Descargar la presentación
La descarga está en progreso. Por favor, espere

1
MSc. Susana Quirós Cognuck
Glándula Suprarrenal MSc. Susana Quirós Cognuck

2
Guía de estudio Objetivo terminal:
Caracterizar los mecanismos que regulan la liberación de las hormonas adrenocorticales y las catecolaminas y analizar, en forma integrada, todas las acciones fisiológicas de dichas hormonas.

3
Anatomía

4
Figure 50-1 Anatomy of the adrenal gland
Figure 50-1 Anatomy of the adrenal gland. An adrenal gland sits on each kidney. The adrenal gland is actually two glands-the cortex and the medulla. The adrenal cortex comprises three layers that surround the medulla. The outermost layer contains the glomerulosa cells that secrete aldosterone, and the two inner layers of cortex (fasciculata and reticularis) synthesize cortisol and sex steroids. The blood supply enters the cortex in the subcapsular region and flows through anastomotic capillary beds while coursing through both the cortex and the medulla. The adrenal medulla contains chromaffin cells that secrete epinephrine and a small amount of norepinephrine. Cada glándula pesa aproximadamente 4 g. Se localizan en el polo superior de cada riñón, en el espacio retroperitoneal. Cada glándula está compuesta por la capsula, corteza y médula. Embriologicamente, la corteza es derivada del mesodermo mientras que la medula de las células de la cresta neural. DHEA: dehydroepiandrosterone
 synthesize cortisol and sex steroids. The blood supply enters the cortex in the subcapsular region and flows through anastomotic capillary beds while coursing through both the cortex and the medulla. The adrenal medulla contains chromaffin cells that secrete epinephrine and a small amount of norepinephrine. Cada glándula pesa aproximadamente 4 g. Se localizan en el polo superior de cada riñón, en el espacio retroperitoneal. Cada glándula está compuesta por la capsula, corteza y médula. Embriologicamente, la corteza es derivada del mesodermo mientras que la medula de las células de la cresta neural. DHEA: dehydroepiandrosterone.")
5
Circulación en la glándula
The adrenal glands sit on the superior poles of the kidneys and receive a rich arterial supply from the inferior, middle, and superior suprarenal arteries. The adrenals are drained by a single suprarenal vein.

6
Figure 42-3 Blood flow through the adrenal gland
Figure 42-3 Blood flow through the adrenal gland. Capsular arteries give rise to sinusoidal vessels that carry blood centripetally through the cortex to the medulla. The medulla receives vascular input from vessels that begin in a subcapsular plexus of the adrenal cortex. The vessels then branch into a capillary network in the cortex only to merge into small venous vessels that branch into a second capillary network within the medulla. This portal blood supply exposes the adrenal medulla to the highest concentrations of glucocorticoids and mineralocorticoids of all somatic tissues.

7
Hormonas de la corteza suprarrenal

8
Esteroidogénesis Figure 42-8 Events involved in the first reaction in the steroidogenic pathway (conversion of cholesterol to pregnenolone) in zona fasciculata cells. ACAT, acyl CoA : cholesterol acyltransferase; CE, cholesterol esters; FC, free cholesterol; HDLR, high-density lipoprotein receptor (also called the scavenger receptor BI [SR-BI]); IMM, inner mitochondrial membrane; LDLR, low-density lipoprotein receptor; OMM, outer mitochondrial membrane; StAR, steroidogenic acute regulatory protein The zona fasciculata is an actively steroidogenic tissue composed of straight cords of large cells. These cells have a "foamy" cytoplasm because they are filled with lipid droplets that represent stored cholesterol esters. These cells make some cholesterol de novo but also import cholesterol from blood in the form of low-density lipoprotein (LDL) and high-density lipoprotein (HDL) particles. Free cholesterol is then esterified and stored in lipid droplets (Fig. 42-8). The adrenal gland has two sources of cholesterol: It can import cholesterol from circulating cholesterol containing low-density lipoprotein (LDL cholesterol) by means of LDL receptor-mediated endocytosis. MORE IMPORTANT. It can synthesize cholesterol de novo from acetate.
 in zona fasciculata cells. ACAT, acyl CoA : cholesterol acyltransferase; CE, cholesterol esters; FC, free cholesterol; HDLR, high-density lipoprotein receptor (also called the scavenger receptor BI [SR-BI]); IMM, inner mitochondrial membrane; LDLR, low-density lipoprotein receptor; OMM, outer mitochondrial membrane; StAR, steroidogenic acute regulatory protein. The zona fasciculata is an actively steroidogenic tissue composed of straight cords of large cells. These cells have a foamy cytoplasm because they are filled with lipid droplets that represent stored cholesterol esters. These cells make some cholesterol de novo but also import cholesterol from blood in the form of low-density lipoprotein (LDL) and high-density lipoprotein (HDL) particles. Free cholesterol is then esterified and stored in lipid droplets (Fig. 42-8). The adrenal gland has two sources of cholesterol: It can import cholesterol from circulating cholesterol containing low-density lipoprotein (LDL cholesterol) by means of LDL receptor-mediated endocytosis. MORE IMPORTANT. It can synthesize cholesterol de novo from acetate.")
9
Figure 50-2. Biosynthesis of adrenal steroids
Figure Biosynthesis of adrenal steroids. This schematic summarizes the synthesis of the adrenal steroids-the mineralocorticoid aldosterone and the glucocorticoid cortisol-from cholesterol. The individual enzymes are shown in the horizontal and vertical boxes; they are located in either the SER or the mitochondria. The SCC enzyme that produces pregnenolone is also known as 20,22-desmolase. The chemical groups modified by each enzyme are highlighted in the reaction product. If the synthesis of cortisol is prevented by any one of several dysfunctional enzymes, other steroid products may be produced in excess. For example, a block in 21α-hydroxylase diminishes production of both cortisol and aldosterone and increases production of the sex steroids. Certain of these pathways are shared in the biosynthesis of the androgens (see Fig. 54-5) and estrogens (see Fig. 55-9).d 11β-HSD1 is highly expressed in certain glucocorticoid target tissues, including liver and subcutaneous and visceral adipose tissue. 11β-HSD2 is expressed highly in the renal distal tubule and collecting duct.
 and estrogens (see Fig. 55-9).d. 11β-HSD1 is highly expressed in certain glucocorticoid target tissues, including liver and subcutaneous and visceral adipose tissue. 11β-HSD2 is expressed highly in the renal distal tubule and collecting duct.")
10
SER

