Descargar la presentación
La descarga está en progreso. Por favor, espere

1
ASMA Básico y actualización

2
© Global Initiative for Asthma Asthma is a heterogeneous disease, usually characterized by chronic airway inflammation. It is defined by the history of respiratory symptoms such as wheeze, shortness of breath, chest tightness and cough that vary over time and in intensity, together with variable expiratory airflow limitation. Definition of asthma NEW! GINA 2014

3
© Global Initiative for Asthma The diagnosis of asthma should be based on: A history of characteristic symptom patterns Evidence of variable airflow limitation, from bronchodilator reversibility testing or other tests Document evidence for the diagnosis in the patient’s notes, preferably before starting controller treatment It is often more difficult to confirm the diagnosis after treatment has been started Asthma is usually characterized by airway inflammation and airway hyperresponsiveness, but these are not necessary or sufficient to make the diagnosis of asthma. Diagnosis of asthma GINA 2014

4
GINA 2014, Box 1-1 © Global Initiative for Asthma NEW!

5
© Global Initiative for Asthma Confirm presence of airflow limitation Document that FEV 1 /FVC is reduced (at least once, when FEV 1 is low) FEV 1 / FVC ratio is normally >0.75 – 0.80 in healthy adults, and >0.90 in children Confirm variation in lung function is greater than in healthy individuals The greater the variation, or the more times variation is seen, the greater probability that the diagnosis is asthma Excessive bronchodilator reversibility (adults: increase in FEV 1 >12% and >200mL; children: increase >12% predicted) Excessive diurnal variability from 1-2 weeks’ twice-daily PEF monitoring (daily amplitude x 100/daily mean, averaged) Significant increase in FEV 1 or PEF after 4 weeks of controller treatment If initial testing is negative: Repeat when patient is symptomatic, or after withholding bronchodilators Refer for additional tests (especially children ≤5 years, or the elderly) Diagnosis of asthma – variable airflow limitation GINA 2014, Box 1-2
 FEV 1 / FVC ratio is normally >0.75 – 0.80 in healthy adults, and >0.90 in children Confirm variation in lung function is greater than in healthy individuals The greater the variation, or the more times variation is seen, the greater probability that the diagnosis is asthma Excessive bronchodilator reversibility (adults: increase in FEV 1 >12% and >200mL; children: increase >12% predicted) Excessive diurnal variability from 1-2 weeks’ twice-daily PEF monitoring (daily amplitude x 100/daily mean, averaged) Significant increase in FEV 1 or PEF after 4 weeks of controller treatment If initial testing is negative: Repeat when patient is symptomatic, or after withholding bronchodilators Refer for additional tests (especially children ≤5 years, or the elderly) Diagnosis of asthma – variable airflow limitation GINA 2014, Box 1-2")
6
Fuente: Harrison 17°Ed. Fisiopatología En la fisiopatología del asma bronquial se deben tener en cuenta los siguientes aspectos: inflamación bronquial, alergia y atopia e hiperrespuesta bronquial.

7
Source: Peter J. Barnes, MD Inflamación asmática-Células y mediadores

8
Formas clínicas Cursa con episodios de disnea con sibilancias, de intensidad variable, intercalados con periodos asintomáticos. Predomina en la infancia. Los episodios pueden estar relacionados con causas desencadenantes alérgicas o no alérgicas (ejercicio, exposición a tóxicos ambientales, infecciones víricas) o no mostrar relación con causas evidentes. La intensidad de las crisis son variables, pudiendo ser leves, percibidas como opresiones torácicas, o presentarse en forma de ataques de gran intensidad. Cuando la crisis es intensa el paciente experimenta sensación de dificultad respiratoria, sobre todo durante la inspiración haciéndose evidente al advertirse la utilización de los músculos auxiliares de la ventilación, por lo cual el paciente debe permanecer sentado. Suelen auscultarse abundantes roncus y sibilancias. ASMA INTERMITENTE
 o no mostrar relación con causas evidentes. La intensidad de las crisis son variables, pudiendo ser leves, percibidas como opresiones torácicas, o presentarse en forma de ataques de gran intensidad. Cuando la crisis es intensa el paciente experimenta sensación de dificultad respiratoria, sobre todo durante la inspiración haciéndose evidente al advertirse la utilización de los músculos auxiliares de la ventilación, por lo cual el paciente debe permanecer sentado. Suelen auscultarse abundantes roncus y sibilancias. ASMA INTERMITENTE.")
9
Se caracteriza por síntomas continuos en forma de tos, sibilancias y sensación disneica oscilante y variable en su intensidad. Los síntomas suelen aumentar por las noches, durante las primeras horas de la madrugada. El empleo de fármacos broncodilatadores es obligado en estos pacientes. Esta forma de presentación clínica es poco frecuente en el asma infantil y suele observarse en los asmáticos que inician la enfermedad en la edad adulta. La tos y la disnea del asma persistente suelen sufrir oscilaciones que pueden guardar relación con alguna enfermedad especifica u ocurrir sin causa aparente. Es característico que los síntomas empeoren durante las primeras horas de la madrugada. ASMA PERSISTENTE

