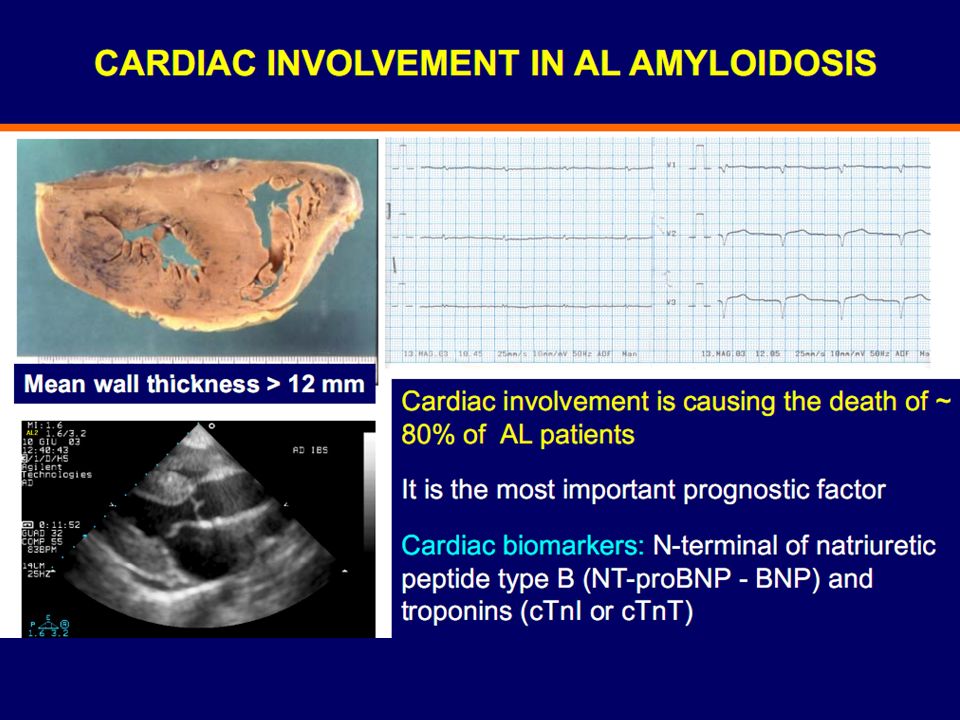
AMILOIDOSIS PRIMARIA Organo Síntoma Diagnóstico diferencial Corazón (20%) Fatiga Insuficiencia cardíaca Arritmias Isquemia Infarto agudo de miocardio Valvulopatias Hipertensión de larga data Miocardiopatia hipertrófica Ecocardiograma: Engrosamiento de las paredes y válvulas Engrosamiento del septum interventricular Birrefringencia característica Textura granular
 Fatiga. Insuficiencia cardíaca. Arritmias. Isquemia. Infarto agudo de miocardio. Valvulopatias. Hipertensión de larga data. Miocardiopatia hipertrófica. Ecocardiograma: Engrosamiento de las paredes y válvulas. Engrosamiento del septum interventricular. Birrefringencia característica. Textura granular.")
44
Diagnóstico diferencial
AMILOIDOSIS PRIMARIA Organo Síntoma Diagnóstico diferencial Riñón (30%) Síndrome nefrótico (edemas) Insuficiencia renal Glomerulopatías membrano proliferativas Glomeropatias membranosas Riñones: Biopsia renal: depósitos en mesangio y membrana basal. El grado de proteinuria no se correlaciona con el deposito de amiloide
 Síndrome nefrótico (edemas) Insuficiencia renal. Glomerulopatías membrano proliferativas. Glomeropatias membranosas. Riñones: Biopsia renal: depósitos en mesangio y membrana basal. El grado de proteinuria no se correlaciona con el deposito de amiloide.")
45
Riñon Normal vs Amiloidoisis