11
Figure 42-9 Summary of the steroidogenic pathways for each of the three zones of the adrenal cortex. The enzymatic reactions are color-coded across zones. sER, smooth endoplasmic reticulum. The stored cholesterol is continually turned back into free cholesterol by a cholesterol ester hydrolyase, a process that is increased in response to the stimulus of cortisol synthesis (e.g., adrenocorticotropic hormone [ACTH]-see later). In the zona fasciculata, cholesterol is converted sequentially to pregnenolone, progesterone, 17-hydroxyprogesterone, 11-deoxycortisol, and cortisol (Figs and 42-10). A parallel pathway in the zona fasciculata involves the conversion of progesterone to 11-deoxycorticosterone (DOC) and then to corticosterone (Fig , C).
. In the zona fasciculata, cholesterol is converted sequentially to pregnenolone, progesterone, 17-hydroxyprogesterone, 11-deoxycortisol, and cortisol (Figs and 42-10). A parallel pathway in the zona fasciculata involves the conversion of progesterone to 11-deoxycorticosterone (DOC) and then to corticosterone (Fig , C).")
12
Cortisol

13
Figure 50-3 The hypothalamic-pituitary-adrenocortical axis
Figure 50-3 The hypothalamic-pituitary-adrenocortical axis. Small-bodied neurons in the paraventricular nucleus of the hypothalamus secrete CRH, a 41-amino acid peptide that reaches the corticotrophs in the anterior pituitary through the long portal veins. CRH binds to a GPCR on the corticotroph membrane, triggering the adenylyl cyclase/cAMP/PKA (AC/cAMP/PKA) pathway. The activation of L-type Ca2+ channels leads to an increase in [Ca2+]i that rapidly leads to the release of preformed ACTH. CRH also increases gene transcription and synthesis of the ACTH precursor, POMC. After its release by corticotrophs, ACTH binds to MC2Rs on the cell membranes in all three layers of the adrenal cortex. This receptor triggers the AC/cAMP/PKA pathway, thus rapidly enhancing the conversion of cholesterol to pregnenolone and more slowly increasing the synthesis of several proteins that are needed for cortisol synthesis. The cerebral cortex can stimulate the hypothalamic neurons to increase their secretion of CRH. Cortisol exerts negative feedback at the level of both the pituitary and hypothalamus. In addition, ACTH produced by the corticotrophs negatively feeds back on the hypothalamic neurons in a short loop. ACTH can be produced by small cell carcinomas of the lung.
 pathway. The activation of L-type Ca2+ channels leads to an increase in [Ca2+]i that rapidly leads to the release of preformed ACTH. CRH also increases gene transcription and synthesis of the ACTH precursor, POMC. After its release by corticotrophs, ACTH binds to MC2Rs on the cell membranes in all three layers of the adrenal cortex. This receptor triggers the AC/cAMP/PKA pathway, thus rapidly enhancing the conversion of cholesterol to pregnenolone and more slowly increasing the synthesis of several proteins that are needed for cortisol synthesis. The cerebral cortex can stimulate the hypothalamic neurons to increase their secretion of CRH. Cortisol exerts negative feedback at the level of both the pituitary and hypothalamus. In addition, ACTH produced by the corticotrophs negatively feeds back on the hypothalamic neurons in a short loop. ACTH can be produced by small cell carcinomas of the lung.")
14
CRH is present in sevaral tissues, including the pancreas, testes and CNS.
Arginine vasopressin is a potent ACTH secretagogue, It probably plays a physiological role in the regulation of ACTH secretion in various stress states. In the corticotrophs of the anterior pituitary, cortisol acts by binding to a cytosolic receptor, which then moves to the nucleus, where it binds to GREs (glucocorticoid response elements) and modulates gene expression and thus inhibits the synthesis of both the CRH receptor and ATCH. Eleved levels of cortisol in plasma inhibit the release of presynthesized ACTH store in vesicles. Plasma cortisol decrease the mRNA and peptide levels of CRH in paraventricular hypothalamic neurons. Cortisol inhibits the release of presynthesized CRH.
 and modulates gene expression and thus inhibits the synthesis of both the CRH receptor and ATCH. Eleved levels of cortisol in plasma inhibit the release of presynthesized ACTH store in vesicles. Plasma cortisol decrease the mRNA and peptide levels of CRH in paraventricular hypothalamic neurons. Cortisol inhibits the release of presynthesized CRH.")
15
Figure 50-4 The primary gene transcript is the preprohormone POMC
Figure 50-4 The primary gene transcript is the preprohormone POMC. The processing of POMC yields a variety of peptide hormones. This processing is different in the anterior and intermediate lobes of the pituitary. In the anterior pituitary, POMC yields a long N-terminal peptide, a joining (J) peptide, ACTH, and β-LPH. In the intermediate pituitary, the same POMC yields a short N-terminal peptide, γ-MSH, J peptide, α-MSH, CLIP, γ-LPH, and β-endorphin. Metabolism by the intermediate lobe is only important during fetal life and pregnancy. (Data from Young JB, Landsberg L: Catecholamines and the adrenal medulla. In Wilson JD, Foster DW, Kronenberg HM, Larsen PR (eds): Williams Textbook of Endocrinology, 9th ed, pp Philadelphia: WB Saunders, 1998.) β-LPH: beta lipotropin POMC is also sinthesized by the appetite-controlling POMC neurons in the hypothalamus. Melanocortins include: ACTH, α-, β-, γ-MSH
