Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Tratamiento de dislipidemias
Dr. Carlos A Aguilar Salinas Departamento de Endocrinología y Metabolismo Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán

2
La eficacia del tratamiento hipolipemiante
Reducción del riesgo Riesgo absoluto 34% 24% 31% 37% 4S (simvastatin) 22.6 Prevención secundaria LIPID (pravastatin) CARE (pravastatin) 15.9 Riesgo a 5 años 13.2 In all, five major morbidity and mortality statin studies in primary or secondary prevention populations have been completed. This pyramid ranks the studies according to the type of patients that were included in each study. It begins with AFCAPS/TexCAPS, a primary prevention study in patients at low risk of CHD and moves to a smaller group of high-risk CHD patients in 4S, a secondary prevention study. In between the two extremes, covering the majority of patients with and at risk of CHD, are WOSCOPS, CARE, and LIPID. The Cholesterol and Recurrent Events (CARE) and Long-Term Intervention With Pravastatin in Ischaemic Disease (LIPID) studies are representative of the majority of patients with CHD, because patients in these trials had cholesterol levels that were, in general, considered to be in the average range (similar to those of the general population) rather than elevated. 7.9 Prevención primaria WOSCOPS (pravastatin) 2.8 AFCAPS/TexCAPS (lovastatin)
 Prevención secundaria. LIPID (pravastatin) CARE (pravastatin) Riesgo a 5 años In all, five major morbidity and mortality statin studies in primary or secondary prevention populations have been completed. This pyramid ranks the studies according to the type of patients that were included in each study. It begins with AFCAPS/TexCAPS, a primary prevention study in patients at low risk of CHD and moves to a smaller group of high-risk CHD patients in 4S, a secondary prevention study. In between the two extremes, covering the majority of patients with and at risk of CHD, are WOSCOPS, CARE, and LIPID. The Cholesterol and Recurrent Events (CARE) and Long-Term Intervention With Pravastatin in Ischaemic Disease (LIPID) studies are representative of the majority of patients with CHD, because patients in these trials had cholesterol levels that were, in general, considered to be in the average range (similar to those of the general population) rather than elevated Prevención primaria. WOSCOPS. (pravastatin) 2.8. AFCAPS/TexCAPS. (lovastatin)")
3
Recomendaciones europeas 2003 Sujetos con alto riesgo cardiovascular
Personas con cardiopatía isquémica o que tengan un riesgo absoluto equivalente (2% por año)*: Enfermedad vascular cerebral sintomática, Aneurisma de la aorta Insuficiencia arterial de miembros inferiores) Casos con alto riesgo por tener: Múltiples factores de riesgo con un riesgo absoluto 0.5% por año ahora o extrapolado a los 60 años. Colesterol 320 mg/dl, LDL-C 240 mg/dl o presión arterial 180/110mmHg Diabetes tipo 2 o tipo 1 con microalbuminuria *(0.5% usando el sistema SCORE) European Heart J 2003: 24:
*: Enfermedad vascular cerebral sintomática, Aneurisma de la aorta. Insuficiencia arterial de miembros inferiores) Casos con alto riesgo por tener: Múltiples factores de riesgo con un riesgo absoluto 0.5% por año ahora o extrapolado a los 60 años. Colesterol 320 mg/dl, LDL-C 240 mg/dl o presión arterial 180/110mmHg. Diabetes tipo 2 o tipo 1 con microalbuminuria. *(0.5% usando el sistema SCORE) European Heart J 2003: 24:")
4
Programa Nacional de Educación en Colesterol 2001
Sujetos con alto riesgo cardiovascular Personas con cardiopatía isquémica o que tengan un riesgo absoluto equivalente (2% por año): Enfermedad vascular cerebral sintomática, Diabetes tipo 2 Aneurisma de la aorta Insuficiencia arterial de miembros inferiores) Casos con 2 o más factores de riesgo con un riesgo absoluto mayor de 1% por año: Tabaquismo Hipertensión arterial (> o = 140/90) Colesterol HDL < 40 mg/dl Historia familiar de cardiopatía isquémica prematura (<55 en hombres y < 65 en mujeres) Edad (hombres > 45; mujeres > 55 años) JAMA 2001; 285:
: Enfermedad vascular cerebral sintomática, Diabetes tipo 2. Aneurisma de la aorta. Insuficiencia arterial de miembros inferiores) Casos con 2 o más factores de riesgo con un riesgo absoluto mayor de 1% por año: Tabaquismo. Hipertensión arterial (> o = 140/90) Colesterol HDL < 40 mg/dl. Historia familiar de cardiopatía isquémica prematura (<55 en hombres y < 65 en mujeres) Edad (hombres > 45; mujeres > 55 años) JAMA 2001; 285:")
5
Tratamiento hipolipemiante en México
Cardiopatía isquemica o equivalente= 7.4% Cardiopatía isquemica 1.3% Diabetes % 2 Factores de riesgo % Riesgo > 2% anual % Riesgo 1-2% anual 6.4% Riesgo <1% anual % Un factor de riesgo % Sin factores de riesgo % Modificación del estilo de vida 27.0% Tratamiento farmacológico 14.4%

