Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Tratamiento de la hepatitis B en 2013
IV Curso para Residentes Director: Rafael Esteban Barcelona, Octubre 2013

2
1 Historia Natural del VHB 2 Desde el portador inactivo a la cirrosis H. 3 Objetivos del Tratamiento 4 5 6 7 Indicaciones Urgentes Tratamiento AgHBe positivo y negativo Rebrote virológico y resistencias Tratamiento de las gestantes Algunas ideas sobre el futuro

3
? Los pacientes infectados por transmisión vertical pasan una fase de inmunotolerancia (alta replicación viral con ALT normal) muy larga (años). En cambio, los infectados en la edad adulta esta fase es más corta. La indicación de tratamiento es en la actualidad durante la fase de hepatitis crónica o la cirrosis hepática, no obstante, se están iniciando ensayos clínicos en la fase de inmunotolerancia
 muy larga (años). En cambio, los infectados en la edad adulta esta fase es más corta. La indicación de tratamiento es en la actualidad durante la fase de hepatitis crónica o la cirrosis hepática, no obstante, se están iniciando ensayos clínicos en la fase de inmunotolerancia.")
5
Razones para su tratamiento: muy infectivos y posibilidad de CHC
Inmunotolerancia VHB Décadas Asintomáticos > 30 años Fibrosis, Cirrosis, C. Hepatocelular > 40 años Aumento brusco de C.Hepatocelular Patients with HBV-DNA <69 UI/ml at wk 192 Razones para su tratamiento: muy infectivos y posibilidad de CHC Tenofovir (TDF) y aún más el Tenofovir y Entricibabina (TDF/FTC) efectivo, sobre todo en mujeres. Chan HL et al. EASL 2013
 y aún más el Tenofovir y Entricibabina (TDF/FTC) efectivo, sobre todo en mujeres. Chan HL et al. EASL")
6
Objetivos del tratamiento en el VHB
Primario Prevenir el desarrollo de cirrosis, fallo hepático y carcinoma hepatocelular Secundario Seroconversión a antiHBe si es AgHBe+vo DNA-VHB negativo (mejor que <10-15 UI/mL) ALT normal AgHBs negativo y seroconversión a anti-HBs La infección nunca puede ser erradicada, ya que el cccDNA permanece en el núcleo de la célula infectada. Lo ideal es negativizar el virus por <10-15 UI/mL según los métodos de PCR en tiempo real
 ALT normal. AgHBs negativo y seroconversión a anti-HBs. La infección nunca puede ser erradicada, ya que el cccDNA permanece en el núcleo de la célula infectada. Lo ideal es negativizar el virus por <10-15 UI/mL según los métodos de PCR en tiempo real.")
7
Importancia de la negativización del DNA-VHB para la prevención del CHC y la progresión de la enfermedad En un artículo muy importante se demostró como la incidencia de CHC va aumentando conforme el DNA-VHB es más alto, lo que demuestra la importancia de negativizar el virus Ya en 2004, se demostró como la lamivudina, fármaco ya no usado, disminuye claramente las posibilidades de progresión de la enfermedad

8
A largo plazo el Tenofovir (5 años) puede revertir la cirrosis hepática y el Entecavir (7 años) disminuir la incidencia de CHC Los nuevos antivirales, Tenofovir y Entecavir, han demostrado que consiguen revertir la cirrosis hepática o prevenir el CHC. El Tenofovir a largo plazo consigue disminuir la puntuación de la fibrosis medida por la escala de Ishak hasta 3 y 4 puntos en un número muy importante de casos. Por otro lado, el Entecavir previene la aparición del CHC comparado con un grupo control. Esto demuestra lo importante que es controlar la viremia.

