Descargar la presentación
La descarga está en progreso. Por favor, espere

1
DRA MONSE IP LESLY CARRILLO
ASMA

3
VEF1 < 80% Consideramos un FEV1 como normal cuando se encuentra en o por encima del 80% de este valor de referencia. Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760

4
VEF1 < 80%

5
halación de un broncodilatador, beta-2 agonista de acción corta
halación de un broncodilatador, beta-2 agonista de acción corta. Se recomienda la utilización de 400 microg. de salbutamol. Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760

6
Mejoría >20% Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760

7
flujo espiratorio máximo)
PEF (Peak Flow Meter) Con mejoría de L/min) > 20% pre-broncodilatador.
 Con mejoría de 60 L/min) > 20% pre-broncodilatador.")
8
DEFINICIÓN Enfermedad inflamatoria crónica de las vías aéreas, la cual existe obstrucción parcial o totalmente reversible, acompañada de HRB. Esta visión del asma tiene implicancias en el diagnóstico y el tratamiento Asma es una enfermedad inflamatoria crónica que afecta a las vías respiratorias periféricas, participando fundamentalmente las células cebadas y los eosinófilos, provocando un estado de hiperreactividad bronquial que se manifiesta, luego de los estímulos provocadores, como un estado de broncoespasmo, el cual es reversible y autolimitado Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760

9
SINTOMAS se asocia a hiperreactividad bronquial (HRB) con episodios recurrentes de: sibilancias Disnea opresión torácica Tos improductiva TOS: MADRUGADA Y NOCHE Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760

10
(20-30min) activación de los
FISIOPATOLOGÍA INFLAMACIÓN: ( hipersensibilidad tipo 1 e IgE) descamación del epitelio de la vía aérea depósitos de colágeno debajo de la membrana basal edema (20-30min) activación de los mastocitos (6-10 hrs después) linfocitos Th2. infiltración de células inflamatorias (neutrófilos, eosinófilos y linfocitos TH2). Eosinófilos. la importancia de la cronicidad (remodelación de la vía aérea) Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760
 descamación del epitelio de la vía aérea. depósitos de colágeno debajo de la membrana basal. edema. (20-30min) activación de los. mastocitos. (6-10 hrs después) linfocitos Th2. infiltración de células inflamatorias (neutrófilos, eosinófilos y linfocitos TH2). Eosinófilos. la importancia de la cronicidad. (remodelación de la vía aérea) Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760.")
11
Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760 CONTROL DEL ASMA El 40% de los niños asmáticos alcanzan un adecuado control de su enfermedad. Se considera no control a la presencia de sintomatología por lo menos 4 veces en 2 semanas o bien manifestaciones nocturnas por lo menos en 2 ocasiones en un mes. Los pacientes con control subóptimo que además no recurren a la medicación de rescate, por lo menos 6 días de la semana son considerados como submedicados. Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760

12
Evaluación del control
Se revisaron 754 niños asmáticos. 63% mostraban buen control. el 48% usaban adecuadamente la medicación de rescate. El 62% de los padres los consideraban controlados. 12% de los padres no coincidían entre si en relación con el control logrado. 35% de los padres consideraban a sus hijos como "intermitentes", sin reconocer la condición crónica alcanzada. 22% de los padres consideraron síntomas dos veces por semana como con buen control. Un control suboptimo fue reportado en el 51% de los chicos hispanos 37% de los niños negros 32% de los niños blancos Solo el 38% de los padres señalaron que se les había indicado que buscaran implementar medidas de control. Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760 Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760

13
DIFERENCIALES fibrosis quística inmunodeficiencia
a partir de los 6 a 7 años, ya pueden aplicarse las definiciones fisiopatológicas más estrictas de los consensos generales

14
índice clínico predictivo de asma de Castro-Rodriguez
aleatoriamente 285 niños con riesgo de asma tratamiento preventivo con un corticoesteroide 2veces al día x dos años o un placebo. (no hubo diferencia entre los grupos) 3er año de estudio: no incluía tratamiento. 4to año, la atención de los niños sólo fue ofrecida por sus propios médicos. Por consiguiente, el tratamiento varió y reflejó lo que sucede en la práctica clínica de la vida real. Estudio PECK 1999 (prevención del asma precoz en los niños) Resultado 2007: "Los corticoesteroides inhalados controlan, pero no previenen, el asma". Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760
 3er año de estudio: no incluía tratamiento. 4to año, la atención de los niños sólo fue ofrecida por sus propios médicos. Por consiguiente, el tratamiento varió y reflejó lo que sucede en la práctica clínica de la vida real. Estudio PECK 1999 (prevención del asma precoz en los niños) Resultado 2007: Los corticoesteroides inhalados controlan, pero no previenen, el asma . Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760.")
15
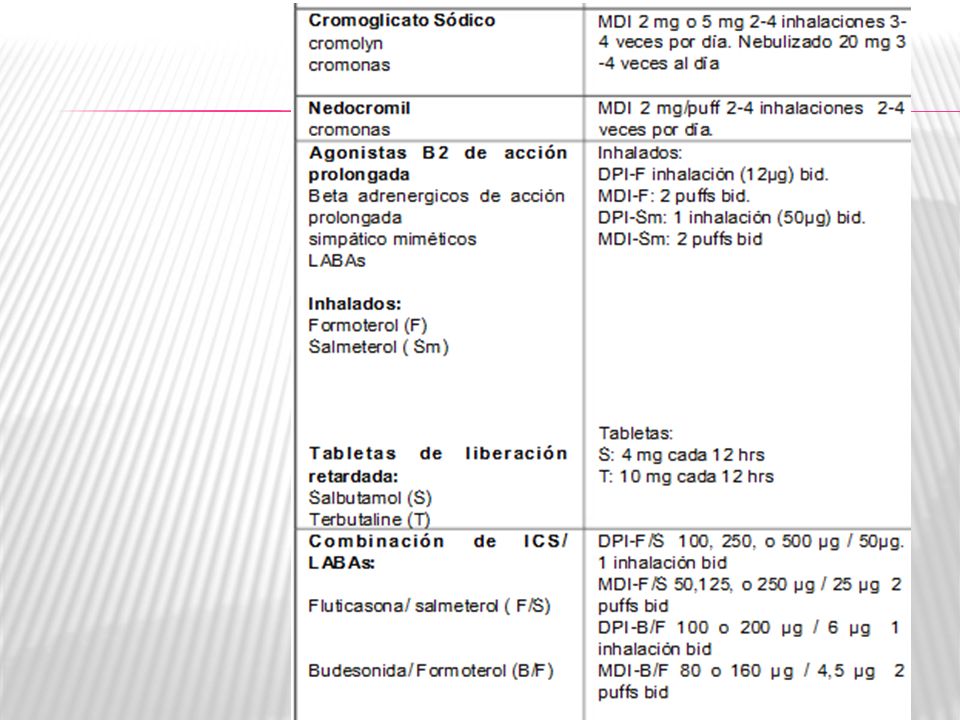
Tratamiento del asma ß2 agonistas Esteroides Anticolinérgicos
F L M O R S B R O N C D I L A T E S Tratamiento del asma ß2 agonistas Esteroides De acción corta Inhalados De acción larga Orales Parenterales Anticolinérgicos Antileucotrienos Xantinas Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760 15

