Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Nefropatía Diabética Consideraciones en el Manejo Clínico
Carlos Chiurchiu Servicio de Nefrología y Programa de Trasplantes Renales Hospital Privado - Centro Médico de Córdoba

2
Mortalidad anual según los estadíos de Nefropatía Diabética
No nefropatía 1.4% (1.3% to 1.5%) Microalbuminuria 3.0% (2.6% to 3.4%) MUERTE Macroalbuminuria 4.6% (3.6% to 5.7%) Elevada creatinina plasmática o terapia de reemplazo renal 19.2% (14.0% to 24.4%) Adler et al. Kidney Int. 2003;63:
 Microalbuminuria. 3.0% (2.6% to 3.4%) MUERTE. Macroalbuminuria. 4.6% (3.6% to 5.7%) Elevada creatinina plasmática o terapia de reemplazo renal. 19.2% (14.0% to 24.4%) Adler et al. Kidney Int. 2003;63:")
3
DIABETES COMO CAUSA DE INSUFICIENCIA RENAL CRÓNICA TERMINAL EN ARGENTINA
35 30 25 20 PORCENTAJE 15 10 5 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 SINTRA, Incucai 2007

4
SUPERVIVENCIA EN HEMODIALISIS
20 40 60 80 100 Supervivencia Acumulada % 50 150 200 250 300 Tiempo (meses) Logrank: p < 0,0001 n:305 n: 71 Diabéticos No Diabéticos Hospital Privado-Centro Médico de Córdoba: período
 Logrank: p < 0,0001. n:305. n: 71. Diabéticos. No Diabéticos. Hospital Privado-Centro Médico de Córdoba: período")
5
RECOMENDACIONES Individuos a riesgo de Medidas a implementar
Enf. Renal Crónica Diabéticos Hipertensos Enf Autoinmunes Infec. Sistémicas Mayores de 60 años Historia fliar enf. Renal Reducción masa renal Antec. de IRA Medidas a implementar Medir la creatinina sérica Evaluar la presencia de proteinuria Estimar el FG Monitorear el índice P/C Source: Kidney Disease Outcome Quality Initiative of the National Kidney Foundation.

7
CASO CLINICO Mujer, 57 años Diabética tipo 2 (15 años de diagnóstico)
HTA (10 años de diagnóstico) Refiere controles de PA en casa de 120/80 Nunca tabaco BMI: 31 Probable SAOS (en estudio) Sin retinopatía Control previo hace 6 meses PA: 155/95 Sin edemas Creatinina: 1.10 mg/dl (previa 0.88 mg/dl) Indice Albúmina/Creatinina urinaria: 28 mg/g K: 5.4 mEq/l Hb glicosilada: 9.4% LDL: 155 mg/dl HDL: 35 mg/dl Triglicéridos: 225 mg/dl Orina completa: normal Medicación: Enalapril 10 mg/día, Atorvastatina 10 mg/día, Metformina 850 mg c/12 hs
 Refiere controles de PA en casa de 120/80. Nunca tabaco. BMI: 31. Probable SAOS (en estudio) Sin retinopatía. Control previo hace 6 meses. PA: 155/95. Sin edemas. Creatinina: 1.10 mg/dl (previa 0.88 mg/dl) Indice Albúmina/Creatinina urinaria: 28 mg/g. K: 5.4 mEq/l. Hb glicosilada: 9.4% LDL: 155 mg/dl. HDL: 35 mg/dl. Triglicéridos: 225 mg/dl. Orina completa: normal. Medicación: Enalapril 10 mg/día, Atorvastatina 10 mg/día, Metformina 850 mg c/12 hs.")
8
¿ Tiene esta paciente caída de la función renal?
¿Es necesario una recolección de orina de 24 hs? ¿ El control de la presión arterial debería ser optimizado? ¿ El valor de K sérico impide seguir utilizando IECAs o ARA II? ¿La optimización del control metabólico mejoraría la salud renal ? ¿ Pudo haberse prevenido la aparición del compromiso renal? ¿ Es necesario interconsultar a un nefrólogo?

9
¿ Tiene esta paciente caída de la función renal?
¿Es necesario una recolección de orina de 24 hs? ¿ El control de la presión arterial debería ser optimizado? ¿ El valor de K sérico impide seguir utilizando IECAs o ARA II? ¿La optimización del control metabólico mejoraría la salud renal ? ¿ Pudo haberse prevenido la aparición del compromiso renal? ¿ Es necesario interconsultar a un nefrólogo?

10
RECOMENDACIONES www.kidney.org/professionals/kdoqi/gfr_calculator.cfm
Source: Kidney Disease Outcome Quality Initiative of the National Kidney Foundation.

11
Estimación del Clearance de Creatinina: Ecuación de Cockroft-Gault
(140-edad) x peso(72 x S.Creat.) (x 0.85 en mujeres) Desarrollada en 249 hombres con creatinina estable Sobrestimación del ClCr en: 1) vegetarianos 2) obesos 3) malnutridos 4) edematosos 5) Bajos FG 50 100 150 200 250 300 Filtrado Glomerular Cockroft Gault Datos de 176 pacientes estudiados en el Hospital Privado Centro Médico de Córdoba
 x peso(72 x S.Creat.) (x 0.85 en mujeres) Desarrollada en 249 hombres. con creatinina estable. Sobrestimación del ClCr en: 1) vegetarianos. 2) obesos. 3) malnutridos. 4) edematosos. 5) Bajos FG Filtrado Glomerular. Cockroft Gault. Datos de 176 pacientes estudiados en el. Hospital Privado Centro Médico de Córdoba.")
12
Generación de las variables
Ecuación MDRD: Generación de las variables ECUACIÓN ABREVIADA 186 x (Creatinina) x (edad)-0.203 (x en mujeres, x en Raza Negra) Levey et al., Ann Int Med, 1999
 x. (edad) (x en mujeres, x en Raza Negra) Levey et al., Ann Int Med,")
13
Ecuación MDRD: Rendimiento
Puede subestimar el FG en ERC estadio 1 Puede sobrestimar el FG en ERC estadios 4-5 4 Estudios en pacientes con ERC: diferencias medias encontradas: -5,5 ml/min hasta +0.9 ml/min/1.73m2 Levey et al., Ann Int Med, 1999

14
Ecuación MDRD: Limitaciones
Relacionadas a la calibración de la creatinina En población con FG > 60 ml/min En pacientes con IRA En diabéticos con hiperfiltración En población oriental (otras etnias?) Levey et al., N Eng J Med 2006
 Levey et al., N Eng J Med")
15
Subestimación del FG con MDRD en Sujetos Diabéticos Tipo 2
Gaspari et al. 2005 200 160 120 MDRD (ml/min/1.73m2) 80 40 y = x r = 0.560 n = 413 40 80 120 160 200 Clearance Plasmático de Iohexol (ml/min/1.73m2)
 y = x r = n = Clearance Plasmático de Iohexol (ml/min/1.73m2)")
16
Estimación del FG en Diabéticos Influencia del Control Metabólico
Detección de FG < 60 ml/min Rigellau V et al. Diabetes Care 2006

17
¿ Tiene esta paciente caída de la función renal?
¿Es necesario una recolección de orina de 24 hs? ¿ El control de la presión arterial debería ser optimizado? ¿ El valor de K sérico impide seguir utilizando IECAs o ARA II? ¿La optimización del control metabólico mejoraría la salud renal ? ¿ Pudo haberse prevenido la aparición del compromiso renal? ¿ Es necesario interconsultar a un nefrólogo?

