Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Complicaciones por CMV asociadas a VIH
Carlos Alvarez MD, MSc, DTM&H Profesor Medicina Pontificia Universidad Javeriana Universidad Nacional de Colombia

2
2.007 7 x Hab.

3
Relacion hombre/mujer por año Colombia 1986 -2003
AÑOS Fuente: Programa ETS - Sida Ministerio de Salud BIomédica Biomédica. 2002; 22:77-88

4
Figura 1. Proporción ajustada de casos notificados de VIH por sexo, Colombia, 1985 – 2008.

5
0.7 y 1.1%

6
0.7 y 1.15%

7
0.7 y 1.3%

8
0.6 y 1.25%

9
% En esta figura se demuestra que todavía hay gente en Colombia que se muere por VIH-SIDA y que generalmente es gente joven (entre años) solo siendo superada por los accidentes de transito y la violencia en esta población. Es decir es paradójico que a pesar que el conocimiento de la enfermedad y hay medicamento efectivos desafortunadamente en nuestro país existe personas que se mueren por la presencia del virus (razones administrativas, diagnósticos tardíos, pacientes no conscientes, pocas opciones terapéuticas, problemas de resistencia a los medicamentos,etc). Edad
 solo siendo superada por los accidentes de transito y la violencia en esta población. Es decir es paradójico que a pesar que el conocimiento de la enfermedad y hay medicamento efectivos desafortunadamente en nuestro país existe personas que se mueren por la presencia del virus (razones administrativas, diagnósticos tardíos, pacientes no conscientes, pocas opciones terapéuticas, problemas de resistencia a los medicamentos,etc). Edad.")
10
Probabilidad de desarrollar sida en 3 años
8.1 MACS bDNA: > 30K 10K-30K 3K-10K 501K-3K <500 RT-PCR: >55K 20K-55K 7K - 20K 1.5K - 7K < 1500 Carga viral Mellors J et al. Ann Int Med 1997;12:946

11
Probabilidad de desarrollar sida a 6 meses
CASCADE. AIDS 2004; 18 (1):51-8].
:51-8].")
12
Probabilidad de desarrollar sida a 6 meses
CASCADE. AIDS 2004; 18 (1):51-8].
:51-8].")
13
Carga Viral y Conteo de CD4
Velocidad: carga Viral Distancia al sitio de impacto: CD4 CV CD4 Sitio de impacto: Enfermedad que define SIDA

14
Carga Viral y Conteo de CD4
Velocidad: carga Viral Distancia al sitio de impacto: CD4 CV CD4 Sitio de impacto: Enfermedad que define SIDA

15
Carga Viral y Conteo de CD4
Velocidad: carga Viral Distancia al sitio de impacto: CD4 CV CD4 Sitio de impacto: Enfermedad que define SIDA

16
Carga Viral y Conteo de CD4
Velocidad: carga Viral Distancia al sitio de impacto: CD4 CV CD4 Sitio de impacto: Enfermedad que define SIDA

17
Carga Viral y Conteo de CD4
Velocidad: carga Viral Distancia al sitio de impacto: CD4 CV CD4 Sitio de impacto: Enfermedad que define SIDA

18
Carga Viral y Conteo de CD4
CV Velocidad: carga Viral Distancia al sitio de impacto: CD4 TARV CD4 Para poder bajarle la velocidad al avión o incluso hacerlo retroceder, tenemos una ayuda que es la administración de la terapia antirretroviral, que actualmente es muy potente. Sitio de impacto: Enfermedad que define SIDA

19
Carga Viral y Conteo de CD4
CV Velocidad: carga Viral Distancia al sitio de impacto: CD4 TARV CD4 Para poder bajarle la velocidad al avión o incluso hacerlo retroceder, tenemos una ayuda que es la administración de la terapia antirretroviral, que actualmente es muy potente. Sitio de impacto: Enfermedad que define SIDA

20
Respuesta a la terapia en pacientes con HAART
N E J M 1998;338:853-60

21
Descenso en morbilidad desde la introducción de HAART
3.5 3.0 2.5 2.0 1.5 1.0 0.5 Incidencia por persona-año Año 1996 1997 1998 1999 2000