9
Elección del fármaco: IFN-PEG o análogos de núcleos(t)idos
INF-Peg Núcleos(t)idos Vía administración Subcutánea Oral Tolerancia Mala Excelente Duración tratamiento 48 semanas Indefinida >80% Supresión máxima DNA log10 4.5 6.9 Genotipo A (AgHBe +vo) Cualquier genotipo Efectividad si DNA>109UI/ml + +++ Seroconversión AgHBe 1 año ~30% ~20% Perdida de AgHBs 1 año 3%-4% 0%-3% (2 años: 3-5%) Resistencias Nula ETV muy escasa, TDF nula CH compensada No recomendable Retrasa descompensación CH descompensada Contraindicado Puede salvar la vida
idos. Vía administración. Subcutánea. Oral. Tolerancia. Mala. Excelente. Duración tratamiento. 48 semanas. Indefinida >80% Supresión máxima DNA log Genotipo. A (AgHBe +vo) Cualquier genotipo. Efectividad si DNA>109UI/ml Seroconversión AgHBe 1 año. ~30% ~20% Perdida de AgHBs 1 año. 3%-4% 0%-3% (2 años: 3-5%) Resistencias. Nula. ETV muy escasa, TDF nula. CH compensada. No recomendable. Retrasa descompensación. CH descompensada. Contraindicado. Puede salvar la vida.")
11
Tratamiento si es corto con LAM y si es largo con ETV o TDV
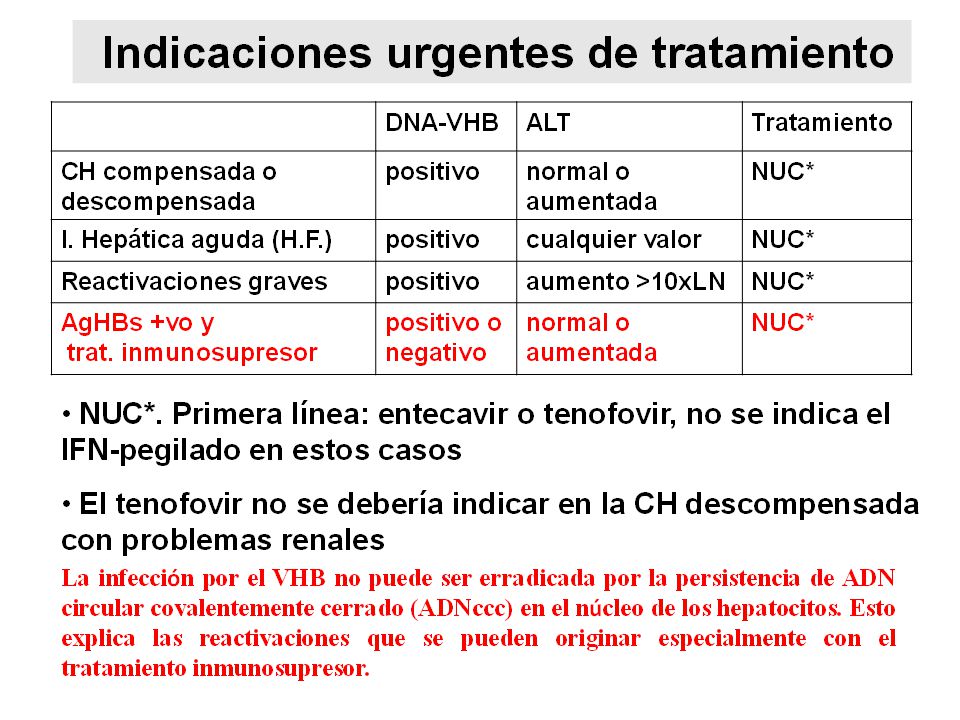
Prevención de las reactivaciones en AgHBs positivo con DNA-VHB positivo o negativo que son sometidos a tratamiento inmunosupresor Tratamiento con alto riesgo de reactivación: Rituximab Monoclonales como el anti-TNF Quimioembolización intraarterial en pacientes CCH y VHB Pacientes en tratamiento con citostáticos y corticoides Trasplantados de médula ósea u órganos sólidos Indicaciones, pacientes con: AgHBs positivo con o sin DNA-VHB AgHBs negativo y anti-HBc positivo Tratamiento si es corto con LAM y si es largo con ETV o TDV

12
Reactivación en pacientes con infección crónica por VHB sometidos a tratamiento citostático o inmunosupresor Tratamiento citostático inmunosupresor Tiempo (semanas) ADN VHB (log 10 copias /ml) ALT (UI/L) HBsAg Tratamiento anticipado Tratamiento diferido de la hepatitis Profilaxis
 ADN VHB (log 10 copias /ml) ALT (UI/L) HBsAg. Tratamiento. anticipado. Tratamiento diferido. de la hepatitis. Profilaxis.")