6
Controversias en el tratamiento de las dislipidemias
Identificación de los mejores candidatos para recibir tratamiento: Diagnóstico etiológico de la dislipidemia Evaluación integral del paciente Responsabilidad social Se requieren de mejores pruebas para identificar sujetos en alto riesgo y de estudios longitudinales en población latinoamericana Componentes del perfil de lípidos a modificar

7
Colesterol No HDL = Colesterol – Colesterol HDL
Objetivos de tratamiento En pacientes con triglicéridos 200 mg/dL Colesterol LDL: objetivo primario Colesterol no HDL: objetivo secundario Colesterol No HDL = Colesterol – Colesterol HDL

8
El colesterol no-HDL es un predictor de mortalidad cardiovascular
Enf. coronaria OR p Cholesterol 1.04 <0.05 HDL-C LDL-C Non HDL-C 1.05 <0.05 TG BARI trial Circulation 2002;106: Diabetes tipo 2 Strong Heart Study Diabetes Care 2003;26:16-23

10
Dislipidemia del síndrome metabólico
El Colesterol-LDL es el objetivo primario de tratamiento Tratamiento de todas las anormalidades del perfil de lípidos Endocrine Practice 2003;9:

11
Controversias en el tratamiento de las dislipidemias
Identificación de los mejores candidatos para recibir tratamiento Elementos del perfil de lípidos a corregir: Corrección de todas las anormalidades presentes El colesterol LDL como meta primaria única es cuestionable Metas a alcanzar

13
Justificación para seleccionar la meta de colesterol LDL < 100 mg/dl

14
¿Cómo seleccionar los niveles óptimos de LDL-C?
Resultado de estudios controlados Estudio PROVE-IT

15
¿Cómo seleccionar los niveles óptimos de LDL-C?
TNT study Existieron 28 muertes no-cardiovasculares adicionales en el grupo de 80 mg NEJM 2005;352

16
¿Cómo seleccionar los niveles óptimos de LDL-C?
Estudio REVERSAL Tratamiento Tratamiento moderado intensivo Volumen de ateroma mm3 Basal ± ± 29 Final ± ±28* Delta ( %) -0.4 (-2.4 a 1.5%)* *p<0.05 JAMA 2004; 291:
 -0.4 (-2.4 a 1.5%)* *p<0.05. JAMA 2004; 291:")
17
¿Cómo seleccionar los niveles óptimos de LDL-C?
Juicio clínico Tratamiento intensivo - 22% Tratamiento habitual % Placebo

18
Controversias en el tratamiento de las dislipidemias
Identificación de los mejores candidatos para recibir tratamiento Elementos del perfil de lípidos considerados como metas de tratamiento Concentraciones de los lípidos séricos a alcanzar: Colesterol LDL 100 mg/dl, Colesterol no HDL 130 mg/dl Triglicéridos 150 mg/dl Colesterol HDL 40 mg/dl (46 mg/dl en mujeres) Instrumentos para alcanzar las metas
 Instrumentos para alcanzar las metas.")
19
Tratamiento de las dislipidemias
Educación + Dieta + Ejercicio + Suspensión del tabaquismo y/o alcoholismo + Eliminar medicamentos con efectos adversos en los lípidos séricos Fármacos hipolipemiantes Médico Nutriologo Paciente Educador Enfermera Familia

