Descargar la presentación
La descarga está en progreso. Por favor, espere

1
ALTERNATIVAS A LA HISTERECTOMIA
Dr. Guido Parra Anaya Ginecólogo-Obstetra Congreso de Medicina Contemporánea 5 de Sept. del 2009 Hotel del Prado PROCREAR

2
Mioma Histerectomía ó miomectomia ??
> De histerectomías anuales en los EEUU Ayse GI et al.J Clin Endocrinol Metab 92: 1979–1982, 2007

3
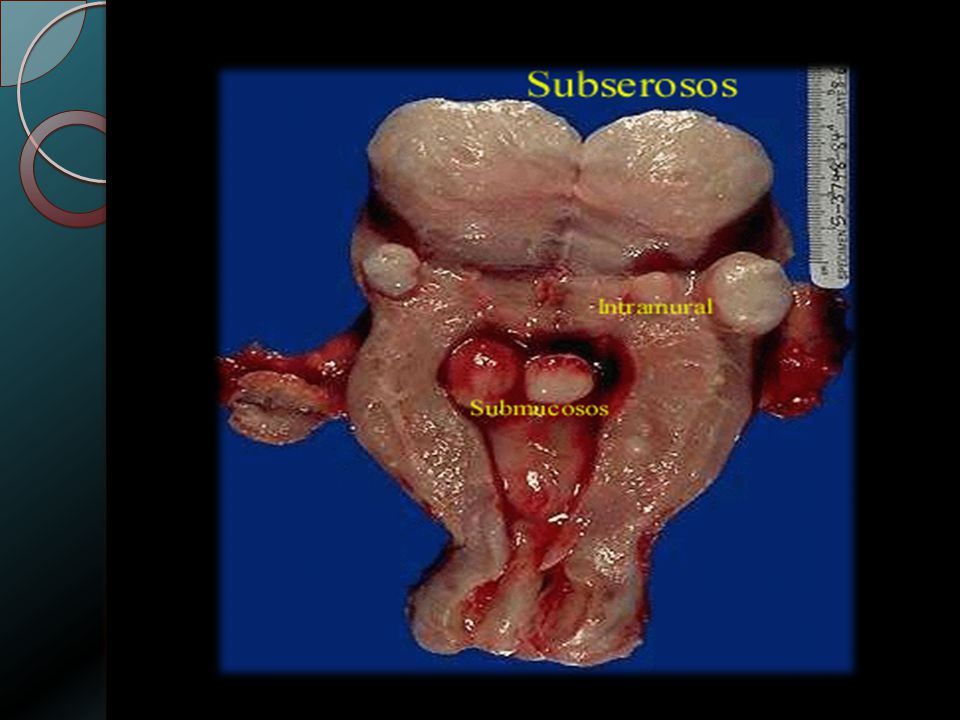
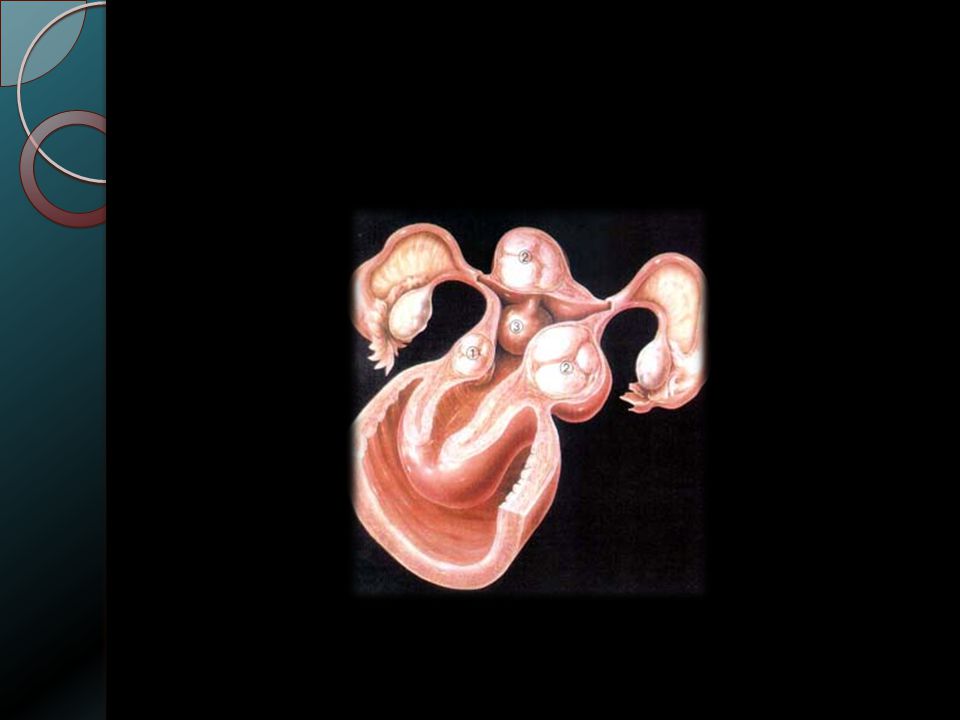
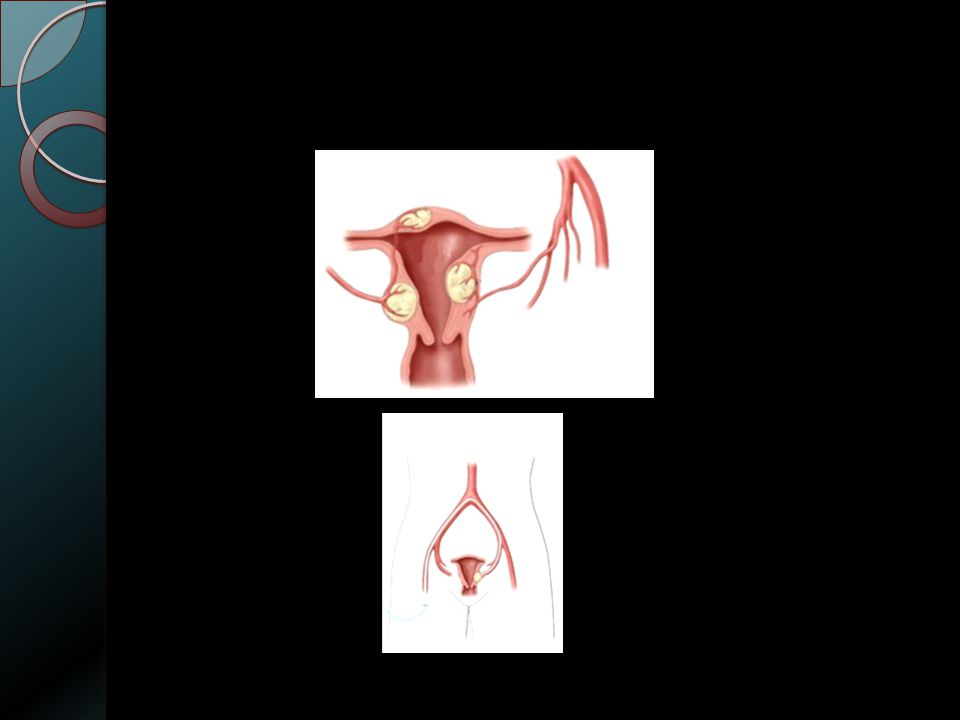
Miomas

4
Causas Benignas de Histerectomías
Miomas uterinos: la principal causa de histerectomías (Hipermenorrea, anemia, presión pélvica ) Incidencia a los 50 años Blancas =70% Negras= 80% Day BD et al…. ultrasound evidence.Am J Obstet Gynecol 2003;188:100–7. (Level II) Porqué ???? Único Tratamiento definitivo que elimina la posibilidad de recurrencia
 Incidencia a los 50 años. Blancas =70% Negras= 80% Day BD et al…. ultrasound evidence.Am J Obstet Gynecol 2003;188:100–7. (Level II) Porqué Único Tratamiento definitivo que elimina la posibilidad. de recurrencia.")
5
Vías para la Histerectomía
Abdominal: Laparotómica -Laparoscópica Vaginal: Tradicional - Asistida por laparoscopia

8
Causas de menorragia Idiopática (sin causa aparente) Miomas
Endometriosis / Adenomiosis Infecciones genitales Pólipos endometriales Hiperplasia de endometrio Enfermedades malignas Trastornos endocrinos o de la coagulación Algunos medicamentos Many women with menorrhagia have idiopathic or dysfunctional uterine bleeding with no obvious cause. However, an underlying cause for menorrhagia can be identified in some women, which can include those listed in this slide.

