Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Tratamiento antirretroviral Principios 1ª
Tratamiento antirretroviral Principios 1ª. Línea de tratamiento Rescates Nuevos Fármacos Dr. Miguel Angel Arreola Pereyra Internista. UMAE HE CMN SIGLO XXI IMSS México D.F.

2
Proteínas de la nucleocápside Proteinas reguladoras
Objetivos del Tx Proteínas de la nucleocápside (zinc-finger) Unión, fusión y entrada Proteasa Viral RNA RNA Proteins Transcriptasa viral RT RNA RNA DNA DNA RT Proteinas reguladoras virales DNA DNA DNA DNA Provirus Integrasa viral
 Unión, fusión y entrada. Proteasa Viral. RNA. RNA. Proteins. Transcriptasa. viral. RT. RNA. RNA. DNA. DNA. RT. Proteinas reguladoras. virales. DNA. DNA. DNA. DNA. Provirus. Integrasa viral.")
3
ANTIRRETROVIRALES 2006 ITRAN P Zidovudina Stavudina ITRANN Didanosina
Indinavir* Saquinavir* Nelfinavir Atazanavir* Amprenavir* Lopinavir* Tipranavir Fosamprenavir Darunavir ITRAN Zidovudina Stavudina Didanosina Zalcitabina Lamivudina Abacavir Tenofovir Emtricitabina ITRANN Efavirenz Nevirapina I. Fusión Enfuvirtida

4
Antirretrovirales aprobados 1987-2006
ATV FPV ENF FTC 25 DRV TPV 20 LPV/ RTV TDF EFV ABC APV Fármacos 15 NFV DLV RTV IDV NVP 10 This slide shows a timeline of the approval of the antiretroviral drugs from the previous slide. The first drug that was approved for the treatment of HIV infection was a nucleoside analogue, zidovudine, which was approved in Over the past quarter of a century, we have seen a number of HIV drugs come into the marketplace. The first PI, saquinavir, was approved in The first NNRTI, nevirapine, was approved in In 2003, the first entry inhibitor was approved, and that was enfuvirtide. SQV 3TC 5 d4T ddC ddI ZDV 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 año Figure does not include fixed-dose combinations.

5
Timeline of Antiretroviral Development
AIDS 1st reported 1981 1984 1985 1987 1991 1992 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 ZDV ddI ddC d4T 3TC, SQV RTV, IDV, NVP NFV, DLV, ZDV/3TC, SQV-gc EFV, ABC 3TC, lamivudine; ABC, abacavir; APV, amprenavir; ATV, atazanavir; d4T, stavudine; ddI, didanosine; ddC, zalcitabine; DLV, delavirdine; DRV, darunavir; ENF enfuvirtide; EFV, efavirenz; FPV, fosamprenavir; FTC, emtricitabine; IDV, indinavir; LPV, lopinavir; NFV, nelfinavir; NVP, nevirapine; RTV, ritonavir; SQV, saquinavir; ; TDF, tenofovir DF; TPV, tipranavir; ZDV, zidovudine; ZDV/3TC, zidovudine/lamivudine. This slide shows a timeline for antiretroviral development over the last 25 years. The first case of AIDS in the United States was reported in The first antiretroviral drug approved in the United States for the treatment of HIV infection was zidovudine. Since its approval in 1987, more than 20 additional agents have been approved. In the late 20th and early 21st centuries, a number of new drugs have come into the marketplace, including reformulations and coformulations of drugs that had been previously available. This evolution in antiretroviral drug therapy has focused on making therapy for HIV‑infected patients simpler in terms of pill burden and dosing frequency. APV LPV/RTV, ddI-EC, ZDV/3TC/ABC TDF EFV-600, 3TC-300, d4T-XR Reformulations ENF, NFV 625, ATV, FTC, FPV ABC/3TC, TDF/FTC, ddI generic Coformulations SQV 500, TPV, ZDV generic, LPV/RTV tabs DRV, TDF/FTC/EFV

6
No se precipiten!!! Primero habrá que tomar en cuenta algunos aspectos.

7
Reglas de oro El primer esquema debe ser efectivo
Debe administrarse 2 veces al día máximo Si existe problema de apego, 1 vez/día No debe incluir tres clases de fármacos No debe coincidir toxicidad

8
Regla de oro Debe valorarse lo que el paciente puede tomar vs lo que debe tomar No insistir en la superioridad de un esquema debe darse prioridad al pacx. El régimen debe iniciarse el mismo día Debe estimularse la participación en estudios clínicos Pros y contras deben comentarse con el paciente

9
Objetivos del tratamiento
Eficacia: Supresión de CV máxima y duradera. Tolerabilidad: Mínimo impacto en las actividades diarias. Seguridad: Toxicidad aceptable. “Rescatabilidad”: Preservación de futuras opciones de tratamiento.