 peptide, ACTH, and β-LPH. In the intermediate pituitary, the same POMC yields a short N-terminal peptide, γ-MSH, J peptide, α-MSH, CLIP, γ-LPH, and β-endorphin. Metabolism by the intermediate lobe is only important during fetal life and pregnancy. (Data from Young JB, Landsberg L: Catecholamines and the adrenal medulla. In Wilson JD, Foster DW, Kronenberg HM, Larsen PR (eds): Williams Textbook of Endocrinology, 9th ed, pp Philadelphia: WB Saunders, 1998.) β-LPH: beta lipotropin. POMC is also sinthesized by the appetite-controlling POMC neurons in the hypothalamus. Melanocortins include: ACTH, α-, β-, γ-MSH.")
16
Figure Overview of the actions of ACTH on target adrenocortical cells. Note that the major second messenger, cAMP, activates immediate protein mediators and also induces the production of later protein mediators. HDL, high-density lipoprotein; LDL, low-density lipoprotein. ACTH binds to the melanocortin 2 receptor (MC2R) located on cells in the zona fasciculata. The effects of ACTH can be subdivided into three phases: The acute effects of ACTH occur within minutes. Cholesterol is rapidly mobilized from lipid droplets by posttranslational activation of cholesterol ester hydrolase and transported to the outer mitochondrial membrane. ACTH both rapidly increases steroidogenic acute regulatory (StAR) protein gene expression and activates StAR protein through protein kinase A (PKA)-dependent phosphorylation. Collectively, these acute actions of ACTH increase pregnenolone levels. The chronic effects of ACTH occur over a period of several hours. These effects involve increasing transcription of the genes encoding the steroidogenic enzymes and their coenzymes. ACTH also increases expression of the LDL receptor and scavenger receptor BI (SR-BI; the HDL receptor). Also, ACTH increase the synthesis of the 3-hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA) reductase that is the rate-limiting enzyme for cholesterol synthesis by the adrenal. The trophic actions of ACTH on the zona fasciculata and zona reticularis occur over a period of weeks and months. This effect is exemplified by atrophy of the zona fasciculata in patients receiving therapeutic (i.e., supraphysiological) levels of glucocorticoid analogues for at least 3 weeks. Under these conditions, the exogenous corticosteroids completely repress CRH and ACTH production, thereby resulting in atrophy of the zona fasciculata and a decline in endogenous cortisol production (Fig ). At the end of therapy, these patients need to be slowly weaned off exogenous glucocorticoids to allow the hypothalamus-pituitary-adrenal axis to reestablish itself and the zona fasciculata to enlarge and produce adequate amounts of cortisol.
 located on cells in the zona fasciculata. The effects of ACTH can be subdivided into three phases: The acute effects of ACTH occur within minutes. Cholesterol is rapidly mobilized from lipid droplets by posttranslational activation of cholesterol ester hydrolase and transported to the outer mitochondrial membrane. ACTH both rapidly increases steroidogenic acute regulatory (StAR) protein gene expression and activates StAR protein through protein kinase A (PKA)-dependent phosphorylation. Collectively, these acute actions of ACTH increase pregnenolone levels. The chronic effects of ACTH occur over a period of several hours. These effects involve increasing transcription of the genes encoding the steroidogenic enzymes and their coenzymes. ACTH also increases expression of the LDL receptor and scavenger receptor BI (SR-BI; the HDL receptor). Also, ACTH increase the synthesis of the 3-hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA) reductase that is the rate-limiting enzyme for cholesterol synthesis by the adrenal. The trophic actions of ACTH on the zona fasciculata and zona reticularis occur over a period of weeks and months. This effect is exemplified by atrophy of the zona fasciculata in patients receiving therapeutic (i.e., supraphysiological) levels of glucocorticoid analogues for at least 3 weeks. Under these conditions, the exogenous corticosteroids completely repress CRH and ACTH production, thereby resulting in atrophy of the zona fasciculata and a decline in endogenous cortisol production (Fig ). At the end of therapy, these patients need to be slowly weaned off exogenous glucocorticoids to allow the hypothalamus-pituitary-adrenal axis to reestablish itself and the zona fasciculata to enlarge and produce adequate amounts of cortisol.")
17
Otros receptores MC Receptor Proteína G asociada Distribución MC1 Gs
Presente en células de la piel, regula síntesis de eumelanina MC3 TGI, cerebro, corazón y placenta. Regulación energética MC4 Pituitaria, dermis. Inhibición de la ingesta de alimentos MC5 Tejido adiposo. Producción de sebo en ratones α-, and γ-MSH act on MC1R in melanocytes to increase the dispersion of pigment granules. Β-, and γ-MSH act on MC5R, mobilize lipids from adipocytes in animals, role in humans is unclear