9
Alternativas Médicas Contraceptivos orales:
Estrógenos y progestinas ó progestinas solas 1ra. Línea para controlar sangrado anormal

10
Agonista de la Gn-Rh Reducción de miomas (35-65% en tres(3) meses, Aprobado por la FDA Efectos secundarios: -Síntomas menopáusicos -Impacto en la densidad mineral ósea Si se adicionan Progestinas reducción hasta del 95% en 24 horas Friedman AJ, Haas ST. Am J Obstet Gynecol 1993;168:751–5. (Level III)
")
11
Moduladores de la Progesterona
Mifepristone= reducción del Volumen del mioma % Steinauer J et al.Obstet Gynecol 2004;103:1331–6. (Level III) Efectos secundarios= Hiperplasia si atipias, elevación de las transaminasas Hepáticas Podrían jugar algún papel pre-operatoriamente
 Efectos secundarios= Hiperplasia si atipias, elevación de las transaminasas Hepáticas. Podrían jugar algún papel pre-operatoriamente.")
12
Inhibidores de las aromatasas
Bloquean la producción de estrógenos ováricos y de la periferia (impide el paso de C19 a estrógenos) (decrece los niveles de E2 después del 1er día de administración) Algunos estudios muestran reducción en los miomas (Varelas FK et al Obstet Gynecol 2007;110:643–9. (Level III) No esta aprobado su uso por la FDA
 (decrece los niveles de E2 después del 1er día de administración) Algunos estudios muestran reducción en los miomas. (Varelas FK et al Obstet Gynecol 2007;110:643–9. (Level III) No esta aprobado su uso por la FDA.")
13
DIU (LNG)
")
14
Qué es Mirena® ? Endoceptivo intrauterino
Liberador de levonorgestrel (20 µg/día) Un solo endoceptivo proporciona 5 años de tratamiento Mirena® consists of a T-shaped polyethylene frame (the T-body) with a steroid reservoir (hormone elastomer core) around the vertical stem. The reservoir consists of a cylinder, made of a mixture of levonorgestrel and silicone (polydimethylsiloxane), containing a total of 52 mg levonorgestrel. The reservoir is covered by a silicone (polydimethylsiloxane) membrane. The T-body is 32 mm in both the horizontal and vertical directions. The polyethylene of the T-body is compounded with barium sulphate, which makes it radio-opaque. A monofilament brown polyethylene removal thread is attached to a loop at the end of the vertical stem of the T-body. Levonorgestrel is a well-established progestogen, used in both contraception and HRT.
 Un solo endoceptivo proporciona 5 años de tratamiento. Mirena® consists of a T-shaped polyethylene frame (the T-body) with a steroid reservoir (hormone elastomer core) around the vertical stem. The reservoir consists of a cylinder, made of a mixture of levonorgestrel and silicone (polydimethylsiloxane), containing a total of 52 mg levonorgestrel. The reservoir is covered by a silicone (polydimethylsiloxane) membrane. The T-body is 32 mm in both the horizontal and vertical directions. The polyethylene of the T-body is compounded with barium sulphate, which makes it radio-opaque. A monofilament brown polyethylene removal thread is attached to a loop at the end of the vertical stem of the T-body. Levonorgestrel is a well-established progestogen, used in both contraception and HRT.")
15
DIU T de Cu MIRENA

16
Dificultades en la inserción 1998-2001 New Zealand
Mira Harrison-Woolrych, Lifeng Zhou and David Coulter NZMJ 8 August 2003,Vol116 (1179): 1-7
: 1-7.")
17
Dificultades Para Quitarlo

18
Reacciones a la inserción del endoceptivo
Mira Harrison-Woolrych, Lifeng Zhou and David Coulter NZMJ 8 August 2003,Vol116 (1179): 1-7
: 1-7.")
19
Levo-Norgestrel- Endoceptivo para Miomas
Resultado Bibliografía Efectos secundarios Pocos Marshall LM et al. Fertil Steril. 8;70:432–9. (Level II) Efecto endometrial local Elevado Wise LA et al. Am J Epidemiol 2004;159:113–23. (Level II-2) Control de sangrado en pacientes con Miomas Positivo Marjoribanks J et al. Cochrane Database of Systematic Reviews 2006, Issue 2. Art. No.: CD DOI: / CD pub2. (Level III) Rata de expulsión del endoceptivo (Miomas) Alto Mercorio F, et al. 2003;67:277–80.
 Efecto endometrial local. Elevado. Wise LA et al. Am J Epidemiol 2004;159:113–23. (Level II-2) Control de sangrado en pacientes con Miomas. Positivo. Marjoribanks J et al. Cochrane. Database of Systematic Reviews 2006, Issue 2. Art. No.: CD DOI: / CD pub2. (Level III) Rata de expulsión del endoceptivo (Miomas) Alto. Mercorio F, et al. 2003;67:277–80.")
21
Mirena® en Cicatriz de Cesárea
Hala FR et al. Int J Gynecol Pathol, Vol. 27, No. 1, January 2008

22
A= 6 meses B=12 meses C= 24 meses
LNG-IUS vs. Ablación endometrial

23
ABLACION ENDOMETRIAL Rolling Ball

24
Histerectomía por fallos en el DIU-LNG
Hala FR et al. Int J Gynecol Pathol, Vol. 27, No. 1, January 2008

25
Eficacia de Mirena® en la menorragia
Mirena reduce efectivamente la pérdida sanguínea menstrual (PSM) * p<0.001 % Reducción 200 150 PSM promedio (ml) 100 (80mL PSM = Menorragia) 50 * - 86% * Andersson and Rybo investigated the effects of Mirena on menstrual blood loss (MBL) in 20 parous women with menorrhagia [1]. The women studied were: aged up to 45 years; had regular periods; had no intermenstrual bleeding or spotting; and had normal or slightly enlarged uteri with no pelvic pathology. Menstrual blood loss was determined by analysis of all used tampons/pads using the alkaline haematin method. The reduction in menstrual blood loss after the insertion of Mirena (compared with the median of two consecutive baseline cycles) is shown in this figure. Median menstrual blood loss was significantly reduced by 86%, 91% and 97% at months 3, 6 and 12, respectively (p<0.001 ). Intermenstrual bleeding or spotting was common during the first 3 cycles, but the frequency diminished gradually with treatment. Reference 1. Andersson JK, Rybo G. Levonorgestrel-releasing intrauterine device in the treatment of menorrhagia. Br J Obstet Gynaecol. 1990; 97: 690-4 - 91% - 97% * Antes de 3 6 12 la inserción Meses de uso de Mirena Andersson and Rybo. Br J Obstet Gynaecol. 1990; 97: 690-4
 * p< % Reducción PSM promedio (ml) 100. (80mL PSM = Menorragia) 50. * - 86% * Andersson and Rybo investigated the effects of Mirena on menstrual blood loss (MBL) in 20 parous women with menorrhagia [1]. The women studied were: aged up to 45 years; had regular periods; had no intermenstrual bleeding or spotting; and had normal or slightly enlarged uteri with no pelvic pathology. Menstrual blood loss was determined by analysis of all used tampons/pads using the alkaline haematin method. The reduction in menstrual blood loss after the insertion of Mirena (compared with the median of two consecutive baseline cycles) is shown in this figure. Median menstrual blood loss was significantly reduced by 86%, 91% and 97% at months 3, 6 and 12, respectively (p<0.001 ). Intermenstrual bleeding or spotting was common during the first 3 cycles, but the frequency diminished gradually with treatment. Reference. 1. Andersson JK, Rybo G. Levonorgestrel-releasing intrauterine device in the treatment of menorrhagia. Br J Obstet Gynaecol. 1990; 97: % - 97% * Antes de la inserción. Meses de uso de Mirena. Andersson and Rybo. Br J Obstet Gynaecol. 1990; 97:")
26
Tto. para hiperplasia endometrial sin atipias n=15 pacientes, no miomas, útero<12 cmts. edad= 49 ± 2.7 años 100% Haimovich S et al, Menopause: The Journal of The North American Menopause Society 2008. Vol. 15, No. 5, pp. 1002/1004

27
Mirena® comparado con la histerectomía (2)
Una alta proporción de portadoras de Mirena® y aquellas a quienes se efectuó histerectomía estuvieron satisfechas o muy satisfechas con su tratamiento a 5 años de seguimiento 94 93 10 20 30 40 50 60 70 80 90 100 Mirena Histerectomía Proporción de satisfechas y muy satisfechas (%) Overall satisfaction with treatment was greater than 90% in both groups. Reference 1. Hurskainen R, Teperi J, Rissanen P, et al. Clinical outcomes and costs with the levonorgestrel-releasing intrauterine system or hysterectomy for treatment of menorrhagia: randomized trial 5-year follow-up. JAMA 2004; 291: Hurskainen et al. JAMA 2004; 291:
 Overall satisfaction with treatment was greater than 90% in both groups. Reference. 1. Hurskainen R, Teperi J, Rissanen P, et al. Clinical outcomes and costs with the levonorgestrel-releasing intrauterine system or hysterectomy for treatment of menorrhagia: randomized trial 5-year follow-up. JAMA 2004; 291: Hurskainen et al. JAMA 2004; 291:")
28
Mirena® comparado con la histerectomía (4)
Mirena es una atractiva alternativa frente a la histerectomía para el tratamiento de la menorragia Mirena: conserva la fertilidad es accesible en niveles primarios de atención evita el riesgo de los procedimientos quirúrgicos tiene una alta relación beneficio/costo Although hysterectomy provides a permanent solution to the problem of menorrhagia, it is associated with surgical complications and relatively high costs. Furthermore, it may not be the most appropriate treatment option for women wishing to retain future fertility. Removal of an anatomically normal uterus occurs in a significant number of cases.