16
ASMA EN PEDIATRIA los factores desencadenantes
(ejercicio físico, virus, alérgenos, rinitis o el sobrepeso) respuesta al tratamiento farmacológico y su cumplimiento Proceso de desarrollo pulmonar, la inmadurez del sistema inmune y el tamaño de sus vías aéreas El asma infantil presenta características propias que lo diferencian del asma en el adulto y que permiten establecer diferenciaciones entre los propios niños asmáticos. Entre ellas se encuentra la historial natural de la enfermedad, la edad del niño, Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760
 respuesta al tratamiento farmacológico y su cumplimiento. Proceso de desarrollo pulmonar, la inmadurez del sistema inmune y el tamaño de sus vías aéreas. El asma infantil presenta características propias que lo diferencian del asma en el adulto y que permiten establecer diferenciaciones entre los propios niños asmáticos. Entre ellas se encuentra la historial natural de la enfermedad, la edad del niño, Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760.")
17
CLASIFICACIÓN

18
CLASIFICACION DEL ASMA
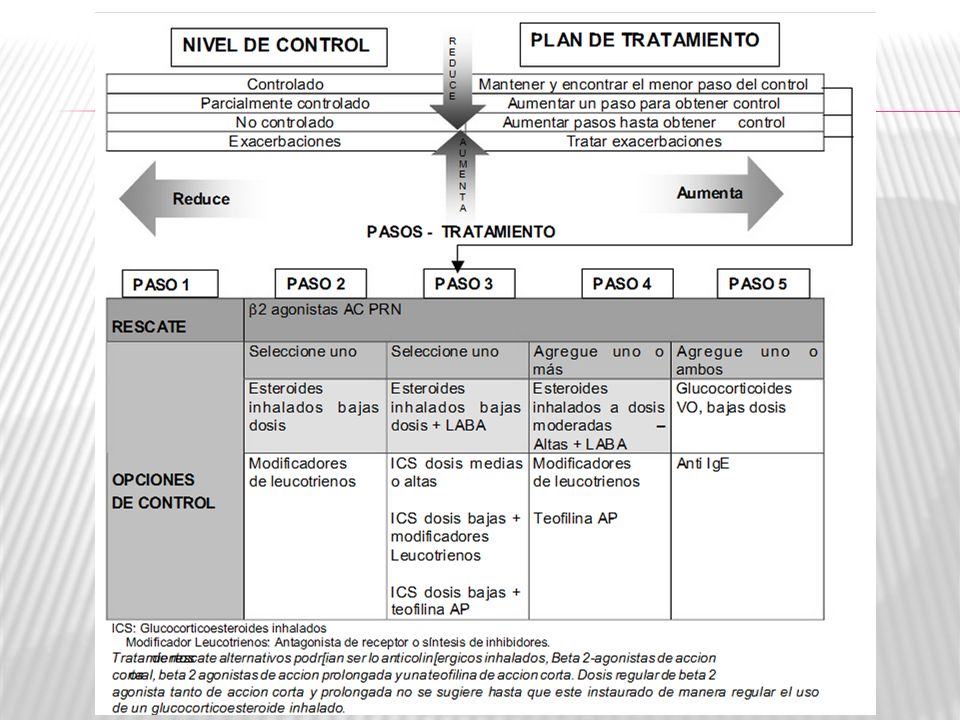
NIVEL DE CONTROL ACCION DE TRATAMIENTO Controlado Mantener el esquema y encontrar la dosis mas simple Parcialmente Controlado Considerar subir de paso para ganar control No controlado Pasos hacia arriba hasta obtener control Exacerbaciones Tratar como exacerbación Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760

21
rescate

22
De control

27
… y los menores de 5 años?