13
Estos pacientes NO tienen una indicación URGENTE de tratamiento y la mejor actitud es la observación ± un año con controles del DNA y ALT antes del tratamiento

14
Divergencia entre métodos Fibrosis avanzada Biopsia Hepática ?
Métodos serológicos y la ET en la toma de decisiones: pacientes con ALT normal o límite de la normalidad y carga viral poco aumentada ALT± normal y carga viral poco aumentada (zona gris) Fibrotest o APRI o Forns y Elastografía Transitoria Coinciden en fibrosis leve Divergencia entre métodos Coinciden en fibrosis avanzada Fibrosis avanzada Biopsia Hepática ? No Biopsia Hepática Biopsia Hepática Tratamiento fibrosis avanzada
 Fibrotest o APRI o Forns. y. Elastografía Transitoria. Coinciden en fibrosis leve. Divergencia entre métodos. Coinciden en fibrosis avanzada. Fibrosis avanzada Biopsia Hepática No Biopsia Hepática. Biopsia Hepática. Tratamiento fibrosis avanzada.")
15
Efectividad de los fármacos de primera línea(EASL 2012)
AgHBe +vo (tratamiento 1 año) IFN-peg Entecavir Tenofovir Seroconversión anti-HBe 30% 21% DNA-VHB <60-80 UI/ml 14% 67% 76% ALT normal 41% 68% AgHBs negativo 3% 2% AgHBe -vo (tratamiento 1 año) IFN-peg Entecavir Tenofovir DNA-VHB <60-80 UI/ml 19% 90% 93% ALT normal 59% 78% 76% AgHBs negativo 4% 0%
 IFN-peg. Entecavir. Tenofovir. Seroconversión anti-HBe. 30% 21% DNA-VHB <60-80 UI/ml. 14% 67% 76% ALT normal. 41% 68% AgHBs negativo. 3% 2% AgHBe -vo (tratamiento 1 año) IFN-peg. Entecavir. Tenofovir. DNA-VHB <60-80 UI/ml. 19% 90% 93% ALT normal. 59% 78% 76% AgHBs negativo. 4% 0%")
16
Virologic Suppression at Year 6
‡ Response HBeAg - Patients (Study 102) HBeAg+ Patients (Study 103) Year 5 Year 6 HBV DNA < 400 copies/mL Intent to treat * , % (n/N) 83 (291/350) 81 (281/345) 65 (160/248) 63 (157/251) On treatment † 99 (292/295) 99.6 (283/284) 97 (170/175) (167/169) LTE TDF (missing = failure/addition of FTC = failure) Observed (missing = excluded/addition of FTC = included) 80% of 585 patients entering the open label phase remained on study at Year 6; 73% of enrolled patients remained on study HBeAg loss/seroconversion rates of 50% and 37%, respectively, th rough 6 years 11% of HBeAg+ patients had confirmed HBsAg loss (8% with serocon version) No resistance to TDF was detected through 6 years TENOFOVIR. Studies 102/103 Virologic Suppression at Year 6 Marcellin P, et al. AASLD 2012; Boston. #374. 6 Neither Truvada (TVD = TDF + FTC) or emtricitabine (FTC) are licensed for use to treat CHB En los AgHBe positivo los NUCs se pueden retirar 12 meses después de la seroconversión, con vigilancia estrecha. En los AgHBe negativo es más improbable retirar la medicación, solo en los AgHBs negativos 16
 HBeAg+ Patients. (Study 103) Year 5. Year 6. HBV DNA < 400 copies/mL. Intent. to. treat. * , % (n/N) 83. (291/350) 81. (281/345) 65. (160/248) 63. (157/251) On treatment. † 99. (292/295) (283/284) 97. (170/175) (167/169) LTE. TDF (missing = failure/addition of FTC = failure) Observed (missing = excluded/addition of FTC = included) 80% of 585 patients entering the open. label phase remained on study at Year 6; 73% of. enrolled patients remained on study. HBeAg loss/seroconversion rates of 50% and 37%, respectively, th. rough 6 years. 11% of HBeAg+ patients had confirmed HBsAg loss (8% with serocon. version) No resistance to TDF was detected through 6 years. TENOFOVIR. Studies 102/103. Virologic Suppression at Year 6. Marcellin P, et al. AASLD 2012; Boston. # Neither. Truvada. (TVD = TDF + FTC) or. emtricitabine. (FTC) are licensed for use to treat CHB. En los AgHBe positivo los NUCs se pueden retirar 12 meses después de la seroconversión, con vigilancia estrecha. En los AgHBe negativo es más improbable retirar la medicación, solo en los AgHBs negativos. 16.")