20
Hipertensión arterial
Pérdida de peso Lípidos séricos Glucemia Hipertensión arterial

21
Cambios en el estilo de vida para el tratamiento de la obesidad abdominal
Objetivo primario: -Crear un déficit de 500 calorias entre la ingesta de alimentos y la actividad física Objetivos intermedios: Identificar los alimentos con densidad calórica alta y sustituirlos Adquirir los conocimientos para saber combinar los alimentos Identificar los determinantes del apetito y de la alimentación Aumentar la actividad física. La meta es realizar un ejercico de poca intensidad y larga duración por 30 a 60 minutos al menos 5 días a la semana

22
CÁLCULO DIETO-TERAPÉUTICO

23
Alternativas ¨nuevas¨ en el tratamiento dietético
Recomendar el consumo de alimentos saludables en vez de prohibir Estimular el consumo de fibra, vegetales, fruta y cereales con alto contenido de fibra, pollo, pescado sustituyendo la ingesta de alimentos ricos en grasa saturada o azucares simples. Limitar el consumo de acidos grasos trans New options to lower LDL-C This slide shows additional options that can lower LDL-C in addition to a diet low in dietary cholesterol and saturated fatty acids. Reference: Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285: Expert Panel. JAMA 2001;285:
 Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285: Expert Panel. JAMA 2001;285:")
24
Ejercicio Favorece la pérdida de peso, disminuye el colesterol , los triglicéridos y aumenta el colesterol-HDL Debe ser isotónico; el ejercicio isométrico disminuye el colesterol-HDL Su inicio debe ser gradual El paciente debe recibir educación sobre sus beneficios, riesgos y la forma de realizarlo Reforzamiento en cada consulta

25
Tratamiento farmacológico de las dislipidemias.
Fármacos de primera elección: Fibratos Estatinas Tratamiento combinado: Estatinas más fibratos Estatinas más ezetimibe Estatinas más ácidos grasos omega 3 Alternativas experimentales

26
Fibratos Disminuyen: Aumentan: Modifican: Triglicéridos 20 - 60%
Colesterol-LDL % Aumentan: Colesterol-HDL % Modifican: La distribución de las subclases de las LDL disminuyendo las más aterogénicas (pequeñas y densas)
")
27
Efecto de los fibratos en hiperlipidemias mixtas
Aguilar-Salinas CA, Metabolism.2001; 50:

28
Efecto de los fibratos en hiperlipidemias mixtas
Aguilar-Salinas CA, Metabolism.2001; 50:

30
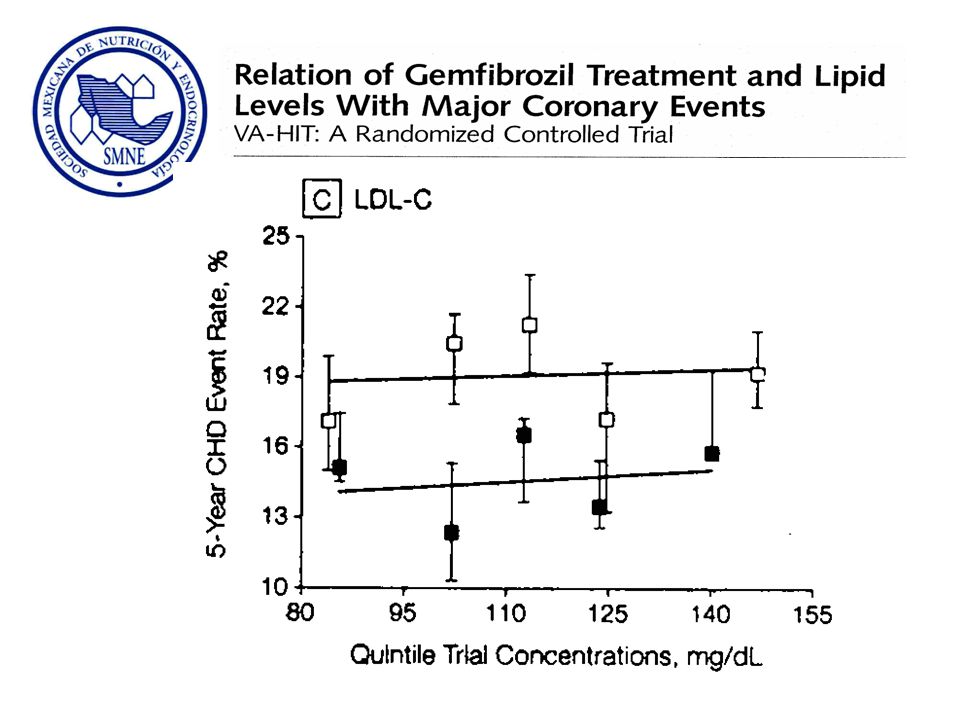
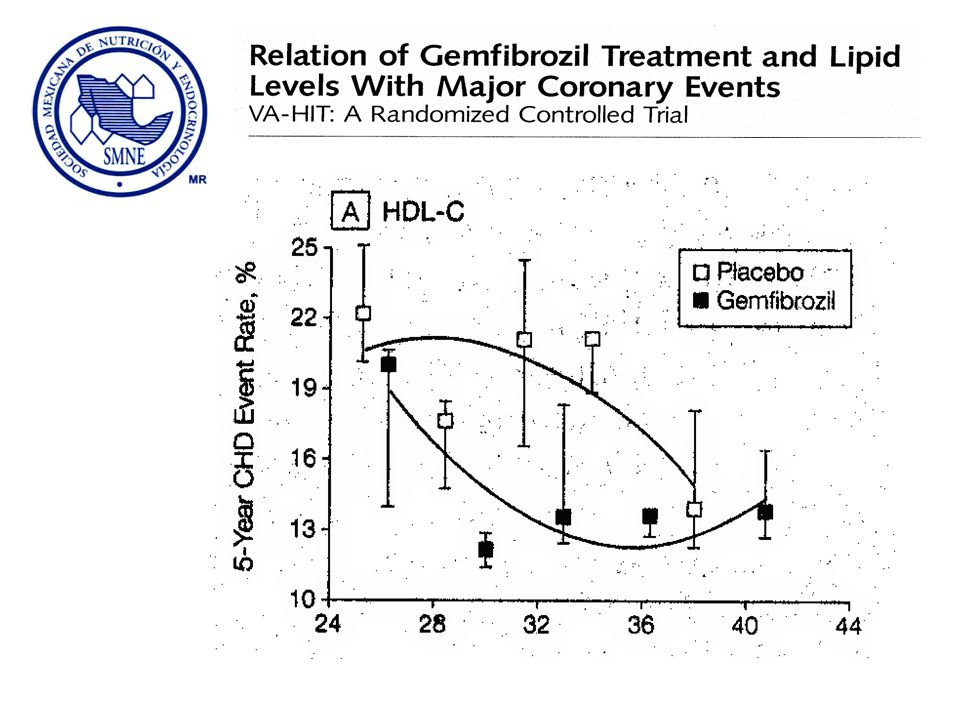
Nuevas evidencias obtenidas del Estudio VA-HIT
La respuesta al tratamiento depende del aumento del colesterol HDL. Por cada 5mg/dl de aumento disminuyeron 11% los eventos cardiovasculares. El tratamiento aumento el colesterol HDL-3 y redujo el colesterol HDL-2. El 77% del beneficio no fue explicado por los cambios en el perfil de lípidos.

