Descargar la presentación
La descarga está en progreso. Por favor, espere

1
DROGAS que RETARDAN la COAGULACION
ANTI-COAGULANTES o ANTI-HEMOSTATICAS Antiplaquetarios, 2. Heparinas, HBPM y heparinoides, y 3. Anticoagulantes Orales

2
En Px y Tx de trombos arteriales y venosos
En Px y Tx de trombos arteriales y venosos. Circulacion extracorporea, dialisis.

4
DROGAS QUE RETARDAN COAGULACION (anti-hemostaticas o anticoagulantes)
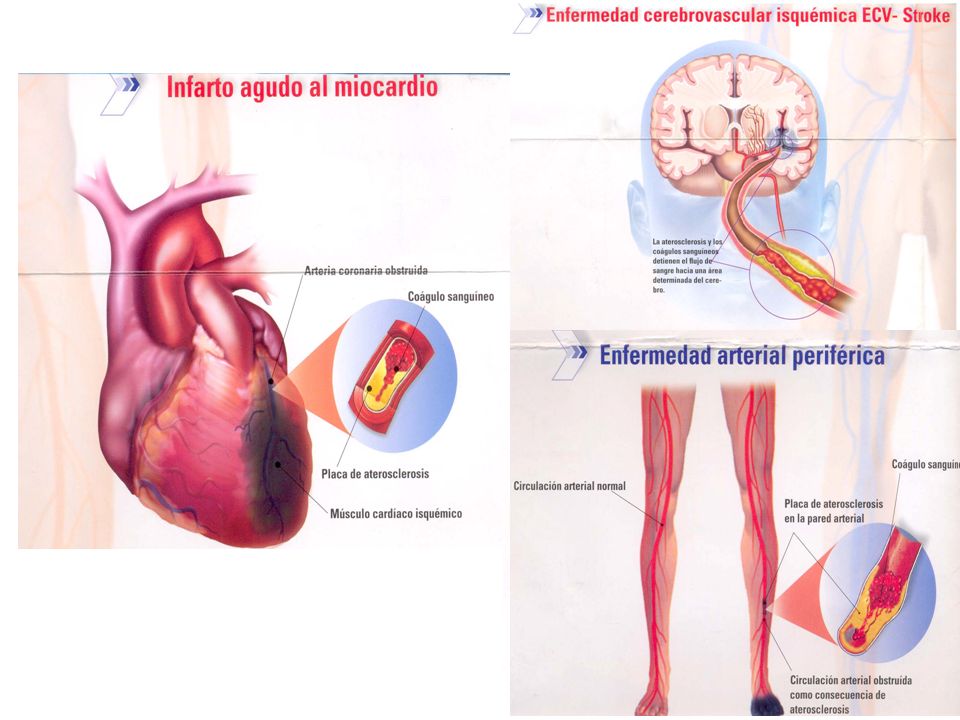
Usadas en: Px y Tx de trombos arteriales y venosos: Enf isquemica miocardio (ASA) Enf cerebro-vascular (ASA). Px trombosis postoperatorias: valvulas cardiacas artificiales, bypass, injertos. Trombosis venosas profundas (AO). Circulacion extracorporea (heparina).
 Enf cerebro-vascular (ASA). Px trombosis postoperatorias: valvulas cardiacas artificiales, bypass, injertos. Trombosis venosas profundas (AO). Circulacion extracorporea (heparina).")
5
DROGAS Q´ RETARDAN COAGULACION
ANTI-PLAQUETARIOS: ASA, dipiridamol, ticlopidina, clopidogrel, inhibidores de glicoproteina I, IIb y IIIa (abciximab, eptifibatide y tirofibam). 2. HEPARINA y HBPM y heparinoides 3. ANTICOAGULANTES ORALES: Warfarina Na (coumadin).
. 2. HEPARINA y HBPM y heparinoides. 3. ANTICOAGULANTES ORALES: Warfarina Na (coumadin).")
6
1. FARMACOS ANTI-PLAQUETARIOS (ASA, dipiridamol, ticlopidina, clopidogrel, inhib GP)
Inhibición de la función de las plaquetas (activación, adhesion y agregación).
.")