46
Amiloidosis Renal

47
Luz Polarizada - Birrefringencia

49
Diagnóstico diferencial
AMILOIDOSIS PRIMARIA Organo Síntoma Diagnóstico diferencial Hígado (22%) Saciedad precoz Pérdida de peso Hepatomegalia ↑ de fosfatasa alcalina Hepatitis Cirrosis biliar primaria Procesos infiltrativos hepáticos
 Saciedad precoz. Pérdida de peso. Hepatomegalia. ↑ de fosfatasa alcalina. Hepatitis. Cirrosis biliar primaria. Procesos infiltrativos hepáticos.")
50
Diagnóstico diferencial
AMILOIDOSIS PRIMARIA Organo Síntoma Diagnóstico diferencial Sistema nervioso autónomo (12%) Hipotensión ortostática Diarreas Cuadros suboclusivos Sindromes de mala absorción Cuadros gastrointestinales de otro orígen
 Hipotensión ortostática. Diarreas. Cuadros suboclusivos. Sindromes de mala. absorción. Cuadros gastrointestinales de. otro orígen.")
51
Diagnóstico diferencial
AMILOIDOSIS PRIMARIA Organo Síntoma Diagnóstico diferencial Nervios periféricos (17%) Polineuropatía sensitivo motora (comienza en miembros inferiores) Polineuropatías asociadas a M.G.U.S. Polineuropatías de otro origen
 Polineuropatía. sensitivo motora. (comienza en miembros inferiores) Polineuropatías asociadas a. M.G.U.S. Polineuropatías de otro origen.")
52
Estudios complementarios
AMILOIDOSIS PRIMARIA Estudios complementarios Componente monoclonal en suero Proteinograma 50% Inmunofijación 90% IgG 33% Cadenas Livianas 25% (80%λ) IgA 10% Cadenas livianas libres Proteinuria en rango nefrótico 30% Cadenas livianas en orina % Fosfatasa alcalina ↑ % Déficit de factor x % Trombocitosis %
 IgA 10% Cadenas livianas libres. Proteinuria en rango nefrótico 30% Cadenas livianas en orina 75% Fosfatasa alcalina ↑ 25% Déficit de factor x 10% Trombocitosis 5-10%")
53
Estudios complementarios
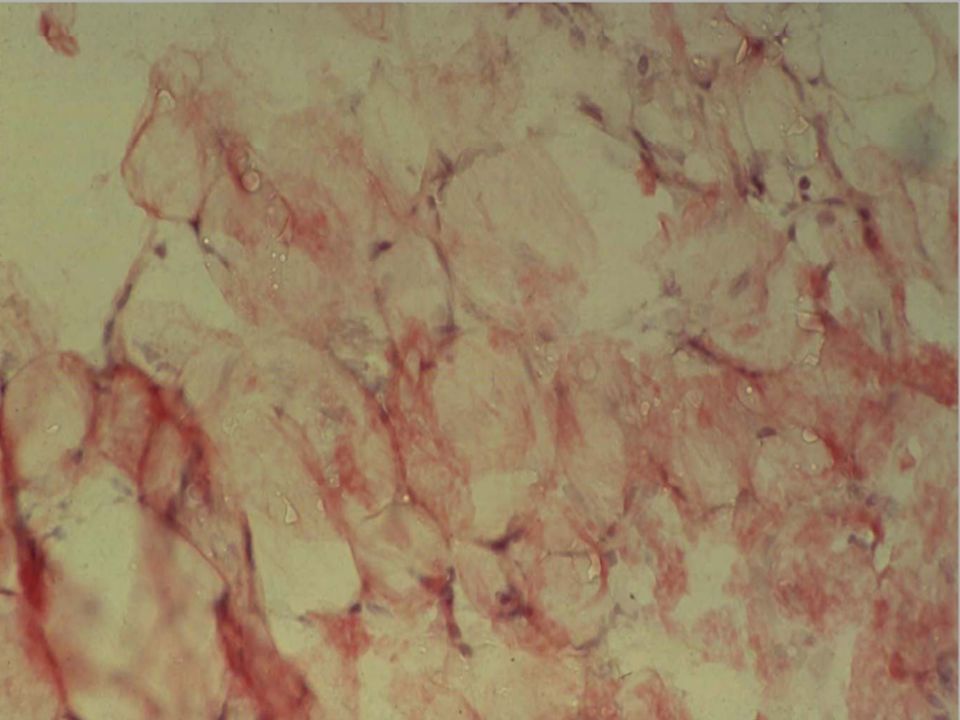
AMILOIDOSIS PRIMARIA Estudios complementarios Estudio de la médula ósea ↑ células plasmáticas < 10% Depósito amiloide (tinción Rojo Congo) Grasa subcutánea 80% Mucosa rectal 70% Médula ósea 55% Biopsia del órgano afectado Ecocardiograma
 Grasa subcutánea 80% Mucosa rectal 70% Médula ósea 55% Biopsia del órgano afectado. Ecocardiograma.")
56
BIOPSIA DE MÉDULA ÓSEA Tinción con rojo Congo

57
AMILOIDOSIS PRIMARIA Diagnóstico
De sospecha: sindrome característico + componente monoclonal sérico y/o urinario Definitivo: depósito de sustancia amiloide tipo AL en la biopsia de un tejido u órgano afectado.