31
Mecanismo de acción de los fibratos
↑Tamaño LDL ↓Triglyceridos This slide summarizes how fibrates act through PPARα to affect multiple aspects of lipid metabolism: decrease triglycerides, increase LDL particle size, increase HDL synthesis, and increase reverse cholesterol transport. Beyond the lipid profile effects, fibrates have also been shown to inhibit the expression of several inflammatory and atherogenic factors. The combined action of fibrates to correct atherogenic lipoprotein abnormalities and reduce inflammation may be especially beneficial at reducing CVD risk. References: Stone NJ, Blum CB. Management of Lipids in Clinical Practice. 5th ed Barbier O, et al. Arterioscler Thromb Vasc Biol. 2002;22: ↑Sintesis HDL ↓Inflamación PPARa ↑ Transporte reversa de colesterol

32
Outcomes in Fibrate Trials: Overall Study Populations
Major CVD Event Rate Trial N Control Drug Rel. RR P Primary Prevention HHS 4081 41.4% 27.3% 34% <.02 Secondary Prevention BIP 3090 15.0% 13.6% 9.4% .26 VA-HIT 2531 21.7% 17.3% 22% .006 Outcomes in Fibrate Trials: Overall Study Populations. HHS – Helsinki Heart study. A randomized double blind intervention in men with gemfibrozil or placebo. Observation on study lasted 5 years. Primary endpoint MI or CAD death. Rel. RR 34%. 1 BIP-Bezafibrate Infarction Prevention Study. A randomized double blind trial in men and women with bezafibrate or placebo. Observation on study lasted 6.2 years. Primary endpoint was fatal or nonfatal myocardial infarction or sudden death. Rel. RR 9.4%. 2 VA-HIT- High-Density Lipoprotein Cholesterol Intervention Trial. A randomized double blind trial in men with CHD with gemfibrozil or placebo.. Observation on study lasted 5.1 years. Primary endpoint was nonfatal myocardial infarction or death from coronary causes. RE. RR 22%. 3 Reference Rubins HB, et al. N Engl J Med. 1999;341: The BIP Study Group. Circulation. 2000;102:21-27. Frick MH, et al. N Engl J Med. 1987;317: Rel. RR indicates relative risk reduction Frick MH, et al. N Engl J Med. 1987;317: The BIP Study Group. Circulation. 2000;102:21-27. Rubins HB, et al. N Engl J Med. 1999;341:

33
Lipid-Lowering Therapy Lipid-Lowering Therapy
Lipid Effects Total Population Did Not Start Other Lipid-Lowering Therapy Started Other Lipid-Lowering Therapy Lipid Effects. The placebo patients experienced notable reductions in both total cholesterol and LDL-cholesterol, with fenofibrate treatment showing additional effects beyond those observed in the placebo patients. The reduction in LDL-C seen in the placebo patients, and a portion of the reduction observed in the fenofibrate patients, are likely due to the substantial proportion of patients who started statin therapy during the trial. Reference The FIELD Study Investigators. Lancet [Early Online Publication]. November 14, 2005. The FIELD Study Investigators. Lancet [Early Online Publication]. November 14, 2005.