7
2) AMPc, accion PGI2=i Adherencia (dipiridamol)
3) i Activacion plaquetaria x ADP x ticlopidina 2) AMPc, accion PGI2=i Adherencia (dipiridamol) 4) i glicoproteinas plaquetarias I, IIb y IIIa (ligan al fibrinogeno—Agregacion) (abciximab, eptifibatide y tirofibam) x 1) Inh del tromboxano A2 plaquetario (ASA)
 i Activacion plaquetaria x ADP. x. ticlopidina. 2) AMPc, accion PGI2=i Adherencia (dipiridamol) 4) i glicoproteinas plaquetarias I, IIb y IIIa (ligan al fibrinogeno—Agregacion) (abciximab, eptifibatide y tirofibam) x. 1) Inh del tromboxano A2 plaquetario (ASA)")
8
1. ASPIRINA MEC ACCION Inh irreversible COX plaquetaria Inh Tx A2 inh la activacion-agregacion. Dosis: inh formacion de prostaciclinab (PGI2 = Inh agregacion plaq y vasodilatacion)!!. Retarda crecimiento de placa ateroescleroticas y sus consecuencias.
!!. Retarda crecimiento de placa ateroescleroticas y sus consecuencias.")
9
ASA Agregación Inh irreversible COX-plaquetaria inh formacion de Tromboxano A2 (de Ac araquidonico) = inh activacion-agreg plaq y vasoconstriccion.
 = inh activacion-agreg plaq y vasoconstriccion.")
10
ASPIRINA (ASA) 80-100 mg/d FCOCINETICA
Absorbe estomago e ID (15-20m). Vida ½ 15-20m. Pero efecto antiplaquetario dura 8-10d. Too megacariocitos. FCOPATOLOGIA Dosis: 100 mg ninguno. Recubrimiento enterico. 900 mg = dolor epigastrico, acidez, nausea, estreñimiento, sangrado.
. Vida ½ 15-20m. Pero efecto antiplaquetario dura 8-10d. Too megacariocitos. FCOPATOLOGIA. Dosis: 100 mg ninguno. Recubrimiento enterico. 900 mg = dolor epigastrico, acidez, nausea, estreñimiento, sangrado.")
11
ASPIRINA (ASA) 80-100 mg/d USOS CLINICOS
(3 afecciones vasculares) 1. Enfermedad Cerebro-Vascular (ataques isquemicos transitorios, trombosis y muerte). 2. Enfermedad cardiaca isquemica (IAM y muerte pctes con angina, re-infarto). 3. Injertos aorto-coronarios de vena safena (retarda o evita la oclusion).
 1. Enfermedad Cerebro-Vascular (ataques isquemicos transitorios, trombosis y muerte). 2. Enfermedad cardiaca isquemica (IAM y muerte pctes con angina, re-infarto). 3. Injertos aorto-coronarios de vena safena. (retarda o evita la oclusion).")
12
Aspirin for Dual Prevention of Venous and Arterial Thrombosis
November 4, NEJM Aspirin for Dual Prevention of Venous and Arterial Thrombosis Theodore E. Warkentin, M.D. Aspirin is conventionally regarded as an agent that prevents arterial thrombosis, an effect mediated through inhibition of platelet cyclooxygenase-1, resulting in decreased synthesis of thromboxane A2(platelet-activating eicosanoid). In high-risk patients, aspirin reduces by one quarter the frequency of arterial thrombosis.1 In 1977, aspirin (at a dose of 600 mg twice daily) was shown to reduce the risk of venous thrombosis when it was given to patients after they had undergone hip arthoplasty.2 Thirty-five years later, guidelines include aspirin as one option for preventing venous thromboembolism after orthopedic surgery.3 However, many experts regard aspirin as inferior therapy for this indication, preferring treatment with conventional anticoagulants (heparin, fondaparinux, or warfarin) or the new oral agents (dabigatran or rivaroxaban). In part, this approach reflects scientific considerations: anticoagulants are especially active in the low-flow, low-shear venous vasculature where fibrin-rich clots form — in contrast to the high-flow, high-shear arterial circulation where platelet adhesion and aggregation are more important. But it also reflects the superior efficacy — albeit shown through indirect comparisons — of anticoagulants over aspirin in postoperative patients.3 Is there a clinical setting in which a moderate venous thromboembolism–preventing activity of aspirin can be exploited? For patients who have had unprovoked venous thromboembolism, the risk of a recurrence of venous thromboembolism after initial “active treatment” with warfarin, dabigatran, or rivaroxaban for 3 to 12 months (or even longer) rises transiently to as high as 20 events per 100 patient-years (and even higher if the active treatment period is <3 months) before settling at a long-term rate of about 5 events per 100 patient-years. Effect of Aspirin on Risk of Recurrence of Venous Thromboembolism (VTE) and