17
Rebote virológico y resistencias
Concepto: Aumento DNA-VHB > 1 log con respecto valor más bajo DNA-VHB detectable si previamente no lo era Resistencias: No descritas con el Tenofovir 1.2% a los 5 años con el Entecavir IMPORTANTE, hay que investigar: Fármacos hepatotóxicos Ingesta de alcohol Y, SOBRE TODO, MALA ADHERENCIA AL TRATAMIENTO

19
Gestación: Clasificación de la FDA de los NUCs
Categoría B Telbivudina Tenofovir (no efecto teratogénico o embriotóxico en animales; no estudios en humanos) Categoría C LAM Adefovir Entecavir (teratogénico o embriotóxico en animales) La seguridad del tratamiento antiviral durante la gestación y la lactancia materna no está bien definida El IFN-peg está contraindicado durante la gestación por su efecto anti-proliferativo
 Categoría C. LAM. Adefovir. Entecavir. (teratogénico o embriotóxico en animales) La seguridad del tratamiento antiviral durante la gestación y la lactancia materna no está bien definida. El IFN-peg está contraindicado durante la gestación por su efecto anti-proliferativo.")
20
Recomendaciones para las gestantes infectadas VHB
Estudio hepático H. no avanzada H. avanzada Prioridad a la gestación Tratamiento No tratar el VHB Fármacos categoría B: tenofovir o telbivudina

21
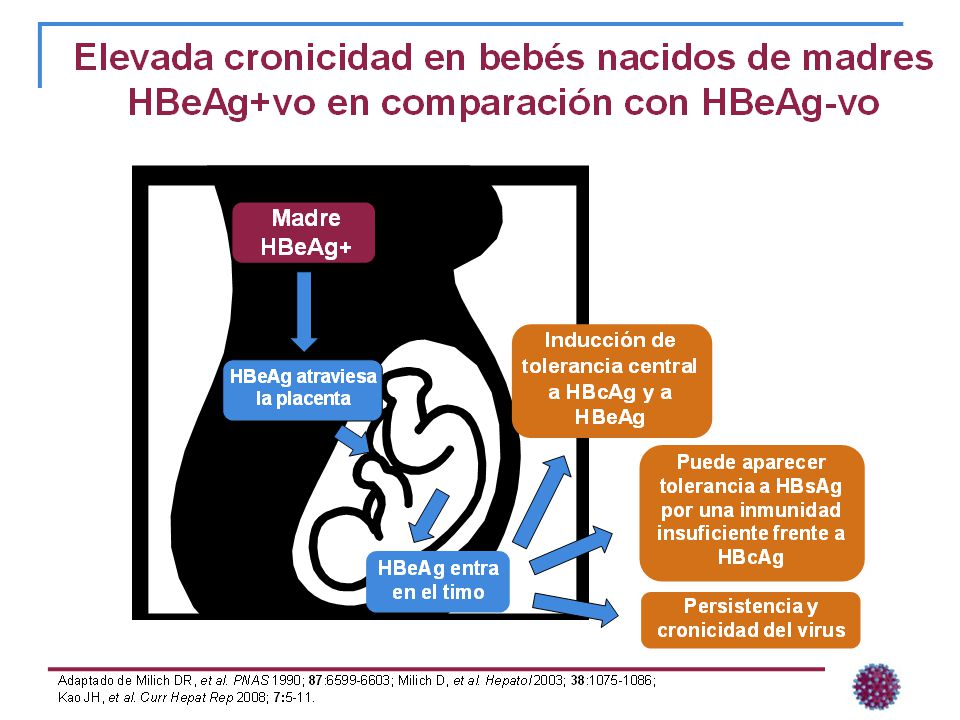
La transmisión vertical del VHB es posible a pesar de la inmunoprofilaxis en los niños si la madre tiene alta carga viral Es recomendable tratar a las gestantes con alta carga viral en el último trimestre para evitar la T.V. a pesar de la correcta inmunoprofilaxis del niño 81 madres AgHBe positivo Carga viral madre: 7 log log log Los niños: vacuna y gammaglobulina Tasa T.V. Ojo: población asiática 6.6% 14.6% 27.7% Wan-Hsin Wen. Journal of Hepatology 2013; 59: 24–30

22
Futuro: mecanismos de acción de IFN-Peg y NUCs
Fig. 1. Combination therapy may lead to restoration of both arms of the immune system, NK cells (top row) as well as CD8+ T cells (middle row), that are typically dysfunctional during chronic HBV infection and only partially restored by either therapy. Effects on human hepatocytes are shown in the bottom row: after cccDNAdriven transcription of the viral RNAs, the pregenomic RNA (pgRNA) is encapsidated and reverse transcribed by the HBV polymerase. Through Golgi and endoplasmatic reticulum the core particles acquire the envelope and are secreted. Transcription of the subgenomic HBV RNAs leads to the production of the envelope proteins, which are needed for virion secretion and to produce the non-infectious subviral particles (SVPs). While NUCs therapy efficiently suppresses HBV replication, IFN administration can also suppress cccDNA transcription and hence viral antigen production. It is intriguing to note that HBV-specific CD8+ T-cell functions could be restored, at least in part, after long-term treatment with