29
Mirena® como alternativa a la histerectomía
Proporción de mujeres que cancelaron su histerectomía a 6 meses 10 20 30 40 50 60 70 80 90 100 Mirena Control Proporción de mujeres (%) *p<0.001 entre grupos Hysterectomy represents a permanent cure for menorrhagia. In this study by Lähteenmäki et al, 56 women with menorrhagia or dysmenorrhoea who were scheduled to have a hysterectomy were randomised in a 1:1 ratio to receive either Mirena (n=28) or to continue their current medical treatment (Control, n=28) [1]. The main outcome measure was the proportion of women cancelling their decision to undergo hysterectomy. At 6 months, the proportion of women who cancelled their hysterectomy was significantly higher in the Mirena group than the control group (64.3% vs 14.3%; p<0.001). In the control group, of the women who cancelled their hysterectomy at 6 months, 2 (50%) wished to continue their current treatment and the other 2 decided to switch to Mirena use. With continued follow-up of an average 3 years (range months), 48% of women in the Mirena group were still continuing with the IUS. Reference 1. Lähteenmäki P, Haukkamaa M, Puolakka J, et al. Open randomised study of use of levonorgestrel releasing intrauterine system as an alternative to hysterectomy. BMJ 1998; 316: Lähteenmäki et al. BMJ 1998; 316:
 *p<0.001 entre grupos. Hysterectomy represents a permanent cure for menorrhagia. In this study by Lähteenmäki et al, 56 women with menorrhagia or dysmenorrhoea who were scheduled to have a hysterectomy were randomised in a 1:1 ratio to receive either Mirena (n=28) or to continue their current medical treatment (Control, n=28) [1]. The main outcome measure was the proportion of women cancelling their decision to undergo hysterectomy. At 6 months, the proportion of women who cancelled their hysterectomy was significantly higher in the Mirena group than the control group (64.3% vs 14.3%; p<0.001). In the control group, of the women who cancelled their hysterectomy at 6 months, 2 (50%) wished to continue their current treatment and the other 2 decided to switch to Mirena use. With continued follow-up of an average 3 years (range months), 48% of women in the Mirena group were still continuing with the IUS. Reference. 1. Lähteenmäki P, Haukkamaa M, Puolakka J, et al. Open randomised study of use of levonorgestrel releasing intrauterine system as an alternative to hysterectomy. BMJ 1998; 316: Lähteenmäki et al. BMJ 1998; 316:")
30
Tratamiento médico de la menorragia
Mirena Progestinas (orales o inyectables) Ácido tranexámico Anti-inflamatorios no esteroideos (AINEs) Anticonceptivos combinados orales Danazol Análogos de la Hormona Liberadora de Gonadotropinas (GnRH) There are a number of medical treatments available for menorrhagia, some of which are listed here. Long-term therapy may be necessary as symptoms usually return on cessation of therapy. As such, the severity and frequency of adverse effects associated with each drug should be taken into account when deciding treatment options. Ultimately, the choice of medical therapy will depend on the woman’s requirement. Key questions to consider when choosing the optimum medical treatment include: Does the patient require contraception? Does the patient suffer painful menstruation? Is the patient able to tolerate hormone treatment? Is the patient trying to conceive? Some women may decline medical therapy and choose surgery as their preferred option.
 Ácido tranexámico. Anti-inflamatorios no esteroideos (AINEs) Anticonceptivos combinados orales. Danazol. Análogos de la Hormona Liberadora de Gonadotropinas (GnRH) There are a number of medical treatments available for menorrhagia, some of which are listed here. Long-term therapy may be necessary as symptoms usually return on cessation of therapy. As such, the severity and frequency of adverse effects associated with each drug should be taken into account when deciding treatment options. Ultimately, the choice of medical therapy will depend on the woman’s requirement. Key questions to consider when choosing the optimum medical treatment include: Does the patient require contraception Does the patient suffer painful menstruation Is the patient able to tolerate hormone treatment Is the patient trying to conceive Some women may decline medical therapy and choose surgery as their preferred option.")
31
Opciones quirúrgicas para tratamiento de la menorragia
Histerectomía Vaginal Abdominal Laparoscópica Ablación/Resección endometrial Laser Balón térmico Microondas Resección transcervical del endometrio (TCRE) Instilación de líquidos Crioterapia Hysterectomy represents a permanent cure for menorrhagia. However, a significant number of women (over one-third [1]) who undergo hysterectomy because of menorrhagia have an anatomically normal uterus removed. In the last decade or so, endometrial ablation/resection has gained popularity as a conservative surgical alternative to hysterectomy. Reference 1. Roy SN, Bhattacharya S. Benefits and risks of pharmacological agents used for the treatment of menorrhagia. Drug Safety 2004: 27; 75-90
 Instilación de líquidos. Crioterapia. Hysterectomy represents a permanent cure for menorrhagia. However, a significant number of women (over one-third [1]) who undergo hysterectomy because of menorrhagia have an anatomically normal uterus removed. In the last decade or so, endometrial ablation/resection has gained popularity as a conservative surgical alternative to hysterectomy. Reference. 1. Roy SN, Bhattacharya S. Benefits and risks of pharmacological agents used for the treatment of menorrhagia. Drug Safety 2004: 27;")
32
Miomectomia(s): Cirugía conservadora
Laparotómica - Mejora la menorragia=81% (40-93%) - Mejora la presión abdominal (60-80%) Recurrencia: 1 mioma= 27% Múltiples= 56% (26% requirieron 2ª. Miomectomia ó histerectomía) Posibilidad de histerectomía inesperada durante la (s) miomectomia(s) < del 1% Laparoscópica Complicaciones Fertilidad postQx Recurrencia 8-11% 57-69% 11,7% (al año) 84,8% (a los 8 años) Nezhat FR et al. Am Assoc Gynecol Laparosc 1998;5:237–40. (Level II-3)
 - Mejora la presión abdominal (60-80%) Recurrencia: 1 mioma= 27% Múltiples= 56% (26% requirieron 2ª. Miomectomia ó histerectomía) Posibilidad de histerectomía inesperada durante la (s) miomectomia(s) < del 1% Laparoscópica. Complicaciones. Fertilidad postQx. Recurrencia. 8-11% 57-69% 11,7% (al año) 84,8% (a los 8 años) Nezhat FR et al. Am Assoc Gynecol Laparosc 1998;5:237–40. (Level II-3)")
33
Miomectomía histeroscópica
Para Tipo 0-I (clasificación Europea) Complicaciones = 1-5% Edema pulmonar Hiponatremia Sangrado intra y post-Qx. Perforación uterina Embolismo gaseoso Infecciones
 Complicaciones = 1-5% Edema pulmonar. Hiponatremia. Sangrado intra y post-Qx. Perforación uterina. Embolismo gaseoso. Infecciones.")
34
miomectomia histeroscópica

