Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Antonio Rivero Román Hospital Univ Reina Sofía Córdoba
Eficacia de los nuevos fármacos o estrategias del TAR: 1.- Inhibidores de la transcriptasa inversa Antonio Rivero Román Hospital Univ Reina Sofía Córdoba

2
Desarrollo ITIAN 1987 91 92 94 95 96 97 98 99 2000 88 90 Ziagen
Combivir Videx Zerit Hivid Epivir Trizivir 01 Viread 02 03 Emtriva 89 93 04 Truvada Kivexa Retrovir 05

3
Esquema ¿ Novedades sobre el uso de 3 ITIAN como terapia de inicio?
¿ Novedades respecto a la pareja de ITIANS para iniciar el TAR ?

4
¿ 3 ITIAN como tratamiento inicial de la infección VIH ?
VENTAJAS TEORICAS Pocos comprimidos. Mínimas interacciones Menos toxicidad metabólica Reserva a los ITINN e IP como opciones futuras

5
ESTRATEGIAS EXPLORADAS
1.- AZT + 3TC + ABC 2.- ABV + 3TC + D4T 3.- ddI + d4T + 3TC 4.- ddI + d4T + ABV 5.- TDF + 3TC + ABV 6.- TDF + 3TC + DDI 7.- AZT + 3TC + DDI 8.- D4T + FTC + ABV 9.- AZT + 3TC + TDF

6
ESTRATEGIAS EXPLORADAS
La combinación AZT + 3TC + ABV es la mas evaluada como terapia inicial La combinación AZT + 3TC + ABC ha demostrado en EC - Mayor eficacia que AZT+3TC+IDV (abierto) - Eficacia similar que AZT+3TC+NFV y AZT+3TC+IDV (DC) - Menor eficacia que AZT+3TC+EFV (+/-) ABV N* % (ITT) < % < % *Estudios CNA 3007 CNA 3014 ACTG5095
 - Eficacia similar que AZT+3TC+NFV y AZT+3TC+IDV (DC) - Menor eficacia que AZT+3TC+EFV (+/-) ABV. N* % (ITT) < % < % *Estudios. CNA CNA ACTG5095.")
7
ACTG-5095

8
¿3 ITIAN como terapia de inicio?
CLAVE N <400 <50 AZT+3TC+DDI MILO % 47% (<20) HIV-NAT % 3TC+TNF+DDI Jemsek 24 SUSPENDIDO POR FVP 3TC+TNF+ABV ESS SUSPENDIDO POR FVP TONUS 38 SUSPENDIDO POR FVP Farting 19 SUSPENDIDO POR FVP TNF + 3TC + ddI Gerstoff % (<20) DDI+D4T+3TC ATLANTIC 40% ABV+3TC+D4T CLASS % ABV+FTC+D4T MKC %
 HIV-NAT % 3TC+TNF+DDI Jemsek 24 SUSPENDIDO POR FVP. 3TC+TNF+ABV ESS SUSPENDIDO POR FVP. TONUS 38 SUSPENDIDO POR FVP. Farting 19 SUSPENDIDO POR FVP. TNF + 3TC + ddI Gerstoff 60 43% (<20) DDI+D4T+3TC ATLANTIC 40% ABV+3TC+D4T CLASS 98 62% ABV+FTC+D4T MKC %")
9
DART: ZDV/3TC + TNF paises con recursos limitados
< 50 at Wk 24 < 400 at Wk 24 ZDV/3TC + TDF N = 300 Estudio Basal CV: 289,500 CD4+: 100 Potenciales ventajas No RHS Embarazo No Interacciones 100 80% 80 71% 61% 60 53% % of Subjects 40 20 ITT M=F OT n = 300 244 Mean log drop: 3.67 3.95 1. Mutuluuza CK, et al. Abstract Ssali F, et al. Abstract 24. CROI 2005

10
¿3 ITIAN como terapia de inicio? Conclusiones
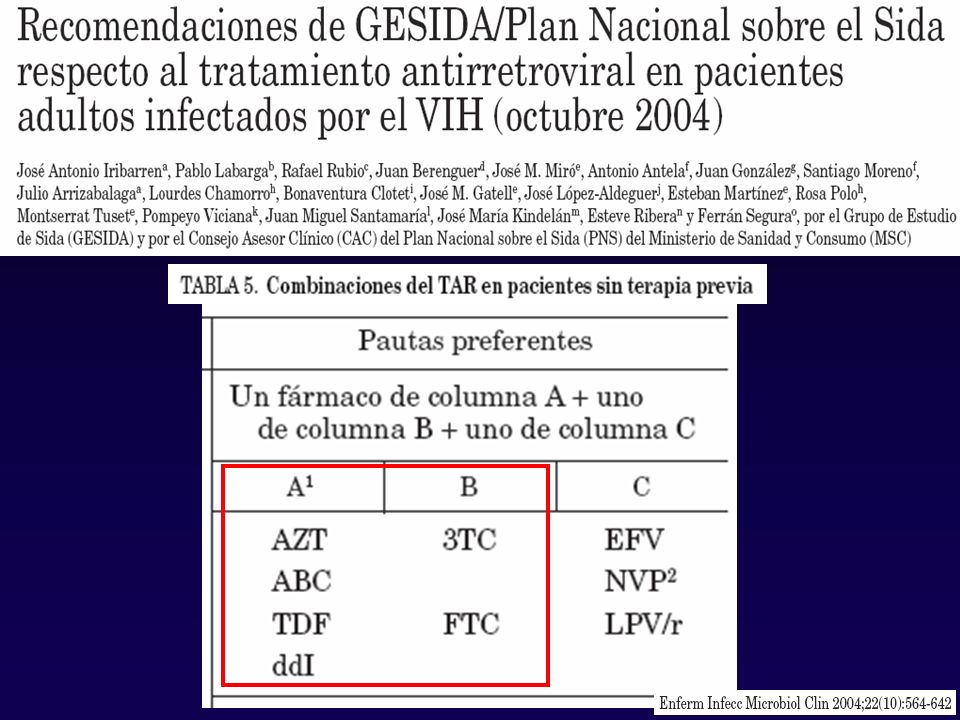
La asociación de 3 ITIAN no es una pauta recomendada como primera línea en el tratamiento inicial de la infección VIH. La combinación AZT + 3TC + ABC puede ser una opción alternativa razonable en pacientes en los que, por cualquier motivo, no resulta aconsejable el empleo de pautas basadas en IP o NN. Existe escasa experiencia con otras combinaciones de 3 ITIAN.