10
Respuesta a la TARAA según los CD4 iniciales
Progresión de la enfermedad Supresión viral Semanas de tratamiento

13
Agentes ARV para el inicio del manejo
-Sin datos clínicos finales. Pueden ser poco efectivos con CV elevadas. Evita usar IP o ITRnAN. Pocas interacciones. Pocas pastillas. Considerar solo en CV < 100,000 copias o en mal apego. 3 ITRAN Poco seguimiento. Resistencia cruzada. Equivalentes a los esquemas con IP. Mejor apego. 2 ITRAN + 1 ITRnAN Superado por esquemas reforzados y en algunos estudios por ITRNN Evidencia clínica de eficacia a largo plazo. Poblaciones específicas, hepatopatas, embarazadas Recomendado 2 ITRAN + 1 IP No reforzado (NFV) Toxicidad común - Muchas pastillas - Interacciones - Evidencia clínica de su efecto. - Eficaz en enfermedad tardía. - Seguimiento a largo plazo. 2 ITRAN + 1 IP/r Desventajas Ventajas Recomendación Esquema Recomendado BHIVA-Up date, 2005 Dr. Arreola
 Toxicidad común. - Muchas pastillas. - Interacciones. - Evidencia clínica de su. efecto. - Eficaz en enfermedad tardía. - Seguimiento a largo plazo. 2 ITRAN + 1 IP/r. Desventajas. Ventajas. Recomendación. Esquema. Recomendado. BHIVA-Up date, Dr. Arreola.")
14
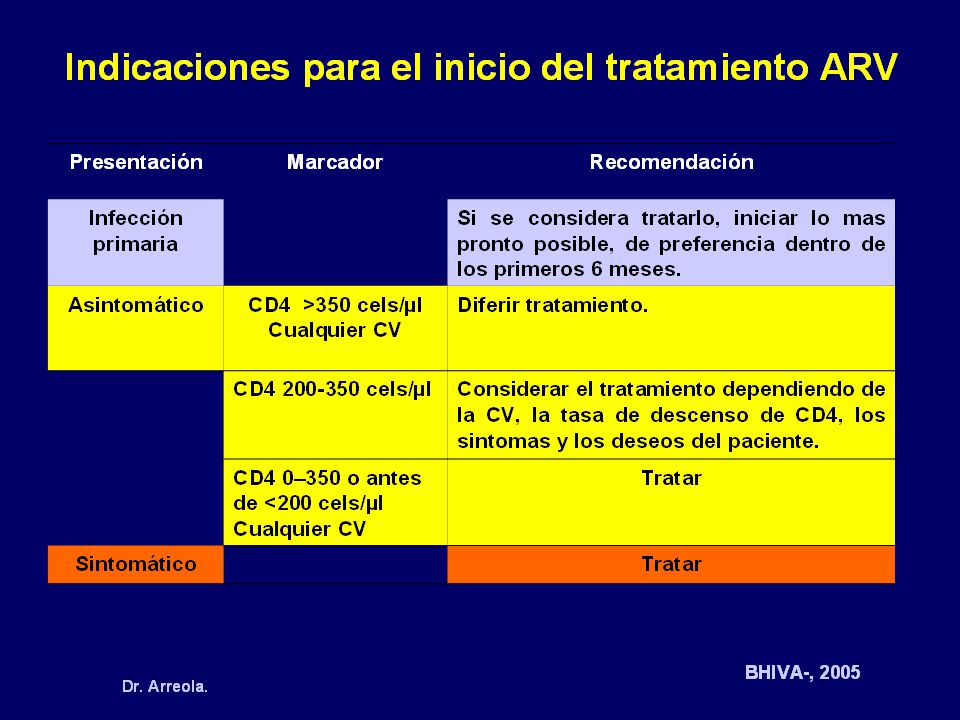
Indicaciones para el inicio del tratamiento ARV
Casos con CD4+<350 Cualquier CV Casos con CD4+>350 Cualquier CV Iniciar tratamiento Diferir tratamiento. Vigilar con CD4+ cada 2-4 meses. DHHS-Febrero, 2004 BHIVA-Marzo, 2004

15
Inicio de tratamiento La TARAA puede iniciarse con CD4+ sustancialmente mas baja de 350 cels/mm3 aprox 200 cel/mm3. Sterling TR, Chaisson RE, Keruly J, Moore RD. When to initiate highly active antiretroviral therapy (HAART): HIV disease progression according to baseline CD4+ level at initiation of therapy among persons with durable virologic suppression. Program and abstracts of the 9th Conference on Retroviruses and Opportunistic Infections; February 24-28, 2002; Seattle, Washington. Abstract 469. King M, Bernstein B, Cernohous P, Mosely J, Bauer E, Sun E. Impact of baseline CD4 cell count and viral load on durability of virologic response through 96 weeks for lopinavir/ritonavir (LPV/r) and nelfinavir (NFV) in a phase III clinical trial. Program and abstracts of the 9th Conference on Retroviruses and Opportunistic Infections; February 24-28, 2002; Seattle, Washington. Abstract 470.
: HIV disease progression according to baseline CD4+ level at initiation of therapy among persons with durable virologic suppression. Program and abstracts of the 9th Conference on Retroviruses and Opportunistic Infections; February 24-28, 2002; Seattle, Washington. Abstract 469. King M, Bernstein B, Cernohous P, Mosely J, Bauer E, Sun E. Impact of baseline CD4 cell count and viral load on durability of virologic response through 96 weeks for lopinavir/ritonavir (LPV/r) and nelfinavir (NFV) in a phase III clinical trial. Program and abstracts of the 9th Conference on Retroviruses and Opportunistic Infections; February 24-28, 2002; Seattle, Washington. Abstract 470.")
16
Esquemas de ARV Potenciales
Existen 23 ARV disponibles. En teoría hay 600 combinaciones triples posibles. En realidad y debido a la resistencia cruzada solo de 3–4 esquemas se pueden aplicar a un solo caso. Éxito Falla Paciente virgen Paciente tratado Paciente multitratado

17
Planeación estratégica del tratamiento ARV
NAN AN IP NAN IP IP AN IP NAN

18
Estrategias para el éxito
Favorecer la supresión viral lo más posible por el mayor tiempo posible Favorecer el apego a los ARV Aprovechar las ventajas farmacocinéticas y farmacodinámicas Secuenciar fármacos de forma racional Preservar opciones futuras Utilizar herramientas de laboratorio adecuadamente (CV, CD4+,genotipo, etc)
")
19
Elección en primera línea
Eficacia Seguridad Efectos adversos autolimitados o de fácil tratamiento Tolerabilidad Adherencia Rescatabilidad El término “rescatabilidad” aunque informal, traduce la propiedad de un fármaco para permitir ser “rescatado”, esto es, permite opciones claras posteriores a su propia falla. No muchos antirretrovirales tienen esta propiedad, que es casi exclusiva de nelfinavir por su favorable perfil de mutaciones, que permite ante su falla usar otros fármacos de su propio grupo, Los IP´s.