18
GUIDELINE 5. ASSESSMENT OF PROTEINURIA
Criterion Standard When screening tests are positive, measurement of protein excretion in a 24-hour collection has been the longstanding “gold standard” for the quantitative evaluation of proteinuria. An alternative method for quantitative evaluation of proteinuria is measurement of the ratio of protein or albumin to creatinine in an untimed “spot” urine specimen. These ratios correct for variations in urinary concentration due to hydration and provide a more convenient method of assessing protein and albumin excretion than that involved with timed urine collections. American Journal of Kidney Diseases,Vol 39, No 2, Suppl 1 (February), 2002
,")
19
¿Por qué es necesario conocer la proteinuria de nuestros pacientes?
La proteinuria es una característica común de las nefropatías crónicas Mayor proteinuria se asocia con mayor riesgo de enfermedad renal crónica Mayor proteinuria se asocia con mayor velocidad en la pérdida del filtrado glomerular La proteinuria se asocia con aumento en el riesgo CV Source: Kidney Disease Outcome Quality Initiative of the National Kidney Foundation.

21
Ritmo circadiano de la proteinuria: Importancia en el Indice P/C
Koopman N, et al .Nephrol Dial Transplant 1989

22
60Kg 70Kg 80Kg

23
Indice P/C como indicador de Proteinuria de 24 hs:
Diabéticos con Nefropatía in assessing the exact amount of proteinuria, the urine P/C ratio may have unacceptably wide limits of agreement in high protein excretion range. Robdy R, et al. Am J Kidney Dis, 1995

24
Indice A/C como indicador de Albuminuria de 24 hs:
Screening de Microalbuminuria en Diabéticos tipo 2 (531 pacientes) Incerti et al.Nephrol Dial Transplant 2005
 Incerti et al.Nephrol Dial Transplant")
25
¿ Tiene esta paciente caída de la función renal?
¿Es necesario una recolección de orina de 24 hs? ¿ El control de la presión arterial debería ser optimizado? ¿ El valor de K sérico impide seguir utilizando IECAs o ARA II? ¿La optimización del control metabólico mejoraría la salud renal ? ¿ Pudo haberse prevenido la aparición del compromiso renal? ¿ Es necesario interconsultar a un nefrólogo?

26
INDICATIONS FOR INITIAL TREATMENT AND GOALS FOR ADULT HYPERTENSIVE DIABETIC PATIENTS
Systolic Diastolic Goal (mmHg) < 130 < 80 Behavioral therapy alone (maximum 3 months) then add pharmacologic treatment Behavioral therapy + 140 90 American Diabetes Association, Diabetes Care 2004
 < 130 < 80. Behavioral therapy alone (maximum. 3 months) then add. pharmacologic treatment. Behavioral therapy + 140 90. American Diabetes Association, Diabetes Care")
27
¿ Tiene esta paciente caída de la función renal?
¿Es necesario una recolección de orina de 24 hs? ¿ El control de la presión arterial debería ser optimizado? ¿ El valor de K sérico impide seguir utilizando IECAs o ARA II? ¿La optimización del control metabólico mejoraría la salud renal ? ¿ Pudo haberse prevenido la aparición del compromiso renal? ¿ Es necesario interconsultar a un nefrólogo?

28
WITHDRAWAL FROM CLINICAL TRIALS ON RAS INHIBITORS BECAUSE OF SEVERE HYPERKALEMIA
non RAS-I Diabetic nephropathy Lewis et al., N Engl J Med, 1993 Lewis et al; N Engl J Med, 2001 RENAAL, N Engl J Med, 2001 Total 3/207 11/579 9/751 23/1531 (1.6%) 0/202 5/1136 2/762 7/2100 (0.3%) Non-diabetic nephropathy Kamper et al., Am J Hypertens, 1992 Hannedouche et al., Br Med J, 1994 Maschio et al., N Engl J Med, 1994 GISEN, Lancet, 1997 Ruggenenti et al., Lancet, 1998 Total 0/35 2/52 5/300 1/78 0/99 8/564 (1.4%) 0/35 2/48 3/283 1/88 1/87 7/521 (1.3%) Averall 31/2101 (1.5%) 14/2621 (0.6%) In patients with chronic renal disease, ACE inhibitors usually increase serum K+ by mEq/L, but induce severe hyperkalemia in no more than 1% to 2 % of cases
 0/202. 5/ /762. 7/2100 (0.3%) Non-diabetic nephropathy. Kamper et al., Am J Hypertens, Hannedouche et al., Br Med J, Maschio et al., N Engl J Med, GISEN, Lancet, Ruggenenti et al., Lancet, Total. 0/35. 2/52. 5/300. 1/78. 0/99. 8/564 (1.4%) 0/35. 2/48. 3/283. 1/88. 1/87. 7/521 (1.3%) Averall. 31/2101 (1.5%) 14/2621 (0.6%) In patients with chronic renal disease, ACE inhibitors usually increase serum K+ by mEq/L, but induce severe hyperkalemia in no more than 1% to 2 % of cases.")
29
EL BLOQUEO DEL SRAA SE ASOCIA CON MENOR PROGRESIÓN HACIA LA MACROPROTEINURIA
Incidencia de macroalbuminuria Cambio en la albuminuria p = 0.006 20 10 9 % 14.9 % 15 NNT: 11 9.7 % - 6 % % 10 % NNT: 5 -10 5.2 % 5 -20 - 30 % -30 150 mg 300 mg 150 mg 300 mg Placebo Irbesartan Placebo Irbesartan Parving et al., N Engl J Med, 2001

30
¿ Tiene esta paciente caída de la función renal?
¿Es necesario una recolección de orina de 24 hs? ¿ El control de la presión arterial debería ser optimizado? ¿ El valor de K sérico impide seguir utilizando IECAs o ARA II? ¿La optimización del control metabólico mejoraría la salud renal ? ¿ Pudo haberse prevenido la aparición del compromiso renal? ¿ Es necesario interconsultar a un nefrólogo?