Major Vascular Events.).7 Could aspirin represent a reasonable intermediate option between the extremes of indefinite anticoagulation and no ongoing anticoagulation, particularly from the additional perspective of concomitant prevention of arterial thrombosis? Indeed, a dual benefit of aspirin in both arterial and venous circulations might be expected: atherosclerosis is a risk factor for unprovoked venous thromboembolism,8 and patients with idiopathic venous thromboembolism are at increased risk for subsequent arterial cardiovascular events.9 Two recent clinical trials, the Warfarin and Aspirin (WARFASA) study4 and the Aspirin to Prevent Recurrent Venous Thromboembolism (ASPIRE) study,5 evaluated aspirin as compared with placebo in patients with unprovoked venous thromboembolism who had completed initial treatment with heparin followed by warfarin for a minimum of 6 weeks (most received therapy for at least 3 months). Both studies used identical low-dose aspirin regimens (100 mg per day) and had similar enrollment criteria and outcome measures, making them amenable to meta-analysis. Together, these two studies indicate that aspirin reduces by one third the rate of recurrence of venous thromboembolism as well as the rate of major vascular events, a composite outcome of venous thromboembolism, stroke, myocardial infarction, or cardiovascular death. Moreover, these benefits were achieved with a low risk of bleeding. The WARFASA study,4 in which 402 patients were included in the analyses, showed a 42% reduction in the rate of recurrence of venous thromboembolism with aspirin as compared with placebo (rate of recurrence, 6.6% vs. 11.2% per year; hazard ratio with aspirin, 0.58; 95% confidence interval [CI], 0.36 to 0.93; P=0.02); however, a few more patients in the aspirin group than in the placebo group had arterial events (8 patients vs. 5 patients), and the rate of the secondary end point of major vascular events (i.e., venous thromboembolism, myocardial infarction, stroke, or cardiovascular death) was nonsignificantly reduced with aspirin (hazard ratio, 0.67; 95% CI, 0.43 to 1.03; P=0.06). In contrast, as now reported in the Journal, 5 the ASPIRE trial, which involved 822 patients, showed a nonsignificant decrease in the rate of recurrent venous thromboembolism with aspirin as compared with placebo (rate of recurrence, 4.8% vs. 6.5% per year; hazard ratio, 0.74; 95% CI, 0.52 to 1.05; P=0.09). However, since arterial thrombotic events occurred only about half as often in the aspirin-treated group as in the placebo group (10 events vs. 19 events), aspirin was associated with a significant reduction in the rate of major vascular events (hazard ratio, 0.66; 95% CI, 0.48 to 0.92; P=0.01). When data from these two trials were pooled, there was a 32% reduction in the rate of recurrence of venous thromboembolism (hazard ratio, 0.68; 95% CI, 0.51 to 0.90; P=0.007) and a 34% reduction in the rate of major vascular events (hazard ratio, 0.66; 95% CI, 0.51 to 0.86; P=0.002). How should these studies influence practice? Before physicians consider prescribing aspirin for patients who have had acute unprovoked venous thromboembolism, it is important that they treat the patients with effective anticoagulation for at least 3 months, to avoid the high risk of early recurrence. For patients who then wish to stop anticoagulation, a switch to aspirin at a dose of 100 mg daily will reduce by one third the risk of recurrent venous thromboembolism, as well as of arterial cardiovascular events, and may also attenuate the early burst of thrombosis recurrence after cessation of oral anticoagulation. Aspirin is inexpensive, does not require monitoring (in contrast to warfarin), and does not accumulate in patients with renal insufficiency (in contrast to dabigatran and rivaroxaban); in addition, if major bleeding occurs or the patient requires urgent surgery, the antiplatelet effects of aspirin can be reversed with transfusion of platelets. Among patients with unprovoked venous thromboembolism who have completed initial anticoagulation, aspirin would seem to be a reasonable option for long-term dual prevention of recurrent venous thromboembolism and arterial cardiovascular events.
