Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Mecanismos de Resistencia
Dra. Alba E. Vega Prof. Asociado Área Microbiología

2
1945. Discurso de aceptación del Premio Nóbel: Sir Alexander Fleming previene sobre el peligro de la resistencia: “No es difícil obtener microbios resistentes a la penicilina en el laboratorio, exponiéndolos a concentraciones que no son suficientes para matarlos; y lo mismo puede suceder en el organismo…” Alexander Flemming

4
Resistencia antimicrobiana
es la pérdida completa o relativa del efecto antimicrobiano contra un microorganismo previamente Sensible Incremento de la CIM

6
Resistencia antimicrobiana
Una población de resistentes naturales está siempre presentes (mutantes resistentes) en todas las poblaciones bacterianas (frecuencia de mutación ) El número de mutantes resistentes aumenta con el inóculo Bajo la presión del antibiótico la subpoblación sensible es inhibida y las mutantes resistentes pueden sobrevivir y transformarse en la población dominante (selección) Bacteria have evolved numerous mechanisms to evade antimicrobial drugs. Chromosomal mutations are an important source of resistance to some antimicrobials. Acquisition of resistance genes or gene clusters, via conjugation, transposition, or transformation, accounts for most antimicrobial resistance among bacterial pathogens. These mechanisms also enhance the possibility of multi-drug resistance. susceptible bacteria bacterias sensibles bacterias resistentes resistant bacteria 6
 en todas las poblaciones bacterianas (frecuencia de mutación ) El número de mutantes resistentes aumenta con el inóculo. Bajo la presión del antibiótico la subpoblación sensible es inhibida y las mutantes resistentes pueden sobrevivir y transformarse en la población dominante (selección) Bacteria have evolved numerous mechanisms to evade antimicrobial drugs. Chromosomal mutations are an important source of resistance to some antimicrobials. Acquisition of resistance genes or gene clusters, via conjugation, transposition, or transformation, accounts for most antimicrobial resistance among bacterial pathogens. These mechanisms also enhance the possibility of multi-drug resistance. susceptible bacteria. bacterias sensibles. bacterias resistentes. resistant bacteria. 6.")
7
Los antibióticos seleccionan la bacteria resistente
7

8
Surgimiento de la resistencia
Penicilinas Década de los 60: Se observan casos de resistencia en todas las regiones del mundo. Entre 1979 y 1987: 0.02% de las S. pneumoniae son resistentes a la penicilina. En el 2008: En los Estados Unidos ~40% de las S. pneumoniae es resistente a las penicilina. When the world finally recognized penicillin for what it was - the most efficacious life-saving drug in the world - it embraced it without question. By the middle of the century, Fleming's discovery had spawned a huge pharmaceutical industry, churning out synthetic penicillins that would treat some of mankind's most ancient scourges, including syphilis, and gangrene. Human society experienced decreased morbidity from warfare, increased food production, and increased life expectancy in large part due to the discovery of antibiotics. Although many improvements in public health and medicine and a decline in infectious disease mortality preceded the introduction of penicillin, antibiotics have made possible further reductions in deaths and disability from infectious disease. Perhaps equally important, they have facilitated the vast expansion of other medical interventions, such as kidney and heart transplants, by allowing clinicians to prevent surgical site infections and infections in immunosuppressed patients, such as organ recipients. Now, growing levels of bacterial resistance to antibiotics threaten our ability not just to treat infectious diseases but also to perform other procedures and treatments that fundamentally depend on affordable and effective antibiotics. Sources: Lewis R. “The Rise of Antibiotic-Resistant Infections”. Gold HS, Moellering RC, Jr. Antimicrobial-drug resistance. N Engl J Med. Nov ;335(19): Pitout JD, Sanders CC, Sanders WE, Jr. Antimicrobial resistance with focus on beta-lactam resistance in gram-negative bacilli. Am J Med. Jul 1997;103(1):51-59.
: Pitout JD, Sanders CC, Sanders WE, Jr. Antimicrobial resistance with focus on beta-lactam resistance in gram-negative bacilli. Am J Med. Jul 1997;103(1):")
9
Resistencia ATM Un problema muy extendido
Cefalosporinas Resistencia [década de los 80] Vancomicina Resistencia [1996] Diseminación a nivel mundial de la cepa 23-F de neumococo resistente a la penicilina SARM SARV ERV VIH TBC-MDR Malaria No region in the world has been excluded from the inexorable spread of increasingly drug-resistant bacteria. Antimicrobial resistance (AMR) is now a serious global phenomenon. Deaths from acute respiratory infections, diarrheal diseases, measles, AIDS, malaria, and tuberculosis account for more than 85% of worldwide mortality from infectious disease. Resistance to first, second, and third-line drugs in most of the pathogens causing these diseases is increasing significantly. Associated costs of moving to second and third line therapy pose an additional economic burden. Added to this is the significant global burden of resistant hospital-acquired infections, the emerging problems of antiviral resistance and the increasing problems of drug resistance in neglected parasitic diseases of poor and marginalized populations. MRSA: Methicillin resistant S. aureus VRSA: Vancomycin resistant S. aureus VRE: Vancomycin resistant Enterococcus HIV: Human Immuno-deficiency virus MDR-TB: Multi-drug resistant tuberculosis Source: Cars, O., Nordberg, P. Antibiotic Resistance – The faceless threat. Published by ReAct, Sweden
 is now a serious global phenomenon. Deaths from acute respiratory infections, diarrheal diseases, measles, AIDS, malaria, and tuberculosis account for more than 85% of worldwide mortality from infectious disease. Resistance to first, second, and third-line drugs in most of the pathogens causing these diseases is increasing significantly. Associated costs of moving to second and third line therapy pose an additional economic burden. Added to this is the significant global burden of resistant hospital-acquired infections, the emerging problems of antiviral resistance and the increasing problems of drug resistance in neglected parasitic diseases of poor and marginalized populations. MRSA: Methicillin resistant S. aureus. VRSA: Vancomycin resistant S. aureus. VRE: Vancomycin resistant Enterococcus. HIV: Human Immuno-deficiency virus. MDR-TB: Multi-drug resistant tuberculosis. Source: Cars, O., Nordberg, P. Antibiotic Resistance – The faceless threat. Published by ReAct, Sweden")
10
RESISTENCIA BACTERIANA
Es la disminución o ausencia de sensibilidad de una cepa bacteriana a uno o varios antibióticos Primaria: natural o intrínseca. No existe blanco de acción para ese antibiótico en ese microorganismo Secundaria: es la que se origina por selección que produce el antibiótico a partir de una población bacteriana sensible

11
Bases genéticas de la resistencia
Natural Resistencia cromosómica: Alteración estructural del DNA cromosómico MUTACIÓN Adquirida Resistencia extracromosómica. Adquisición de DNA extracromosómico 11

12
EVENTOS GENÉTICOS DE LA RESISTENCIA
Bacteria Sensible Bacteria Resistente Mutación XX Bacteria Resistente Transferencia genética 12

13
Transferencia del gen vanA de
E. faecalis a S. aureus 13

14
Resistencia adquirida a los antimicrobianos MECANISMOS
Producción de enzimas inactivantes que convierten a la droga activa en producto inerte Β-lactamasas Pencilina Enzimas adenilantes Estreptomicina Enzimas acetilantes Cloranfenicol Cambios de permeabilidad celular al medicamento Tetraciclinas Cambio estructural de la zona de acción del medicamento Alteración Prot P10 (30 S ribosomal) Estreptomicina Eliminación mediante bomba de eflujo Desarrollo de vías metabólicas alternativas Síntesis de una enzima resistente Capacidad para usar ácido fólico preformado, no requieren PABA Producción incrementada de PABA
 Estreptomicina. Eliminación mediante bomba de eflujo. Desarrollo de vías metabólicas alternativas. Síntesis de una enzima resistente. Capacidad para usar ácido fólico preformado, no requieren PABA. Producción incrementada de PABA.")
15
1. Inactivación enzimática de la droga
- Hidrólisis (Beta lactamasas) - Modificación química
 - Modificación química.")
16
2. Cambios en el sitio blanco
* Cambio de PBP ( Penicilinas , Cefalosporinas) * Subunidad ribosomal 30S (Estreptomicina, Tetraciclina) Subunidad ribosomal 50S - por mutación en una proteina, Eritromicina (L4 o L12) - metilación del ARN 23S, Eritromicina y Lincosamidas * Enzimas ADN girasa, ARN polimerasa, Quinolonas, Rifampicina
 * Subunidad ribosomal 30S (Estreptomicina, Tetraciclina) Subunidad ribosomal 50S. - por mutación en una proteina, Eritromicina (L4 o L12) - metilación del ARN 23S, Eritromicina y Lincosamidas. * Enzimas ADN girasa, ARN polimerasa, Quinolonas, Rifampicina.")
17
3. Disminución de la permeabilidad de la membrana
Naturaleza de la membrana externa Gram negativa: Resistencia intrínseca a ATM hidrofóbicos Disminución en la síntesis de porinas: Afecta la entrada de ATM hidrofílicos

18
4. Sistemas de Eflujo

19
BOMBAS DE EFLUJO

20
5. Vías metabólicas alternativas
Variante de DHFR, Trimetroprim Variante de la dehidropteroato sintetasa, Sulfametoxazol

21
Fuente: Todar K. Todar’s Online Textbook of Bacteriology
En línea en:

22
MECANISMOS DE RESISTENCIA EN ATB BETA-LACTAMICOS
1) PRODUCCION DE BETA-LACTAMASAS 2) ALTERACION DE (PBP) - Reducción en la afinidad en las PBP pre-existentes - Pérdida o aumento en la cantidad de PBP - Aparación de PBP nuevas (ej PBP 2a) ALTERACION DE PERMEABILIDAD DE LA MEMBRANA EXTERNA EFLUJO
 PRODUCCION DE BETA-LACTAMASAS. 2) ALTERACION DE (PBP) - Reducción en la afinidad en las PBP pre-existentes. - Pérdida o aumento en la cantidad de PBP. - Aparación de PBP nuevas (ej PBP 2a) ALTERACION DE PERMEABILIDAD DE LA MEMBRANA EXTERNA. EFLUJO.")
23
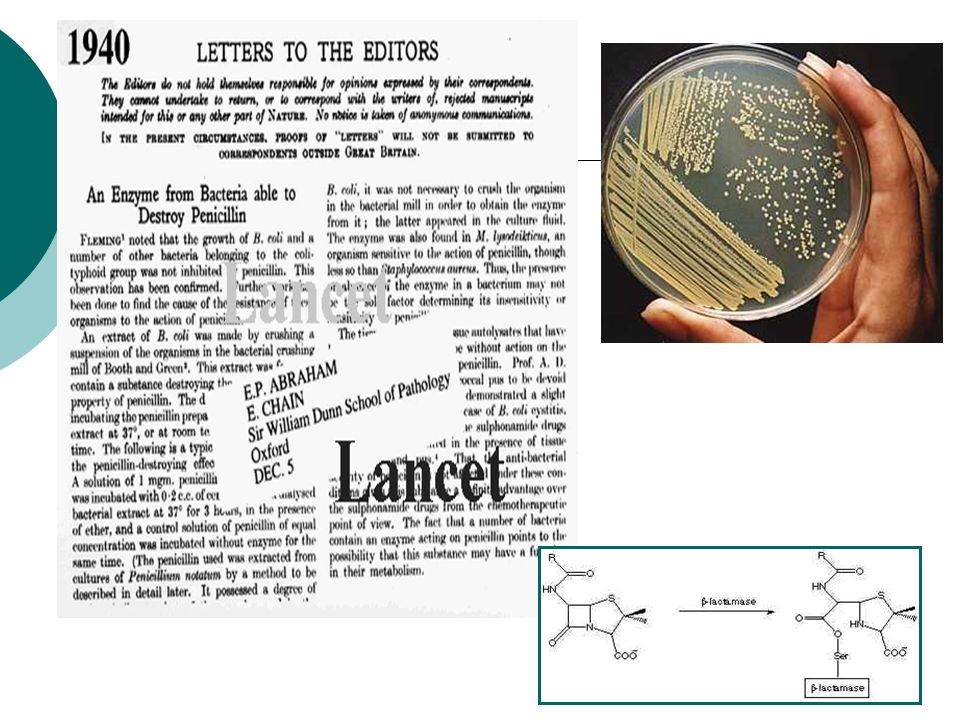
Penicilinasa (ß Lactamasa)
La producción de βlactamasas plasmídicas (TEM-1, TEM-2 y SHV-1) por bacterias gramnegativas es el principal mecanismo de resistencia bacteriana a los antibióticos betalactámicos. Figura 25.
 por bacterias gramnegativas es el principal mecanismo. de resistencia bacteriana a los antibióticos betalactámicos. Figura")
24
PBP modificadas, que no pueden ser reconocidas por el antibiótico

