Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Osteomielits Y Artritis Séptica
Dra. Alejandra Soriano

2
OSTEOMIELITIS

3
DEFINICIÓN Proceso inflamatorio asociado a destrucción ósea y causado por un microorganismo infeccioso. OM puede ser local o generalizada. Puede comprometer la médula y corteza ósea, periostio y tejido blando adyacente. OMA: días y/o semanas OMC: meses (incluso años)
")
4
EPIDEMIOLOGÍA FRECUENCIA - En USA: 1/ 5000 niños <13 años (c/año).
- Internacional : > OMC en países en vías de desarrollo por poco acceso a servicios de salud. - Etnia: > en niños afroamericanos. - Sexo: 2,5 H / 1 M - Edad: 50 % niños pre-escolares

5
PATOGENIA EN OSTEOMIELITIS
Vía hematógena Foco contiguo de infxn Herida penetrante Traumatismo Isquemia HUESO > SUSCEPTIBILIDAD Cuerpos Extraños Exposición Ósea Infección Ósea “El Involucro o Hueso Nuevo” (Absc. Subperióstico o de tejs blandos; forma hueso nuevo alrededor del secuestro) FAGOCITOS Pus Bacterias penetran y se adhieren a osteoblastos (película protectora rica en polisacáridos) Liberación enzimas Cronicidad de Infxn Lisis ósea “Secuestro o Hueso Muerto” (necrosis isq. Ósea que separa fragmentos desvascularizados)
 FAGOCITOS. Pus. Bacterias penetran y. se adhieren a osteoblastos. (película protectora rica. en polisacáridos) Liberación enzimas. Cronicidad de Infxn. Lisis ósea. Secuestro o Hueso Muerto (necrosis isq. Ósea que separa fragmentos desvascularizados)")
6
Agentes Causales Desarrollo de OM depende del microorganismo y de factores del huésped Causas 1) Staphylococcus aureus: + frecuente (70-90%). 2) Streptococcus agalactie 3) Streptococcus pneumoniae 4) Streptococcus pyogenes: 10% de O.M.H, historia de infxn por varicela, fiebre, leucocitosis. 5) BGN y SGB son más frecuentes en RN 6) Pseudomona aeruginosa: Herida penetrante (zuela de zapatos) en el pie. Causes: Staphylococcus aureus is the most common pathogen, followed by Streptococcus pneumoniae and Streptococcus pyogenes. Community-associated methicillin-resistant S aureus has also become an increasing problem recently (and is the most common cause in many regions). Gram-negative bacteria and group B streptococci frequently are seen in newborns. Pseudomonas aeruginosa often is associated with osteomyelitis and osteochondritis following penetrating wounds of the foot through a tennis shoe. Immunocompromised children are prone to infection with a variety of fungi and bacteria. Bony lesions due to Bartonella henselae (cause of catscratch disease) have also been reported. Salmonella is an important cause of osteomyelitis in children with sickle cell disease and other hemoglobinopathies. Kingella kingae, a fastidious gram-negative rod, is increasingly recognized as a cause of osteoarticular infections, particularly in the first 2 years of life and following a respiratory tract infection. Anaerobes: Bacteroides, Fusobacterium, Clostridium, and Peptostreptococcus are rare causes
 Streptococcus agalactie. 3) Streptococcus pneumoniae. 4) Streptococcus pyogenes: 10% de O.M.H, historia de infxn por varicela, fiebre, leucocitosis. 5) BGN y SGB son más frecuentes en RN. 6) Pseudomona aeruginosa: Herida penetrante. (zuela de zapatos) en el pie. Causes: Staphylococcus aureus is the most common pathogen, followed by Streptococcus pneumoniae and Streptococcus pyogenes. Community-associated methicillin-resistant S aureus has also become an increasing problem recently (and is the most common cause in many regions). Gram-negative bacteria and group B streptococci frequently are seen in newborns. Pseudomonas aeruginosa often is associated with osteomyelitis and osteochondritis following penetrating wounds of the foot through a tennis shoe. Immunocompromised children are prone to infection with a variety of fungi and bacteria. Bony lesions due to Bartonella henselae (cause of catscratch disease) have also been reported. Salmonella is an important cause of osteomyelitis in children with sickle cell disease and other hemoglobinopathies. Kingella kingae, a fastidious gram-negative rod, is increasingly recognized as a cause of osteoarticular infections, particularly in the first 2 years of life and following a respiratory tract infection. Anaerobes: Bacteroides, Fusobacterium, Clostridium, and Peptostreptococcus are rare causes.")
7
Agentes Causales 7) Niños Inmunodeprimidos: gran variedad de hongos y bacterias. 8) Bartonella henselae: en niños muy delgados con arañazo de gato. 9) Salmonella: Drepanocíticos y Hemoglobinopatías 10) Kingella kingae: Fastidioso GN, < 2 años de vida y asociado a IVRS, estomatitis 11) Anaerobios (raros): Bacteroides, Fusobacterium, Clostridium, Peptostreptococcus Asociado con mordeduras, mastoiditis, sinusitis crónica o infección dental. Causes: Staphylococcus aureus is the most common pathogen, followed by Streptococcus pneumoniae and Streptococcus pyogenes. Community-associated methicillin-resistant S aureus has also become an increasing problem recently (and is the most common cause in many regions). Gram-negative bacteria and group B streptococci frequently are seen in newborns. Pseudomonas aeruginosa often is associated with osteomyelitis and osteochondritis following penetrating wounds of the foot through a tennis shoe. Immunocompromised children are prone to infection with a variety of fungi and bacteria. Bony lesions due to Bartonella henselae (cause of catscratch disease) have also been reported. Salmonella is an important cause of osteomyelitis in children with sickle cell disease and other hemoglobinopathies. Kingella kingae, a fastidious gram-negative rod, is increasingly recognized as a cause of osteoarticular infections, particularly in the first 2 years of life and following a respiratory tract infection. Anaerobes: Bacteroides, Fusobacterium, Clostridium, and Peptostreptococcus are rare causes
 Bartonella henselae: en niños muy delgados con arañazo de gato. 9) Salmonella: Drepanocíticos y Hemoglobinopatías. 10) Kingella kingae: Fastidioso GN, < 2 años de vida y asociado a IVRS, estomatitis. 11) Anaerobios (raros): Bacteroides, Fusobacterium, Clostridium, Peptostreptococcus. Asociado con mordeduras, mastoiditis, sinusitis crónica o infección dental. Causes: Staphylococcus aureus is the most common pathogen, followed by Streptococcus pneumoniae and Streptococcus pyogenes. Community-associated methicillin-resistant S aureus has also become an increasing problem recently (and is the most common cause in many regions). Gram-negative bacteria and group B streptococci frequently are seen in newborns. Pseudomonas aeruginosa often is associated with osteomyelitis and osteochondritis following penetrating wounds of the foot through a tennis shoe. Immunocompromised children are prone to infection with a variety of fungi and bacteria. Bony lesions due to Bartonella henselae (cause of catscratch disease) have also been reported. Salmonella is an important cause of osteomyelitis in children with sickle cell disease and other hemoglobinopathies. Kingella kingae, a fastidious gram-negative rod, is increasingly recognized as a cause of osteoarticular infections, particularly in the first 2 years of life and following a respiratory tract infection. Anaerobes: Bacteroides, Fusobacterium, Clostridium, and Peptostreptococcus are rare causes.")
8
Agentes Causales De Acuerdo Con La Edad