31
Reversión de la ND con el Tx de Pancreas
Basal 5 años 10 años Cl Cr (ml/min) 108.2 74.2 74.1 Album. (mg/día) 103 30 20 Hb Glic (%) 8.7 5.3 5.5 Fioretto P, et al. N Eng J Med 1998
 Album. (mg/día) Hb Glic. (%) Fioretto P, et al. N Eng J Med")
32
INCIDENCIA DE MICRO Y MACROALBUMINURIA
CON CONTROL METABÓLICO INTENSIVO Retinopatía Basal NO Retinopatía Basal SI MICRO MICRO MACRO MACRO DCCT Research Group N Eng J Med 1993

33
CONTROL METABÓLICO INTENSIVO Y EVENTOS VASCULARES: (11
CONTROL METABÓLICO INTENSIVO Y EVENTOS VASCULARES: ( Diabéticos tipo 2) Relative Risk (95% CI) Eventos Macro Incidencia Nefropatía -0.60 -0.80 0.80 ADVANCE Collaborative Group. N Eng J Med 2008
 Relative Risk (95% CI) Eventos Macro. Incidencia Nefropatía ADVANCE Collaborative Group. N Eng J Med")
36
¿ Tiene esta paciente caída de la función renal?
¿Es necesario una recolección de orina de 24 hs? ¿ El control de la presión arterial debería ser optimizado? ¿ El valor de K sérico impide seguir utilizando IECAs o ARA II? ¿La optimización del control metabólico mejoraría la salud renal ? ¿ Pudo haberse prevenido la aparición del compromiso renal? ¿ Es necesario interconsultar a un nefrólogo?

37
THE BENEDICT TRIAL Patients End point Target HbA1C Target BP
1,204 subjects with type 2 diabetes, high blood pressure and normal urinary albumin excretion Progression to microalbuminuria < 7.0 %* ≤ 120/80 mmHg* * ADA guidelines, Diabetes Care 1998 Ruggenenti et al., N Eng J Med, 2004

38
Study design Randomisation RUN-IN TREATMENT PERIOD
RAS inhibitors withdrawal Trandolapril (2mg/d) ndCCBs withdrawal Verapamil S.R. (240 mg/d) Randomisation Trandolapril (2mg/d) plus Verapamil S.R. (180 mg/d) Placebo -6 -5 -4 -3 -2 -1 6 12 18 24 30 36 weeks months Overnight UAE Blood pressure and routine laboratory tests Ruggenenti et al., N Eng J Med, 2004
 ndCCBs withdrawal. Verapamil S.R. (240 mg/d) Randomisation. Trandolapril (2mg/d) plus Verapamil S.R. (180 mg/d) Placebo weeks. months. Overnight UAE. Blood pressure and routine laboratory tests. Ruggenenti et al., N Eng J Med,")
39
Arterial Blood Pressure (mmHg)
Blood pressure according to treatment group 160 Systolic 150 140 130 Arterial Blood Pressure (mmHg) 120 Trandolapril Verapamil 110 Trandolapril plus Verapamil 100 Placebo Diastolic 90 80 70 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 Follow-up (months) Ruggenenti et al., N Eng J Med, 2004
 120. Trandolapril. Verapamil Trandolapril plus Verapamil Placebo. Diastolic Follow-up (months) Ruggenenti et al., N Eng J Med,")
40
of Microalbuminuria (%)
Placebo (30 events) 15 10 of Microalbuminuria (%) Cumulative Incidence 5 Trandolapril plus verapamil (17 events) A.F. (95 % C.I.) = 0.39 ( ) p = 0.01 6 12 18 24 30 36 42 48 Follow-up (months) No. at Risk Trandolapril plus Verapamil Placebo 300 249 229 232 214 217 203 210 187 201 176 192 164 162 136 115 89 Ruggenenti et al., N Eng J Med, 2004
 of Microalbuminuria (%) Cumulative Incidence. 5. Trandolapril. plus. verapamil. (17 events) A.F. (95 % C.I.) = 0.39 ( ) p = Follow-up (months) No. at Risk. Trandolapril plus. Verapamil. Placebo Ruggenenti et al., N Eng J Med,")
41
Cumulative incidence of
Placebo (30 events) 15 NNT: 8 10 Cumulative incidence of microalbuminuria (%) 5 Trandolapril (18 events) A.F. (95 % C.I.) = 0.47 ( ) p = 0.01 6 12 18 24 30 36 42 48 Follow-up (months) No. at Risk Trandolapril Placebo 301 300 254 229 237 214 224 203 207 187 198 176 188 164 149 136 104 89 Ruggenenti et al., N Eng J Med, 2004
 15. NNT: Cumulative incidence of. microalbuminuria (%) 5. Trandolapril. (18 events) A.F. (95 % C.I.) = 0.47 ( ) p = Follow-up (months) No. at Risk. Trandolapril. Placebo Ruggenenti et al., N Eng J Med,")
42
Cumulative incidence of
Verapamil (36 events) 15 Placebo (30 events) 10 Cumulative incidence of microalbuminuria (%) 5 6 12 18 24 30 36 42 48 Follow-up (months) No. at Risk Verapamil Placebo 303 300 234 229 210 214 202 203 189 187 181 176 174 164 134 136 98 89 Ruggenenti et al., N Eng J Med, 2004
 15. Placebo. (30 events) 10. Cumulative incidence of. microalbuminuria (%) Follow-up (months) No. at Risk. Verapamil. Placebo Ruggenenti et al., N Eng J Med,")
43
* * * p < 0.05 vs. enalapril E F F E C T S O F E N A L A P R I L (
1 m g / d a y ) I N N O N - O B E S E S U B J E C T S W I T H T Y P E 2 D I A B E T E S , N O R M A L B L O O D P R E S S U R E A N D N O R M O A L B U M I N U R I A 40 * 30 UAE (mg/24 h) 20 10 110 * 105 ) Placebo (n=79) Mean Blood Pressure mmHg 100 Enalapril (n=77) ( 95 90 1 2 3 4 5 6 Years * p < 0.05 vs. enalapril Ravid et al., Ann Intern Med 1998
 I. N. N. O. N. - O. B. E. S. E. S. U. B. J. E. C. T. S. W. I. T. H. T. Y. P. E. 2. D. I. A. B. E. T. E. S. , N. O. R. M. A. L. B. L. O. O. D. P. R. E. S. S. U. R. E. A. N. D. N. O. R. M. O. A. L. B. U. M. I. N. U. R. I. A. 40. * 30. UAE. (mg/24 h) * 105. ) Placebo (n=79) Mean Blood Pressure. mmHg Enalapril (n=77) ( Years. * p < 0.05 vs. enalapril. Ravid et. al., Ann Intern Med")
44
¿ Tiene esta paciente caída de la función renal?
¿Es necesario una recolección de orina de 24 hs? ¿ El control de la presión arterial debería ser optimizado? ¿ El valor de K sérico impide seguir utilizando IECAs o ARA II? ¿La optimización del control metabólico mejoraría la salud renal ? ¿ Pudo haberse prevenido la aparición del compromiso renal? ¿ Es necesario interconsultar a un nefrólogo?