20
¿Qué es una estrategia de secuenciación y como lograrla?
La estrategia de secuenciación se refiere al uso de ARV en primera línea de tratamiento que permite opciones futuras de tratamiento con otros agentes de la misma clase y contribuye a prolongar el tiempo total de tratamiento en los pacientes. Algunos IP´s como SQV permiten el uso de otras opciones de tratamiento con IP´s, cuando presenta falla, por su favorable perfil de mutaciones asociadas a resistencia. Estos deben ser considerado como primera opción de tratamiento para todos los pacientes con infección por VIH. LEER. NFV produce como mutación primaria la D30N, que además de disminuir la capacidad replicativa viral, no tiene resistencias cruzadas con el resto de los IP hasta ahora disponibles, lo que lo hace de elección en primera línea de tratamiento ARV.

21
¿Cómo se están usando actualmente los ARV?
2 NRTIs+PI PI = Nelfinavir 1st line 2nd line 2 NRTIs+NNRTI NNRTI = efavirenz 2 NRTIs+2nd PI PI = Lopinavir/r, saquinavir/r 3rd line

22
¿Cómo se están usando actualmente los ARV?
B 2 NRTIs+PI PI = Nelfinavir 2 NRTIs+NNRTI NNRTI = efavirenz, IP/r (SQV/r, IDV/r) 1st line 2nd line 2 NRTIs+NNRTI NNRTI = efavirenz 2 NRTIs+PI PI = Otros IP/r, EFV, NVP 2 NRTIs+2nd PI PI = Lopinavir/r, saquinavir/r 2 NRTIs+2nd PI PI = Lopinavir/r, saquinavir/r 3rd line
 1st line. 2nd line. 2 NRTIs+NNRTI. NNRTI = efavirenz. 2 NRTIs+PI. PI = Otros IP/r, EFV, NVP. 2 NRTIs+2nd PI. PI = Lopinavir/r, saquinavir/r. 2 NRTIs+2nd PI. PI = Lopinavir/r, saquinavir/r. 3rd line.")
23
¿Cómo se están usando actualmente los ARV?
B C 2 NRTIs+PI PI = Nelfinavir 2 NRTIs+NNRTI NNRTI = efavirenz, IP/r (SQV/r, IDV/r) 2 ITRN+IP / R SQV/r, ATV/r, LPV/r 1st line OR 2 NRTIs+NNRTI NNRTI = efavirenz 2 NRTIs+PI PI =Otros IP/r, EFV, NVP 2NRTIs+NNRTI(NNRTI = efavirenz 2nd line 2 NRTIs+2nd PI PI = Lopinavir/r, saquinavir/r 2 NRTIs+2nd PI PI = Lopinavir/r, saquinavir/r 2NRTIs+PI PI = doble booster ENF 3rd line Los virus resistentes empiezan a emerger y las opciones de tratamiento cada vez son más limitadas
 2 ITRN+IP / R. SQV/r, ATV/r, LPV/r. 1st line. OR. 2 NRTIs+NNRTI. NNRTI = efavirenz. 2 NRTIs+PI. PI =Otros IP/r, EFV, NVP. 2NRTIs+NNRTI(NNRTI = efavirenz. 2nd line. 2 NRTIs+2nd PI. PI = Lopinavir/r, saquinavir/r. 2 NRTIs+2nd PI. PI = Lopinavir/r, saquinavir/r. 2NRTIs+PI. PI = doble booster. ENF. 3rd line. Los virus resistentes empiezan a emerger y las opciones de tratamiento cada vez son más limitadas.")
24
Tratamiento del VIH Planificación a futuro
IP reforzado ? ? ? ? Inicio de tratamiento con IP´s RESCATES NFV + 2ITRAN SQV/r + 2ITRAN IP/r + EFV + 2ITRAN

25
Tratamiento del VIH Planificación a futuro
IP reforzado Duda resuelta, Otro IP/r e incluso ITRNN Inicio de tratamiento con IP´s RESCATES NFV + 2ITRAN SQV/r, ATV/r, otro IP/r ó + 2ITRAN ITRNN IP/r + EFV + 2ITRAN

26
Circulación Sistémica
¿Cómo actúa el refuerzo o booster? Circulación Sistémica Cmin > EC 50/90 SQV SQV HGC SQV SGC Vena Hepática Arteria hepática Absorción CYP450 Glycoprotein En el caso de saquinavir, como cualquier otro IP, tiene que lograrse una absorción eficiente y lo más completa posible, sin embargo esto se logra, ahora sabemos, de forma parcial y una parte del medicamento de excreta directamente por vía intestinal. Al pasar la mucosa intestinal, el fármaco se tiene que enfrentar a algunos sistemas enzimáticos que complicarán su farmacocinética principalmente en intestino y en hígado. El metabolismo hepático disminuirá la biodisponibilidad del fármaco por sus sistemas enzimáticos de detoxificación, lo que impedirá que el 100% del medicamento logre su objetivo. Los dos pasos más importantes a superar es, mejorar la absorción y disminuir la tasa de metabolismo del medicamento como podemos verlo en amarillo, para que finalmente al torrente circulatorio se vierta más fármaco disponible para actividad antiviral... Porta CYP450 3A4 Intestino Metabolismo

27
Circulación sistémica
RTV Cmin > EC50/90 SQV SQV HGC SQV SGC SQV Vena hepática Arteria hepática Metabolismo Absorción CYP450 Glycoprotein Con el refuerzo de dosis bajas de ritonavir aplicado a un IP, como saquinavir, logramos mejorar la absorción por medio del bloqueo de sistemas enzimáticos como el CYP450 en intestino. Después, ya con más fármaco “absorbido”, también en hígado se bloquea, pro acción del ritonavir, la actividad del sistema de citocromo p-450, lo que impide el rápido metabolismo del IP en acción, en este caso, saquinavir y llegará más fármaco al torrente circulatorio, como siempre es deseado. Esto no es otra cosa que, mejorar o REFORZAR la farmacocinética del IP. Además, a nivel intracelular actuará en otro sistema de depuración, el sistema de la glicoproteína de la membrana, que se encarga de detoxificar, “sacando” el fármaco del espacio intracelular. Al inhibir esta glicoproteína por medio del ritonavir, el saquinavir permanece más tiempo actuando a nivel intracelular lo que aporta otra ventaja más al mecanismo de acción antirretroviral. CYP450 Porta Intestino