11
Esquema ¿ Algo nuevo sobre el uso de 3 ITIAN como terapia de inicio?
¿ Con que pareja de ITIANS debemos iniciar el TAR ?: Novedades

12
Desarrollo ITIAN 1987 91 92 94 95 96 97 98 99 2000 88 90 Ziagen
Combivir Videx Zerit Hivid Epivir Trizivir 01 Viread 02 03 Emtriva 89 93 04 Truvada Kivexa Retrovir 05

14
ELECTIVO AZT TNF + 3TC ó FTC ALTERNATIVA ABC DDI + 3TC ó FTC D4T

16
DATOS PROCEDENTES DE ESTUDIOS RANDOMIZADOS
Clásicas AZT + 3TC D4T + 3TC Nuevas TNF + 3TC/FTC ABC + 3TC Emergentes DDI + 3TC/FTC

17
AZT + 3TC Primera coformulación: “gold estándar”
Escasas interacciones farmacológicas Amplia experiencia en múltiples estudios DMP-006 (EFV vs IDV) CNA (EFV+AZT+3TC vs EFV+3TC+ABC) DMP-034 (ATV vs EFV) Combine (NVP vs NFV) ACTG 384 (AZT/3TC vs DDI/D4T & EFV vs NFV
 CNA (EFV+AZT+3TC vs EFV+3TC+ABC) DMP-034 (ATV vs EFV) Combine (NVP vs NFV) ACTG 384 (AZT/3TC vs DDI/D4T & EFV vs NFV.")
18
DMP-006: Porcentaje de pacientes con VIH ARN <50 Copias/mL ITT:NC=F
Estudio DMP-006 DMP-006: Porcentaje de pacientes con VIH ARN <50 Copias/mL ITT:NC=F

19
AZT + 3TC : Inconvenientes
Pauta BID 3TC bien tolerado AZT Mielosupresión Toxicidad Mitocondrial Miopatia Intolerancia

20
3TC/d4T VENTAJAS No restricciones dietéticas
Larga duración de respuesta ABT- 720 Gran experiencia en EC randomizados ABT - 863 GS - 903 INCONVENIENTES Toxicidad mitocondrial Trastornos metabólicos: Lipoatrofia, hiperlipemia Neuropatía periférica

21
M98-863: Porcentaje de pacientes con carga viral ARN VIH <400 copias/ml

22
3TC/FTC + DDI VENTAJAS INCONVENIENTES Administración QD
Escasa experiencia en EC randomizados Estudio FTC-301 (n=286) Maggiolo et al (n=34) Berenguer et al (GESIDA) en fase de reclutamiento Datos procedentes de estudios observacionales
 Maggiolo et al (n=34) Berenguer et al (GESIDA) en fase de reclutamiento. Datos procedentes de estudios observacionales.")
23
3TC/FTC + DDI

24
N=65 T4 (media)=311 RNA-VIH>5 log=43%
=311 RNA-VIH>5 log=43%")
25
Eficacia de la asociación de Videx (ddI), Epivir (3TC) y Sustiva (efavirenz) una vez al Día en pacientes con infección por VIH naïve. Estudio VESD J. Santos, R. Palacios, J. de la Torre, M.C. Gálvez, F. Lozano, M.J. Ríos, A. Rivero, L.F. Pérez-Cortés, M. López y GAEI. Estudio prospectivo, abierto, no controlado, observacional y multicéntrico en pacientes sin tratamiento antirretroviral previo que inician un régimen terapéutico con didanosina + lamivudina + efavirenz.

