Descargar la presentación
La descarga está en progreso. Por favor, espere

1
AVANCES EN EL TRATAMIENTO DEL CÁNCER RENAL AVANZADO

2
CÁNCER RENAL AVANZADO. INTRODUCCION
30% de cáncer renal se presenta como enfermedad avanzada Pronóstico sombrío (spv 8 m) La inmunoterapia (IL-2 e IFN) era el tratamiento estándar hasta la fecha Recientemente se han identificado dianas específicas: fármacos antiangiogénicos (ITK y mAb) ASCO 06 estudio randomizado Sunitinib frente a IFN. Primer beneficio demostrado sobre inmunoterapia.
 La inmunoterapia (IL-2 e IFN) era el tratamiento estándar hasta la fecha. Recientemente se han identificado dianas específicas: fármacos antiangiogénicos (ITK y mAb) ASCO 06 estudio randomizado Sunitinib frente a IFN. Primer beneficio demostrado sobre inmunoterapia.")
3
CLASIFICACION HISTOLOGICA
Carcinoma de células claras (80%) es el más frecuente Carcinoma papilar (15%) Carcinoma cromófobo y oncocitoma (5%) Carcinoma de los conductos colectores (<1%) Variante sarcomatoide: puede coexistir con cualquiera de los subtipos anteriores y conlleva un comportamiento más agresivo del tumor.
 es el más frecuente. Carcinoma papilar (15%) Carcinoma cromófobo y oncocitoma (5%) Carcinoma de los conductos colectores (<1%) Variante sarcomatoide: puede coexistir con cualquiera de los subtipos anteriores y conlleva un comportamiento más agresivo del tumor.")
5
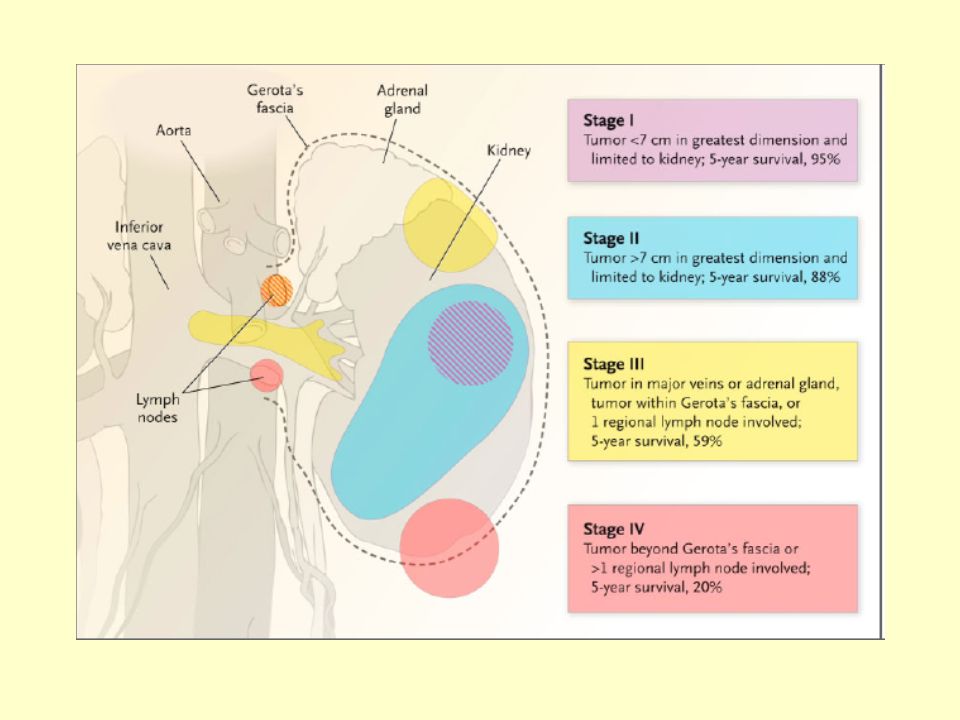
TRATAMIENTO DEL CÁNCER RENAL POR ESTADIOS
Estadios I y II Nefrectomía radical o parcial con o sin linfadenctomía regional Radioterapia paliativa Estadio III Nefrectomía radical Linfadenectomía regional Radioterapia paliativa Treatment strategies This table outlines the standard treatment for RCC at different stages. Surgical resection of the tumour is the primary treatment for localised RCC. This is achieved by radical nephrectomy, which involves the complete removal of Gerota’s fascia and its contents, including the kidney and the adrenal gland. Regional lymphadenectomy is often performed at the time of radical nephrectomy, although its role in prolonged survival has not been demonstrated.[1] In patients with metastatic disease, palliative nephrectomy and resection of metastases are often performed, although prolongation of survival seems to occur only in patients with solitary metastases. Metastatic RCC is largely a chemotherapy-resistant tumour, with modest response rates and no clearly demonstrated survival benefit. Hormonal therapy is also ineffective; a review by Kjaer concluded that RCC is neither hormone dependant nor hormone responsive.[2] Best results have been obtained with immunotherapy, which has demonstrated reproducible complete and durable tumour responses in a significant minority of patients. 1. Cancer: Principles and practice of oncology (5th edition). Devita VT, Hellman S, Rosenberg SA (eds); Lippincott-Raven Publishers: 1997. 2. Kjaer M. The role of medroxyprogesterone acetate (MPA) in the treatment of renal adenocarcinoma. Cancer Treat Rev 1988; 15: 195. Estadio IV Nefrectomía citorreductiva Resección de metástasis Radioterapia paliativa Tratamientos sistémicos: inmunoterapia, quimioterapia Antiangiogénicos