28
No termine sus opciones prematuramente
Tiempo de terapia (años) Resistencia cruzada Regimen A Regimen B Regimen C Regimen D Falla
 Resistencia cruzada. Regimen A. Regimen B. Regimen C. Regimen D. Falla.")
29
Perdida de las opciones de tratamiento secuenciadas
Juicio convencional “La realidad” Tiempo Falla 1 Falla 1 Tiempo Falla 2 Las opciones son aún amplias en la falla 1 pero los esquemas posteriores serán afectados por la resistencia cruzada y quedaremos sin medicamentos con rapidez Falla 3 Falla 4

30
2006 Update of IAS-USA Guidelines for Initial Therapy
Recommended Components of Initial Antiretroviral Therapy* NRTIs NNRTIs PIs TDF/FTC† EFV LPV/RTV ZDV/3TC‡ (NVP) ATV/RTV ABC/3TC‡ FPV/RTV SQV/RTV 3TC, lamivudine; ABC, abacavir; ATV, atazanavir; EFV, efavirenz; FPV, fosamprenavir; FTC, emtricitabine; LPV, lopinavir; NVP, nevirapine; RTV, ritonvair; SQV, saquinavir; TDF, tenofovir; ZDV, zidovudine. *Therapy should consist of 2 NRTIs + either an NNRTI or PI. †Or 3TC. ‡Or FTC. Hammer S, et al. JAMA. 2006;296:
 ATV/RTV. ABC/3TC‡ FPV/RTV. SQV/RTV. 3TC, lamivudine; ABC, abacavir; ATV, atazanavir; EFV, efavirenz; FPV, fosamprenavir; FTC, emtricitabine; LPV, lopinavir; NVP, nevirapine; RTV, ritonvair; SQV, saquinavir; TDF, tenofovir; ZDV, zidovudine. *Therapy should consist of 2 NRTIs + either an NNRTI or PI. †Or 3TC. ‡Or FTC. Hammer S, et al. JAMA. 2006;296:")
31
2006 Update of IAS-USA Guidelines for Initial Therapy
Recommended Components of Initial Antiretroviral Therapy* NRTIs NNRTIs PIs TDF/FTC† EFV LPV/RTV ZDV/3TC‡ (NVP) ATV/RTV ABC/3TC‡ FPV/RTV SQV/RTV 3TC, lamivudine; ABC, abacavir; ATV, atazanavir; EFV, efavirenz; FPV, fosamprenavir; FTC, emtricitabine; LPV, lopinavir; NVP, nevirapine; RTV, ritonvair; SQV, saquinavir; TDF, tenofovir; ZDV, zidovudine. *Therapy should consist of 2 NRTIs + either an NNRTI or PI. †Or 3TC. ‡Or FTC. Hammer S, et al. JAMA. 2006;296:
 ATV/RTV. ABC/3TC‡ FPV/RTV. SQV/RTV. 3TC, lamivudine; ABC, abacavir; ATV, atazanavir; EFV, efavirenz; FPV, fosamprenavir; FTC, emtricitabine; LPV, lopinavir; NVP, nevirapine; RTV, ritonvair; SQV, saquinavir; TDF, tenofovir; ZDV, zidovudine. *Therapy should consist of 2 NRTIs + either an NNRTI or PI. †Or 3TC. ‡Or FTC. Hammer S, et al. JAMA. 2006;296:")
32
Esquemas más usuales Tercer componente (IP) SQV/r ATV/r IDV/r FPV/r
ITRN ZDV+LMV ZDV+ddI ZDV+ABC STV+ABC STV+LMV TDF+LMV TDF+FTC ABC+LMV Tercer componente (IP) SQV/r ATV/r IDV/r FPV/r LPV/r Ó ITRNN EFV NVP
 SQV/r. ATV/r. IDV/r. FPV/r. LPV/r. Ó ITRNN. EFV. NVP.")
33
Conclusiones 1a. Línea de tratamiento

34
¿Por qué SI, SQV/r? Alta barrera genética
Escaso producción de mutaciones de resistencia (Staccato, QUAD, MaxCmin) Alta tolerabilidad (no importó cantidad de cápsulas, mejora con SQV 500mg) Baja toxicidad Resultados a largo plazo Switch a presentación de tabletas sin merma de opciones terapéuticas.
 Alta tolerabilidad (no importó cantidad de cápsulas, mejora con SQV 500mg) Baja toxicidad. Resultados a largo plazo. Switch a presentación de tabletas sin merma de opciones terapéuticas.")
35
¿Por qué no, LPV/r? Alta barrera genética que impide secuenciación.
Alta toxicidad lipídica en márgenes prohibitivos en un porcentaje de pacientes (30% y 11%) Impide opciones futuras incluso las pensadas con nuevos fármacos como enfuvirtida a menos que se cuente con genotipo No ofrece ventajas de seguridad y eventos adversos como las manifestaciones gastrointestinales y otros que están presentes en el resto de los ARV.
 Impide opciones futuras incluso las pensadas con nuevos fármacos como enfuvirtida a menos que se cuente con genotipo. No ofrece ventajas de seguridad y eventos adversos como las manifestaciones gastrointestinales y otros que están presentes en el resto de los ARV.")
36
¿Por qué no, FPV/r? Alta incidencia de reacciones dermatológicas graves (rash aprox en 19%). Potencia similar a nelfinavir cuando se refuerza Resistencia cruzada con otros IP actuales No ofrece ventajas de seguridad y eventos adversos como las manifestaciones gastrointestinales y otros que están presentes en el resto de los ARV.