58
Manifestaciones clínicas Factores pronósticos adversos
PRONOSTICO Y EVOLUCION Media de SRV global → 2 años Variable según sindrome asociado Manifestaciones clínicas SRV Insuficiencia cardíaca Hipotensión ortostática Síndrome nefrótico Polineuropatía periférica 6 meses 1 año 2 años 5 años Factores pronósticos adversos Pérdida de peso Hepatomegalia Presencia de cadenas livianas en orina Β2-microglobulina ↑ Indice proliferación celular ↑

59
ALGORITMO DIAGNOSTICO
Manifestación clínica sugestiva Biopsia MO Biopsia rectal Biopsia órgano afecto Si (-) Biopsia grasa subcutánea (tinción de Rojo Congo) + Proteinograma e IF sérica + urinaria Mielograma Familiar Secundaria Senil Si (-) Componente monoclonal Depósito cadena ligera Ig + AL
 Biopsia grasa subcutánea. (tinción de Rojo Congo) + Proteinograma e IF sérica + urinaria. Mielograma. Familiar. Secundaria. Senil. Si (-) Componente monoclonal. Depósito cadena ligera Ig. + AL.")
60
AMILOIDOSIS PRIMARIA TRATAMIENTO Melfalán – Dexametasona
Melfalán – Dexametasona – Talidomida Ciclofosfamida – Dexametasona – Talidomida Bortezomid - Dexametasona TAMO – Alternativa prometedora en pacientes < de 70 años con solo uno o dos órganos afectados Respuestas hematológicas y de órganos pero Gran morbimortalidad relacionada con el trasplante Tasa de mortalidad por el trasplante: 25 al 30%

61
Caso Clínico Paciente de 39 años, sin antecedentes clínicos relevantes
Inicia su enfermedad hace aproximadamente 4-5 meses con edemas progresivos de Miembro Inferiores Evaluada por nefrología donde se constata Síndrome Nefrótico con Proteinuria Inicial de 10.2g/24hs

62
Biopsia Renal Cilindro córtico medular que contiene hasta 15 glomérulos por corte, los mismos se hallan difusamente alterados por el deposito de un material acidófilo homogéneo en el mesangio y paredes capilares (subendotelial y subepitelial). Positivos con el Rojo Congo y Tioflavina T. Túbulos con atrofia (1%). Intersticio con fibrosis leve. En la muestra se incluye un segmento de pared arterial con leve fibrosis intimal. Algunas arteriolas presentan hipertrofia muscular y otros escasos depósitos de amiloide segmentarios. Inmunofluorescencia IgG, IgA, IgM, C1q, C3 y Fibrinógeno: Negativos. Cadenas Lambda Positivas en mesangio glomerular. Inmunohistoquimica. Proteína Amiloide A. negativa. Dco de Amiloidosis Renal Clase IV (deposito difuso mesangiocapilar).
. Positivos con el Rojo Congo y Tioflavina T. Túbulos con atrofia (1%). Intersticio con fibrosis leve. En la muestra se incluye un segmento de pared arterial con leve fibrosis intimal. Algunas arteriolas presentan hipertrofia muscular y otros escasos depósitos de amiloide segmentarios. Inmunofluorescencia IgG, IgA, IgM, C1q, C3 y Fibrinógeno: Negativos. Cadenas Lambda Positivas en mesangio glomerular. Inmunohistoquimica. Proteína Amiloide A. negativa. Dco de Amiloidosis Renal Clase IV (deposito difuso mesangiocapilar).")
63
Examen Físico se encuentra en regular estado gral, debilidad generalizada, con edemas de MMII, no impresiona hepatoesplenomegalia, no púrpura ni signos de equimosis en piel, no impronta de lengua, como así tampoco hipotensión postural, no signos de disautonomia, si refiere parestesias en extremidades a predominio de manos, también refiere alteraciones en el ritmo evacuatorios con periodos de constipación que alteran con episodios de diarrea.