. Devita VT, Hellman S, Rosenberg SA (eds); Lippincott-Raven Publishers: Kjaer M. The role of medroxyprogesterone acetate (MPA) in the treatment of renal adenocarcinoma. Cancer Treat Rev 1988; 15: 195. Estadio IV. Nefrectomía citorreductiva. Resección de metástasis. Radioterapia paliativa. Tratamientos sistémicos: inmunoterapia, quimioterapia. Antiangiogénicos.")
6
INMUNOTERAPIA EN CÁNCER RENAL
15 años de experiencia con IL-2 e IFN Varios estudios fase II Fase III resultados heterogeneos Algunas regresiones tumorales en una enfermedad quimiorresistente

7
EL SISTEMA INMUNE PUEDE RECONOCER LAS CELULAS TUMORALES
The immune system can recognise tumour cells It is known that the immune system is capable of recognising tumour cells, offering a possible treatment strategy for cancer. This slide illustrates how tumour antigens are processed by the immune system and how this ultimately can result in tumour cell kill. First, dendritic cells capture antigens released by cancer cells. After intracellular processing, antigenic peptides are loaded onto major histocompatibility complex (MHC) molecules on the surface of the dendritic cell. Specific T-cells recognise these MHC-peptide complexes and are activated. The activated T-cells proliferate and secrete cytokines, in particular IL-2. Certain cytokines may have a direct cytotoxic effect on the tumour, whereas other cytokines (such as IL-2), act via further stimulation and activation of the effector mechanisms. Consequently, immunotherapy with cytokines has been identified as a potential cancer treatment strategy. IL = interleukin 2 GM-CSF = granulocyte-macrophage colony-stimulating factor Adapted from Armstrong A, et al. Br Med J 2001; 323: 1289
 molecules on the surface of the dendritic cell. Specific T-cells recognise these MHC-peptide complexes and are activated. The activated T-cells proliferate and secrete cytokines, in particular IL-2. Certain cytokines may have a direct cytotoxic effect on the tumour, whereas other cytokines (such as IL-2), act via further stimulation and activation of the effector mechanisms. Consequently, immunotherapy with cytokines has been identified as a potential cancer treatment strategy. IL-2 = interleukin 2 GM-CSF = granulocyte-macrophage colony-stimulating factor. Adapted from Armstrong A, et al. Br Med J 2001; 323:")
8
INMUNOTERAPIA EN CÁNCER RENAL
Interleukina 2 (IL-2) Altas dosis iv: U/kg cada 8 h cinco días consecutivos (máximo 14 dosis consecutivas) RR 15%, mediana duración 19 m (si RP), 60% > 90% regresión de enf mesurable Efectos adversos graves frecuentes (hospitalización) Dosis bajas iv no mantienen eficacia (menos RR) pero sin diferencia en spv Regímenes bajas dosis sc: RR 22%, duración 12 m, 5% spv a 10 a Efectos secundarios manejables (ambulatorio) F predictivos de respuesta: Expresión de CAIX en >85% Histología de cél claras con presencia de patrón alveolar Ausencia de m1 oseas y hepáticas MSKCC No comparativos frente a placebo