37
¿Por qué no, Efavirenz? Resistencia cruzada temprana con su grupo terapéutico. Alto costo en el manejo de eventos adversos en grupos de pacientes No ofrece ventajas con respecto a seguridad comparado con IP´s. (misma dislipidemia que SQV; FOCUS) Debería reservarse para tratamientos posteriores, para acompañar terapias doblebooster o nuevas terapias como la enfuvirtida, donde se usará por menos tiempo Los estudios a largo plazo, han mostrado una incidencia alta de efectos adversos psiquiátricos, difíciles de tratar y costosos para institución y pacientes.
 Debería reservarse para tratamientos posteriores, para acompañar terapias doblebooster o nuevas terapias como la enfuvirtida, donde se usará por menos tiempo. Los estudios a largo plazo, han mostrado una incidencia alta de efectos adversos psiquiátricos, difíciles de tratar y costosos para institución y pacientes.")
38
¿Por qué no, Indinavir? Alta resistencia cruzada
Recomendado solo en terapias booster, que han demostrado su aumento de toxicidad, renal y en general para IP´s Baja tolerabilidad en nuevos esquemas de tratamiento

39
¿Por qué no, Atazanavir? Tiene un perfil de seguridad parecido a todos los antirretrovirales. Presencia de hiperbilirrubinemia hasta en 15% de los pacientes tratados en los primeras 8 semanas Mismo patrón de mutaciones de resistencia que amprenavir y nelfinavir (no aporta ventajas) Experiencia en el manejo en la terapia antirretroviral (usar con reservas en pocos pacientes de inicio)
 Experiencia en el manejo en la terapia antirretroviral (usar con reservas en pocos pacientes de inicio)")
40
Conclusiones Optimización de los antirretrovirales en base a perfiles de resistencia Uso de ARV que permitan una correcta secuenciación Evitar resistencias cruzadas en los primeros esquemas de tratamiento, (en etapas posteriores será imposible) Uso de esquemas que demuestran seguridad y tolerabilidad (garantizan adherencia) Uso razonado de nucleósidos e inhibidores de proteasa, que es el grupo que ofrece la posibilidad de secuenciación real.
 Uso de esquemas que demuestran seguridad y tolerabilidad (garantizan adherencia) Uso razonado de nucleósidos e inhibidores de proteasa, que es el grupo que ofrece la posibilidad de secuenciación real.")
41
Conclusiones La guías terapéuticas representan una referencia de tratamiento que debe ser adecuada a nuestra realidad Los esquemas que ofrecen la posibilidad de ser rescatados deben ser elegidos en 1a. Línea de tratamiento Saquinavir otorga ventajas en estos aspectos como tratamiento de primera línea

42
Conclusión ¿Que debemos hacer?
Optimización de los antirretrovirales en base a perfiles de resistencia, seguridad y farmacoeconomía Uso de ARV que permitan secuenciación Evitar resistencias cruzadas documentadas Privilegiar esquemas que demuestran tolerabilidad y seguridad, no solo potencia… Uso razonado de nucleósidos e inhibidores de proteasa en la secuencia ARV

43
RESCATES

44
¿Qué pasa con las resistencias en la actualidad?

45
SPREAD: Transmitted Drug Resistance in Europe, 2002-2003
17-nation study in Europe and Israel 1083 newly diagnosed patients in Overall prevalence of any resistance: 9% 71% of pts with drug resistance had single mutation Implies little loss of susceptibility to boosted PIs 10 9.1 8 6 5.4 Prevalence of Mutations, , % For more information, go to: 4 3.0 2.6 2 0.7 Any NRTI NNRTI PI ≥ 2 Classes Wensing AMJ, et al. IAC Abstract TUAB00101.

46
Prevalence of Mutations, %
Transmitted Drug Resistance Over Time: SPREAD and CATCH Comparison of data from SPREAD (Europe and Israel) with earlier retrospective data from CATCH (Europe) 14 NRTI 12 NNRTI 10 PI 8 Prevalence of Mutations, % 6 For more information, go to: 4 2 96-97 98-99 02-03 CATCH SPREAD Wensing AMJ, et al. IAC Abstract TUAB00101.
 with earlier retrospective data from CATCH (Europe) 14. NRTI. 12. NNRTI. 10. PI. 8. Prevalence of Mutations, % 6. For more information, go to: Track=Resistance CATCH. SPREAD. Wensing AMJ, et al. IAC Abstract TUAB")
47
21st Century: Era of Reformulations, Coformulations, New Approaches
Year Reformulation Coformulation New Agents New Approaches 2000 ddI-EC LPV/RTV ZDV/3TC/ABC 2001 TDF 2002 EFV-600 3TC-300 d4T-XR* 2003 NFV 625 FPV ATV FTC ENF Fusion inhibitor 2004 ddI generic ABC/3TC TDF/FTC Entry inhibitors 2005 SQV 500 ZDV generic LPV/RTV tabs TPV Integrase inhibitors 2006 TDF/FTC/EFV DRV Maturation inhibitor 3TC, lamivudine; ABC, abacavir; ATV, atazanavir; d4T, stavudine; ddI, didanosine; DRV, darunavir; EFV, efavirenz; FTC, emtricitabine; LPV, lopinavir; NFV, nelfinavir; RTV, ritonavir; SQV, saquinavir; TDF, tenofovir; TPV, tipranavir; ZDV, zidovudine. The next 2 tables explore some of these specific reformulations, coformulations, and new approaches to therapy to which I have just referred. The first table lists the drug reformulations that have been developed between 2000 and The reformulated drugs come from all classes of antiretrovirals and function to increase bioavailability and decrease pill burden. We have also seen coformulations of a number of agents in the NRTI and PI classes and development of new agents. In 2003, for the first time since 1995, a new class was introduceda fusion inhibitor, enfuvirtide. Novel approaches have also been explored, that is, drugs that work at new and different points in the HIV infection cycle. These include entry inhibitors, integrase inhibitors, and maturation inhibitors. I will discuss some of those agents later in the presentation. So, in these last several years, we have seen prolific development of new drugs and new approaches.

48
Tratamiento de rescate
Concepto múltiple: Cualquier manejo cuando ya se usaron todos los ARVs disponibles. Cuando hay resistencia a los 3 tipos de medicamentos. Todos los manejos con ARV´s después de fallar el primer IP usado.