10
En algunos asmáticos la enfermedad se presenta en forma de tos persistente, disnea de esfuerzo u opresión torácica. El diagnostico de asma atípica debe considerarse sobre todo si la tos se acompaña de sibilancias y la exploración de la función ventilatoria muestra una obstrucción bronquial reversible con un broncodilatador. ASMA ATÍPICA

11
Pruebas específicas Pruebas alérgicas cutáneas. Determinación de la IgE: Valores superiores a 100 UI/mL (240 mg/L) suelen considerarse altos. Función pulmonar: Pico Flujo (PEF) Espirometría FEV 1 FEV 1 /FVC. VEF1: Volumen Máximo Expirado en 1 segundo VCF: Volumen Total expirado VEF1/VCF: porcentaje de aire expirado en el primer segundo con respecto al total
 suelen considerarse altos. Función pulmonar: Pico Flujo (PEF) Espirometría FEV 1 FEV 1 /FVC. VEF1: Volumen Máximo Expirado en 1 segundo VCF: Volumen Total expirado VEF1/VCF: porcentaje de aire expirado en el primer segundo con respecto al total.")
12
© Global Initiative for Asthma Time (seconds) Volume Note: Each FEV 1 represents the highest of three reproducible measurements Typical spirometric tracings FEV 1 12345 Normal Asthma (after BD) Asthma (before BD) Flow Volume Normal Asthma (after BD) Asthma (before BD) GINA 2014
 Volume Note: Each FEV 1 represents the highest of three reproducible measurements Typical spirometric tracings FEV Normal Asthma (after BD) Asthma (before BD) Flow Volume Normal Asthma (after BD) Asthma (before BD) GINA 2014")
13
Hiperreactividad bronquial © Global Initiative for Asthma

14
1. Asthma control - two domains Assess symptom control over the last 4 weeks Assess risk factors for poor outcomes, including low lung function 2. Treatment issues Check inhaler technique and adherence Ask about side-effects Does the patient have a written asthma action plan? What are the patient’s attitudes and goals for their asthma? 3. Comorbidities Think of rhinosinusitis, GERD, obesity, obstructive sleep apnea, depression, anxiety These may contribute to symptoms and poor quality of life Assessment of asthma GINA 2014, Box 2-1

15
© Global Initiative for Asthma GINA assessment of asthma control GINA 2014, Box 2-2A

16
© Global Initiative for Asthma GINA assessment of asthma control GINA 2014, Box 2-2B

17
Tratamiento farmacológico BRONCODILATADORESANTIINFLAMATORIOS 0 Simpaticomiméticos β 2. 0 Teofilinas. 0 Antimuscarínicos. 0 Corticoides. 0 Cromonas. 0 Antileucotrienos.

18
Agonistas β 2 SALBUTAMOL TERBUTALINA Vía inhalatoria - inicio: 1´- peak: 15-60´ - dura: 4 a 6hs Se utilizan cuando hay síntomas y para prevención. ACCIÓN CORTA

19
SALMETEROL FORMOTEROL OLOCATEROL (dura 24Hs – NUEVO!!!) Vía inhalatoria - inicio: 3 a 10´- dura: 12 hs NO deben ser usados como monoterapia para el tratamiento del asma a largo término. Se pueden usar en combinación con corticoides inhalados para el control y prevención de síntomas en asma moderado a severo. EA: mínimos. El uso indiscriminado aumentan la inestabilidad de la enfermedad ACCIÓN LARGA Agonistas β 2