NUCsThus, in contrast to lymphocytes isolated from IFN-treated patients, efficient suppression of HBV infection achieved after long-term treatment with NUCs may also favor some restoration of HBV-specific T-cell reactivity [32]. In contrast, NUC therapy was not shown to lead to a functional recovery of NK cells [27]. In sum, two very important conclusions can be drawn from these studies. First, PegIFNa and NUCs have differential effects on the innate and adaptive immune responses, and second, both drugs have shown some capabilities to restore impaired immune functions in chronic HBV infection. These results may have important clinical implications since they provide the rationale for a re-evaluation of combination therapy with PegIFNa and NUCs in chronic HBV infection. Indeed, it should be the goal of combination therapy to restore both arms of the immune system to improve the possibility of complete virus control. Combination therapy approaches that were evaluated in the past did not show improvement of post-therapy response rates [33,34]. It should be noted, however, that less potent NUCs were used in those studies and both therapies were started at the same time. The time schedule of therapy might indeed be a critical issue in this scenario, since NUC therapy typically requires several weeks until HBV replication is completely suppressed and months before the HBsAg levels begin to decrease. This is in sharp contrast to the treatment with PegIFNa, which can induce a much more rapid HBsAg decline; presumably by inducing both suppression of cccDNA transcription [15] and enhancement of TRAIL mediated cytotoxic effector functions against the infected hepatocytes [24]. Furthermore, combination therapy based on the use of PegIFNa and polymerase inhibitors has already revealed its stronger capacity in reducing the amounts of HBcAg-positive hepatocytes and cccDNA loads, compared to monotherapy [35,36]. Combining these clinical observations with the novel immunological findings discussed above, it is tempting to speculate that a late add-on therapy of PegIFNa to an ongoing NUC administration might be most beneficial. According to this scenario, NUC therapy would first lead to strong suppression of viremia, thereby assisting restoration of HBV-specific CD8+ T cells and, subsequently, PegIFNa will be added to accelerate the decline of circulating and intrahepatic viral antigens [37] and to allow expansion of NK cells (Fig. 1). Journal of Hepatology 2013 vol. 58 j 205–209 Robert Thimme, Maura Dandri. Journal of Hepatology 2013
