Descargar la presentación
La descarga está en progreso. Por favor, espere

1
TRATAMIENTO DE LA BIPOLARIDAD
Dr. Eugenio Olea B. Unidad Docente Facultad de Medicina de la Universidad de Chile-Instituto Psiquiátrico Vicepresidente de la Sociedad Chilena de Psiquiatría Biológica

2
COMPLEJIDAD CLÍNICA DE LA BIPOLARIDAD
TRATAMIENTO EN LAS DIFERENTES ETAPAS ESTRUCTURACIÓN DE LA TERAPIA GUIAS CLÍNICAS

3
The heterogeneity of bipolar disorder
What factors contribute? Comorbid conditions Severity of illness Presentation Presence of Mild Rapid cycling Psychosis Substance dependence Mixed episodes Depression Personality disorder Moderate Anxiety Phobias Severe PTSD Agitation = multiple treatment targets ADHD Aggression PTSD = post-traumatic stress disorder; ADHD = attention deficit hyperactivity disorder; OCD = obsessive compulsive disorder OCD

4
EVOLUCION DE LOS TRASTORNOS DEL ANIMO

5
Multidimensionalidad del Trastorno Bipolar
Mania subsindromática (Hipomania) Mania Depresión Mantención (Distimia) Bipolar disorder is multidimensional{163;} As previously mentioned, bipolar disorder is characterized by dramatic mood swings. This schematic illustrates the multidimensionality of the disease. Between full-blown manic and depressive episodes, patients may also experience subsyndromal depression or mania. Resolution of an episode, on its own or with treatment, results in a normal mood state being maintained until the next episode. Some patients may meet the criteria for both a manic and a depressive episode in the same period, resulting in a mixed state.
 Mania. Depresión. Mantención. (Distimia) Bipolar disorder is multidimensional{163;} As previously mentioned, bipolar disorder is characterized by dramatic mood swings. This schematic illustrates the multidimensionality of the disease. Between full-blown manic and depressive episodes, patients may also experience subsyndromal depression or mania. Resolution of an episode, on its own or with treatment, results in a normal mood state being maintained until the next episode. Some patients may meet the criteria for both a manic and a depressive episode in the same period, resulting in a mixed state.")
6
Tipos Clínicos Trastorno Bipolar I Manía Unipolar Trastorno Bipolar II
Manía Psicótica Episodios Mixtos Cicladores rápidos Trastorno Bipolar II Ciclotimia

7
TRATAMIENTO

8
Paradigma Terapéutico en Bipolaridad
Estabilizador adicional Antipsicótico Antidepresivo Ansiolítico Estabilizador fundamental

9
Qué es un antimaníaco fundamental?
Un medicamento que se considera básico para el tratamiento, ya sea de la fase aguda como la de mantención de la enfermedad Tiene que ser capaz de: Estabilizar los síntomas maníacos de fase aguda Cooperar para el manejo de los síntomas depresivos Cooperar en la prevención de recurrencias, tanto depresivas como maníacas

10
Tratamiento Farmacoterapia. Aguda y profiláctica
Estabilizadores del ánimo Antipsicóticos Antidepresivos Psicoterapia y Psicoeducación Rehabilitación

11
Medicamentos Utilizados en Trastorno Bipolar I Centro Stanley de Trastorno Bipolar
Monoterapia 2 medicamentos 3 medicamentos 4 o más medicamentos % del Total.N= 457 19% 28% 25%