9
Factores De Riesgo de OM y Sus Agentes Causales

10
Huesos Largos son los más afectados en pediatría

11
CLASIFICACIÓN DE LA OSTEOMIELITIS

12
CLASIFICACIÓN DE LA O.M.A
Hay 3 tipos diferentes: OM Hematógena (O.M.H) OM Asociada a Foco Contiguo de Infxn OM Secundaria a Insuf. Vascular
 OM Asociada a Foco Contiguo de Infxn. OM Secundaria a Insuf. Vascular.")
13
OM HEMATÓGENA (Patogenia)
Origen a partir de bacteremia sintomática y/o asintomática Metáfisis: inicia infxn Inflamación y Replicación local en cortocircuitos AV Pus ↑ Presión Intracapilar

14
OM HEMATÓGENA (Clínica)
> niños con síntomas en primeras 2 sem Dolor agudo, persistente y progresivo sobre hueso afectado Fiebre Edema + eritema en zona circunscrita a hueso Limitación a la movilidad de articulación OM con cultivos positivos (en relac. con cultivos negativos) : antecedentes de trauma, celulitis, fiebre
 : antecedentes de trauma, celulitis, fiebre.")
15
OM HEMATÓGENA (Clínica)
Neonatos .Poco frecuente .S. aureus, BEGN, SGB .Infección severa 50% (múltiples huesos, tejidos y articulaciones adyacentes) .Factores predisponentes: sitios de catéteres, electrodos en cuero cabelludo, punciones. .Pseudoparálisis puede ser único síntoma .Irritabilidad, fiebre, edema, eritema (poco eviedentes) .Dx tardió por signos inespecíficos Osteomyelitis in a neonate is an uncommon but serious infection. It often results from hematogenous spread of microorganisms in patients with indwelling venous catheters. Presenting signs and symptoms include fever, irritability, refusal to move the affected limb, and redness and swelling over the affected area. Diagnosis may be delayed because of nonspecific signs of illness. Infection involving multiple bones and contiguous joints and soft tissue is common. Neonatal osteomyelitis S aureus, enteric gram-negative bacilli (eg, Escherichia coli, Klebsiella species), and group B streptococci are common pathogens. IV sites, scalp electrodes, and puncture wounds are often predisposing factors. Diagnosis may be delayed because swelling and erythema may not be evident at onset. Decreased movement (pseudoparalysis) of the affected area may be the only symptom. As many as 50% of affected newborns may have multiple bone involvement. Associated arthritis is also common. Unlike radiographic findings in older children, plain radiographs of newborns often have a lytic area at the time of diagnosis. Perform a complete evaluation for serious bacterial infection before initiating empirical treatment with antibiotics (eg, nafcillin and gentamicin, nafcillin and cefotaxime). A significant number of patients develop permanent sequelae due to involvement of the adjacent joint and damage to the cartilaginous growth plate.
 .Factores predisponentes: sitios de catéteres, electrodos en cuero. cabelludo, punciones. .Pseudoparálisis puede ser único síntoma. .Irritabilidad, fiebre, edema, eritema (poco eviedentes) .Dx tardió por signos inespecíficos. Osteomyelitis in a neonate is an uncommon but serious infection. It often. results from hematogenous spread of microorganisms in patients with indwelling. venous catheters. Presenting signs and symptoms include fever, irritability, refusal to move the affected limb, and redness and swelling over the affected. area. Diagnosis may be delayed because of nonspecific signs of illness. Infection. involving multiple bones and contiguous joints and soft tissue is common. Neonatal osteomyelitis. S aureus, enteric gram-negative bacilli (eg, Escherichia coli, Klebsiella species), and group B streptococci are common pathogens. IV sites, scalp electrodes, and puncture wounds are often predisposing factors. Diagnosis may be delayed because swelling and erythema may not be evident at onset. Decreased movement (pseudoparalysis) of the affected area may be the only symptom. As many as 50% of affected newborns may have multiple bone involvement. Associated arthritis is also common. Unlike radiographic findings in older children, plain radiographs of newborns often have a lytic area at the time of diagnosis. Perform a complete evaluation for serious bacterial infection before initiating empirical treatment with antibiotics (eg, nafcillin and gentamicin, nafcillin and cefotaxime). A significant number of patients develop permanent sequelae due to involvement of the adjacent joint and damage to the cartilaginous growth plate.")
16
OM HEMATÓGENA (Clínica)
Lactante .Irritabilidad .Posición antiálgica de miembro afectado .Celulitis .Fiebre