18
Figure 50-5 Rhythm of ACTH and cortisol
Figure 50-5 Rhythm of ACTH and cortisol. The corticotrophs release ACTH in a circadian rhythm, greater in the early morning hours and less late in the afternoon and early evening. Superimposed on the circadian rhythm is the effect on the corticotrophs of the pulsatile secretion of CRH by the hypothalamus. Thus, ACTH levels exhibit both circadian and pulsatile behavior. Although both ACTH and cortisol are secreted episodically, the duration of the ACTH bursts is briefer, reflecting the shorter half-life of ACTH in plasma. (Data from Young JB, Landsberg L: Catecholamines and the adrenal medulla. In Wilson JD, Foster DW, Kronenberg HM, Larsen PR (eds): Williams Textbook of Endocrinology, 9th ed, pp Philadelphia: WB Saunders, 1998.) The pituitary secretes ACTH with a circadian rhytm. The suprachiasmatic nucleus of the hypothalamus, which lies above the optic chiasm and receives input from the retina, controls the circadian rhytm. The greatest ACTH secretory activity occurs in the early morning and diminishes late in the afternoon and early evening. CRH is released in pulses. Because the half life of cortisol is much longer the that of ACTH, the period of the pulsatile changes in cortisol is longer and the magnitude of the excursions is damped in comparison with those of ACTH.
: Williams Textbook of Endocrinology, 9th ed, pp Philadelphia: WB Saunders, 1998.) The pituitary secretes ACTH with a circadian rhytm. The suprachiasmatic nucleus of the hypothalamus, which lies above the optic chiasm and receives input from the retina, controls the circadian rhytm. The greatest ACTH secretory activity occurs in the early morning and diminishes late in the afternoon and early evening. CRH is released in pulses. Because the half life of cortisol is much longer the that of ACTH, the period of the pulsatile changes in cortisol is longer and the magnitude of the excursions is damped in comparison with those of ACTH.")
19
Transporte del cortisol
Transcortina 90% Albúmina 7% Libre 3% The interrelationships of free and bound cortisol. The dashed arrow indicates that cortisol inhibits ACTH secretion. The value for free cortisol is an approximation; in most studies, it is calculated by subtracting the protein-bound cortisol from the total plasma cortisol. Cortisol is bound in the circulation to anglobulin called transcortin or corticosteroid-binding globulin (CBG). A minor degree of binding to albumin also takes place. The half-life of cortisol in the circulation is about 60–90 min. Bound steroids is physiologically inactive. In addition, relatively little free cortisol is found in the urine because of protein binding. The bound cortisol functions as a circulating reservoir of hormone that keeps a supply of free cortisol available to the tissues. At normal levels of total plasma cortisol (13.5 ug/dL or 375 nmol/L), very little free cortisol is present in the plasma, but the binding sites on CBG become saturated when the total plasma cortisol exceeds 20 ug/dL. At higher plasma levels, binding to albumin increases, but the main increase is in the unbound fraction.
. A minor degree of binding to albumin also takes place. The half-life of cortisol in the circulation is about 60–90 min. Bound steroids is physiologically inactive. In addition, relatively little free cortisol is found in the urine because of protein binding. The bound cortisol functions as a circulating reservoir of hormone that keeps a supply of free cortisol available to the tissues. At normal levels of total plasma cortisol (13.5 ug/dL or 375 nmol/L), very little free cortisol is present in the plasma, but the binding sites on CBG become saturated when the total plasma cortisol exceeds 20 ug/dL. At higher plasma levels, binding to albumin increases, but the main increase is in the unbound fraction.")
20
Transcortina Proteína ligadora de corticosteroides (CBG)
Glicoproteína de 383 aa con afinidad por el cortisol 30 veces mayor que por la aldosterona Sintetizada en el hígado

21
Acción fisiológica del Cortisol
Acción en el aspecto psicológico Acción en el tracto gastrointestinal Acción metabólica Acción en el sistema reproductivo Acción en el desarrollo fetal Acción antiflamatoria e inmunosupresora Acción cardiovascular Acción en el hueso Acción en el tejido conectivo Acción en el músculo Acción en el riñón Effects of Cortisol on the Reproductive Systems Reproduction exacts a considerable anabolic cost on the organism. In humans, reproductive behavior and function are dampened in response to stress. Cortisol decreases the function of the reproductive axis at the hypothalamic, pituitary, and gonadal levels.