28
la European Academy of Allergology and Clinical Immunology (EAACI) y la American Academy of Allergy Athsma and Immunology (AAAAI). 28 Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760

29
PRACTALL Asma: enfermedad crónica más común de la niñez en paises industrializados La medicina basada en evidencia es limitada en asma pediátrica. Su historia natural es variable. Múltiples desencadenantes Fenotipos/fisiopatología específica de la edad Sin guías pediátricas exclusivas PRACTALL EAACI / AAAAI Consensus Report Bacharier LB, et al. Allergy. 2008;63(1):5–34 Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760
:5–34. Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760.")
30
PRACTALL Diagnóstico sospechado en lactantes basado en observación de sibilancias recurrentes y episodios de tos, en donde la evaluación a largo plazo será necesaria para confirmar el diagnóstico. PRACTALL EAACI / AAAAI Consensus Report Bacharier LB, et al. Allergy. 2008;63(1):5–34. 30 Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760
:5– Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760.")
31
PRACTALL SIBILANTE TRANSITORIO
Silban los primeros 2-3 años pero NO después de los 3 años. SIBILANTE NO ATOPICO Desencadenado por infecciones virales, remite posteriormente. ASMA PERSISTENTE Sibilancias asociadas con manifestaciones de atopia (eczema, rinitis y conjuntivitis alérgica, alergia a alimentos) eosonofília en sangre e IgE Elevada. Sensibilización mediada por IgE especifica a alimentos y posteriormente a alérgenos inhalantes comunes. Sensibilización a inhalantes antes de los 3 años, especialmente a alérgenos perennes intradomiciliarios. Historia de asma en los padres. SIBILANTE INTERMITENTE GRAVE Pocos episodios agudos asociado con morbilidad mínima fuera del tiempo de enfermedad del aparato respiratorio. Características atópicas como eczema, sensibilización alérgica, y eosinofília periférica. Siempre debemos de manejar diagnosticos diferenciales de asma, y estar pendientes de la historia de patrones de sibilancias recurrentes. Allergy Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760 31
 eosonofília en sangre e IgE Elevada. Sensibilización mediada por IgE especifica a alimentos y posteriormente a alérgenos inhalantes comunes. Sensibilización a inhalantes antes de los 3 años, especialmente a alérgenos perennes intradomiciliarios. Historia de asma en los padres. SIBILANTE INTERMITENTE GRAVE. Pocos episodios agudos asociado con morbilidad mínima fuera del tiempo de enfermedad del aparato respiratorio. Características atópicas como eczema, sensibilización alérgica, y eosinofília periférica. Siempre debemos de manejar diagnosticos diferenciales de asma, y estar pendientes de la historia de patrones de sibilancias recurrentes. Allergy Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:")
32
Tratamiento Farmacólogico (Niños <2 Años)
PRACTALL EAACI / AAAAI Consensus Report Tratamiento Farmacólogico (Niños <2 Años) Ref 1, p 18, C1, Box 1 Diagnóstico de Asma : >3 episodios de obstrucción bronquial reversible en un período de 6 meses β2-agonistas intermitentes Primera opción a pesar de evidencia conflictiva LTRA Terapia de control diario para sibilancias desencadenadas por virus (tratamiento a corto o largo plazo) corticosteroides nebulizados o inhalados Terapia de control diario para asma persistentea Primera línea de tratamiento cuando hay evidencia de atópia/alergia corticosteroides oralesb Episodios de obstrucción agudos y recurrentes The Pediatric Consensus Report notes that the diagnosis and treatment of asthma in patients 0 to 2 years of age pose the greatest challenges due to the limited availability of clinical evidence.1 For example, there is no clear basis for determining how frequent a child’s obstructive episodes should be before the decision is made to initiate continuous therapy with an ICS or LTRA.1 The consensus report recommends that a diagnosis of asthma be considered in a child 2 years of age or younger who has had more than 3 documented episodes of reversible bronchial obstruction within a period of 6 months.1 For these children, intermittent therapy with a β2-agonist is recommended as first-line therapy despite conflicting evidence. In Europe, this therapy would be administered orally, whereas in the United States, therapy would be administered as inhalation therapy via jet nebulizers.1 An LTRA can be used as daily controller therapy on either a long- or short- term basis for children 2 years of age or younger who have viral wheezing.1 Nebulized corticosteroids or ICS therapy delivered via metered-dose inhalers with spacers are recommended as daily controller therapy in these young patients who have persistent asthma. This is particularly relevant in cases of severe disease or those that require frequent use of oral corticosteroids. Evidence of atopy and allergy in these cases should lower the decision threshold for the use of ICS, which may be considered for first-line therapy.1 Oral corticosteroids, such as prednisone 1 to 2 mg/kg/day for 3 to 5 days, may be appropriate in children 2 years of age or younger who experience acute and frequently recurrent obstructive episodes.1 Ref 1, p 17, C2, ¶4 , L1-3 Ref 1, p 17, C2, ¶4 , L8-12 Ref 1, p 18, C1, Box 1, Bullet 1 Ref 1, p 18, C1, Box 1, Bullet 2 Ref 1, p 18, C1, Box 1, Bullet 3 Ref 1, p 18, C1, Box 1, Bullets 4,5 Ref 1, p 18, C1, Box 1, Bullet 6 b, 1 a 2 mg/kg/día de prednisona de 3 a 5 días durante fase de obstrucción aguda que se presente frecuente recurrentemente. Bacharier LB, et al. Allergy. 2008;63(1):5–34. 32 Reference Bacharier LB, Boner A, Carlsen K-H, et al; the European Pediatric Asthma Group. Diagnosis and treatment of asthma in childhood: a PRACTALL consensus report. Allergy. 2008;63(1):5–34. Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760