45
DERIVACION PRECOZ VS TARDIA
Kinchen et al. An Inter Med 2002, 137

46
MORTALIDAD Y DERIVACION TARDIA
Kazmi et al. NDT 2004, 19, 1808

47
TRASPLANTE Y DERIVACION TARDIA
Cass et al. AJKD 2003, 42, 1043

48
SITUACION CLINICA DEL PACIENTE CON IRC AL MOMENTO DE DERIVACION AL NEFROLOGO
EXPERIENCIA EN UN HOSPITAL POLICLINICO Serv. de Nefrología. Hosp. Privado-Centro Médico de Córdoba Carrera de Posgrado en Nefrología Univ. Católica de Córdoba. Argentina

49
CRITERIOS DE INCLUSION
SITUACION CLINICA AL MOMENTO DE DERIVACION AL NEFROLOGO CRITERIOS DE INCLUSION Primera visita al nefrólogo. TFG (Cockorff) < 60 ml/min. Caracteristicas basales al momento de la derivación n Edad (años) Sexo (M / F) 63 57,7 ± 17,3 45 /18
 < 60 ml/min. Caracteristicas basales al momento de la derivación. n. Edad (años) Sexo (M / F) ,7 ± 17,3. 45 /18.")
50
LUGAR DE LA 1º CONSULTA AL NEFRÓLOGO
Nº Ptes 20 18 52,9 % 16 47,1 % 14 12 10 8 6 4 2 CONSULTORIO EXTERNO INTERNADO

51
FACTORES COMORBIDOS DIABETES DBT (39,7%) NO-DBT (60,3%)
 NO-DBT (60,3%)")
52
FACTORES COMORBIDOS IECA - ARA DIURETICOS
MEDICAMENTOS ANTI- HTA EN DIABETES IECA - ARA DIURETICOS % 80 70 60 50 40 30 20 10 SI NO SI NO

53
FACTORES COMORBIDOS Patología N (%) Anemia Dislipemia IAM / ATC ACV ICC E. Hepáticas Vascular periférica Tabaquismo 14 (37,8) 17 (70,8) 8 (26,6) 2 (6,9) 1 (3,7) 6 (21,4) 9 (32,1)
 17 (70,8) 8 (26,6) 2 (6,9) 1 (3,7) 6 (21,4) 9 (32,1)")
54
DATOS BIOQUIMICOS X ± DS Rango Creatinina, mg/dl Urea, mg/dl Ac Urico, mg/dl HTO, % HB, g/dl 2,9 ± 2,1 100 ± 53,4 6,8 ± 2,0 37,3 ± 6,3 12,1 ± 1,8 0,9 – 11,7 20 – 242 3,9 – 10,7 28,9 – 51,0 8,3 – 15,4

55
DATOS BIOQUIMICOS NIVELES DE CREATININA
% 50 45 40 35 30 25 20 15 10 5 < 1,5 1,5 - 3,0 > 3,0 Creat, mg/dl

56
NIVELES DE CREATININA SEGÚN ETIOLOGIA
DATOS BIOQUIMICOS NIVELES DE CREATININA SEGÚN ETIOLOGIA 5 4,5 4 3,5 3 2,5 2 1,5 1 0,5 GMN DBT PKD NTI NAE OTROS

57
Insuficiencia Renal Crónica
Complicaciones de la Insuficiencia Renal Crónica Estadios de Enfermedad Renal % Pacientes afectados HTA Hiperparat. Anemia Hiperfosfatemia Inactividad Hipoalbuminem. NHANES III: J Am Soc Nephrol 13: 504–510, 2002

58
Calcificaciones coronarias en Diabéticos
90 CAC < 10 80 CAC 70 CAC CAC > 400 60 No IRC IRC 3-5 50 IRC 1-2 % 40 30 20 10 Kramer H et al, J Am Soc Nephrol 2005

59
CASO CLINICO Varón, 66 años Diabético tipo 2 (20 años de diagnóstico)
IAM a los 50 años Fumador 30 cig/día desde los 18 años BMI: 28 Retinopatía diabética proliferativa (laser bilateral) Control previo hace 1 año PA: 165/105 Edema MMII ++ Creatinina: 3.5 mg/dl (previa 2.8 mg/dl) Indice Proteínas/Creatinina urinaria: 2.7 g/g K: 4.8 mEq/l Hb glicosilada: 8.5% LDL: 145 mg/dl HDL: 48 mg/dl Triglicéridos: 290 mg/dl Orina completa: Prot +++, Gluc ++, Hemoglobina + Medicación: Losartán 100 mg/día, Hidroclorotiazida 25 mg/día, Atenolol 50 mg/día, Atorvastatina 20 mg/día, AAS 100 mg/día, Insulinoterapia
 Control previo hace 1 año. PA: 165/105. Edema MMII ++ Creatinina: 3.5 mg/dl (previa 2.8 mg/dl) Indice Proteínas/Creatinina urinaria: 2.7 g/g. K: 4.8 mEq/l. Hb glicosilada: 8.5% LDL: 145 mg/dl. HDL: 48 mg/dl. Triglicéridos: 290 mg/dl. Orina completa: Prot +++, Gluc ++, Hemoglobina + Medicación: Losartán 100 mg/día, Hidroclorotiazida 25 mg/día, Atenolol 50 mg/día, Atorvastatina 20 mg/día, AAS 100 mg/día, Insulinoterapia.")
60
¿ Cuál sería el esquema hipotensor a utilizar ?
¿Es de utilidad usar IECAs o ARA II ante esta función renal? ¿ Cuál es superior entre ambas categorias? ¿ La asociación de IECAs con ARA II es útil? ¿Existen otros tratamientos que aporten beneficio? ¿ Es posible pensar en el Trasplante renal en un paciente diabético?

61
¿ Cuál sería el esquema hipotensor a utilizar ?
¿Es de utilidad usar IECAs o ARA II ante esta función renal? ¿ Cuál es superior entre ambas categorias? ¿ La asociación de IECAs con ARA II es útil? ¿Existen otros tratamientos que aporten beneficio? ¿ Es posible pensar en el Trasplante renal en un paciente diabético?

62
The risk of macrovascular and microvascular complications in type 2 diabetes is strongly associated with blood pressure UKPDS (36): BMJ 2000;321:
: BMJ 2000;321:")
63
Rate of major cardiovascular events
according to Diastolic Blood Pressure DBP Goal < 90 < 85 25 – 20 – 15 – 10 – 5 – 0 – 25 – 20 – 15 – 10 – 5 – 0 – P <0.005 for trend < 80 P <0.5 for trend Rate/1000 person/year This slide summarizes the data in the patients with diabetes. It is kind of confusing and hard to read, but it shows you the relative risk, major cardiovascular events--all MIs, all CVAs, cardiovascular mortality, total mortality; the bars represent the difference between the diastolic of 90 versus 85, 85 versus 80. The point is that in several of these major categories, major cardiovascular event, mortality--that in the patients with diabetes, there was a striking degree of protection by achieving the lower blood pressure goal. They found the overall study was somewhat positive. But in many of these studies, the data in the diabetic population was much more strikingly positive. It is kind of a recurring theme in these studies. The one subset that benefits from the most intensive, aggressive therapy are the diabetic patients. So lowering blood pressure is good. All patients n: 18790 Diabetic n: 1501 HOT Study: Lancet 1998