17
OM HEMATÓGENA (Clínica)
Niños Mayores .OM pélvica en 1-11% .Dolor pélvico, lumbalgia, dolor abdominal .Limitación a la movilización de cadera, incapacidad para apoyar peso de extremidad .Dolor exquisito localizado .Periostio + denso y corteza ósea + gruesa = infx local. Pelvic osteomyelitis is reported in 1% to 11% of all cases of acute hematogenous osteomyelitis and typically affects older children [13]. Symptoms include hip, buttock, low back, or abdominal pain. Fever may be absent. Findings on physical examination include tenderness of the pelvic bones, pain with hip movement, decreased range of motion at the hip, and refusal or inability to bear weight. Any bone in the pelvis may be involved, but the ilium tends to be affected most often, presumably because of its rich blood supply. Symptoms and findings frequently are nonspecific and poorly localized and often are attributed to other diagnoses, such as pyogenic arthritis of the hip or appendicitis. Establishing the correct diagnosis often is delayed.

18
DIAGNÓSTICO DE O.M.A Clínica + Laboratorio + Rx Leucocitosis (50%)
VES ↑ (80-90%): 3-5 días inicio síntomas (Elevado hasta 3-4 semanas post-tx) PCR ↑ (98%): 48 hrs inicio de síntomas (Normaliza 7-10 post-tx) The diagnosis of osteomyelitis depends primarily on clinical findings and corroborative laboratory and radiographic results. The WBC count may be normal or increased. Erythrocyte sedimentation rate (ESR) is elevated in 80% to 90% of cases, and C-reactive protein (CRP) is elevated in 98% of cases. ESR generally peaks 3 to 5 days after admission, and CRP peaks within 48 hours of admission. CRP typically returns to normal 7 to 10 days after appropriate therapy. ESR may remain elevated for 3 or 4 weeks, even with appropriate therapy [14]. Patients who require surgical incision and drainage procedures may have prolonged time to normalization of ESR or CRP
: 3-5 días inicio síntomas. (Elevado hasta 3-4 semanas post-tx) PCR ↑ (98%): 48 hrs inicio de síntomas. (Normaliza 7-10 post-tx) The diagnosis of osteomyelitis depends primarily on clinical findings and. corroborative laboratory and radiographic results. The WBC count may be normal. or increased. Erythrocyte sedimentation rate (ESR) is elevated in 80% to. 90% of cases, and C-reactive protein (CRP) is elevated in 98% of cases. ESR. generally peaks 3 to 5 days after admission, and CRP peaks within 48 hours of. admission. CRP typically returns to normal 7 to 10 days after appropriate therapy. ESR may remain elevated for 3 or 4 weeks, even with appropriate therapy [14]. Patients who require surgical incision and drainage procedures may have prolonged. time to normalization of ESR or CRP.")
19
DIAGNÓSTICO DE O.M.A Se debe establecer el agente causal
Cultivo (–) que NO responde a Tx se debe realizar biopsia de tej. Óseo S. aureus
 que NO. responde a Tx se. debe realizar biopsia. de tej. Óseo. S. aureus.")
20
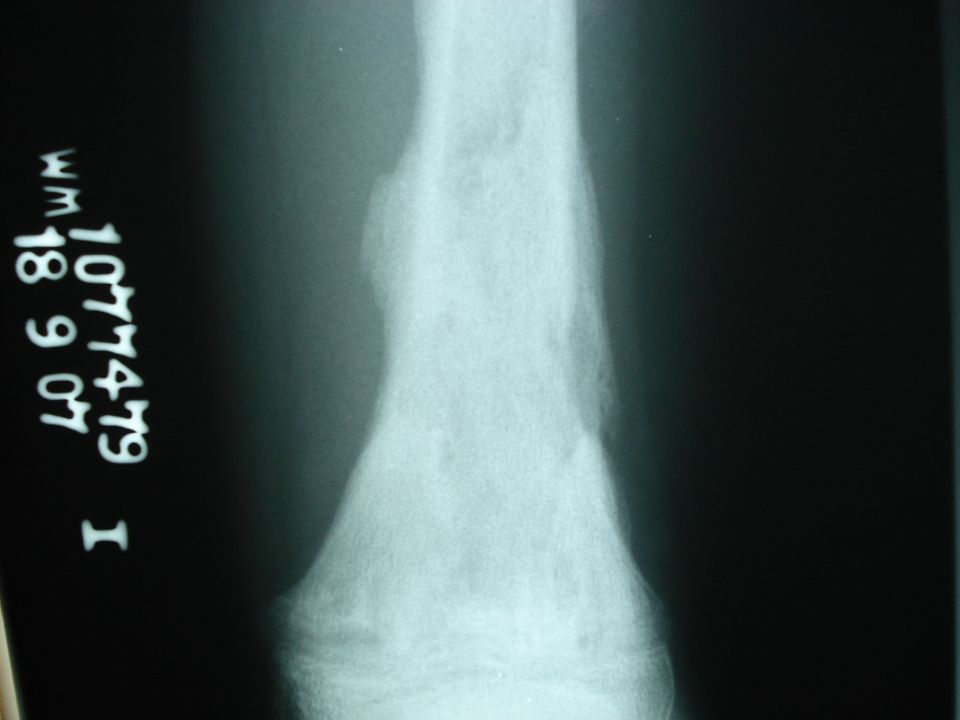
DIAGNÓSTICO DE O.M.A Radiografía
Rx simple: edema de tejs. blandos, útil para detectar tumores óseos, fracturas y evolución de fracturas. Signos radiológicos tardíos días post inicio Sx (destrxn ósea) .Osteopenia, lesiones líticas, y cambios periósticos. .Ausencia de éstos NO excluye OMA
 .Osteopenia, lesiones líticas, y cambios periósticos. .Ausencia de éstos NO excluye OMA.")
26
Medicina Nuclear

28
DIAGNÓSTICO DE O.M.A Ultrasonido
De utilidad en diagnóstico temprano de O.M.A o de colecciones purulentas en tejs. Blandos