35
UAE

36
UAE=Embolización de las arterias uterinas
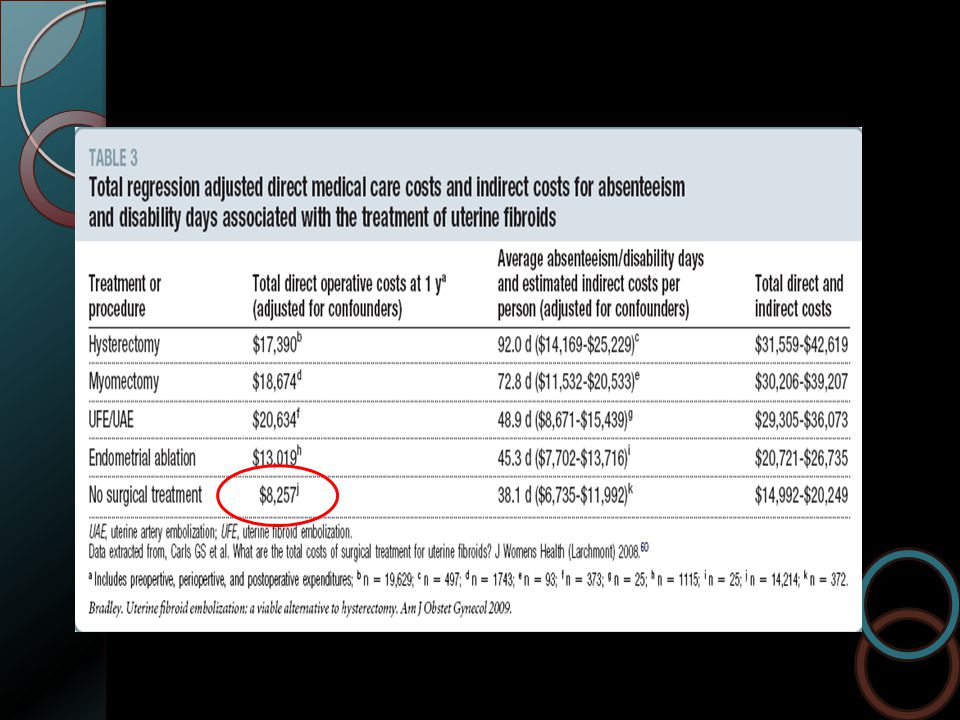
Transcutaneo a través de las arterias Femorales (partículas de Alcohol Polivinil Glicol en microesferas) Objetivos: Desvascularización del mioma e involución A los tres(3) meses = 42% de reducción, 60% de reducción en el sangrado menstrual Dias Trabajo Complic. Mayores Readmisión UAE 28.1 4,9% 11,1% Histerect 63.4 2,7% 0 %
 Objetivos: Desvascularización del mioma e involución. A los tres(3) meses = 42% de reducción, 60% de reducción en el sangrado menstrual. Dias Trabajo. Complic. Mayores. Readmisión. UAE ,9% 11,1% Histerect ,7% 0 %")
37
UAE vs. Miomectomia UEA es una buena alternativa a la Histerectomía
Procedimiento Reoperación Satisfacción Histerect. Post UAE 29% 39% 13,7% Miomectomia 3% 30% 4,4% UEA es una buena alternativa a la Histerectomía ACOG Practice Bolettin-Obts Ginecol. VOL. 112, NO. 2, PART 1, AUGUST 2008 Hehenkamp WJ et al. RCT Embolisation versus Hysterectomy(EMMY) Trial. Radiology 2008;246:
 Trial. Radiology 2008;246:")
38
Bradley L. Am J Obstet Gynecol.2009
4 muertes-2007 2=embolismo pulmonar 1= septicemia 1= CIVD Bradley L. Am J Obstet Gynecol.2009

39
HIFUS guiado por RMI Tiempo Reducción Tamaño Reducción Síntomas
6 meses 13,5% 71% 12 meses 9,4% 51% ACOG Practice Bolettin-Obts Ginecol. VOL. 112, NO. 2, PART 1, AUGUST 2008

40
Rol de Mirena® en el tratamiento de la menorragia
Altamente efectiva en reducir la pérdida sanguínea Bien tolerado Eficaz alternativa a la cirugía Alta tasa de continuación con Mirena® Alta tasa de satisfacción para la usuaria Anticoncepción efectiva This slide summarises the role of Mirena in the treatment of idiopathic menorrhagia. Mirena is the most effective pharmacological treatment available for menorrhagia. It is highly effective in reducing menstrual blood loss and is good alternative to surgery for the treatment of menorrhagia It provides effective contraception simultaneously with menorrhagia treatment It preserves fertility: there is a rapid return to ‘normal’ fertility on cessation of treatment It offers convenience It is cost-effective And the majority of patients are highly satisfied with it Conserva la fertilidad Alta relación beneficio/costo Conveniente

41
Gracias

44
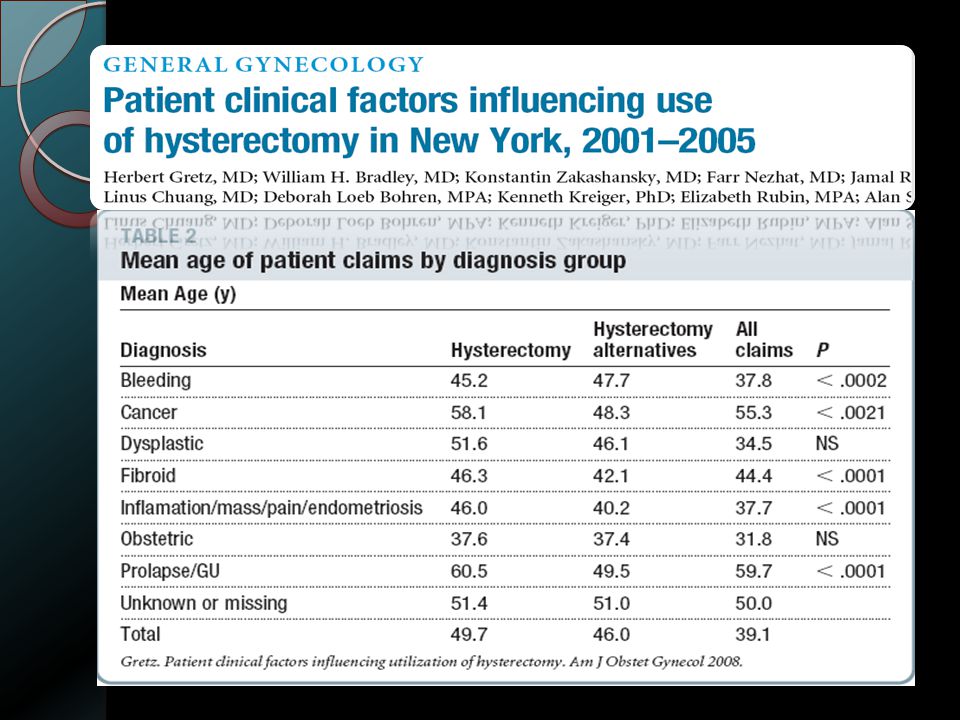
Provider characteristics: age and gender
American Journal of Obstetrics & Gynecology OCTOBER 2008

58
¿Para qué se usa Mirena®?
Indicaciones: Anticoncepción Menorragia idiopática Protección contra la hiperplasia endometrial, durante la terapia de reemplazo estrogénica There are 3 indications for Mirena®: contraception, treatment of idiopathic menorrhagia, and endometrial protection during oestrogen replacement therapy. This presentation focuses on the use of Mirena® in the treatment of menorrhagia.