. In high-risk patients, aspirin reduces by one quarter the frequency of arterial thrombosis.1. In 1977, aspirin (at a dose of 600 mg twice daily) was shown to reduce the risk of venous thrombosis when it was given to patients after they had undergone hip arthoplasty.2 Thirty-five years later, guidelines include aspirin as one option for preventing venous thromboembolism after orthopedic surgery.3 However, many experts regard aspirin as inferior therapy for this indication, preferring treatment with conventional anticoagulants (heparin, fondaparinux, or warfarin) or the new oral agents (dabigatran or rivaroxaban). In part, this approach reflects scientific considerations: anticoagulants are especially active in the low-flow, low-shear venous vasculature where fibrin-rich clots form — in contrast to the high-flow, high-shear arterial circulation where platelet adhesion and aggregation are more important. But it also reflects the superior efficacy — albeit shown through indirect comparisons — of anticoagulants over aspirin in postoperative patients.3. Is there a clinical setting in which a moderate venous thromboembolism–preventing activity of aspirin can be exploited For patients who have had unprovoked venous thromboembolism, the risk of a recurrence of venous thromboembolism after initial active treatment with warfarin, dabigatran, or rivaroxaban for 3 to 12 months (or even longer) rises transiently to as high as 20 events per 100 patient-years (and even higher if the active treatment period is <3 months) before settling at a long-term rate of about 5 events per 100 patient-years. Effect of Aspirin on Risk of Recurrence of Venous Thromboembolism (VTE) and Major Vascular Events.).7 Could aspirin represent a reasonable intermediate option between the extremes of indefinite anticoagulation and no ongoing anticoagulation, particularly from the additional perspective of concomitant prevention of arterial thrombosis Indeed, a dual benefit of aspirin in both arterial and venous circulations might be expected: atherosclerosis is a risk factor for unprovoked venous thromboembolism,8 and patients with idiopathic venous thromboembolism are at increased risk for subsequent arterial cardiovascular events.9. Two recent clinical trials, the Warfarin and Aspirin (WARFASA) study4 and the Aspirin to Prevent Recurrent Venous Thromboembolism (ASPIRE) study,5 evaluated aspirin as compared with placebo in patients with unprovoked venous thromboembolism who had completed initial treatment with heparin followed by warfarin for a minimum of 6 weeks (most received therapy for at least 3 months). Both studies used identical low-dose aspirin regimens (100 mg per day) and had similar enrollment criteria and outcome measures, making them amenable to meta-analysis. Together, these two studies indicate that aspirin reduces by one third the rate of recurrence of venous thromboembolism as well as the rate of major vascular events, a composite outcome of venous thromboembolism, stroke, myocardial infarction, or cardiovascular death. Moreover, these benefits were achieved with a low risk of bleeding. The WARFASA study,4 in which 402 patients were included in the analyses, showed a 42% reduction in the rate of recurrence of venous thromboembolism with aspirin as compared with placebo (rate of recurrence, 6.6% vs. 11.2% per year; hazard ratio with aspirin, 0.58; 95% confidence interval [CI], 0.36 to 0.93; P=0.02); however, a few more patients in the aspirin group than in the placebo group had arterial events (8 patients vs. 5 patients), and the rate of the secondary end point of major vascular events (i.e., venous thromboembolism, myocardial infarction, stroke, or cardiovascular death) was nonsignificantly reduced with aspirin (hazard ratio, 0.67; 95% CI, 0.43 to 1.03; P=0.06). In contrast, as now reported in the Journal, 5 the ASPIRE trial, which involved 822 patients, showed a nonsignificant decrease in the rate of recurrent venous thromboembolism with aspirin as compared with placebo (rate of recurrence, 4.8% vs. 6.5% per year; hazard ratio, 0.74; 95% CI, 0.52 to 1.05; P=0.09). However, since arterial thrombotic events occurred only about half as often in the aspirin-treated group as in the placebo group (10 events vs. 19 events), aspirin was associated with a significant reduction in the rate of major vascular events (hazard ratio, 0.66; 95% CI, 0.48 to 0.92; P=0.01). When data from these two trials were pooled, there was a 32% reduction in the rate of recurrence of venous thromboembolism (hazard ratio, 0.68; 95% CI, 0.51 to 0.90; P=0.007) and a 34% reduction in the rate of major vascular events (hazard ratio, 0.66; 95% CI, 0.51 to 0.86; P=0.002). How should these studies influence practice Before physicians consider prescribing aspirin for patients who have had acute unprovoked venous thromboembolism, it is important that they treat the patients with effective anticoagulation for at least 3 months, to avoid the high risk of early recurrence. For patients who then wish to stop anticoagulation, a switch to aspirin at a dose of 100 mg daily will reduce by one third the risk of recurrent venous thromboembolism, as well as of arterial cardiovascular events, and may also attenuate the early burst of thrombosis recurrence after cessation of oral anticoagulation. Aspirin is inexpensive, does not require monitoring (in contrast to warfarin), and does not accumulate in patients with renal insufficiency (in contrast to dabigatran and rivaroxaban); in addition, if major bleeding occurs or the patient requires urgent surgery, the antiplatelet effects of aspirin can be reversed with transfusion of platelets. Among patients with unprovoked venous thromboembolism who have completed initial anticoagulation, aspirin would seem to be a reasonable option for long-term dual prevention of recurrent venous thromboembolism and arterial cardiovascular events.")