 Altas dosis iv: U/kg cada 8 h cinco días consecutivos (máximo 14 dosis consecutivas) RR 15%, mediana duración 19 m (si RP), 60% > 90% regresión de enf mesurable. Efectos adversos graves frecuentes (hospitalización) Dosis bajas iv no mantienen eficacia (menos RR) pero sin diferencia en spv. Regímenes bajas dosis sc: RR 22%, duración 12 m, 5% spv a 10 a. Efectos secundarios manejables (ambulatorio) F predictivos de respuesta: Expresión de CAIX en >85% Histología de cél claras con presencia de patrón alveolar. Ausencia de m1 oseas y hepáticas. MSKCC. No comparativos frente a placebo.")
9
INMUNOTERAPIA EN CÁNCER RENAL
Interferon (IFN ) Monoterapia RR 15%, duración 4 m Dosis diarias de 5-10 mU Varios estudios aleatorizados han evaluado el impacto de IFN en spv demostrando un modesto beneficio Fase III Vinblastina frente a Vinblastina+IFN con mejor supervivencia para el tratamiento combinado (38 vs 68 sem) Estudio comparativo entre IFN y acetato de megestrol demuestra un 28% de reducción en el riesgo de muerte a favor de interferon y un aumento significativo en la mediana de supervivencia (8.5 vs 6 m). Fármaco adecuado para combinar con nuevas dianas terapéuticas y se convierte en la rama control de estudios fase III.
 Monoterapia RR 15%, duración 4 m. Dosis diarias de 5-10 mU. Varios estudios aleatorizados han evaluado el impacto de IFN en spv demostrando un modesto beneficio. Fase III Vinblastina frente a Vinblastina+IFN con mejor supervivencia para el tratamiento combinado (38 vs 68 sem) Estudio comparativo entre IFN y acetato de megestrol demuestra un 28% de reducción en el riesgo de muerte a favor de interferon y un aumento significativo en la mediana de supervivencia (8.5 vs 6 m). Fármaco adecuado para combinar con nuevas dianas terapéuticas y se convierte en la rama control de estudios fase III.")
10
INMUNOTERAPIA EN CÁNCER RENAL
Combinación IL-2 + IFN: Fase III francés con 425 pacientes comparó IL-2 dosis intermedias vs IFN vs IL-2 + IFN, la tasa de respuestas fue superior para la combinación (6.5% vs 7.5% vs 18.6 %), tambien mejoró la SLE sin embargo no hubo diferencias significativas en OS Negrier S. N Engl J Med 1998;338:1272.
, tambien mejoró la SLE sin embargo no hubo diferencias significativas en OS. Negrier S. N Engl J Med 1998;338:1272.")
11
Inmunoterapia en estudios Fase III
Regimen Nº de Pts % Respuesta spv MRCRCC IFN MPA 174 176 14% 2% SI Gordon et al IFN + Thalidomide 169 175 8% 3% No Negrier et al IL-2 IL-2 + IFN 138 147 140 7% 19% Yang et al High dose IL-2 Low dose IL-2 SC IL-2 96 92 93 21% 11% 10% 1Lancet 1999;353:14; 2ASCO 2004, Abs 4516; 3NEJM 1998;338:1272; 4JCO 2003;21:3127; *Medroxyprogesterone

12
FACTORES PRONOSTICOS SLP SG
Cinco factores predictores de peor supervivencia: IK < 80% LDH > 1.5 veces el valor normal Hb por debajo del valor normal Calcio > 10 mg/dl Intervalo < 1 año desde nefrectomía SLP SG Riesgo favorable (0) m m Riesgo intermedio (1-2) m m Riesgo desfavorable (3-5) m m Motzer RJ J Clin Oncol 2002; 20:289
 8.3 m 30 m. Riesgo intermedio (1-2) 5.3 m 14 m. Riesgo desfavorable (3-5) 2.5 m 5 m. Motzer RJ J Clin Oncol 2002; 20:289.")
