Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Dr. Gustavo Márquez Salom , MD, FACP (Hon)
Calcioantagonistas en el tratamiento de la hipertensión en pacientes con diabetes Dr. Gustavo Márquez Salom , MD, FACP (Hon) Profesor Especial, División de Lípidos y Diabetes, Universidad Nacional de Colombia Miembro Emérito de la Asociación Colombiana de Medicina Interna Miembro honorario de la Sociedad Colombiana de Cardiología Delegado de ALAD para Colombia Expresidente de la Federación Diabetológica Colombiana Expresidente de la Fundación Colombiana de Diabetes Presidente de ASOPIE
 Profesor Especial, División de Lípidos y Diabetes, Universidad Nacional de Colombia. Miembro Emérito de la Asociación Colombiana de Medicina Interna. Miembro honorario de la Sociedad Colombiana de Cardiología. Delegado de ALAD para Colombia. Expresidente de la Federación Diabetológica Colombiana. Expresidente de la Fundación Colombiana de Diabetes. Presidente de ASOPIE.")
2
Calcioantagonistas o bloqueadores de canales de calcio
Grupo heterogéneo de medicamentos con mecanismo de acción similar Diferencias farmacológicas importantes en cuanto a indicaciones, contraindicaciones e interacciones diferentes Potencia antihipertensiva diferente equivalente a dosis comparables Monoterapia: Se puede pero no se debe Terapia combinada con diurético previo o IECAs o ARA II (reducción de efectos secundarios)
")
3
Vías Comunes de Eliminación del Medicamento
CIRCULACION SISTEMICA Eliminado inalterado por los riñones CYP 450 OH Fase II Metabolismo Fase I Glucurónido Sulfato HIGADO Unas pocas drogas son conjugadas directamente (metabolismo fase II) sin ser primero biotransformados por las enzimas citocromo P 450. Los metabolitos resultantes de la Fase I, Fase II, o ambas, son usualmente farmacológicamente inactivos o por lo menos, menos activos. VENA PORTA A los riñones para eliminación Adaptado de Hansten. Science & Medicine. 1998;5:16-25.
 sin ser primero biotransformados por las enzimas citocromo P 450. Los metabolitos resultantes de la Fase I, Fase II, o ambas, son usualmente farmacológicamente inactivos o por lo menos, menos activos. VENA PORTA. A los riñones para eliminación. Adaptado de Hansten. Science & Medicine. 1998;5:")
4
Interacciones medicamentosas
Atorvastatina Cerivastatina Lovastatina Simvastatina CYP 450 3A4 2D6 Reacciones adversas Ketoconazol Eritromicina Diltiazem Mibefradil Itraconazol Fibratos Muchos medicamentos comúnmente prescritos inhiben significativamente el sistema citocromo P 450 3A4. Esto puede incrementar las concentraciones en plasma de atorvastatina, cerivastatina, lovastatina y simvastatina, aumentando la posibilidad de reacciones adversas a medicamentos, tales como mialgia y rabdomiólisis. NOTA: Las siguientes combinaciones han resultado en rabdomiólisis: Lovastatina e itraconazol1 Simvastatina y ciclosporina5 Lovastatina y eritromicina2 Simvastatina y nefazodone6,7 Lovastatina y ciclosporina3 Simvastatina e itraconazol8 Lovastatina y diltiazem4 Simvastatina y mibefradil9 Las siguientes combinaciones han dado como resultado niveles aumentados en plasma de atorvastatina: Atorvastatina y eritromicina10 Atorvastatina e itraconazol11 1. Lees RS et al. N Engl J Med 1995;333: Ballantyne CM et al. J Am Coll Cardiol 1992; 19: Corpier CL. JAMA 1988;260(2): Ahmad S. Am Heart J 1993;126: Meier C et al. Schweiz Med Wochen 1995;125: Jacobson RH et al. JAMA 1997;277: Jody DN. JAMA 1997;277: Segaert MF et al. Reactions 1996;622: FDA report Yang B-B, et al. Pharm Res 1996;13:S Data on file. BMS. * 1. Lees RS et al. N Engl J Med 1995;333: Ballantyne CM et al. J Am Coll Cardiol 1992; 19: Corpier CL. JAMA 1988;260(2): Ahmad S. Am Heart J 1993;126: Meier C et al. Schweiz Med Wochen 1995;125: Jacobson RH et al. JAMA 1997;277: Jody DN. JAMA 1997;277: Segaert MF et al. Reactions 1996;622: FDA report 1997.
: Ahmad S. Am Heart J 1993;126: Meier C et al. Schweiz Med Wochen 1995;125: Jacobson RH et al. JAMA 1997;277: Jody DN. JAMA 1997;277: Segaert MF et al. Reactions 1996;622: FDA report Yang B-B, et al. Pharm Res 1996;13:S Data on file. BMS. * 1. Lees RS et al. N Engl J Med 1995;333: Ballantyne CM et al. J Am Coll Cardiol 1992; 19: Corpier CL. JAMA 1988;260(2): Ahmad S. Am Heart J 1993;126: Meier C et al. Schweiz Med Wochen 1995;125: Jacobson RH et al. JAMA 1997;277: Jody DN. JAMA 1997;277: Segaert MF et al. Reactions 1996;622: FDA report")
5
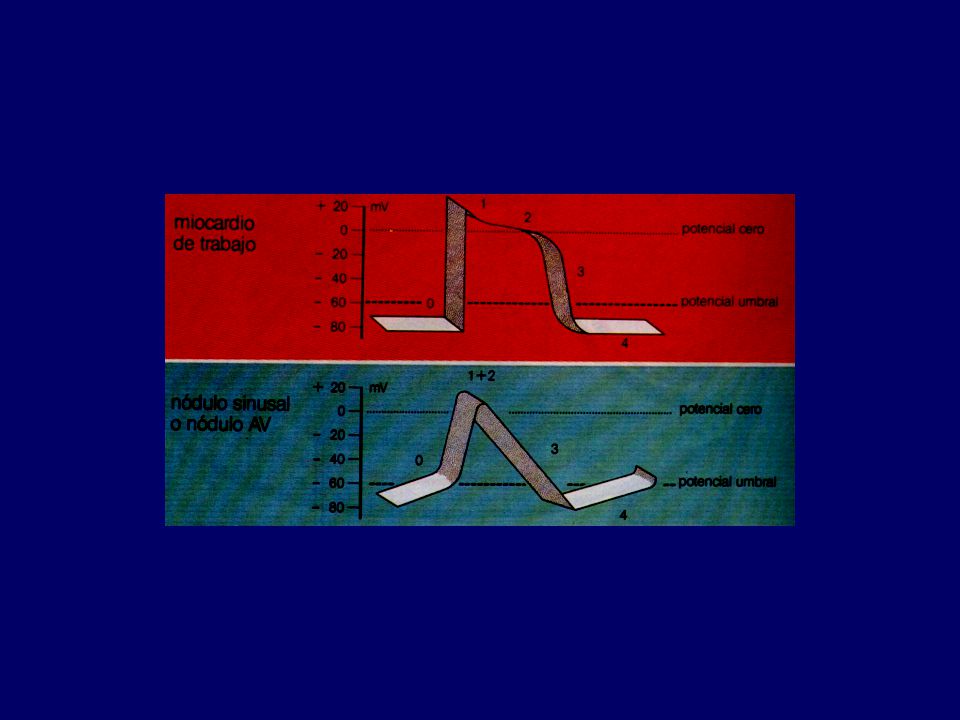
Ingreso de calcio por sistema transverso tubular en cuya profundidad se encuentran la mayoría de canales lentos que lo conducen al interior de las fibras, originando contracción.