26
ESTUDIO VESD Nº Casos 163 Casos de sida 63 (37,7%)
Neumonía P. jirovenci 15 casos Tuberculosis 13 casos Candidiasis esofágica 13 casos Encefalitis toxoplasma 5 casos Sarcoma de Kaposi casos Non Hodgking limphoma 2 casos LMP casos Otros casos Linfocitos CD4 (cells/ml) (45-228) % pacientes con <200 CD4/ml 69,5 % pacientes con <50 CD4/ml 26,3 % pacientes con >5 log10 de RNA-VIH/ml 63,1
 142 (45-228) % pacientes con <200 CD4/ml 69,5. % pacientes con <50 CD4/ml 26,3. % pacientes con >5 log10 de RNA-VIH/ml 63,1.")
27
ESTUDIO VESD: < 50 cop/ml
88,2 % 62,9%

28
ESTUDIO VESD 200 +1991,2 150 CD4 80 - 1 - 3 Log -4,041,2 - 5

29
ABC/3TC coformulados VENTAJAS
Administración QD sin restricción dietética. No interacciones. Ensayos clinicos con ABC y/o 3TC bid CNA (EFV + ABC + 3TC) Class (ABC + 3TC + FOSv vs EFV) ABCDE (ABC vs d4T + 3TC + EFV) NEAT (ABC + 3TC + FPV vs NFV) SOLO (ABC + 3TC + FPV vs NFV) Ensayos clínicos con ABC/3TC en QD coformulados ó no ZODIAC (ABC + 3TC (QD vs BID) + EFV CNA (ABC/3TC + EFV vs TDF) INCONVENIENTES Reacciones de hipersensibilidad a Abacavir
 Class (ABC + 3TC + FOSv vs EFV) ABCDE (ABC vs d4T + 3TC + EFV) NEAT (ABC + 3TC + FPV vs NFV) SOLO (ABC + 3TC + FPV vs NFV) Ensayos clínicos con ABC/3TC en QD coformulados ó no. ZODIAC (ABC + 3TC (QD vs BID) + EFV. CNA (ABC/3TC + EFV vs TDF) INCONVENIENTES. Reacciones de hipersensibilidad a Abacavir.")
30
ABC + 3TC (ITT nc=f). Pacientes Naive
ABCbid+3TCbid+EFV Aleatorizado / Naive / n=97 / CD4 basal >50 CLASS ABCbid+3TCbid+APVrqd Aleatorizado / Naive / n=96 / CD4 basal >50 CLASS ABCbid+3TCbid+EFV Aleatorizado / Naive / n=324 / CD4 basal >50 CNA30024 ABCbid+3TCqd+EFV Aleatorizado / Naive / n=384 / CD4 basal >50 ZODIAC ABCqd+3TCqd+EFV Aleatorizado / Naive / n=386 / CD4 basal >50 ZODIAC ABCbid+3TCbid+FPVbid Aleatorizado / Naive / n=166 NEAT ABCbid+3TCbid+NFVbid Aleatorizado / Naive / n=83 NEAT ABCbid+3TCbid+FPVrqd Aleatorizado / Naive / n=322 SOLO ABCbid+3TCbid+NFVbid Aleatorizado / Naive / n=322 SOLO ABCbid+3TCqd+EFV Aleatorizado / Naive / n=97 ABCDE ABC/3TCqd+EFV Aleatorizado / Naive / n=169 ESS30009 % pacientes CV <50 c/ml a 48 semanas 1. Barlett. IAC Barcelona, 2002, TuOrB1189 2. De Jesus. Clin Infect Dis 2004; 39: 3. Gazzard. ICAAC Chicago, 2004, H-1722b 4. Rodri-French. JAIDS 2004; 35:22-32 5. Schurmann D. HIV Glasgow, 2002, PL 14.4 6. Podzamczer D. CROI San Francisco, 2004, 716 7. Gallant J. IAS Rio de Janeiro, 2005

31
ABC/3TC. Eficacia Estudio Zodiac
20 40 60 80 100 BL 2 4 8 12 16 24 28 32 36 44 48 Semanas CV < 50 cp/mL (%) ABC QD + 3TC + EFV ABC BID + 3TC + EFV
 ABC QD + 3TC + EFV. ABC BID + 3TC + EFV.")
32
Estudio SOLO: Pacientes <50 c/mL (ITT)
Antiretroviral naive / No CD4 entry criteria / random 1:1 ITT M=F ITT Stratified Difference (95% CI): 3% (-5%, 11%) FAPV 1400mg + RTV 200mg QD + ABC 300mg + 3TC 150mg BID N=322 treated 55% 53% NFV 1250mg BID + ABC 300mg + 3TC 150mg BID N=327 treated Gathe J et al. AIDS 2004; 18:
: 3% (-5%, 11%) FAPV 1400mg + RTV 200mg QD + ABC 300mg + 3TC 150mg BID. N=322 treated. 55% 53% NFV 1250mg BID + ABC 300mg + 3TC 150mg BID. N=327 treated Gathe J et al. AIDS 2004; 18:")
33
TDF + FTC VENTAJAS: Coformulación Administración QD
Experiencia en ensayos clínicos con TDF+3TC. Extrapolación a FTC INCONVENIENTES Poca experiencia en el largo plazo Toxicidad renal Osteopenia

34
Estudio GS 903 82% 81% TDF+3TC+EFV d4T+3TC+EFV Semanas 2 4 8 12 16 20
2 4 8 12 16 20 24 28 32 36 40 44 48 60 80 100 TDF+3TC+EFV d4T+3TC+EFV 82% 81% Gallant JE. JAMA 2004;292:

35
ESTUDIO M TDF + FTC. 20 40 60 80 100 8 16 24 32 48 Semana Proportion <50 copies/mL LPV/r QD + TDF/FTC (n=115) LPV/r BID + TDF/FTC (n=75) 70% 64% Gathe J. 11th CROI; Abstract 570
 LPV/r BID + TDF/FTC (n=75) 70% 64% Gathe J. 11th CROI; Abstract 570.")
36
ESTUDIOS COMPARATIVOS
FTC 301: FTC+ddI vs ddI+d4T * GS-903: 3TC+TDF vs d4T+3TC * GS-934: FTC+TDF vs AZT+3TC * CNA 30024: 3TC+ABC vs AZT+3TC * ABCDE: 3TC + ABC vs d4T + 3TC* * Mas EFV

37
3TC/ABC vs AZT/3TC. Estudio CNA 30024: Diseño
ABC/3TC/EFV vs AZT/3TC/EFV Doble ciego de no inferioridad No se utilizaron Combos Cambios en EFV y 3TC permitidos 649 pacientes naive Objetivo principal Pacientes con CV < 50 copias/mL semana 48 De Jesus CID 2004;39:

38
CNA30024: % pacientes <50 Cop/mL
ABC: 70% ZDV: 69% De Jesus. Clin Infect Dis 2004; 39:

39
3TC/ABC vs AZT/3TC. Estudio CNA 30024: Eficacia
ABC/3TC AZT/3TC ITT* 74% 71% OT* 96% 98% * CV < 50 copias/mL a 48 semanas De Jesus CID 2004;39:

40
CNA30024: Cambio medio de CD4 209 155 (p=0.005, based on AAUCMB)
ITT - Exposed, Observed = ITT- Exposed, No imputation for missing values (p=0.005, based on AAUCMB) 209 155 De Jesus. Clin Infect Dis 2004; 39:
 De Jesus. Clin Infect Dis 2004; 39:")
41
3TC/ABC vs AZT/3TC. Estudio CNA 30024 Seguridad
ABC/3TC (n = 324) AZT/3TC (n = 325) Cualquier EA 226 (70%) 250 (77%) EA que llevan a suspensión 16 (5%) 25 (8%) EA mas frecuentes Nausea 6,8% 11,4% Vómitos 2% 10% Anemia 3,2% 5,5% Neutropenia 5,2% 11,7% Sospecha HS ABC 9% 3% Hipersensibilidad ABC 6% De Jesus CID 2004;39:
 AZT/3TC. (n = 325) Cualquier EA. 226 (70%) 250 (77%) EA que llevan a suspensión. 16 (5%) 25 (8%) EA mas frecuentes. Nausea. 6,8% 11,4% Vómitos. 2% 10% Anemia. 3,2% 5,5% Neutropenia. 5,2% 11,7% Sospecha HS ABC. 9% 3% Hipersensibilidad ABC. 6% De Jesus CID 2004;39:")
42
Estudio ABCDE: Pacientes <50 c/mL (ITT)
d4T + 3TCqd + EFV (n=122) ABCbid + 3TCqd + EFV (n=115) Podzamczer D. CROI San Francisco, 2004, 716
 ABCbid + 3TCqd + EFV (n=115) Podzamczer D. CROI San Francisco, 2004, 716.")
43
FTC+DDI vs DDI+D4T: Estudio 301
Semana 48 FTC QD ddI QD EFV QD Estudio 301 d4T placebo DISEÑO Naive (n=571) Randomizado 1:1 Doble ciego d4T BID Semana 48 ddI QD EFV QD FTC placebo Cahn P. 10th CROI; 2003; Boston, Mass. Poster 606.
 Randomizado 1:1. Doble ciego. d4T. BID. Semana 48. ddI. QD. EFV. QD. FTC placebo. Cahn P. 10th CROI; 2003; Boston, Mass. Poster 606.")
44
FTC/ddI vs ddI/d4T: Estudio FTC-301 % Pacientes <50 Copias/mL
Intent to Treat (Missing=Failure) 100 80 74% 58% 60 % patients with HIV-1 RNA <50 copies/mL FTC+ddI+EFV 40 d4T+ddI+EFV Naive (n=571) Randomizado 1:1 Doble ciego p=0.0001 20 BL 4 8 12 16 20 24 28 32 36 40 44 48 Weeks Cahn P. 10th CROI; 2003; Boston, Mass. Poster 606.
 % 58% 60. % patients with HIV-1 RNA <50 copies/mL. FTC+ddI+EFV. 40. d4T+ddI+EFV. Naive (n=571) Randomizado 1:1. Doble ciego. p= BL Weeks. Cahn P. 10th CROI; 2003; Boston, Mass. Poster 606.")
45
Estudio 903: Diseño ART-naïve patients (N = 600) randomized 1:1
144 weeks ART-naïve patients (N = 600) randomized 1:1 Stratification by: Plasma HIV RNA >/100,000 copies/mL CD4 count /<200 cells/mm³ 144 weeks TDF = tenofovir disoproxil fumarate 3TC = lamivudine Gallant JE et al. JAMA 2004;292:
 randomized 1:1. Stratification by: Plasma HIV RNA >/100,000 copies/mL. CD4 count /<200 cells/mm³. 144 weeks. TDF = tenofovir disoproxil fumarate. 3TC = lamivudine. Gallant JE et al. JAMA 2004;292:")
46
D4T/3TC vs TDF/3TC: Estudio GS 903
Semanas 2 4 8 12 16 20 24 28 32 36 40 44 48 60 80 100 TDF+3TC+EFV d4T+3TC+EFV 82% 81% Gallant JE. JAMA 2004;292:

47
TDF/FTC vs AZT/3TC. Estudio GS 934 Descripción
TDF/FTC/EFV vs CBV/EFV Abierto de no inferioridad Solo se utilizó CBV como Combo Cambios en EFV permitidos 499 pacientes naive Objetivo principal Pacientes con CV < 500 copias/mL semana 48 Arribas JR et al. 18th Int. Conf. on Antiv. Res. Barcelona Abstract LB-01..

48
TDF/FTC vs AZT/3TC. Estudio GS 934 Eficacia
10 20 30 40 50 60 70 80 90 BL 8 16 24 32 48 Semanas % Respondedores TDF/FTC 77% AZT/3TC 68% p = 0.034 CV < 50 copias /mL

49
Patients with HIV-1 RNA < 50 copies/mL [TLOVR] (%)
TDF/FTC vs AZT/3TC. Estudio GS 934 Eventos Adversos Diferencias en eficacia fundamentalmente debidas a diferncias en retiradas por EA Patients with HIV-1 RNA < 50 copies/mL [TLOVR] (%) 77% 68% FTC + TDF + EFV ZDV/3TC + EFV (ITT n = 509) 20 40 60 80 BL 8 16 24 32 48 100 Weeks AEs leading to D/C FTC + TDF + EFV (n = 257) ZDV/3TC + EFV (n = 254) Any AE 10 (4%) 23 (9%)* Anemia or ↓ hemoglobin 14 (6%) Nausea 1 (1%) 4 (2%) Fatigue 3 (1%) Vomiting 2 (1%) Dermatitis (NNRTI) Neutropenia Anton Pozniak presented 48-week data for the GS934 study, one of the most important clinical trials looking at antiretroviral therapy in naive patients. In this large trial, 511 treatment-naive patients were randomized to receive efavirenz plus either coformulated zidovudine/lamivudine or tenofovir and emtricitabine. At 48 weeks, rates of virologic suppression were greater in the tenofovir plus emtricitabine arm compared with the zidovudine/lamivudine arm, with similar results for cut-off values < 400 copies/mL and < 50 copies/mL. When patients with baseline NNRTI resistance were excluded from the intent-to-treat analysis, 80% of tenofovir plus emtricitabine patients and 70% of zidovudine/lamivudine patients achieved virologic suppression to < 400 copies/mL. The differences in efficacy were primarily driven by a greater discontinuation rate among zidovudine/lamivudine patients due to adverse events (shown in the table), since discontinuation equaled failure in the final data analysis. Overall, 9% of zidovudine/lamivudine patients discontinued treatment due to adverse events, primarily anemia, but also some nausea, vomiting, fatigue, and neutroopenia. In comparison, only 4% of tenofovir plus emtricitabine patients discontinued due to adverse events. Excluding pts with baseline NNRTI resistance FTC + TDF 80% vs ZDV/3TC 70% (P = .021) Pozniak AL, et al. IAS Abstract WeOa0202. * P = .016
![Patients with HIV-1 RNA < 50 copies/mL [TLOVR] (%)](http://slideplayer.es/slide/314346/2/images/49/Patients+with+HIV-1+RNA+%3C+50+copies%2FmL+%5BTLOVR%5D+%28%25%29.jpg "TDF/FTC vs AZT/3TC. Estudio GS 934 Eventos Adversos. Diferencias en eficacia fundamentalmente debidas a diferncias en retiradas por EA. Patients with HIV-1 RNA < 50 copies/mL [TLOVR] (%) 77% 68% FTC + TDF + EFV ZDV/3TC + EFV. (ITT n = 509) BL Weeks. AEs leading to D/C. FTC + TDF + EFV. (n = 257) ZDV/3TC + EFV. (n = 254) Any AE. 10 (4%) 23 (9%)* Anemia or ↓ hemoglobin. 14 (6%) Nausea. 1 (1%) 4 (2%) Fatigue. 3 (1%) Vomiting. 2 (1%) Dermatitis (NNRTI) Neutropenia. Anton Pozniak presented 48-week data for the GS934 study, one of the most important clinical trials looking at antiretroviral therapy in naive patients. In this large trial, 511 treatment-naive patients were randomized to receive efavirenz plus either coformulated zidovudine/lamivudine or tenofovir and emtricitabine. At 48 weeks, rates of virologic suppression were greater in the tenofovir plus emtricitabine arm compared with the zidovudine/lamivudine arm, with similar results for cut-off values < 400 copies/mL and < 50 copies/mL. When patients with baseline NNRTI resistance were excluded from the intent-to-treat analysis, 80% of tenofovir plus emtricitabine patients and 70% of zidovudine/lamivudine patients achieved virologic suppression to < 400 copies/mL. The differences in efficacy were primarily driven by a greater discontinuation rate among zidovudine/lamivudine patients due to adverse events (shown in the table), since discontinuation equaled failure in the final data analysis. Overall, 9% of zidovudine/lamivudine patients discontinued treatment due to adverse events, primarily anemia, but also some nausea, vomiting, fatigue, and neutroopenia. In comparison, only 4% of tenofovir plus emtricitabine patients discontinued due to adverse events. Excluding pts with baseline NNRTI resistance. FTC + TDF 80% vs ZDV/3TC 70% (P = .021) Pozniak AL, et al. IAS Abstract WeOa0202. * P =")
50
TDF/FTC vs AZT/3TC. Estudio GS 934 Incremento CD4+
75 125 175 225 BL 8 16 24 32 40 48 Semanas Δ medio de CD4+ FTC/TDF +190 células/μL CBV células/μL