13
INMUNOTERAPIA TRAS NEFRECTOMÍA
Beneficio en supervivencia en pacientes sometidos a nefrectomía previa a la administración de inmunoterapia demostrado en dos estudios aleatorizados Supervivencia mediana (meses) SWOG 11.1 (n=120) 8.1 (n=121) 1 EORTC 2 Nefrectomía radical + IFN - 17.0 IL-2 based immunotherapy after nephrectomy Two randomised studies have been carried out, one by the Southwest Oncology Group (SWOG) and the other by the European Organisation for Research and Treatment of Cancer (EORTC) Genitourinary Group, to establish whether nephrectomy prior to immunotherapy with IFN- improved overall survival in patients with metastatic RCC compared to treatment with immunotherapy alone.[1,2] In the SWOG trial, patients were randomly assigned to two treatment groups. The first group underwent radical nephrectomy followed by IFN- therapy (n=120), while the second group received IFN- alone (n=121). The median survival in the first group was 11.1 months, compared to 8.1 months with immunotherapy alone (p=0.05).[1] In the EORTC trial, 83 patients were randomised to either radical nephrectomy plus IFN- immunotherapy or to IFN- alone. Time to progression (5 vs 3 months) and median duration of survival (17 vs 7 months) were significantly longer in those patients who had undergone prior nephrectomy.[2] Both trials therefore clearly indicate an important survival benefit for patients undergoing nephrectomy prior to immunotherapy treatment. 1. Flanigan RC, Salmon SE, Blumenstein BA, et al. Nephrectomy followed by interferon alfa-2b compared with interferon alfa-2b alone for metastatic renal cell cancer. N Engl J Med 2001; 345: 1655–9. 2. Mickisch GH, Garin A, van Poppel H, and the EORTC Genitourinary Group. Radical nephrectomy plus interferon-alfa-based immunotherapy compared with interferon-alfa alone in metastatic renal cell carcinoma: a randomised trial. Lancet 2001; 358: 966–70. a (n=42) IFN- solo 7.0 (n=43) 1Flanigan RC, et al. N Eng J Med 2001; 345: 1655; 2Mickisch GHJ, et al. Lancet 2001; 358: 966
 SWOG (n=120) 8.1. (n=121) 1. EORTC. 2. Nefrectomía radical. + IFN IL-2 based immunotherapy after nephrectomy. Two randomised studies have been carried out, one by the Southwest Oncology Group (SWOG) and the other by the European Organisation for Research and Treatment of Cancer (EORTC) Genitourinary Group, to establish whether nephrectomy prior to immunotherapy with IFN- improved overall survival in patients with metastatic RCC compared to treatment with immunotherapy alone.[1,2] In the SWOG trial, patients were randomly assigned to two treatment groups. The first group underwent radical nephrectomy followed by IFN- therapy (n=120), while the second group received IFN- alone (n=121). The median survival in the first group was 11.1 months, compared to 8.1 months with immunotherapy alone (p=0.05).[1] In the EORTC trial, 83 patients were randomised to either radical nephrectomy plus IFN- immunotherapy or to IFN- alone. Time to progression (5 vs 3 months) and median duration of survival (17 vs 7 months) were significantly longer in those patients who had undergone prior nephrectomy.[2] Both trials therefore clearly indicate an important survival benefit for patients undergoing nephrectomy prior to immunotherapy treatment. 1. Flanigan RC, Salmon SE, Blumenstein BA, et al. Nephrectomy followed by interferon alfa-2b compared with interferon alfa-2b alone for metastatic renal cell cancer. N Engl J Med 2001; 345: 1655–9. 2. Mickisch GH, Garin A, van Poppel H, and the EORTC Genitourinary Group. Radical nephrectomy plus interferon-alfa-based immunotherapy compared with interferon-alfa alone in metastatic renal cell carcinoma: a randomised trial. Lancet 2001; 358: 966–70. a. (n=42) IFN- solo (n=43) 1Flanigan RC, et al. N Eng J Med 2001; 345: 1655; 2Mickisch GHJ, et al. Lancet 2001; 358: 966.")