49
Tratamiento de rescate
Concepto: Falla virológica: falla virológica incompleta ó carece de respuesta RNAVIH a terapia ARV. -Rv incompleta: RNA VIH >400copias/ml por 24 semanas ó > 50 copia/ml por 48 semanas naive -Rebote virológico, posterior a supresión VIH, se detecta RNA VIH

50
Tratamiento de rescate
Concepto: Falla virológica: Falta de incremento CD cel/mm3, en el 1er año de tratamiento ó disminución por debajo del basal .(naive 150cel) Progresión clínica: Presencia ó recurrencia de eventos relacionados con infección VIH
 Progresión clínica: Presencia ó recurrencia de eventos relacionados con infección VIH.")
51
Tratamiento de rescate
Prescripción “a ciegas” y sin guía por GT: Lo habitual; solo se pueden generar pocos esquemas de manejo que funcionen (¡con un poco de suerte!) en forma adecuada (al margen de sus componentes). En general deberá considerarse como “tratamiento de rescate” todo aquel que se genere después de la falla del segundo esquema TARAA (bien secuenciado).
 en forma adecuada (al margen de sus componentes). En general deberá considerarse como tratamiento de rescate todo aquel que se genere después de la falla del segundo esquema TARAA (bien secuenciado).")
52
Razones para cambiar el TARAA
Tratamiento de rescate Razones para cambiar el TARAA Cambio de esquema sin falla virológica: Toxicidad/intolerancia. Simplificación???. Cambio de esquema con falla virológica: Utilidad del GT. Cambio de medicamentos (al menos 2 o todos) Suspensión (IET): CD4+ y CV basal adecuadas. Riesgo/beneficio. Deseos del paciente.
 Suspensión (IET): CD4+ y CV basal adecuadas. Riesgo/beneficio. Deseos del paciente.")
53
Tratamiento de rescate
Rescate con LPV/r LPV ha mejorado los Tx de rescate; debe considerarse seriamente las severas alteraciones de los lípidos que produce. Alta barrera genética. Benéfico en casos con historia de manejo extensa. Su uso con otros IPs, debe considerarse después del fracaso del primer IP, (requiere de 6-8 mutaciones para su falla), pero no es elegible para su uso en pacientes sin manejo previo. Kempf et al 2001
, pero no es elegible para su uso en pacientes sin manejo previo. Kempf et al")
54
Tratamiento de rescate
Rescate con doble esquema de IP reforzado Abordaje actual y útil; uso de bajas dosis de RTV como refuerzo de otros IP (todos excepto NFV). IDV puede en frecuencia y severidad de efectos secundarios renales al ser reforzado. El mas efectivo es LPV/r+SQV por la sinergia existente entre ambos; no se afecta como LPV+APV. El uso conjunto de LPV con FPV también resulta en de las concentraciones de ambos. Los resultados clínicos han demostrado también mejores resultados con la combinación LPV+SQV que con la de LPV+APV. Molla et al. 2002 ACTG A5234 Zala et al 2002
. IDV puede en frecuencia y severidad de efectos secundarios renales al ser reforzado. El mas efectivo es LPV/r+SQV por la sinergia existente entre ambos; no se afecta como LPV+APV. El uso conjunto de LPV con FPV también resulta en de las concentraciones de ambos. Los resultados clínicos han demostrado también mejores resultados con la combinación LPV+SQV que con la de LPV+APV. Molla et al ACTG A5234. Zala et al")
55
Estudios de PK con esquemas de 2 IPs “reforzados”
Atazanavir + Saquinavir + /r: Esquema de una vez al día: 300/1600/100 mg QD. ATV y /r independientemente los niveles de SQV. Pendientes estudios de seguridad y eficacia. Fosamprenavir + Saquinavir + /r: Estudios con 700/ o 100 mg BID. Dosis óptima de /r: 200 mg. /r 100 mg solo si se hace TDM. Bien tolerado. A number of pharmacokinetic studies examined interactions between dual-boosted protease inhibitors Atazanavir + Saquinavir + Ritonavir One study evaluated ATV, SQV and RTV - an all once-daily regimen that investigated SQV levels when given with RTV and when given with both ATV and RTV in 18 HIV-infected patients SQV levels were higher when coadministered with both ATV and RTV, compared with administration of SQV with RTV alone (SQV geometric mean trough concentration 184 vs 87 ng/mL), indicating that ATV and RTV have independent effects in boosting SQV concentrations In general, the regimen was well tolerated in this small study, although increases in total and indirect bilirubin were seen, and 4 of 20 patients developed scleral icterus and 2 jaundice The atazanavir concentrations were comparable with those seen with an atazanavir/ritonavir 300/100 regimen Fosamprenavir + Saquinavir + Ritonavir In a second study, SQV levels were determined with a dose of SQV/RTV 1000/100 mg BID, and then compared to SQV levels after the addition of FOS 700 mg BID, in a total of 18 HIV-infected patients SQV levels were reduced with the addition of FOS, probably because of the enzyme-inducing effects of amprenavir When an additional 100 mg of RTV was added to the regimen (ie, FOS/SQV/RTV 700/1000/200 mg BID), the SQV levels were the same as if given with RTV alone The regimen was well tolerated - and the data are promising for further evaluation of this regimen It appears that the interactions among these three agents can be effectively managed, which is in contrast to the interactions among a fosamprenavir, lopinavir/ritonavir regimen (discussed on the next slide) Both of these dual-boosted PI regimens require further clinical studies to evaluate their safety and virologic efficacy Boffito M, et al. #607. CROI 2004