20
Metilxantinas - Teofilinas 0 La teofilina de acción sostenida es una alternativa para combinar junto a corticoides inhalados en pacientes con asma leve a moderado. 0 Podría tener un leve efecto anti-inflamatorio y se debe controlar los niveles de teofilina sérica. (ideal: 5 a 15 mg/l) 0 Vía oral o IV. 0 EA: náuseas y vómitos. Concentraciones altas de teofilina: taquicardia, arritmias, convulsiones.
 0 Vía oral o IV. 0 EA: náuseas y vómitos. Concentraciones altas de teofilina: taquicardia, arritmias, convulsiones..")
21
Antimuscarínicos (anticolinérgicos) Actúan inhibiendo los receptores muscarínicos (M1 – M3) BROMURO DE IPRATROPIO (SAMA) BROMURO DE TIOTROPIO (LAMA) GLICOPIRRONIO (LAMA) Vía inhalatoria Reduce el tono vagal intrínseco de la vía aérea Indicacion: Asma Refractaria
 Actúan inhibiendo los receptores muscarínicos (M1 – M3) BROMURO DE IPRATROPIO (SAMA) BROMURO DE TIOTROPIO (LAMA) GLICOPIRRONIO (LAMA) Vía inhalatoria Reduce el tono vagal intrínseco de la vía aérea Indicacion: Asma Refractaria")
22
Corticoides Bloquea la fase tardía de la reacción ante alérgenos, reduce la hiperrespuesta de las vías aéreas e inhibe la migración y activación de las células inflamatorias. Son los más potentes y efectivos anti- inflamatorios disponibles. Los corticoides inhalados son usados para el control del asma a largo término. Períodos cortos de corticoides vía oral son usados cuando se comienza un tratamiento a largo plazo para tener una respuesta rápida. Para los casos de asma severo se pueden usar corticoides vía oral.

23
VÍA INHALATORIA Budesonide (200mcg puff /12hs) Fluticasona (100mcg puff/12hs) Beclometasona VÍA ORAL Prednisona (40mg/d) Prednisolona (40mg/d) VÍA IV Hidrocortisona(100- 200mg) Metilprednisona (40mg) EFECTOS ADVERSOS: Inhalados: Disfonía, candidiasis VO: Alt. del eje HHS, Cushing, osteo-porosis, retardo del crecimiento

24
Modificadores de Leucotrienos Antileucotrienos: MONTELUKAST: p/ > 1 año – 10mg/d ZAFIRLUKAST: p/ > 7 años – 20mg/12hs Inhibidor de la 5 lipo-oxigenasa: *ZILEUTON: p/ > 12 años con control estricto de la función hepática. 600mg/6hs Los antileucotrienos son una alternativa para el tratamiento del asma leve persistente. Administrados VO EA: elevación de las transaminasas

25
Omalizunab (Xolair ®)(Anti-IgE) es un anticuerpo monoclonal que previene la unión de la IgE con receptores de alta afinidad de los basófilos y mastocitos. Es utilizado para el tratamiento adyuvante en > de 12 años con alergia y asma severa persistente, de difícil control. Vía SC cada 2-4 semanas $$$ ES MUY COSTOSO Inmunomoduladores (Ac monoclonar anti IgE)
.")
26
© Global Initiative for Asthma Stepwise approach to control asthma symptoms and reduce risk GINA 2014, Box 3-5 NEW!

27
© Global Initiative for Asthma Stepwise management - pharmacotherapy *For children 6-11 years, theophylline is not recommended, and preferred Step 3 is medium dose ICS **For patients prescribed BDP/formoterol or BUD/ formoterol maintenance and reliever therapy GINA 2014, Box 3-5 (upper part)
")
28
© Global Initiative for Asthma Step 1 – as-needed inhaled short-acting beta 2 -agonist (SABA) *For children 6-11 years, theophylline is not recommended, and preferred Step 3 is medium dose ICS **For patients prescribed BDP/formoterol or BUD/formoterol maintenance and reliever therapy GINA 2014, Box 3-5, Step 1
 *For children 6-11 years, theophylline is not recommended, and preferred Step 3 is medium dose ICS **For patients prescribed BDP/formoterol or BUD/formoterol maintenance and reliever therapy GINA 2014, Box 3-5, Step 1")
29
© Global Initiative for Asthma Step 2 – low-dose controller + as-needed inhaled SABA *For children 6-11 years, theophylline is not recommended, and preferred Step 3 is medium dose ICS **For patients prescribed BDP/formoterol or BUD/formoterol maintenance and reliever therapy GINA 2014, Box 3-5, Step 2

30
© Global Initiative for Asthma Step 3 – one or two controllers + as-needed inhaled reliever *For children 6-11 years, theophylline is not recommended, and preferred Step 3 is medium dose ICS **For patients prescribed BDP/formoterol or BUD/formoterol maintenance and reliever therapy GINA 2014, Box 3-5, Step 3