25
La modificación de las PORINAS de la membrana externa de los G (-)
La modificación de las PORINAS de la membrana externa de los G (-). Disminuye su permeabilidad a los antibióticos beta-lactámicos, y así el antibiótico no puede interactuar con su proteína blanco (PBP)
. Disminuye su permeabilidad a los antibióticos beta-lactámicos, y así el antibiótico no puede interactuar con su proteína blanco (PBP)")
26
Eflujo La bacteria es capaz de expulsar el atb mediante un mecanismo de transporte activo que consume atp Bombas de eflujo redalyc.uaemex.mx/.../863/ / html

27
Producción de enzimas (betalactamasas)
Es el principal mecanismo de resistencia frente a los betalactamicos, especialmente en G-negativos ( también pueden producirlas G-positivos y anaerobios). Las betalactamasas hidrolizan el anillo betalactamico y por tanto inactivan el antibiótico antes de su unión con las PBP. Su producción puede estar mediada por plásmidos o puede estar cromosómicamente codificada. En el primer caso, pueden ser transferibles y los inhibidores de betalactamasas suelen inactivarlas; Ej las producidas por S. aureus sensible a la meticilina, Haemophilus influenzae, Moraxella catarrhalis, E.coli, K.pneumoniae, algunas enterobacterias y anaerobios,como Bacteroides fragilis.
. Las betalactamasas hidrolizan el anillo betalactamico y por tanto inactivan el antibiótico antes de su unión con las PBP. Su producción puede estar mediada por plásmidos o puede estar cromosómicamente codificada. En el primer caso, pueden ser transferibles y los inhibidores de betalactamasas suelen inactivarlas; Ej las producidas por S. aureus sensible a la meticilina, Haemophilus influenzae, Moraxella catarrhalis, E.coli, K.pneumoniae, algunas enterobacterias y anaerobios,como Bacteroides fragilis.")
28
Producción de enzimas (betalactamasas)
En el caso de los microorganismos con betalactamasas de origen cromosómico (como Enterobacter spp., Pseudomonas spp., Citrobacter spp., Morganella spp. y Serratia spp.) estos son a menudo inducibles (aumenta su producción tras la exposición a betalactamicos, especialmente cefalosporinas) y no son sustrato de los inhibidores de las betalactamasas . Hay muchos tipos de betalactamasas en función de los betalactamicos que hidrolizan. El uso (y abuso) de los antibióticos durante décadas ha favorecido la evolución de estas enzimas hacia una nueva generación, las llamadas BLEE, que son capaces de hidrolizar las cefalosporinas de tercera generación y el monobactamico aztreonam
 estos son a menudo inducibles (aumenta su producción tras la exposición a betalactamicos, especialmente cefalosporinas) y no son sustrato de los inhibidores de las betalactamasas . Hay muchos tipos de betalactamasas en función de los betalactamicos que hidrolizan. El uso (y abuso) de los antibióticos durante décadas ha favorecido la evolución de estas enzimas hacia una nueva generación, las llamadas BLEE, que son capaces de hidrolizar las cefalosporinas de tercera generación y el monobactamico aztreonam.")
29
Gramnegativos productores de betalactamasa de espectro extendido (BLEE)
Las BLEE confieren resistencia a las cefalosporinas de espectro extendido (por ej. ceftriaxona, cefotaxima y ceftazidima), al aztreonam y a oximinobetalactámicos relacionados. 1983: Primera documentación de betalactamasas plasmídicas capaces de hidrolizar las cefalosporinas de espectro extendido con una cadena lateral oximino, denominadas colectivamente betalactamasas de espectro extendido. Derivadas de mutaciones de genes plasmídicos para TEM-1, TEM-2 o SHV-1 que extienden el espectro de antibióticos betalactámicos sensibles a hidrólisis por esas enzimas. Gram negatives commonly express plasmid-encoded β-lactamases (e.g., TEM-1, TEM-2, and SHV-1) which confer resistance to penicillins but not to expanded-spectrum cephalosporins . However, in Germany in 1983, the extended-spectrum b-lactamases (ESBLs) were detected. ESBLs are beta-lactamases that hydrolyze extended-spectrum cephalosporins with an oxyimino side chain. These cephalosporins include cefotaxime, ceftriaxone, and ceftazidime, as well as the oxyimino-monobactam aztreonam. Typically, they derive from genes for TEM-1, TEM-2, or SHV-1 by mutations that alter the amino acid configuration around the active site of these β-lactamases. This extends the spectrum of β-lactam antibiotics susceptible to hydrolysis by these enzymes. Emery, CL. Detection and clinical significance of extended-spectrum β-lactamases in a tertiary-care medical center. Clin. Microbiol. 1997; 35: Bradford PA. Extended-spectrum β-lactamases in the 21st century: characterization, epidemiology, and detection of this important resistance threat. Clin Microbiol Rev. 2001; 48:933-51 Bush K et al. A functional classification scheme for beta-lactamases and its correlations with molecular structure. Antimicrob Agents Chemother 1995;39: Fuente:
, al aztreonam y a oximinobetalactámicos relacionados. 1983: Primera documentación de betalactamasas plasmídicas capaces de hidrolizar las cefalosporinas de espectro extendido con una cadena lateral oximino, denominadas colectivamente betalactamasas de espectro extendido. Derivadas de mutaciones de genes plasmídicos para TEM-1, TEM-2 o SHV-1 que extienden el espectro de antibióticos betalactámicos sensibles a hidrólisis por esas enzimas. Gram negatives commonly express plasmid-encoded β-lactamases (e.g., TEM-1, TEM-2, and SHV-1) which confer resistance to penicillins but not to expanded-spectrum cephalosporins . However, in Germany in 1983, the extended-spectrum b-lactamases (ESBLs) were detected. ESBLs are beta-lactamases that hydrolyze extended-spectrum cephalosporins with an oxyimino side chain. These cephalosporins include cefotaxime, ceftriaxone, and ceftazidime, as well as the oxyimino-monobactam aztreonam. Typically, they derive from genes for TEM-1, TEM-2, or SHV-1 by mutations that alter the amino acid configuration around the active site of these β-lactamases. This extends the spectrum of β-lactam antibiotics susceptible to hydrolysis by these enzymes. Emery, CL. Detection and clinical significance of extended-spectrum β-lactamases in a tertiary-care medical center. Clin. Microbiol. 1997; 35: Bradford PA. Extended-spectrum β-lactamases in the 21st century: characterization, epidemiology, and detection of this important resistance threat. Clin Microbiol Rev. 2001; 48: Bush K et al. A functional classification scheme for beta-lactamases and its correlations with molecular structure. Antimicrob Agents Chemother 1995;39: Fuente: ArticleId=2941.")
30
Significación clínica de las BLEE
Las BLEE se encuentran en Klebsiella, E. coli , Enterobacter, Proteus, Citrobacter, Pseudomonas Los plásmidos responsables de la producción de BLEE frecuentemente portan genes que codifican resistencia a otras clases de medicamentos (aminoglicósidos). Factores de riesgo Pacientes en estado crítico Hospitalización prolongada ( días) Dispositivos médicos invasivos Tratamiento ATM intensivo The ESBLs are frequently plasmid encoded. Plasmids responsible for ESBL production frequently carry genes encoding resistance to other drug classes (for example, aminoglycosides). Therefore, antibiotic options in the treatment of ESBL-producing organisms are extremely limited. Carbapenems are the treatment of choice for serious infections due to ESBL-producing organisms, yet carbapenem-resistant isolates have recently been reported. ESBL-producing organisms may appear susceptible to some extended-spectrum cephalosporins. However, treatment with such antibiotics has been associated with high failure rates. Known risk factors for colonization and/or infection with organisms harboring ESBLs include admission to an intensive care unit, recent surgery, instrumentation, prolonged hospital stay and antibiotic exposure, especially to extended-spectrum beta-lactam antibiotics. Use of extended-spectrum antibiotics exerts a selective pressure for emergence of ESBL producing gram negatives. The resistance plasmids can then be transferred to other bacteria of a variety of species. Giske, CG et al. Clinical and economic impact of common multidrug-resistant gram-negative bacilli. Antimicrob. Agents Chemother 2008; 52: Fung, HB et al. Current Issues in Gram-Negative Resistance: Extended-Spectrum Beta-Lactamases and Inducible Beta-Lactamases. Journal of Pharmacy Practice 2001; 14: 6-17 Yang, K. Diagnosis and Treatment of Extended-Spectrum and AmpC ß-Lactamase-Producing Organisms. The Annals of Pharmacotherapy 2007; 41: Paterson, DL. Extended-Spectrum ß-Lactamases: a Clinical Update. Clin. Microbiol. Rev. 2005; 18: Fuente:
. Factores de riesgo. Pacientes en estado crítico. Hospitalización prolongada ( días) Dispositivos médicos invasivos. Tratamiento ATM intensivo. The ESBLs are frequently plasmid encoded. Plasmids responsible for ESBL production frequently carry genes encoding resistance to other drug classes (for example, aminoglycosides). Therefore, antibiotic options in the treatment of ESBL-producing organisms are extremely limited. Carbapenems are the treatment of choice for serious infections due to ESBL-producing organisms, yet carbapenem-resistant isolates have recently been reported. ESBL-producing organisms may appear susceptible to some extended-spectrum cephalosporins. However, treatment with such antibiotics has been associated with high failure rates. Known risk factors for colonization and/or infection with organisms harboring ESBLs include admission to an intensive care unit, recent surgery, instrumentation, prolonged hospital stay and antibiotic exposure, especially to extended-spectrum beta-lactam antibiotics. Use of extended-spectrum antibiotics exerts a selective pressure for emergence of ESBL producing gram negatives. The resistance plasmids can then be transferred to other bacteria of a variety of species. Giske, CG et al. Clinical and economic impact of common multidrug-resistant gram-negative bacilli. Antimicrob. Agents Chemother 2008; 52: Fung, HB et al. Current Issues in Gram-Negative Resistance: Extended-Spectrum Beta-Lactamases and Inducible Beta-Lactamases. Journal of Pharmacy Practice 2001; 14: Yang, K. Diagnosis and Treatment of Extended-Spectrum and AmpC ß-Lactamase-Producing Organisms. The Annals of Pharmacotherapy 2007; 41: Paterson, DL. Extended-Spectrum ß-Lactamases: a Clinical Update. Clin. Microbiol. Rev. 2005; 18: Fuente:")
31
AMINOGLUCOSIDOS Modificación del sitio blanco ribosomal
Hidrólisis enzimática (estearasa) Alteración de los sistemas de producción energética, cierra los canales iónicos, de modo que el ATB no puede ingresar al citoplasma
 Alteración de los sistemas de producción energética, cierra los canales iónicos, de modo que el ATB no puede ingresar al citoplasma.")
32
Acción de la cloranfenicol- acetil- transferasa