13
CONTRAINDICACIONES e INTERACCIONES
ASPIRINA (ASA) mg/d CONTRAINDICACIONES e INTERACCIONES NO en pctes gastritis o ulcerosos (x irritacion e i COX-1). NO en pctes con trastornos hemostaticos congenitos o adquiridos, trombocitopenias. NO junto a dipiridamol y/o cumarinicos (potencializa). NO en asmaticos. Embarazadas??
 mg/d. CONTRAINDICACIONES e INTERACCIONES. NO en pctes gastritis o ulcerosos (x irritacion e i COX-1). NO en pctes con trastornos hemostaticos congenitos o adquiridos, trombocitopenias. NO junto a dipiridamol y/o cumarinicos (potencializa). NO en asmaticos. Embarazadas")
14
2. DIPIRIDAMOL (PERSANTIN tab 75mg TID)
Es pirimido-pirimidina, antitrombotica y vasodilatadora. x`↑ accion de prostaciclina (PgI2)
")
15
DIPIRIDAMOL Adherencia Agregación
3) AMPc, accion PgI2 = inh adherencia de plaquetas al colageno y subendotelio Adherencia Agregación
 AMPc, accion PgI2 = inh adherencia de plaquetas al colageno y subendotelio. Adherencia. Agregación.")
16
DIPIRIDAMOL (PERSANTIN tab 75mg, TID)
ASA y cumarinicos potencializan efecto antitrombotico. 75 mg tid v.o. Efectos 2rios: nausea, malestar abdominal y cefalea. USOS Antitrombotico xa valvulas cardiacas artificiales

17
FARMACOS ANTIPLAQUETARIOS 3. TICLOPIDINA (Ticlid 250mg bid)
Derivado tienopiridina (too clopidogrel). +potente q’ ASA, pero…neutropenia y trombocitopenia!!
. +potente q’ ASA, pero…neutropenia y trombocitopenia!!")
18
FARMACOS ANTIPLAQUETARIOS 3. TICLOPIDINA (Ticlid 250mg bid)
-inh activacion-agregacion plaquetaria por ADP, colageno, Ac araquidon y trombina. -Bloquea la interaccion de plaquetas con F. von Willebrand (desmopresina↑) y fibrinogeno. -Prolonga el tiempo de hemorragia (N=1-6 min). Ticlopidina y T Ticlopidina
 y fibrinogeno. -Prolonga el tiempo de hemorragia (N=1-6 min). Ticlopidina y. T. Ticlopidina.")
19
TICLOPIDINA (Ticlid 250mg bid)
Su efecto se observa en h y persiste x varios dias. USOS Tx y Px ataques isquemicos transitorios (+ASA). Enfermedad isquemica cardiaca (+angina inestable, bypass coronarios) pero… neutropenia y trombocitopenia …
. Enfermedad isquemica cardiaca (+angina inestable, bypass coronarios) pero… neutropenia y trombocitopenia …")
20
FARMACOS ANTIPLAQUETARIOS 4. CLOPIDOGREL (Plavix, Clentel 75mg)
MEC ACCION = a ticlopidina (inh ADP) Efecto max en 3-5 d (75 mg). Pero 300mg en 4-6h y dura x 5-7 d. USO. En Sd coronarios agudos, (+ASA).
 Efecto max en 3-5 d (75 mg). Pero 300mg en 4-6h y dura x 5-7 d. USO. En Sd coronarios agudos, (+ASA).")
21
FARMACOS ANTIPLAQUETARIOS 4. CLOPIDOGREL
FCOPATOLOGIA Sangrados (1.4%): tubo digestivo, hematomas, epistaxis, hematuria, conjuntivales e intracraneales. Raro es neutropenia, anemia aplasica, diarrea y exantemas.
: tubo digestivo, hematomas, epistaxis, hematuria, conjuntivales e intracraneales. Raro es neutropenia, anemia aplasica, diarrea y exantemas.")