64
Modification of Diet in Renal Disease study
840 patients with non-diabetic proteinuric nephropathies Mean glomerular filtration rate (GFR) decline and achieved follow-up blood pressure Results of the Modification of Diet in Renal Disease study showed that in patients with non-diabetic proteinuric renal disease, targeting treatment at BP levels of 125/75 mmHg or less reduced GFR decline more effectively than if the target was 140/90 mmHg. However, 48% of patients in the lower BP group received ACEi therapy vs 28% in the usual BP group. Thus, the benefit recorded in the low BP group was affected by use of ACEi. Peterson JC et al. Ann Intern Med, 1995
 decline and. achieved follow-up blood pressure. Results of the Modification of Diet in Renal Disease study showed that in patients with non-diabetic. proteinuric renal disease, targeting treatment at BP levels of 125/75 mmHg or less reduced GFR. decline more effectively than if the target was 140/90 mmHg. However, 48% of patients in the. lower BP group received ACEi therapy vs 28% in the usual BP group. Thus, the benefit recorded in the low BP group was affected by use of ACEi. Peterson JC et al. Ann Intern Med,")
65
Jafar TH et. Ann Intern Med, 2003
Relative risk for kidney disease progression based on current level of SBP and current proteinuria 11 randomized, controlled trials comparing the efficacy of antihypertensive regimens with or without ACE inhibitors A meta-analysis of 11 randomised trials of ACEi therapy in 1860 people with non-diabetic chronic kidney disease showed that systolic BP reduction to less than 120 mmHg did not offer additional renoprotection compared with targets of mmHg, and reduction to 110 mmHg or less even accelerated progression of renal disease. n = 1860 patients Jafar TH et. Ann Intern Med, 2003

66
The decrease in risk for each 10 mm Hg reduction of SBP for macro and microvascular complications
UKPDS (36): BMJ 2000;321:
: BMJ 2000;321:")
67
ACE inhibitors versus dihydropyridine
calcium channel blockers in diabetic patients 12 Nisoldipine 16 Amlodipine 9 12 % 6 % 8 Fosinopril Enalapril 4 3 ABCD trial: But it doesn't tell us anything about the relative efficacy of the different classes of drugs. So there have now been a couple of studies directly comparing ACE inhibitors versus dihydropyridine calcium channel blockers when it comes to cardiovascular protection. This one and the next study I am going to show you are both published around the same time, in This was the ABCD trial, which was a prospective, randomized, controlled trial of 470 hypertensive patients with type 2 diabetes, randomized to enalapril or nisoldipine. And this study, I believe, they actually stopped a little bit early because when they looked at fatal or non-fatal MIs, they found a significant difference in that the patients on the calcium channel blocker arm were five times more likely to have a significant event as compared to the patients on the ACE inhibitor. FACET trial: A very similar study, published around the same time--and these will all be discussed again Friday afternoon, was the FACET trial. Different drugs, same design, fosinopril versus amlodipine, a prospective, randomized, control trial of 380 patients followed for 3 1/2 years. When they looked at a combined outcome of acute MI, stroke, or hospitalization for angina, again they found a significant difference, with the ACE providing superior cardiovascular effect. Most cardiologists, as I understand it, are not taking this to mean that calcium channel blockers are bad for the heart; it is just that ACE inhibitors are better. But I think it is starting to be a fairly consistent story here that in patients with diabetes who have a huge cardiovascular risk anyway, ACE inhibitors are kind of a reasonable thing to have in the regimen. ABCD trial 470 Hipertensive patients 5 years follow up MI: secondary end point FACET trial 380 Hipertensive patients 3.5 years follow up Combined End Point: MI, stroke, angina

68
CAPPP study: ACE inhibitor therapy associated with
reduction in endpoints : Diabetic vs Total population The Captopril Prevention Project was a fairly large trial, as well. This was a hypertension trial, not specifically a diabetes trial. It was a trial of captopril versus conventional therapy with about 11,000 patients. What they found in the entire group was that there was really no significant difference in the incidence of these various endpoints. But in the diabetic subgroup, which was pretty small--only 600 patients with diabetes, the ACE inhibitor was associated with a significant reduction in most of the endpoints . Some of that data is shown here. The yellow lines are the diabetic subjects, and the orange lines are the total population. As you can see, for the total population as a whole, they all crossed a line of identity, whereas the ACE inhibitor did show a benefit in the diabetic patients. Interestingly in this study and in the HOPE study--both of those studies found that in patients who did not have diabetes going into the study that being on the ACE inhibitor arm reduced your risk of developing diabetes, which I think is very interesting. It has now been shown in two good-sized studies Hansson L , et al. Lancet 1999

69
no clinical proteinuria previous cardiovascular event or at least
EFFECTS ON RAMIPRIL ON CARDIOVASCULAR AND MICROVASCULAR OUTCOMES IN PATIENTS WITH TYPE 2 DIABETES ENROLLED IN THE HOPE STUDY THE MICRO-HOPE STUDY - age > 55 years no clinical proteinuria previous cardiovascular event or at least one other cardiovascular risk factor HOPE Study Investigators, Lancet, 2002