 as well as CD8+ T cells (middle row), that are typically dysfunctional during chronic HBV infection and only partially restored by either therapy. Effects on human hepatocytes are shown in the bottom row: after cccDNAdriven transcription of the viral RNAs, the pregenomic RNA (pgRNA) is encapsidated and reverse transcribed by the HBV polymerase. Through Golgi and endoplasmatic reticulum the core particles acquire the envelope and are secreted. Transcription of the subgenomic HBV RNAs leads to the production of the envelope proteins, which are needed for virion secretion and to produce the non-infectious subviral particles (SVPs). While NUCs therapy efficiently suppresses HBV replication, IFN administration can. also suppress cccDNA transcription and hence viral antigen production. It is intriguing to note that HBV-specific CD8+ T-cell functions could be restored, at least in part, after long-term treatment with NUCsThus, in contrast to lymphocytes isolated from IFN-treated patients, efficient suppression of HBV infection achieved after long-term treatment with NUCs may also favor some restoration of HBV-specific T-cell reactivity [32]. In contrast, NUC therapy was not shown to lead to a functional recovery of NK cells [27]. In sum, two very important conclusions can be drawn from these studies. First, PegIFNa and NUCs have differential effects on the innate and adaptive immune responses, and second, both drugs have shown some capabilities to restore impaired immune functions in chronic HBV infection. These results may have important clinical implications since they provide the rationale for a re-evaluation of combination therapy with PegIFNa and NUCs in chronic HBV infection. Indeed, it should be the goal of combination therapy to restore both arms of the immune system to improve the possibility of complete virus control. Combination therapy approaches that were evaluated in the past did not show improvement of post-therapy response rates [33,34]. It should be noted, however, that less potent NUCs were used in those studies and both therapies were started at the same time. The time schedule of therapy might indeed be a critical issue in this scenario, since NUC therapy typically requires several weeks until HBV replication is completely suppressed and months before the HBsAg levels begin to decrease. This is in sharp contrast to the treatment with PegIFNa, which can induce a much more rapid HBsAg decline; presumably by inducing both suppression of cccDNA transcription [15] and enhancement of TRAIL mediated cytotoxic effector functions against the infected hepatocytes [24]. Furthermore, combination therapy based on the use of PegIFNa and polymerase inhibitors has already revealed its stronger capacity in reducing the amounts of HBcAg-positive hepatocytes and cccDNA loads, compared to monotherapy [35,36]. Combining these clinical observations with the novel immunological findings discussed above, it is tempting to speculate that a late add-on therapy of PegIFNa to an ongoing NUC administration might be most beneficial. According to this scenario, NUC therapy would first lead to strong suppression of viremia, thereby assisting restoration of HBV-specific CD8+ T cells and, subsequently, PegIFNa will be added to accelerate the decline of circulating and intrahepatic viral antigens [37] and to allow expansion of NK cells (Fig. 1). Journal of Hepatology 2013 vol. 58 j 205–209. Robert Thimme, Maura Dandri. Journal of Hepatology")