22
Acción antiflamatoria
Figure 2. Three General Mechanisms of Action of Glucocorticoids and the Glucocorticoid Receptor in the Inhibition of Inflammation. TNF-alpha denotes tumor-necrosis factor alpha, HSP heat-shock protein, mRNA messenger RNA, and P phosphate. The three mechanisms are nongenomic activation, DNA- dependent regulation, and protein interference mechanisms (e.g., NF-kB elements). Black arrows denote activation, the red line inhibition, the red dashed arrow repression, and the red X lack of product (i.e., no mRNA). Nuclear factor-kB (NF-kB): An inflammatory transcription factor composed of two polypeptides from the Rel family of proteins. In the nucleus, NF-kB binds DNA sequences called NF-kB elements and stimulates the transcription of cytokines, chemokines, cell adhesion molecules, complement factors, and receptors for these molecules. NF-kB also induces the transcription of cyclooxygenase 2, an enzyme essential for prostaglandin production. The glucocorticoid receptor (GR) is primarily located in the cytoplam, where in its unbound form it is complexed to a chaperone protein. Binding of cortisol causes the chaperone to dissociate from the GR and thus allows the cortisol-GR complex to translocate to the nucleus. In the nucleus cortisol-receptor complex associates with glucocorticoid response elements (GREs) on the 5´untraslated region of multiple genes to either enhance or diminish gene expression. Activity of the glucocorticoid-receptor complex requires dimerization of two identical receptor complexes at the near-polindromic nucleotide site of the GRE on the chromatin.
. Black arrows denote activation, the red line inhibition, the red dashed arrow repression, and the red X lack of product (i.e., no mRNA). Nuclear factor-kB (NF-kB): An inflammatory transcription factor composed of two polypeptides from the Rel family of proteins. In the nucleus, NF-kB binds DNA sequences called NF-kB elements and stimulates the transcription of cytokines, chemokines, cell adhesion molecules, complement factors, and receptors for these molecules. NF-kB also induces the transcription of cyclooxygenase 2, an enzyme essential for prostaglandin production. The glucocorticoid receptor (GR) is primarily located in the cytoplam, where in its unbound form it is complexed to a chaperone protein. Binding of cortisol causes the chaperone to dissociate from the GR and thus allows the cortisol-GR complex to translocate to the nucleus. In the nucleus cortisol-receptor complex associates with glucocorticoid response elements (GREs) on the 5´untraslated region of multiple genes to either enhance or diminish gene expression. Activity of the glucocorticoid-receptor complex requires dimerization of two identical receptor complexes at the near-polindromic nucleotide site of the GRE on the chromatin.")
23
Acción antiflamatoria
Figure 4. Partial Molecular Architecture Underlying the Glucocorticoid-Induced Antagonism of Inflammation. Inflammatory pathways are characterized by positive feedback loops (i.e., cytokines activate NF-kB, which in turn stimulates the synthesis of more cytokines) and by redundancy (i.e., cytokines also activate c-Jun–Fos). The glucocorticoid receptor inhibits these pathways at multiple points by directly blocking the transcription of inflammatory proteins by NF-kB and activator protein 1 and by inducing the expression of antiinflammatory proteins such as IkB, annexin I, and MAPK phosphatase I. 5-LOX denotes 5-lipoxygenase, and COX-2 cyclooxygenase 2. Red lines denote inhibition, and black arrows activation. An interactive version of this figure is available with the full text of the article at The inflammatory response to injury consists of local dilation of capillaries and increased capillary permeability with resultant local edema and accumulation of white blood cells. These steps are mediated by prostaglandins, thromboxanes, and leukotrienes. Cortisol inhibits phospholipase A2, a key enzyme in prostaglandin, leukotriene, and thromboxane synthesis.
 and by redundancy (i.e., cytokines also activate c-Jun–Fos). The glucocorticoid receptor inhibits these pathways at multiple points by directly blocking the transcription of inflammatory proteins by NF-kB and activator protein 1 and by inducing the expression of antiinflammatory proteins such as IkB, annexin I, and MAPK phosphatase I. 5-LOX denotes 5-lipoxygenase, and COX-2 cyclooxygenase 2. Red lines denote inhibition, and black arrows activation. An interactive version of this figure is available with the full text of the article at The inflammatory response to injury consists of local dilation of capillaries and increased capillary permeability with resultant local edema and accumulation of white blood cells. These steps are mediated by prostaglandins, thromboxanes, and leukotrienes. Cortisol inhibits phospholipase A2, a key enzyme in prostaglandin, leukotriene, and thromboxane synthesis.")
24
Acción inmunosupresora
CORTISOL Inhibe quimiotaxis Estabiliza membranas lisosomales Promueve la liberación de neutrófilos desde la médula ósea Inhibe actividad fagocitítica de los neutrófilos Antiinflammatory and Immunosuppressive Actions Inflammation and immune responses are often part of the response to stress. However, inflammation and immune responses have the potential for significant harm and may cause death if they are not held in homeostatic balance. As a stress hormone, cortisol plays an important role in maintaining immune homeostasis. Cortisol, along with epinephrine and norepinephrine, represses the production of proinflammatory cytokines and stimulates the production of antiinflammatory cytokines Cortisol also stabilizes lysosomal membranes, thereby decreasing release of the proteolytic enzymes that augment local swelling. In response to injury, leukocytes normally migrate to the site of injury and leave the vascular system. These effects are inhibited by cortisol, as is the phagocytic activity of neutrophils, although release of neutrophils from bone marrow is stimulated. Analogues of glucocorticoid are frequently used pharmacologically because of their antiinflammatory properties. Cortisol inhibits the immune response, and for this reason glucocorticoid analogues have been used as immunosuppressants in organ transplants. High cortisol levels decrease the number of circulating T lymphocytes (particularly helper T lymphocytes) and reduce their ability to migrate to the site of antigenic stimulation. Glucocorticoids promote atrophy of the thymus and other lymphoid tissue. Although corticosteroids inhibit cellular-mediated immunity, antibody production by B lymphocytes is not impaired. Inhibe el número de linfocitos TH Cortisol a niveles suprafisiológicos Reduce la habilidad de los linfocitos TH de llegar a los Ags Atrofia de timo y otros tejidos linfoides
 and reduce their ability to migrate to the site of antigenic stimulation. Glucocorticoids promote atrophy of the thymus and other lymphoid tissue. Although corticosteroids inhibit cellular-mediated immunity, antibody production by B lymphocytes is not impaired. Inhibe el número de linfocitos TH. Cortisol a niveles suprafisiológicos. Reduce la habilidad de los linfocitos TH de llegar a los Ags. Atrofia de timo y otros tejidos linfoides.")
25
Estimula síntesis de EPO
Acción cardiovascular Cortisol CATECOLAMINAS Mantiene el GC ↑ tono arteriolar ↑ PA Estimula síntesis de EPO Cardiovascular Actions Cortisol has permissive actions on catecholamines and thereby contributes to cardiac output and blood pressure. Cortisol stimulates erythropoietin synthesis and hence increases red blood cell production. Anemia occurs when cortisol is deficient, and polycythemia occurs when cortisol levels are excessive. Cortisol reinforces its effects on blood glucose by its positive effects on the cardiovascular system.