33
Bases genéticas de la resistencia adquirida
Alteración estructural del DNA cromosómico MUTACIÓN Resistencia cromosómica Adquisición de DNA extracromosómico Resistencia extracromosómica (epidémica o infecciosa) Plásmidos de Resistencia conjugativos ( R) Características Infecciosidad Resistencia a varias drogas a la vez Plásmidos de Resistencia no conjugativos ( r ) (se transfieren por tansducción)
 Plásmidos de Resistencia conjugativos ( R) Características. Infecciosidad. Resistencia a varias drogas a la vez. Plásmidos de Resistencia no conjugativos ( r ) (se transfieren por tansducción)")
34
Mutaciones cromosómicas puntuales:
MECANISMOS GENETICOS DE LA APARICION Y DISEMINACION DE LA RESISTENCIA ATB Mutaciones cromosómicas puntuales: Eventos de ocurrencia espontánea, persistente y se transmite por herencia Son de difícil detección Son de baja frecuencia Resistencia a una sola droga

35
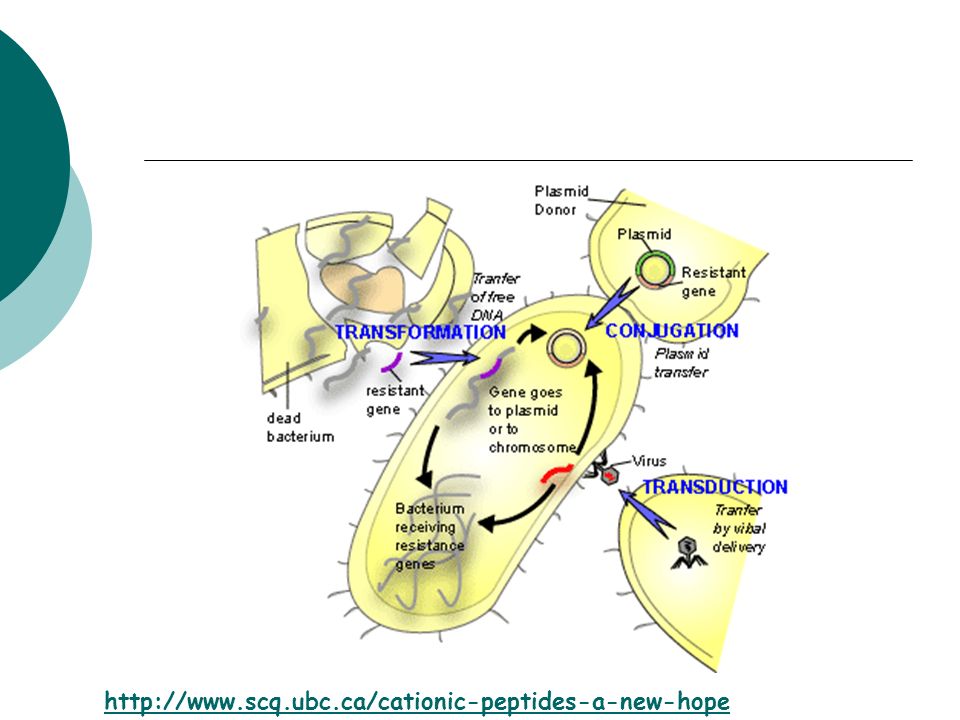
Adquisición de nuevos genes:
MECANISMOS GENETICOS DE LA APARICION Y DISEMINACION DE LA RESISTENCIA ATB Adquisición de nuevos genes: - Transformación (poca importancia clínica) - Transducción (DNA plasmídico incorporado a un fago y transferido a otra bacteria) Conjugación (Plásmidos R) Transposición: (plásmido a plásmido; plásmido a cromosoma)
 - Transducción (DNA plasmídico incorporado a un fago y transferido a otra bacteria) Conjugación (Plásmidos R) Transposición: (plásmido a plásmido; plásmido a cromosoma)")
37
Mapa genético de plásmido de resistencia R conjugativo

38
Plásmido de resistencia
38

39
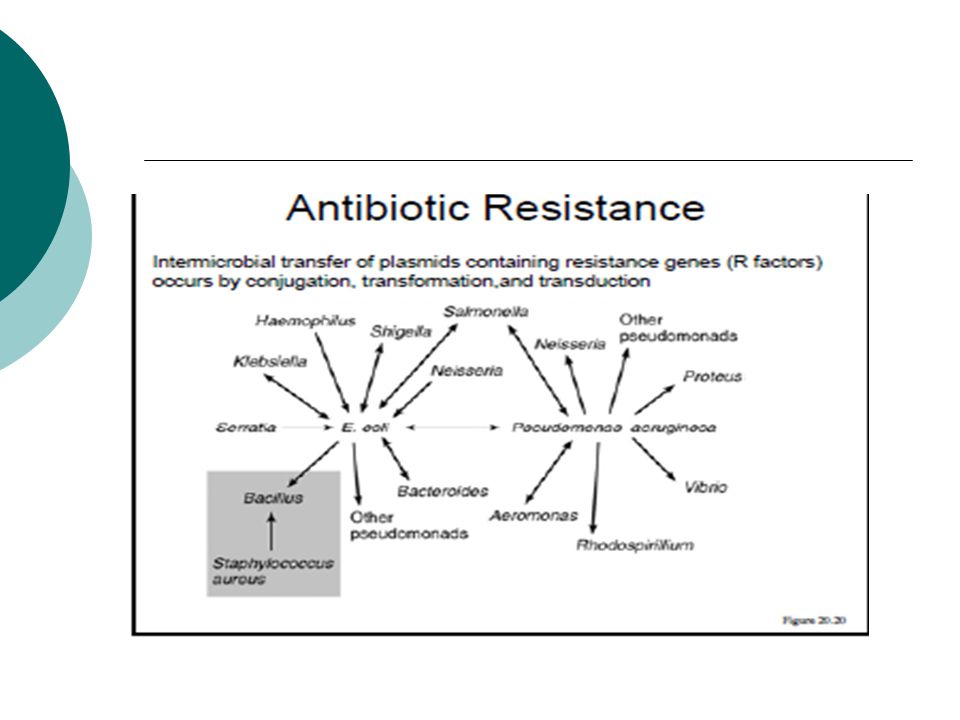
PLASMIDOS R Transportan genes de resistencia a los antibióticos, y con frecuencia varios genes de resistencia son transportados por un único plásmido R Determinante R agrupación de genes de resistencia del plásmido R (complejo de transposones) Factor de transferencia de resistencia región con genes involucrados en la transferencia de resistencia mediante conjugación
 Factor de transferencia de resistencia región con genes involucrados en la transferencia de resistencia mediante conjugación.")
40
Transmisión del factor R
ENTEROBACTERIACEAE Neisseria gonorreae Haemophilus influenzae Grupo Vibrio Pasteurella pestis Grupo Pseudomonas Conjugación

42
Plásmidos de resistencia no conjugativos
Son elementos genéticos autorreplicantes Residencia estable en el huésped Espectro de resistencia menor Menor tamaño Se transfieren por transducción (fago) Presentes en Gram negativas y Gram positivas
 Presentes en Gram negativas y Gram positivas.")
43
Factores que contribuyen al aumento de cepas resistentes

44
Carga provocada por las enfermedades
Las infecciones resistentes aumentan el tiempo de hospitalización de los pacientes y las tasas de mortalidad. Incremento del 5.02% en el riesgo de mortalidad por infección con Enterobacter resistente a las cefalosporinas. S. aureus resistente a la meticilina vs. S. aureus sensible a la meticilina. 20.1% vs. 6.7% de mortalidad relacionada con infecciones de heridas quirúrgicas. Pseudomonas aeruginosa resistentes a múltiples medicamentos. Se triplica la mortalidad. La duración de la estancia en el hospital aumenta 1.7 veces. Mortality from a resistant infection increases for multiple reasons, but, primarily, because of a delay in effective treatment of the resistant infection AMR, increased need for surgery, and other procedures. Comparing the onset of adequate treatment for susceptible versus resistant strains illustrates the how extensively delayed treatment affects patient outcomes. The median interval between obtaining a sample for culture and initiating antibiotics: 51 hours for resistant infections vs 16 hours for susceptible infections. The number of patients who receive effective treatment within 24 hours: 36% vs 68% for resistant to susceptible strains. The number of patients who receive effective treatment within 48 hours: 48% vs 90% for resistant to susceptible strains. These numbers show that within two days, less than half of the people with resistant infections receive the proper treatment. Without proper care, the infection can spread, making it even harder to eliminate (Cosgrove). One method to avoid misdiagnosing resistant infections is to identify patients at high risk for harboring antimicrobial resistant strains. These people include individuals in long-term care facilities and patients with a long or recent history of antimicrobial use. Patients falling into either category should alert the physician. When treating these patients, the doctor may elect to begin treatment with a stronger antimicrobial or, more ideally, perform a rapid susceptibility test to determine the resistance of the organism. In either case, being aware of the possibility of resistance may help to reduce the time to effective treatment. Sources: Cosgrove, S. The Relationship between AMR and Patient Outcomes: Mortality, length of Hospital Stay and Health Care Costs. Clinical Infectious Disease, 2006, 42:S82–S89. Lautencbach, Metlay, Biker, Edelstein, Fishman. Association between FQ Resistance and Mortality in E. Coli and Klebsiella pneumo infections: The Role of Inadequate Empirical AMR Therapy. Clinical Infectious Disease, 2005, 41: Image:
. One method to avoid misdiagnosing resistant infections is to identify patients at high risk for harboring antimicrobial resistant strains. These people include individuals in long-term care facilities and patients with a long or recent history of antimicrobial use. Patients falling into either category should alert the physician. When treating these patients, the doctor may elect to begin treatment with a stronger antimicrobial or, more ideally, perform a rapid susceptibility test to determine the resistance of the organism. In either case, being aware of the possibility of resistance may help to reduce the time to effective treatment. Sources: Cosgrove, S. The Relationship between AMR and Patient Outcomes: Mortality, length of Hospital Stay and Health Care Costs. Clinical Infectious Disease, 2006, 42:S82–S89. Lautencbach, Metlay, Biker, Edelstein, Fishman. Association between FQ Resistance and Mortality in E. Coli and Klebsiella pneumo infections: The Role of Inadequate Empirical AMR Therapy. Clinical Infectious Disease, 2005, 41: Image:")
45
Reservorios animales Definición: Enfermedad en animales que pueden transmitirla a los humanos en condiciones de contacto cercano y/o cuando se produce una mutación genética del patógeno. Reservorios animales comunes: cerdos aves, vida silvestre acuática Patógenos: Influenza, enfermedad de Lyme, virus Ebola ¿Cómo ocurre la transferencia? Influenza: Virus RNA con un reservorio aviar El virus se replica en el tracto intestinal de las aves acuáticas. El virus se disemina en las poblaciones de aves mediante el contacto con las heces. Intermediario entre las aves y los humanos: el cerdo Los cerdos sirven de hospederos a virus de las aves y los seres humanos. Los humanos entran en contacto con cerdos infectados con influenza y adquieren la enfermedad. Págin6 Sources: Glass, G, et al. Satellite imagery characterizes local animal reservoir populations of Sin Nombre virus in the southwestern United States. Proceedings of the National Academy of Science , 99: Donahue, J, et al. Reservoir Competence of White-Footed Mice for Lyme Disease Spirochetes. The American Journal of Tropical Hygiene and Medicine. 1987, 36: Image:

46
Localización de la enfermedad Debido a la resistencia, los países dedican millones de dólares cada año a la contención y tratamiento de las infecciones. Esos gastos no sólo afectan al sector de la salud, sino a toda la economía. Causas del incremento de los gastos: Laboratorios y servicios de rayos X adicionales Tratamientos alternativos más costosos Estancias más prolongadas en los hospitales Procedimientos más complejos para el control de las infecciones Deterioro de la calidad de vida Incremento de la cobertura de los seguros privados Incremento de los gastos generales de los servicios de salud Incremento del costo de la vigilancia epidemiológica Aumento de la carga de la familia de la persona infectada Incremento de los gastos de las compañías donde trabajan los pacientes debido al ausentismo The economic burden continues to rise as the number of resistant infections increases as well as the number of drugs to which each microorganism is resistant. As evidenced by the calculations, antimicrobial resistance is taking a financial toll not only on our hospitals but on economies, as well. Examples of costs: Additional hospital charges for MRSA in the USA Median total cost for MSSA primary nosocomial infections = $9,661 Median cost for MRSA primary nosocomial infections = $27,083 Approximate 3-fold increase in hospital costs from resistance Note: this is only the increase in hospital costs from MRSA; it does not include the costs associated with other resistance infections. Also, the number of resistant bugs continues to increase, making these numbers underestimates. Treatment for resistant infections in US = $4-7 billion per year £500,000 to contain a 5 week outbreak of MRSA in general hospitals. Sources: Murray A. Abramson, Daniel J. Sexton. Nosocomial Methicillin-Resistant and Methicillin-Susceptible Staphylococcus aureus Primary Bacteremia: At What Costs? Infection Control Hospital Epidemiology,1999;20:408–411. Richard Smith, Milton Yago, Michael Millar, Jo Coast. Assessing the macroeconomic impact of a healthcare problem: The application of computable general equilibrium analysis to antimicrobial resistance. Journal of Health Economics, 2005, 24: React. Economic Impact of Antibiotic Resistance. Fact sheet from React, 2008. Image Source: West Investments Ltd. 46

47
S. aureus resistente a la meticilina (SARM)
Hasta el 30-40% de las personas son portadores asintomáticos de S. aureus 70-80% of S. aureus es resistente a las penicilinas Problema de la localización de la enfermedad: MRSARM-AH vs. SARM-AC por ej. SARM-AH resistente a las quinolonas en Unidades de Cuidados Intensivos (UCI) de adultos vs. SARM-AC sensible a las quinolonas en clínicas pediátricas de atención ambulatoria MRSA: Perhaps the most epidemiologically important of all the antibiotic-resistant bacteria. With up to 40-60% of S. aureus carriers having a form resistant to penicillins (depending on the country), it medical problem of truly global proportions. In the U.S. alone, there are an estimated 90,000 cases of invasive S. aureus a year, contributing to the cause of death in an estimated 18,000 people. In fact, nearly 7% of patients coming into the hospital test positive for MRSA on admission--with the anterior nares being the most common site for MRSA inhabitance. This raises the point of community-acquired MRSA with hospital-acquired MRSA. In contrast to earlier years, in which clinical distinction was made between these diseases, they are now consider to be one and the same. While they may differ in exposure and etiology, they are the same clinical disease, and may present in the same fashion--most often as small, red skin lesions that progress to ulceration. Moreover, they are defined by the same criteria: namely, the S. aureus strain must have an oxacillin minimum inhibitory concentration of greater than or equal to 4 mcg/mL. Nevertheless, differing local resistance patterns continues to cause problems with MRSA. Examples of localized resistance have lead to reports to quinalone resistance in MRSA from inpatients when outpatients display quinalone-sensitivity. Such examples demonstrate the complexity of antibiotic resistance patterns (especially when considered on a national and international scale). Sources: Klevens RM, Morrison MA, Nadle J, et al. Invasive methicillin-resistant Staphylococcus aureus infections in the United States. JAMA. Oct ;298(15): Wisplinghoff H, Bischoff T, Tallent SM, Seifert H, Wenzel RP, Edmond MB. Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study. Clin Infect Dis. Aug ;39(3): Sanford MD, Widmer AF, Bale MJ, Jones RN, Wenzel RP. Efficient detection and long-term persistence of the carriage of methicillin-resistant Staphylococcus aureus. Clin Infect Dis. Dec 1994;19(6): Eveillard M, de Lassence A, Lancien E, Barnaud G, Ricard JD, Joly-Guillou ML. Evaluation of a strategy of screening multiple anatomical sites for methicillin-resistant Staphylococcus aureus at admission to a teaching hospital. Infect Control Hosp Epidemiol. Feb 2006;27(2): Huang SS, Rifas-Shiman SL, Warren DK, et al. Improving methicillin-resistant Staphylococcus aureus surveillance and reporting in intensive care units. J Infect Dis. Feb ;195(3): Furuno JP, McGregor JC, Harris AD, et al. Identifying groups at high risk for carriage of antibiotic-resistant bacteria. Arch Intern Med. Mar ;166(5): Fuente:
 de adultos vs. SARM-AC sensible a las quinolonas en clínicas pediátricas de atención ambulatoria. MRSA: Perhaps the most epidemiologically important of all the antibiotic-resistant bacteria. With up to 40-60% of S. aureus carriers having a form resistant to penicillins (depending on the country), it medical problem of truly global proportions. In the U.S. alone, there are an estimated 90,000 cases of invasive S. aureus a year, contributing to the cause of death in an estimated 18,000 people. In fact, nearly 7% of patients coming into the hospital test positive for MRSA on admission--with the anterior nares being the most common site for MRSA inhabitance. This raises the point of community-acquired MRSA with hospital-acquired MRSA. In contrast to earlier years, in which clinical distinction was made between these diseases, they are now consider to be one and the same. While they may differ in exposure and etiology, they are the same clinical disease, and may present in the same fashion--most often as small, red skin lesions that progress to ulceration. Moreover, they are defined by the same criteria: namely, the S. aureus strain must have an oxacillin minimum inhibitory concentration of greater than or equal to 4 mcg/mL. Nevertheless, differing local resistance patterns continues to cause problems with MRSA. Examples of localized resistance have lead to reports to quinalone resistance in MRSA from inpatients when outpatients display quinalone-sensitivity. Such examples demonstrate the complexity of antibiotic resistance patterns (especially when considered on a national and international scale). Sources: Klevens RM, Morrison MA, Nadle J, et al. Invasive methicillin-resistant Staphylococcus aureus infections in the United States. JAMA. Oct ;298(15): Wisplinghoff H, Bischoff T, Tallent SM, Seifert H, Wenzel RP, Edmond MB. Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study. Clin Infect Dis. Aug ;39(3): Sanford MD, Widmer AF, Bale MJ, Jones RN, Wenzel RP. Efficient detection and long-term persistence of the carriage of methicillin-resistant Staphylococcus aureus. Clin Infect Dis. Dec 1994;19(6): Eveillard M, de Lassence A, Lancien E, Barnaud G, Ricard JD, Joly-Guillou ML. Evaluation of a strategy of screening multiple anatomical sites for methicillin-resistant Staphylococcus aureus at admission to a teaching hospital. Infect Control Hosp Epidemiol. Feb 2006;27(2): Huang SS, Rifas-Shiman SL, Warren DK, et al. Improving methicillin-resistant Staphylococcus aureus surveillance and reporting in intensive care units. J Infect Dis. Feb ;195(3): Furuno JP, McGregor JC, Harris AD, et al. Identifying groups at high risk for carriage of antibiotic-resistant bacteria. Arch Intern Med. Mar ;166(5): Fuente:")
48
Enterococos Cocos grampositivos anaeróbicos facultativos
Especies comensales del intestino humano: E. faecalis (90-95%) y E. faecium (5-10%). Producen infecciones clínicas importantes, como infecciones del tracto urinario, bacteremia, endocarditis bacteriana, diverticulitis y meningitis Alto nivel de resistencia endémica a los ATM: Algunos Enterococos son íntrinsecamente resistentes a los antibióticos β-lactámicos (algunas penicilinas y prácticamente todas las cefalosporinas), así como aminoglicosidos. En las dos últimas décadas han surgido cepas particularmente virulentas de Enterococos las que son resistentes a la vancomicina (conocidas como ERV o enterococos resistentes a la vancomicina) Enterococci are the leading cause of nosocomial infection (or secondary infection acquired while in a hospital). They are responsible for approximately 110,000 cases of urinary tract infection, 25,000 cases of bacteremia, 40,000 wound infections, and 1,100 cases of endocarditis yearly in the United States. To infect hosts enterococci primarily colonize mucosal surfaces. They also must evade host defenses although little is known about the actual mechanism of evasion. The pathogenicity of the organism is believed to be closely associated with its ability to produce cytolysin, a toxin that causes rupture of a variety of target membranes, including bacterial cells, erythrocytes, and other mammalian cells. Enterococci inhabit the gastrointestinal tract, the oral cavity, and the vagina in humans as normal commensals. A potential reason for the emergence of E. faecalis as a causative agent of nosocomial infection is the robust nature of this organism. E. faecalis has an intrinsic ability to grow in hypotonic, hypertonic, acidic, or alkaline conditions and to withstand detergents, oxidative stress, and desiccation Doe Joint Genome Institute. Organism Details, Enterococcus faecalis DO. March 22, 2005. Fischetti VA et al. (editors) Gram-Positive Pathogens. ASM Press 2000 Ryan KJ (editors) Sherris Medical Microbiology, 4th ed., McGraw Hill, 294–5 2004 Murray, BE. The life and times of the Enterococcus. Clinical Microbiology Reviews. 1990; 3, 46-65 Fuente:
 y E. faecium (5-10%). Producen infecciones clínicas importantes, como infecciones del tracto urinario, bacteremia, endocarditis bacteriana, diverticulitis y meningitis. Alto nivel de resistencia endémica a los ATM: Algunos Enterococos son íntrinsecamente resistentes a los antibióticos β-lactámicos (algunas penicilinas y prácticamente todas las cefalosporinas), así como aminoglicosidos. En las dos últimas décadas han surgido cepas particularmente virulentas de Enterococos las que son resistentes a la vancomicina (conocidas como ERV o enterococos resistentes a la vancomicina) Enterococci are the leading cause of nosocomial infection (or secondary infection acquired while in a hospital). They are responsible for approximately 110,000 cases of urinary tract infection, 25,000 cases of bacteremia, 40,000 wound infections, and 1,100 cases of endocarditis yearly in the United States. To infect hosts enterococci primarily colonize mucosal surfaces. They also must evade host defenses although little is known about the actual mechanism of evasion. The pathogenicity of the organism is believed to be closely associated with its ability to produce cytolysin, a toxin that causes rupture of a variety of target membranes, including bacterial cells, erythrocytes, and other mammalian cells. Enterococci inhabit the gastrointestinal tract, the oral cavity, and the vagina in humans as normal commensals. A potential reason for the emergence of E. faecalis as a causative agent of nosocomial infection is the robust nature of this organism. E. faecalis has an intrinsic ability to grow in hypotonic, hypertonic, acidic, or alkaline conditions and to withstand detergents, oxidative stress, and desiccation. Doe Joint Genome Institute. Organism Details, Enterococcus faecalis DO. March 22, Fischetti VA et al. (editors) Gram-Positive Pathogens. ASM Press Ryan KJ (editors) Sherris Medical Microbiology, 4th ed., McGraw Hill, 294– Murray, BE. The life and times of the Enterococcus. Clinical Microbiology Reviews. 1990; 3, Fuente:")
49
Enterococos resistentes a la vancomicina (ERV)
Vancomicina forma complejo con D-alanil-D-alanina de los precursores normales de peptidoglicano de la pared celular, inhibiendo la síntesis de la pared celular. Los genes asociados con los ERV codifican una ligasa responsable de la síntesis del D-alanil-D-lactato, que se incorpora a la porción terminal del precursor de PG de la pared celular. - Limita el enlace de la vancomicina y el precursor del peptidoglicano Se han descrito 6 fenotipos enterocócicos resistentes a los glicopéptidos: - VanA y VanB son los más importantes clínicamente - VanA es el más distribuido Of the six phenotypes for VRE resistance that have been reported, VanA and VanB are most clinically relevant: VanA phenotype, induces high level resistance to both vancomycin and teicoplanin while VanB induces variable levels of resistance to vancomycin but is sensitive to teicoplanin. Van A and Van B are usually associated with E.faecalis and E.faecium, but Van A is more widely distributed and thus the predominant type of resistance reported. Moreover, vancomycin resistance has appeared preferentially in E.faecium, which is inherently more resistant to multiple drugs making therapy extremely problematic. Wood, AJ. Vancomycin resistant enterococcal infections. New England Journal of Medicine. 2000; 342, Fuente:

50
Significación clínica del ERV
Factores de riesgo relacionados con los hospitales Admisión en una U Cuidados Intensivos Proximidad a pacientes con ERV Duración de la hospitalización Múltiples ingresos en la unidad Alimentación enteral Factores de riesgo relacionados con los medicamentos Cantidad, tipo y duración de la terapia ATM Uso de vancomicina Uso de cefalosporina de tercera generación Antibióticos antianaeróbicos (clindamicina) Fluoroquinolonas (como el ciprofloxacina) Preparaciones pre-operatorias de colon La mayoría de las infecciones con ERV pueden tratarse con antibióticos que no sean la vancomicina. Las personas colonizadas con ERV (las bacterias están presentes, pero no aparecen síntomas de infección) generalmente no necesitan tratamiento. Enterococci are very tolerant organisms and can survive easily on the hands of health care personnel. Patient-to-patient spread by health care personnel has been documented. Strict observance of hand-washing policies would then be a key element in controlling the spread of epidemic strains of enterococci or any other organism. Cohorting of infected and colonized patients with poor hygiene has been used to prevent the spread of this organism. Proper barriers such as gloves and gowns when soiling is likely are important in preventing dissemination. Each health care facility through collaboration of its quality improvement and infection control programs such as pharmacy, reference microbiology laboratory, nursing, physicians, housekeeping services should develop a comprehensive, institutional-specific strategic plan to detect, prevent and control infection and colonization with VRE. Recommendations for preventing the spread of vancomycin resistance: recommendations of the Hospital Infection Control Practices Advisory Committee (HICPAC) Centers for Disease Control and Prevention. MMWR (1995); 44 (RR-12):1-13 Noskins, GA. Recovery of vancomycin-resistant enterococci on fingertips and environmental surfaces. Infection Control Hospital Epidemiology. 1995: 16;
 Fluoroquinolonas (como el ciprofloxacina) Preparaciones pre-operatorias de colon. La mayoría de las infecciones con ERV pueden tratarse con antibióticos que no sean la vancomicina. Las personas colonizadas con ERV (las bacterias están presentes, pero no aparecen síntomas de infección) generalmente no necesitan tratamiento. Enterococci are very tolerant organisms and can survive easily on the hands of health care personnel. Patient-to-patient spread by health care personnel has been documented. Strict observance of hand-washing policies would then be a key element in controlling the spread of epidemic strains of enterococci or any other organism. Cohorting of infected and colonized patients with poor hygiene has been used to prevent the spread of this organism. Proper barriers such as gloves and gowns when soiling is likely are important in preventing dissemination. Each health care facility through collaboration of its quality improvement and infection control programs such as pharmacy, reference microbiology laboratory, nursing, physicians, housekeeping services should develop a comprehensive, institutional-specific strategic plan to detect, prevent and control infection and colonization with VRE. Recommendations for preventing the spread of vancomycin resistance: recommendations of the Hospital Infection Control Practices Advisory Committee (HICPAC) Centers for Disease Control and Prevention. MMWR (1995); 44 (RR-12):1-13. Noskins, GA. Recovery of vancomycin-resistant enterococci on fingertips and environmental surfaces. Infection Control Hospital Epidemiology. 1995: 16;")
51
SAIV/SARV SAIV SARV Se desconoce el mecanismo exacto de resistencia
Aumento anormal del espesor de los dipéptidos D-ala D-ala de la pared celular Disminución de la penetrancia de los antibióticos Ausencia del gen vanA SARV Agrupamiento de genes vanA Transferencia plasmídica Elemento genético móvil Tn1546 del ERV Provoca la producción de dipéptido D-ala D-lac de la pared celular Reducción del enlace a vancomicina As with MRSA, the genetics behind vancomycin resistance have been well studied. VRSA, like MRSA, contains a prominent gene cluster--known as vanA--that is not active in normal S. aureus isolates. vanA is harbored in a mobile genetic element originally found in vancomycin-resistant enterococci (VRE). This mobile genetic element finds its way to S. aureus via a plasmid-mediated transfer from VRE. Once inside the S. aureus bacteria, vanA encodes for an alternative cell wall dipeptide composed of D-ala D-lac, rather than the normal D-ala D-ala. This D-ala D-lac dipeptide prevents vancomycin from binding to S. aureus, thereby granting the bacteria resistance. It would be logical to think that VISA shared a similar mechanism of resistance. Interestingly, it does not. VISA, in fact, has a resistance signature distinct from not only VRSA but also MRSA and VRE as well. Whereas the other three contain a vanA gene, VISA does not. Rather, VISA resistance is not well understood, but it seems to rely on increased synthesis of normal D-ala D-ala dipeptides, resulting in an abnormally thickened cell wall. This increased synthesis may be due to a polymorphism in the accessory gene regulator, agr, but this is not universal among VISA isolates. Given that vancomycin is one of the most powerful antibiotics at our disposal, the question of treatment for VISA/VRSA is still a great debate. Unfortunately, there is no easy treatment, and no existing treatment has been particularly effective. Chloramphenicol, rifampin, TMX-SMX, and ciprofloxacin, among many other options, have been tried with varying degrees of success. Sources: Noble WC, Virani Z, Cree RG. Co-transfer of vancomycin and other resistance genes from Enterococcus faecalis NCTC to Staphylococcus aureus. FEMS Microbiol Lett. Jun ;72(2): Clark NC, Weigel LM, Patel JB, Tenover FC. Comparison of Tn1546-like elements in vancomycin-resistant Staphylococcus aureus isolates from Michigan and Pennsylvania. Antimicrob Agents Chemother. Jan 2005;49(1): Courvalin P. Clin Infect Dis 2006; 42:Suppl 1:S25 Courvalin P. Vancomycin resistance in gram-positive cocci. Clin Infect Dis. Jan ;42 Suppl 1:S25-34. Howden BP, Johnson PD, Ward PB, Stinear TP, Davies JK. Isolates with low-level vancomycin resistance associated with persistent methicillin-resistant Staphylococcus aureus bacteremia. Antimicrob Agents Chemother. Sep 2006;50(9): Walsh TR, Howe RA. The prevalence and mechanisms of vancomycin resistance in Staphylococcus aureus. Annu Rev Microbiol. 2002;56: Staphylococcus aureus resistant to vancomycin--United States, MMWR Morb Mortal Wkly Rep 2002; 51:565 Figuras tomadas de Applebaum PC. Clin Microbiol Infect 2006(12):16-23
. This mobile genetic element finds its way to S. aureus via a plasmid-mediated transfer from VRE. Once inside the S. aureus bacteria, vanA encodes for an alternative cell wall dipeptide composed of D-ala D-lac, rather than the normal D-ala D-ala. This D-ala D-lac dipeptide prevents vancomycin from binding to S. aureus, thereby granting the bacteria resistance. It would be logical to think that VISA shared a similar mechanism of resistance. Interestingly, it does not. VISA, in fact, has a resistance signature distinct from not only VRSA but also MRSA and VRE as well. Whereas the other three contain a vanA gene, VISA does not. Rather, VISA resistance is not well understood, but it seems to rely on increased synthesis of normal D-ala D-ala dipeptides, resulting in an abnormally thickened cell wall. This increased synthesis may be due to a polymorphism in the accessory gene regulator, agr, but this is not universal among VISA isolates. Given that vancomycin is one of the most powerful antibiotics at our disposal, the question of treatment for VISA/VRSA is still a great debate. Unfortunately, there is no easy treatment, and no existing treatment has been particularly effective. Chloramphenicol, rifampin, TMX-SMX, and ciprofloxacin, among many other options, have been tried with varying degrees of success. Sources: Noble WC, Virani Z, Cree RG. Co-transfer of vancomycin and other resistance genes from Enterococcus faecalis NCTC to Staphylococcus aureus. FEMS Microbiol Lett. Jun ;72(2): Clark NC, Weigel LM, Patel JB, Tenover FC. Comparison of Tn1546-like elements in vancomycin-resistant Staphylococcus aureus isolates from Michigan and Pennsylvania. Antimicrob Agents Chemother. Jan 2005;49(1): Courvalin P. Clin Infect Dis 2006; 42:Suppl 1:S25. Courvalin P. Vancomycin resistance in gram-positive cocci. Clin Infect Dis. Jan ;42 Suppl 1:S Howden BP, Johnson PD, Ward PB, Stinear TP, Davies JK. Isolates with low-level vancomycin resistance associated with persistent methicillin-resistant Staphylococcus aureus bacteremia. Antimicrob Agents Chemother. Sep 2006;50(9): Walsh TR, Howe RA. The prevalence and mechanisms of vancomycin resistance in Staphylococcus aureus. Annu Rev Microbiol. 2002;56: Staphylococcus aureus resistant to vancomycin--United States, MMWR Morb Mortal Wkly Rep 2002; 51:565. Figuras tomadas de Applebaum PC. Clin Microbiol Infect 2006(12):")
52
Factores que influyen en el desarrollo y diseminación de la resistencia
Urbanización acelerada Contaminación y degradación ambiental Cambios demográficos Epidemia de SIDA Crecimiento del comercio y los viajes internacionales Papel de la pobreza Acceso a medicamentos sin receta Alimentos para animales Productos de limpieza antibacterianos Medicamentos falsificados Image Source: United Nations - Trend towards Urbanization of the World's Population Página 52