 Ref 1, p 18, C1, Box 1. Diagnóstico de Asma : >3 episodios de obstrucción bronquial reversible en un período de 6 meses. β2-agonistas intermitentes. Primera opción a pesar de evidencia conflictiva. LTRA. Terapia de control diario para sibilancias desencadenadas por virus (tratamiento a corto o largo plazo) corticosteroides nebulizados o inhalados. Terapia de control diario para asma persistentea. Primera línea de tratamiento cuando hay evidencia de atópia/alergia. corticosteroides oralesb. Episodios de obstrucción agudos y recurrentes. The Pediatric Consensus Report notes that the diagnosis and treatment of asthma in patients 0 to 2 years of age pose the greatest challenges due to the limited availability of clinical evidence.1 For example, there is no clear basis for determining how frequent a child’s obstructive episodes should be before the decision is made to initiate continuous therapy with an ICS or LTRA.1. The consensus report recommends that a diagnosis of asthma be considered in a child 2 years of age or younger who has had more than 3 documented episodes of reversible bronchial obstruction within a period of 6 months.1. For these children, intermittent therapy with a β2-agonist is recommended as first-line therapy despite conflicting evidence. In Europe, this therapy would be administered orally, whereas in the United States, therapy would be administered as inhalation therapy via jet nebulizers.1. An LTRA can be used as daily controller therapy on either a long- or short- term basis for children 2 years of age or younger who have viral wheezing.1. Nebulized corticosteroids or ICS therapy delivered via metered-dose inhalers with spacers are recommended as daily controller therapy in these young patients who have persistent asthma. This is particularly relevant in cases of severe disease or those that require frequent use of oral corticosteroids. Evidence of atopy and allergy in these cases should lower the decision threshold for the use of ICS, which may be considered for first-line therapy.1. Oral corticosteroids, such as prednisone 1 to 2 mg/kg/day for 3 to 5 days, may be appropriate in children 2 years of age or younger who experience acute and frequently recurrent obstructive episodes.1. Ref 1, p 17, C2, ¶4 , L1-3. Ref 1, p 17, C2, ¶4 , L8-12. Ref 1, p 18, C1, Box 1, Bullet 1. Ref 1, p 18, C1, Box 1, Bullet 2. Ref 1, p 18, C1, Box 1, Bullet 3. Ref 1, p 18, C1, Box 1, Bullets 4,5. Ref 1, p 18, C1, Box 1, Bullet 6. b, 1 a 2 mg/kg/día de prednisona de 3 a 5 días durante fase de obstrucción aguda que se presente frecuente recurrentemente. Bacharier LB, et al. Allergy. 2008;63(1):5– Reference. Bacharier LB, Boner A, Carlsen K-H, et al; the European Pediatric Asthma Group. Diagnosis and treatment of asthma in childhood: a PRACTALL consensus report. Allergy. 2008;63(1):5–34. Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760.")
33
PRACTALL Tratamiento Farmacólogico (Niños >2 Años)
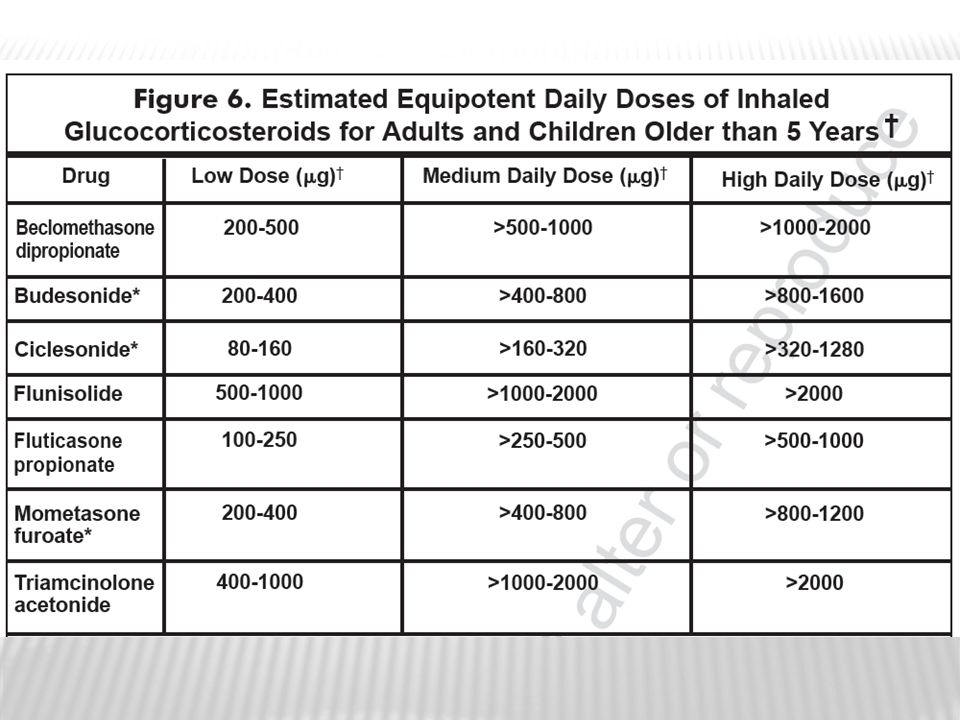
CSI (200 µg BDP o equivalente) O LTRAa (Dosis dependiente de edad) Ref 1, p 15, C1, Fig 3 Bajar en caso apropiado CONTROL INSUFICIENTEb Incrementar dosis de CSI (400 µg BDP o equivalente) O Adicionar a CSI un LTRA Un paso arriba para conseguir el control CONTROL INSUFICIENTEc Ref 1, p 15, C1, Fig 3 Ref 1, p 15, C2, ¶4, ICS, Bullets 1,3,5; ¶5, LTRA Bullet 1, C1, Fig 3; p 16, C1, Bullet 2 Ref 1, p 16, C1, Bullet 8 Bajar en caso apropiado The approach to pharmacologic treatment of asthma recommended for children older than 2 years of age in the Pediatric Consensus Report is summarized in this slide. The approach is based on first-line therapies followed by a series of step-ups to more-intensive therapy to overcome insufficient control and step-downs to less-intensive therapy, if appropriate.1 First-line controller therapy may involve either an inhaled corticosteroid (ICS), at a dose of 200 µg of beclomethasone dipropionate equivalent, or a leukotriene receptor antagonist (LTRA) at an age-dependent dose in pediatric patients with persistent asthma. An LTRA may be an especially appropriate choice in patients with concomitant asthma and rhinitis.1 Evidence of insufficient control with first-line therapy should prompt the treating physician to ask the patient, parent, and/or caregivers about compliance with prescribed therapy and allergen avoidance, and to reevaluate the patient’s diagnosis of asthma.1 For pediatric patients confirmed to have uncontrolled asthma, the ICS dose could be doubled or an ICS could be added to LTRA therapy. Continued failure to achieve asthma control should prompt the physician to ask again about compliance issues and consider referring the patient to a specialist. Therapeutic options at this point include doubling the ICS dose again, adding an LTRA to ICS therapy, or adding a long-acting 2- agonist (LABA).1 Safety concerns with LABAs have been raised recently, suggesting that their use should be restricted to add-on therapy to ICS when indicated.1 Subsequent failure to achieve asthma control in pediatric patients may necessitate the use of theophylline or oral corticosteroids.1 Incrementar dosis de CSI (800 µg BDP o equivalente) O Adicionar LTRA a CSI Adicionar LABA CONTROL INSUFICIENTEc Considerar otras opciones Teofilina Corticoides orales aLTRA son particularmente útiles si el paciente tiene rinitis concomitante; bRevisar apego al tratamiento, control ambiental y reevaluar el diagnóstico; cRevisar apego al tratamiento y considerar referrir al especialista. CSI=corticosteroides inhalados; LTRA=antagonistas del receptor de leucotrienos; BDP=Dipropionato de beclometasona; LABA=Agonista β2-de acción prolongada. Bacharier LB, et al. Allergy. 2008;63(1):5–34. 33 Reference Bacharier LB, Boner A, Carlsen K-H, et al; the European Pediatric Asthma Group. Diagnosis and treatment of asthma in childhood: a PRACTALL consensus report. Allergy. 2008;63(1):5–34. Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760
