Descargar la presentación
La descarga está en progreso. Por favor, espere

1
CASO VIERNES Dr. Catalá, Andrés

2
Motivo de consulta Neurólogo solicita estudio para detectar organicidad. 38 años, episodios iterativos de convulsiones diarias desde hace 1 semana. Hace 8 años mismo episodio resolviendo espontáneamente. Abuelo fallecido por tumor cerebral. No cefalea ni otra signosintomatología asociada a déficit focal neurológico. Sin antecedentes de consumo de medicación. No traumatismos.

7
Diagnósticos diferenciales
Metástasis cerebral Absceso cerebral piogénico Tuberculoma Infección fúngica Infección parasitaria Espacios vasculares

8
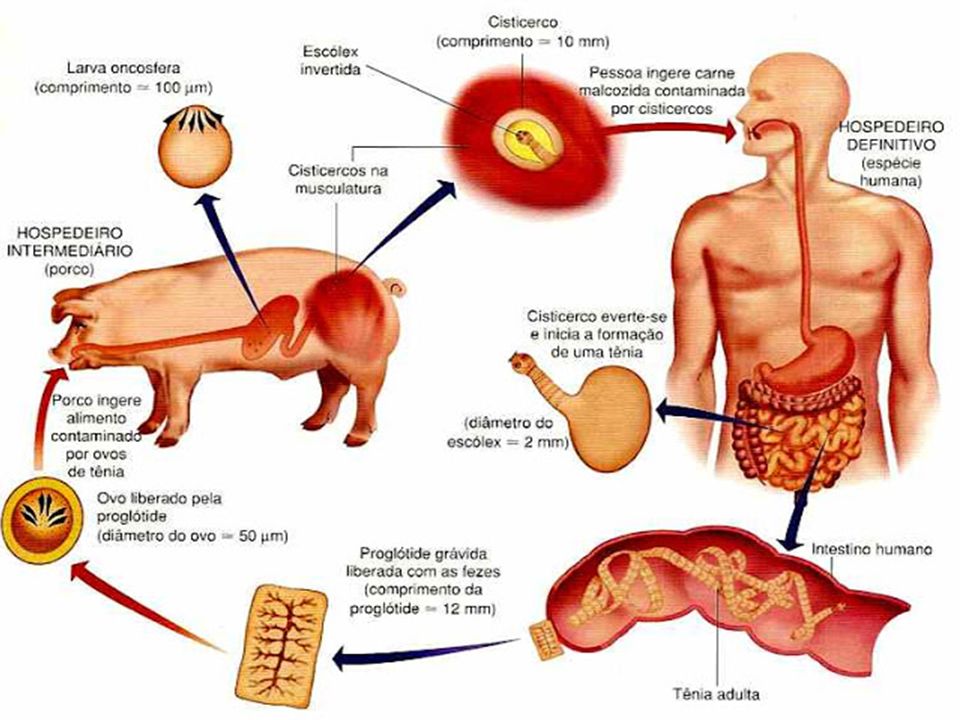
Neurocisticercosis

11
Estadíos Vesicular Vesicular- coloide Nodular-granular
Nodular calcificado Subaracnoideo Intraventricular Cisternal Demographics and clinical presentation The disease is endemic in Central and South America, Asia and Africa. There is a variable time interval between point of infection and the onset of symptoms (ranging from 1-30 years). Clinical presentation includes 1 : seizures - most common cause of seizures in young adults in endemic areas 2 headaches hydrocephalus altered mental status neurological deficits