22
DHHS 2009: ¿Cuando comenzar?
CD4+ Cell Count Recommendation < 350 cells/mm³ Start HAART cells/mm³ Start HAART* > 500 cells/mm³ Panel divided† Clinical Conditions Favoring Initiation of Therapy Regardless of CD4+ Cell Count History of AIDS-defining illness Certain acute opportunistic infections Pregnancy HIVAN HBV coinfection when HBV treatment is indicated CD4+ count decline > 100 cells/mm3 per yr HIV-1 RNA > 100,000 copies/mL DHHS, US Department of Health and Human Services; HBV, hepatitis B virus; HIVAN, HIV-associated nephropathy. This slide lists the DHHS guidelines released on World AIDS Day, December 1, The guidelines state that HAART should be initiated at CD4+ cell counts between 350 and 500 cells/mm^3. The asterisk indicates that 55% of panel members strongly recommended initiation at these CD4+ cell counts and 45% moderately recommended it. Essentially, all members of the panel at least moderately recommended initiating therapy when the CD4+ count is ≤ 500 cells/mm^3. The final category is CD4+ cell counts > 500 cells/mm^3, and on this issue, the panel was equally divided. One half of the members favored initiating therapy regardless of CD4+ cell count—that is, even in those patients with CD4+ cell counts > 500 cells/mm^3—whereas the remaining one half thought that the recommendations should view this number as an optional threshold for initiation of therapy. There are some conditions listed that favor initiation of antiretroviral therapy regardless of the CD4+ cell count, including history of an AIDS-defining illness, certain opportunistic infections, pregnancy, HIV-associated nephropathy, hepatitis B coinfection when hepatitis B treatment is indicated, rapid CD4+ cell count decline, and a high HIV-1 RNA level. The trend clearly is toward increased numbers of people falling into the category for which recommendations to start therapy are positive. *Panel divided: 55% strongly recommend and 45% moderately recommend. †50% favor initiating therapy at this stage; 50% view initiating therapy at this stage as optional. DHHS. Available at:

23
El problema del diagnóstico tardio
Conteo Células CD4+ entre pacientes con diagnóstico de novo por VIH 500 400 300 CD4+ Cell Count (cells/mm3) The problem of late diagnosis is not a new one. This slide depicts data from the Johns Hopkins HIV clinic cohort beginning at the start of the HAART era and showing CD4+ cell counts for patients initiating therapy. The results show the disappointing finding that CD4+ cell counts at treatment initiation have not increased over time. Care providers are not identifying patients at earlier stages of disease and are not initiating treatment at higher CD4+ cell counts. It is likely that this outcome is not caused by providers choosing to delay initiation of therapy, but rather is the result of a failure to diagnose patients at a time when earlier initiation of therapy is possible. 200 100 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 Calendar Year Moore RD, et al. CROI Abstract 805..
 The problem of late diagnosis is not a new one. This slide depicts data from the Johns Hopkins HIV clinic cohort beginning at the start of the HAART era and showing CD4+ cell counts for patients initiating therapy. The results show the disappointing finding that CD4+ cell counts at treatment initiation have not increased over time. Care providers are not identifying patients at earlier stages of disease and are not initiating treatment at higher CD4+ cell counts. It is likely that this outcome is not caused by providers choosing to delay initiation of therapy, but rather is the result of a failure to diagnose patients at a time when earlier initiation of therapy is possible Calendar Year. Moore RD, et al. CROI Abstract")
24
Acceso a la terapia ATRV
WHO. UNAIDS. UNICEF. Towards universal access: scaling up priority HIV/AIDS interventions in the health sector, Progress report, 2007

25
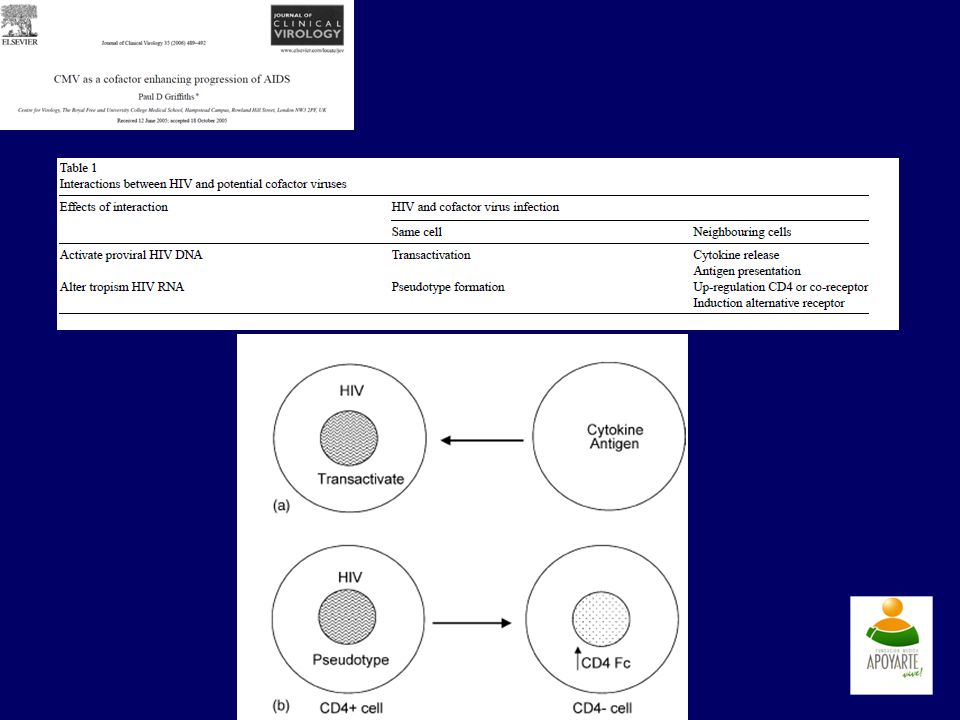
Consecuencias de la infección viral sobre la muerte celular