6
Vasorelajación medidada por bloqueo de canales de Calcio Tipo L

7
Receptores de Canales tipo L
Bloqueo de receptor dihidropiridínico: Nifedipina, nisoldipino, nimodipino, felodipino, amlodipino, isradipino, nicardipino, nitrendipino, lacidipino,lercanidipino, manidipino Bloqueo de receptor fenilalquilamínico: Verapamilo, gallopamilo Bloqueo de receptor benzotiazepínico: Diltiazem CLASIFICACION FUNCIONAL: DIHIDROPIRIDINICOS NO DIHIDROPIRIDINICOS

8
Características Agentes antihipertensivos potentes, dosis dependiente.
Eficaces en cualquier rango de ingestión de sal Seguridad establecida por estudios clínicos con los BCC de acción prolongada Efecto metabólico neutro. Utilidad en tratamiento de pacientes con hiperglucemia, SM o IR y dislipidemia Menor protección en riesgo de infarto miocárdico e I.C.C

9
Preferencias Ancianos mayores de 55 años (con diuréticos)
Evitar en monoterapia en pacientes diabéticos En diabéticos - terapia combinada necesaria si hay proteinuria o disfunción renal Efecto metabólico neutro. Utilidad en tratamiento de pacientes con hiperglucemia, SM o IR y dislipidemia Raza negra Hipertensión sistólica aislada Prevención de enfermedad cerebro-vascular