12
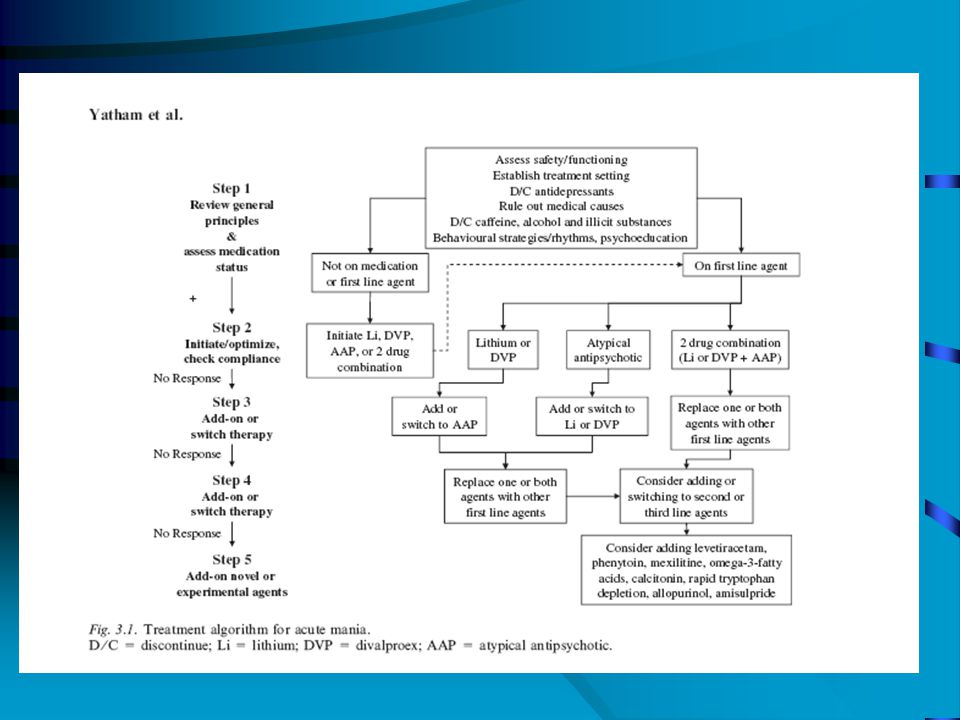
OPCIONES DE TRTATAMIENTO
Litio Antipsicóticos atípicos Olanzapina Risperidona Quetiapina Ziprasidona Aripiprazol Clozapina Antipsicóticos típicos Haloperidol Clorpromazina Valproato Lamotrigina Carbamazepina Otros anticonvulsivos Antidepresivos A range of agents are available. These have been approved either for specific uses in bipolar disorder or for uses other than in bipolar patients, such as for schizophrenia, seizures and unipolar depression.

13
Eficacia del Litio Euphoric mania 60% Mixed state 40%
Psychotic mania % Rapid cycling (3–4 episodes/year) % Ultra-rapid cycling (episode cycles within weeks/days) ~ placebo Ultra-ultra rapid cycling ~ placebo (episode cycles within hours) Silverstone T, Romans S. Drugs 1996;51:367–82 Maj M et al. Psychopharmacology (Berl) 1989;98:535–8 Post RM et al. Neuropsychopharmacology 1998;19:206–19
 25% Ultra-rapid cycling (episode cycles within weeks/days) ~ placebo. Ultra-ultra rapid cycling ~ placebo (episode cycles within hours) Silverstone T, Romans S. Drugs 1996;51:367–82 Maj M et al. Psychopharmacology (Berl) 1989;98:535–8 Post RM et al. Neuropsychopharmacology 1998;19:206–19.")
14
Antipsicóticos atípicos en Trastorno Bipolar: Resumen
Tratamiento agudo Tratamiento de Mantención/Continuación Mania Depresión Olanzapina ++ + Risperidona - ? Quetiapina Ziprasidona Aripiprazol Asenapina Paliperidona ++ = al menos un buen RCT mostró efectos clínicamente significativos + = al menos un RCT mostró algún efecto - = RCT evidenciaof falta de efecto clínicamente significativo ? = Información incierta o estudio no controlado ni disponible

15
Clozapina en Manía Resistente
Slope b for BPRS score 30 20 *p<0.004 10 -10 Improvement -20 Clozapine Treatment as usual -30 Randomised, 1-year trial aSABD and BDI patients (n=38) bLinear regression slope of scores over time Horizontal lines represent mean slopes Suppes et al 1999
 bLinear regression slope of scores over time. Horizontal lines represent mean slopes. Suppes et al")
16
Olanzapina versus placebo en manía Aguda
Mean change from baseline in YMRS total score (LOCF) Improvement ** * Study I 3 weeks Study II 4 weeks 28.7a (n=70) 27.7a (n=69) 28.8a (n=54) 29.4a (n=56) *p=0.004; **p=0.02 aBaseline score Tohen et al 1999; 2000
 Improvement. ** * Study I 3 weeks. Study II 4 weeks. 28.7a (n=70) 27.7a (n=69) 28.8a (n=54) 29.4a. (n=56) *p=0.004; **p=0.02 aBaseline score. Tohen et al 1999;")
17
Olanzapina como Terapia asociada en Manía
Change in YMRS total score from baseline to Week 6 Improvement * Olanzapine + MSa 22.31b MS alonea 22.67b *p=0.003; n=344 6-week, double-blind, randomised, placebo-controlled trial aEither valproate or lithium; bbaseline score MS = mood stabiliser Tohen et al 2002