64
Estudios Hto 38.7 hb 13.2, plaq , Gb (69/21/7/1/0), VSG 50 TGP/O 14/17 FAL 136 (normal) Creat 0.6, urea 29, Clearance de Creat ml/min, calcio 7.7, Fosfatemia Coagulograma normal. TP 40% Kptt 30”. Proteinograma Electroforético:P:T: 4.1/Alb.:2.12 /0.17 /0.78 /0.48 /0.55 de Gamma. Inmunofijacion Negativa. Uroproteinograma g/24hs de proteinuria glomerular de alta Selectividad. Bence Jones Negativa. Ecocardiograma: Diametros del VI conservado, Función sistólica Normal AI y RAo Normal, septum normal, no signos de Derrame pericardico. Fracción de acortamiento 44%. ECG Normal, en trazado y en la intensidad del Voltaje. Troponina T / I : Normal. BNP 758 (alterado > de 450)
, VSG 50 TGP/O 14/17 FAL 136 (normal) Creat 0.6, urea 29, Clearance de Creat ml/min, calcio 7.7, Fosfatemia 4.2. Coagulograma normal. TP 40% Kptt 30 . Proteinograma Electroforético:P:T: 4.1/Alb.:2.12 /0.17 /0.78 /0.48 /0.55 de Gamma. Inmunofijacion Negativa. Uroproteinograma g/24hs de proteinuria glomerular de alta Selectividad. Bence Jones Negativa. Ecocardiograma: Diametros del VI conservado, Función sistólica Normal AI y RAo Normal, septum normal, no signos de Derrame pericardico. Fracción de acortamiento 44%. ECG Normal, en trazado y en la intensidad del Voltaje. Troponina T / I : Normal. BNP 758 (alterado > de 450)")
65
Estudios II Ecografía Abdominal: Hígado y bazo con diámetros conservados, homogéneos. EMG de 4 Miembros: Dentro de características normales (Velocidad de Conducción Motora y Sensitiva Normal, P.U.M Normales, Fibrilaciones ausentes, patrón de Reclutamiento: interferencial).
.")
66
Estudios III Estudio de Medula Ósea:
CMF: 2% de células plasmáticas Patológicas Monoclonales cadena Lambda (citoplasmática) Expresión fuete de CD38++, CD138++. Anatomía Patologica: celularidad del 60% relación M/E conservada, se identifica un 12% de células plasmáticas siendo positivas para CD138 y cadena liviana Lambda. Se observa deposito de material amiloide (positivo con Rojo Congo y Tioflavina T/ luz polarizada) en tejido adventicial perivascular. Trama reticulinica Conservada. CTG 46 XX [15]. Dco Plasmocitosis Monoclonal / Amiloidosis.
 Expresión fuete de CD38++, CD Anatomía Patologica: celularidad del 60% relación M/E conservada, se identifica un 12% de células plasmáticas siendo positivas para CD138 y cadena liviana Lambda. Se observa deposito de material amiloide (positivo con Rojo Congo y Tioflavina T/ luz polarizada) en tejido adventicial perivascular. Trama reticulinica Conservada. CTG 46 XX [15]. Dco Plasmocitosis Monoclonal / Amiloidosis.")
67
Estudios IV Biopsia de Grasa Subcutánea: Deposito de un material acidófilo homogéneo, entre células grasas y en segmento de pared vascular, que muestra positividad con Rojo Congo y Tioflavina T. Con Diagnostico de: AMILOIDOSIS PRIMARIA SISTEMICA TIPO AL.

68
Tratamiento Inicia Tratamiento con Protocolo CTD
(Ciclofosfamida 500 mg VO días , Talidomida 100mg/día continuo; Dexametasona 40 ciclos de 4 días 1-4 y 9-12)
")
69
Evolución Luego de completar 2 ciclos de tratamiento intercurre con dos internaciones 1º con cuadro de disnea, se descarta TEP, completa tto ATB por Neumonía, 20 días posteriores 2º nuevo episodio de astenia y disnea progresiva hasta CF IV- reposo- se constata derrame pleural bilateral con franco predominio derecho casi masivo, requiere drenaje con características de trasudado, se asume como probable etiología por Insuficiencia cardiaca congestiva.

70
Evolución Debido a esta intercurrencia se asume como progresión de enfermedad sistémica. Realizando 5º ciclo de Bortezomib asociado Ciclofosfamida y dexametasona (CyBorD) . En plan de reevaluacion general, con nuevo dosaje de BNP/ProBNP., Troponina T/I, Cadenas Livianas Libres.
 . En plan de reevaluacion general, con nuevo dosaje de BNP/ProBNP., Troponina T/I, Cadenas Livianas Libres.")
71
Evolucion Se realiza Nueva Bp de Medula que evidencia dismunucion del componente amiloide. Cadenas Livianas Libre: precipitacion muy debil – Normalizacion de ProBNP Se asume como buena Respuesta Parcial se encuentra en plan de Consolidar con TAMO

72
¡MUCHAS GRACIAS! 72

165
What you can see here is that there’s absolutely no relationship between IgM and bone marrow involvement. You can have patients who have very little disease involvement but who make a lot of IgM. Many times, we have to treat these patients because they’re symptomatic from hyperviscosity because their IgM level is very high. At the other extreme, you can have patients who have a lot of disease involvement of their bone marrow but make very little IgM. For this reason, there’s no cutoff. It’s important to recognize this because you can have 2 patients that have the same IgM level but have vastly different underlying disease burden. 165