 O. LTRAa. (Dosis dependiente de edad) Ref 1, p 15, C1, Fig 3. Bajar en caso apropiado. CONTROL INSUFICIENTEb. Incrementar dosis de CSI (400 µg BDP o equivalente) O. Adicionar a CSI un LTRA. Un paso arriba para conseguir el. control. CONTROL INSUFICIENTEc. Ref 1, p 15, C1, Fig 3. Ref 1, p 15, C2, ¶4, ICS, Bullets 1,3,5; ¶5, LTRA Bullet 1, C1, Fig 3; p 16, C1, Bullet 2. Ref 1, p 16, C1, Bullet 8. Bajar en caso apropiado. The approach to pharmacologic treatment of asthma recommended for children older than 2 years of age in the Pediatric Consensus Report is summarized in this slide. The approach is based on first-line therapies followed by a series of step-ups to more-intensive therapy to overcome insufficient control and step-downs to less-intensive therapy, if appropriate.1. First-line controller therapy may involve either an inhaled corticosteroid (ICS), at a dose of 200 µg of beclomethasone dipropionate equivalent, or a leukotriene receptor antagonist (LTRA) at an age-dependent dose in pediatric patients with persistent asthma. An LTRA may be an especially appropriate choice in patients with concomitant asthma and rhinitis.1. Evidence of insufficient control with first-line therapy should prompt the treating physician to ask the patient, parent, and/or caregivers about compliance with prescribed therapy and allergen avoidance, and to reevaluate the patient’s diagnosis of asthma.1. For pediatric patients confirmed to have uncontrolled asthma, the ICS dose could be doubled or an ICS could be added to LTRA therapy. Continued failure to achieve asthma control should prompt the physician to ask again about compliance issues and consider referring the patient to a specialist. Therapeutic options at this point include doubling the ICS dose again, adding an LTRA to ICS therapy, or adding a long-acting 2- agonist (LABA).1. Safety concerns with LABAs have been raised recently, suggesting that their use should be restricted to add-on therapy to ICS when indicated.1. Subsequent failure to achieve asthma control in pediatric patients may necessitate the use of theophylline or oral corticosteroids.1. Incrementar dosis de CSI (800 µg BDP o equivalente) O. Adicionar LTRA a CSI. Adicionar LABA. CONTROL INSUFICIENTEc. Considerar otras opciones. Teofilina. Corticoides orales. aLTRA son particularmente útiles si el paciente tiene rinitis concomitante; bRevisar apego al tratamiento, control ambiental y reevaluar el diagnóstico; cRevisar apego al tratamiento y considerar referrir al especialista. CSI=corticosteroides inhalados; LTRA=antagonistas del receptor de leucotrienos; BDP=Dipropionato de beclometasona; LABA=Agonista β2-de acción prolongada. Bacharier LB, et al. Allergy. 2008;63(1):5– Reference. Bacharier LB, Boner A, Carlsen K-H, et al; the European Pediatric Asthma Group. Diagnosis and treatment of asthma in childhood: a PRACTALL consensus report. Allergy. 2008;63(1):5–34. Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760.")
34
PRACTALL Identificación del Tipo de Asma
Ref 1, p 9, Fig 2 Fenotipo de Asma en Niños >2 Años de edad ¿El paciente está completamente bien entre los episodios de síntomas? Sí No ¿Es el ejercicio el desencadenante más comun o el único factor precipitante? ¿Las gripes son el factor desencadenante más comun? Various asthma phenotypes can be defined on the basis of the child’s age and asthma triggers. Recognition of these different phenotypes and disease severity can help provide better direction for prognosis and therapeutic strategies.1 This slide summarizes an approach to determining asthma phenotypes in children older than 2 years of age. In this approach, the initial question is based on whether the child is completely well between symptomatic periods.1 If the child is well beween such periods, possible phenotypes are virus-induced asthma and exercise-induced asthma, depending on the precipitating factors. For either of these phenotypes, the possibility that the child may also be atopic must be explored.1 The child who is not completely well between symptomatic periods and does not meet the criteria for virus- or exercise-induced asthma may have clinically relevant allergic sensitization. In this case, the child may have allergen-induced asthma or unresolved asthma. In the latter case, different etiologies, including irritant exposure and as-yet not evident allergies, may need to be considered.1 Among preschool children 3 to 5 years of age, persistence of asthma symptoms during the year can be a key differentiator of asthma phenotype. Since viruses are the most common trigger in these children, viral-induced asthma is an appropriate diagnosis among these patients whose symptoms disappear completely between episodes and usually recur following a cold. The phenotype of exercise-induced asthma can also be observed in this age group.1 Tests for the presence of specific immunoglobin E (IgE) antibodies, such as skin prick or in vitro tests, should be performed to obtain information that may supplement clinical information regarding a relationship between exposure to a potential allergen and the occurrence of asthma symptoms. Findings of such antibodies are consistent with the phenotype of allergen-induced asthma. The Pediatric Consensus Report emphasized that atopy is a risk factor for the persistence of asthma, regardless of any observation that allergens are or are not obvious triggers of disease activity in an individual child. The absence of a specific allergic trigger may indicate a phenotype of nonallergic asthma. The clinician should consider this phenotype with caution, however, since the failure to identify an allergic trigger may reflect the fact that a specific allergic trigger was not detected.1 Among school-age children 6 to 12 years of age, the differentiators of asthma phenotypes are identical to those in younger children; however, the clinician should consider that cases of allergen- induced asthma are more common and visible in the older children, and seasonality may be a more evident factor. Finally, virus-induced asthma should also be considered in these children since it is still common.1 ¿El paciente tiene sensibilización alérgica clínicamente relevante? Ref 1, p 8, C2, ¶6, L1-4; p 9, C1, L1-3 Ref 1, p 9, Fig 2 Ref 1, p 9, C1, ¶3, L1-4, C2, L1-4, Fig 2 Ref 1, p 9, C2, ¶1, L1-12 Ref 1, p 9, C2, ¶2, L1-7 No No Sí Sí Sí No Asma inducida por virusa Asma inducida por Ejercicioa Asma inducida por Alergenos Asma no resueltaa,b aLos niños pueden ser atópicos. bDiferentes Etiologías, incluyendo exposición a irritantes y no tiene alergias evidentes, puede incluirse aquí. PRACTALL EAACI / AAAAI Consensus Report Bacharier LB, et al. Allergy. 2008;63(1):5–34. 34 Reference Bacharier LB, Boner A, Carlsen K-H, et al; the European Pediatric Asthma Group. Diagnosis and treatment of asthma in childhood: a PRACTALL consensus report. Allergy. 2008;63(1):5–34. Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760
