Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Dr. Christian Campos Neumología y Medicina Interna
Derrame Pleural

2
Histología pleural Mesotelio
Tapiza la capa más externa de la pleura visceral Cuboides o columnares según la estreches 15 – 40 µm de diámetro y varían el mismo con la presión transpulmonar Grosor de 7 µm Microvellosidades : 600 por célula Unidas por desmosomas y uniones estrechas Tiñen con mesotelina y calretinina Pleura parietal tiene grosor fijo Pleura visceral varía de grosor Región craneal es delgada Región caudal es gruesa Pleura visceral contiene más colágeno Facilita unión de Vasos y linfáticos al TC pulmonar Capas de la pleura visceral Endopleura : más externa , células mesoteliales Externa elástica: TC colágeno tipo I Vascular o intersticial : vasos y linfáticos Pleura parietal : Dos láminas : una vascular y otra de TC

3
Fisiología pleural Liquido pleural se forma de vasos sistémicos en ambas pleuras y fluye al espacio Espacio pleural es similar a espacio intersticial Presión intrapleural es menor que la presión intersticial de cada una de los tejidos pleurales La diferencia de presión es el gradiente de movimiento de líquido al espacio La pleura tienen poca resistencia al movimiento de proteína o líquido PHYSIOLOGY OF THE PLEURAL SPACE NORMAL PLEURAL LIQUID AND PROTEIN TURNOVER In the last 10 to 15 years, a consensus has developed that normal pleural liquid arises from the systemic pleural vessels in both pleurae, flows across the leaky pleural membranes into the pleural space, and exits the pleural space via the parietal pleural lymphatics[29] ( Fig ). In this way, the pleural space is analogous to other interstitial spaces of the body. There are several lines of evidence for this explanation: Intrapleural pressure is lower than the interstitial pressure of either of the pleural tissues.[30] This pressure difference constitutes a gradient for liquid movement into but not out of the pleural space. The pleural membranes are leaky to liquid and protein. Whether tested in vitro[31] [32] or in situ,[33] the pleura offers little resistance to liquid or protein movement. Mesothelial cells have not been shown to generate an electrical potential difference, as would be expected if there were active transport across them.[31] [32] Although normal pleural liquid has been reported to be alkaline with a higher bicarbonate than plasma,[34] there is no evidence yet for mesothelial participation in generating a bicarbonate gradient. If indeed the mesothelial layer is leaky, it is difficult to explain how mesothelial cells could maintain such a gradient.
. In this way, the pleural space is analogous to other interstitial spaces of the body. There are several lines of evidence for this explanation: Intrapleural pressure is lower than the interstitial pressure of either of the pleural tissues.[30] This pressure difference constitutes a gradient for liquid movement into but not out of the pleural space. The pleural membranes are leaky to liquid and protein. Whether tested in vitro[31] [32] or in situ,[33] the pleura offers little resistance to liquid or protein movement. Mesothelial cells have not been shown to generate an electrical potential difference, as would be expected if. there were active transport across them.[31] [32] Although normal pleural liquid has been reported to be alkaline with a higher bicarbonate than plasma,[34] there is no evidence yet for mesothelial participation in generating a bicarbonate gradient. If indeed the mesothelial layer is leaky, it is difficult to explain how mesothelial cells could maintain such a gradient.")
4
Presiones pleurales Pared espacio Pulmonar 34 34 8 8 26 26 30 11 5 5
8 8 Capilar pulmonar Capilar parietal Presión osmótica Presión hidrostática

5
Clínica Dolor torácico Tos Disnea Inflamación de pleura parietal
Distorsión pulmonar Disnea Ineficiencia mecánica de músculos respiratorios desplazados por la pared Common symptoms of patients with effusions are pleuritic chest pain, cough, and dyspnea. It appears that the three symptoms are due to different causes. Pleuritic chest pain derives from inflammation of the parietal pleura, the site of pleural pain fibers. Occasionally, this symptom is accompanied by an audible or palpable pleural rub, reflecting the movement of abnormal pleural tissues. Cough may be due to distortion of the lung, in the same way as cough follows lung collapse from a pneumothorax. Dyspnea is most likely caused by the mechanical inefficiency of the respiratory muscles that are stretched by the outward displacement of the chest wall and the downward displacement of the diaphragm.