29
DIAGNÓSTICO DE O.M.A Gammagrafía ósea trifásica con Tc-99m
Sensibilidad % 20% de Falsos negativos en primeros días de enfermedad Demuestra ↑ activ. Osteoblástica Distingue OM-celulitis profunda Tumores óseos, fracturas, artritis, cirugía pueden ↑ activ. Osteoblástica también

30
DIAGNÓSTICO DE O.M.A RMN Indicac. principales: gamma óseo (-), sospecha de OM vertebral o pélvica Gran utilidad para visualizar abscesos en tejs. Blandos asociados con OM, edema de Méd. Ósea y destrucción ósea. Mejor resolución espacial que gamma óseo. Examen de elección si se va a drenar un absceso Limitaciones: requiere sedación, alto costo, incapacidad de valorar si otros huesos están afectados. MR imaging gives excellent resolution of bone and soft tissue. It is particularly useful for visualizing soft tissue abscess associated with osteomyelitis, bone marrow edema, and bone destruction. Contrast enhancement with gadolinium is used to look for areas of abscess formation [18]. If pelvic or vertebral body osteomyelitis is suspected, MR imaging is the imaging study of choice. MR imaging gives better spatial resolution than bone scan and is preferred if a surgical procedure to diagnose or drain an abscess is necessary. Limitations of MR imaging include the need for sedation in younger children, high cost, and inability to assess easily whether other bones are affected.

31
DIAGNÓSTICO DIFERENCIALES
LLA LMA Mordeduras de Animales Artritis Séptica Enf. Del Arañazo de gato Síndrome de niño agredido Sarcoma de Ewing Tumores neuroectod. primitivos Enf. De Gaucher Gonorrea Infección por Hib Neuroblastoma Osteosarcoma Poliarteritis Nodosa

32
TRATAMIENTO DE O.M.A

33
TRATAMIENTO DE O.M.A Éxito del tx depende de: Tx empírico:
.Selección, administración y curso adecuados del ATB .Identificar el agente causal .Iniciar tx temprano con base en patógenos + frec. .Intervención qx cuando sea necesaria Tx empírico: .Depende de: Edad del niño,Historia y valoración clínica .Debe haber cobertura contra S. aureus .En OM no complicadas

34
TRATAMIENTO EMPÍRICO DE O.M.A
Lactantes de 0-2 meses .Cubrir contra: S. aureus, S. agalactie, BEGN Niños 2 meses – 5 años .Cubrir contra: S. aureus, S. pneumoniae, S. pyogenes, *K. kingae y Hib (si inmunización incompleta) *Se ha reportado resistencia a Clindamicina y Clotrimazole
 *Se ha reportado resistencia a Clindamicina y Clotrimazole.")
35
TRATAMIENTO EMPÍRICO DE O.M.A
ATB anti-estafilocóccicos: Nafcicilina, Vancomicina, Clindamicina, Cefazolina Hib: cefas 3ª generac. + clindamicina

36
TRATAMIENTO DE O.M.A SEGÚN AGENTE CAUSAL ESPECÍFICO
Se inicia Antibioticoterapia de acuerdo con agente causal y sensibilidad a ATB del mismo. Si cultivo (-), pero hay mejoría con tx empírico, éste se continúa. Si cultivo (-) y no mejoría con tx empírico: .Replantear dx .Biopsia de tej. Óseo .Otro cultivo .RMN
, pero hay mejoría con tx empírico, éste se continúa. Si cultivo (-) y no mejoría con tx empírico: .Replantear dx. .Biopsia de tej. Óseo. .Otro cultivo. .RMN.")
37
TRATAMIENTO DE O.M.A CONTRA MRSA
Infxs por MRSA en aumento Varios *CA-MRSA son susceptibles a Clindamicina Considerar Vancomicina como alternativa a clindamicina para Tx empírico en quienes habitan en sitios propensos a CA-MRSA Otros ATB (IV) alternativos: vancomicina, TMX-sulfa, linezolid Infection caused by MRSA is increasingly common in many communities. Many isolates of CA-MRSA are susceptible to clindamycin. Isolates of S. aureus that are erythromycin resistant and clindamycin susceptible should be evaluated for the presence of inducible macrolide-lincosamide-streptogramin B (MLSB) resistance. This evaluation is done by means of a ‘‘D’’ test, performed by many hospital laboratories. Although some children treated with clindamycin for an infection with MRSA of the MLSB phenotype clear their infection, it is recommended that in the setting of serious infection, clindamycin should not be used if this phenotype is identified. Alternative drugs to consider for treatment of osteomyelitis caused by MRSA include intravenous vancomycin, trimethoprim-sulfamethoxasole, and linezolid. Bone and joint infections caused by MRSA should be managed in consultationwith an expert in infectious disease. Empirical use of these antibiotics before organism identification and susceptibility testing depends on severity of illness and incidence of MRSA in the community. *S. aureus meticilino resistente adquirido en comunidad
 alternativos: vancomicina, TMX-sulfa, linezolid. Infection caused by MRSA is increasingly common in many communities. Many isolates of CA-MRSA are susceptible to clindamycin. Isolates of S. aureus. that are erythromycin resistant and clindamycin susceptible should be evaluated. for the presence of inducible macrolide-lincosamide-streptogramin B (MLSB) resistance. This evaluation is done by means of a ‘‘D’’ test, performed by many. hospital laboratories. Although some children treated with clindamycin for an. infection with MRSA of the MLSB phenotype clear their infection, it is recommended. that in the setting of serious infection, clindamycin should not be. used if this phenotype is identified. Alternative drugs to consider for treatment of osteomyelitis caused by MRSA. include intravenous vancomycin, trimethoprim-sulfamethoxasole, and linezolid. Bone and joint infections caused by MRSA should be managed in consultationwith an expert in infectious disease. Empirical use of these antibiotics before. organism identification and susceptibility testing depends on severity of illness. and incidence of MRSA in the community. *S. aureus meticilino resistente adquirido en comunidad.")
38
¿Cuándo se cambia de Tx parenteral a Tx oral?
Depende de: .Disponibilidad de un ATB adecuado .Capacidad de ingesta de ATB del niño .Compromiso y confiabilidad de padres .Ausencia de alteraciones de TGI que afecten la absorción del ATB .Monitoreo de ATB: Test de Schlichter (determinar poder bactericida en suero)
")
39
¿Cuándo se cambia de Tx parenteral a Tx oral?
Tx oral, generalmente, inicia cuando: . Niño cursa afebril .↓ signos y síntomas de infxn .↓ PCR Tx oral .Efectivo con buen seguimiento médico .ATB oral: >2-3 veces de dosis usual .Valorar suspensión si está asintomático a las 4 sem y tiene una VES nl