18
Rápida Mejoría de la Depresión Bipolar Olanzapina vs Placebo
OLZ (n=351) -2 PBO (n=355) -4 * *p<.05 vs OLZ OLZ=9.7 mg -6 * -8 * Visitwise Improvement from Baseline in MADRS (LOCF) * * * -10 -12 -14 -16 ANIMATED to distinguish OFC -18 -20 1 2 3 4 6 8 Weeks OLZ separates statistically from PBO at every week (1, 2, 3, 4, 6, and 8) postbaseline Olanzapine-fluoxetine combination group not depicted. Tohen M et al. Presented at: 155th APA Annual Meeting; May 18-23, 2002; Philadelphia, Pa.
 -2. PBO (n=355) -4. * *p<.05 vs OLZ OLZ=9.7 mg. -6. * -8. * Visitwise Improvement from Baseline in MADRS (LOCF) * * * ANIMATED to distinguish OFC Weeks. OLZ separates statistically from PBO at every week (1, 2, 3, 4, 6, and 8) postbaseline. Olanzapine-fluoxetine combination group not depicted. Tohen M et al. Presented at: 155th APA Annual Meeting; May 18-23, 2002; Philadelphia, Pa.")
19
Combinación Olanzapina-fluoxetina (OFC) superior a olanzapina sola mejorando síntomas depresivos en depresión bipolar MADRS change from baseline Placebo (n=355) Olanzapine 5-20 mg/day (n=351) -4 * OFC 6 or 12 mg/day + 25 or 50 mg/day (n=82) * -8 * * † † -12 † † † -16 -20 1 2 3 4 5 6 7 8 Weeks *p<0.05 vs olanzapine and vs OFC; †p<0.05 vs OFC 8-week, double-blind, randomised trial Tohen et al 2002
 Olanzapine 5-20 mg/day (n=351) -4. * OFC 6 or 12 mg/day + 25 or 50 mg/day (n=82) * -8. * * † † -12. † † † Weeks. *p<0.05 vs olanzapine and vs OFC; †p<0.05 vs OFC. 8-week, double-blind, randomised trial. Tohen et al")
20
Quetiapina mejora Manía rápidamente en Monoterapia YMRS
Study 1 + 2 * ** *** *** *** Quetiapine improves mania as early as Day 4. Monotherapy{163;165;} The efficacy of quetiapine in treating mania was evaluated by measuring change from baseline in YMRS Total score. This slide shows the results of an analysis of pooled data from the monotherapy studies. Change in YMRS was measured over the 84-day study period, with the primary study endpoint being change from baseline at Day 21. A statistically significant difference between the quetiapine- and placebo-treated groups was observed as early as Day 4 (–3.5 vs –2.2, respectively; P<0.05). This difference grew more pronounced and remained statistically significant throughout the study. Day 21: QTP –13.6; PBO –7.8; P<0.001. Day 84: QTP –19.0; PBO –9.6; P<0.001. Definitions/Additional information: - Baseline YMRS: QTP 33.3; PBO 33.5 - The ITT population comprised all evaluable individuals in the safety population who had at least one pre- and postrandomization YMRS assessment - Statistical significance was calculated by analysis of covariance (ANCOVA) with the baseline score as a covariate, treatment and study as fixed effect, and center as random effect. - Values shown are least square means - In addition to being statistically significant, the difference between the treatment groups was clinically significant, as determined by CGI-BP criteria (see slides 61 and 62). ITT, intent-to-treat LOCF, last observation carried forward PBO, placebo QTP, quetiapine YMRS, Young Mania Rating Scale *** *** *** *** 4 7 14 21 28 42 56 70 84 * P<0.05 ** P<0.01 *** P<0.001 ITT, LOCF