10
Algorithm for Treatment of Hypertension
Lifestyle Modifications Not at Goal Blood Pressure (<140/90 mmHg) (<130/80 mmHg for those with diabetes or chronic kidney disease) Initial Drug Choices Stage 2 Hypertension (SBP >160 or DBP >100 mmHg) 2-drug combination for most (usually thiazide-type diuretic and ACEI, or ARB, or BB, or CCB) Stage 1 Hypertension (SBP 140–159 or DBP 90–99 mmHg) Thiazide-type diuretics for most. May consider ACEI, ARB, BB, CCB, or combination. Without Compelling Indications Drug(s) for the compelling indications Other antihypertensive drugs (diuretics, ACEI, ARB, BB, CCB) as needed. With Compelling Indications Not at Goal Blood Pressure Optimize dosages or add additional drugs until goal blood pressure is achieved. Consider consultation with hypertension specialist.
 (<130/80 mmHg for those with diabetes or chronic kidney disease) Initial Drug Choices. Stage 2 Hypertension (SBP >160 or DBP >100 mmHg) 2-drug combination for most (usually thiazide-type diuretic and ACEI, or ARB, or BB, or CCB) Stage 1 Hypertension (SBP 140–159 or DBP 90–99 mmHg) Thiazide-type diuretics for most. May consider ACEI, ARB, BB, CCB, or combination. Without Compelling Indications. Drug(s) for the compelling indications. Other antihypertensive drugs (diuretics, ACEI, ARB, BB, CCB) as needed. With Compelling Indications. Not at Goal Blood Pressure. Optimize dosages or add additional drugs until goal blood pressure is achieved. Consider consultation with hypertension specialist.")
11
Compelling Indications for Individual Drug Classes
Initial Therapy Options Clinical Trial Basis Diabetes Chronic kidney disease Recurrent stroke prevention THIAZ, BB, ACE, ARB, CCB ACEI, ARB THIAZ, ACEI NKF-ADA Guideline, UKPDS, ALLHAT NKF Guideline, Captopril Trial, RENAAL, IDNT, REIN, AASK PROGRESS

12
Compelling Indications for Individual Drug Classes
Initial Therapy Options Clinical Trial Basis Heart failure Postmyocardial infarction High CAD risk THIAZ, BB, ACEI, ARB, ALDO ANT. BB, ACEI, ALDO ANT THIAZ, BB, ACEI, CCB ACC/AHA Heart Failure Guideline, MERIT- HF, COPERNICUS, CIBIS, SOLVD, AIRE, TRACE, ValHEFT, RALES ACC/AHA Post-MI Guideline, BHAT, SAVE, Capricorn, EPHESUS ALLHAT, HOPE, ANBP2, LIFE, CONVINCE

13
CALCIOANTAGONISTAS DIHIDROPIRIDINICOS
ADMINISTRACION AGUDA Corazón ↓ TA CAIDA DE R.V.S TAQUICARDIA REFLEJA AUMENTO DEL GASTO CARDIACO Los bloqueadores de los canales del calcio de corta acción conducen a una activación neuro-hormonal refleja del sistema nervioso simpático, caracterizada por taquicardia e incremento del gasto cardíaco ,de las catecolaminas plasmáticas y de actividad de la renina plasmática. Abernethy DR. Pharmacologic and pharmacokinetic profile of mibefradil, aT- and L-type calcium channel antagonist. Am J Cardiol 1997; 80: 4C-11C. Weiner DA. Calcium channel blockers. Med Clin North Am 1988; 72:

14
CALCIOANTAGONISTAS DIHIDROPIRIDINICOS
USO CRONICO Corazón ↓ TA CAIDA DE R.V.S FC REGRESA A N.P.T VOLUMEN DE EXPULSION REGRESA A N.P.T GASTO CARDIACO REGRESA A N.P.T

15
CALCIOANTAGONISTAS NO DIHIDROPIRIDINICOS
USO CRONICO Corazón ↓ TA PEQUEÑA REDUCCION DEL GASTO CARDIACO EN REPOSO Y CON EL EJERCICIO AUMENTO COMPENSATORIO DEL VOLUMEN DE EXPULSION Tienen efecto inotrópico negativo por lo cual están contraindicados en paciente con I.C.C

16
BCC de larga duración Resultados no extrapolables a los de acción corta ALLHAT E INSIGHT entre otros Estudios Clínicos apoyan el uso de BCC dihidropiridínicos de larga duración y una dosis diaria en el tratamiento de la hipertensión arterial No se recomienda BCC de acción corta en el tratamiento agudo o crónico de pacientes hipertensos

17
CALCIOANTAGONISTAS Y CIRCULACION CORONARIA
REDUCEN DEMANDA DE 02 POR EL MIOCARDIO REDUCEN POSTCARGA REDUCEN TRABAJO CARDIACO AUMENTAN FLUJO CORONARIO EN MIOCARDIO ISQUEMICO DURANTE OCLUSION NO AFECTAN PRECARGA NO ALTERAN RETORNO VENOSO

19
Efectos antiarrítmicos de las fenilalquilaminas
Descienden la frecuencia cardíaca Protege de alteraciones SV paroxísticas y taquicárdicas Desciende la frecuencia cardíaca en taquiarritmia absoluta Impide taquicardia refleja consecuente a vasodilatación PRA