26
Acción en el hueso Effects of Cortisol on Bone
Glucocorticoids increase bone resorption. They have multiple actions that alter bone metabolism. Glucocorticoids decrease intestinal Ca++ absorption and renal Ca++ reabsorption. Both mechanisms serve to lower serum [Ca++]. As serum [Ca++] drops, secretion of parathyroid hormone (PTH) increases, and PTH mobilizes Ca++ from bone by stimulating resorption of bone. In addition to this action, glucocorticoids directly inhibit osteoblast bone-forming functions (see Chapter 39). Although glucocorticoids are useful for treating the inflammation associated with arthritis, excessive use will result in bone loss (osteoporosis). RANK: receptor por activación de NF-κB RANKL: ligando para el RANK
 increases, and PTH mobilizes Ca++ from bone by stimulating resorption of bone. In addition to this action, glucocorticoids directly inhibit osteoblast bone-forming functions (see Chapter 39). Although glucocorticoids are useful for treating the inflammation associated with arthritis, excessive use will result in bone loss (osteoporosis). RANK: receptor por activación de NF-κB. RANKL: ligando para el RANK.")
27
Inhibe proliferación de fibroblastos y formación de colágeno
Cortisol Inhibe proliferación de fibroblastos y formación de colágeno Acción en el tejido conectivo Actions of Cortisol on Connective Tissue Cortisol inhibits fibroblast proliferation and collagen formation. In the presence of excessive amounts of cortisol, the skin thins and is more readily damaged. The connective tissue support of capillaries is impaired, and capillary injury, or bruising, is increased.

28
Hiperpolariza la membrana, haciendo su estimulación más difícil
Journal of Endocrinology (2008) 197, 1–10 Niveles ↑ cortisol Proteolísis Acción en el músculo esquelético Dolor Debilidad Hipokalemia Hiperpolariza la membrana, haciendo su estimulación más difícil Actions of Cortisol on Muscle When cortisol levels are excessive, muscle weakness and pain are common symptoms. The weakness has multiple origins. In part, it is a result of the excessive proteolysis that cortisol produces. High cortisol levels can result in hypokalemia (via mineralocorticoid actions), which can produce muscle weakness because it hyperpolarizes and stabilizes the muscle cell membrane and thus makes stimulation more difficult. Figure 3 Local growth factors production plays a crucial role in glucocorticoid-induced muscle atrophy. Glucocorticoids can cause muscle atrophy by altering the muscle production of IGF-I and myostatin, two growth factors exhibiting opposite effects on muscle mass development. Decrease in IGF-I together with increase in myostatin both induced by glucocorticoids inhibit satellite cells activation as well as myoblast proliferation and differentiation. In mature muscle fibers, these growth factor changes cause down- regulation of protein synthesis and stimulation of protein degradation.
 197, 1–10. Niveles ↑ cortisol. Proteolísis. Acción en el músculo esquelético. Dolor. Debilidad. Hipokalemia. Hiperpolariza la membrana, haciendo su estimulación más difícil. Actions of Cortisol on Muscle. When cortisol levels are excessive, muscle weakness and pain are common symptoms. The weakness has multiple origins. In part, it is a result of the excessive proteolysis that cortisol produces. High cortisol levels can result in hypokalemia (via mineralocorticoid actions), which can produce muscle weakness because it hyperpolarizes and stabilizes the muscle cell membrane and thus makes stimulation more difficult. Figure 3 Local growth factors production plays a crucial role in glucocorticoid-induced muscle atrophy. Glucocorticoids can cause muscle atrophy by altering the muscle production of IGF-I and myostatin, two growth factors exhibiting opposite effects on muscle mass development. Decrease in IGF-I together with increase in myostatin both induced by glucocorticoids inhibit satellite cells activation as well as myoblast proliferation and differentiation. In mature muscle fibers, these growth factor changes cause down- regulation of protein synthesis and stimulation of protein degradation.")
29
Acción en el riñón ADH CORTISOL ↑ GC ↑ TFG
Actions of Cortisol on the Kidney Cortisol inhibits the secretion and action of antidiuretic hormone (ADH), and thus it is an ADH antagonist. In the absence of cortisol, the action of ADH is potentiated, which makes it difficult to increase free water clearance in response to a water load and increases the likelihood of water intoxication. Cortisol increases the glomerular filtration rate by both increasing cardiac output and acting directly on the kidney. Although cortisol binds to the mineralocorticoid receptor with high affinity, this action is normally blocked by inactivation of cortisol to cortisone by the enzyme 11β-HSD2. However, the mineralocorticoid activity (i.e., renal Na+ and H2O retention, K+ and H+ excretion) of cortisol depends on the relative amount of cortisol (or synthetic glucocorticoids) and the activity of 11β-HSD2. Certain agents (such as compounds in black licorice) inhibit 11β-HSD2 and thereby increase the mineralocorticoid activity of cortisol.
, and thus it is an ADH antagonist. In the absence of cortisol, the action of ADH is potentiated, which makes it difficult to increase free water clearance in response to a water load and increases the likelihood of water intoxication. Cortisol increases the glomerular filtration rate by both increasing cardiac output and acting directly on the kidney. Although cortisol binds to the mineralocorticoid receptor with high affinity, this action is normally blocked by inactivation of cortisol to cortisone by the enzyme 11β-HSD2. However, the mineralocorticoid activity (i.e., renal Na+ and H2O retention, K+ and H+ excretion) of cortisol depends on the relative amount of cortisol (or synthetic glucocorticoids) and the activity of 11β-HSD2. Certain agents (such as compounds in black licorice) inhibit 11β-HSD2 and thereby increase the mineralocorticoid activity of cortisol.")
30
Acción en el CNS Deficiencia de Cortisol Exceso de Cortisol
Puede provocar: Depresión Apatía Irritabilidad Inicialmente: Sensación de bienestar Posteriormente: Labilidad afectiva Insomnio ↓ sueño REM Psicosis franca Psychological Effects of Cortisol Psychiatric disturbances are associated with either excessive or deficient levels of corticosteroids. Excessive corticosteroids can initially produce a feeling of well-being, but continued excessive exposure eventually leads to emotional lability and depression. Frank psychosis can occur with either excessive or deficient hormone. Cortisol increases the tendency for insomnia and decreases rapid eye movement (REM) sleep. People who are deficient in corticosteroids tend to be depressed, apathetic, and irritable.
 sleep. People who are deficient in corticosteroids tend to be depressed, apathetic, and irritable.")
31
Acción en el tracto gastro intestinal
Hipercortisolismo Ausencia de Cortisol Acción en el tracto gastro intestinal ↓ la motilidad GI La mucosa GI degenera ↓ producción de enzimas y de ácido ↑ riesgo de desarrollo de úlceras Efecto trófico en la mucosa GI TGI Media la estimulación de secreción de pepsina y ácido gástrico CORTISOL Actions of Cortisol on the Gastrointestinal Tract Cortisol exerts a trophic effect on the GI mucosa. In the absence of cortisol, GI motility decreases, GI mucosa degenerates, and GI acid and enzyme production decreases. Because cortisol stimulates appetite, hypercortisolism is frequently associated with weight gain. The cortisol-mediated stimulation of gastric acid and pepsin secretion increases the risk for development of ulcers.