34
Primary End Point 11% Reduction P=.16
Fenofibrate was associated with a nonsignificant, 11% reduction in the incidence of the primary end point, nonfatal MI, or CHD death (5.2% event rate for the fenofibrate group compared with 5.9% for the placebo group, P=.16). Reference The FIELD Study Investigators. Lancet [Early Online Publication]. November 14, 2005. The FIELD Study Investigators. Lancet [Early Online Publication]. November 14, 2005.
. Reference. The FIELD Study Investigators. Lancet [Early Online Publication]. November 14, The FIELD Study Investigators. Lancet [Early Online Publication]. November 14,")
35
Secondary End Point: Total CVD Risk
11% Reduction P=.035 Secondary End Point: Total CVD Risk. Fenofibrate significantly reduced the incidence of total cardiovascular events (11% reduction, P=.035). Reference The FIELD Study Investigators. Lancet [Early Online Publication]. November 14, 2005. The FIELD Study Investigators. Lancet [Early Online Publication]. November 14, 2005.
. Reference. The FIELD Study Investigators. Lancet [Early Online Publication]. November 14, The FIELD Study Investigators. Lancet [Early Online Publication]. November 14,")
36
Adjustment for Statin Use
Primary End Point: CHD Events Secondary End Point: Total CVD Events Adjustment for Statin Use. After adjustment for statin use, fenofibrate was associated with a significant improvement in the primary end point (19% reduction in CHD events, P=.01) and secondary end point (15% reduction in total CVD events, P=0.04). Reference The FIELD Study Investigators. Lancet [Early Online Publication]. November 14, 2005. P=.16 P=.01 P=.035 P=.004 Abbreviations: Adj, adjusted for statin use; Nonadj, nonadjusted risk The FIELD Study Investigators. Lancet [Early Online Publication]. November 14, 2005.
 and secondary end point (15% reduction in total CVD events, P=0.04). Reference. The FIELD Study Investigators. Lancet [Early Online Publication]. November 14, P=.16. P=.01. P=.035. P=.004. Abbreviations: Adj, adjusted for statin use; Nonadj, nonadjusted risk. The FIELD Study Investigators. Lancet [Early Online Publication]. November 14,")
37
Microvascular Disease
Laser Treatment for Retinopathy Progression of Albuminuria* P<.001 P=.002 Microvascular Disease. In addition to the beneficial effects on macrovascular disease, fenofibrate also significantly improved 2 indicators of microvascular disease. Patients treated with fenofibrate experienced lower rates of laser treatment for retinopathy and a reduced progression of albuminuria. Fenofibrate is the only lipid-lowering agent that has been shown to improve both macrovascular and microvascular disease in patients with type 2 diabetes. Reference The FIELD Study Investigators. Lancet [Early Online Publication]. November 14, 2005. Abbreviations: Feno, fenofibrate group; P, placebo group *Progression of albuminuria was defined as the proportion of patients who progressed either from normoalbuminuria to microalbuminuria or from microalbuminuria to macroalbuminuria The FIELD Study Investigators. Lancet [Early Online Publication]. November 14, 2005.

38
Clinically Important Adverse Events Occurring in <2% of Patients
Placebo n = 4900 Fenofibrate n = 4895 Newly diagnosed cancer 7.6% 8.0% Deep-vein thrombosis 1.0% 1.4% Pulmonary embolism 0.7% 1.1% Pancreatitis 0.5% 0.8% Myositis* 0.02% 0.04% Rhabdomyolysis† 0.06% Renal disease requiring dialysis 0.4% 0.3% ALT x ULN 0.2% >5x ULN CPK x ULN 0.1% >10x ULN 0.08% Creatinine increase >200 μmol/L 1.5% Clinically Important Adverse Events Occurring in <2% of Patients. Fenofibrate treatment was well tolerated. One of the important aspects of this study was the finding that even in a study conducted in almost patients, lasting 5 years, and in the presence of a significant proportion of patients taking fenofibrate plus statins, relatively few clinically significant muscle-related adverse events were observed. In particular, only 3 out of the 9795 patients experienced myositis. Notably, only 4 patients experienced rhabdomyolysis, which fully resolved after discontinuation of the study medication. Moreover, the incidences of alanine aminotransferase elevation and creatine phosphokinase elevation were not significantly different between placebo and fenofibrate treatment. Therefore, this study provides important corroborating evidence that fenofibrate therapy is safe, even when combined with statins. Reference The FIELD Study Investigators. Lancet [Early Online Publication]. November 14, 2005. *Myositis was experienced by 1 placebo and 2 fenofibrate patients †Rhabdomyolysis was experienced by 1 placebo and 3 fenofibrate patients Abbreviations: ALT, alanine aminotransferase, CPK, creatine phosphokinase, ULN, upper limit of normal The FIELD Study Investigators. Lancet [Early Online Publication]. November 14, 2005.