. Clinical presentation includes 1 : seizures - most common cause of seizures in young adults in endemic areas 2 headaches. hydrocephalus. altered mental status. neurological deficits.")
12
Estadío Vesicular DOT SIGN
Pre and post contrast CT images through the brain demonstrates a hyperdense rounded focus in the region of the cuneus / precuneus surrounded by a small amount of oedema. Following contrast administration there is prominent ring enhancement with a central dot ("cyst with dot sign").
.")
15
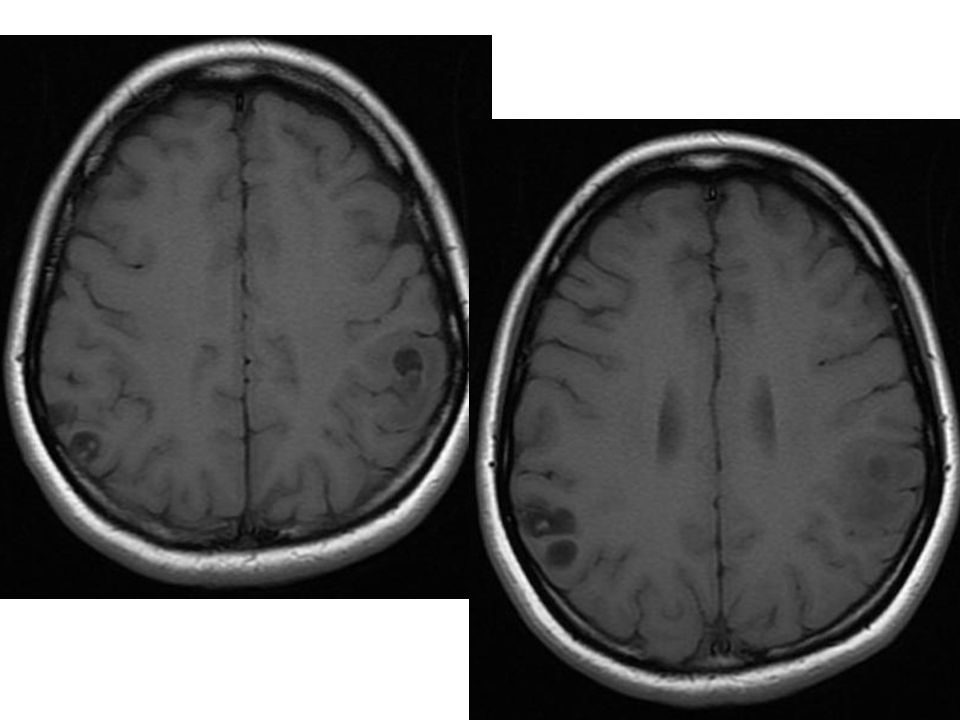
Estadío Vesicular Coloide
Brain tumors show predominant white matter edema, unless this cysts which usually have grey and white matter edema.

16
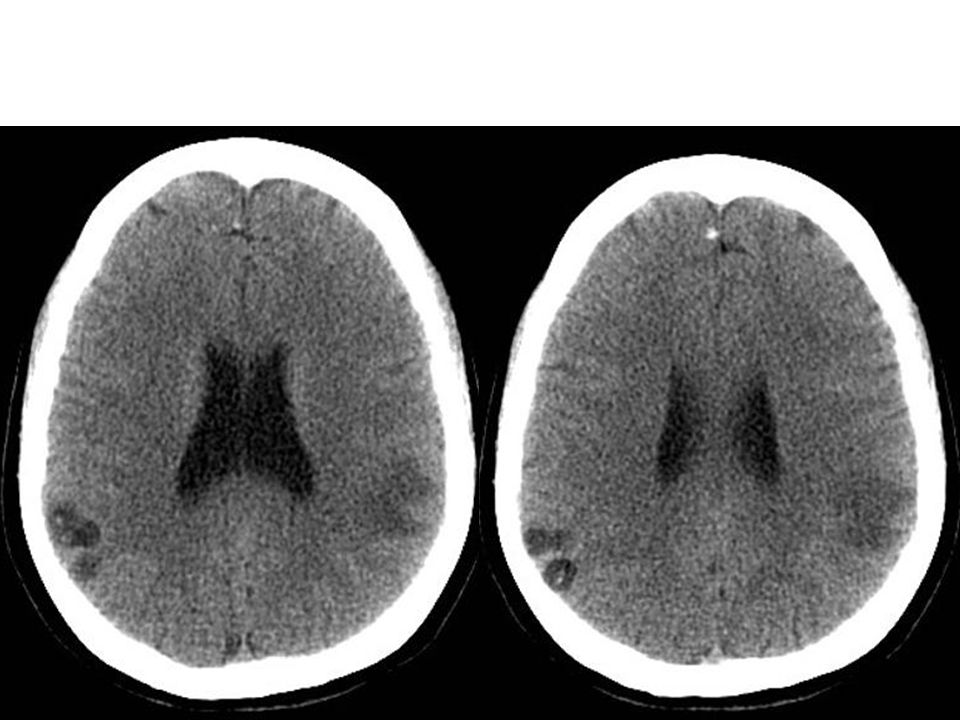
Estadío Nodular- granuloma
On CT he had a well defined a 0.8 x 1.0 cm.round lesion seen in the left frontal region..The centreof the lesion was hypointense,with a calcific focus in the periphery.There was ring enhancement of the lesion.Grade 1 odema was seen around the lesion.Rest of the brain parenchyma,ventricles,scalp were normal. The cyst as it degenerates and dies, sets up an inflammatory reaction that can act as an epileptic focus. Once dead and calcified these lesions are less likely to cause epilepsy and are often an incidental finding on CT brain performed for another clinical reason.