59
Anticoncepción con Mirena®
Mirena® proporciona anticoncepción a través de 3 acciones combinadas movilidad espermática Inhibición de la moco cervical Engrosamiento del Prevención de la proliferación endometrial The mechanism by which Mirena® provides contraceptive protection is not completely understood, but it probably depends on a combination of 3 different actions: Thickening of cervical mucus Inhibition of sperm motility and function inside the uterus and the ovarian tubes Suppression of endometrial growth by making the endometrium unresponsive to oestrogen A weak foreign-body reaction is also present and in some women, ovulation is inhibited. As a method of contraception, the efficacy of Mirena® compares well with that of female sterilisation, with the added benefit of reversibility [1]. Reported pregnancy rates in the first year of Mirena® use range from 0.0 to 0.2%, and the cumulative rates over 5 years range from 0.5 to 1.1%. The typical pregnancy rate for female sterilisation is 0.5% within the first year. Mirena® has the advantage over oral contraceptives in that there is no user failure (e.g. forgetting to take the Pill). Many women greatly appreciate the convenience of up to 5 years’ contraceptive protection from a single Mirena® system. Reference 1. Trussell J. Contraceptive efficacy. In: Contraceptive Technology: Seventeenth Revised Edition (Hatcher RA, Trussell J, Stewart F, et al., eds.) Irvington Publishers: New York, 1998.
. Many women greatly appreciate the convenience of up to 5 years’ contraceptive protection from a single Mirena® system. Reference. 1. Trussell J. Contraceptive efficacy. In: Contraceptive Technology: Seventeenth Revised Edition (Hatcher RA, Trussell J, Stewart F, et al., eds.) Irvington Publishers: New York,")
60
Efectos endometriales con Mirena®
Ciclo menstrual en una mujer con Mirena Ciclo menstrual normal Efecto hormonal local Menstruación Ovulación Ovulación Mirena® induces profound morphological and biochemical changes in the endometrium, mainly as a result of the high endometrial levonorgestrel concentrations. This figure shows the endometrial changes that occur with Mirena treatment compared with the normal cyclical changes. After only a few weeks of Mirena® use, the glands of the endometrium become atrophic, the stroma decidualised, and the epithelium inactive. Vascular changes include thickening of the arterial wall, suppression of the spiral arterioles and capillary thrombosis. A weak foreign body response may also occur and is characterised by an increase in white blood cell infiltration. The endometrium becomes uniformly atrophic and suppressed within 3 menstrual cycles of Mirena® insertion and persists in this thin, inactive state, with no further histological development, throughout continued long-term treatment. As a result of the potent mucosal suppression caused by the local release of levonorgestrel, the endometrium becomes unresponsive to oestradiol, irrespective of ovarian function. Suppression of endometrial growth results in less menstrual shedding than normal, leading to substantial decreases in the number of days of bleeding and amount of menstrual blood loss. Amenorrhea may occur in some women. After removal of Mirena®, the endometrium returns to normal and menstruation resumes within 30 days. Días del ciclo

61
¿Qué es la menorragia? Sangrado menstrual que se presenta en intervalos normales (21─35 días), pero con Sangrado abundante ( 80 ml) o Duración prolongada ( 7 días) La pérdida sanguínea menstrual excesiva puede causar preocupación, vergüenza, molestias e inconveniencias. Al cabo de varios ciclos puede causar anemia por deficiencia de hierro. Menorrhagia is heavy or prolonged menstrual bleeding over several consecutive menstrual cycles. Heavy periods are unpleasant, inconvenient and worrisome. In some case, the bleeding may be so severe that it interrupts normal daily routine like work, school and social life. Subjectively, menorrhagia is defined as a complaint by the patient of excessive menstrual bleeding over several consecutive cycles. Objectively, it is defined as menstrual blood loss 80 ml per menstruation or bleeding that last 7 days. Excessive menstrual bleeding should be evaluated by a doctor in order to rule out potentially serious underlying conditions that may be causing the problem. Persistent heavy periods can lead to anaemia, which can cause tiredness, shortness of breath, faintness and even angina. These secondary symptoms of menorrhagia would also prompt women to see the doctor for treatment. References Peto V, Coulter A, Bond A. Factors affecting general practice practitioners’ recruitment of patients in a prospective study. Fam Pract 1993; 10: Coulter A, Bradlow J, Agass M, et al. Outcomes of referrals to gynaecology outpatient clinics for menstrual problems: an audit of general practice records. Br J Obstet Gynaecol 1991; 98: McPherson A, Andersson ABM, editors. Women’s problems in general practice. Oxford University Press. 1983: 21-24
 o. Duración prolongada ( 7 días) La pérdida sanguínea menstrual excesiva puede causar preocupación, vergüenza, molestias e inconveniencias. Al cabo de varios ciclos puede causar anemia por deficiencia de hierro. Menorrhagia is heavy or prolonged menstrual bleeding over several consecutive menstrual cycles. Heavy periods are unpleasant, inconvenient and worrisome. In some case, the bleeding may be so severe that it interrupts normal daily routine like work, school and social life. Subjectively, menorrhagia is defined as a complaint by the patient of excessive menstrual bleeding over several consecutive cycles. Objectively, it is defined as menstrual blood loss 80 ml per menstruation or bleeding that last 7 days. Excessive menstrual bleeding should be evaluated by a doctor in order to rule out potentially serious underlying conditions that may be causing the problem. Persistent heavy periods can lead to anaemia, which can cause tiredness, shortness of breath, faintness and even angina. These secondary symptoms of menorrhagia would also prompt women to see the doctor for treatment. References. Peto V, Coulter A, Bond A. Factors affecting general practice practitioners’ recruitment of patients in a prospective study. Fam Pract 1993; 10: Coulter A, Bradlow J, Agass M, et al. Outcomes of referrals to gynaecology outpatient clinics for menstrual problems: an audit of general practice records. Br J Obstet Gynaecol 1991; 98: McPherson A, Andersson ABM, editors. Women’s problems in general practice. Oxford University Press. 1983:")
62
Asesoría Beneficios y riesgos Expectativas del patrón de sangrado
Todas las mujeres deben recibir asesoría antes del uso de Mirena® : Beneficios y riesgos Expectativas del patrón de sangrado Studies show that proper counselling of women before Mirena® insertion increases patient satisfaction and improves the continuation rate. Prospective patients should be informed of the benefits and risks of using Mirena®, and the expected bleeding pattern. Mirena® causes changes in bleeding pattern in all women from those of reproductive age to those in the perimenopause. Women should be informed that Mirena® causes a significant reduction in the overall volume of menstrual bleeding and, with long-term use, that amenorrhea is common in many women. However, women should be warned that frequent intermenstrual bleeding and spotting is common during the first few months of use, and that persistence with treatment usually results in markedly fewer, if any, bleeding or spotting episodes after 6 months of treatment. Women should also be reassured that the absence of bleeding with long-term Mirena use is not a health concern, but may even be beneficial. Una asesoría adecuada mejora la tasa de continuación en el uso de Mirena®

