Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Pedro Pérez Segura Oncología Médica - HCSC
CETUXIMAB: CONSOLIDANDO EL ESTÁNDAR DE TRATAMIENTO EN CÁNCER ESCAMOSO DE CABEZA Y CUELLO Pedro Pérez Segura Oncología Médica - HCSC

2
TRAYECTORIA DE CETUXIMAB
Aprob CTX 1ªL ESMO/ASCO CDDP CDDP+¿? TPF EXTREME QoL No impacto SG EXTREME ¿?

3
CETUXIMAB 90 – 100% tumores de cabeza y cuello expresan en su superficie EGFR (factor de crecimiento epidérmico). EGFR regula la progresión del ciclo celular de las células tumorales, la reparación celular y la supervivencia, y por tanto, está involucrado en la formación de mtx Anticuerpo monoclonal que se une al EGFR, promoviendo su degradación y por tanto realizando actividad antitumoral Efecto sinérgico con rt y qt.

4
ENFERMEDAD LOCALMENTE AVANZADA: INDUCCIÓN

5
Posner, 2007 – TAX 324 TPF Docetaxel 75 mg/m2 IV Cisplatino 100 mg/m2 IV 5-FU mg/m2/d IV x 4 días Cada 3 semanas por 3 ciclos (n = 280) Estadio III/IV Irresecables + Resecables candidatos a preservación (n=172) (N = 501) CRT Carboplatino AUC 1,5, semanal RDT diaria 5 días /semana Seguido de cirugía si enfermedad residual PF Cisplatino 100 mg/m2 IV 5-FU mg/m2/d PC x 5 días Cada 3 semanas por 3 ciclos (n = 259) Orofaringe 50% Laringe 20% Hipofaringe 15% C. Oral 10% N Engl J Med 2007;357:
 (N = 501) CRT Carboplatino AUC 1,5, semanal RDT diaria 5 días /semana. Seguido de cirugía si enfermedad residual. PF Cisplatino 100 mg/m2 IV 5-FU mg/m2/d PC x 5 días Cada 3 semanas por 3 ciclos (n = 259) Orofaringe 50% Laringe 20% Hipofaringe 15% C. Oral 10% N Engl J Med 2007;357:")
6
Superioridad del triplete en términos de:
Respuestas: 64% vs 72% SV LE: vs 13 meses Supervivencia global: vs 30 meses Reducción riesgo muerte: 30%

7
TPF CETUXIMAB RT CETUXIMAB
Estudio NEO-TPF TPF CETUXIMAB RT CETUXIMAB TPF (4 ciclos) Docetaxel: Cisplatino: 5-FU: 75 mg/m2 dia 1 750 mg/m2 dias 1–5 ERBITUX: Dosis inicial 400 mg/m2 en ciclo 1, dia 1, después 250 mg/m2 dia 1, 8, 15 en inducción 250 mg/m2 semanalmente con RT RT: Rt acelerada con boost concomitante(70 Gy) Objetivo principal: tasa de respuesta tras el 2º y 4º ciclo Objetivos secundarios: tasa de respuesta completa, seguridad y toxicidad
 Docetaxel: Cisplatino: 5-FU: 75 mg/m2 dia mg/m2 dias 1–5. ERBITUX: Dosis inicial 400 mg/m2 en ciclo 1, dia 1, después 250 mg/m2 dia 1, 8, 15 en inducción. 250 mg/m2 semanalmente con RT. RT: Rt acelerada con boost concomitante(70 Gy) Objetivo principal: tasa de respuesta tras el 2º y 4º ciclo. Objetivos secundarios: tasa de respuesta completa, seguridad y toxicidad.")
8
La QT de inducción con Cetuximab + TPF proporciona una alta tasa de respuestas
EFICACIA (n=47)a Respuesta completa, % 26 Respuesta parcial, % 57 Enfermedad estable, % 6 Progresión, % 3 Control de enf. = 89% ORR = 83% Toxicidad Toxicidades grado 3 más comunes Neutropenia, 26%; Neutropenia febril, 24%; diarrea, 14%; mucositis, 14%
a. Respuesta completa, % 26. Respuesta parcial, % 57. Enfermedad estable, % 6. Progresión, % 3. Control. de enf. = 89% ORR = 83% Toxicidad. Toxicidades grado 3 más comunes. Neutropenia, 26%; Neutropenia febril, 24%; diarrea, 14%; mucositis, 14%")
9
TRATAMIENTO CONCOMITANTE: RT + CTX