40
TRATAMIENTO ORAL DE O.M.A

41
TRATAMIENTO FINAL DE LA OSTEOMIELITIS
Duración depende de: .Infección (agente etiológico) .Respuesta clínica .Factores de riesgo subyacentes Promedio de ATB terapia: 3-6 sem.
 .Respuesta clínica. .Factores de riesgo subyacentes. Promedio de ATB terapia: 3-6 sem.")
42
PRONÓSTICO Tx < 3 semanas: alto % de recidiva (> 19%)
5% de recurrencia a pesar de Tx adecuado (médico y qx) NO se ha visto diferencias entre infxs por MRSA y No MRSA Progresión de O.M.H a O.M.C: 5% Secuelas: alterac. crecimiento óseo, fx patolog., asimetría de miembros, artritis.
 NO se ha visto diferencias entre infxs por MRSA y No MRSA. Progresión de O.M.H a O.M.C: 5% Secuelas: alterac. crecimiento óseo, fx patolog., asimetría de miembros, artritis.")
43
ARTRITIS SÉPTICA

44
DEFINICIÓN Presencia de agentes microbianos en el espacio articular o sinovial. Artritis Séptica Aguda: Predomino de bacterias Artritis Séptica Crónica: Predomino de hongos y micobacterias. Artritis Reactiva: Inflamación de la articulación posterior a una infxn bacteriana en algún otro sitio. Artritis Séptica Aguda = EMERGENCIA (falla en dx y tx provoca discapacidad debido a destrucción de cartílago articular)
")
45
EPIDEMIOLOGÍA Frecuencia . + en niños que adultos
. Incidencia actual es desconocida Mortalidad: poco frecuente Etnia: Todas Sexo: 2H:1M Edad: < 3 años

46
Hialuronidasa Bacteriana:
PATOGENIA Líquido Sinovial 1. Viscoso + Ácido hialurónico con IgG 2. Concentrac. de glucosa y electrolitos similares al plasma 3. Lubrica, amortigua y nutre al cartílago avascular de la Articulación 4. Producido por la rica vascularización de memb. sinovial Hialuronidasa Bacteriana: ↓ viscosidad y func. del líq. Sinov. The synovial space may be invaded by one of three routes: (1) hematogenous seeding, (2) local spread from a contiguous infection, and (3) traumatic or surgical infection. Synovial fluid is viscous with IgG and hyaluronic acid. It has glucose and electrolyte concentrations similar to plasma. It serves to lubricate, cushion, and nourish the avascular cartilage of the joint. The rich capillary network of the synovial membrane is responsible for production of the synovial fluid. This capillary network allows microbes to seed the synovial space. Bacterial hyaluronidase decreases the viscosity and thus the function of the synovial fluid. Joint pain is felt with stress on the joint capsule.
 hematogenous seeding, (2) local spread from a contiguous infection, and (3) traumatic or surgical infection. Synovial fluid is viscous with IgG and hyaluronic acid. It has glucose and electrolyte concentrations similar to plasma. It serves to lubricate, cushion, and nourish the avascular cartilage of the joint. The rich capillary network of the synovial membrane is responsible for production of the synovial fluid. This capillary network allows microbes to seed the synovial space. Bacterial hyaluronidase decreases the viscosity and thus the function of the synovial fluid. Joint pain is felt with stress on the joint capsule.")
47
PATOGENIA Infección de la memb. Sinovial a partir de diseminación hematógena de bacterias (principalmente) Resp. Inflam.: migración de PMN, produxn de enzimas proteolíticas y secreción de citokinas por condrocitos Degradac. de cartílago articulación: 8 hrs post-pico de infxn. Cartílago sufre daño conocido como “espectador inocente” por acción de neutrófilos que liberan O2 reactivos, proteasas lisosomales y se da una “autodigestión”) Pyogenic arthritis usually occurs as a result of infection of the vascular synovium by means of hematogenous dissemination of bacteria. An acute inflammatory response follows, resulting in migration of polymorphonuclear WBCs, production of proteolytic enzymes, and cytokine secretion by chondrocytes. Degradation of articular cartilage begins 8 hours after onset of infection [28]. In children younger than 18 months of age, pyogenic arthritis can result from extension of a metaphyseal bone infection through transphyseal blood vessels.
 Pyogenic arthritis usually occurs as a result of infection of the vascular synovium. by means of hematogenous dissemination of bacteria. An acute inflammatory. response follows, resulting in migration of polymorphonuclear WBCs, production of proteolytic enzymes, and cytokine secretion by chondrocytes. Degradation of articular cartilage begins 8 hours after onset of infection [28]. In children younger than 18 months of age, pyogenic arthritis can result from. extension of a metaphyseal bone infection through transphyseal blood vessels.")
48
PATOGENIA Niños < 18 m: A.S producto de extensión de infxn metafisiaria por medio de vasos trans-fisis. Neonatos y Niños pequeños: S.A + O.M.A Infxn de fémur proximal y húmero frecuentemente involucra la articulac. de la cadera y del hombro debido a que metáfisis proximal de estos hh son intracapsulares. In children younger than 18 months of age, pyogenic arthritis can result from extension of a metaphyseal bone infection through transphyseal blood vessels. The growth plate, the epiphysis, and eventually the joint space may be infected. Infection of the proximal femur and humerus often involves the hip and shoulder joints because the proximal metaphysis of each of these bones is intracapsular.