32
Acción Metabólica ↑ proteolísis ↓ síntesis proteica
↑ GLICEMIA ↑ Gluconeogénesis en hígado ↑ efecto de catecolaminas en lipólisis ↓ recaptura de glucosa en músculo mediada por GLUT 4 ↑ expresión de: PEPCK Fructosa 1,6 bifosfatasa Glucosa 6 fosfatasa CORTISOL PEPCK : fosfoenolpiruvato carboxikinasa

33
CORTISOL requerido para el desarrollo normal de
SNC Piel Retina TGI CORTISOL requerido para el desarrollo normal de Pulmón Induce a la diferenciación y maduración de las células alveolares tipo II Acción durante el desarrollo fetal Effects of Cortisol during Fetal Development Cortisol is required for normal development of the CNS, retina, skin, GI tract, and lungs. The best studied system is the lungs, in which cortisol induces differentiation and maturation of type II alveolar cells. During late gestation these cells produce surfactant, which reduces surface tension in the lungs and thus allows the onset of breathing at birth.

34
Figure 14-12 The principal sites of action of glucocorticoids in humans highlighting some of the consequences of glucocorticoid excess. CNS, Central nervous system; GI, gastrointestinal; FSH, follicle-stimulating hormone; GH, growth hormone; LH, luteinizing hormone; TSH, thyroid-stimulating hormone.

35
Aldosterona

36
Regulation of aldosterone release by the renin-angiotensin-aldosterone system. A decrease in the effective circulating blood volume triggers the release of renin from the juxtaglomerular apparatus in the kidney. Renin cleaves angiotensinogen, the hepatic precursor of angiotensin peptides, to form angiotensin I. Angiotensin I is converted to angiotensin II by angiotensin-converting enzyme (ACE), which is bound to the membrane of endothelial cells, predominantly in the pulmonary circulation. Angiotensin II is a potent vasoconstrictor and stimulates the production of aldosterone in the zona glomerulosa of the adrenal cortex. Aldosterone production is also stimulated by potassium, ACTH, norepinephrine, and endothelins.
, which is bound to the membrane of. endothelial cells, predominantly in the pulmonary circulation. Angiotensin II is a potent vasoconstrictor and. stimulates the production of aldosterone in the zona glomerulosa of the adrenal cortex. Aldosterone production is also stimulated by potassium, ACTH, norepinephrine, and endothelins.")
37
Transporte de la aldosterona
CBG ∼21% Albúmina ∼42% Libre ∼37% CBG: corticosteroid-binding globulin = transcortin

38
Figure 35-13B In B, 11β-HSD2 prevents cortisol (a glucocorticoid), which is present at high plasma concentrations, from having mineralocorticoid effects in the target cell. In C, with the enzyme blocked, cortisol acts as a mineralocorticoid. GR, glucocorticoid receptor.

39
Médula Adrenal

40
Catecolaminas Norepinefrina Epinefrina

41
Figure 50-8 A and B, Synthesis and degradation of catecholamines
Figure 50-8 A and B, Synthesis and degradation of catecholamines. In A, the horizontal arrows indicate enhancement of the reaction. MAO, monoamine oxidase. COMT, catecolamina-O-methyl transferase

42
Figure 50-9 Cellular view of catecholamine synthesis
Figure 50-9 Cellular view of catecholamine synthesis. The chromaffin cell synthesizes and stores epinephrine in a sequence of four enzymatic and three transport steps. AADC, amino acid decarboxylase; DA, dopamine; DBH, dopamine β-hydroxylase; Epi, epinephrine; NE, norepinephrine; TH, tyrosine hydroxylase; VMAT, vesicular monoamine transport; PNMT, phenylethanolamine-N- methyl-transferase