17
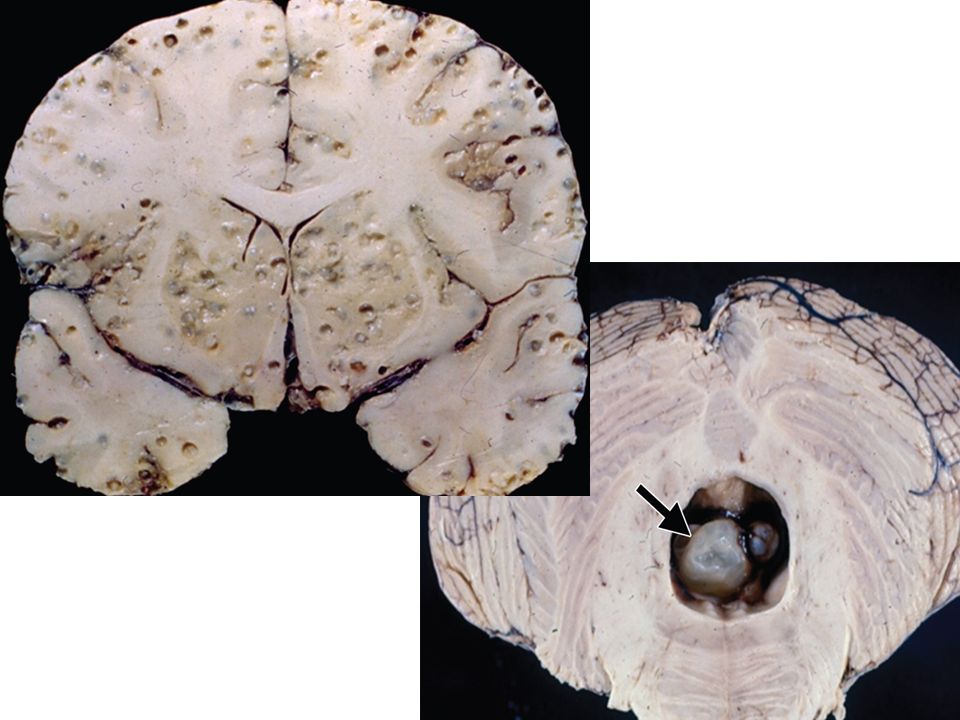
Estadío Nódulo calcificado

18
Complicaciones Subaracnoidea: Arteritis con o sin infartos.
Respuesta inflamatoria: gliosis, edema y aracnoiditis Si es Intraventricular: cierto grado de obstrucción. Síndrome de HTE.