. This difference grew more pronounced and remained statistically significant throughout the study. Day 21: QTP –13.6; PBO –7.8; P< Day 84: QTP –19.0; PBO –9.6; P< Definitions/Additional information: - Baseline YMRS: QTP 33.3; PBO The ITT population comprised all evaluable individuals in the safety population who had at least one pre- and postrandomization YMRS assessment. - Statistical significance was calculated by analysis of covariance (ANCOVA) with the baseline score as a covariate, treatment and study as fixed effect, and center as random effect. - Values shown are least square means. - In addition to being statistically significant, the difference between the treatment groups was clinically significant, as determined by CGI-BP criteria (see slides 61 and 62). ITT, intent-to-treat. LOCF, last observation carried forward. PBO, placebo. QTP, quetiapine. YMRS, Young Mania Rating Scale. *** *** *** *** * P<0.05. ** P<0.01. *** P< ITT, LOCF.")
21
Quetiapina mejora Manía significativamnete al día 21 en Monoterapia YMRS
Study 1 Study 2 * * * * Change From Baseline Quetiapine significantly improves mania at Day 21. Monotherapy{163;165;} Similarly, the two individual monotherapy studies, graphed separately in this slide, show that the groups treated with quetiapine monotherapy demonstrated significantly greater improvement in YMRS scores compared to groups treated with placebo. In both studies, this difference was statistically significant at Day 21, and the quetiapine-treated group continued to improve through the end of the 84-day study period. Haloperidol and lithium, used for assay sensitivity in these studies, were also statistically better than placebo in reducing YMRS scores at Day 21. Definitions/Additional information: - The primary efficacy variable was change in YMRS Total scores at Day 21 and the primary comparison was between QTP and PBO. - Study 1 baseline (Day 1) YMRS scores (mean values): QTP 34.0; PBO 33.1; HAL 32.3 - Study 2 baseline (Day 1) YMRS scores (mean values): QTP 32.7; PBO 34.0; Li 33.3 - Study 1 change from baseline at Day 21: QTP –12.3 (P=0.010 vs PBO); PBO –8.3; HAL –15.7 (P<0.001 vs PBO) - Study 2 change from baseline at Day 21: QTP –14.6 (P<0.001 vs PBO); PBO –6.7; Li –15.2 (P<0.001 vs PBO) - Values shown are least square means HAL, haloperidol ITT, intent-to-treat Li, lithium LOCF, last observation carried forward PBO, placebo QTP, quetiapine YMRS, Young Mania Rating Scale *P<0.01 vs PBO ITT, LOCF
 YMRS scores (mean values): QTP 34.0; PBO 33.1; HAL Study 2 baseline (Day 1) YMRS scores (mean values): QTP 32.7; PBO 34.0; Li Study 1 change from baseline at Day 21: QTP –12.3 (P=0.010 vs PBO); PBO –8.3; HAL –15.7 (P<0.001 vs PBO) - Study 2 change from baseline at Day 21: QTP –14.6 (P<0.001 vs PBO); PBO –6.7; Li –15.2 (P<0.001 vs PBO) - Values shown are least square means. HAL, haloperidol. ITT, intent-to-treat. Li, lithium. LOCF, last observation carried forward. PBO, placebo. QTP, quetiapine. YMRS, Young Mania Rating Scale. *P<0.01 vs PBO. ITT, LOCF.")
22
Trastorno Bipolar: No tratados vs Tratados Tasa de Mortalidad Estandarisadas
* 30 No tratados Tratados 25 *p<.001 **p<.05 20 % de Pacientes 15 10 [Keywords] 629, Angst, global, 03/07/2002, Monte Carlo, Monaco, bipolar, course, outcome, disorder, Kelli Carson, Lilly, Eric Hoefflin, mortality, untreated, graph, Zyprexa, olanzapine### 5 * * ** * Neoplasmas Accidentes Suicidio Cardio- vascular Cerebro- vascular Otros Zurich Cohort, N=158 deaths ( ). Angst F, et al. J Affective Disord. 2002; 68:
. Angst F, et al. J Affective Disord. 2002; 68:")
Presentaciones similares