20
CALCIOANTAGONISTAS Y CIRCULACION CEREBRAL
LOS DIHIDROPIRIDINICOS AUMENTAN MARCADAMENTE EL FLUJO CEREBRAL. LOS NO DIHIDROPIRIDINICOS TIENEN EFECTO MENOR. PROTECCION NEURONAL DURANTE ISQUEMIA PREVIENEN VASOESPASMO CEREBRAL

21
CALCIOANTAGONISTAS EFECTOS RENALES
DILATACION ARTERIOLAR AFERENTE MAYOR CON DIHIDROPIRIDINICOS CAMBIOS EN LA HEMODINAMIA INTRARRENAL AUMENTO DEL FLUJO PLASMATICO RENAL MODIFICACION DE LA TFG (↑) EFECTO DIURETICO Y NATRIURETICO EFECTOS SEGÚN TONO VASCULAR PREVIO
 EFECTO DIURETICO Y NATRIURETICO. EFECTOS SEGÚN TONO VASCULAR PREVIO.")
22
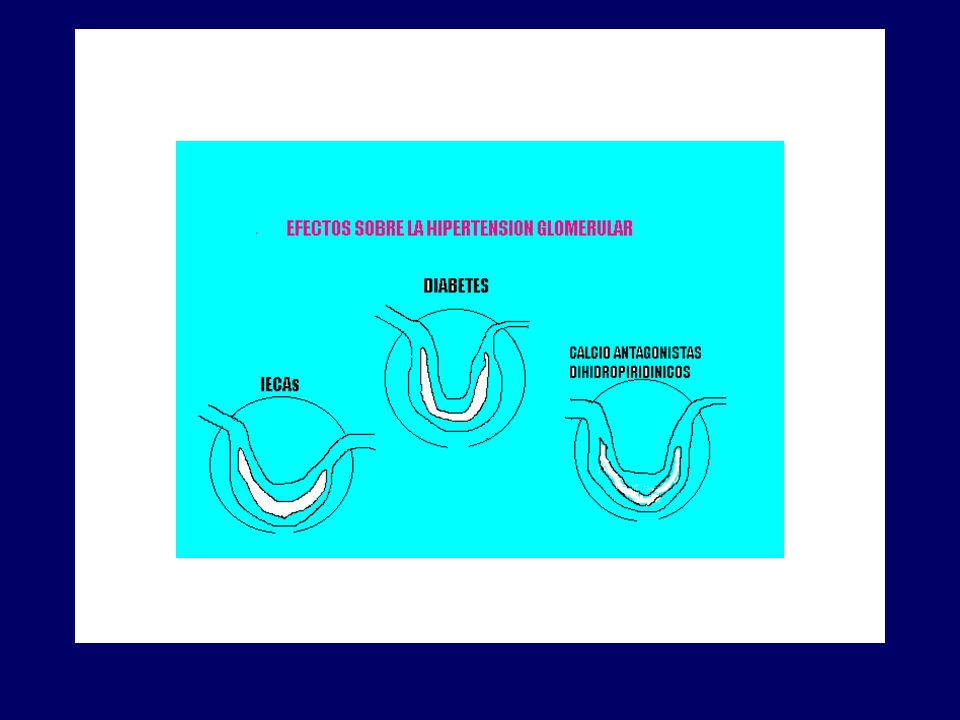
Dilatación mayor de arteriola aferente por CA dihidropiridínicos
Lercanidipino y manidipino efecto balanceado en arteriolas aferentes y eferentes Sabbatini, et al. Effect of calcium antagonists on glomerular arterioles in spontaneously hypertensive rats. Hypertension 2000; 35:

24
ACE Inhibitors vs. Other Antihypertensives
in Patients with Type 2 Diabetes and Proteinuria (CCB) (BB) Non-ACE inhibitor ACE inhibitor Proteinuria 4.1 3.0 3 ACE inhibitor vs conventional therapy Walker et al (n=86) 9.6 6.4 Lebovitz et al (n=46) 1.4 (CCB) 3.3 (BB) 1.0 5 CCB vs beta blocker Bakris et al (n=52) 6.5 7.0 ACE inhibitor vs beta blocker Nielsen et al (n=36) 5.5 ACE inhibitor vs CCB Estacio et al (n=83) 1.2 2.0 2 Fogari et al (n=51) Decline in GFR (ml/min/yr) Follow-up (y) Treatment Investigator Antihypertensive treatment slows the rate of declining renal function in patients with diabetic nephropathy,1,2,3,4 although it remains unclear whether one antihypertensive class provides better renal protection than another. Large, long-term, double-blind, randomized comparison trials are needed to determine which is more important, the degree of blood pressure reduction or the class of antihypertensive agent used. In a meta-analysis of 100 trials, the relative effect of different antihypertensive agents on proteinuria and renal function was assessed in patients with diabetes.3 Compared with other antihypertensive agents, ACE inhibitors demonstrated the greatest reductions in urinary albumin excretion, while ACE inhibitors and calcium channel blockers (CCBs) appeared to have the greatest benefits on glomerular filtration rate (GFR). However, a second meta-analysis suggested that at maximal antihypertensive doses, there was no significant difference between the antiproteinuric effects of ACE inhibitors and those of other antihypertensive drugs.5 Most of the published comparative studies are of short duration (only one year or less), and several are open-label and included only small numbers of patients or heterogeneous groups of type 1 and type 2 diabetic patients. Completed studies thus show conflicting results, with ACE inhibitors demonstrating greater effects on proteinuria and the rate of decline in kidney function in some studies,4,6,7 while other studies demonstrate no differences between ACE inhibitors and other classes of antihypertensive agents on proteinuria 8 or on the rate of decline of GFR.7,9,10,11,12 As shown in the table above, six randomized double-blind studies have been performed comparing ACE inhibition with non-ACE inhibition in type 2 diabetic patients with nephropathy.13 All the studies demonstrate a beneficial effect of blood pressure reduction on both albuminuria and the rate of decline in GFR. However, ACE inhibitors were not demonstrated to be superior to non-ACE agents in these patients. Except for one study, no significant differences were found between the decline in GFR in patients treated with and without ACE inhibitors. Large, long-term, double-blind, randomized comparison trials are needed to determine which is more important, the degree of blood pressure reduction or the class of antihypertensive agent used. 1 Lewis et al, Bjorck et al, Nielsen et al, 1997. 2 Parving et al, Bakris et al, Estacio et al, 2000. 3 Kasiske et al, Melbourne Diabetic Nephropathy Study Group, 1991. 4 Ismail et al, Lacourciere et al, Parving, 2001b. 5 Weidmann et al, Velussi et al, 1996. Parving H-H et al. Curr Opin Nephrol Hypertens 2001;10:
 (BB) Non-ACE inhibitor. ACE inhibitor. Proteinuria ACE inhibitor vs. conventional therapy. Walker et al. (n=86) Lebovitz et al. (n=46) 1.4 (CCB) 3.3 (BB) CCB vs beta blocker. Bakris et al. (n=52) ACE inhibitor vs beta blocker. Nielsen et al. (n=36) 5.5. ACE inhibitor vs CCB. Estacio et al. (n=83) Fogari et al. (n=51) Decline in GFR (ml/min/yr) Follow-up (y) Treatment. Investigator. Antihypertensive treatment slows the rate of declining renal function in patients with diabetic nephropathy,1,2,3,4 although it remains unclear whether one antihypertensive class provides better renal protection than another. Large, long-term, double-blind, randomized comparison trials are needed to determine which is more important, the degree of blood pressure reduction or the class of antihypertensive agent used. In a meta-analysis of 100 trials, the relative effect of different antihypertensive agents on proteinuria and renal function was assessed in patients with diabetes.3 Compared with other antihypertensive agents, ACE inhibitors demonstrated the greatest reductions in urinary albumin excretion, while ACE inhibitors and calcium channel blockers (CCBs) appeared to have the greatest benefits on glomerular filtration rate (GFR). However, a second meta-analysis suggested that at maximal antihypertensive doses, there was no significant difference between the antiproteinuric effects of ACE inhibitors and those of other antihypertensive drugs.5 Most of the published comparative studies are of short duration (only one year or less), and several are open-label and included only small numbers of patients or heterogeneous groups of type 1 and type 2 diabetic patients. Completed studies thus show conflicting results, with ACE inhibitors demonstrating greater effects on proteinuria and the rate of decline in kidney function in some studies,4,6,7 while other studies demonstrate