70
THE MICROHOPE STUDY Clinical outcomes for Ramipril and placebo group
Relative Risk (95% CI) Primary outcomes Combined Myocardial infarction Stroke Cardiovascular death Secondary outcomes But in micro-HOPE, which was just published, they specifically showed the data from the diabetic subjects. It was quite impressive. This slide shows you reduction in risks. So the higher the bar, the better. The combined outcome, MI, CVA, cardiovascular disease I think that is, and overt proteinuria. As you can see, there was a significant reduction in risk, on the order of about 30 percent for most of these, all of them significant in the diabetic population. So in these type 2 diabetic patients, it appeared as though treatment with ramipril was extremely effective in preventing major cardiovascular disease. It is one of the bigger studies we have out there. Total mortality Revascularization Overt nephropathy - 50% - 25% 25% HOPE Study Investigators, Lancet, 2002
 Primary outcomes. Combined. Myocardial infarction. Stroke. Cardiovascular death. Secondary outcomes. But in micro-HOPE, which was just published, they specifically showed the data from the diabetic subjects. It was quite impressive. This slide shows you reduction in risks. So the higher the bar, the better. The combined outcome, MI, CVA, cardiovascular disease I think that is, and overt proteinuria. As you can see, there was a significant reduction in risk, on the order of about 30 percent for most of these, all of them significant in the diabetic population. So in these type 2 diabetic patients, it appeared as though treatment with ramipril was extremely effective in preventing major cardiovascular disease. It is one of the bigger studies we have out there. Total mortality. Revascularization. Overt nephropathy. - 50% - 25% 25% HOPE Study Investigators, Lancet,")
71
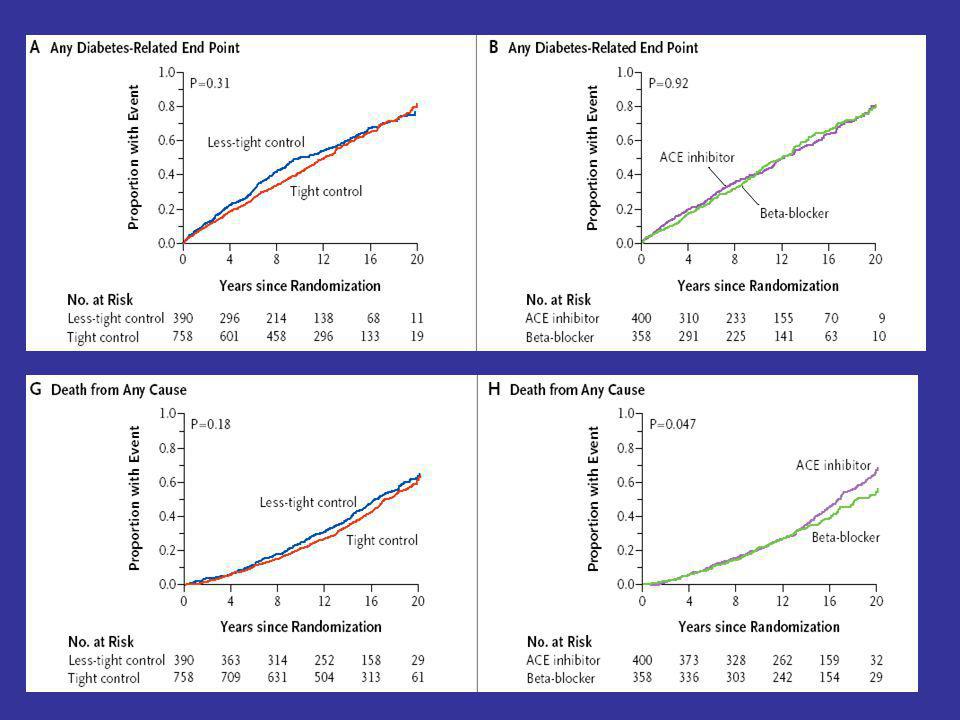
ATENOLOL AND CAPTOPRIL IN REDUCING RISK OF MACRO
AND MICROVASCULAR COMPLICATIONS: UKPDS 39 hypertensive type 2 diabetic patients The one possible exception to the story that ACE inhibitors are better is the UKPDS, the gigantic United Kingdom study in patients with type 2 diabetes. They looked at two issues: Tight blood pressure control versus less tight; and then they compared captopril to atenolol. This slide shows you the value of treating blood pressure. In the patients who received better blood pressure control, the relative risk of microvascular disease, microalbuminuria, and retinopathy was significantly reduced. But they found no difference between captopril and atenolol when it came to the incidence of cardiovascular events, etc. So that is kind of the one exception to this otherwise fairly consistent story that ACE inhibitors are superior. But, obviously, atenolol may be a cardioprotective drug, as well Myocardial infarction, sudden death, stroke, peripheral vascular disease and renal failure Less tight BP control: 154/87 Captopril: 144/83 Atenolol: 143/81 UKPDS (39) BMJ, 1998
 BMJ,")
72
Cardiovascular morbidity and mortality in patients with diabetes in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): Inclusion criteria Design Treatment Follow-up Main end point - Diabetes (both types) - Hypertension SBP: mmHg and/or DBP: mmHg - Left ventricular hypertrophy - Randomized, double blind - Losartan ( mg/day) n = 586 - Atenolol ( mg/day) n = 609 - 4.7 ± 1.1 years Combined cardiovascular mortality, stroke, miocardial infarction Lindholm et al., Lancet, 2002
 - Hypertension SBP: mmHg and/or. DBP: mmHg. - Left ventricular hypertrophy. - Randomized, double blind. - Losartan ( mg/day) n = Atenolol ( mg/day) n = ± 1.1 years. Combined cardiovascular mortality, stroke, miocardial infarction. Lindholm et al., Lancet,")
73
Blood pressure and metabolic control were comparable
in the two treatment groups throughout the whole study period Lingholm et al., Lancet, 2002

74
Average Drugs Needed to Achieve
Blood Pressure Goal I want to make the point that multiple drugs are needed. This is why we need data on what happens when you use multiple drugs. This slide just shows you the average number of drugs needed to get to goal in a bunch of the big studies. They are not all diabetes studies: UKPDS, ABCD, MDRD, HOT and ASK. As you can see, the number of drugs needed ranges from about 2.8 up to about 3.9. The point is, as you all know from your practice, you need a bunch of drugs. What we don't know is what the combination of drugs will do.

75
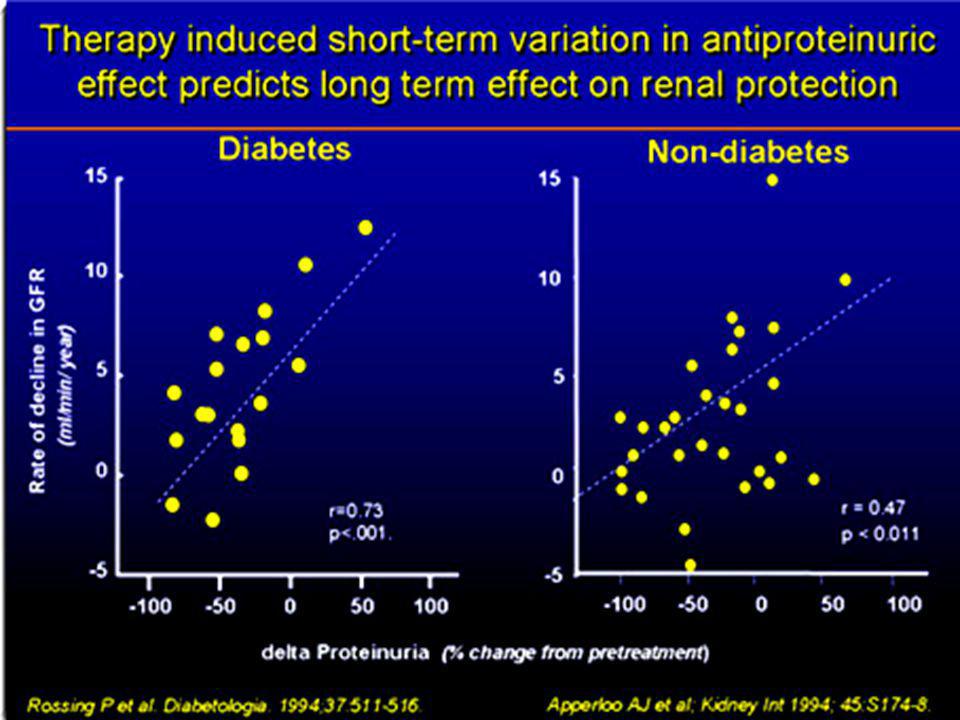
MAP (mmHg) GFR (ml/min/year) Diabetes Non-diabetes Untreated HTN
95 98 101 104 107 110 113 116 119 r = 0.69; p < 0.05 -2 -4 -6 GFR (ml/min/year) -8 -10 -12 Untreated HTN -14 130/85 140/90 Diabetes Non-diabetes Parving et al., Br Med J, 1989 Viberti et al., JAMA, 1993 Hebert et al., Kidney Int, 1994 Lebovitz et al., Kidney Int, 1994 Bakris et al., Kidney Int, 1996 Bakris et al., Hypertension, 1997 Klahr et al., N Engl J Med, 1993 Maschio et al., N Engl J Med, 1996 GISEN Group, Lancet, 1997 Bakris et al., Am J Kidney Dis, 2000
 Untreated HTN / /90. Diabetes. Non-diabetes. Parving et al., Br Med J, Viberti et al., JAMA, Hebert et al., Kidney Int, Lebovitz et al., Kidney Int, Bakris et al., Kidney Int, Bakris et al., Hypertension, Klahr et al., N Engl J Med, Maschio et al., N Engl J Med, GISEN Group, Lancet, Bakris et al., Am J Kidney Dis,")
78
¿ Cuál sería el esquema hipotensor a utilizar ?
¿Es de utilidad usar IECAs o ARA II ante esta función renal? ¿ Cuál es superior entre ambas categorias? ¿ La asociación de IECAs con ARA II es útil? ¿Existen otros tratamientos que aporten beneficio? ¿ Es posible pensar en el Trasplante renal en un paciente diabético?