53
Urbanización acelerada
Se espera que en Asia y África la población urbana se duplique y llegue a ser de alrededor de 3.4 miles de millones en 2030. El crecimiento de una población más allá de sus recursos trae como resultado el hacinamiento y una deficiente higiene y saneamiento. Debido a la deficiente higiene y saneamiento, aumenta la prevalencia de las enfermedades. Aislados de E. coli de zonas urbanas de Nigeria mostraron una resistencia antimicrobiana considerablemente mayor que los de zonas rurales y suburbanas del SO de Nigeria. Africa now has 350 million urban dwellers, more than the populations of Canada and the United States combined, and in 2008, for the first time in history, half of the earth’s population will live in urban areas. This rapid urbanization is often not accompanied by a rapid increase in resources, especially in developing countries. Complicating this situation is the negative impact of poverty, which also plagues many developing country urban dwellers. These factors create settings that encourage the spread of infection. For instance, more than 1/3 of the world’s population lacks access to proper excreta disposal, which is discouraging since proper sanitation has been shown to prevent disease, especially diarrhea, trachoma and intestinal diseases. Improper sewage disposal, on the other hand, encourages AMR transmission and exchange of AMR genes among bacteria. It is not difficult to see why disease and AMR transmit so easily in situations with improper sewage systems, such as the case in Nairobi's slums, where plastic bags, or "floating toilets," are commonly used as containers for excreta disposal and then thrown into the street. Sources: Aiello AE, Larson EL. What is the evidence for a causal link between hygiene and infections? The Lancet Infectious Diseases, 2002, 2(2): Byarugaba DK. A view on antimicrobial resistance in developing countries and responsible risk factors. International Journal of Antimicrobial Agents, 2004, 24(2): Cairncross S. Sanitation in the developing world: current status and future solutions. International Journal of Environmental Health Research, 2003, 13 Suppl 1:S Okeke IN, Lamikanra A, Edelman R. Socioeconomic and behavioral factors leading to acquired bacterial resistance to antibiotics in developing countries. Emerging Infectious Diseases, 1999, 5(1):18-27. State of the world 2007: our urban future. Washington, DC, Worldwatch Institute, 2006 ( accessed 22 July 2008).
: Byarugaba DK. A view on antimicrobial resistance in developing countries and responsible risk factors. International Journal of Antimicrobial Agents, 2004, 24(2): Cairncross S. Sanitation in the developing world: current status and future solutions. International Journal of Environmental Health Research, 2003, 13 Suppl 1:S Okeke IN, Lamikanra A, Edelman R. Socioeconomic and behavioral factors leading to acquired bacterial resistance to antibiotics in developing countries. Emerging Infectious Diseases, 1999, 5(1): State of the world 2007: our urban future. Washington, DC, Worldwatch Institute, 2006 ( accessed 22 July 2008).")
54
Contaminación ambiental
Contaminación fecal del suministro de agua provocada por fugas en tanques sépticos o por el escurrimiento de estiércol desde los campos. Las heces contenidas en el agua hacen que patógenos humanos o animales entren en contacto con bacterias potencialmente resistentes. Esa agua se utiliza para beber o para regar los campos. Aumento de niveles de contaminación atmosférica por ozono Más microorganismos se incorporan al agua de beber debido al incremento de las lluvias y del escurrimiento. Mayor riesgo de transferencia de la resistencia. Applying manure to crops has the potential for runoff into surrounding water supplies. Antibiotics present in the manure, therefore, also end up in the water. A study of rivers across the US found that 50% of surface water was contaminated with antibiotics. Year-long monitoring of manure runoff from fields showed that small quantities (>5%) of dissolved antibiotics (chlorotetracycline, tylosin, and monensin) were lost through leaching and runoff. This study also concluded that the majority of runoff occurred during the fall. A simple strategy to minimize the runoff is spring manure application instead of fall. Sources: Harakeha, S, et al. Antimicrobial-resistance of Streptococcus pneumoniae isolated from the Lebanese environment. Marine Environmental Research, 2006, 62: Berg,G, et al. The rhizosphere as a reservoir for opportunistic human pathogenic bacteria. Environmental Microbiology, 2005, 7: Dolliver, H. et al. Antibiotic losses in leaching and surface runoff from manure-amended agricultural land. Journal of Environmental Quality, 2008, 37: Martins da Costa, P, et al. Antimicrobial Resistance in Enterococcus spp. Isolated in inflow, effluent and sludge from municipal sewage water treatment plants. Water Research, 2006, 40: Image: feww.wordpress.com 54
 of dissolved antibiotics (chlorotetracycline, tylosin, and monensin) were lost through leaching and runoff. This study also concluded that the majority of runoff occurred during the fall. A simple strategy to minimize the runoff is spring manure application instead of fall. Sources: Harakeha, S, et al. Antimicrobial-resistance of Streptococcus pneumoniae isolated from the Lebanese environment. Marine Environmental Research, 2006, 62: Berg,G, et al. The rhizosphere as a reservoir for opportunistic human pathogenic bacteria. Environmental Microbiology, 2005, 7: Dolliver, H. et al. Antibiotic losses in leaching and surface runoff from manure-amended agricultural land. Journal of Environmental Quality, 2008, 37: Martins da Costa, P, et al. Antimicrobial Resistance in Enterococcus spp. Isolated in inflow, effluent and sludge from municipal sewage water treatment plants. Water Research, 2006, 40: Image: feww.wordpress.com. 54.")
55
Epidemia de SIDA y cambios demográficos
Las personas que viven con VIH / SIDA, los jóvenes y los ancianos tienen una menor capacidad natural para combatir las infecciones. Se hace más fácil la transmisión y la diseminación de las infecciones Son mayores las probabilidades de surgimiento y diseminación de la resistencia Más pacientes inmunocomprometidos en una población The AIDS epidemic is a strong risk factor for the formation of AMR. Because HIV diminishes a body’s ability to fight infections, many PLWHA frequently use antimicrobials prophalactially and to treat infections. Indeed, it is likely that HIV is impacting the state of AMR. An Italian study found that individual exposure to beta-lactams, multiple hospitalizations, and low CD4+ cell number were all independent risk factors for MRSA infections in PLWHA. Since CD4+ cells are used by the body to fight infection, the lower the CD4+ number, the more immunocompromised one is. Notably, once highly active antiretroviral therapy (HAART) usage increased, the prevalence of MRSA bacteraemia in PLWHA decreased, indicating that bolstering a PLWHA’s immune system could correlate with a lower prevalence of AMR infections. A frequently overlooked social factor that can exacerbate AMR is the effect of a high concentration of very young and old patients in a health care system. Since it is easier for infection to take root in these populations, the effects of the shifting patient population on the spread of infection should be examined. Sources: Byarugaba DK. A view on antimicrobial resistance in developing countries and responsible risk factors. International Journal of Antimicrobial Agents, 2004, 24(2): Livermore DM. Bacterial resistance: origins, epidemiology, and impact. Clinical Infectious Diseases, 2003, 36(Suppl 1):S11-23. Tumbarello M et al. Risk factors and predictors of mortality of methicillin-resistant Staphylococcus aureus (MRSA) bacteraemia in HIV-infected patients. The Journal of Antimicrobial Chemotherapy, 2002, 50(3):
 usage increased, the prevalence of MRSA bacteraemia in PLWHA decreased, indicating that bolstering a PLWHA’s immune system could correlate with a lower prevalence of AMR infections. A frequently overlooked social factor that can exacerbate AMR is the effect of a high concentration of very young and old patients in a health care system. Since it is easier for infection to take root in these populations, the effects of the shifting patient population on the spread of infection should be examined. Sources: Byarugaba DK. A view on antimicrobial resistance in developing countries and responsible risk factors. International Journal of Antimicrobial Agents, 2004, 24(2): Livermore DM. Bacterial resistance: origins, epidemiology, and impact. Clinical Infectious Diseases, 2003, 36(Suppl 1):S Tumbarello M et al. Risk factors and predictors of mortality of methicillin-resistant Staphylococcus aureus (MRSA) bacteraemia in HIV-infected patients. The Journal of Antimicrobial Chemotherapy, 2002, 50(3):")
56
Globalización del comercio y los viajes
Debido a la globalización, los microbios viajan más rápido y más lejos; ninguna región escapa a sus efectos. La RAM es más marcada en los países en desarrollo. Los organismos comensales RAM generalmente son parte de la flora intestinal normal de los habitantes de países en desarrollo. La migración urbana, los deficientes sistemas de alcantarillado y el hacinamiento estimulan la diseminación de la RAM. La mayoría de las cepas tifoideas resistentes a múltiples medicamentos de los Estados Unidos provienen de 6 países en desarrollo. Globalization requires that efforts be made on an international, coordinated level. National initiatives will be ineffective if neighboring countries do not engage in similar measures. To date, no country has fully implemented the WHO's 2001 Global Strategy for Containment of AMR, with varying levels of commitment in different nations. In addition to MDR-typhoid in the US, many other instances of resistant infections spreading globally exist. Two examples include MRSA outbreaks in Canada that originated in an Indian village and genetically-identical strains of resistant S. pneumoniae that have been found in Iceland, Europe, and Latin America. Source: Cargo air carrier routes. Vancouver, British Columbia, Canada, Vancouver Airport Authority, ( accessed 23 July 2008). Memish ZA, Venkatesh S, Shibl AM. Impact of travel on international spread of antimicrobial resistance. International Journal of Antimicrobial Agents Feb;21(2): Okeke IN et al. Antimicrobial resistance in developing countries. Part II: strategies for containment. The Lancet Infectious Diseases, 2005, 5(9): 56
. Memish ZA, Venkatesh S, Shibl AM. Impact of travel on international spread of antimicrobial resistance. International Journal of Antimicrobial Agents Feb;21(2): Okeke IN et al. Antimicrobial resistance in developing countries. Part II: strategies for containment. The Lancet Infectious Diseases, 2005, 5(9):")
57
RESISTENCIA A LOS ANTIBIÓTICOS
Cría de animales El uso de dosis subclínicas de antibióticos en los alimentos para animales propicia el desarrollo de microorganismos resistentes, tales como Campylobacter, Salmonella, E. coli y E.nterococcus faecium. Los humanos consumen carne roja o de ave contaminada con organismos resistentes. La ingestión de bacterias RAM modifica la microbiota intestinal normal. Posible adquisición de una infección resistente El uso de antibióticos en animales crea reservorios de resistencia. RESISTENCIA A LOS ANTIBIÓTICOS To prevent infection in animals, many farms add antibiotics to animal feed at sub-clinical doses, selecting for resistat bacteria. . (22) Once bacteria are resistant, they have the potential of spreading this resistant to a variety of other bacteria living in a diverse range of environments, including the human digestive tract.. When an individual ingests exogenous bacteria containing AMR genes, AMR genes transfer to bacteria that comprise the mircobiota of the intestine and to other foreign microorganisms with which it comes in contact. A study showed the transfer of vanA resistance gene (VRE) from E. faecium strain of animal origin to an E. faecium strain of human origin in the human intestine. Since no selective antimicrobial pressure was applied during the study, colonization with resistant bacteria was transient. However, it is reasonable to assume that if a selective pressure of antimicrobials is introduced, colonization with resistant bacteria would have persisted. Since enterococci are typically found in meat and milk products ranging from 10*2 to 10*5 per gram (30), the potential AMR transfer is high. This poses increased risk for immunocompromised patients, who are more susceptible (22). Fortunately, studies show that removing antimicrobials from animal feed decreases the rate of antimicrobial resistance. Denmark, like the rest of Europe, has banned the use of certain growth promoting antimicrobials, avoparcin in 1995, virginiamycin in 1998 and in 1999 producers voluntarily stopped the use of all antimicrobial growth promoters. Because the Danish surveillance system is well-developed, many trends seen around the EU have been quantified by the Danish. After stopping the use of antimicrobial growth promoters, there has been a decrease in the amount of resistance to all antibiotics. For instance, the erythromycin resistant E. faecium reached a peak among broilers in 1997 at 76.3%. However, after restricting use of virginiamycin, resistance decreased to 12.7% in 2000 (27). Similar resistance trends are seen for vancomycin and avilamycin. Similar results have been seen throughout Europe; resistance prevalence has declined rapidly following the removal of growth promoters in pigs and chickens, suggesting that in the absence of selective pressure, a susceptible population begins to replace resistant strains (26). Extensive guidelines in this area have been made in the past year by a joint commission of the FAO/WHO/OIE. The interventions that the commission recommends are continued monitoring of AMR in foodborne pathogens as well as risk management measures, including the use of guidelines, vaccinations policies, and development of alternative treatments. Other possible interventions consist of standardizing international methods, namely the MIC, frequently updating risk assessments, and employing resources to help developing countries contain and monitor AMR. Sources: Robin Bywater, Malcolm McConville, Ian Phillips and Thomas Shyrock. The susceptibility to growht-promotion antibiotics of E. faecium isolates from pigs and chickens in Europe. Journal of Antimicrobial Chemotherapy, 2005, 56: Frank Aarestrup, Anne Mette Seyfarth, Hanne-Dorthe Emborg, Karl Pedersen, Rene Hendriksen, Flemming Bager. Effect of Abolishment of the Use of Antimicrobial Agents for Growth Promotion on Occurrence of AMR in Fecal Enterococci from Food Animals in Denmark. Anitmicrobial Agents and Chemotherapy, 2001, 45: Lester, Moller, Sorensen, Monnet, Hammerum. In Vivo Transfer of the van A Resistance Gene from an Enterococcus faecium isolate of animal origin to an E. faecium isolate of human origin in the intestines of human volunteers. Antimicrobial Agents and Chemotherapy, 2006, 50: 57