19
Diagnósticos diferenciales
Metástasis Tuberculoma Espacios vasculares Absceso piogénico

20
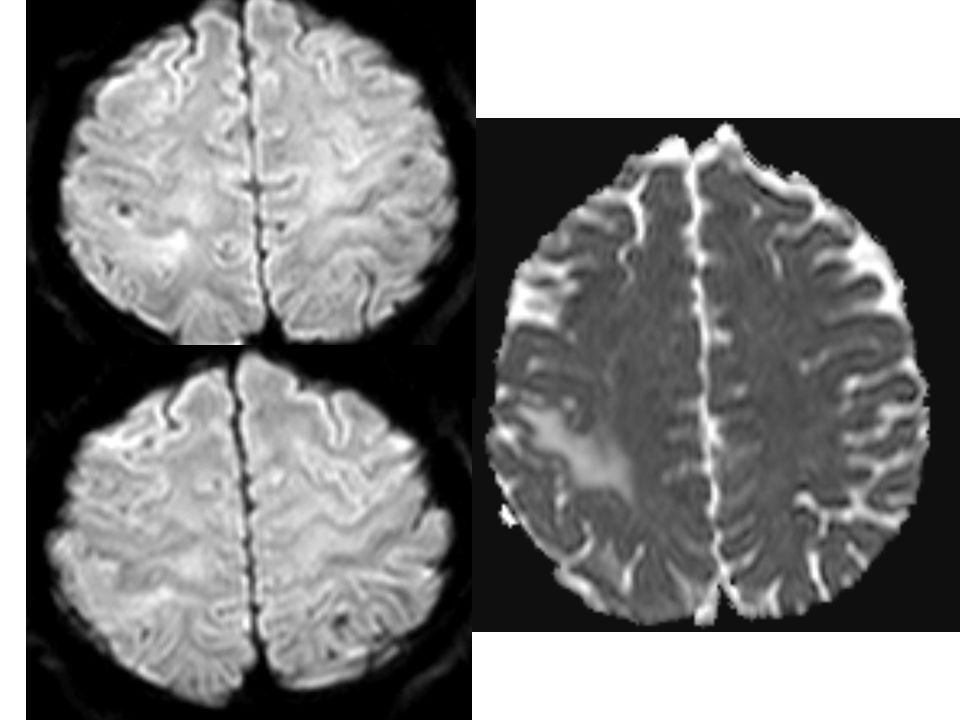
Metástasis Within the parieto-occipital region on the left is a very rounded brightly peripherally enhancing mass located near the grey-white junction, surrounded by a moderate amount of vasogenic oedema. The central region of lower signal intensity does not enhance nor does it restrict (DWI not shown). Features are consistent with the patient's known metastatic disease. SIGNO DEL OJO DE TORO O DEL TIRO AL BLANCO. Tb aparece en abceso cerebral.
. Features are consistent with the patient s known metastatic disease. SIGNO DEL OJO DE TORO O DEL TIRO AL BLANCO. Tb aparece en abceso cerebral.")
21
Tuberculoma Hiv negativo de filipinas

22
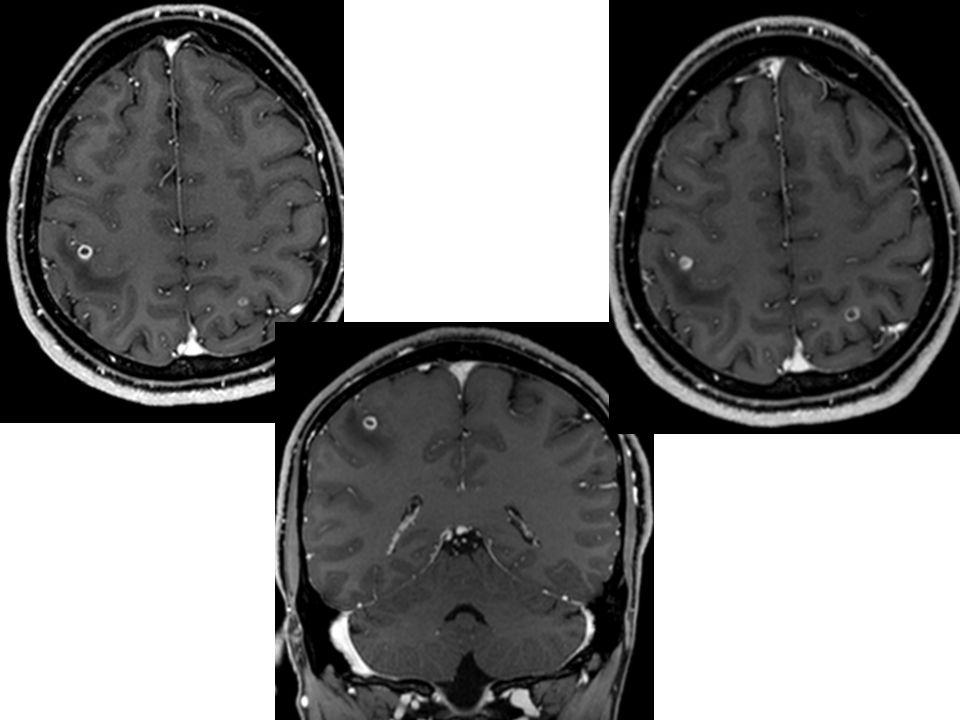
Absceso piogénico Multiple cerebral ring enhancing lesions with central restricted diffusion and surrounding oedema. Case Discussion: Typical appearances of cerebral abscesses. Note the T2 dark rim.