49
EMERGENCIA ORTOPÉDICA
En Articulac. de cadera los mediadores inflamat., bacterias, y fluidos aumentan presión y comprimen vasos intra articulares y la irrigación de la cabeza femoral. Si no se diagnostica o no se trata: osteonecrosis y consecuente osteomielitis OSTEONECROSIS OSTEOMIELITIS Hematogenous spread to the synovium is the most common route by which microorganisms enter a joint. Other entry occurs directly following a penetrating trauma or contiguously from an adjacent osteomyelitis, a rare event in older children. Due to their unique anatomy, neonates and young children often have coexisting SA and osteomyelitis. The bony cortex is thin and the periosteum is loose. Blood vessels connecting the metaphysis and epiphysis serve as a conduit by which bony infection may easily reach the joint space. Pressure necrosis within any joint may destroy synovium or cartilage, but SA of the hip is a true orthopedic emergency. In the hip, inflammatory mediators, bacteria, and fluids increase pressure within the joint, compress intra-articular vessels, and impair blood supply to the femoral head. If the condition remains undiagnosed and untreated, contiguous spread may cause osteonecrosis and lead to osteomyelitis.

50
Más Frecuente

51
ETIOLOGÍA NEONATOS .E. coli, SGB, Bacilos GN, Candida < 2 MESES
Staphylococcus aureus (+ común en TODAS las edades) NEONATOS .E. coli, SGB, Bacilos GN, Candida < 2 MESES .S. agalactie, Neisseria gonorrhoeae, BEGN 2 MESES – 5 AÑOS .S. pyogenes, S. pneumoniae, K. kingae, Hib (no inmunización) 5 AÑOS . S. pyogenes (SGA) Causes: Neonates: Staphylococcus aureus is the most common cause, but Escherichia coli, group B streptococci, and other gram-negative bacilli also cause SA. Children aged 2 months to 5 years H influenzae type B was the most common cause prior to the widespread use of vaccines. In a series of 61 children diagnosed with a known pathogen between , H influenzae type B caused the infection in about half of the children. Thanks to the success of immunization programs, incidence of SA has declined dramatically. S aureus is now the most likely etiologic agent in children of all ages followed by group A streptococci and Streptococcus pneumoniae. Adolescents: Neisseria gonorrhoeae is the suspected cause for those with either polyarticular or monoarticular disease. Other Group A streptococcus is reported in a number of children with active varicella-zoster infection. Salmonella is suspected in those with sickle cell anemia. Mycobacterium tuberculosis is a rare cause of chronic pyogenic arthritis. If identifiable risk factors are present, then a purified protein derivative (PPD) should be placed for the child with culture-negative disease. Kingella kingae has been noted to cause SA in children younger than 5 years in Israel and is an emerging pathogen in the United States. Rarely, fungi or anaerobes may be found within a septic joint. A common cause of reactive arthritis is the spirochete Borrelia burgdorferi. Children typically present with a monoarthritis, in the absence of fever, weeks to months after being bitten by a tick. Less common causes of reactive arthritis include mycoplasma and viruses.
 NEONATOS. .E. coli, SGB, Bacilos GN, Candida. < 2 MESES. .S. agalactie, Neisseria gonorrhoeae, BEGN. 2 MESES – 5 AÑOS. .S. pyogenes, S. pneumoniae, K. kingae, Hib (no inmunización) 5 AÑOS. . S. pyogenes (SGA) Causes: Neonates: Staphylococcus aureus is the most common cause, but Escherichia coli, group B streptococci, and other gram-negative bacilli also cause SA. Children aged 2 months to 5 years. H influenzae type B was the most common cause prior to the widespread use of vaccines. In a series of 61 children diagnosed with a known pathogen between , H influenzae type B caused the infection in about half of the children. Thanks to the success of immunization programs, incidence of SA has declined dramatically. S aureus is now the most likely etiologic agent in children of all ages followed by group A streptococci and Streptococcus pneumoniae. Adolescents: Neisseria gonorrhoeae is the suspected cause for those with either polyarticular or monoarticular disease. Other. Group A streptococcus is reported in a number of children with active varicella-zoster infection. Salmonella is suspected in those with sickle cell anemia. Mycobacterium tuberculosis is a rare cause of chronic pyogenic arthritis. If identifiable risk factors are present, then a purified protein derivative (PPD) should be placed for the child with culture-negative disease. Kingella kingae has been noted to cause SA in children younger than 5 years in Israel and is an emerging pathogen in the United States. Rarely, fungi or anaerobes may be found within a septic joint. A common cause of reactive arthritis is the spirochete Borrelia burgdorferi. Children typically present with a monoarthritis, in the absence of fever, weeks to months after being bitten by a tick. Less common causes of reactive arthritis include mycoplasma and viruses.")
52
ETIOLOGÍA OTROS .N. gonorrhoeae: adolescentes sexualmente activos
con afección poli o monoarticular .SGA: infxn activa de Varicella-Zoster .Salmonella: Drepanocitosis .M. tuberculosis: causa rara de A.S crónica .K. kingae: Asociada con estomatitis y faringitis, < 5 años en Israel, ↑ en USA .Hongos y Anaerobios: en articulac. sépticas .Borrelia burgdorferi: espiroqueta frecuente en artritis reacitva (otros: mycoplasma, virus) Adolescents: Neisseria gonorrhoeae is the suspected cause for those with either polyarticular or monoarticular disease. Other Group A streptococcus is reported in a number of children with active varicella-zoster infection. Salmonella is suspected in those with sickle cell anemia. Mycobacterium tuberculosis is a rare cause of chronic pyogenic arthritis. If identifiable risk factors are present, then a purified protein derivative (PPD) should be placed for the child with culture-negative disease. Kingella kingae has been noted to cause SA in children younger than 5 years in Israel and is an emerging pathogen in the United States. Rarely, fungi or anaerobes may be found within a septic joint. A common cause of reactive arthritis is the spirochete Borrelia burgdorferi. Children typically present with a monoarthritis, in the absence of fever, weeks to months after being bitten by a tick. Less common causes of reactive arthritis include mycoplasma and viruses.
 Adolescents: Neisseria gonorrhoeae is the suspected cause for those with either polyarticular or monoarticular disease. Other. Group A streptococcus is reported in a number of children with active varicella-zoster infection. Salmonella is suspected in those with sickle cell anemia. Mycobacterium tuberculosis is a rare cause of chronic pyogenic arthritis. If identifiable risk factors are present, then a purified protein derivative (PPD) should be placed for the child with culture-negative disease. Kingella kingae has been noted to cause SA in children younger than 5 years in Israel and is an emerging pathogen in the United States. Rarely, fungi or anaerobes may be found within a septic joint. A common cause of reactive arthritis is the spirochete Borrelia burgdorferi. Children typically present with a monoarthritis, in the absence of fever, weeks to months after being bitten by a tick. Less common causes of reactive arthritis include mycoplasma and viruses.")
53
CAUSAS INFECCIOSAS DE ARTRITIS REACTIVA