22
Posted 11/17/2009 FDA notified healthcare professionals of new safety information concerning an interaction between clopidogrel (Plavix), an anti-clotting medication, and omeprazole (Prilosec/Prilosec OTC), a proton pump inhibitor (PPI) used to reduce stomach acid. New data show that when clopidogrel and omeprazole are taken together, the effectiveness of clopidogrel is reduced. Patients at risk for heart attacks or strokes who use clopidogrel to prevent blood clots will not get the full effect of this medicine if they are also taking omeprazole. Separating the dose of clopidogrel and omeprazole in time will not reduce this drug interaction. Other drugs that are expected to have a similar effect and should be avoided in combination with clopidogrel include: cimetidine, fluconazole, ketoconazole, voriconazole, etravirine, felbamate, fluoxetine, fluvoxamine, and ticlopidine.
, an anti-clotting medication, and omeprazole (Prilosec/Prilosec OTC), a proton pump inhibitor (PPI) used to reduce stomach acid. New data show that when clopidogrel and omeprazole are taken together, the effectiveness of clopidogrel is reduced. Patients at risk for heart attacks or strokes who use clopidogrel to prevent blood clots will not get the full effect of this medicine if they are also taking omeprazole. Separating the dose of clopidogrel and omeprazole in time will not reduce this drug interaction. Other drugs that are expected to have a similar effect and should be avoided in combination with clopidogrel include: cimetidine, fluconazole, ketoconazole, voriconazole, etravirine, felbamate, fluoxetine, fluvoxamine, and ticlopidine.")
23
5. INHIBIDORES de GLICOPROTEINAS IIb / IIIa (abciximab, eptifibatide y tirofiban)
Nuevo grupo de antiagregantes plaquetarios i.v. Ventajas: efecto fcologico en 5 min. Reversion efecto en 4-8 h.

24
X Evitan q’ GP de plaquetas se unan a fibrinogeno.
5. INHIBIDORES de GLICOPROTEINAS IIb / IIIa (abciximab, eptifibatide y tirofiban) Evitan q’ GP de plaquetas se unan a fibrinogeno. X
 Evitan q’ GP de plaquetas se unan a fibrinogeno. X.")
25
2. HEPARINAS 2.1. Heparinas comerciales de pulmon de buey o mucosa intestinal de cerdo ( d PM). -Dosis mg/kg peso. -↑tiempo de coagulacion de 6 a 30 min. -Accion dura de 1.5 a 4 hoo. -Se destruye x la heparinasa. 2.2. Heparinas de bajo peso molecular (HBPM, 5.000). 2.3. Heparinoides (sinteticos).
 Heparinoides (sinteticos).")
26
CID, cirrosis H, Sd nefrotico, CO, Pre-eclampsia, L-asparaginasa.
2. HEPARINAS MECANISMO de ACCION Heparina se une a cofactor heparinico (antitrombina-III, (AT-III) inh proteasas de coagulacion (trombina y factores IXa y Xa). AT-III disminuido en? CID, cirrosis H, Sd nefrotico, CO, Pre-eclampsia, L-asparaginasa.
 inh proteasas de coagulacion (trombina y factores IXa y Xa). AT-III disminuido en CID, cirrosis H, Sd nefrotico, CO, Pre-eclampsia, L-asparaginasa.")
27
Medicion laboratorio del efecto?: TT+++, TTP++ y TP+.
HEPARINA Medicion laboratorio del efecto?: TT+++, TTP++ y TP+. Actividad anti-coagulante depende de: dosis, via adm, origen de heparina (mucosa+ o pulmon), sal sodica o calcicasc, alto o bajo p.m. y concentracion de AT-III.
, sal sodica o calcicasc, alto o bajo p.m. y concentracion de AT-III.")
28
HEPARINA USOS CLINICOS Vida ½ 90 min. 1. Trombosis venosa (s.c.)
2. Tromboembolismo (i.v.) 3. Anticoagulacion general (circulacion extracorporea), cirugia vascular. 4. Post-cirugia: Px trombosis venosa profunda y embolia pulmonar (HBPM: mejor biodisponibilidad, vida ½ +prl y +efecto anti-factor Xa).
 3. Anticoagulacion general (circulacion extracorporea), cirugia vascular. 4. Post-cirugia: Px trombosis venosa profunda y embolia pulmonar (HBPM: mejor biodisponibilidad, vida ½ +prl y +efecto anti-factor Xa).")
29
PRECAUCIONES Y CONTRAINDICACIONES:
HEPARINA PRECAUCIONES Y CONTRAINDICACIONES: Usar s.c., x’ no requiere control lab Enfermedades hemorragicas activas (excepto CID). Trombocitopenia severa
. Trombocitopenia severa.")
30
INTERACCIONES: HEPARINA POTENCIALIZAN EFECTO Anticoagulantes Orales
Antiplaquetarios INHIBICION de EFECTO x: digitalicos, tetraciclinas, nicotina y antihistaminicos.