39
Outcomes in Fibrate Trials: Diabetic or Metabolic Syndrome
Major CVD Event Rate Trial N Control Drug Rel. RR P Primary Prevention HHS* 292 13.0% 3.9% 71% <.005 FIELD† 7664 10.8% 8.9% 19% .004 Secondary Prevention BIP‡ 1470 18.4% 14.1% 25% .03 VA-HIT§ 769 29.4% 21.2% 32% Outcomes in Fibrate Trials: Diabetic or Metabolic Syndrome. This table shows the outcomes of primary prevention in the FIELD trial along with the results of subanalyses of the other fibrate trials described earlier in this presentation. In FIELD, there was a significant 19% reduction (8.9% event rate for the fenofibrate group, compared with 10.8% event rate in the placebo group) in total cardiovascular disease events in patients with no prior cardiovascular disease (n=7664 or 78% of the total population). References 1. Manninen V, et al. Circulation. 1992;85:37-45. 2. Tenenbaum A, et al. Arch Intern Med. 2005;165: 3. Rubins HB, et al. Arch Intern Med. 2002;162: 4. The FIELD Study Investigators. Lancet [Early Online Publication]. November 14, 2005. Rel. RR indicates relative risk reduction *Patients with triglycerides >204 mg/dL and an LDL/HDL >5 †Patients with no prior CVD ‡ Patients with the metabolic syndrome; baseline HDL-C, 33 mg/dL; triglycerides, 170 mg/dL §Patients with diabetes; baseline HDL-C, 31 mg/dL; triglycerides, 164 mg/dL Manninen V, et al. Circulation. 1992;85:37-45. Tenenbaum A, et al. Arch Intern Med. 2005;165: Rubins HB, et al. Arch Intern Med. 2002;162: The FIELD Study Investigators. Lancet [Early Online Publication]. November 14, 2005.
 in total cardiovascular disease events in patients with no prior cardiovascular disease (n=7664 or 78% of the total population). References. 1. Manninen V, et al. Circulation. 1992;85: Tenenbaum A, et al. Arch Intern Med. 2005;165: Rubins HB, et al. Arch Intern Med. 2002;162: The FIELD Study Investigators. Lancet [Early Online Publication]. November 14, Rel. RR indicates relative risk reduction. *Patients with triglycerides >204 mg/dL and an LDL/HDL >5. †Patients with no prior CVD. ‡ Patients with the metabolic syndrome; baseline HDL-C, 33 mg/dL; triglycerides, 170 mg/dL. §Patients with diabetes; baseline HDL-C, 31 mg/dL; triglycerides, 164 mg/dL. Manninen V, et al. Circulation. 1992;85: Tenenbaum A, et al. Arch Intern Med. 2005;165: Rubins HB, et al. Arch Intern Med. 2002;162: The FIELD Study Investigators. Lancet [Early Online Publication]. November 14,")
40
Estatinas Disminuyen: Colesterol total 15- 55% Colesterol-LDL 20- 80%
Triglicéridos % Elevan: Colesterol-HDL % No modifican: Lp(a) Subclases de las LDL
 Subclases de las LDL.")
41
Colesterol total, colesterol-LDL, apo B
Hidroximetilglutaril- CoA Estatinas Hidroximetilglutaril CoA reductasa Mevalonato Menor síntesis intracelular de colesterol Aumento en el número de receptores-LDL Colesterol total, colesterol-LDL, apo B LDL

42
Mecanismo de acción de las estatinas
1. Inhibición de la secreción hepática de lipoproteínas 2. Disminución de la síntesis de las LDL al aumentar la remoción de sus precursores 3. Aumento de la elminación de las LDL 1 VLDL IDL 2 3 IDL LDL