6
Exploración Desviación traqueal contralateral Posición antiálgica
Aumento de espacios intercostales Abombamiento torácico FVT ausente MV ausente ( DP “puro”) MV disminuido (DP con atelectasia) Matidez
 MV disminuido (DP con atelectasia) Matidez.")
7
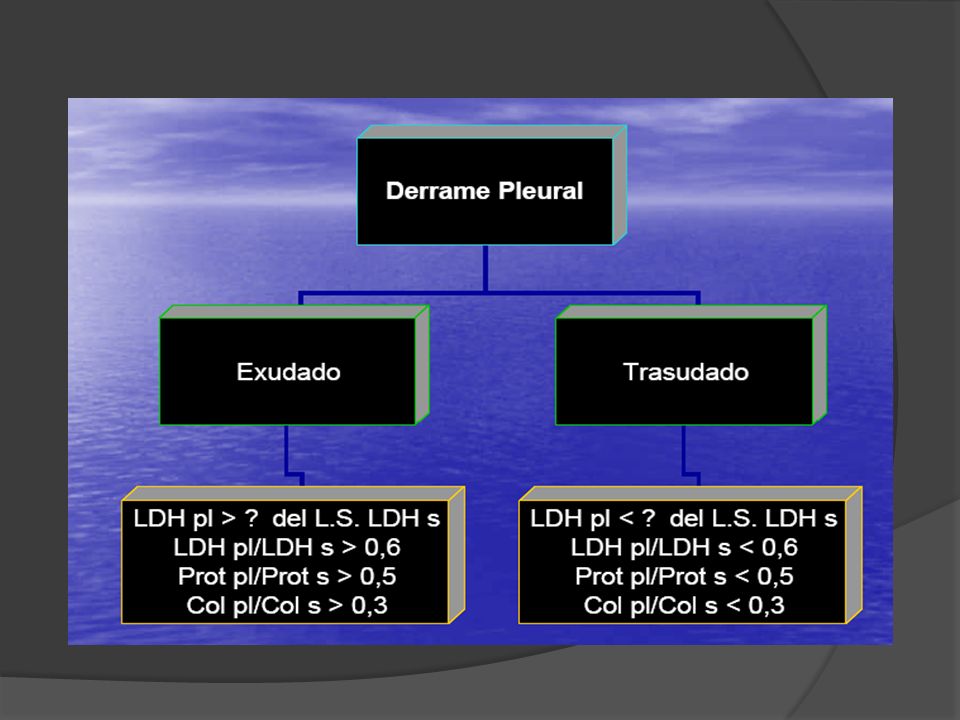
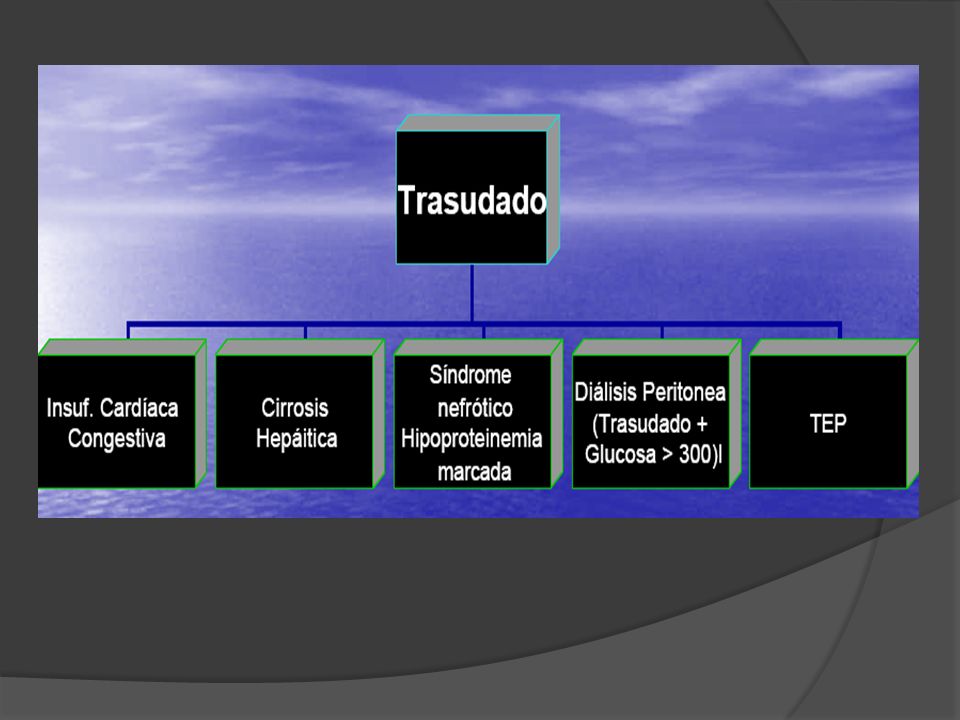
Abordaje diagnóstico Trasudado Exudado
Factores sistémicos que influyen sobre producción y absorción Exudado Factores locales que influyen sobre formación y absorción de líquido pleural. Procedimientos diagnósticos adicionales APPROACH TO PATIENTS WITH PLEURAL EFFUSION The possibility of a pleural effusion should be considered whenever a patient with an abnormal chest radiograph is evaluated. Increased densities on the chest radiograph are frequently attributed to parenchymal infiltrates when they actually represent pleural fluid. Free pleural fluid gravitates to the most dependent part of the thoracic cavity, which is the posterior costophrenic sulcus when the patient is upright. Therefore, if the posterior costophrenic angle is blunted or if the posterior part of the diaphragm is not visible on the lateral chest radiograph, bilateral decubitus chest radiographs or an ultrasonic examination of the pleural space should be obtained to ascertain whether free pleural fluid is present. If the distance between the inside of the thoracic cavity and the outside of the lung is less than 10 mm, the pleural effusion is not likely to be clinically significant and, in any case, will be difficult to sample by thoracentesis. If the distance is greater than 10 mm, an effort should be made to determine the cause of the pleural effusion.