 Once bacteria are resistant, they have the potential of spreading this resistant to a variety of other bacteria living in a diverse range of environments, including the human digestive tract.. When an individual ingests exogenous bacteria containing AMR genes, AMR genes transfer to bacteria that comprise the mircobiota of the intestine and to other foreign microorganisms with which it comes in contact. A study showed the transfer of vanA resistance gene (VRE) from E. faecium strain of animal origin to an E. faecium strain of human origin in the human intestine. Since no selective antimicrobial pressure was applied during the study, colonization with resistant bacteria was transient. However, it is reasonable to assume that if a selective pressure of antimicrobials is introduced, colonization with resistant bacteria would have persisted. Since enterococci are typically found in meat and milk products ranging from 10*2 to 10*5 per gram (30), the potential AMR transfer is high. This poses increased risk for immunocompromised patients, who are more susceptible (22). Fortunately, studies show that removing antimicrobials from animal feed decreases the rate of antimicrobial resistance. Denmark, like the rest of Europe, has banned the use of certain growth promoting antimicrobials, avoparcin in 1995, virginiamycin in 1998 and in 1999 producers voluntarily stopped the use of all antimicrobial growth promoters. Because the Danish surveillance system is well-developed, many trends seen around the EU have been quantified by the Danish. After stopping the use of antimicrobial growth promoters, there has been a decrease in the amount of resistance to all antibiotics. For instance, the erythromycin resistant E. faecium reached a peak among broilers in 1997 at 76.3%. However, after restricting use of virginiamycin, resistance decreased to 12.7% in 2000 (27). Similar resistance trends are seen for vancomycin and avilamycin. Similar results have been seen throughout Europe; resistance prevalence has declined rapidly following the removal of growth promoters in pigs and chickens, suggesting that in the absence of selective pressure, a susceptible population begins to replace resistant strains (26). Extensive guidelines in this area have been made in the past year by a joint commission of the FAO/WHO/OIE. The interventions that the commission recommends are continued monitoring of AMR in foodborne pathogens as well as risk management measures, including the use of guidelines, vaccinations policies, and development of alternative treatments. Other possible interventions consist of standardizing international methods, namely the MIC, frequently updating risk assessments, and employing resources to help developing countries contain and monitor AMR. Sources: Robin Bywater, Malcolm McConville, Ian Phillips and Thomas Shyrock. The susceptibility to growht-promotion antibiotics of E. faecium isolates from pigs and chickens in Europe. Journal of Antimicrobial Chemotherapy, 2005, 56: Frank Aarestrup, Anne Mette Seyfarth, Hanne-Dorthe Emborg, Karl Pedersen, Rene Hendriksen, Flemming Bager. Effect of Abolishment of the Use of Antimicrobial Agents for Growth Promotion on Occurrence of AMR in Fecal Enterococci from Food Animals in Denmark. Anitmicrobial Agents and Chemotherapy, 2001, 45: Lester, Moller, Sorensen, Monnet, Hammerum. In Vivo Transfer of the van A Resistance Gene from an Enterococcus faecium isolate of animal origin to an E. faecium isolate of human origin in the intestines of human volunteers. Antimicrobial Agents and Chemotherapy, 2006, 50:")
58
Acuicultura Como ocurre en la cría de animales, frecuentemente se usan antibióticos en la acuicultura, las granjas comerciales y el cultivo de mariscos para prevenir las infecciones. Mecanismos de diseminación de organismos resistentes a los antibióticos: Traslado de peces y por consiguiente de las bacterias antibióticas que ellos portan de un entorno a otro Los alimentos no consumidos por los peces y las heces, ambos conteniendo antibióticos, se depositan en el fondo del criadero junto con los sedimentos naturales. Los antibióticos se lixivian del sedimento y viajan a sitios distantes. Contaminación de los criaderos de peces con aguas no tratadas que contienen flora intestinal normal y patógenos. In the past 20 years, industrial aquaculture has quadrupled in size, and a faster rate of growth in the industry has been predicted for the future. However, responsible practices in aquaculture have not evolved like the industry itself. Developing countries around the globe currently use prophylactic antibiotics indiscriminately, selecting for not only resistant fish pathogens but human pathogens, as well. The main concern with prophylactic antibiotics in aquaculture is the spread of resistance from fish pathogens to human pathogens. Several cases have been well documented, strongly suggesting that this transfer has taken place. The drug-resistant outbreaks of Salmonella enterica serotype Typhimurium DT104 in the United States and Europe was traced to the Far East (Angulo). The plasmid in Salmonella enterica contained genes for tetracycline and flouroquinolone resistance, which were traced to the fish pathogens Vibrio damsela and Vibrio anduillarum. Not an isolated case, other fish pathogens have been shown to transfer resistance to human pathogens, as well. Aeromonas salmonicida through the plasmid IncU, containing resistance to sulfonamides, trimethoprims, and tetracycline, have transferred resistance to the human pathogens around the globe, including Aeromonas hydrophila, Aeromonas caviae and E. coli (Rhodes). The use of antibiotics in aquaculture increase rates of AMR in human pathogens, posing a threat to our current treatment of human infections. Several techniques have been suggested to decrease the dependence on antimicrobial agents, including vaccines and improved water sanitation. Vaccines exist for more than 15 fish pathogens. Vaccines are not a substantial upfront cost, and the economic impact of the vaccine favors the investment, to the extent that only a marginal improvement in survival is necessary to pay for the investment of the vaccine. When choosing between vaccines, minor differences in the overall vaccine efficacy produce substantially greater profits (Ragnar). Sanitation measures aim to eliminate or reduce the number of fish pathogens present in the water. Current techniques include UV light radiation, chemicals such as hypochlorous acid and ozone. Furthermore, new technologies continue to be developed to improve the quality and sanitation of industry water in economical manners. Sources: Rhodes,et all. Distribution of Oxytetracycline Resistance Plasmids between Aeromonads in Hospital and Aquaculture Environments: Implications of Tn1721 in Dissemination of the Tetracycline Resistant Determinant TetA. Applied and Environmental Microbiology, 2000, 66: Angulo,et al. Changes in antimicrobial resistance in Salmonella enterica serovar Typhimurium. Emerging Infectious Disease, 2006, 6:436-8. Ragnar, et al. Effects of disease risk, vaccine efficacy and market price on the economics of fish vaccination. Aquaculture, 2006, 256:42-49. Fortt A et al. The Use and Abuse of Antibiotics in Salmon Farming. Oceana Publication, 2007, 23. Documented Cases of AMR transfer and human infection: The plasmid in human Salmonella enterica contained genes for tetracycline and flouroquinolone resistance, whichh were traced to the fish pathogens Vibrio damsela and Vibrio anduillarum. The drug-resistant outbreaks of Salmonella enterica serotype Typhimurium DT104 in the United States and Europe was traced to the Far East (36). Evidence that AMR is a global issue.
. The plasmid in Salmonella enterica contained genes for tetracycline and flouroquinolone resistance, which were traced to the fish pathogens Vibrio damsela and Vibrio anduillarum. Not an isolated case, other fish pathogens have been shown to transfer resistance to human pathogens, as well. Aeromonas salmonicida through the plasmid IncU, containing resistance to sulfonamides, trimethoprims, and tetracycline, have transferred resistance to the human pathogens around the globe, including Aeromonas hydrophila, Aeromonas caviae and E. coli (Rhodes). The use of antibiotics in aquaculture increase rates of AMR in human pathogens, posing a threat to our current treatment of human infections. Several techniques have been suggested to decrease the dependence on antimicrobial agents, including vaccines and improved water sanitation. Vaccines exist for more than 15 fish pathogens. Vaccines are not a substantial upfront cost, and the economic impact of the vaccine favors the investment, to the extent that only a marginal improvement in survival is necessary to pay for the investment of the vaccine. When choosing between vaccines, minor differences in the overall vaccine efficacy produce substantially greater profits (Ragnar). Sanitation measures aim to eliminate or reduce the number of fish pathogens present in the water. Current techniques include UV light radiation, chemicals such as hypochlorous acid and ozone. Furthermore, new technologies continue to be developed to improve the quality and sanitation of industry water in economical manners. Sources: Rhodes,et all. Distribution of Oxytetracycline Resistance Plasmids between Aeromonads in Hospital and Aquaculture Environments: Implications of Tn1721 in Dissemination of the Tetracycline Resistant Determinant TetA. Applied and Environmental Microbiology, 2000, 66: Angulo,et al. Changes in antimicrobial resistance in Salmonella enterica serovar Typhimurium. Emerging Infectious Disease, 2006, 6: Ragnar, et al. Effects of disease risk, vaccine efficacy and market price on the economics of fish vaccination. Aquaculture, 2006, 256: Fortt A et al. The Use and Abuse of Antibiotics in Salmon Farming. Oceana Publication, 2007, 23. Documented Cases of AMR transfer and human infection: The plasmid in human Salmonella enterica contained genes for tetracycline and flouroquinolone resistance, whichh were traced to the fish pathogens Vibrio damsela and Vibrio anduillarum. The drug-resistant outbreaks of Salmonella enterica serotype Typhimurium. DT104 in the United States and Europe was traced to the Far East (36). Evidence that AMR is a global issue.")
59
Productos de limpieza antibacterianos
Generalmente los jabones antibacterianos contienen triclosán. No se ha demostrado que proporcionen ninguna protección contra las infecciones. Se desconoce su efecto sobre la resistencia. Los productos de limpieza antibacterianos generalmente contienen compuestos de amonio cuaternario. Se han utilizado durante décadas. En los hogares donde su uso es elevado se ha observado un incremento de la resistencia. Es necesario continuar investigando esos compuestos: es posible que su uso frecuente estimule la RAM. Antibacterial soaps containing the common ingredients triclosan or trilocarban have not been shown to offer any added infection protection and their effects on resistance are unknown. Their potential harm should be further researched: although no increase in AMR was shown in three community settings, these soaps increased in vitro resistance in ten of eleven studies. The usage of antibacterial cleaning products containing quaternary ammonium compounds, such as benzalkonium chloride, has also correlated with increased resistance. Little literature on this subject exists, however, and more is needed to definitively determine the impact on resistance. Image source: Sources: Aiello AE et al. Antibacterial cleaning products and drug resistance. Emerging Infectious Diseases, 2005, 11(10): Aiello AE, Larson EL, Levy SB. Consumer antibacterial soaps: effective or just risky? Clinical Infectious Diseases, 2007, 45(Suppl 2):S 59