 antibodies, such as skin prick or in vitro tests, should be performed to obtain information that may supplement clinical information regarding a relationship between exposure to a potential allergen and the occurrence of asthma symptoms. Findings of such antibodies are consistent with the phenotype of allergen-induced asthma. The Pediatric Consensus Report emphasized that atopy is a risk factor for the persistence of asthma, regardless of any observation that allergens are or are not obvious triggers of disease activity in an individual child. The absence of a specific allergic trigger may indicate a phenotype of nonallergic asthma. The clinician should consider this phenotype with caution, however, since the failure to identify an allergic trigger may reflect the fact that a specific allergic trigger was not detected.1. Among school-age children 6 to 12 years of age, the differentiators of asthma phenotypes are identical to those in younger children; however, the clinician should consider that cases of allergen- induced asthma are more common and visible in the older children, and seasonality may be a more evident factor. Finally, virus-induced asthma should also be considered in these children since it is still common.1. ¿El paciente tiene sensibilización alérgica clínicamente relevante Ref 1, p 8, C2, ¶6, L1-4; p 9, C1, L1-3. Ref 1, p 9, Fig 2. Ref 1, p 9, C1, ¶3, L1-4, C2, L1-4, Fig 2. Ref 1, p 9, C2, ¶1, L1-12. Ref 1, p 9, C2, ¶2, L1-7. No. No. Sí. Sí. Sí. No. Asma inducida por virusa. Asma inducida por Ejercicioa. Asma inducida por Alergenos. Asma no resueltaa,b. aLos niños pueden ser atópicos. bDiferentes Etiologías, incluyendo exposición a irritantes y no tiene alergias evidentes, puede incluirse aquí. PRACTALL EAACI / AAAAI Consensus Report. Bacharier LB, et al. Allergy. 2008;63(1):5– Reference. Bacharier LB, Boner A, Carlsen K-H, et al; the European Pediatric Asthma Group. Diagnosis and treatment of asthma in childhood: a PRACTALL consensus report. Allergy. 2008;63(1):5–34. Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760.")
35
PRACTALL Conclusiones
Ref 1, p 8, C2, ¶6; p 10, Bullet 2 Ref 1, p 13, C2, ¶4 Ref 1, p 20, C1, Bullet 1 Ref 1, p 15, Fig 3, C2, LTRA, Bullet 1, ICS, Bullet 1 Ref 1, p 20, C1, Bullet 2 Ref 1, p 21, C1, Bullet 6 Identificar el fenotipo de asma. El manejo incluye control ambiental y educación. Tratamiento de la inflamación de la vía aérea que conlleve al control óptimo. CSI y LTRAs están recomendados como terapia controladora inicial. Hasta que tengamos disponible nueva evidencia de la efectividad y seguridad a largo plazo, los AAP no deben ser utilizados sin CSI. La Inmunoterapia en conjunto con el control ambiental y farmacoterapia. In summary, the Pediatric Consensus Report provides specific recommendations for management of asthma in childhood. Fundamentally, comprehensive asthma management in children must feature avoidance measures, pharmacotherapy, and education. Identification of asthma phenotype should be attempted, including evaluation of atopic status.1 Because asthma symptoms most often occur in the setting of inflammation, the guidelines recommend that the main goal of controller therapy should be to reduce bronchial inflammation. In fact, treatment of airway inflammation is needed to achieve optimal asthma control. ICS and LTRAs are recommended first-line treatments for persistent asthma. LTRAs are also recommended first-line treatment in mild asthma. LABAs should not be used without an appropriate dose of ICS until further evidence of effectiveness and long-term safety becomes available.1 Immunotherapy may be appropriate for selected patients.1 Ref 1, p 13, C2, ¶5 (Management), L1-5; p 10, C1, Bullet 2 Ref 1, p 10, C1, last ¶, L1-4; p 15, C2, ¶3, L1,2; p 20, C1, Bullet 1 Ref 1, p 13, C2, ¶5 (Management), L5,6 PRACTALL EAACI / AAAAI Consensus Report Bacharier LB, et al. Allergy. 2008;63(1):5–34. 35 Reference Bacharier LB, Boner A, Carlsen K-H, et al; the European Pediatric Asthma Group. Diagnosis and treatment of asthma in childhood: a PRACTALL consensus report. Allergy. 2008;63(1):5–34. Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760
, L1-5; p 10, C1, Bullet 2. Ref 1, p 10, C1, last ¶, L1-4; p 15, C2, ¶3, L1,2; p 20, C1, Bullet 1. Ref 1, p 13, C2, ¶5 (Management), L5,6. PRACTALL EAACI / AAAAI Consensus Report. Bacharier LB, et al. Allergy. 2008;63(1):5– Reference. Bacharier LB, Boner A, Carlsen K-H, et al; the European Pediatric Asthma Group. Diagnosis and treatment of asthma in childhood: a PRACTALL consensus report. Allergy. 2008;63(1):5–34. Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760.")
36
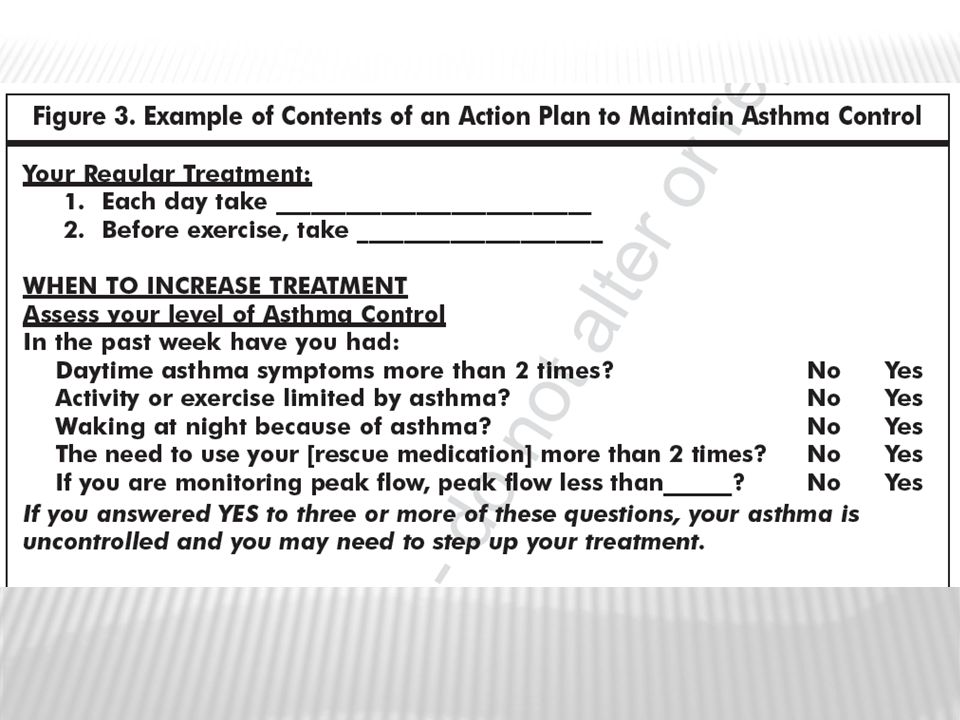
POST PRACTALL Los objetivos principales del tratamiento del asma consisten en Alcanzar y mantener el control de los síntomas. Mantener actividades normales, incluso el ejercicio, Mantener la función pulmonar lo más próximo a lo normal Prevenir las exacerbaciones del asma. Evitar los efectos nocivos de los medicamentos. Prevenir la mortalidad por asma. Guía de Práctica Clínica Para el Diagnóstico y Tratamiento de Asma. Enero de 2008 Dr. Martín Becerril Angeles Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760