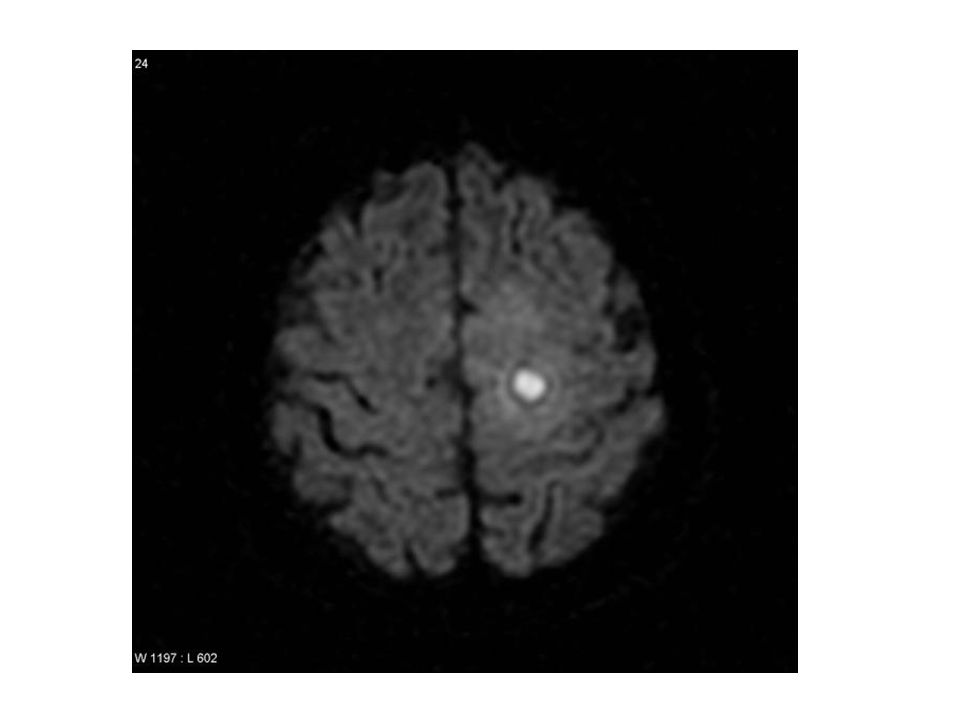
24
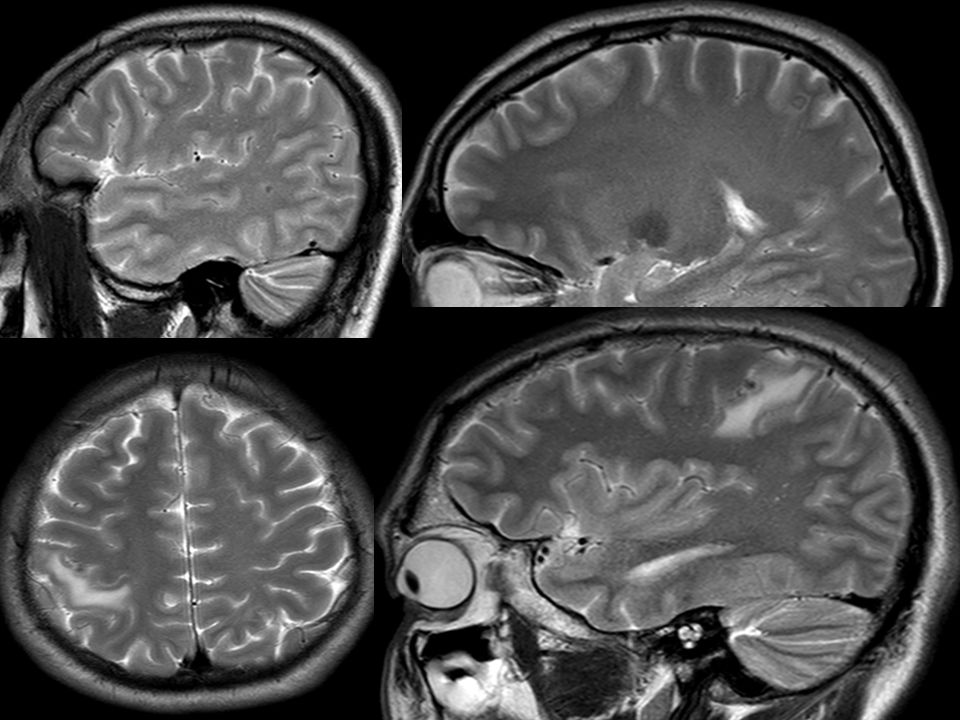
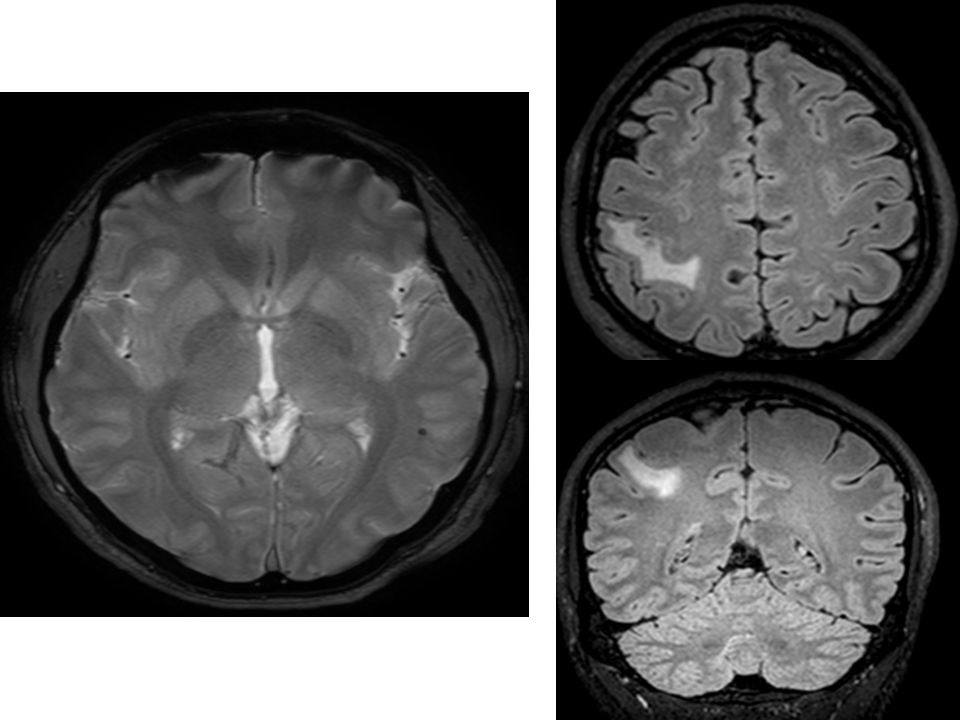
Espacios vasculares : DIAG DIFERENCIAL CON DOT SIGN IN THE CYST de NEUROCISTICERCOSIS. Peri vascular spaces (PVS), also known as Virchow-Robin (VR) spaces, are pial lined intersitital fluid filled spaces that surround perforating vessels 1. They do not have a direct connection with the subarachnoid space and in fact the fluid within them is slightly different. MRI of the brain demonstrates numerous CSF intensity spaces scattered through the left frontal lobe. These align themselves with white matter tracts and perimedullary veins. The content fully attenuates on FLAIR and there is surrounding gliosis or enhancement. Although prominent in size and atypical in location appearances are consistent with incidentalperivascular spaces. They are typically less than 5 mm in diameter, but can reach much larger sizes, so calledgiant peri vascular space or tumefactive perivascular space, and can exert enough mass effect to be symptomatic. They tend to enlarge with age and with hypertension. When very numerous the brain can have a colander-like appearance referred to as etat crible(as opposed to numerous lacunes = etat lacunaire) Most commonly they are located in the lower half of the basal ganglia especially along the line of the anterior commissure 3. They are also found in substantia nigra dentate nucleus subinsular region - "subinsular bright spots" corpus callosum and cingulate gyrus The cortical regions are spared. In contrast to lacunar