, indicating that ATV and RTV have independent effects in boosting SQV concentrations. In general, the regimen was well tolerated in this small study, although increases in total and indirect bilirubin were seen, and 4 of 20 patients developed scleral icterus and 2 jaundice. The atazanavir concentrations were comparable with those seen with an atazanavir/ritonavir 300/100 regimen. Fosamprenavir + Saquinavir + Ritonavir. In a second study, SQV levels were determined with a dose of SQV/RTV 1000/100 mg BID, and then compared to SQV levels after the addition of FOS 700 mg BID, in a total of 18 HIV-infected patients. SQV levels were reduced with the addition of FOS, probably because of the enzyme-inducing effects of amprenavir. When an additional 100 mg of RTV was added to the regimen (ie, FOS/SQV/RTV 700/1000/200 mg BID), the SQV levels were the same as if given with RTV alone. The regimen was well tolerated - and the data are promising for further evaluation of this regimen. It appears that the interactions among these three agents can be effectively managed, which is in contrast to the interactions among a fosamprenavir, lopinavir/ritonavir regimen (discussed on the next slide) Both of these dual-boosted PI regimens require further clinical studies to evaluate their safety and virologic efficacy. Boffito M, et al. #607. CROI")
56
Estudios de PK con esquemas de 2 IPs “reforzados”
Fosamprenavir + Lopinavir/r: PK puede ser diferente que para APV + LPV/r: APV y LPV/r. La repercusión en los niveles de APV no se corrigen: Separando las dosis 4-12 hs. Dando /r 200 mg. FAPV a 1400 mg BID. Mal tolerado (GI). No debe usarse. Two pharmacokinetic studies examined the interactions between FOS and LPV/RTV Previous work has shown that when FOS and LPV/RTV are coadministered there are substantial and significant reductions in the concentrations of amprenavir (when given as FOS) and LPV These two studies investigated different strategies to try to manage these drug interactions One study (abstract 612) investigated different doses of both drugs The control regimen was FOS 700 mg and LPV/RTV 400/100 mg, all given BID The study treatments were: FOS 1400 mg BID + LPV/RTV 533/133 mg, and FOS 700 mg + RTV 100 mg + LPV/RTV 400/100 LPV/r mg, all BID Concentrations of APV and LPV were measured With both strategies, concentrations of APV were still substantially reduced (> 50%) compared with the control arm In addition, in both strategies there were a large number of withdrawals for adverse events The authors concluded that neither of these strategies were successful in correcting the drug interactions, and that the drugs should not be coadministered as no dosing recommendations can be made Abstract 611 examined the same interaction, but investigated different methods of trying to overcome the interaction, including a 4-hour separation in the administration of FOS (700 mg mg of RTV BID) and LPV/RTV (400/100 mg BID), and a 12-hour separation with once-daily administration (FOS 1400 mg mg RTV once daily in the AM, and LPV/RTV 800/200 mg once daily in the PM) Compared with the control regimen in which drugs were administered simultaneously, separating the dosages by either 4 hours or 12 hours did not correct the substantial reduction seen in APV concentrations Consistent with the authors of abstract 612, these authors also recommended that these drugs not be used in combination as no dose recommendation can be made The bottom line remains that FOS and LPV/RTV should not be coadministered at this time as no dosing recommendations can be made that overcome the drug interaction Corbett AH, et al. #611. CROI 2004 2. Wire MB, et al. #612. CROI 2004
. No debe usarse. Two pharmacokinetic studies examined the interactions between FOS and LPV/RTV. Previous work has shown that when FOS and LPV/RTV are coadministered there are substantial and significant reductions in the concentrations of amprenavir (when given as FOS) and LPV. These two studies investigated different strategies to try to manage these drug interactions. One study (abstract 612) investigated different doses of both drugs. The control regimen was FOS 700 mg and LPV/RTV 400/100 mg, all given BID. The study treatments were: FOS 1400 mg BID + LPV/RTV 533/133 mg, and. FOS 700 mg + RTV 100 mg + LPV/RTV 400/100 LPV/r mg, all BID. Concentrations of APV and LPV were measured. With both strategies, concentrations of APV were still substantially reduced (> 50%) compared with the control arm. In addition, in both strategies there were a large number of withdrawals for adverse events. The authors concluded that neither of these strategies were successful in correcting the drug interactions, and that the drugs should not be coadministered as no dosing recommendations can be made. Abstract 611 examined the same interaction, but investigated different methods of trying to overcome the interaction, including. a 4-hour separation in the administration of FOS (700 mg mg of RTV BID) and LPV/RTV (400/100 mg BID), and. a 12-hour separation with once-daily administration (FOS 1400 mg mg RTV once daily in the AM, and LPV/RTV 800/200 mg once daily in the PM) Compared with the control regimen in which drugs were administered simultaneously, separating the dosages by either 4 hours or 12 hours did not correct the substantial reduction seen in APV concentrations. Consistent with the authors of abstract 612, these authors also recommended that these drugs not be used in combination as no dose recommendation can be made. The bottom line remains that FOS and LPV/RTV should not be coadministered at this time as no dosing recommendations can be made that overcome the drug interaction. Corbett AH, et al. #611. CROI Wire MB, et al. #612. CROI")
57
Tiempo de cambio de Tx En presencia de supresión incompleta el paso del tiempo acumula mutaciones El cambio temprano o la intensificación, frena las mutaciones. El cambio tardio se asocia a pobre respuesta. Primer esquema Acumulo de mutaciones Segundo esquema Tardío Intermedio Carga Viral Temprano Tiempo Gallant J.-2002