51
Conclusiones de estudios comparativos
FTC/ddI superior a d4T/ddI (FTC-301) TDF/3TC no inferior a d4T/3TC pero mejor tolerado (GS-903) TDF/FTC superior a AZT/3TC (GS-934) ABC/3TC no inferior a AZT/3TC (CNA-30024).
 TDF/3TC no inferior a d4T/3TC pero mejor tolerado (GS-903) TDF/FTC superior a AZT/3TC (GS-934) ABC/3TC no inferior a AZT/3TC (CNA-30024).")
52
¿DEBEMOS TENER EN CUENTA EL PRECIO A LA HORA DE ELEGIR EL REGIMEN INICIAL?
REGIMEN COSTE ANUAL AZT + 3TC co-formulado euros 3TC + ABC coformulado euros FTC + TDF euros 3TC + DDI (400) euros 3TC + DDI (250) euros
 3744 euros. 3TC + DDI (250) 3027 euros.")
53
¿Podemos prescindir de NRTI en el tratamiento de pacientes naives?
Estudio DMP-006 100 80 60 40 20 144 132 120 108 96 84 72 48 36 24 16 12 8 4 * EFV + AZT + 3TC EFV + IDV IDV + AZT + 3TC 55% 34% Patients With HIV RNA <400 (%)
")
54
TAR SIN ITIAN VENTAJAS TEORICAS: Evitar toxicidad mitocondrial
¿Efecto protector de ITIANs sobre reservorios del VIH?