infarcts encountered more frequently in the upper half of the putamen, perivascular spaces are seen more often in the lower half. Types Perivascular spaces are divided into three main types 4: type 1 - located in the area supplied by the lenticulostriate arteries entering the basal ganglia. type 2 - located in the area supplied by the perforating medullary arteries as they enter the cortical gray matter. type 3 - located in the midbrain. Associations They are usually idiopathic, although they are seen in greater frequency in mucopolysaccharidoses 1, e.g. Hunter disease, Hurler disease some muscular dystrophies
, also known as Virchow-Robin (VR) spaces, are pial lined intersitital fluid filled spaces that surround perforating vessels 1. They do not have a direct connection with the subarachnoid space and in fact the fluid within them is slightly different. MRI of the brain demonstrates numerous CSF intensity spaces scattered through the left frontal lobe. These align themselves with white matter tracts and perimedullary veins. The content fully attenuates on FLAIR and there is surrounding gliosis or enhancement. Although prominent in size and atypical in location appearances are consistent with incidentalperivascular spaces. They are typically less than 5 mm in diameter, but can reach much larger sizes, so calledgiant peri vascular space or tumefactive perivascular space, and can exert enough mass effect to be symptomatic. They tend to enlarge with age and with hypertension. When very numerous the brain can have a colander-like appearance referred to as