10
Cet initial dose (400 mg/m2)
Study design of phase III radiotherapy ± cetuximab in head and neck cancer RT + Cetuximab Cet initial dose (400 mg/m2) Cet (250 mg/m2) + RT (wks 2–8) Locally advanced SCCHN stage III/IV, non-metastatic oropharynx, hypopharynx or larynx N=424 R RT Primary endpoint: Duration of locoregional control Secondary endpoints: OS, PFS, RR, QoL, and safety Bonner JA, et al. N Engl J Med 2006;354:567–578 Curran D, et al. J Clin Oncol 2007;25:2191–2197 Cet, cetuximab; OS, overall survival; PFS, progression-free survival; QoL, quality of life; RR, relative response; RT radiotherapy; SCCHN, squamous cell carcinoma of the head & neck
 Cet (250 mg/m2) + RT (wks 2–8) Locally advanced SCCHN. stage III/IV, non-metastatic. oropharynx, hypopharynx or larynx. N=424. R. RT. Primary endpoint: Duration of locoregional control. Secondary endpoints: OS, PFS, RR, QoL, and safety. Bonner JA, et al. N Engl J Med 2006;354:567–578. Curran D, et al. J Clin Oncol 2007;25:2191–2197. Cet, cetuximab; OS, overall survival; PFS, progression-free survival; QoL, quality of life; RR, relative response; RT radiotherapy; SCCHN, squamous cell carcinoma of the head & neck.")
11
RT + CTX significantly improves LRC and 5-year OS in LASCCHN
Locoregional control (%) 100 80 60 40 20 10 30 50 14.9 months 24.4 months HR=0.68 [95% CI: 0.52–0.89] p=0.005 3-year control rate 47% 34% RT RT + cet Months HR=0.73 [95% CI: 0.56–0.95] p=0.018 100 OS (%) 5-year survival rate 36% 46% 49.0 months 29.3 months 20 40 60 80 Months No. at risk RT 213 122 80 51 30 10 RT + cet 211 143 101 66 35 9 No. at risk RT 213 162 122 98 85 77 49 RT+ cet 211 177 136 117 105 90 Bonner JA, et al. N Engl J Med 2006;354:567-78 Bonner JA, et al. Lancet Oncol 2010;11:21–28 HR, hazard ratio; LA-SCCHN, locally advanced squamous cell carcinoma of the head & neck; LRC, locoregional control
 months months. HR=0.68 [95% CI: 0.52–0.89] p= year control rate. 47% 34% RT. RT + cet. Months. HR=0.73 [95% CI: 0.56–0.95] p= OS (%) 5-year survival rate. 36% 46% 49.0 months months Months. No. at risk. RT RT + cet No. at risk. RT RT+ cet Bonner JA, et al. N Engl J Med 2006;354: Bonner JA, et al. Lancet Oncol 2010;11:21–28. HR, hazard ratio; LA-SCCHN, locally advanced squamous cell carcinoma of the head & neck; LRC, locoregional control.")
14
ENFERMEDAD AVANZADA / RECURRENTE