63
Antes de la inserción de Mirena
Exploración física Descartar trastornos endometriales Evaluar posibles dificultades para la inserción y prepararse con premedicación (v.g. AINEs), bloqueo paracervical o dilatación cervical. Consultar en la “Información para Prescribir” detalles acerca de las contraindicaciones para el uso de Mirena It is very important that the patient is assessed as to their suitability for Mirena use. The Mirena® prescribing information should be consulted to exclude patients that are contraindicated. Contraindications for Mirena® include: pregnancy; current or recurrent pelvic inflammatory disease; lower genital tract infection; postpartum endometritis; infected abortion during the past three months; cervicitis; cervical dysplasia; uterine or cervical malignancy; undiagnosed abnormal uterine bleeding; congenital or acquired uterine anomaly including fibroids if they distort the uterine cavity; conditions associated with increased susceptibility to infections; acute liver disease or liver tumour; and hypersensitivity to constituents of the preparation. A physical examination including pelvic examination, palpation of the breast and cervical smear (if needed) should be performed. The position and size of the uterus should be determined. Fundal positioning of Mirena is important in order to ensure that the whole endometrium is exposed to uniform levels of levonorgestrel. Mirena® should be inserted by appropriately trained personnel, and instructions for insertion should be carefully followed. Insertion should be done within seven days from the onset of menstruation or immediately after a first trimester abortion. Replacement with a new system can be done any time during the cycle.
, bloqueo paracervical o dilatación cervical. Consultar en la Información para Prescribir detalles acerca de las contraindicaciones para el uso de Mirena It is very important that the patient is assessed as to their suitability for Mirena use. The Mirena® prescribing information should be consulted to exclude patients that are contraindicated. Contraindications for Mirena® include: pregnancy; current or recurrent pelvic inflammatory disease; lower genital tract infection; postpartum endometritis; infected abortion during the past three months; cervicitis; cervical dysplasia; uterine or cervical malignancy; undiagnosed abnormal uterine bleeding; congenital or acquired uterine anomaly including fibroids if they distort the uterine cavity; conditions associated with increased susceptibility to infections; acute liver disease or liver tumour; and hypersensitivity to constituents of the preparation. A physical examination including pelvic examination, palpation of the breast and cervical smear (if needed) should be performed. The position and size of the uterus should be determined. Fundal positioning of Mirena is important in order to ensure that the whole endometrium is exposed to uniform levels of levonorgestrel. Mirena® should be inserted by appropriately trained personnel, and instructions for insertion should be carefully followed. Insertion should be done within seven days from the onset of menstruation or immediately after a first trimester abortion. Replacement with a new system can be done any time during the cycle.")
64
Farmacocinética del levonorgestrel después de la inserción de Mirena®
Liberación continua del fármaco Mirena® no causa ‘picos y caídas’, observados con la administración oral de progestinas Se alcanzan niveles endometriales de progestina muy elevados, no así con la administración oral: Concentración de levonorgestrel (ng/g de tejido húmedo) Endoceptivo (30μg/día) Administración oral (250μg) Endometrio 808 3.5 Levonorgestrel is continuously released from Mirena, which means that there are no ‘peaks and troughs’ in serum levonorgestrel levels. In this table, endometrial levonorgestrel concentrations achieved with a 30μg/day levonorgestrel-releasing system after days of use were about 230-times higher than with an oral preparation containing 250μg levonorgestrel used daily for 7 days [1]. Reference 1. Nilsson CG, Haukkamaa M, Vierola H, et al. Tissue concentrations of levonorgestrel in women using a levonorgestrel-releasing IUD. Clin Endocrinol 1982; 17: 529–36 Nilsson et al., 1982
 Endoceptivo (30μg/día) Administración oral (250μg) Endometrio Levonorgestrel is continuously released from Mirena, which means that there are no ‘peaks and troughs’ in serum levonorgestrel levels. In this table, endometrial levonorgestrel concentrations achieved with a 30μg/day levonorgestrel-releasing system after days of use were about 230-times higher than with an oral preparation containing 250μg levonorgestrel used daily for 7 days [1]. Reference. 1. Nilsson CG, Haukkamaa M, Vierola H, et al. Tissue concentrations of levonorgestrel in women using a levonorgestrel-releasing IUD. Clin Endocrinol 1982; 17: 529–36. Nilsson et al.,")
65
Niveles séricos bajos de levonorgestrel con Mirena®
El uso local es lo lógico! Levonorgestrel plasmático (pg/mL) “Local is logical” – local administration of levonorgestrel into the uterus with Mirena® results in much lower serum levels than with conventional oral administration. In a clinical study of postmenopausal women, an oral dose of 250 µg levonorgestrel resulted in systemic exposure levels that were substantially higher than those achieved with Mirena® [1]. Reference 1. Suhonen SP, Holmström T, Allonen HO, et al. Intrauterine and subdermal progestin administration in postmenopausal hormone replacement therapy. Fertil Steril 1995; 63: 336–42. 250 µg VO de levonorgestrel Años de uso de Mirena Suhonen et al. Fertil Steril 1995; 63: 336–42
 Local is logical – local administration of levonorgestrel into the uterus with Mirena® results in much lower serum levels than with conventional oral administration. In a clinical study of postmenopausal women, an oral dose of 250 µg levonorgestrel resulted in systemic exposure levels that were substantially higher than those achieved with Mirena® [1]. Reference. 1. Suhonen SP, Holmström T, Allonen HO, et al. Intrauterine and subdermal progestin administration in postmenopausal hormone replacement therapy. Fertil Steril 1995; 63: 336– µg VO de. levonorgestrel. Años de uso de Mirena Suhonen et al. Fertil Steril 1995; 63: 336–42.")
66
Mirena incrementa la hemoglobina y la ferritina séricas
126 128 130 132 134 136 138 140 1 2 3 4 5 6 7 8 9 10 11 12 Meses de uso de Mirena Hemoglobina sérica promedio (g/L) 5 10 15 20 25 30 35 1 2 3 4 6 7 8 9 11 12 Meses de uso de Mirena Ferritina sérica promedio µg/L) #p<0.01 * # *p<0.001 # The reduction in menstrual blood loss in the Andersson and Rybo study was accompanied by significant increases in serum haemoglobin and ferritin levels [1]. Overall, these result suggest that Mirena is effective in “normalising” serum haemoglobin and iron storage in women with menorrhagia. Other studies have confirmed that Mirena effectively reduces menstrual blood loss and improves serum haemoglobin and ferritin levels in idiopathic menorrhagia [2], and even in the presence of underlying pathologies such as uterine leiomyomas and adenomyosis [3,4]. References Andersson JK, Rybo G. Levonorgestrel-releasing intrauterine device in the treatment of menorrhagia. Br J Obstet Gynaecol. 1990; 97: 690-4 Xiao B, Wu S-C, Chong J, et al. Therapeutic effects of levonorgestrel-releasing intrauterine system in treatment of idiopathic menorrhagia. Fertil Steril 2003; 79: 963-9 Grigorieva V, Chen-Mok M, Tarasova M, et al. Use of a levonorgestrel-releasing intrauterine system to treat bleeding related to uterine leiomyomas. Fertil Steril 2003; 79: Fedele L, Bianchi S, Raffaelli R, et al. Treatment of adenomyosis-associated menorrhagia with a levonorgestrel-releasing intrauterine device. Fertil Steril 1997; 68: 426-9 Andersson and Rybo. Br J Obstet Gynaecol. 1990; 97: 690-4
 Meses de uso de Mirena. Ferritina sérica. promedio µg/L) #p<0.01. * # *p< # The reduction in menstrual blood loss in the Andersson and Rybo study was accompanied by significant increases in serum haemoglobin and ferritin levels [1]. Overall, these result suggest that Mirena is effective in normalising serum haemoglobin and iron storage in women with menorrhagia. Other studies have confirmed that Mirena effectively reduces menstrual blood loss and improves serum haemoglobin and ferritin levels in idiopathic menorrhagia [2], and even in the presence of underlying pathologies such as uterine leiomyomas and adenomyosis [3,4]. References. Andersson JK, Rybo G. Levonorgestrel-releasing intrauterine device in the treatment of menorrhagia. Br J Obstet Gynaecol. 1990; 97: Xiao B, Wu S-C, Chong J, et al. Therapeutic effects of levonorgestrel-releasing intrauterine system in treatment of idiopathic menorrhagia. Fertil Steril 2003; 79: Grigorieva V, Chen-Mok M, Tarasova M, et al. Use of a levonorgestrel-releasing intrauterine system to treat bleeding related to uterine leiomyomas. Fertil Steril 2003; 79: Fedele L, Bianchi S, Raffaelli R, et al. Treatment of adenomyosis-associated menorrhagia with a levonorgestrel-releasing intrauterine device. Fertil Steril 1997; 68: Andersson and Rybo. Br J Obstet Gynaecol. 1990; 97:")
67
Mirena® comparada con noretisterona
Mirena es al menos tan efectivo como la noretisterona en reducir la pérdida sanguínea menstrual (PSM) 105 120 6 20 40 60 80 100 140 Mirena Noretisterona PSM promedio (mL) Basal 3 meses 64 44 10 20 30 40 50 60 70 80 90 100 Mirena Noretisterona Grado de satisfacción con el tratamiento Mirena is at least as effective as norethisterone in the treatment of idiopathic menorrhagia. In this study, 44 women were randomised to Mirena (n=22) or norethisterone (n=22) treatment over 3 months [1]. Oral norethisterone 5mg was taken three times daily from day 5 to day 26 of the menstrual cycle for 3 consecutive cycles. Menstrual blood loss was objectively assessed by analysis of all used tampons/pads using the alkaline haematin method. As shown in this figure, menstrual blood loss at 3 months was significantly reduced in both groups. However, more women liked using Mirena than norethisterone (64% vs 44%). In addition, more women wished to continue treatment with Mirena (76%) than with norethisterone (22%) Reference 1. Irvine GA, Campbell-Brown MB, Lumsden MA, et al. Randomised comparative trial of the levonorgestrel intrauterine system and norethisterone for treatment of idiopathic menorrhagia. Br J Obstet Gynaecol 1998; 105: 592-8 Irvine et al. Obstet Gynaecol 1998; 105: 592-8
 Mirena. Noretisterona. PSM promedio (mL) Basal. 3 meses Mirena. Noretisterona. Grado de satisfacción. con el tratamiento. Mirena is at least as effective as norethisterone in the treatment of idiopathic menorrhagia. In this study, 44 women were randomised to Mirena (n=22) or norethisterone (n=22) treatment over 3 months [1]. Oral norethisterone 5mg was taken three times daily from day 5 to day 26 of the menstrual cycle for 3 consecutive cycles. Menstrual blood loss was objectively assessed by analysis of all used tampons/pads using the alkaline haematin method. As shown in this figure, menstrual blood loss at 3 months was significantly reduced in both groups. However, more women liked using Mirena than norethisterone (64% vs 44%). In addition, more women wished to continue treatment with Mirena (76%) than with norethisterone (22%) Reference. 1. Irvine GA, Campbell-Brown MB, Lumsden MA, et al. Randomised comparative trial of the levonorgestrel intrauterine system and norethisterone for treatment of idiopathic menorrhagia. Br J Obstet Gynaecol 1998; 105: Irvine et al. Obstet Gynaecol 1998; 105:")
68
Mirena® comparada con flurbiprofeno y ácido tranexámico