etat crible(as opposed to numerous lacunes = etat lacunaire) Most commonly they are located in the lower half of the basal ganglia especially along the line of the anterior commissure 3. They are also found in substantia nigra. dentate nucleus. subinsular region - subinsular bright spots corpus callosum and cingulate gyrus. The cortical regions are spared. In contrast to lacunar infarcts encountered more frequently in the upper half of the putamen, perivascular spaces are seen more often in the lower half. Types. Perivascular spaces are divided into three main types 4: type 1 - located in the area supplied by the lenticulostriate arteries entering the basal ganglia. type 2 - located in the area supplied by the perforating medullary arteries as they enter the cortical gray matter. type 3 - located in the midbrain. Associations. They are usually idiopathic, although they are seen in greater frequency in. mucopolysaccharidoses 1, e.g. Hunter disease, Hurler disease. some muscular dystrophies.")
25
Differential diagnosis
For small "run of the mill" PVSs consider -choroid fissure cyst -lacunar infarcts rim of gliosis seen best on FLAIR neutral or negative mass effect -neurocysticercosis cyst with a dot sign enhancement calcification -CNS cryptococcosis : if multiple

26
Albendazol y prazicuantel
Tratamiento Albendazol y prazicuantel

27
Bibliografía y webgrafía
STAT DX Radiopaedia Radiographics:

28
Muchas gracias!

Presentaciones similares







 SÍNDROMES FOCALES (TRONCO ENCÉFALO) CLÍNICA EPILEPSIA ESCLEROSIS MÚLTIPLE. CLÍNICA CEFALEAS.>")








>")