15
EXTREME 15

16
EXTREME: Study Design Patients with previously untreated metastatic or recurrent head and neck SCC Randomized Group A Cetuximab 400 mg/m2 initial dose then 250 mg/m2/wk + either Carboplatin AUC 5, Day 1 or Cisplatin 100 mg/m2 IV, Day 1 + 5-FU 1000 mg/m2 IV, Day 1-4: 3-wk cycles Group B Either Carboplatin AUC 5, Day 1 or Cisplatin 100 mg/m2 IV, Day 1 + 5-FU 1000 mg/m2 IV, Day 1-4: 3-wk cycles Subsequently, a larger study was run in Europe. This was called the EXTREME study. The patients were treated with either cisplatin/5‑FU or carboplatin and 5‑FU for a maximum of 6 cycles. The investigational group (Group A) also received cetuximab with a loading dose and weekly maintenance and cetuximab was continued after the conclusion of the chemotherapy 6 cycles. 6 chemotherapy cycles maximum Cetuximab No treatment Progressive disease or unacceptable toxicity Vermorken JB, et al. N Engl J Med. 2008;359:
 also received cetuximab with a loading dose and weekly maintenance and cetuximab was continued after the conclusion of the chemotherapy 6 cycles. 6 chemotherapy cycles maximum. Cetuximab. No treatment. Progressive disease or unacceptable toxicity. Vermorken JB, et al. N Engl J Med. 2008;359:")
17
Vermorken JB, et al. NEJM 2008; 359: 1116-27
Fase III, randomizado, multicéntrico 80 centros en 17 países Europeos No requerida detección de EGFR Pacientes no pretratados con CECC R/M Estratificados según: Régimen de quimioterapia KPS (<80 vs. ≥80) Tratamiento: Platino (cisplatino o carboplatino) + 5-FU +/- Erbitux Vermorken JB, et al. NEJM 2008; 359: 17
 Tratamiento: Platino (cisplatino o carboplatino) + 5-FU +/- Erbitux. Vermorken JB, et al. NEJM 2008; 359:")
18
Características Basales
QT Basada en Platino + ERBITUX (n=222) QT Basada en Platino sola (n=220) Mediana de edad, años 56 57 Hombre/Mujer, % 89/11 92/8 Extensión de la enfermedad, % Recurrencia local Metástasis 53 47 54 46 KPS, % <80 ≥80 12 88 11 89 a Metastasis con o sin recurrencia local Vermorken JB et al. N Engl J Med 2008;359:1116–1127 18 18
 QT Basada en Platino sola (n=220) Mediana de edad, años Hombre/Mujer, % 89/11. 92/8. Extensión de la enfermedad, % Recurrencia local. Metástasis KPS, % <80. ≥ a Metastasis con o sin recurrencia local. Vermorken JB et al. N Engl J Med 2008;359:1116–")
19
Tasa de respuestas 36 20 CR=0.9 CR = 6.8 Tasa respuestas objetivas (%)
10/04/2017 36 40 30 20 Tasa respuestas objetivas (%) 20 10 Adding Erbitux means almost doubling the response rate. Adding Erbitux to platinum-based chemotherapy nearly doubles the response rate. A significant increase in the overall response rate, from 20% to 36%, is achieved by adding Erbitux to platinum-based chemotherapy. Nearly twice as many patients will respond to the treatment when Erbitux is added to the chemotherapy you are using. CR=0.9 CR = 6.8 QT sola QT + ERBITUX Tasa respuestas objetivas (CR+PR) Odds ratio (95% CI): 2.33 (1.50–3.60); p<0.001 Vermorken JB et al. N Engl J Med 2008;359:1116–1127 19 19