no differences between ACE inhibitors and other classes of antihypertensive agents on proteinuria 8 or on the rate of decline of GFR.7,9,10,11,12. As shown in the table above, six randomized double-blind studies have been performed comparing ACE inhibition with non-ACE inhibition in type 2 diabetic patients with nephropathy.13 All the studies demonstrate a beneficial effect of blood pressure reduction on both albuminuria and the rate of decline in GFR. However, ACE inhibitors were not demonstrated to be superior to non-ACE agents in these patients. Except for one study, no significant differences were found between the decline in GFR in patients treated with and without ACE inhibitors. Large, long-term, double-blind, randomized comparison trials are needed to determine which is more important, the degree of blood pressure reduction or the class of antihypertensive agent used. 1 Lewis et al, Bjorck et al, Nielsen et al, Parving et al, Bakris et al, Estacio et al, Kasiske et al, Melbourne Diabetic Nephropathy Study Group, Ismail et al, Lacourciere et al, Parving, 2001b. 5 Weidmann et al, Velussi et al, Parving H-H et al. Curr Opin Nephrol Hypertens 2001;10:")
25
PREVINIENDO MICROALBUMINURIA EN DIABETES TIPO 2
Ruggenenti P, Fassi A, et al. for the Bergamo Nephrologic Diabetes Complications (BENEDICT) Investigators. N.Engl. J. Med 2004; 351:
 Investigators. N.Engl. J. Med 2004; 351:")
26
PREVINIENDO MICROALBUMINURIA EN DIABETES TIPO 2
Ruggenenti P, Fassi A, et al. for the Bergamo Nephrologic Diabetes Complications (BENEDICT) Investigators. N.Engl. J. Med 2004; 351:
 Investigators. N.Engl. J. Med 2004; 351:")
27
Ruggenenti P, Fassi A, et al
Ruggenenti P, Fassi A, et al. for the Bergamo Nephrologic Diabetes Complications (BENEDICT) Investigators. N.Engl. J. Med 2004; 351:
 Investigators. N.Engl. J. Med 2004; 351:")
28
Estudio IDNT- Irbesartan Tiempo para doblar creatinina
N Engl J Med 2001;345: Sujetos (%) 6 12 18 24 30 36 42 48 54 meses 60 10 20 40 50 70 Irbesartan Amlodipino Control RRR 33% P=0.003 P=NS RRR 37% P<0.001 Patients assigned to the irbesartan group had a 33% reduction in the risk of doubling of baseline serum creatinine vs. the control group (placebo in addition to other nonexcluded antihypertensive therapies), p=0.003, and a 37% RRR vs. the amlodipine group, p< 1 Lewis et al, 2001.
 meses Irbesartan. Amlodipino. Control. RRR 33% P= P=NS. RRR 37% P< Patients assigned to the irbesartan group had a 33% reduction in the risk of doubling of baseline serum creatinine vs. the control group (placebo in addition to other nonexcluded antihypertensive therapies), p=0.003, and a 37% RRR vs. the amlodipine group, p< Lewis et al,")
29
IDNT Tiempo para llegar a estado final de ERC
40 Irbesartan Control + amlodipine RRR 23% P=0.04 30 Subjects (%) Subjects (%) 20 Compared with the control and amlodipine groups combined, irbesartan significantly reduced the risk of ESRD by 23% (p=0.04). There was a 23% reduction of the risk of ESRD (p=0.07) when patients receiving irbesartan were compared with those in either the amlodipine or control group (placebo in addition to other nonexcluded antihypertensive therapies).1 Since the control and amlodipine groups did not differ significantly in the composite primary endpoint or in the risk of doubling of serum creatinine or developing ESRD, irbesartan was compared with these two non-renin-angiotensin system-blocking groups combined. Compared with the control and amlodipine groups combined, irbesartan significantly reduced the risk of ESRD by 23% (p=0.04).2 1 Lewis et al, 2001. 2 Data on file, Bristol-Myers Squibb and Sanofi-Synthelabo. 10 6 12 18 24 30 36 42 48 54 60 Follow-up (mo) Data on file, Bristol-Myers Squibb and Sanofi-Synthelabo.
 Subjects. (%) 20. Compared with the control and amlodipine groups combined, irbesartan significantly reduced the risk of ESRD by 23% (p=0.04). There was a 23% reduction of the risk of ESRD (p=0.07) when patients receiving irbesartan were compared with those in either the amlodipine or control group (placebo in addition to other nonexcluded antihypertensive therapies).1 Since the control and amlodipine groups did not differ significantly in the composite primary endpoint or in the risk of doubling of serum creatinine or developing ESRD, irbesartan was compared with these two non-renin-angiotensin system-blocking groups combined. Compared with the control and amlodipine groups combined, irbesartan significantly reduced the risk of ESRD by 23% (p=0.04).2. 1 Lewis et al, Data on file, Bristol-Myers Squibb and Sanofi-Synthelabo Follow-up (mo) Data on file, Bristol-Myers Squibb and Sanofi-Synthelabo.")
30
"Por lo tanto, no se debe recomendar monoterapia con un bloqueador de los canales del calcio dihidropiridínico en el diabético hipertenso con microalbuminuria o reducción de la tasa de filtración glomerular" “ Hay sugerencia reciente de que verapamilo, siendo un bloqueador de los canales del calcio no dihidropiridínico, es incapaz de prevenir microalbuminuria en diabéticos tipo 2 hipertensos, por lo que tampoco debe usarse como monoterapia"