14
IL-2 based immunotherapy after nephrectomy
IL-2 TRAS NEFRECTOMIA Análisis retrospectivo de supervivencia en pacientes con mRCC tratados con nefrectomía + IL-2, nefrectomía + IFN-, or IFN- solo Nefrectomía + IL-2 Nefrectomía + IFN- IFN- solo P < 0.05 IL-2 based immunotherapy after nephrectomy The SWOG and EORTC studies did not address the question of what type of immunotherapy is most effective following nephrectomy. To answer this question Pantuck et al. retrospectively analysed the records of 89 metastatic RCC patients who had been treated with IL-2 after nephrectomy, and compared the survival of these patients with the 120 patients from the SWOG study who received IFN- post-nephrectomy.[1] The median survival of patients who underwent nephrectomy and subsequently received IL-2 was 16.7 months, whereas the median survival of the patients who received IFN- post-nephrectomy was 11.1 months (p<0.05). The 5-year survival was considerably higher for nephrectomised patients who received IL-2 than for those who received IFN- (20% vs 10%).[2] 1. Pantuck AJ, Belldegrun AS, Figlin RA. Nephrectomy and interleukin-2 for metastatic renal cell carcinoma. N Engl J Med 2001; 345: 1711–2. 2. Pantuck AJ, Zisman A, Chao D, et al. A comparison of interferon versus interleukin-2 following nephrectomy for metastatic renal cell carcinoma. ASCO 2002: Abstract 755. Mejores resultados con nefrectomía + IL-2 Supervivencia mediana 16.7 meses Spv a 5 años 20% Pantuck AJ, et al. N Engl J Med 2001; 345: 1711
. The 5-year survival was considerably higher for nephrectomised patients who received IL-2 than for those who received IFN- (20% vs 10%).[2] 1. Pantuck AJ, Belldegrun AS, Figlin RA. Nephrectomy and interleukin-2 for metastatic renal cell carcinoma. N Engl J Med 2001; 345: 1711–2. 2. Pantuck AJ, Zisman A, Chao D, et al. A comparison of interferon versus interleukin-2 following nephrectomy for metastatic renal cell carcinoma. ASCO 2002: Abstract 755. Mejores resultados con nefrectomía + IL-2. Supervivencia mediana 16.7 meses. Spv a 5 años 20% Pantuck AJ, et al. N Engl J Med 2001; 345:")
15
INMUNOTERAPIA EN CÁNCER RENAL
Análisis Cochrane inmunoterapia en mRCC 52 estudios randomizados 5989 pacientes 685 (11%) RP o RC (0-39 %) RC observadas en 2.9% de población evaluada Mediana supervivencia 13.3 m (6-27 m) No correlación entre tasa de remisiones y OS El impacto de IL-2 en spv no ha sido realmente investigado y su uso está basado en la tasa de RR IFN consigue discreta mejoría en spv y es una opción en pacientes ambulatorios con buen PS
 RP o RC (0-39 %) RC observadas en 2.9% de población evaluada. Mediana supervivencia 13.3 m (6-27 m) No correlación entre tasa de remisiones y OS. El impacto de IL-2 en spv no ha sido realmente investigado y su uso está basado en la tasa de RR. IFN consigue discreta mejoría en spv y es una opción en pacientes ambulatorios con buen PS.")