31
© Global Initiative for Asthma Step 4 – two or more controllers + as-needed inhaled reliever *For children 6-11 years, theophylline is not recommended, and preferred Step 3 is medium dose ICS **For patients prescribed BDP/formoterol or BUD/formoterol maintenance and reliever therapy GINA 2014, Box 3-5, Step 4

32
© Global Initiative for Asthma Step 5 – higher level care and/or add-on treatment *For children 6-11 years, theophylline is not recommended, and preferred Step 3 is medium dose ICS **For patients prescribed BDP/formoterol or BUD/formoterol maintenance and reliever therapy GINA 2014, Box 3-5, Step 5

33
© Global Initiative for Asthma How to distinguish between uncontrolled and severe asthma GINA 2014, Box 2-4 NEW!

34
© Global Initiative for Asthma Managing exacerbations in primary care GINA 2014, Box 4-3 (1/3) NEW!
 NEW!")
35
© Global Initiative for Asthma GINA 2014, Box 4-3 (2/3)
")
36
© Global Initiative for Asthma GINA 2014, Box 4-3 (3/3)
")
37
© Global Initiative for Asthma Difficulty confirming the diagnosis of asthma Symptoms suggesting chronic infection, cardiac disease etc Diagnosis unclear even after a trial of treatment Features of both asthma and COPD, if in doubt about treatment Suspected occupational asthma Refer for confirmatory testing, identification of sensitizing agent, advice about eliminating exposure, pharmacological treatment Persistent uncontrolled asthma or frequent exacerbations Uncontrolled symptoms or ongoing exacerbations or low FEV 1 despite correct inhaler technique and good adherence with Step 4 Frequent asthma-related health care visits Risk factors for asthma-related death Near-fatal exacerbation in past Anaphylaxis or confirmed food allergy with asthma Indications for considering referral, where available GINA 2014, Box 3-10 (1/2)
")
38
“BRONQUITIS” ASMATICA/BRONQUIOLITIS

39
Exp

40
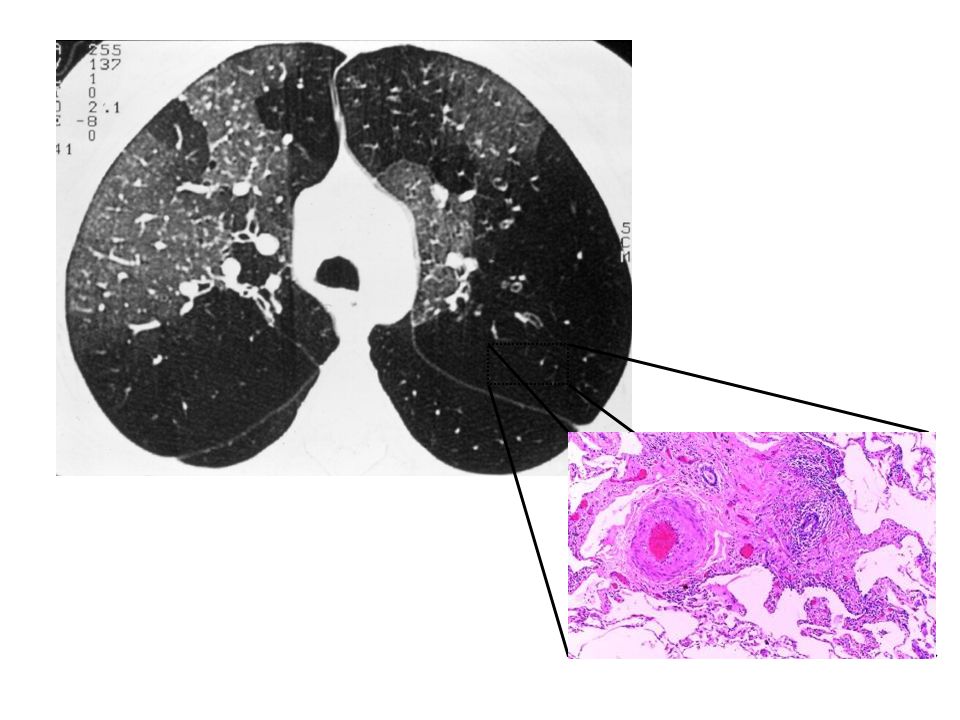
Bronquiolitis Obliterante

Presentaciones similares