23
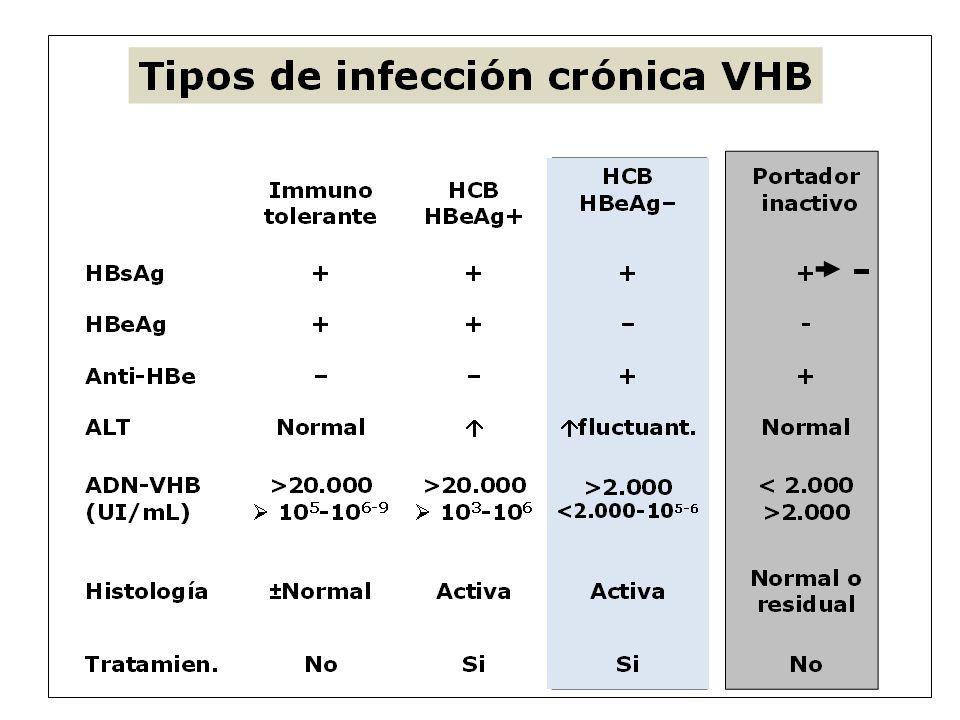
Figura 1. Historia natural y los tipos de infección crónica: desde la fase de Inmunotolerancia, de dudosa indicación de tratamiento, hasta el Portador Inactivo. Los pacientes infectados por transmisión vertical pasan una fase de inmunotolerancia (alta replicación viral con ALT normal) muy larga (años). En cambio, los infectados en la edad adulta esta fase es más corta. La indicación de tratamiento es en la actualidad durante la fase de hepatitis crónica o la cirrosis hepática, no obstante, se están iniciando ensayos clínicos en la fase de inmunotolerancia.
 muy larga (años). En cambio, los infectados en la edad adulta esta fase es más corta. La indicación de tratamiento es en la actualidad durante la fase de hepatitis crónica o la cirrosis hepática, no obstante, se están iniciando ensayos clínicos en la fase de inmunotolerancia.")
24
Δ Ishak Fibrosis Score over 5 Years
Change in Ishak Scores at Year 5 for Patients with Cirrhosis at Baseline In subjects with cirrhosis at baseline (Ishak fibrosis score 5-6), 74% (71/96) experienced reversal of cirrhosis at Week 240; 70/96 showed a reduction in Ishak fibrosis score of at least 2 points Δ Ishak Fibrosis Score over 5 Years Marcellin P, et al. The Lancet 2012; Published ahead of print: /S (12)
, 74% (71/96) experienced reversal of cirrhosis at Week 240; 70/96 showed a reduction in Ishak fibrosis score of at least 2 points. Δ Ishak Fibrosis Score over 5 Years. Marcellin P, et al. The Lancet 2012; Published ahead of print: /S (12)")
25
357. Results Comparison of HCC cumulative incidence rates between the ETV-treated group and the non-treated control group after PS matching Control (n=316) ETV (n=316) Log-rank test: p<0.001 Treatment duration (yr) Cumulative development rates of HCC (%) 1 3 5 7 10 20 30 40 50 4.0% 7.2% 10.0% 13.7% 3.7% 2.5% 1.2% 0.7% 316 277 246 223 200 187 170 2 44 101 185 264 No at risk ETV Control Hosaka T, et al. AASLD 2012, Boston, MA. Poster 357. Available at: long-term.entecavir.treatment.reduces.hepatocellular.carcinoma.html?history_id=61579 [Accessed November 2012].
 ETV (n=316) Log-rank test: p< Treatment duration (yr) Cumulative development rates of HCC (%) % 7.2% 10.0% 13.7% 3.7% 2.5% 1.2% 0.7% No at risk. ETV. Control. Hosaka T, et al. AASLD 2012, Boston, MA. Poster 357. Available at: long-term.entecavir.treatment.reduces.hepatocellular.carcinoma.html history_id=61579 [Accessed November 2012].")