55
EFV + 2 NRTIs Superior to LPV/r + EFV NRTI-Sparing Regimen
ACTG A5116: rollover from ACTG 388 ACTG 388: IDV vs IDV + EFV vs IDV + NFV, each with ZDV/3TC ACTG A5116: EFV + 2 NRTIs vs LPV/r (533/133) + EFV w/o NRTIs EFV + 2 NRTIs superior to LPV/r + EFV at median 2.1 yrs FU[1] Shorter time to treatment D/C (P < .001) and shorter time to virologic failure or toxicity-related D/C (P = .0015) Virologic failure: 6% vs 12% D/C for toxicity: 5% vs 17% LPV/r associated with ↑ lipids; EFV with ↑ glucose and insulin Significant loss of limb fat in NRTI-containing arm—mostly ZDV/3TC—vs gain in in NRTI-sparing arm[2] PI + NNRTI regimen better for lipoatrophy, but worse overall for toxicity Standard Efavirenz Regimen Appears Superior to Efavirenz plus Lopinavir/Ritonavir NRTI-Sparing Regimen By Mark Mascolini February 25, 2005 Among patients already responding well to antiretrovirals, efavirenz plus 2 nucleoside reverse transcriptase inhibitors (NRTIs) proved safer and possibly more potent than efavirenz plus lopinavir/ritonavir.[1] The results of this study were presented at the 12th Conference on Retroviruses and Opportunistic Infections in Boston, Massachusetts. In a previous study of patients with advanced HIV disease, indinavir plus efavirenz was superior to indinavir alone, which was in turn superior to indinavir plus nelfinavir, all combined with 2 NRTIs. Patients in this study who responded to therapy were enrolled in the current study, in which the University of Miami's Margaret Fischl, MD, and AIDS Clinical Trials Group (ACTG) colleagues evaluated the benefit of switching to either a protease inhibitor-sparing regimen or a NRTI-sparing regimen. In the current study, 236 patients received either efavirenz plus lopinavir/ritonavir (at the increased dose of 155/133 mg twice daily) without NRTIs or efavirenz plus an NRTI backbone of zidovudine/didanosine, zidovudine/lamivudine, didanosine/stavudine, or stavudine/lamivudine. At study entry, no patient demonstrated a confirmed virologic rebound or virus resistant to protease inhibitors, nonnucleoside reverse transcriptase inhibitors, zidovudine, didanosine, or stavudine. The baseline median CD4+ cell count was 479 cells/mm3 in the efavirenz plus NRTIs group and 469 cells/mm3 in the efavirenz plus lopinavir/ritonavir arm. Of the patients taking efavirenz and NRTIs, 74% maintained a viral load below 50 copies/mL through a median 110 weeks of follow-up, vs 66% of patients taking lopinavir/ritonavir plus efavirenz. Treatment with lopinavir/ritonavir plus efavirenz also yielded significantly higher levels of total cholesterol, low-density lipoprotein cholesterol, and triglycerides. At the end of follow-up, the investigators noted 7 virologic failures in the efavirenz plus NRTIs arm and 14 in the NRTI-sparing arm. Toxicity-induced dropouts numbered 6 and 20, respectively. Time to virologic failure or toxicity-related discontinuation significantly favored efavirenz plus NRTIs (P = .0015). Time to virologic failure alone also favored this arm, but the difference from the NRTI-sparing regimen did not reach statistical significance (P = .06). Adverse effects resulting from treatment with efavirenz plus NRTIs included progressive loss of limb fat, as detailed in another report at the conference,[2] in addition to significant increases in glucose and insulin levels. Dr. Fischl noted that these relatively small changes may be clinically meaningless. An adherence analysis remains to be completed, but Dr. Fischl noted that a preliminary look at compliance showed little difference between regimens. She agreed with a questioner who noted that the higher lopinavir/ritonavir dose may have inflated toxicity rates in that group. References 1. Fischl M, Bassett R, Collier A, et al. Randomized, controlled trial of lopinavir/ritonavir + efavirenz vs efavirenz + 2 nucleoside reverse transcriptase inhibitors following a first suppressive 3- or 4-drug regimen in advanced HIV disease. Program and abstracts of the 12th Conference on Retroviruses and Opportunistic Infections; February 22-25, 2005; Boston, Massachusetts. Abstract 121. 2. Tebas P, Zhang J, Yarasheski K, et al. Switch to a protease inhibitor-containing/nucleoside reverse transcriptase inhibitor-sparing regimen increases appendicular fat and serum lipid levels without affecting glucose metabolism or bone mineral density: the results of a prospective randomized trial, ACTG 5125s. Program and abstracts of the 12th Conference on Retroviruses and Opportunistic Infections; February 22-25, 2005; Boston, Massachusetts. Abstract 40. 1. Fischl M, et al. Abstract Tebas P, et al. Abstract 40. CROI 2005
 + EFV w/o NRTIs. EFV + 2 NRTIs superior to LPV/r + EFV at median 2.1 yrs FU[1] Shorter time to treatment D/C (P < .001) and shorter time to virologic failure or toxicity-related D/C (P = .0015) Virologic failure: 6% vs 12% D/C for toxicity: 5% vs 17% LPV/r associated with ↑ lipids; EFV with ↑ glucose and insulin. Significant loss of limb fat in NRTI-containing arm—mostly ZDV/3TC—vs gain in in NRTI-sparing arm[2] PI + NNRTI regimen better for lipoatrophy, but worse overall for toxicity. Standard Efavirenz Regimen Appears Superior to Efavirenz plus Lopinavir/Ritonavir NRTI-Sparing Regimen. By Mark Mascolini. February 25, Among patients already responding well to antiretrovirals, efavirenz plus 2 nucleoside reverse transcriptase inhibitors (NRTIs) proved safer and possibly more potent than efavirenz plus lopinavir/ritonavir.[1] The results of this study were presented at the 12th Conference on Retroviruses and Opportunistic Infections in Boston, Massachusetts. In a previous study of patients with advanced HIV disease, indinavir plus efavirenz was superior to indinavir alone, which was in turn superior to indinavir plus nelfinavir, all combined with 2 NRTIs. Patients in this study who responded to therapy were enrolled in the current study, in which the University of Miami s Margaret Fischl, MD, and AIDS Clinical Trials Group (ACTG) colleagues evaluated the benefit of switching to either a protease inhibitor-sparing regimen or a NRTI-sparing regimen. In the current study, 236 patients received either efavirenz plus lopinavir/ritonavir (at the increased dose of 155/133 mg twice daily) without NRTIs or efavirenz plus an NRTI backbone of zidovudine/didanosine, zidovudine/lamivudine, didanosine/stavudine, or stavudine/lamivudine. At study entry, no patient demonstrated a confirmed virologic rebound or virus resistant to protease inhibitors, nonnucleoside reverse transcriptase inhibitors, zidovudine, didanosine, or stavudine. The baseline median CD4+ cell count was 479 cells/mm3 in the efavirenz plus NRTIs group and 469 cells/mm3 in the efavirenz plus lopinavir/ritonavir arm. Of the patients taking efavirenz and NRTIs, 74% maintained a viral load below 50 copies/mL through a median 110 weeks of follow-up, vs 66% of patients taking lopinavir/ritonavir plus efavirenz. Treatment with lopinavir/ritonavir plus efavirenz also yielded significantly higher levels of total cholesterol, low-density lipoprotein cholesterol, and triglycerides. At the end of follow-up, the investigators noted 7 virologic failures in the efavirenz plus NRTIs arm and 14 in the NRTI-sparing arm. Toxicity-induced dropouts numbered 6 and 20, respectively. Time to virologic failure or toxicity-related discontinuation significantly favored efavirenz plus NRTIs (P = .0015). Time to virologic failure alone also favored this arm, but the difference from the NRTI-sparing regimen did not reach statistical significance (P = .06). Adverse effects resulting from treatment with efavirenz plus NRTIs included progressive loss of limb fat, as detailed in another report at the conference,[2] in addition to significant increases in glucose and insulin levels. Dr. Fischl noted that these relatively small changes may be clinically meaningless. An adherence analysis remains to be completed, but Dr. Fischl noted that a preliminary look at compliance showed little difference between regimens. She agreed with a questioner who noted that the higher lopinavir/ritonavir dose may have inflated toxicity rates in that group. References. 1. Fischl M, Bassett R, Collier A, et al. Randomized, controlled trial of lopinavir/ritonavir + efavirenz vs efavirenz + 2 nucleoside reverse transcriptase inhibitors following a first suppressive 3- or 4-drug regimen in advanced HIV disease. Program and abstracts of the 12th Conference on Retroviruses and Opportunistic Infections; February 22-25, 2005; Boston, Massachusetts. Abstract Tebas P, Zhang J, Yarasheski K, et al. Switch to a protease inhibitor-containing/nucleoside reverse transcriptase inhibitor-sparing regimen increases appendicular fat and serum lipid levels without affecting glucose metabolism or bone mineral density: the results of a prospective randomized trial, ACTG 5125s. Program and abstracts of the 12th Conference on Retroviruses and Opportunistic Infections; February 22-25, 2005; Boston, Massachusetts. Abstract Fischl M, et al. Abstract Tebas P, et al. Abstract 40. CROI")
56
% RNA-VIH < 50 a las 48 semanas
Estudios en Naïve con respuesta (<50 cp/ml) > 65% % RNA-VIH < 50 a las 48 semanas COMBINE (NVP+ZDV/3TC) 2NN (NVP BID+d4T+3TC) ZODIAC (EFV+ABC QD+3TC) M (LPV/r+d4T+3TC) ZODIAC (EFV+ABC+3TC) CNA30024 (EFV+ZDV+3TC) 2NN (NVP QD+d4T+3TC) 2NN (EFV+d4T+3TC) CNA30024 (EFV+ABC+3TC) M (LPV/r+FTC+TDF QD) FTC301 (EFV+FTC+ddI QD) DMP (EFV+D4T+3TC) CLASS (EFV+ABC+3TC) ANRS (EFV+ddI+3TC) M (LPV/r+d4T+3TC) Dart 1 (EFV+ddI-EC+3TC) GS903 (EFV+d4T+3TC) GS903 (EFV+TDF+3TC) ANRS 091 (EFV+ddI+FTC) NNRTI Boosted PI 40 50 60 70 80 90 100 Bartlett JA et al. Abstract 586. CROI 2005
 > 65% % RNA-VIH < 50 a las 48 semanas. COMBINE (NVP+ZDV/3TC) 2NN (NVP BID+d4T+3TC) ZODIAC (EFV+ABC QD+3TC) M (LPV/r+d4T+3TC) ZODIAC (EFV+ABC+3TC) CNA30024 (EFV+ZDV+3TC) 2NN (NVP QD+d4T+3TC) 2NN (EFV+d4T+3TC) CNA30024 (EFV+ABC+3TC) M (LPV/r+FTC+TDF QD) FTC301 (EFV+FTC+ddI QD) DMP (EFV+D4T+3TC) CLASS (EFV+ABC+3TC) ANRS (EFV+ddI+3TC) M (LPV/r+d4T+3TC) Dart 1 (EFV+ddI-EC+3TC) GS903 (EFV+d4T+3TC) GS903 (EFV+TDF+3TC) ANRS 091 (EFV+ddI+FTC) NNRTI. Boosted PI Bartlett JA et al. Abstract 586. CROI")
57
Resistencias inducidas por 3TC/ABC. Estudio CNA 30021 (Zodiac)
770 pacientes en el estudio 70 con fracaso virológico 31 con estudio virológico Genotipo Fenotipo real