26
CITOMEGALOVIRUS Familia Betaherpesviridae Prevalencia: 80-90%
Primoinfección: Dos primeras décadas de vida. Infección asintomática

27
Células del sistema inmune
Fibroblastos Macrofago Monocito Neutrofilo PMN Eosinofilo Basofilo Células endoteliales Células musculo liso Celula progenitora LATENCIA PERSISTENCIA

28
Mecanismos de Infección CMV
Infección primaria: D + /R - Productos sanguíneos Replicación rápida Reactivación: R + Replicación lenta Superinfección: D + /R +

29
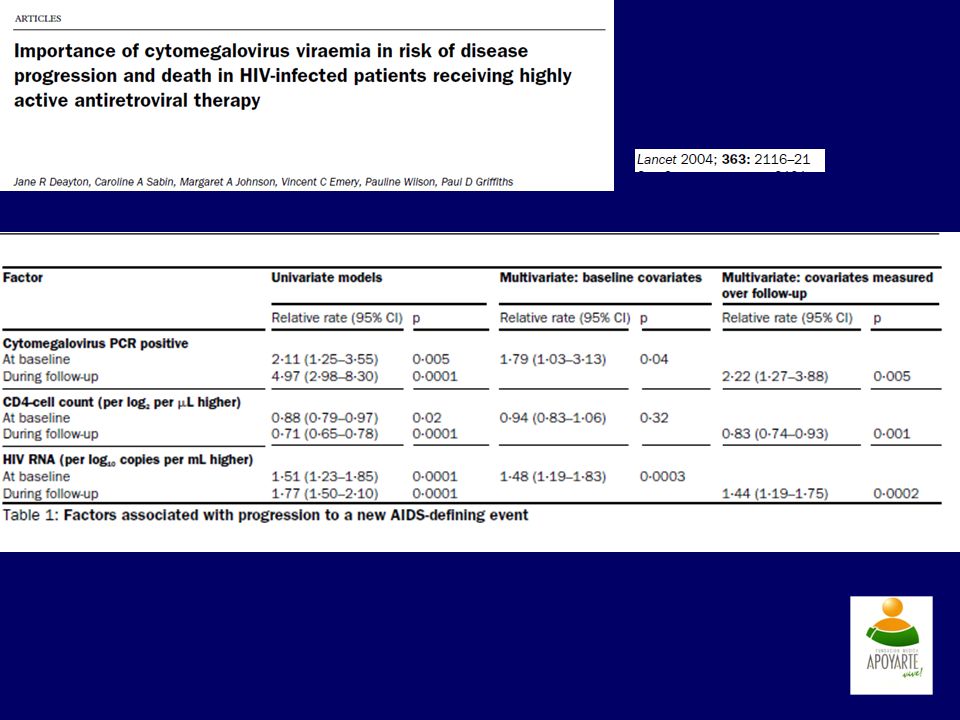
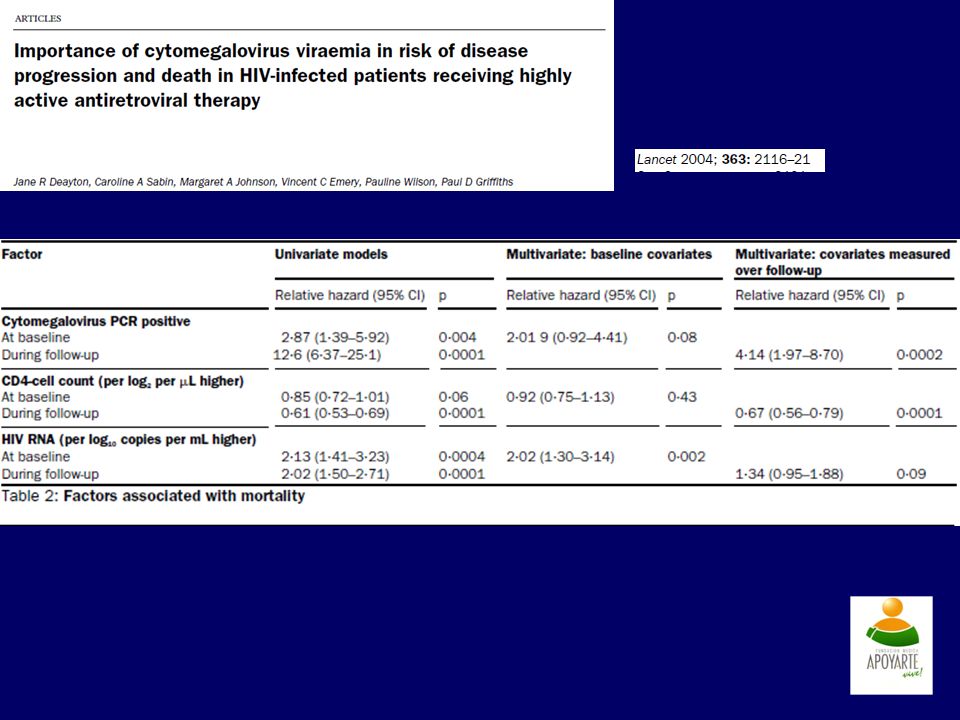
DINAMICA VIRAL Vol 7 July 2007