8
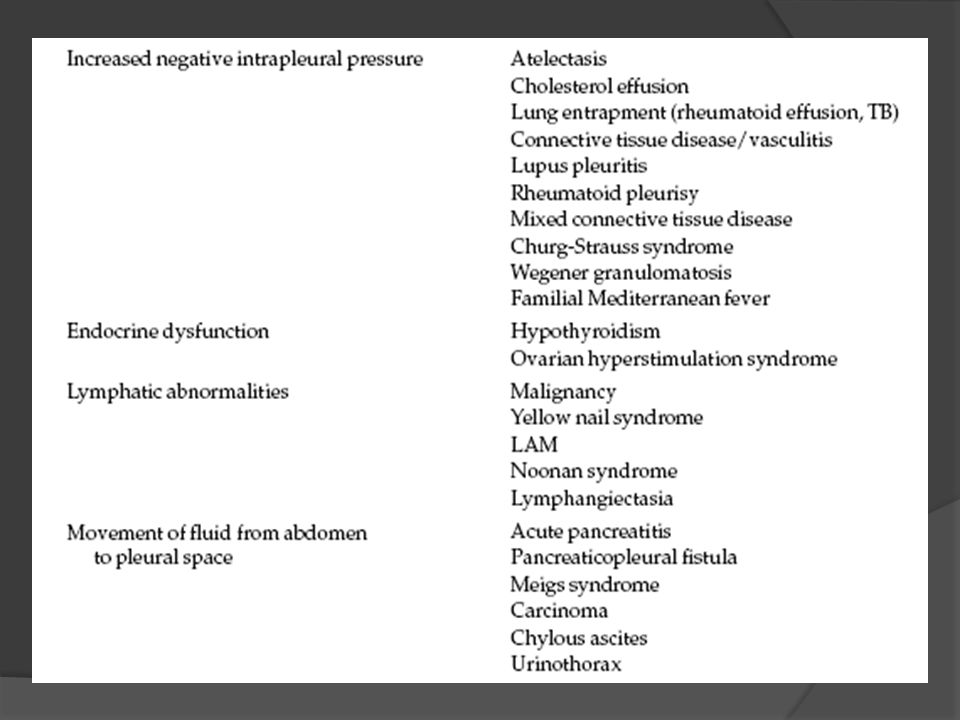
Mecanismos de producción
MECANISMO - EJEMPLO- CLASIFICACIÓN AUMENTO DE LA PRESIÓN MICROVASCULAR-----INSUFICIENCIA CARDIACA TRANSUDADO DISMINUCIÓN DE LA PRESIÓN PERIMICROVASC—ATELECTASIA --TRANSUDADO DISMINUCIÓN DE LA PRESIÓN ONCÓTICA----HIPOALBUMINEMIA--TRANSUDADO AUMENTO DE LA PERMEABILIDAD CAPILAR---NEUMONÍA--EXUDADO DISMINUCIÓN DEL DRENAJE LINFÁTICO CÁNCER ---EXUDADO COMUNICACIÓN PLEURO-PERITONEAL--HIDROTORAX HEPATICO---TRANSUDADO RUPTURA DEL DUCTO TORACICO---QUILOTORAX EXUDADO

9
Causas por frecuencia

10
Derrame Pleural , Criterios

13
Apariencia Pútrido empiema Viscoso mesotelioma Amarillo Paja Trasudado
Sanguinolento Maligno, TEP , Trauma Blanco Quilotórax o Colesterol Pútrido empiema Viscoso mesotelioma

14
CANCER

15
Apariencia Amarillo verdoso AR Negro Aspergillus niger Café Derrame crónico Ruptura absceso amebiano

16
Apariencia y valores

17
RX

23
Análisis

24
Amilasa pleural Pancreatitis Aguda : 4-20% Pancreatitis Crónica
Perforación esofágica Amilasa pleural / amilasa sérica > 1.0