58
Acumulación de TAMs en estudio CNA-3005
Número de pacientes en % Semanas de tratamiento tras fracaso virológico Staszewski S JAMA Mar 7;285(9):
:")
59
TDF/3TC. Desarrollo mutaciones resistencia Estudio GS 903
M. Miller. XII International HIV Drug Resistance Workshop. Abstract 135. Los Cabos. Junio 2003

61
Estudio MONTANA: HIV-1 RNA <400 y <50 copias/mL
ITT (NC=F) 20 40 60 80 100 4 8 12 16 24 28 32 36 85% RNA <400 copias/mL 80% RNA <50 copias/mL % Meses Piloto FTC+ddI +EFV, QD Pacientes naïve (n=40) CD4+ >100 cells/mm3 HIV-1 RNA >5000 c/ml Molina JM, et al. 2nd IAS, Paris, 2003, Poster # 594.
 % RNA <400 copias/mL. 80% RNA <50 copias/mL. % Meses. Piloto FTC+ddI +EFV, QD. Pacientes naïve (n=40) CD4+ >100 cells/mm3. HIV-1 RNA >5000 c/ml. Molina JM, et al. 2nd IAS, Paris, 2003, Poster # 594.")
62
3TC/ABC vs AZT/3TC. Estudio CNA 30024 Cifras CD4+
ABC/3TC AZT/3TC Basal* 267 258 Semana 48* + 209 + 155 * células/μL De Jesus CID 2004;39:

Presentaciones similares



>")
>")