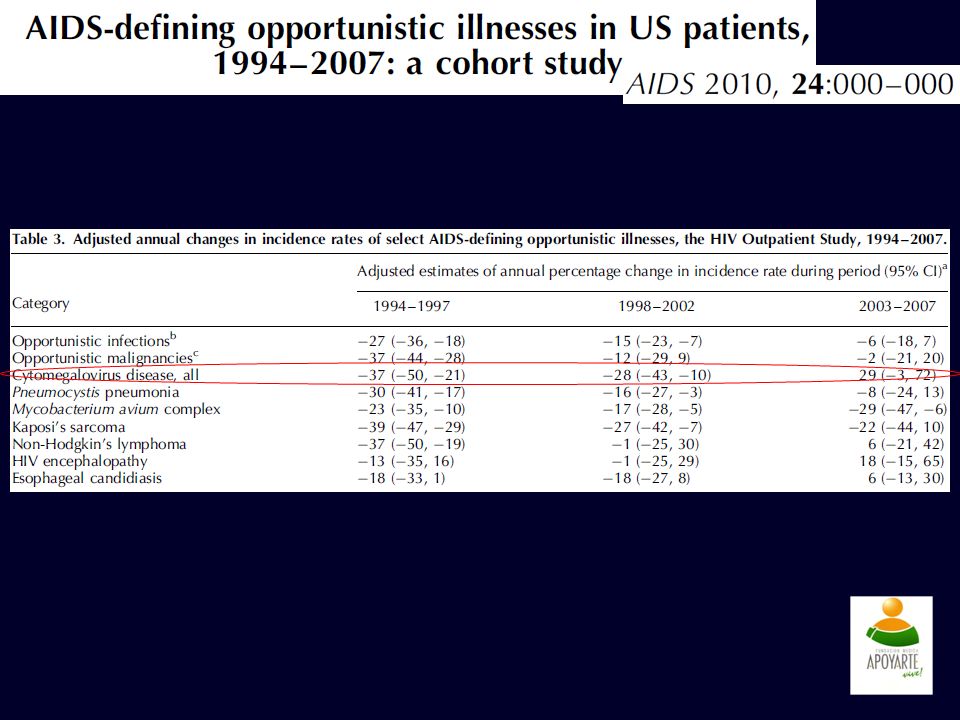
30
DINAMICA VIRAL Vol 7 July 2007

43
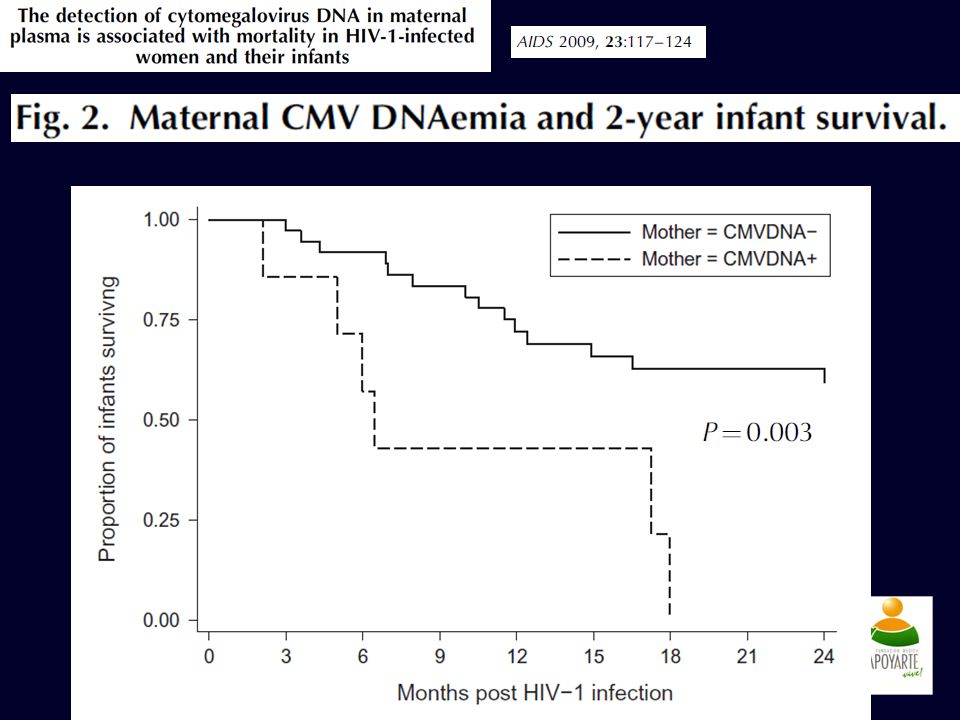
Log rank test <104.