 Adding Erbitux means almost doubling the response rate. Adding Erbitux to platinum-based chemotherapy nearly doubles the response rate. A significant increase in the overall response rate, from 20% to 36%, is achieved by adding Erbitux to platinum-based chemotherapy. Nearly twice as many patients will respond to the treatment when Erbitux is added to the chemotherapy you are using. CR=0.9. CR = 6.8. QT sola. QT + ERBITUX. Tasa respuestas objetivas (CR+PR) Odds ratio (95% CI): 2.33 (1.50–3.60); p< Vermorken JB et al. N Engl J Med 2008;359:1116–")
20
Supervivencia Libre de Progresión
1.0 | | | | | | | | | | | QT sola 0.9 QT + ERBITUX | | | | | | | | | | | | | | | | 0.8 | | | HR [95%CI]: 0.54 [0.43–0.67] | | | p <0.001 0.7 | | | 0.6 | | | | 5.6 meses + 2.3 meses % Libre Progresión 0.5 3.3 meses | | | 0.4 | | | | | 0.3 | | | | | 0.2 | | 0.1 | | | 0.0 3 6 9 12 15 Riesgo Pacientes PFS (meses) QT sola 220 103 29 8 3 1 QT + ERBITUX 222 138 72 29 12 7 Vermorken JB, et al. New Engl J Med 2008;359:1116–27
 QT sola QT + ERBITUX Vermorken JB, et al. New Engl J Med 2008;359:1116–27.")
21
Probalidad Supervivencia Tiempo Supervivencia (meses)
Supervivencia Global 1.0 | | | | | 0.9 | QT sola | QT + ERBITUX | | 0.8 HR [95%CI]: 0.80 [0.64–0.99] | | | p=0.04 0.7 | 0.6 + 2.7 meses 10.1 months 7.4 months 10.1 meses Probalidad Supervivencia 0.5 7.4 meses | 0.4 | | 0.3 | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | 0.2 | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | 0.1 0.0 3 6 9 12 15 18 21 24 Tiempo Supervivencia (meses) Riesgo Pacientes QT sola 220 173 127 83 65 47 19 8 1 QT + ERBITUX 222 184 153 118 82 57 30 15 3 Vermorken JB, et al. New Engl J Med 2008;359:1116–27
 Riesgo Pacientes. QT sola QT + ERBITUX Vermorken JB, et al. New Engl J Med 2008;359:1116–27.")
22
Eventos adversos G 3/4 However, there were 9 cases of sepsis
in the cetuximab group, as compared with 1 case in the chemotherapy-alone group (P = 0.02), and there were 11 cases of hypomagnesemia in the cetuximab group, as compared with 3 cases in the chemotherapy-alone group (P = 0.05) Vermorken JB, et al. New Engl J Med 2008;359:1116–27
, and. there were 11 cases of hypomagnesemia in the. cetuximab group, as compared with 3 cases in the. chemotherapy-alone group (P = 0.05) Vermorken JB, et al. New Engl J Med 2008;359:1116–27.")
23
EXTREME: QoL Mesia R et al. Ann Oncol 2010; 21: 1967–1973.
Mesia R et al. Ann Oncol Oct;21(10): 23 23
:")
24
Mesia R et al. Ann Oncol. 2010 Oct;21(10):1967-73
:")
25
EXTREME: Control de síntomas
Mesia R et al. Ann Oncol Oct;21(10):
:")
26
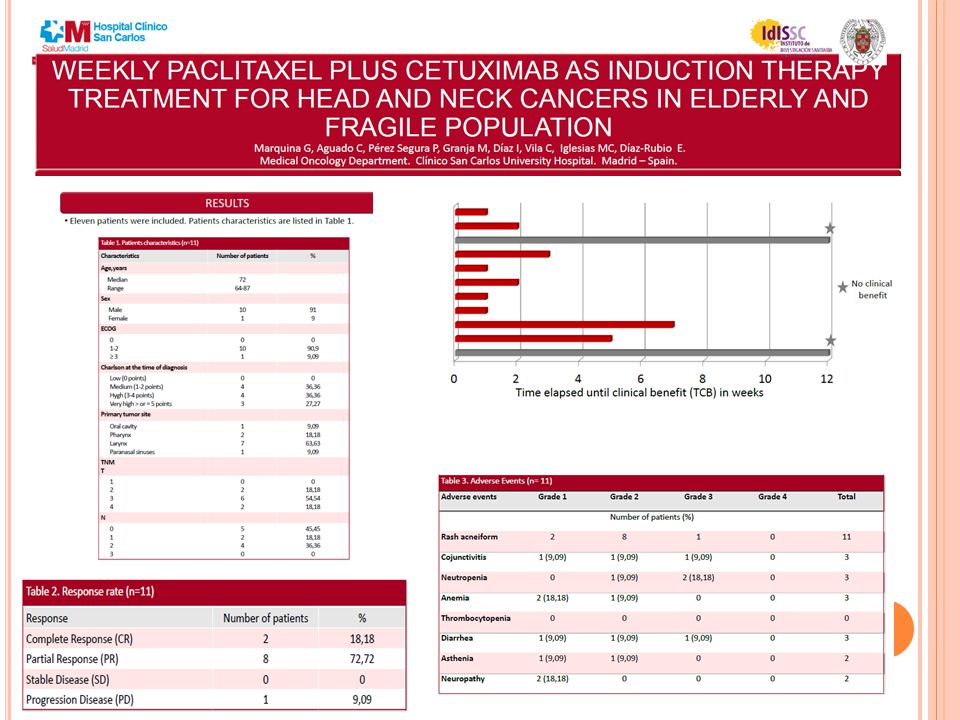
ERBITAX Estudio fase II con taxol semanal
* ERBITAX Estudio fase II con taxol semanal *Uso experimental fuera de indicación autorizada