79
EFECTOS DEL CAPTOPRIL EN LA PROGRESIÓN HACIA LA INSUFICIENCIA RENAL
EN DIABÉTICOS TIPO 1 PROTEINÚRICOS 25 50 75 100 Captopril Tratamiento convencional % con duplicación de la creatinina Creatinina basal > 1.5 mg/dl 1 2 3 4 2 – 0 – - 2 – - 4 – 6 – 8 – 40 – - 20 – 0 – 60 – P <.001 Reducción de la MAP (mm Hg) % Reducción de la Proteinuria NS Lewis et al. N Engl J Med. 1993
 % Reducción. de la. Proteinuria. NS. Lewis et al. N Engl J Med")
80
RENAAL Reduction of Endpoints in NIDDM with the AII Antagonist Losartan
ESRD type 2 diabetes - Age years - Alb/Cr ratio >300 mg/g, - S Creat mg/dL, 10 20 30 P % with event Risk Reduction: 28% L p=0.002 12 24 36 48 Months NNT: 32

81
RENAAL ESRD by Baseline Level of Serum Creatinine
20 40 60 sCr < 2.0 mg/dL ³ 2.0 mg/dL RR: % % p= sCr ³ 2.0 mg/dL % with event P sCr < 2.0 mg/dL L P L 12 24 36 48 Months sCr (mg/dL) <2.0/³ 2.0 P (+CT) 482/280 463/252 424/186 254/93 33/9 33/9 33/9 33/9 33/9 33/9 L (+CT) 482/269 468/246 429/196 269/106 51/18 51/18 51/18 51/18 51/18 51/18
 <2.0/³ 2.0. P (+CT) 482/ / / /93. 33/9. 33/9. 33/9. 33/9. 33/9. 33/9. L (+CT) 482/ / / / /18. 51/18. 51/18. 51/18. 51/18. 51/18.")
82
¿ Cuál sería el esquema hipotensor a utilizar ?
¿Es de utilidad usar IECAs o ARA II ante esta función renal? ¿ Cuál es superior entre ambas categorias? ¿ La asociación de IECAs con ARA II es útil en Nefropatía DBT? ¿Existen otros tratamientos que aporten beneficio? ¿ Es posible pensar en el Trasplante renal en un paciente diabético?

83
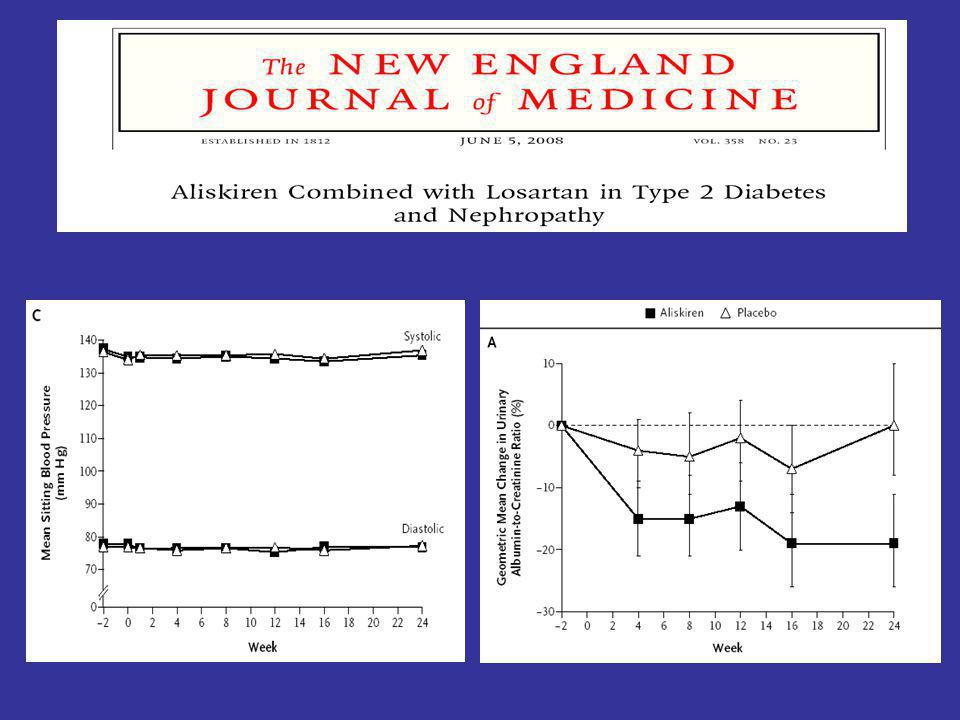
IECAs o ARAII en Nefropatía Diabética: DETAIL study
250 type 2 diabetic patients Mild-moderate hypertensive Albuminuria < 1000 μ/min 80% microalbuminuric - S Creat mg/dl Barnett et al., N Eng J Med, 2004

84
¿ Cuál sería el esquema hipotensor a utilizar ?
¿Es de utilidad usar IECAs o ARA II ante esta función renal? ¿ Cuál es superior entre ambas categorias? ¿ La asociación de IECAs con ARA II es útil en Nefropatía DBT? ¿Existen otros tratamientos que aporten beneficio? ¿ Es posible pensar en el Trasplante renal en un paciente diabético?