Mirena® es significativamente más efectivo que el flurbiprofeno y que el ácido tranexámico para reducir la pérdida sanguínea menstrual (PSM). -83 -24.4 -47.5 -100 -90 -80 -70 -60 -50 -40 -30 -20 -10 Mirena Flurbiprofeno (FL) Ácido Tranexámico Porcentaje de cambio de la PSM a partir de la basal * P<0.05 (FL vs AT) *** **P<0.01 (Mirena vs AT) ** ***P<0.001 (Mirena vs FL) Mirena is more effective than flurbiprofen, and tranexamic acid in the treatment of idiopathic menorrhagia. In this study, the first 20 women to enrol were treated with Mirena and 15 other women who subsequently enrolled were treated with flurbiprofen (100 mg twice daily for 5 days) or tranexamic acid (1.5 g three times daily for 3 days and 1 g twice daily for another 4 days) for two consecutive cycles before crossing over to other treatment for the subsequent 2 cycles [1]. Treatment with flurbiprofen or tranexamic acid was started on the first day of menstruation. Menstrual blood loss was objectively assessed by analysis of all used tampons/pads using the alkaline haematin method. As shown in this figure, menstrual blood loss at 3 months was greater than 80% compared with baseline in the Mirena group. Menstrual blood loss compared with baseline was further reduced by 96% at 12 months follow-up. In comparison, flurbiprofen and tranexamic acid only reduced menstrual blood loss by an average 24.4% and 47.5% compared with baseline, respectively. Mirena was the only treatment to reduce the mean menstrual blood loss to below 80mL per menstruation, the upper limit of ‘normal’ menstrual loss. Long-term treatment with either flurbiprofen or tranexamic acid would not be expected to result in greater subsequent reduction in menstrual blood loss than that observed in this study because both treatments, unlike Mirena, do not suppress or modulate the cyclical endometrial build up. Reference Milsom I, Andersson K, Andersch B, Rybo G. A comparison of flubiprofen, tranexamic acid, and a levonorgestrel-releasing intrauterine contraceptive device in the treatment of idiopathic menorrhagia. Am J Obstet Gynecol 1991; 164: * Milsom et al. Am J Obstet Gynecol 1991; 164:
 Mirena. Flurbiprofeno. (FL) Ácido. Tranexámico. Porcentaje de cambio de la. PSM a partir de la basal. * P<0.05 (FL vs AT) *** **P<0.01 (Mirena vs AT) ** ***P<0.001 (Mirena vs FL) Mirena is more effective than flurbiprofen, and tranexamic acid in the treatment of idiopathic menorrhagia. In this study, the first 20 women to enrol were treated with Mirena and 15 other women who subsequently enrolled were treated with flurbiprofen (100 mg twice daily for 5 days) or tranexamic acid (1.5 g three times daily for 3 days and 1 g twice daily for another 4 days) for two consecutive cycles before crossing over to other treatment for the subsequent 2 cycles [1]. Treatment with flurbiprofen or tranexamic acid was started on the first day of menstruation. Menstrual blood loss was objectively assessed by analysis of all used tampons/pads using the alkaline haematin method. As shown in this figure, menstrual blood loss at 3 months was greater than 80% compared with baseline in the Mirena group. Menstrual blood loss compared with baseline was further reduced by 96% at 12 months follow-up. In comparison, flurbiprofen and tranexamic acid only reduced menstrual blood loss by an average 24.4% and 47.5% compared with baseline, respectively. Mirena was the only treatment to reduce the mean menstrual blood loss to below 80mL per menstruation, the upper limit of ‘normal’ menstrual loss. Long-term treatment with either flurbiprofen or tranexamic acid would not be expected to result in greater subsequent reduction in menstrual blood loss than that observed in this study because both treatments, unlike Mirena, do not suppress or modulate the cyclical endometrial build up. Reference. Milsom I, Andersson K, Andersch B, Rybo G. A comparison of flubiprofen, tranexamic acid, and a levonorgestrel-releasing intrauterine contraceptive device in the treatment of idiopathic menorrhagia. Am J Obstet Gynecol 1991; 164: * Milsom et al. Am J Obstet Gynecol 1991; 164:")
69
Mirena® comparado con ablación/resección endometrial
Mirena tiene eficacia comparable a la resección endometrial en la reducción de la pérdida sanguínea menstrual (PSM) 184.8 203.2 38.8 23.5 50 100 150 200 250 Mirena Resección endometrial PSM promedio Basal 12 meses Mirena has been shown to be comparable with endometrial resection in reducing menstrual bleeding. In this study [1], Crosignani et al. randomised 70 premenopausal women aged 38 years or older with dysfunctional uterine bleeding to receive Mirena or undergo endometrial resection. Women who were uncertain whether they wished to retain their fertility were excluded from the study. Uterine bleeding was quantified by the semi-quantitative pictorial blood loss assessment score (PBAC). There was a 79% reduction in mean bleeding score in the Mirena group compared with a 89% reduction in the endometrial resection group at 12 month follow-up. The between-group difference in monthly bleeding scores at 12 months were statistically significant. Amenorrhea or hypomenorrhea was reported by 65% of patients in the Mirena® group and 71% in the resection group at 12 months. However, health-related quality of life perception was not significantly different between the two groups. Reference Crosignani PG, Vercellini P, Mosconi P, et al. Levonorgestrel-releasing intrauterine device versus hysteroscopic endometrial resection in the treatment of dysfunctional uterine bleeding. Obstet Gynecol 1997; 90: Crosignani et al. Obstet Gynecol 1997; 90:
 Mirena. Resección. endometrial. PSM promedio. Basal. 12 meses. Mirena has been shown to be comparable with endometrial resection in reducing menstrual bleeding. In this study [1], Crosignani et al. randomised 70 premenopausal women aged 38 years or older with dysfunctional uterine bleeding to receive Mirena or undergo endometrial resection. Women who were uncertain whether they wished to retain their fertility were excluded from the study. Uterine bleeding was quantified by the semi-quantitative pictorial blood loss assessment score (PBAC). There was a 79% reduction in mean bleeding score in the Mirena group compared with a 89% reduction in the endometrial resection group at 12 month follow-up. The between-group difference in monthly bleeding scores at 12 months were statistically significant. Amenorrhea or hypomenorrhea was reported by 65% of patients in the Mirena® group and 71% in the resection group at 12 months. However, health-related quality of life perception was not significantly different between the two groups. Reference. Crosignani PG, Vercellini P, Mosconi P, et al. Levonorgestrel-releasing intrauterine device versus hysteroscopic endometrial resection in the treatment of dysfunctional uterine bleeding. Obstet Gynecol 1997; 90: Crosignani et al. Obstet Gynecol 1997; 90:")
70
Mirena® comparado con ablación/resección endometrial (2)
Ambos tratamientos aumentaron significativamente hemoglobina, hematocrito y hierro Incremento promedio desde la basal Hemoglobina (g/l) Hematocrito (%) Hierro sérico (mg/l) Mirena 21 5.7 522 Ablación/resección endometrial 22 5.9 558 Accompanying the reduction in menstrual bleeding were significant (p<0.001) increases in serum haemoglobin, haematocrit, and iron by month 6 in both treatment groups. Reference Crosignani PG, Vercellini P, Mosconi P, et al. Levonorgestrel-releasing intrauterine device versus hysteroscopic endometrial resection in the treatment of dysfunctional uterine bleeding. Obstet Gynecol 1997; 90: Crosignani et al. Obstet Gynecol 1997; 90:
 Hematocrito (%) Hierro sérico (mg/l) Mirena Ablación/resección endometrial Accompanying the reduction in menstrual bleeding were significant (p<0.001) increases in serum haemoglobin, haematocrit, and iron by month 6 in both treatment groups. Reference. Crosignani PG, Vercellini P, Mosconi P, et al. Levonorgestrel-releasing intrauterine device versus hysteroscopic endometrial resection in the treatment of dysfunctional uterine bleeding. Obstet Gynecol 1997; 90: Crosignani et al. Obstet Gynecol 1997; 90:")
71
Mirena® comparado con ablación/resección endometrial (3)
Ambos tratamientos tienen altas tasas de satisfacción 85 94 10 20 30 40 50 60 70 80 90 100 Mirena Resección endometrial Proporción de satisfechas y muy satisfechas (%) Treatment satisfaction was high in both groups with 85% of women being satisfied or very satisfied with Mirena compared with 94% in the resection group at 12-month follow-up. Reference Crosignani PG, Vercellini P, Mosconi P, et al. Levonorgestrel-releasing intrauterine device versus hysteroscopic endometrial resection in the treatment of dysfunctional uterine bleeding. Obstet Gynecol 1997; 90: Crosignani et al. Obstet Gynecol 1997; 90:
 Treatment satisfaction was high in both groups with 85% of women being satisfied or very satisfied with Mirena compared with 94% in the resection group at 12-month follow-up. Reference. Crosignani PG, Vercellini P, Mosconi P, et al. Levonorgestrel-releasing intrauterine device versus hysteroscopic endometrial resection in the treatment of dysfunctional uterine bleeding. Obstet Gynecol 1997; 90: Crosignani et al. Obstet Gynecol 1997; 90:")
72
Resumen de estudios que comparan Mirena® con ablación/resección endometrial
Reducción en la pérdida sanguínea menstrual (vigilancia) Henshaw et al., 2002 Mirena ® Ablación con microondas 20 35 82% (promedio 20.9 meses) 73% (promedio 8.3 meses) Barrington et al., 2003 Mirena® Ablación con balón térmico 25 71% (6 meses) 50% (6 meses) Istre and Trolle, 2001 Resección endometrial transcervical 30 29 90% (12 meses) 98% (12 meses) Kittelsen and Istre, 1998 24 Similar results have been reported in other studies for Mirena and a variety of endometrial ablation/resection methods [1-4]. Overall, these result suggest that Mirena is a good alternative to endometrial ablation/resection. Importantly, Mirena does not compromise future fertility, unlike the endometrial ablation/resection methods. References Istre P, Trolle B. Treatment of menorrhagia with the levonorgestrel intrauterine system versus endometrial resection. Fertil Steril 2001; 76: 304-9 Kittelsen N, Istre O. A randomised study comparing levonorgestrel-releasing intrauterine system (LNG IUS) and transcervical resection of the endometrium in the treatment of menorrhagia: preliminary results. Gynaecol Endoscopy 1998; 7: 61-5 Henshaw R, Coyle C, Low S, et al. A retrospective cohort study comparing microwave endometrial ablation with levonorgestrel-releasing intrauterine device in the management of heavy menstrual bleeding. Aust NZ J Obstet Gynaecol 2002; 42: 205-9 Barrington JW, Angamuthu S, Arunkalaivanan AS, et al. Comparison between the levonorgestrel intrauterine system (LNG-IUS) and thermal balloon ablation in the treatment of menorrhagia. Eur J Obstet Gynecol Reprod Biol 2003; 108: 72-4
 Henshaw et al., Mirena ® Ablación con microondas % (promedio 20.9 meses) 73% (promedio 8.3 meses) Barrington et al., Mirena® Ablación con balón térmico % (6 meses) 50% (6 meses) Istre and Trolle, Resección endometrial transcervical % (12 meses) 98% (12 meses) Kittelsen and Istre, Similar results have been reported in other studies for Mirena and a variety of endometrial ablation/resection methods [1-4]. Overall, these result suggest that Mirena is a good alternative to endometrial ablation/resection. Importantly, Mirena does not compromise future fertility, unlike the endometrial ablation/resection methods. References. Istre P, Trolle B. Treatment of menorrhagia with the levonorgestrel intrauterine system versus endometrial resection. Fertil Steril 2001; 76: Kittelsen N, Istre O. A randomised study comparing levonorgestrel-releasing intrauterine system (LNG IUS) and transcervical resection of the endometrium in the treatment of menorrhagia: preliminary results. Gynaecol Endoscopy 1998; 7: Henshaw R, Coyle C, Low S, et al. A retrospective cohort study comparing microwave endometrial ablation with levonorgestrel-releasing intrauterine device in the management of heavy menstrual bleeding. Aust NZ J Obstet Gynaecol 2002; 42: Barrington JW, Angamuthu S, Arunkalaivanan AS, et al. Comparison between the levonorgestrel intrauterine system (LNG-IUS) and thermal balloon ablation in the treatment of menorrhagia. Eur J Obstet Gynecol Reprod Biol 2003; 108:")
73
Mirena® como una alternativa a la histerectomía (2)
“El uso del endoceptivo liberador de levonorgestrel [Mirena] es una buena alternativa a la histerectomía en el tratamiento de la menorragia y debe considerarse antes de la histerectomía u otros tratamientos invasivos” Lähteenmäki et al went on to concluded that [1]: “The use of Mirena is a good conservative alternative to hysterectomy in the treatment of menorrhagia and should be considered before hysterectomy or other invasive treatment” Reference 1. Lähteenmäki P, Haukkamaa M, Puolakka J, et al. Open randomised study of use of levonorgestrel releasing intrauterine system as an alternative to hysterectomy. BMJ 1998; 316: Lähteenmäki et al. BMJ 1998; 316:

74
Mirena® comparado con la histerectomía
Tanto Mirena® como la histerectomía se asociaron con una mejoría significativa en la calidad de vida relacionada a la salud (RAND-36) excepto funcionamiento físico, durante 5 años de seguimiento 20 Mirena 15 Histerectomía 10 Cambio en la puntuación del RAND-36 después de 5 años 5 In this study, 236 Finnish women referred to 5 university hospitals for complaints of menorrhagia were randomised to Mirena (n= 119) or hysterectomy (117) and followed-up for 5 years [1]. After 5 years’ follow-up the two groups did not differ substantially in terms of health-related quality of life (HRQL) or psychosocial well-being. In both groups, HRQL measured by the RAND-36 questionnaire improved significantly in all dimension except physical function. Reference 1. Hurskainen R, Teperi J, Rissanen P, et al. Clinical outcomes and costs with the levonorgestrel-releasing intrauterine system or hysterectomy for treatment of menorrhagia: randomized trial 5-year follow-up. JAMA 2004; 291: Dolor -5 Energía Bienestar emocional Salud general Funcionamiento social físico/funcional Rol Funcionamiento físico funcional/emocional Rol Dimensión del RAND-36 Hurskainen et al. JAMA 2004; 291:
 excepto funcionamiento físico, durante 5 años de seguimiento. 20. Mirena. 15. Histerectomía. 10. Cambio en la puntuación del. RAND-36 después de 5 años. 5. In this study, 236 Finnish women referred to 5 university hospitals for complaints of menorrhagia were randomised to Mirena (n= 119) or hysterectomy (117) and followed-up for 5 years [1]. After 5 years’ follow-up the two groups did not differ substantially in terms of health-related quality of life (HRQL) or psychosocial well-being. In both groups, HRQL measured by the RAND-36 questionnaire improved significantly in all dimension except physical function. Reference. 1. Hurskainen R, Teperi J, Rissanen P, et al. Clinical outcomes and costs with the levonorgestrel-releasing intrauterine system or hysterectomy for treatment of menorrhagia: randomized trial 5-year follow-up. JAMA 2004; 291: Dolor. -5. Energía. Bienestar. emocional. Salud general. Funcionamiento. social. físico/funcional. Rol. Funcionamiento. físico. funcional/emocional. Rol. Dimensión del RAND-36. Hurskainen et al. JAMA 2004; 291:")
75
Mirena® comparado con la histerectomía (3)
Los costos totales (directos e indirectos) de la atención médica fueron 40% más bajos con Mirena® que con la histerectomía a 5 años de seguimiento 5000 4660 4000 3000 Costos totales (US dls) 2817 2000 Although 42% of the women assigned to Mirena eventually underwent hysterectomy, the discounted direct and indirect costs were 40% lower in the Mirena group than in the hysterectomy group. These results suggest that Mirena is a cost-effective alternative to hysterectomy in the treatment of menorrhagia. Reference 1. Hurskainen R, Teperi J, Rissanen P, et al. Clinical outcomes and costs with the levonorgestrel-releasing intrauterine system or hysterectomy for treatment of menorrhagia: randomized trial 5-year follow-up. JAMA 2004; 291: 1000 Mirena Histerectomía Hurskainen et al. JAMA 2004; 291:
 de la atención médica fueron 40% más bajos con Mirena® que con la histerectomía a 5 años de seguimiento Costos totales (US dls) Although 42% of the women assigned to Mirena eventually underwent hysterectomy, the discounted direct and indirect costs were 40% lower in the Mirena group than in the hysterectomy group. These results suggest that Mirena is a cost-effective alternative to hysterectomy in the treatment of menorrhagia. Reference. 1. Hurskainen R, Teperi J, Rissanen P, et al. Clinical outcomes and costs with the levonorgestrel-releasing intrauterine system or hysterectomy for treatment of menorrhagia: randomized trial 5-year follow-up. JAMA 2004; 291: Mirena. Histerectomía. Hurskainen et al. JAMA 2004; 291:")
Presentaciones similares













.>")



>")