31
Reacciones de hipersensibilidad:
HEPARINA FCOPATOLOGIA Sangrado: Tubo digestivo y v. urinarias, <suprarrenales, ovario y retroperitoneo. Sitio de inyeccion: Irritacion, eritema, dolor, hematoma y ulceracion. Reacciones de hipersensibilidad: Escalofrio, fiebre, urticaria, asma, rinitis, lagrimeo, n-v y shock.

32
Procesos tromboticos!. x Ac que activan plaquetas trombos.
HEPARINA FCOPATOLOGIA Trombocitopenia. 5.5% pctes que reciben heparina bovina y 1% de origen porcino (<30% plaquetas STOP). Procesos tromboticos!. x Ac que activan plaquetas trombos.
. Procesos tromboticos!. x Ac que activan plaquetas trombos.")
33
HEPARINAS de BAJO PESO MOLECULAR (5.000 daltons)
Son fragmentos de Heparina, producidas x despolimerizacion. Enoxaparina (Clexane) Nadroparina (Fraxiparina) Dalteparina (Fragmin) MEC ACCION. Union a la AT-III
 Nadroparina (Fraxiparina) Dalteparina (Fragmin) MEC ACCION. Union a la AT-III.")
34
HEPARINAS DE BAJO PESO MOLECULAR (5.000 daltons)
Diferencias con Heparina? Actividad contra factor Xa Actividad anticoagulante + predecible biodisponibilidad Vida ½90m y actividad +prolongada (2-4v). Ligan <a proteinas plasmaticas
. Ligan <a proteinas plasmaticas.")
35
HEPARINAS DE BAJO PESO MOLECULAR (5.000 daltons)
< sangrados x: A) inh < a plaquetas B) No ↑ la permeabilidad microvascular C) <interferencia entre plaquetas y pared vascular. USOS: Px y Tx tromboembolismos venosos, angina inestable y trombosis cerebrales agudas.
 inh < a plaquetas. B) No ↑ la permeabilidad microvascular. C) <interferencia entre plaquetas y pared vascular. USOS: Px y Tx tromboembolismos venosos, angina inestable y. trombosis cerebrales agudas.")
36
HEPARINAS DE BAJO PESO MOLECULAR (5.000 daltons)
EFECTOS SECUNDARIOS < que H no fraccionada (trombocitopenia). No cruzan placenta (eleccion en embarazadas).
. No cruzan placenta (eleccion en embarazadas).")
37
HEPARINAS ANTIDOTO Sulfato protamina (Sol 1%).
1 mg protamina neutraliza 100 U de Heparina. - Hipotension y reaccion anafilactoides.

38
3. ANTICOAGULANTES ORALES (cumadinicos y indandionas)
Enfermedad hemorragica ganado Canada, trebol dulce (bishidroxicumarina) protrombina. +++warfarina sodica (coumadin), +fenprocumon y +etilbiscumacetato
 protrombina. +++warfarina sodica (coumadin), +fenprocumon y +etilbiscumacetato.")
39
ANTICOAGULANTES ORALES WARFARINA SODICA (coumadin)
Quimicamente = a Vit K (competicion) carboxilacion terminal de F. coagulacion orden (VII, IX, X y II ineficaces). Cumarinicos son antagonistas de Vit K (carboxilasa). Tiempo de latencia para efecto hoo
 carboxilacion terminal de F. coagulacion orden (VII, IX, X y II ineficaces). Cumarinicos son antagonistas de Vit K (carboxilasa). Tiempo de latencia para efecto hoo.")
40
WARFARINA SODICA (coumadin)
FCOCINETICA -v.o. absorcion completa (max 12 h)– 97% liga albumina Metabolizacion en hepatocitos --– orina. -Vida ½: 40 h. -Cruzan la placenta, Evitar en embarazadas. No leche materna.
– 97% liga albumina. Metabolizacion en hepatocitos. --– orina. -Vida ½: 40 h. -Cruzan la placenta, Evitar en embarazadas. No leche materna.")
41
WARFARINA SODICA (coumadin)
FCOPATOLOGIA Sangrado (vias urinarias) Raras: Dermatitis, urticaria, Necrosis cutanea (x trombosis vasos pqños), alopecia, Nausea, dolor abdominal.
 Raras: Dermatitis, urticaria, Necrosis cutanea (x trombosis vasos pqños), alopecia, Nausea, dolor abdominal.")