31
CALCIOANTAGONISTAS PROTECCION ORGANICA
● REDUCEN HVI ● EJERCEN ACCION ANTIANGINOSA ● ACCION ANTIESPASTICA CORONARIA ● UTILES EN ECV ● MENOR DESARROLLO DE ATEROSCLEROSIS ● NEFROPROTECCION ● LIBRES DE CAMBIOS METABOLICOS ADVERSOS ● NO PROPICIAN INSULINO - RESISTENCIA

32
CALCIOANTAGONISTAS CONTRAINDICACIONES
● USO COMBINANDO CON BETABLOQUEADORES ● DISFUNCION SISTOLICA VI ● SINDROME DEL SENO ENFERMO ● BLOQUEOS A-V DE 2o. Y 3o. GRADOS

33
Eficacia de la terapia antihipertensiva de primera línea en estudios comparativos
Medicamento Disminución desde La presión basal en mm Hg Diferencia ( 99% CI) Tiazidas v. ß--bloqueadores Tiazidas ß - bloqueador -26.6 -24.3 -2.3* (-3.1 to - 1.5) (-0.8 to 0.3) (-0.9 to 1.4) 6.0* (3.7 to 8.3) 3.0* (1.2 to 4.8) -0.2* (-3.6 to - 0.3) -25.1 -15.5 -15.2 -23.0 -29.0 -23.1 -13.0 -16.0 B. CC Tiazidas v. B. De CC Inhibidores ECA v. B. CC Inhibidores ECA Sistólica Diastólica *p<0.01, al comparar con 0. En un meta-análisis reciente sobre la eficacia antihipertensiva de los grupos utilizados como primer paso farmacológico se pudo apreciar: 1. La efectividad de los grupos farmacológicos es diferente 2. Las tiazidas son el grupo más efectivo para reducir la presión sistólica comparativamente con b-bloqueadores, calcioantagonistas e IECA’s 3. No se aprecia ninguna diferencia entre tiazida,b-bloqueador y calcioantagonistas en sus efectos para reducir la presión diastólica, mientras que los IECAS producen la menor reducción. Wright JM, JAMC 1999; 161: 25-32
 Tiazidas v. ß--bloqueadores. Tiazidas. ß - bloqueador * (-3.1 to - 1.5) -0.2 (-0.8 to 0.3) -0.2 (-0.9 to 1.4) 6.0* (3.7 to 8.3) 3.0* (1.2 to 4.8) -0.2* (-3.6 to - 0.3) B. CC. Tiazidas v. B. De CC. Inhibidores ECA v. B. CC. Inhibidores ECA. Sistólica. Diastólica. *p<0.01, al comparar con 0. En un meta-análisis reciente sobre la eficacia antihipertensiva de los grupos utilizados como primer paso farmacológico se pudo apreciar: 1. La efectividad de los grupos farmacológicos es diferente. 2. Las tiazidas son el grupo más efectivo para reducir la presión sistólica comparativamente con b-bloqueadores, calcioantagonistas e IECA’s. 3. No se aprecia ninguna diferencia entre tiazida,b-bloqueador y calcioantagonistas en sus efectos para reducir la presión diastólica, mientras que los IECAS producen la menor reducción. Wright JM, JAMC 1999; 161:")
34
Riesgo relativo de eventos CV y mortalidad Calcioantagonistas (BCCs) vs. placebo
Nº de eventos* BCCs (n=2.815) Placebo (n=2.705) Riesgo relativo (95% IC) Acc. Isqu. Cerebr. (Ictus) ,61 (0,44–0,85) Enfermedad coronaria ,79 (0,59–1,06) Insuficiencia cardíaca ,72 (0,48–1,07) Eventos CV mayores ,72 (0,59–0,87) Muerte CV ,72 (0,52–0,98) Mortalidad total ,87 (0,70–1,09) 0,5 1,0 2,0 Riesgo relativo A favor de BCCs A favor de placebo * Se incluyen PREVENT y Syst-Eur. Los rombos representan la suma de todos los efectos estimados de acuerdo a un IC del 95% y se centran en el promedio del riesgo relativo. Blood Pressure Lowering Treatment Trialists’ Collaboration. Lancet. 2000; 356: 22