45
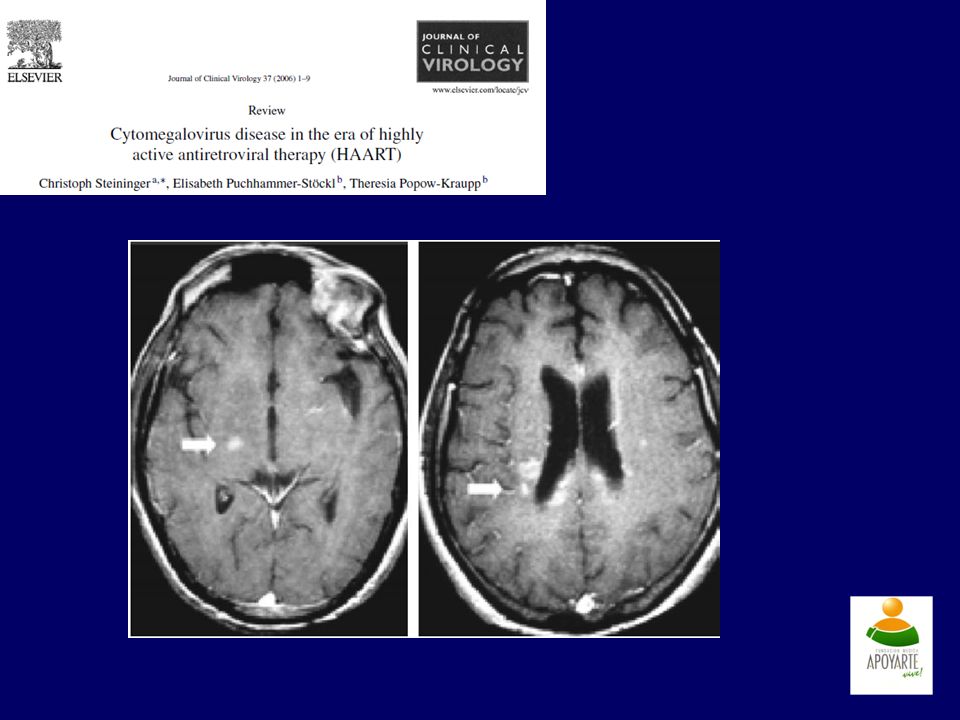
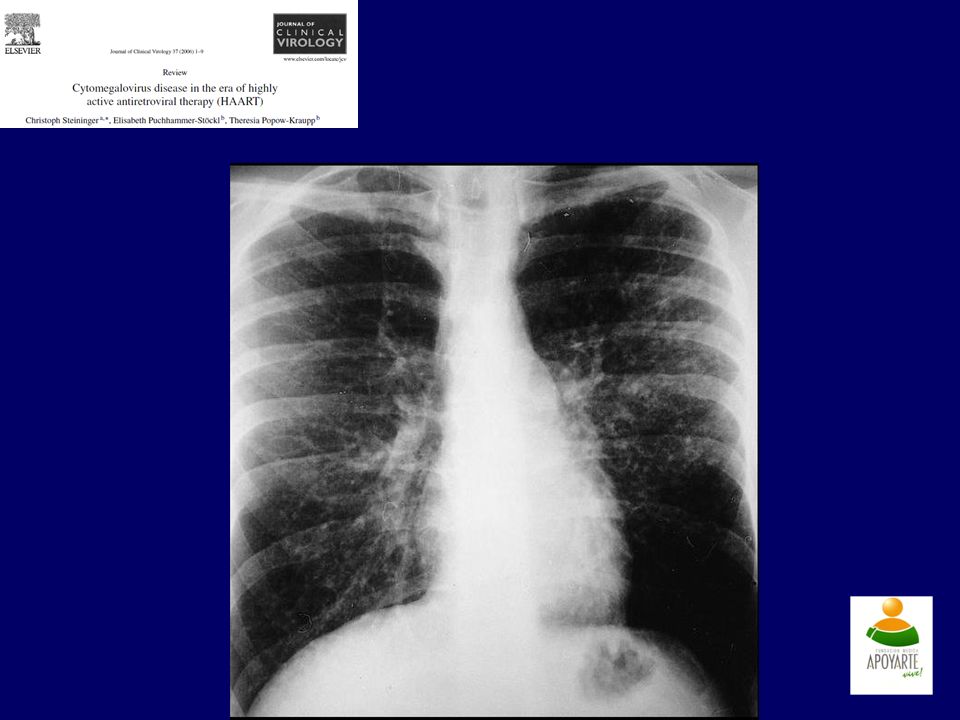
SINDROMES CLINICOS EFECTOS DIRECTOS EFECTOS INDIRECTOS
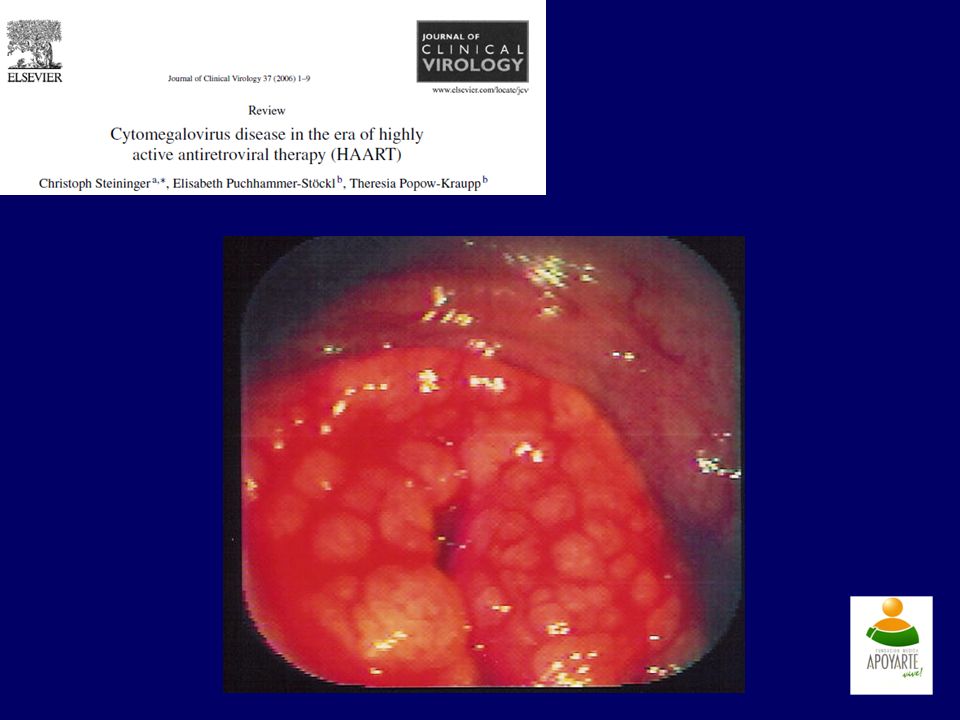
EFECTOS NO CLINICOS Síndrome viral Hepatitis Enf. gastrointestinal Encefalitis Neumonitis Nefritis Mortalidad Infecciones bacterianas Infecciones micóticas Infecciones Virales: Herpes Hepatitis C Aumento costos Hospitalización prolongada