42
WARFARINA SODICA (coumadin)
USOS CLINICOS Px y Tx de trombosis y tromboembolias (embolia pulmonar, tromb venosas profundas+, ataques isquemicos transitorios SNC). Px embolias: estenosis mitral, valvulas card artific, fibrilacion Auricular. IAM (+ASA) Px trombosis postOperatorias (HepBPM).
. Px embolias: estenosis mitral, valvulas card artific, fibrilacion Auricular. IAM (+ASA) Px trombosis postOperatorias (HepBPM).")
43
WARFARINA SODICA, (coumadin)
CONTRAINDICACIONES Pctes con tendencia hemorragica (trombocitopenia, enfermedad vascular o trastornos de coagulacion). Pctes sometidos a cirugias SNC y ojo Pctes hipertensos (diast 110 mmHg) Pctes lesiones tubo digestivo Pctes IH e IR o Sd mala absorcion RELATIVAS: no control, toman otras drogas, Policitemia, ancianos, alcoholismo, embarazo.
. Pctes sometidos a cirugias SNC y ojo. Pctes hipertensos (diast 110 mmHg) Pctes lesiones tubo digestivo. Pctes IH e IR o Sd mala absorcion. RELATIVAS: no control, toman otras drogas, Policitemia, ancianos, alcoholismo, embarazo.")
44
WARFARINA SODICA (coumadin tab 5mg)
INTERACCIONES MEDICAMENTOSAS DROGAS Q´ POTENCIALIZAN: AINES, cloroquina, TMP-SMX, metronidazol, antidepresivos 3, Eritro, INH, etc. DROGAS Q´ INHIBEN: Rifampicina, Barbituricos, Griseofulvina, corticoesteroides, colestiramina,Vit K, barbituricos, estrogenos, etc.

45
WARFARINA SODICA (coumadin tab 5mg)
CONTROL LABORATORIO? TP (intervalos 1-3 sem). (TT para heparina). ANTIDOTO?. Vitamina K (K1) mg y se normaliza en 24h. Si hemorragia es importante (10-20 ml/kg plasma humano fresco congelado) y se corrige en min/.
. (TT para heparina). ANTIDOTO . Vitamina K (K1) mg y se normaliza en 24h. Si hemorragia es importante (10-20 ml/kg plasma humano fresco congelado) y se corrige en min/.")
46
May. 2014 The Division of Drug Information (DDI) is CDER's focal point for public inquiries. We serve the public by providing information on human drug products and drug product regulation by FDA. The U.S. Food and Drug Administration today approved Zontivity (vorapaxar) tablets to reduce the risk of heart attack, stroke, cardiovascular death, and need for procedures to restore the blood flow to the heart in patients with a previous heart attack or blockages in the arteries to the legs. Zontivity is the first in a new class of drug, called a protease-activated receptor-1 (PAR-1) antagonist. It is an anti-platelet agent, designed to decrease the tendency of platelets to clump together to form a blood clot. By decreasing the formation of blood clots, Zontivity decreases the risk of heart attack and stroke. Like other drugs that inhibit blood clotting, Zontivity increases the risk of bleeding, including life-threatening and fatal bleeding. Bleeding is the most commonly reported adverse reaction in people taking Zontivity. The drug’s prescribing information (label) includes a Boxed Warning to alert health care professionals about this risk. Zontivity must not be used in people who have had a stroke, transient ischemic attack (TIA), or bleeding in the head, because the risk of bleeding in the head is too great. For more information, please visit: Zontivity.
 is CDER s focal point for public inquiries. We serve the public by providing information on human drug products and drug product regulation by FDA. The U.S. Food and Drug Administration today approved Zontivity (vorapaxar) tablets to reduce the risk of heart attack, stroke, cardiovascular death, and need for procedures to restore the blood flow to the heart in patients with a previous heart attack or blockages in the arteries to the legs. Zontivity is the first in a new class of drug, called a protease-activated receptor-1 (PAR-1) antagonist. It is an anti-platelet agent, designed to decrease the tendency of platelets to clump together to form a blood clot. By decreasing the formation of blood clots, Zontivity decreases the risk of heart attack and stroke. Like other drugs that inhibit blood clotting, Zontivity increases the risk of bleeding, including life-threatening and fatal bleeding. Bleeding is the most commonly reported adverse reaction in people taking Zontivity. The drug’s prescribing information (label) includes a Boxed Warning to alert health care professionals about this risk. Zontivity must not be used in people who have had a stroke, transient ischemic attack (TIA), or bleeding in the head, because the risk of bleeding in the head is too great. For more information, please visit: Zontivity.")
Presentaciones similares