43
Eficacia de las estatinas
Dosis/dia Atorvastatina Fluvastatina Lovastatina Pravastatina Simvastatina 10 mg –39% –22% –30% 20 mg –43% –27% –32% –38% 40 mg –50% –25% –34% –41% 80 mg –60% –36% –42% –47% The LDL-C–lowering efficacy of the currently available statins The relative LDL-C–lowering efficacy of the various statins is presented in this slide. This information was taken from the prescribing information in the 2001 Physicians' Desk Reference. While the data do not represent a head-to-head comparison in the same patient population, they do allow us to see the relative LDL-C–lowering potency of the currently available statins. These reductions are superior to those achieved by any other lipid-modifying agents. The LDL-C reductions are dose-dependent and log-linear. With each doubling of the dose, an additional 6–7% reduction in LDL-C is usually achieved. Changes in high-density lipoprotein cholesterol (HDL-C) are usually modest, in the 5–10% range, and not consistently dose related; increases in HDL-C are greater in patients with low HDL-C and elevated triglycerides. Reference: Physicians' desk reference. 55th ed. Montvale, NJ: Medical Economics Company, Inc., 2001. Physician’s Desk Reference. 55th ed. Montvale, NJ: Medical Economics, 2001.
 are usually modest, in the 5–10% range, and not consistently dose related; increases in HDL-C are greater in patients with low HDL-C and elevated triglycerides. Reference: Physicians desk reference. 55th ed. Montvale, NJ: Medical Economics Company, Inc., Physician’s Desk Reference. 55th ed. Montvale, NJ: Medical Economics,")
44
Directos: Indirectos: Efectos antiaterogénicos de las estatinas:
Por acción del fármaco Indirectos: Disminuyendo la concentración de un precursor en la síntesis de colesterol (Ubiquinona, dolicol, isoprenilación) Disminuyendo la concentración sérica de lipoproteinas aterogénicas
 Disminuyendo la concentración sérica de lipoproteinas aterogénicas.")
46
Ezetimibe: Inhibidor de la absorción de colesterol
Ezetemibe ??

47
Ezetimibe + Simvastatin: Efectos sobre el colesterol LDL
10 mg 20 mg 40 mg 80 mg EZE 10 mg + Simva 10 mg Mean % Change * p<0.01 combinación versus estatina Davidson M et al. ACC 2002: Abstract.

48
Adherencia al tratamiento a un año: pacientes post infarto
LDL Pre-CHAMP 1992–93 Post-CHAMP 1994–95 <100 mg/dl 6% 58% 100–130 mg/dl 15% 16% 130–160 mg/dl 18% 4% >160 mg/dl 14% 0% Sin seguimiento 48% 22% Results: adherence to NCEP treatment goals in patients 1 year post MI The adherence to NCEP treatment goals in patients 1 year after myocardial infarction pre-CHAMP and post-CHAMP are shown in this slide. As a result of CHAMP, there was a significant (almost 10-fold) improvement in the percentage of patients reaching an LDL-C of <100 mg/dl 1 year after hospital discharge (P<0.001). In the 1994–1995 time frame, this represents one of the best treatment rates reported in patients with documented CHD. This study demonstrates that in-hospital initiation of lipid-lowering medications results in more patients reaching their LDL-C goal as compared with conventional management. Reference: Fonarow GC, Gawlinski A, Moughrabi S, Tillisch JH. Improved treatment of coronary heart disease by implementation of a Cardiac Hospitalization Atherosclerosis Management Program: CHAMP. Am J Cardiol. 2001;87: Fonarow GC et al. Am J Cardiol 2001;87:
 improvement in the percentage of patients reaching an LDL-C of <100 mg/dl 1 year after hospital discharge (P<0.001). In the 1994–1995 time frame, this represents one of the best treatment rates reported in patients with documented CHD. This study demonstrates that in-hospital initiation of lipid-lowering medications results in more patients reaching their LDL-C goal as compared with conventional management. Reference: Fonarow GC, Gawlinski A, Moughrabi S, Tillisch JH. Improved treatment of coronary heart disease by implementation of a Cardiac Hospitalization Atherosclerosis Management Program: CHAMP. Am J Cardiol. 2001;87: Fonarow GC et al. Am J Cardiol 2001;87:")
49
Conclusiones VLDL VLDLR IDL HDL-3 HDL-2 LDL LDL densas
Colesterol no HDL Fibratos Modificaciones del estilo de vida HDL-3 HDL-2 LDL LDL densas Colesterol LDL Estatinas

Presentaciones similares





. Panel de expertos en detección, evaluación y tratamiento del colesterol alto.>")