16
Patogénesis del CCR

17
Vías moleculares en RCC

18
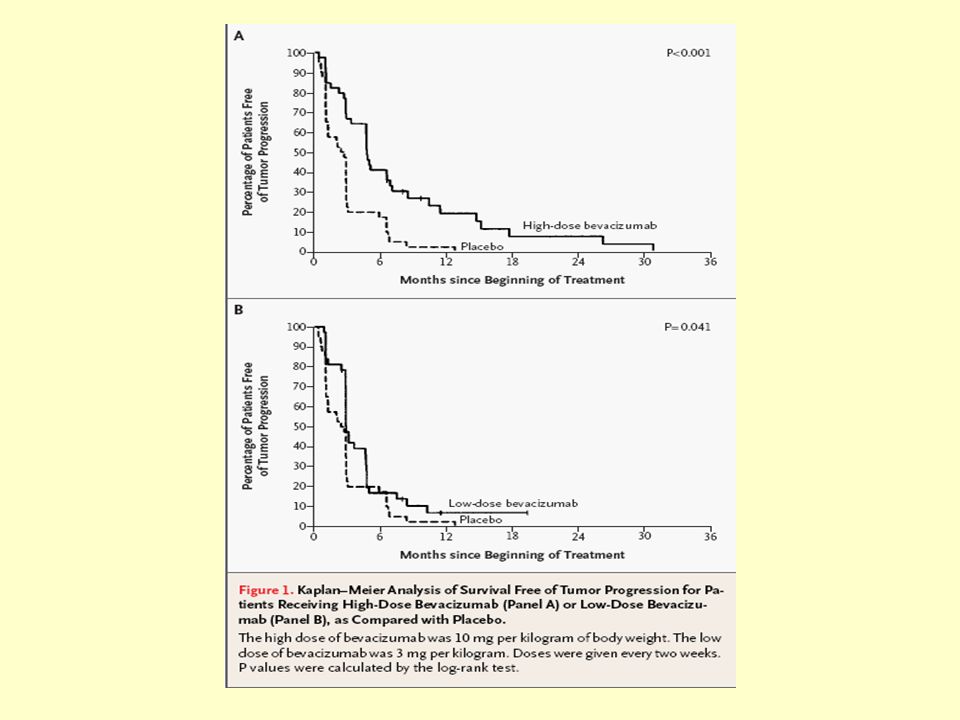
BEVACIZUMAB (Avastin )
Mab anti-VEGF Fase II randomizado pacientes mRCC refractarios n=116, dos dosis (3 y 10 mg/kg cada 2 sem) vs placebo, mediana seguimiento 27 m, RP 10% TTP 4.8 m vs 2.5 m (p<0.001) favorable a la dosis alta frente a placebo, sin diferencia en OS. Yang JC, N Engl J Med 2003; 349:427
 vs placebo, mediana seguimiento 27 m, RP 10% TTP 4.8 m vs 2.5 m (p<0.001) favorable a la dosis alta frente a placebo, sin diferencia en OS. Yang JC, N Engl J Med 2003; 349:427.")
20
BEVACIZUMAB (Avastin )
Fase III en primera linea mRCC en curso: IFNa2b 9 mU sc (3/sem) vs IFN+Bevacizumab 10 mg/kg cada 2 sem Objetivo primario: OS Bevacizumab en combinación con IL-2 en curso Fase II Bevacizumab + erlotinib: RO 25%, 61% EE, seguimiento 15 m spv 18 m 60% (1) Fase II randomizado misma combinación en 1ª linea (n=100) no ventaja en RR ni SLP (1) Hainsworth JD, J Clin Oncol 2005; 23:7889.
 vs IFN+Bevacizumab 10 mg/kg cada 2 sem. Objetivo primario: OS. Bevacizumab en combinación con IL-2 en curso. Fase II Bevacizumab + erlotinib: RO 25%, 61% EE, seguimiento 15 m spv 18 m 60% (1) Fase II randomizado misma combinación en 1ª linea (n=100) no ventaja en RR ni SLP. (1) Hainsworth JD, J Clin Oncol 2005; 23:7889.")