188
188

191
191

193
193

194
194

195
195

200
cp, centipoises; HA, hemagglutinin; HCT, hematocrit; PLT, platelet; Sxs, symptoms; WBC, white blood cell count. Even though this is a lymphoma, it’s very rare that you can actually see either adenopathy or splenomegaly, which only occur in about 15% of patients. Most of the disease is actually found in the bone marrow, and as a result, the patients can develop myelosuppression and require therapy. Very commonly, we have to treat patients, not because of the bulk of disease, but because of the IgM being produced; if you make too much IgM, it can lead to hyperviscosity syndrome. Roughly 90% of the IgM that we make is kept in the intravascular space because IgM is a big bulky molecule. If the IgM levels go up, it can trigger hyperviscosity levels to go up, resulting in nose bleeds, headaches, as well as impaired vision. You tend to see this happen when the patient’s IgM levels usually exceed either mg/dL or 4 centipoise. Another way patients can get into trouble is because the IgM acts as an autoantibody. Most typically, it tends to either bind the myelin sheaths of nerves, causing their destruction and resulting in a peripheral sensory neuropathy. This can occur in about 20% to 22% of patients with Waldenström’s. You can also see patients develop cryoglobulins. This is when the IgM under cold conditions can precipitate and cause blocking of peripheral blood vessels, leading to acrocyanosis. Sometimes these patients also get peripheral ulcerations. Patients can develop cold agglutinins where, under cold conditions, the IgM can bind to red blood cells, causing their destruction. We’ve even had patients who, looking at summer vs winter, can have up to a 10-percentage point difference in their hematocrit.

205
cp, centipoises; HA, hemagglutinin; HCT, hematocrit; PLT, platelet; Sxs, symptoms; WBC, white blood cell count. Even though this is a lymphoma, it’s very rare that you can actually see either adenopathy or splenomegaly, which only occur in about 15% of patients. Most of the disease is actually found in the bone marrow, and as a result, the patients can develop myelosuppression and require therapy. Very commonly, we have to treat patients, not because of the bulk of disease, but because of the IgM being produced; if you make too much IgM, it can lead to hyperviscosity syndrome. Roughly 90% of the IgM that we make is kept in the intravascular space because IgM is a big bulky molecule. If the IgM levels go up, it can trigger hyperviscosity levels to go up, resulting in nose bleeds, headaches, as well as impaired vision. You tend to see this happen when the patient’s IgM levels usually exceed either mg/dL or 4 centipoise. Another way patients can get into trouble is because the IgM acts as an autoantibody. Most typically, it tends to either bind the myelin sheaths of nerves, causing their destruction and resulting in a peripheral sensory neuropathy. This can occur in about 20% to 22% of patients with Waldenström’s. You can also see patients develop cryoglobulins. This is when the IgM under cold conditions can precipitate and cause blocking of peripheral blood vessels, leading to acrocyanosis. Sometimes these patients also get peripheral ulcerations. Patients can develop cold agglutinins where, under cold conditions, the IgM can bind to red blood cells, causing their destruction. We’ve even had patients who, looking at summer vs winter, can have up to a 10-percentage point difference in their hematocrit.

206
What you can see here is that there’s absolutely no relationship between IgM and bone marrow involvement. You can have patients who have very little disease involvement but who make a lot of IgM. Many times, we have to treat these patients because they’re symptomatic from hyperviscosity because their IgM level is very high. At the other extreme, you can have patients who have a lot of disease involvement of their bone marrow but make very little IgM. For this reason, there’s no cutoff. It’s important to recognize this because you can have 2 patients that have the same IgM level but have vastly different underlying disease burden. 206

210
This slide shows an overview of the presentation
This slide shows an overview of the presentation. The introduction will discuss the epidemiology, clinical presentation, diagnosis, and staging of myeloma and the initial approaches to treatment, including current options and novel agents and combinations. There will be a brief discussion of autologous stem cell transplantation in patients with myeloma and how to care for patients who are not transplantation eligible. 210

211
In this slide, we see a funduscopic examination of a patient with Waldenström’s with hyperviscosity syndrome, and you can see the dilated retinal blood vessels. In fact, you can see this kind of “sausage” appearance to these retinal vessels because you have periodic smooth muscle apertures that control the blood flow and, if you distend them out, you can see that the retinal vessels actually look like sausages. 211

Presentaciones similares