85
CANDESARTAN AND LISINOPRIL MICROALBUMINURIA (CALM) STUDY
Adjusted risk reduction (at 24 weeks) in SBP, DBP, and urinary A/C ratio in 197 type 2 diabetics with hypertension and microalbuminuria Candesartan Lisinopril Combination n = 66 n = 64 n = 67 1 D SBP (mmHg) 10 20 30 40 50 DBP urinary A/C ratio (%) 60 16 mg/day Mogensen et al., Br Med J, 2000
 in SBP, DBP, and urinary A/C ratio in 197 type 2 diabetics with hypertension and microalbuminuria. Candesartan. Lisinopril. Combination. n = 66. n = 64. n = D. SBP. (mmHg) DBP. urinary A/C ratio. (%) mg/day. Mogensen et al., Br Med J,")
86
ADDITIVE EFFECT OF ACE INHIBITION AND ANGIOTENSIN II RECEPTOR BLOCKADE
Blood Pressure - Crossover study Type 1 DM Overt nephropathy Treatment: Placebo Benazepril 20 mg/day Valsartan 80 mg/day Combination (full doses) 150 100 mmHg 50 Placebo Benazepril Valsartan Combination 1000 Albuminuria 500 mg/24 hs Placebo Benazepril Valsartan Combination Jacobsen et. al. J Am Soc Nephrol 2003
 mmHg. 50. Placebo. Benazepril. Valsartan. Combination Albuminuria mg/24 hs. Placebo. Benazepril. Valsartan. Combination. Jacobsen et. al. J Am Soc Nephrol")
87
¿ Cuál sería el esquema hipotensor a utilizar ?
¿Es de utilidad usar IECAs o ARA II ante esta función renal? ¿ Cuál es superior entre ambas categorias? ¿ La asociación de IECAs con ARA II es útil en Nefropatía DBT? ¿Existen otros tratamientos que aporten beneficio? ¿ Es posible pensar en el Trasplante renal en un paciente diabético?

88
BENEFICIAL EFFECTS OF ADDING SPIRONOLACTONE TO ANTIHIPERTENSIVE TREATMENT IN TYPE 2 DIABETES NEPHROPATHY Crossover study: (8 weeks per period) - Spironolactone 25 mg/day vs. - Placebo -20 patients with type 2 DM -Overt nephropathy -Full doses of inhibition on RASS Albuminuria p < 0.001 1.5 1.0 (g/24 hours) 0.5 Placebo Spironolactone Rossing et. al. Diabetes Care 2005
 - Spironolactone 25 mg/day vs. - Placebo. -20 patients with type 2 DM. -Overt nephropathy. -Full doses of inhibition on RASS. Albuminuria. p < (g/24 hours) 0.5. Placebo. Spironolactone. Rossing et. al. Diabetes Care")
90
Difference in GFR decline (ml/min/month)
EFFECT OF LIPID REDUCTION ON THE PROGRESSION OF RENAL DISEASE: GFR Meta analysis of studies with statins, fibrates and probucol Trials N° of patients Difference in change of GFR (95% CI) Smulders et al., 1997 Aranda et al., 1994 Rayner et al., 1996 Thomas et al., 1993 Nielsen et al., 1993 Tonolo et al., 1993 Buemi et al., 1999 Hommel et al., 1992 Scanferla et al., 1991 Lam et al., 1995 Olbricht et al., 1999 Nishimuria et al., 1999 TOTAL 15 16 17 18 19 21 24 34 43 118 362 p = 0.008 Treatment worse Treatment better -5 -3 -1 1 3 5 7 Difference in GFR decline (ml/min/month) Fried et al., Kidney Int, 2001
 Smulders et al., Aranda et al., Rayner et al., Thomas et al., Nielsen et al., Tonolo et al., Buemi et al., Hommel et al., Scanferla et al., Lam et al., Olbricht et al., Nishimuria et al., TOTAL p = Treatment worse. Treatment better Difference in GFR decline (ml/min/month) Fried et al., Kidney Int,")
91
Transcription factors
INTERACTION BETWEEN THE RENIN-ANGIOTENSIN SYSTEM AND STATINS ACE-inhibitors AT2 ACE Transcription factors (rho, rac, rab...) AIIRA ANG I ANG II AT1 Other districts NF-kB STATINS - Chemoattraction, adhesion, inflammation - proliferation, differentiation, sclerosis - increased ROS production - endothelial dysfunction LDL, VLDL sdLDL
 AIIRA. ANG I. ANG II. AT1. Other districts. NF-kB. STATINS. - Chemoattraction, adhesion, inflammation. - proliferation, differentiation, sclerosis. - increased ROS production. - endothelial dysfunction. LDL, VLDL. sdLDL.")
92
Tonelli M, et al. J Am Soc Nephrol 16: 3748–3754, 2005.
Pravastatin 40 mg daily versus placebo. Median follow-up was 64 mo. Stage 2 or early stage 3 CKD and diabetes both are associated with higher cardiovascular risk, and pravastatin reduces cardiovascular event rates in people with neither, one, or both characteristics. Given the high absolute benefit of pravastatin in patient with diabetes and stage 2 or early stage 3 CKD, this population in particular should be targeted for widespread use of statins. Tonelli M, et al. J Am Soc Nephrol 16: 3748–3754, 2005.

93
Riesgo* de Insuficiencia Renal Crónica Terminal
en Diabeticos según cuartilos de Hemoglobina R.R. (95 % C.I.) < 11.3 11.3 – 12.5 12.5 – 13.8 13.8 El valor predictivo de la Insuficiencia Renal y microalbuminuria es comparable al de la enfermedad coronaria preexistente y aún superior cuando ambas están asociadas 0.5 1 1.25 1.5 2.0 2.5 Incremento del riesgo Ajustado según edad, sexo, raza, BMI, tabaquismo, función renal, albuminuria, perfil lipídico, calcio, fósforo y PA. RENAAL Study: Kidney International Vol. 66, 2004
 < 11.3 – 12.5 – El valor predictivo de la Insuficiencia Renal y microalbuminuria es comparable al de la enfermedad coronaria preexistente y aún superior cuando ambas están asociadas Incremento del riesgo. Ajustado según edad, sexo, raza, BMI, tabaquismo, función renal, albuminuria, perfil lipídico, calcio, fósforo y PA. RENAAL Study: Kidney International Vol. 66,")
94
Targets: REMISSION CLINIC Blood pressure < 120/80 mmHg
Proteinuria < 0.3 g/24 h LDL < 100 mg/dl LDL + VLDL < 130 mg/dl HbA1c < 7.5 % (diabetics) Ruggenenti et al., Lancet, 2001
 Ruggenenti et al., Lancet,")
95
¿ Cuál sería el esquema hipotensor a utilizar ?
¿Es de utilidad usar IECAs o ARA II ante esta función renal? ¿ Cuál es superior entre ambas categorias? ¿ La asociación de IECAs con ARA II es útil en Nefropatía DBT? ¿Existen otros tratamientos que aporten beneficio? ¿ Cuáles son los resultados del Trasplante renal en un diabético?

96
SOBREVIDA DEL INJERTO Supervivencia Acumulada Logrank: p= 0.6
1 ,8 ,6 Logrank: p= 0.6 Supervivencia Acumulada No DBT DBT ,4 ,2 10 20 30 40 50 60 No DBT DBT Tiempo (meses)
")
97
SOBREVIDA DEL PACIENTE
1 Supervivencia acumulada ,8 ,6 Logrank: p= 0.9 ,4 No DBT DBT ,2 10 20 30 40 50 60 No DBT DBT Tiempo (meses)
")
Presentaciones similares

















 15,000 Mexicanos 43.2% HAS (Salud Publica de México 2010) EUA 1999-2000 29-31% >18 años 58-65.>")