54
Clínica de A.S Dolor articular con precedentes de trauma o infección respiratoria Artralgia de aparición súbita + edema, fiebre, irritabilidad y cojera Cadera: dolor referido a ingle, muslo o rodilla Pseudoparálisis (neonatos) Clinical manifestations Trauma or upper respiratory tract infection often precedes joint symptoms. Symptoms of pyogenic arthritis include acute onset of joint pain, fever, irritability, and limp. Pain associated with pyogenic arthritis of the hip may be referred to the groin, thigh, or knee. Findings on physical examination include redness, swelling, and warmth over the affected joint. The child complains of pain with movement of the joint and restricted range of motion. Patients should be evaluated for signs of pharyngitis, rash, heart murmur, hepatosplenomegaly, and evidence of other joint or bone involvement.
 Clinical manifestations. Trauma or upper respiratory tract infection often precedes joint symptoms. Symptoms of pyogenic arthritis include acute onset of joint pain, fever, irritability, and limp. Pain associated with pyogenic arthritis of the hip may be. referred to the groin, thigh, or knee. Findings on physical examination include. redness, swelling, and warmth over the affected joint. The child complains of. pain with movement of the joint and restricted range of motion. Patients should. be evaluated for signs of pharyngitis, rash, heart murmur, hepatosplenomegaly, and evidence of other joint or bone involvement.")
55
EXAMEN FÍSICO EN A.S Edema y Aumento de temperatura
sobre articulación afectada Posición antiálgica de miembro afectado Limitación al movimiento Deben evaluarse por: .Faringitis .Rash .Soplo Cardiaco .Hepatoesplenomegalia .Afección en otras articulaciones

56
ARTICULACIONES MÁS AFECTADAS EN PEDIATRÍA EN ARTRITIS SÉPTICA
2ª 1ª 3ª Neonatos: Poliarticular

57
DIAGNÓSTICO DIFERENCIAL
Sinovitis Transitoria .Causa + común de dolor de cadera en niños .Predomina en niños 5-10 años de edad .Afebril o Fiebre baja .Dolor usualmente unilateral .Dolor moderado-severo que despiertan a niño en las noches Enfermedad de Legg-Calve-Perthes .Necrosis avascular de cabeza fémur .Dolor leve y cojera .Edad pico: 7 años Differential diagnosis The most common cause of hip pain in childhood is transient synovitis. Transient synovitis predominates in children 5 to 10 years old. The child generally has low-grade fever or is afebrile. Pain is usually unilateral, but may be bilateral in some cases. Pain ranges from mild to severe enough to wake the child up at night. Physical examination generally reveals a non–ill-appearing child with decreased range of motion of the hip joint. Other causes of joint pain and swelling include reactive arthritis, juvenile rheumatoid arthritis, trauma, and malignancy. Legg-Calve´-Perthes disease is an idiopathic avascular necrosis of the capital femoral epiphysis and may cause mild pain and limp in boys (mean age 7 years). Slipped capital femoral epiphysis is the most common hip disorder of adolescents; symptoms may include abnormal gait, pain, and abnormal range of motion of the hip joint.
. Slipped capital femoral epiphysis. is the most common hip disorder of adolescents; symptoms may include abnormal. gait, pain, and abnormal range of motion of the hip joint.")
58
DIAGNÓSTICO DIFERENCIAL
Artritis Reumatoidea Juvenil Trauma Malignidad Enf. Kawasaki Enf. De Lyme Fiebre Reumática Enfermedad del Suero