26
ALT± normal (zona gris)
")
27
Entecavir. Respuesta virológica (DNA-VHB negativo) a los 5 años de tratamiento en pacientes AgHBe positivo y negativo HBeAg(+) HBeAg(-) 100% 100% 97% 98% 98% 100 100 96% 88% 88% 90% 74% 80 80 63% 60 60 Patients % Patients % 38% 40 40 20 20 6 12 24 36 48 60 Months 6 12 24 36 48 60 Patients on follow up 67 66 48 42 32 11 338 327 296 265 227 86 Lampertico P, et al. AASLD 2012, Boston, MA. Poster 366. Available at lampertico.entecavir.treatment.for.nuc.na.field.practice.patients.with.html?history_id= [Accessed November 2012]
 HBeAg(-) 100% 100% 97% 98% 98% % 88% 88% 90% 74% % Patients % Patients % 38% Months Patients. on follow up Lampertico P, et al. AASLD 2012, Boston, MA. Poster 366. Available at lampertico.entecavir.treatment.for.nuc.na.field.practice.patients.with.html history_id= [Accessed November 2012]")
28
Reactivación en pacientes con infección crónica por VHB sometidos a tratamiento citostático o inmunosupresor Tratamiento citostático/ inmunosupresor Tiempo (semanas) ADN VHB (log 10 copias /ml) ALT (UI/L) HBsAg
 ADN VHB (log 10 copias /ml) ALT (UI/L) HBsAg.")
29
Recomendaciones para las pacientes previamente tratadas en estado de gestación
No hay un consenso general Si la hepatopatía NO es avanzada, parar el tratamiento y monitorizar el DNA y ALT en la gestación y restaurar el tratamiento en el pos-parto Si la hepatopatía es avanzada, cambiar a fármacos de la categoría B, si no los tenía, y continuar el tratamiento SE HA CAMBIADO Fármacos categoría B: tenofovir o telbivudina

30
Diferencias más importantes entre el IFN-peg y los NUC
Interferón pegilado Núcleos(t)idos Vía administración Subcutánea Oral Tolerancia Mala Excelente Duración tratamiento 48 semanas Indefinida >80% Supresión máxima DNA log10 4.5 6.9 Genotipo A (AgHBe +vo) Cualquier genotipo Efectividad si DNA>109UI/ml + +++ Seroconversión AgHBe 1 año ~30% ~20% Seroconversión AgHBe >1 año No disponible 30-50% Perdida de AgHBs 1 año 3%-4% 0%-3% (2 años: 3-5%) Resistencias Nula LAM++++ TBV+++ ADV++ ETV- TDF- CH compensada No recomendable Retrasa descompensación CH descompensada Contraindicado Puede salvar la vida Coste/ 1 año 8.318 € (α-2a) ETV € (0.5 mg) TDV €
idos. Vía administración. Subcutánea. Oral. Tolerancia. Mala. Excelente. Duración tratamiento. 48 semanas. Indefinida >80% Supresión máxima DNA log Genotipo. A (AgHBe +vo) Cualquier genotipo. Efectividad si DNA>109UI/ml Seroconversión AgHBe 1 año. ~30% ~20% Seroconversión AgHBe >1 año. No disponible % Perdida de AgHBs 1 año. 3%-4% 0%-3% (2 años: 3-5%) Resistencias. Nula. LAM++++ TBV+++ ADV++ ETV- TDF- CH compensada. No recomendable. Retrasa descompensación. CH descompensada. Contraindicado. Puede salvar la vida. Coste/ 1 año € (α-2a) ETV € (0.5 mg) TDV €")
31
Razones para su tratamiento: muy infectivos y posibilidad de CHC
Patients with HBV-DNA <69 UI/ml at wk 192 Razones para su tratamiento: muy infectivos y posibilidad de CHC El tratamiento con tenofovir (TDF) y aún más el Tenofovir más Entricibabina (TDF/FTC) fue efectivo, sobre todo en mujeres. Chan HL et al. EASL 2013
 y aún más el Tenofovir más Entricibabina (TDF/FTC) fue efectivo, sobre todo en mujeres. Chan HL et al. EASL")
Presentaciones similares