: Aiello AE, Larson EL, Levy SB. Consumer antibacterial soaps: effective or just risky Clinical Infectious Diseases, 2007, 45(Suppl 2):S")
60
Acceso a medicamentos sin receta
En muchos países en desarrollo es fácil obtener antibióticos en los hospitales, farmacias sin receta Características de los medicamentos sin receta que contribuyen a la RAM: Calidad subestándar Dosis subterapéuticas Automedicación inapropiada Es fácil obtener antibióticos sin receta en las nuevas farmacias de Internet o en las de servicio por correo. Existen pocas regulaciones para monitorear las ventas de medicamentos por Internet. Es difícil imponer restricciones a la venta de esos medicamentos debido a las características de Internet y de las ventas internacionales. In many situations legal and illegal over-the-counter access to antimicrobials leads to injudicious drug use. Often antimicrobials are frequently obtained without the guidance of a physician or other knowledgeable prescriber in developing countries. This may cause consumers to erroneously determine their need for antimicrobials, as well as the optimal dose and length of treatment. Even if they seek outside advice on using antimicrobials for their symptoms, like from a pharmacist or untrained drug seller, this information can easily be inaccurate. Inappropriate over-the-counter drug use is not restricted to indigent people in developing countries. Larson and Grullon-Figueroa found that in Manhattan, New York, 34 of 34 pharmacies in a Hispanic neighbourhood sold OTC antibiotics, even though antibiotic sales require a prescription in the US. Additionally, antibiotics for fish, which have the same active ingredients as the ones that humans use, are widely sold OTC in pet stores across the US. Recently, a new method of drug acquisition has been created through internet pharmacies. While some online pharmacies obey the laws of their place of residence, many do not. Online pharmacies are capable of selling substandard or counterfeit drugs, as well as good quality drugs for which the consumer has no legitimate use for. Effective regulation of these pharmacies is still a new and relatively untested field. Some interventions, such as a seal of pharmaceutical quality issued by the national pharmaceutical licensing board, are in progress and provide consumers with a stronger security that they will receive quality medications. In general, though, internet pharmacies will be difficult to effectively regulate due to their non-physical nature and international reach. Sources: Chalker J et al. Effectiveness of a multi-component intervention on dispensing practices at private pharmacies in Vietnam and Thailand--a randomized controlled trial. Social Science & Medicine, 2005, 60(1): Grigoryan L, et al. and Self-Medication with Antibiotics and Resistance (SAR) Consortium. Determinants of self-medication with antibiotics in Europe: the impact of beliefs, country wealth and the healthcare system. The Journal of Antimicrobial Chemotherapy, 2008, 61(5): Internet pharmacy logo. London, England, Royal Pharmaceutical Society, ( accessed 22 July 2008). Larson E, Grullon-Figueroa L. Availability of antibiotics without prescription in New York City. Journal of Urban Health : Bulletin of the New York Academy of Medicine, 2004, 81(3): Okeke IN et al. Antimicrobial resistance in developing countries. Part II: strategies for containment. The Lancet Infectious Diseases, 2005, 5(9): Okeke IN, Lamikanra A, Edelman R. Socioeconomic and behavioral factors leading to acquired bacterial resistance to antibiotics in developing countries. Emerging Infectious Diseases, 1999, 5(1):18-27. Reeves D. The 2005 Garrod Lecture: the changing access of patients to antibiotics--for better or worse? The Journal of Antimicrobial Chemotherapy, 2007, 59(3): Statement of William K. Hubbard Commissioner for Policy, Planning and Legislation, Food and Drug Administration. Washington, DC, United States Food and Drug Administration, and Consumer Affairs, Foreign Commerce, and Tourism, on Commerce, Science and Transportation, ( accessed 22 July 2008).
: Grigoryan L, et al. and Self-Medication with Antibiotics and Resistance (SAR) Consortium. Determinants of self-medication with antibiotics in Europe: the impact of beliefs, country wealth and the healthcare system. The Journal of Antimicrobial Chemotherapy, 2008, 61(5): Internet pharmacy logo. London, England, Royal Pharmaceutical Society, ( accessed 22 July 2008). Larson E, Grullon-Figueroa L. Availability of antibiotics without prescription in New York City. Journal of Urban Health : Bulletin of the New York Academy of Medicine, 2004, 81(3): Okeke IN et al. Antimicrobial resistance in developing countries. Part II: strategies for containment. The Lancet Infectious Diseases, 2005, 5(9): Okeke IN, Lamikanra A, Edelman R. Socioeconomic and behavioral factors leading to acquired bacterial resistance to antibiotics in developing countries. Emerging Infectious Diseases, 1999, 5(1): Reeves D. The 2005 Garrod Lecture: the changing access of patients to antibiotics--for better or worse The Journal of Antimicrobial Chemotherapy, 2007, 59(3): Statement of William K. Hubbard Commissioner for Policy, Planning and Legislation, Food and Drug Administration. Washington, DC, United States Food and Drug Administration, and Consumer Affairs, Foreign Commerce, and Tourism, on Commerce, Science and Transportation, ( accessed 22 July 2008).")
61
Medicamentos falsificados y de calidad subestándar
Los ATM parecen ser los productos más falsificados en los países en desarrollo. Los medicamentos para la tuberculosis, la malaria y el VIH son los más comunes. Pero también se falsifican antibióticos 'antiguos’: penicilina, tetraciclina, cotrimoxazol, cloramfenicol. Un estudio realizado por la OMS en 7 países africanos encontró que entre % de los antimaláricos eran falsos. La ineficacia de muchas de las leyes en vigor en los países en desarrollo facilita la venta de medicamentos falsificados. Además, en muchos casos las condiciones de almacenamiento y transporte en esos países conducen a la degradación y la pérdida de la eficacia de los medicamentos. Holograma auténtico del artusenato Copia en una hoja de plata While it seems logical that a high prevalence of sub-therapeutic medications will increase the selective pressure for resistance to form, and thus add to the problem of AMR, evidence proving this series of events is lacking. The lack of studies examining this link should not be mistaken for a lack of causation, however. Several studies do cite cases of resistance likely hastened by a high presence of substandard medications. For instance, Kelesidis et al. concludes that the high prevalence of substandard chloramphenicol and co-trimoxazole in Burma could have contributed to the high rate of typhoid antibiotic resistance in the region. The lack of direct evidence speaks to the need for further studies on the extent of the effects of counterfeit and substandard drugs on AMR. Sources: Aldhous P. Counterfeit pharmaceuticals: murder by medicine. Nature, 2005, 434: Byarugaba DK. A view on antimicrobial resistance in developing countries and responsible risk factors. International Journal of Antimicrobial Agents, 2004, 24(2): Kelesidis T et al. Counterfeit or substandard antimicrobial drugs: a review of the scientific evidence. The Journal of Antimicrobial Chemotherapy, 2007, 60(2): Newton PN et al. Counterfeit anti-infective drugs. The Lancet Infectious Diseases, 2006, 6(9): Okeke IN, Lamikanra A, Edelman R. Socioeconomic and behavioral factors leading to acquired bacterial resistance to antibiotics in developing countries. Emerging Infectious Diseases, 1999, 5(1):18-27. Falsificación Fuente: Aldhous, P. Nature, 2005.
: Kelesidis T et al. Counterfeit or substandard antimicrobial drugs: a review of the scientific evidence. The Journal of Antimicrobial Chemotherapy, 2007, 60(2): Newton PN et al. Counterfeit anti-infective drugs. The Lancet Infectious Diseases, 2006, 6(9): Okeke IN, Lamikanra A, Edelman R. Socioeconomic and behavioral factors leading to acquired bacterial resistance to antibiotics in developing countries. Emerging Infectious Diseases, 1999, 5(1): Falsificación. Fuente: Aldhous, P. Nature,")
62
Pobreza FACTORES QUE DIFICULTAN LA PREVENCIÓN DE LAS INFECCIONES:
FACTORES QUE DIFICULTAN EL CONTROL DE LAS INFECCIONES: Insuficiente consumo de calorías y nutrientes Deficiente higiene y saneamiento Hacinamiento Falta de acceso a las instalaciones de salud Falta de acceso a los medicamentos Falta de instrucción acerca de los antimicrobianos Falta de dinero para comprar los medicamentos del ciclo completo de tratamiento These co-factors affect infection prevention and control in the following ways: Malnutrition and starvation affect the body’s natural ability to fight infection. Poor hygiene and sanitation significantly increase the risk of infection (see Rapid Urbanization slide). Crowded conditions that outgrow resources can lead to poor sanitation and increase the probability of coming in contact with infections due to increased close contact with others. Inaccessible health facilities decrease one’s ability to get an accurate diagnosis and treat their infection. In developing countries rural communities are especially affected, like in Uganda where only 49% of the population lives within 5 km of a health care facility. When drugs are inaccessible, infection is allowed to continue and spread. Having insufficient funds to buy drugs can lead to the sharing of prescriptions among families or not buying the full course of antimicrobials, and both of these actions can increase AMR. Sources: Byarugaba DK. Antimicrobial resistance in developing countries and responsible risk factors. International Journal of Antimicrobial Agents 2004, 24(2): Okeke IN, Lamikanra A, Edelman R. Socioeconomic and behavioral factors leading to acquired bacterial resistance to antibiotics in developing countries. Emerging Infectious Diseases, 1999, 5(1):18-27. Mientras más sean las infecciones, mayores serán las probabilidades de que la RAM aparezca y se disemine.
. Crowded conditions that outgrow resources can lead to poor sanitation and increase the probability of coming in contact with infections due to increased close contact with others. Inaccessible health facilities decrease one’s ability to get an accurate diagnosis and treat their infection. In developing countries rural communities are especially affected, like in Uganda where only 49% of the population lives within 5 km of a health care facility. When drugs are inaccessible, infection is allowed to continue and spread. Having insufficient funds to buy drugs can lead to the sharing of prescriptions among families or not buying the full course of antimicrobials, and both of these actions can increase AMR. Sources: Byarugaba DK. Antimicrobial resistance in developing countries and responsible risk factors. International Journal of Antimicrobial Agents 2004, 24(2): Okeke IN, Lamikanra A, Edelman R. Socioeconomic and behavioral factors leading to acquired bacterial resistance to antibiotics in developing countries. Emerging Infectious Diseases, 1999, 5(1): Mientras más sean las infecciones, mayores serán. las probabilidades de que la RAM aparezca y se disemine.")
63
¿Qué podemos hacer? LOS HOSPITALES
Perfeccionar el control de las infecciones hospitalarias Poner en vigor las regulaciones de los comités de protección al paciente LAS PERSONAS Higiene personal Informar a los demás acerca del problema LOS MEDICOS Indicar los medicamentos correctamente Instruir a los pacientes acerca del uso correcto de los antibióticos Recopilar más información sobre el alcance de la resistencia LOS GOBIERNOS Incrementar el acceso a medicamentos apropiados en todos los países Revitalizar las innovaciones en la esfera de los antibióticos Revitalizar las innovaciones relacionadas con tecnologías de diagnóstico rápido Revitalizar las vacunas dirigidas a organismos RAM Adapted from WHO, Alliance for Patient Safety, departmental report, 2007

64
Normas para el uso de antimicrobianos
No utilizar más de 2 antimicrobianos. No asociar antimicrobianos de una misma familia. Preferir siempre un bactericida a un bacteriostático. Trabajar en colaboración con el laboratorio de microbiología. No administrar antimicrobianos sin conocer los riesgos. No usar antimicrobianos de alta toxicidad en pacientes ambulatorios. Evaluar cuidadosamente el uso profiláctico de antimicrobianos. Recordar que el último antimicrobiano del mercado no es necesariamente el mejor.

65
http://www. elmundo. es/elmundosalud/2011/08/31/noticias/1314808040
66
Muchas gracias!!!

Presentaciones similares