21
Sorafenib es activo contra el tumor y la vascularización
Tumor cell Blood vessel cell [slide 2] BAY : A Novel Oral Multi-Kinase Inhibitor that Acts on the Tumor and Vasculature1 BAY is a novel oral multi-kinase inhibitor that targets serine/threonine and receptor tyrosine kinases in both the tumor cell and tumor vasculature. In preclinical models, BAY prevented tumor growth by combining two anticancer activities: inhibition of tumor cell proliferation and tumor angiogenesis. In preclinical studies BAY was shown to inhibit tumor cell proliferation by targeting the Raf/MEK/ERK signaling pathway at the level of Raf. BAY also demonstrated an antiangiogenic effect by targeting the receptor tyrosine kinases VEGFR-2 and PDGFR and their associated signaling cascades. Idea of vertical and horizontal inhibition Sorafenib has been shown to inhibit tumor cell proliferation in vitro by targeting the Raf/MEK/ERK signaling pathway at the level of Raf kinase Sorafenib demonstrated an antiangiogenic effect in vitro by targeting the receptor tyrosine kinases VEGFR-2 and PDGFR and their associated signaling cascades *Both anticancer activities were observed in preclinical models Wilhelm S et al. Cancer Res. 2004;64:7099–109 1. Wilhelm S, Carter C, Tang LY, et al. BAY exhibits broad spectrum oral antitumor activity and targets the Raf/MEK/ERK pathway and receptor tyrosine kinases involved in tumor progression and angiogenesis. Cancer Res. 2004;64:7099–109

22
SORAFENIB (Nexavar, BAY 43-9006)
Inhibidor dual: Raf kinasa y VEGFR/PDGFR Inhibe proliferación célula tumoral y angiogénesis Dosis 400 mg dos veces/día v.o. Fase II discontinuación randomizada mRCC n=202, a las 12 sem: si cambios <25% frente al basal, randomizados a Sorafenib vs placebo 12 sem más >25 % reducción continuaban con sorafenib pacientes con >25% crecimiento, discontinuación tto. Objetivo primario: porcentaje de pacientes randomizados libres de progresión a las 24 sem Resultados: 50% pacientes sorafenib vs 18% placebo libres de progresión (p ) Mediana SLP mayor para sorafenib (24 sem) frente a placebo (6 sem) p Efectos secundarios: HFS, rash cutaneo, HTA, astenia
 Mediana SLP mayor para sorafenib (24 sem) frente a placebo (6 sem) p Efectos secundarios: HFS, rash cutaneo, HTA, astenia.")
23
SORAFENIB (Nexavar, BAY 43-9006)
Fase III controlado con placebo 903 pacientes refractarios a CK demostró una ventaja en SLP favorable al brazo de tratamiento (24 vs 12 sem p< ) a pesar de RO 2% RECIST (76% EE). Ventaja SLP en todos subgrupos pcos. Pacientes de la rama placebo fueron cruzados a sorafenib, datos confusos de OS Sorafenib aprobado diciembre 05 por FDA para tto cáncer renal avanzado En investigación: combinación con Avastin, fase II refractarios a Avastin y sunitinib, combinación con IFN frente a IFN solo, randomizado combinación con Avastin y Tensirolimus…
 a pesar de RO 2% RECIST (76% EE). Ventaja SLP en todos subgrupos pcos. Pacientes de la rama placebo fueron cruzados a sorafenib, datos confusos de OS. Sorafenib aprobado diciembre 05 por FDA para tto cáncer renal avanzado. En investigación: combinación con Avastin, fase II refractarios a Avastin y sunitinib, combinación con IFN frente a IFN solo, randomizado combinación con Avastin y Tensirolimus…")
24
SUNITINIB (Sutent, SU 11248)
Inhibidor potente y selectivo de VEGFR-2 y PDGFR-B, FLT-3, c-Kit Dosis 50 mg/dia v.o. 4 sem-2 sem descanso Dos fase II en refractarios a CK (RR 39 y 40%, EE 28 y 23%, PD 25 y 31%). Toxicidad G1-2 y algún G3 (astenia, diarrea, nauseas) TTP 8.7 m y OS 16.4 m, en el otro no alcanzada) Beneficio clínico 70-75% pacientes Aprobado FDA enero 06
. Toxicidad G1-2 y algún G3 (astenia, diarrea, nauseas) TTP 8.7 m y OS 16.4 m, en el otro no alcanzada) Beneficio clínico 70-75% pacientes. Aprobado FDA enero 06.")