59
DIAGNÓSTICO DE A.S Debe ser pronto para evitar daño al
cartílago articular Debe determinarse agente causal Dx se establece a partir de los hallazgos clínicos + análisis líq. Sinovial Artrocentesis debe realizarse lo antes posible Diagnosis Diagnosis of pyogenic arthritis must be made promptly to prevent damage to the articular cartilage. Every attempt should be made to establish a microbiologic diagnosis. Blood and joint fluid should be obtained for aerobic and anaerobic cultures. Joint fluid should be inoculated directly into blood culture bottles to enhance identification of fastidious organisms such as K. kingae. Gram stain and cell count also should be performed on joint fluid. A WBC count of 50,000/mm3 or greater with a predominance of polymorphonuclear cells is consistent with bacterial infection, but also is seen sometimes with rheumatologic disease. The peripheral WBC count, ESR, and CRP are generally elevated, although occasionally CRP is normal, especially with infection caused by K. kingae. If N. gonorrhoeae is suspected, cultures of joint fluid, blood, pharynx, skin lesion, cervix, urethra, vagina, and rectum should be obtained and inoculated onto special media. N. gonorrhoeae also can be detected by nucleic acid amplification techniques using urine, urethral, cervical, or vaginal specimens. A throat culture for S. pyogenes should be sent if the patient has signs or symptoms of pharyngitis. Antibody titers to antistreptolysin O and anti-DNase B also may be useful to diagnose infection with S. pyogenes. Lyme disease serology (including Western blot) is used to diagnose Lyme arthritis in a patient with the appropriate exposure history. Plain radiographs of adjacent bone are useful in evaluating for other causes of joint pain and swelling, including trauma, malignancy, and osteomyelitis. The prompt diagnosis of pyogenic arthritis of the hip is important to prevent serious permanent long-term sequelae. Untreated infection of the hip can result in vascular compromise and ischemic necrosis of the femoral head. Differentiation between pyogenic arthritis and transient synovitis of the hip is challenging. Several studies have shown that a combination of clinical and laboratory features can assist in differentiating these diagnoses (Table 6). Kocher et al [34] found that
 is used to diagnose Lyme arthritis in a patient with the appropriate. exposure history. Plain radiographs of adjacent bone are useful in evaluating. for other causes of joint pain and swelling, including trauma, malignancy, and osteomyelitis. The prompt diagnosis of pyogenic arthritis of the hip is important to prevent. serious permanent long-term sequelae. Untreated infection of the hip can result in. vascular compromise and ischemic necrosis of the femoral head. Differentiation. between pyogenic arthritis and transient synovitis of the hip is challenging. Several studies have shown that a combination of clinical and laboratory features. can assist in differentiating these diagnoses (Table 6). Kocher et al [34] found that.")
60
DIAGNÓSTICO DE A.S Líquido Sinovial
Cultivo de L.S tiene pobre sensibilidad (60-70%). Debe enviarse: Tinción de Gram, cultivos por aerobios y anaerobios,
. Debe enviarse: Tinción de Gram, cultivos por aerobios y anaerobios,")
61
DIAGNÓSTICO DE A.S Líquido Sinovial
Valores indicativos de infxn bacteriana: . Leucos > /mL /mL . PMN 90% . Glucosa en L.S 30% de la glucosa sérica .

62
DIAGNÓSTICO DE A.S Hemocultivo
. 1/3 de los pacientes presentan un hemocultivo (+) en A.S
 en A.S.")
63
DIAGNÓSTICO DE A.S Radiografía
No diferencia edema periarticular y trauma local de derrame verdadero en articulación. Muestra un derrame articular como un ensanchamiento en el espacio articular con desplazamientos. Puede ser útil para descartar tumores, fracturas, enf. De Perthes, entre otros.

64
DIAGNÓSTICO DE A.S Ultrasonido
- Método sencillo y no costoso para detectar derrame articular de cadera. - > sensibilidad que Rx - Examen de elección para detectar derrames de cadera y en caso de ser (+) permite guiar la aspiración articular.
 permite guiar la aspiración articular.")
65
DIAGNÓSTICO DE A.S Gamma Óseo En casos de afxn multifocal en neonatos
Permite detectar posible osteomielitis

66
TRATAMIENTO DE A.S El éxito se basa en una rápida descompresión del espacio articular e inicio con ATB. Manejo conjunto ortopedia-infectología Artrocentesis puede ser un método diagnóstico y/o terapéutico

67
TRATAMIENTO MÉDICO DE A.S
Inmovilizar (“tablilla”) articulación afectada Iniciar ATB empírica ATB específica a partir de agente causal específico Promover a los 2-3 días leves movimientos de extremidad afectada para estimular extensión de tendones y prevenir contracturas
 articulación afectada. Iniciar ATB empírica. ATB específica a partir de agente causal específico. Promover a los 2-3 días leves movimientos de extremidad afectada para estimular extensión de tendones y prevenir contracturas.")
68
TRATAMIENTO QX EN A.S Artrotomía y Drenaje qx urgente en:
.Infx en articulación de cadera/hombro .En otras articulac. si NO hay mejoría qx a los 3 días de haber iniciado ATB .Artrocentesis con gran cantidad de pus y/o escombros o material contaminante En los demás casos: aspiración (a repetic.)
")
69
TRATAMIENTO EMPÍRICO DE A.S
< 2 meses .Clindamicina/Vancomicina + Cefas 3ª para cubrir contra S. aureus y BEGN < 2 meses – 5 años .ATB contra S. aureus, S. pyogenes y K. kingae Usar ceftriaxone si se sospecha N. gonorrhoeae

70
TRATAMIENTO EMPÍRICO DE A.S
ATB anti-estafilocóccicos: Nafcicilina, Vancomicina, Clindamicina, Cefazolina Hib: cefas 3ª generac. + clindamicina

71
TRATAMIENTO DE A.S Igual que en O.M.A debe usarse tx IV hasta mejoría clínica y normalización de marcadores inflamatorios. Terapia ATB oral es igual que en la O.M.A

72
TRATAMIENTO DE A.S En casos NO complicados de A.S:
.Terapia corta de ATB IV (3-4 días) con posterior seguimiento de Tx oral permite disminuir estadía en Hospital En un estudio en C.R, un tx de 4 días con dexametasona + ATB adecuado + tratamiento qx demostró ↓ de síntomas y de alteraciones articulares a largo plazo.
 con posterior seguimiento de Tx oral. permite disminuir estadía en Hospital. En un estudio en C.R, un tx de 4 días. con dexametasona + ATB adecuado. + tratamiento qx demostró ↓ de síntomas y de. alteraciones articulares a largo plazo.")
73
COMPLICACIONES En 10-25% de todos los casos En casos con Hib:
.Meningitis (10-30%) .Osteomielitis (5-10%) .Celulitis (10-30%) .Neumonía (5%) Cualquier agente causal: .Osteonecrosis .Crecimiento óseo anormal .Cojera .Inestabilidad de articulación afectada .Movilidad limitada
 .Osteomielitis (5-10%) .Celulitis (10-30%) .Neumonía (5%) Cualquier agente causal: .Osteonecrosis. .Crecimiento óseo anormal. .Cojera. .Inestabilidad de articulación. afectada. .Movilidad limitada.")
Presentaciones similares










>")