46
CUADROS CLINICOS Hepatitis Nefritis:
Elevación Fosfatasa alcalina y γ- Glutamil transferasa. Elevación aminotrasnferasas. Bilirubinas casi normales. Nefritis: Glomerulopatia Necrosis células endoteliales

54
INFECCION VIH AGUDA Manifestaciones clínicas: * Fiebre : 97%
* Adenopatías : 77 % * Faringitis: 73% * Erupción: 70% * Mialgia o artralgia : 58% * Otros: Diarrea, meningitis, cefalea, naúsea y/o vómito.

58
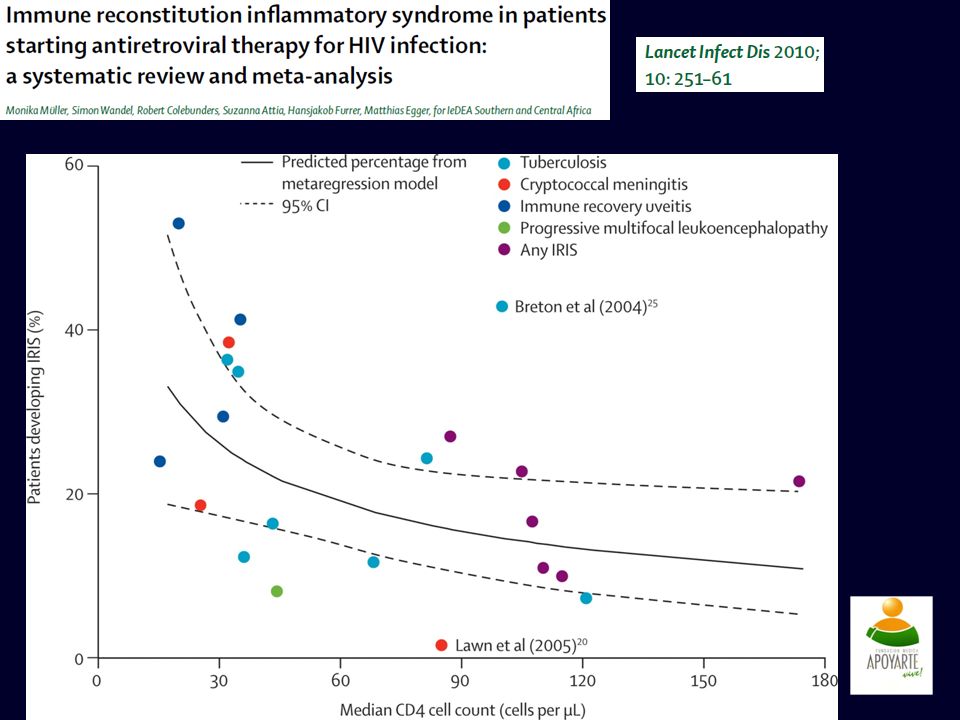
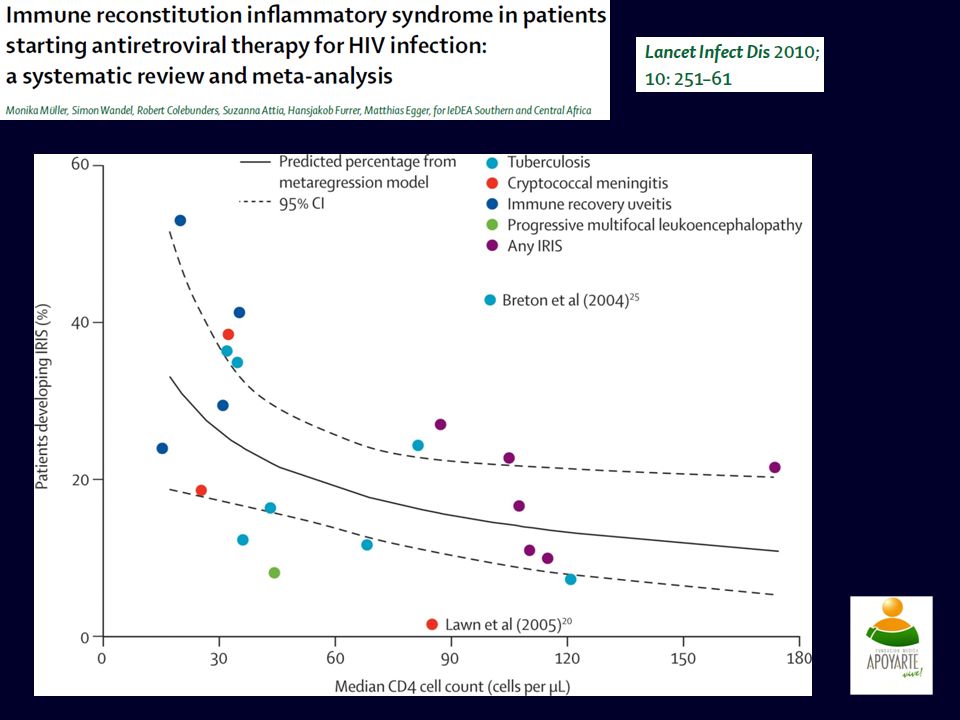
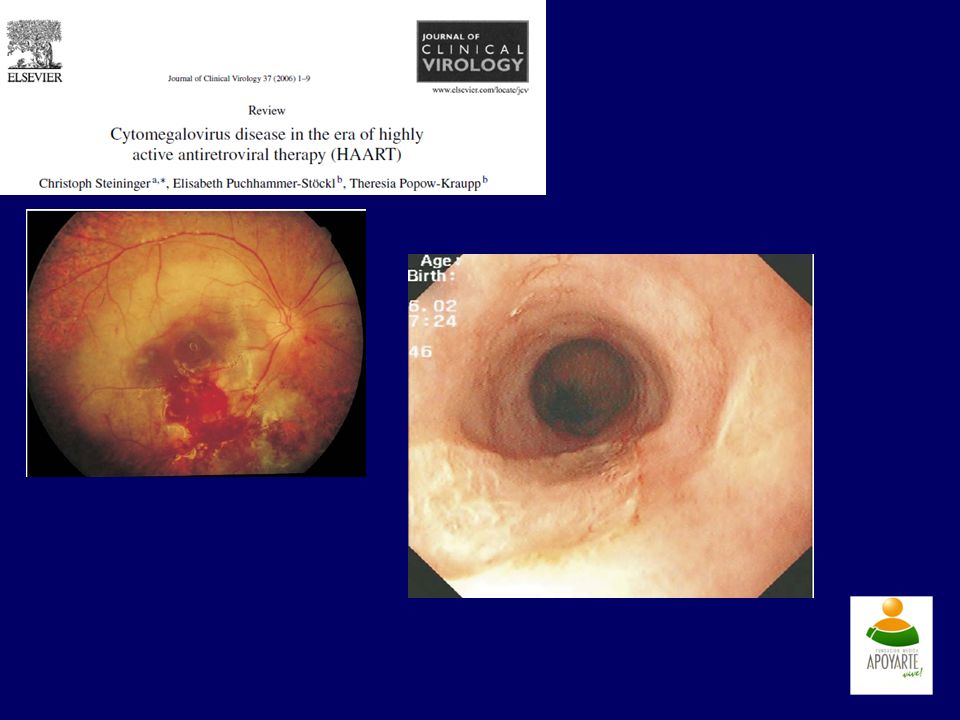
CMV como SRI Retinitis aguda tras inicio de TAR
5/418 pacientes (172 casos con Ig G +) PCR predictor de aparición Menos necrosis retiniana y mas inflamacion Vitritis en pacientes con historia pasada de retinitis. Afectación extraocular AIDS 1999;13:1497