58
El tiempo como factor determinante del grado de resistencia a IP
Tiempo de falla “No esperar mucho tiempo para cambiar tratamiento” Número de mutantes Respuesta a otros medicamentos

59
ELECCIÓN DEL SEGUNDO ESQUEMA ANTIRRETROVIRAL
DE ACUERDO AL TRATAMIENTO USADO. Esquema inicial Primer rescate ESQUEMA INICIAL CON 2 ITRAN Y 1 ITRNN 2 ITRAN + EFV o NVP 2 nuevos ITRAN* + NFV ó SQV/rit (recordar no adecuado p / secuencia) ESQUEMA INICIAL CON 2 ITRAN Y 1 IP 2 ITRAN + NFV 2 nuevos ITRAN* + SQV/rit ó IDV/ r (recordar toxicidad) 2 ITRAN + SQV 2 nuevos ITRAN* + SQV/r ó AMP/rit 2 ITRAN + AMP 2 nuevos ITRAN* + SQV/r ó LPV/rit ESQUEMA INICIAL CON 2 ITRAN Y 2 IP (DOSIS COMPLETA O REFORZADO)** 2 ITRAN + SQV/rit 2 ITRAN + AMP/rit 2 ITRAN + LPV/rit NO EXISTE UNA OPCION CLARA PARA SECUENCIAR 2 ITRAN + SQV/RIT 400/ 400 ESQUEMA INICIAL CON TRIPLE NUCLEOSIDO AZT-3TC-ABC D4T-ddI-NFV ó IDV/rit ó SQV/rit Otras combinaciones de 3 ITRAN 2 nuevos ITRAN* + NFV (difícilmente no nucleósidos, por Resist cruzada Probablemente, booser y doble booster Probablemente doble booster
 ESQUEMA INICIAL CON 2 ITRAN Y 1 IP. 2 ITRAN + NFV. 2 nuevos ITRAN* + SQV/rit ó IDV/ r (recordar toxicidad) 2 ITRAN + SQV. 2 nuevos ITRAN* + SQV/r ó AMP/rit. 2 ITRAN + AMP. 2 nuevos ITRAN* + SQV/r ó LPV/rit. ESQUEMA INICIAL CON 2 ITRAN Y 2 IP (DOSIS COMPLETA O REFORZADO)** 2 ITRAN + SQV/rit. 2 ITRAN + AMP/rit. 2 ITRAN + LPV/rit. NO EXISTE UNA OPCION CLARA PARA SECUENCIAR. 2 ITRAN + SQV/RIT 400/ 400. ESQUEMA INICIAL CON TRIPLE NUCLEOSIDO. AZT-3TC-ABC. D4T-ddI-NFV ó IDV/rit ó SQV/rit. Otras combinaciones de 3 ITRAN. 2 nuevos ITRAN* + NFV (difícilmente no nucleósidos, por Resist cruzada. Probablemente, booser y doble booster. Probablemente doble booster.")
60
Secuencia de TARAA= un éxito terapéutico
A Éxito virológico!

61
Enfuvirtida FuzeonTM

62
Mecanismo de Acción Aproximación de la partícula viral a los
receptores CD4 Adhesión de la gp 120 a los receptores CD4 Unión de la proteína gp 120 a los co-receptores CD4+ Desprendimiento de la proteína gp 120 Inserción de la gp 41 Retracción de la partícula viral hacia la célula Inhibe la fusión Aparece FUZEON

63
Enfuvirtida + TO cambio promedio de CV y CD4 desde el inicio (On-Treatment)
166 150 119 CD4 mean change from BL 100 CD4 50 Viral load -1.0 RNA mean change from BL - 1.90 - 2.07 -2.0 8 16 24 32 40 48 56 64 72 80 88 96 Study Week CD4 661 478 337 VL 661 495 352

64
Conclusiones La carga viral disminuye considerablemente desde el inicio de la terapia La respuesta de CD4s y CV se mantiene durante 96 semanas FUZEON fue bien tolerado y en general no se relaciono con toxicidad sistémica No se presentaron eventos adversos adicionales entre la semana 48 y la 96. La reacción en el sitio de la inyección fue el evento adverso presente.

65
RESIST 1 TPV/r vs Otros IP/r En presencia de mutaciones a IP
En ausencia de mutaciones a IP (1-2) Análisis a 24 semanas Porcentaje de pacientes con eficacia (> 1 log) Schapiro
 Análisis a 24 semanas. Porcentaje de pacientes con. eficacia (> 1 log) Schapiro.")
68
RESIST 2 TPV/r vs LPV/r Terapia optimizada por genotipo
Dos medicamentos activos Pacientes pretratados 2 1.5 LPV/r TPV/r (log promedio) Carga viral 1 0.5 semanas Cooper
 Carga viral semanas. Cooper.")
69
Booster de TMC (power) Estudio en pacientes con
experiencia triple clase Seguimiento a 24 semanas (multicéntrico) TO+ENF+TMC 114/r (600/100mg BID) vs Otro IP/r La dosis ya fue seleccionada Tolerancia adecuada y comparable a otros esquemas booster 2 -1.85 -0.72 RNA CV log (-) TMC 1 % pts CV < 50 copias IP/r Haubrich
 TO+ENF+TMC 114/r (600/100mg BID) vs Otro IP/r. La dosis ya fue seleccionada. Tolerancia adecuada y comparable a otros esquemas booster RNA CV log (-) TMC. 1. % pts CV < 50 copias. IP/r. Haubrich.")
71
Estimated Timeline for New Antiretrovirals
CXCR4 inhibitors Entry inhibitor (anti-gp120, CCR5) GS-9137 Maturation inhibitor MK-0518 TNX-355 Integrase inhibitor Maraviroc PA-457 2006 2007 2008 2009 2010 This is my personal estimation on the timeline for new antiretrovirals. Some of these drugs, such as MK-0518 and etravirine, are now available through expanded access schemes for use in treatment-experienced patients. Etravirine TMC278 PI Brecanavir NNRTI Vicriviroc Apricitabine NRTI
 GS Maturation inhibitor. MK TNX-355. Integrase inhibitor. Maraviroc. PA This is my personal estimation on the timeline for new antiretrovirals. Some of these drugs, such as MK-0518 and etravirine, are now available through expanded access schemes for use in treatment-experienced patients. Etravirine. TMC278. PI. Brecanavir. NNRTI. Vicriviroc. Apricitabine. NRTI.")
72
Conclusión Rescates Surgen cada vez más antirretrovirales de los mismo grupos existentes, aun esperamos llegada de otros inhibidores de entrada o de integrasa. La última innovación fue enfuvirtida por su distinto mecanismo de acción (IF). En los estudios con fármacos anteriores y actuales, Enfuvirtida ha marcado una diferencia evidente en los resultados de carga viral y CD4, con respecto a esquemas sin enfuvirtida (TPV y Darunavir)
. En los estudios con fármacos anteriores y actuales, Enfuvirtida ha marcado una diferencia evidente en los resultados de carga viral y CD4, con respecto a esquemas sin enfuvirtida (TPV y Darunavir)")
Presentaciones similares









>")







>")