25
Eosinofilia pleural (>10%)
Neumotórax Causa + común Hemotórax 1-2 semanas posterior Drogas Dantrolene, Bromocriptina, Nitrofurantoina TEP Hongos Histoplasma, Coccidioides CSS En 30% de casos de CSS DANTEC

26
Eosinofilia pleural Idiopáticos 40% derrames El predominio eosinofílico reduce la probabilidad de TB 10x y de malignidad 2x Predominio Eosinófilos (DANTEc)
")
27
Polimorfonucleares Neumonía Aguda TEP

28
Predominio Linfocitos
TB Causa + común, 90-95% linfos Tumor 50% Reumatismo Crónico Asociado a atrape pulmonar REQLUTs

29
Citología Citología Células mesoteliales inespecíficas, pero si
> 2% a 3% excluye diagnóstico de TB Puede no diagnosticar malignidad

30
Glucosa Menos de 60mg/dl: < 30 mg/dl AR
paraneumónico (<40 mg/dl > SDT) Tumor , TB, Hemotórax, < 30 mg/dl AR < 60 mg/dl y pH < 7,30 altamente sugestivo de malignidad
 Tumor , TB, Hemotórax, < 30 mg/dl AR. < 60 mg/dl y pH < 7,30 altamente sugestivo de malignidad.")
31
Glucosa LENTA : LES. Empiema, NEO, TB, AR

32
pH < 7,0 < 7.20 empiema paraneumónico complicado/ empiema
Acidosis, AR , TB , Tumor , hemotórax, ruptura esofágica, paragonimiasis

33
Serologías ANA Factor Reumatoide
> 1:160 o > nivel sérico sugiere LES Factor Reumatoide >1:320 or > nivel sérico sugiere derrame por A.R.

34
ADA ADA < 32 IU/L hace improbable TB
60 IU/L mejor valor de corte para valores predictivos positivos o negativos. Falsos positivos con Linfoma AR, LES y adenocarcinoma

35
Imágenes en Derrames

36
Rx Obliteración Ángulo Costofrénico (75cc)
Opacidad Ángulo Costofrénico (175cc) Eliminación del Ángulo Costofrénico 500cc Derrame a nivel de la cuarta costilla significa aproximadamente 1000 cc.
 Eliminación del Ángulo Costofrénico 500cc. Derrame a nivel de la cuarta costilla significa aproximadamente 1000 cc.")
37
DP LOCULADO

38
Rx Derrame Pleural con Cardiomegalia ICC : unilateral izquierdo 10-15%
Miocarditis/ Pericarditis Miocardiopatía Autoinmune : FR, LES, AR Tumor , metástasis mesotelioma Síndrome pospericardiotomía

39
ICC

40
Rx Derrame Pleural con múltiples masas Metástasis Mesotelioma MM
Asociado a destrucción costal

41
Rx Derrame Pleural con atelectasias Ca broncogénico , Linfoma Posqx
Tumor Ca broncogénico , Linfoma TB Neumonía con derrame o empiema

42
DP Y ATELECTASIA

43
DP Y ATELECTASIA

44
Rx Derrame Pleural con engrosamiento hiliar
Tumor Ca broncogénico, Linfoma , Metas TB Hongos histoplasma TEP

45
Rx Derrame Pleural crónico Mesotelioma y adenocarcinoma
TB Tumor Mesotelioma y adenocarcinoma Metastásico de ovario Tratamientos

46
Rx Derrame Pleural con enfermedades abdominales Absceso subfrénico
Absceso hepático amibiano PA

47
Derrame sub-pulmonar Elevan la base del pulmón
Simula parálisis del hemidiafragma. La base de la curvatura del pulmón está desviada lateralmente. En el lado izdo separación marcada del pulmón con la burbuja estómago sugiere Derrame sub-pulmonar.

48
Derrame sub-pulmonar

49
Derrames Loculados Los ángulos entre la masa pleural y el pulmón son obtusos. La superficie de la masa pleural generalmente es suave. Contenido de la masa es homogéneo. Más común en: Piotórax Pleuritis tuberculosa.

50
US Mucho más sensible que el Rx para detectar derrames pleurales
Detecta complicaciones Septos Lóculos Permite guiar toracentesis Cantidad de líquido

51
US derrame pleural

52
US Lóculos

53
Tomografía Detecta derrames pequeños < 10mm.
Medición del grosor de la pleura. Distinción de empiema del absceso pulmonar. Valoración del pulmón adyacente. Determinar localización masa pulmonar y su composición. Determinación de fístulas broncopleurales

54
DP LOCULADO

55
DP LOCULADO

56
TAC

Presentaciones similares