 PCR predictor de aparición. Menos necrosis retiniana y mas inflamacion. Vitritis en pacientes con historia pasada de retinitis. Afectación extraocular. AIDS 1999;13:1497.")
59
GANCICLOVIR TRATAMIENTO
9-[2-HIDROXI-L-(HIDROXI-1-HIDROXIMETIL)-ETOXIMETIL] GUANINA. FOSCARNET CIDOFOVIR GANCICLOVIR
-ETOXIMETIL] GUANINA. FOSCARNET. CIDOFOVIR. GANCICLOVIR.")
60
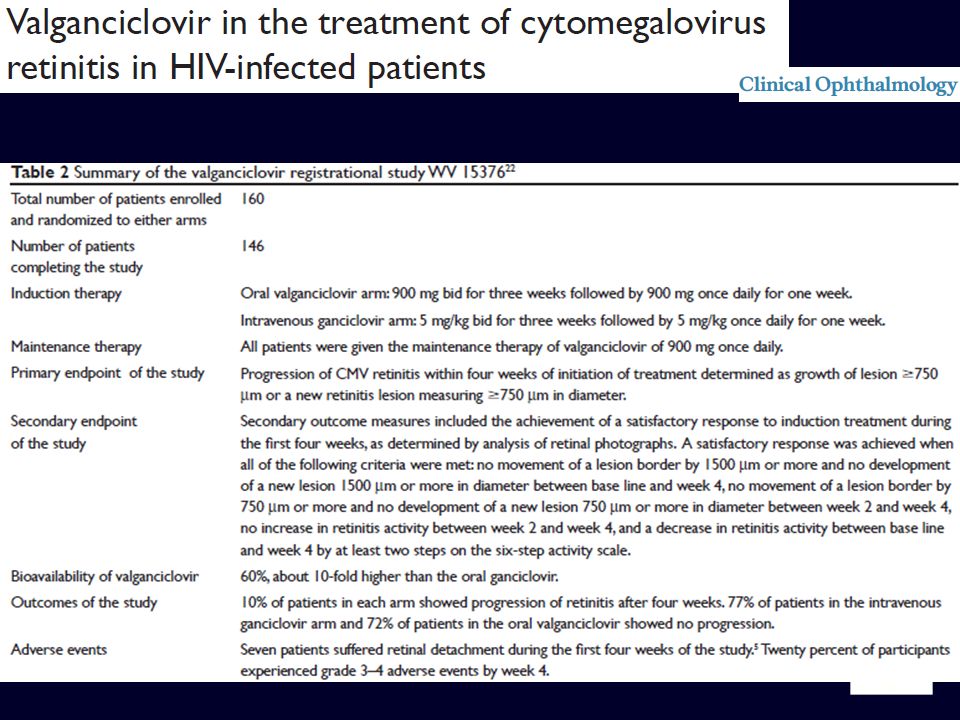
TRATAMIENTO medicamento Dosis y duración Mecanismo de acción
Efectos adversos Ganciclovir 5 mg IV c/12 horas por 2-4 semanas Inhibe ADN polimerasa Supresión medula ósea Nefrotoxicidad Valganciclovir 900 mg cada 12 horas Foscarnet 60 mg IV c/8 horas por 2-4 semanas Anemia, nefrotoxicidad Anemia, convulsiones Cidofovir 5 mg IV c/semana por 2 semanas, luego c/ 2 semanas Neutropenia Hipotonia ocular

62
Otras alternativas Vacunas Microbicidas CROI 2004;283:

Presentaciones similares