27
ERBITAX Estudio fase II con taxol semanal
* ERBITAX Estudio fase II con taxol semanal Criterios de inclusión: Pcts con CECC R/M (laringe, faringe, cavidad oral) > 18 años KPS ≥ 70% Se permite QT previa si se ha administrado 6 meses antes Respuesta medida por TAC / RMN cada 6 semanas n= 46 Objetivo primario: Tasa de respuesta objetiva Objetivo secundario: Duración de respuesta, PFS, OS, Seguridad. Cetuximab (dosis inicial 400 mg/m2, luego 250 mg/m2 semanal) Paclitaxel (80 mg/m2) semanal Hasta progresión o toxicidad CECC Recurrente/mtx *Uso experimental fuera de indicación autorizada Hitt R, Irigoyen A, Cortes-Funes H, et al.; the Spanish Head and Neck Cancer Cooperative Group (TTCC). Ann Oncol Aug 23 (Epub ahead of print)
 > 18 años. KPS ≥ 70% Se permite QT previa si se ha administrado 6 meses antes Respuesta medida por TAC / RMN cada 6 semanas. n= 46. Objetivo primario: Tasa de respuesta objetiva. Objetivo secundario: Duración de respuesta, PFS, OS, Seguridad. Cetuximab. (dosis inicial 400 mg/m2, luego 250 mg/m2 semanal) + Paclitaxel. (80 mg/m2) semanal. Hasta progresión o toxicidad. CECC. Recurrente/mtx. *Uso experimental fuera de indicación autorizada. Hitt R, Irigoyen A, Cortes-Funes H, et al.; the Spanish Head and Neck Cancer Cooperative Group (TTCC). Ann Oncol Aug 23 (Epub ahead of print)")
28
Erbitax: Eficacia * Mejor respuesta n % RC 10 22 RP 15 33 EE 12 26 PE
11 54% OR 80% DCR *Uso experimental fuera de indicación autorizada Hitt R, Irigoyen A, Cortes-Funes H, et al.; the Spanish Head and Neck Cancer Cooperative Group (TTCC). Ann Oncol Aug 23 (Epub ahead of print)
. Ann Oncol Aug 23 (Epub ahead of print)")
29
Erbitax: Eficacia * Mediana SLP 4.2 meses (95% IC 2.9–5.5 )
Mediana SG 8.1 meses (95% IC 6.6–9.6 ) *Uso experimental fuera de indicación autorizada Hitt R, Irigoyen A, Cortes-Funes H, et al.; the Spanish Head and Neck Cancer Cooperative Group (TTCC). Ann Oncol Aug 23 (Epub ahead of print)
 *Uso experimental fuera de indicación autorizada. Hitt R, Irigoyen A, Cortes-Funes H, et al.; the Spanish Head and Neck Cancer Cooperative Group (TTCC). Ann Oncol Aug 23 (Epub ahead of print)")
30
Erbitax: Seguridad * Grado 3-4 N % Neutropenia 6 13 Neutropenia febril
2 Diarrea Astenia 8 17 Mucositis 3 7 Neuropatia / parestesias 5 11 Acne-like rash 24 Conjuntivitis 4 Reacciones infusionales a aPaclitaxel *Uso experimental fuera de indicación autorizada Hitt R, Irigoyen A, Cortes-Funes H, et al.; the Spanish Head and Neck Cancer Cooperative Group (TTCC). Ann Oncol Aug 23 (Epub ahead of print)
. Ann Oncol Aug 23 (Epub ahead of print)")
31
Conclusiones La combinación de Cetuximab + paclitaxel semanal es activa en primera línea de CECC R/M: 54% de tasa de respuestas SLP 4.2 meses SG 8.1 meses La combinación es bien tolerada “ ” *Uso experimental fuera de indicación autorizada Hitt R, Irigoyen A, Cortes-Funes H, et al.; the Spanish Head and Neck Cancer Cooperative Group (TTCC). Ann Oncol Aug 23 (Epub ahead of print)
. Ann Oncol Aug 23 (Epub ahead of print)")
32
FUTURO DE CETUXIMAB EN CCC
1.- Enfermedad localmente avanzada - Fármaco incorporado a los protocolos “habituales” - RT + Cetuximab ¿para todos? 2.- Enfermedad avanzada / recurrente - Esquemas con Cetuximab y sin platinos ???? - Tratamiento de mantenimiento tras respuesta 3.- Tratamiento de inducción - ¿Aporta algo al TPF? - ¿Podemos evitar el platino a cambio de taxanos+Cetuximab? 4.- QoL a largo plazo - HPV / p16

Presentaciones similares

















, fue un dramaturgo, poeta y actor inglés. Conocido en ocasiones como el Bardo de Avon (o.>")