37
POST PRACTALL Antileucotrienos
Los antileucotrienos son una alternativa para pacientes con reacciones adversas por esteroides inhalados o incapaces de usarlos, y en aquellos con rinitis alérgica asociada En los menores de 5 años con asma intermitente los antileucotrienos pueden disminuir las crisis asmáticas inducidas por virus En niños mayores de 5 años con esteroides inhalados en dosis bajas y asma mal controlada agregar antileucotrienos produce una mejoría clínica moderada y reduce las exacerbaciones Guía de Práctica Clínica Para el Diagnóstico y Tratamiento de Asma. Enero de 2008 Dr. Martín Becerril Angeles Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760

38
POST PRACTALL Varios meta-análisis han demostrado que la adición de un LABA es más efectiva que aumentar la dosis de los ICS, en cuanto a la mejoría en el control del asma y reducción en exacerbaciones. Los pacientes que recibieron tratamiento combinado utilizaron poca medicacion de rescate y tuvieron mayor adherencia En el caso ICS como monoterapia, la reducción de dosis puede resultar en pérdida del control del asma Adicionar salmeterol mejora la sintomatología, pero a expensas de incrementar los riesgos de presentar eventos adversos medicamentosos. (palpitaciones, temblor, cefalea y calambres musculares) John Oppenheimer y Harold S. Nelson, Seguridad de los ß-agonistas de larga duración en el asma: una revisión Curr Opin Pulm Med 2008, 14:64-69 Delea TE, et al. Effects of fluticasone propionate/salmeterol combination on asthma-related health care resource utilization and costs and adherence in children and adults with asthma. Clin Ther Mar;30(3): Cates C, Cates M "Regular treatment with salmeterol for chronic asthma: serious adverse events" Cochrane Database of Systematic Reviews 2008 Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760
 John Oppenheimer y Harold S. Nelson, Seguridad de los ß-agonistas de larga duración en el asma: una revisión Curr Opin Pulm Med 2008, 14: Delea TE, et al. Effects of fluticasone propionate/salmeterol combination on asthma-related health care resource utilization and costs and adherence in children and adults with asthma. Clin Ther Mar;30(3): Cates C, Cates M Regular treatment with salmeterol for chronic asthma: serious adverse events Cochrane Database of Systematic Reviews Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760.")
39
GINA 2010 En menores de 4 años se propone inhalador presurizado de ICS con dosis medida, con espaciador con mascarilla. En los mayores de 4 años se prefiere el espaciador con boquilla En caso de decidirse por la presentación nebulizada se prefiere hacerlo con mascarilla Global Strategy for the Diagnosis and Management of Asthma in Children 5 years and Youngers 2010 Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760