 Placebo (n=2.705) Riesgo relativo (95% IC) Acc. Isqu. Cerebr. (Ictus) ,61 (0,44–0,85) Enfermedad coronaria ,79 (0,59–1,06) Insuficiencia cardíaca ,72 (0,48–1,07) Eventos CV mayores ,72 (0,59–0,87) Muerte CV ,72 (0,52–0,98) Mortalidad total ,87 (0,70–1,09) 0,5. 1,0. 2,0. Riesgo relativo. A favor de BCCs. A favor de placebo. * Se incluyen PREVENT y Syst-Eur. Los rombos representan la suma de todos los efectos estimados de acuerdo a un IC del 95% y se centran en el promedio del riesgo relativo. Blood Pressure Lowering Treatment Trialists’ Collaboration. Lancet. 2000; 356:")
36
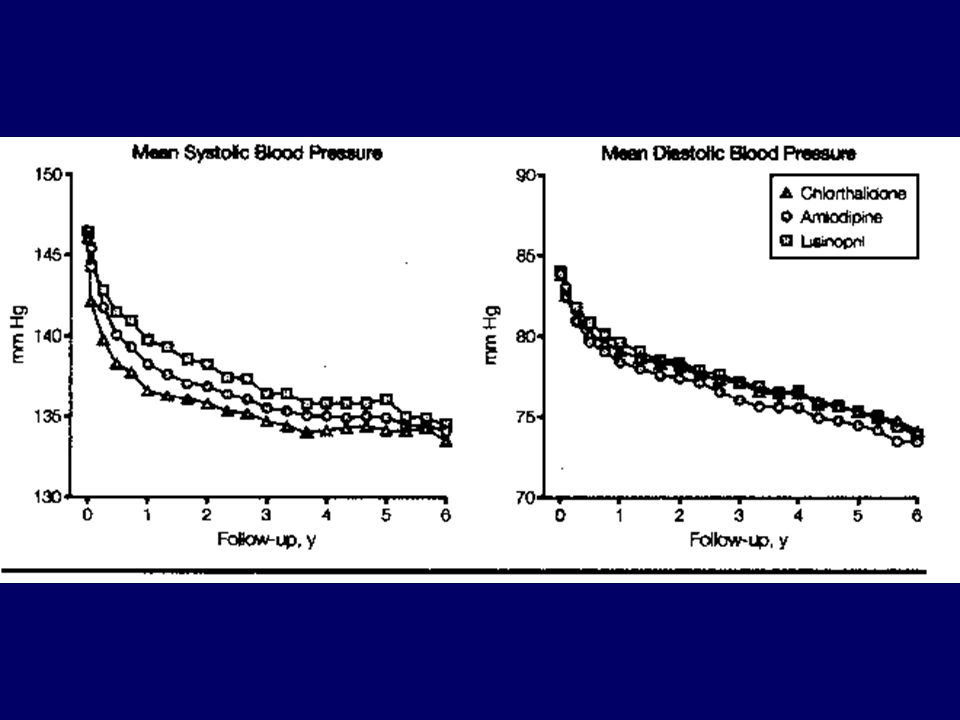
Enfermedad coronaria fatal o IM no fatal: No hubo diferencia entre Amlodipino (0.98;95%: ;p=0.65) o Lisinopril Vs Clortalidona
 o Lisinopril Vs Clortalidona")
37
Meta-análisis. Staessen and Wang J. Hypertens. 2003; 21: 1055-1076
9 estudios con pacientes randomizados comparando CALCIOANTAGONISTAS Vs ANTIHIPERTENSIVOS TRADICIONALES hasta Marzo 1/ 2003 No hubo diferencias en todas las causas de mortalidad CV total, todos los eventos CV, ACV, IM e ICC. Mortalidad total: 0.98, 95% ( , P = 0.42) Para ACV: Alcanzó significancia estadística a favor de CALCIOANTAGONISTAS, al excluir estudio CONVINCE (0.90, 95% ,P = 0.02) Los CALCIOANTAGONISTAS dieron la menor protección contra falla cardíaca incluyendo o excluyendo al CONVINCE*. *Controlled Onset Verapamil Investigation of Cardiovascular Endpoints (CONVINCE) JAMA 2003; 289:
 Para ACV: Alcanzó significancia estadística a favor de CALCIOANTAGONISTAS, al excluir estudio CONVINCE (0.90, 95% ,P = 0.02) Los CALCIOANTAGONISTAS dieron la menor protección contra falla cardíaca incluyendo o excluyendo al CONVINCE*. *Controlled Onset Verapamil Investigation of Cardiovascular Endpoints (CONVINCE) JAMA 2003; 289:")
38
CONDICIONES QUE FAVORECEN EL USO DE CALCIOANTAGONISTAS
DIHIDROPIRIDINAS Pacientes ancianos Hipertensión sistólica aislada Angina de pecho Enfermedad vascular periférica Aterosclerosis carotídea Embarazo Diabetes VERAPAMILO, DILTIAZEM Angina de pecho, alto riesgo de enfermed coronaria Aterosclerosis carotídea Taquicardia supraventricular

39
Otros efectos indeseables frecuentes
Edema pedal Rubor Cefalea Mareo Constipación

40
Curso de patologías del pie 9 de Abril / Centro Médico Almirante Colón- Club de Bridge Gratuito…! Talleres interactivos durante la mañana Panel de Expertos por la tarde Informes e inscripciones:: Tels y

41
G R A C I A S Informes e inscripciones:: Tels y

Presentaciones similares