43
Regulación autocrina y paracrina de la liberación de catecolaminas
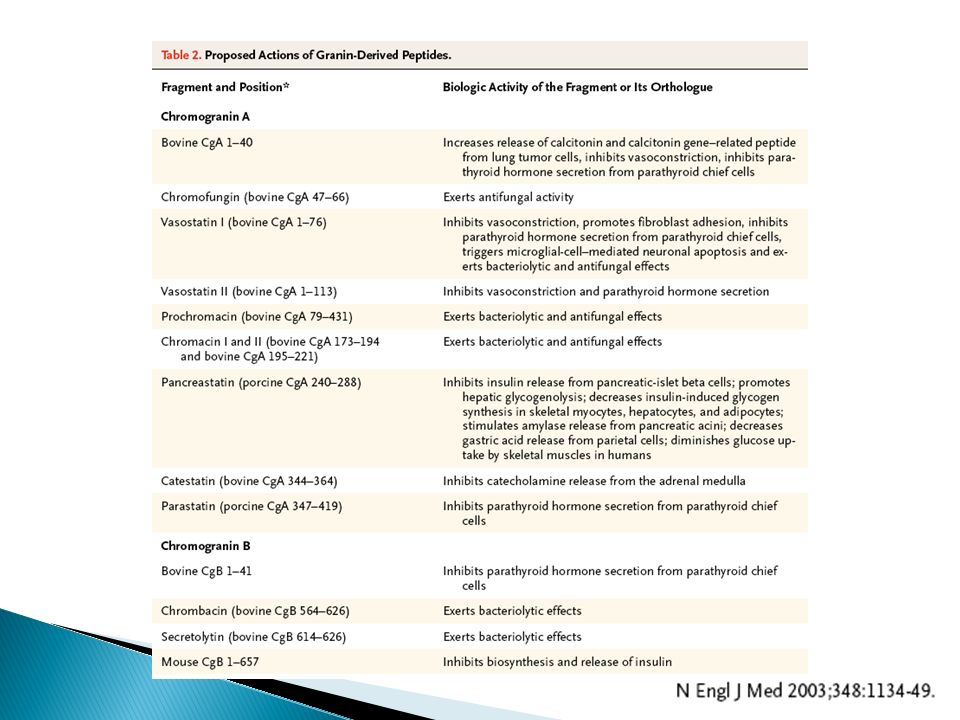
Figure 4. Autocrine–Paracrine Regulation of Catecholamine Release from Sympathoadrenal Chromaffin Cells by Catestatin. The physiologic secretagogue acetylcholine binds to the agonist pocket on the nicotinic cholinergic receptor, triggering sodium influx and consequent membrane depolarization, which activates calcium influx through voltage-gated channels and leads to exocytotic release of the chromaffin-granule cargo. After the cargo has been released, catestatin exerts potent antagonistic effects on nicotinic cholinergic signaling, resulting in negative-feedback modulation of catecholamine release. Arrows with plus signs indicate stimulation, and the arrow with a minus sign inhibition.

45
Figure 42-5 Stimuli that enhance the secretion of catecholamines.

46
Receptores adrenérgicos

47
Respuesta simpáticoadrenal al ejercicio
Figure 42-6 Some of the individual actions of catecholamines that contribute to the integrated sympathoadrenal response to exercise. An informative example of the major physiological roles of catecholamines is the sympathoadrenal response to exercise. Exercise is similar to the "fight or flight" response, but without the subjective element of fear, and involves a greater adrenomedullary response (i.e., endocrine role of epinephrine) than a sympathetic nervous response (i.e., neurotransmitter role of norepinephrine). The overall goal of the sympathoadrenal system during exercise is to meet the increased energy demands of skeletal and cardiac muscle while maintaining sufficient oxygen and glucose supply to the brain. The response to exercise includes the following major physiological actions of epinephrine (Fig. 42-6):Increased blood flow to muscles is achieved by the integrated action of norepinephrine and epinephrine on the heart, veins and lymphatics, and nonmuscular (e.g., splanchnic) and muscular arteriolar beds. Epinephrine promotes glycogenolysis in muscle. Exercising muscle can also utilize free fatty acids (FFAs), and epinephrine and norepinephrine promote lipolysis in adipose tissue. The actions just described increase circulating levels of lactate and glycerol, which can be used by the liver as gluconeogenic substrates to increase glucose. Epinephrine increases blood glucose by increasing hepatic glycogenolysis and gluconeogenesis. The promotion of lipolysis in adipose tissue is also coordinated with an epinephrine-induced increase in hepatic ketogenesis. Finally, the effects of catecholamines on metabolism are reinforced by the fact that they stimulate glucagon secretion (β2 receptors) and inhibit insulin secretion (α2 receptors). Efficient production of ATP during normal exercise (i.e., a 1-hour workout) also requires efficient exchange of gases with an adequate supply of oxygen to exercising muscle. Catecholamines promote this by relaxation of bronchiolar smooth muscle. Catecholamines decrease energy demand by visceral smooth muscle. In general, a sympathoadrenal response decreases overall motility of the smooth muscle in the gastrointestinal (GI) and urinary tracts, thereby conserving energy where it is not needed.
 than a sympathetic nervous response (i.e., neurotransmitter role of norepinephrine). The overall goal of the sympathoadrenal system during exercise is to meet the increased energy demands of skeletal and cardiac muscle while maintaining sufficient oxygen and glucose supply to the brain. The response to exercise includes the following major physiological actions of epinephrine (Fig. 42-6):Increased blood flow to muscles is achieved by the integrated action of norepinephrine and epinephrine on the heart, veins and lymphatics, and nonmuscular (e.g., splanchnic) and muscular arteriolar beds. Epinephrine promotes glycogenolysis in muscle. Exercising muscle can also utilize free fatty acids (FFAs), and epinephrine and norepinephrine promote lipolysis in adipose tissue. The actions just described increase circulating levels of lactate and glycerol, which can be used by the liver as gluconeogenic substrates to increase glucose. Epinephrine increases blood glucose by increasing hepatic glycogenolysis and gluconeogenesis. The promotion of lipolysis in adipose tissue is also coordinated with an epinephrine-induced increase in hepatic ketogenesis. Finally, the effects of catecholamines on metabolism are reinforced by the fact that they stimulate glucagon secretion (β2 receptors) and inhibit insulin secretion (α2 receptors). Efficient production of ATP during normal exercise (i.e., a 1-hour workout) also requires efficient exchange of gases with an adequate supply of oxygen to exercising muscle. Catecholamines promote this by relaxation of bronchiolar smooth muscle. Catecholamines decrease energy demand by visceral smooth muscle. In general, a sympathoadrenal response decreases overall motility of the smooth muscle in the gastrointestinal (GI) and urinary tracts, thereby conserving energy where it is not needed.")
Presentaciones similares








>")