40
GINA 2010 Prácticamente no hay estudios en menores de 4 años
El tratamiento NUNCA por menos de tres (3) meses Global Strategy for the Diagnosis and Management of Asthma in Children 5 years and Youngers 2010 Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760
 meses. Global Strategy for the Diagnosis and Management of Asthma in Children 5 years and Youngers Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760.")
41
GINA 201o De no lograrse el control con esteroides inhalados se doblará la dosis del esteroide, aunque otra opción es adicionar antileucotrienos Pobre control obliga a considerar otros diagnósticos o el empleo de teofilinas o de esteroides orales Descontrol hará pensar en virus o en alergia respiratoria Global Strategy for the Diagnosis and Management of Asthma in Children 5 years and Youngers 2010 Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760

42
GINA 2010 Agitación, astenia y confusión durante una exacerbación harán pensar en hipoxemia La severidad se manifiesta como taquicardia, cianosis o marcada hipoventilación Global Strategy for the Diagnosis and Management of Asthma in Children 5 years and Youngers 2010 Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760

43
GINA 2009 Se considera de difícil control y requiere manejo hospitalario la falta de respuesta a tres dosis de un rescatador, taquipnea sin respuesta al broncodilatador, disnea continua, cianosis, tiraje y/o desaturación por debajo de 92% Global Strategy for the Diagnosis and Management of Asthma in Children 5 years and Youngers 2009 Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760

44
GINA 2009 El asma de difícil control se maneja con oxigenoterapia, beta dos agonista de acción rápida como rescatador, ipratropio, esteroides sistémicos y aminofilina Preferentemente en UCI Global Strategy for the Diagnosis and Management of Asthma in Children 5 years and Youngers 2009 Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760

45
ATS 2009 La inflamación se incrementa por infección viral (clínica o latente) y eso produce resistencia a los esteroides La inflamación explica la exacerbación y la remodelación. El tabaquismo pasivo incrementa la respuesta inflamatoria E. Bel Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760

46
ATS 2009 Existe un mecanismo molecular complejo en la presencia del asma, sin saber si cada fenotipo tiene un mecanismo diferente y sin saber si esto se asocia con la manifestación clínica de la enfermedad En todos los casos hay respuesta a los broncodilatadores P. WOODRUFF Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760

47
ATS 2009 La diferencia celular de los diferentes fenotipos parece localizarse en eosinofilos y neutrofilos No eosinofilos= resistencia a esteroides Eosinofilos= mayor riesgo a casos severos I. PAVORD Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760

48
Bibliografía-

49
GRACIAS. Smith LA et al, Modifiable Risk Factors for Suboptimal Control and Controller Medication underuse among Children with asthma Pediatrics 2008, 122:760 49

Presentaciones similares