25
Mecanismo de acción Sunitinib
Pérdida de función de proteina VHL ↑ VEGF ↑ PDGF VEGF PDGF VEGFR PDGFR Pericito/Fibroblasto/ Músculo liso vascuar célula vascular endotelial Sunitinib Permeabilidad vascular Supervivencia celular proliferación, migración Formación y maduración vascular Inhibición de la patogénesis y progresión en RCC

26
Sunitinib 2ª línea Referencia n RR (%) Sunitinib en tto 2ª línea
Ensayo 1 Ensayo 2 Motzer et al Motzer et al 63 106 40% % Tto de 2ª línea convencional Citoquinas Varios (datos históricos) Escudier et al Motzer et al 3% 4% Tto de 1ª línea convencional Interferon-alfa Altas dosis Interleukina-2 Motzer et al Fyfe et al 11% % 1JCO 2006;24:16-24; 2ASCO 2005; Abs 4508; 3JCO 1999;17: ; 4JCO 2004;22: ; 5JCO 2002;20: ; 6JCO 1995;13:
 Escudier et al Motzer et al % 4% Tto de 1ª línea convencional. Interferon-alfa Altas dosis Interleukina-2. Motzer et al Fyfe et al % 14% 1JCO 2006;24:16-24; 2ASCO 2005; Abs 4508; 3JCO 1999;17: ; 4JCO 2004;22: ; 5JCO 2002;20: ; 6JCO 1995;13:")
27
Fase III ASCO 06 R A N D O M I Z C N=750 Estratificación
LDH 1.5 vs >1.5xULN ECOG PS 0 vs 1 Presencia vs ausencia de nefrectomía Sunitinib (N=375) An ongoing phase III is comparing SUTENT with interferon-alpha (IFN-) as first-line therapy in patients with metastatic clear-cell RCC. The intent of this trial is to obtain information about the efficacy and safety of SUTENT when used as initial therapy in this condition, compared with a standard cytokine-based alternative therapy. This is a randomized, open-label, multicenter trial comparing oral SUTENT therapy with subcutaneously injected IFN- therapy in patients with metastatic RCC that had not been previously treated with systemic immunotherapy, chemotherapy, or hormonal therapy, or with any other investigational systemic therapy. The projected accrual for this trial is a total of 690 patients, 345 in each treatment arm. SUTENT will be administered according to the standard regimen used in the phase II trials: 50 mg/day in repeated 6-week cycles consisting of 4 weeks’ consecutive on treatment, followed by 2 weeks’ off treatment. IFN- will be administered as 9 million units (MU) three times daily. The primary end point is progression-free survival (PFS). Secondary end points include RECIST-defined overall response rate and overall survival. Data on file. Pfizer Inc, New York, NY. IFN- (N=375)
 An ongoing phase III is comparing SUTENT with interferon-alpha (IFN-) as first-line therapy in patients with metastatic clear-cell RCC. The intent of this trial is to obtain information about the efficacy and safety of SUTENT when used as initial therapy in this condition, compared with a standard cytokine-based alternative therapy. This is a randomized, open-label, multicenter trial comparing oral SUTENT therapy with subcutaneously injected IFN- therapy in patients with metastatic RCC that had not been previously treated with systemic immunotherapy, chemotherapy, or hormonal therapy, or with any other investigational systemic therapy. The projected accrual for this trial is a total of 690 patients, 345 in each treatment arm. SUTENT will be administered according to the standard regimen used in the phase II trials: 50 mg/day in repeated 6-week cycles consisting of 4 weeks’ consecutive on treatment, followed by 2 weeks’ off treatment. IFN- will be administered as 9 million units (MU) three times daily. The primary end point is progression-free survival (PFS). Secondary end points include RECIST-defined overall response rate and overall survival. Data on file. Pfizer Inc, New York, NY. IFN- (N=375)")
28
Study Objectives Progression-free survival
Primary Endpoint Progression-free survival 90% power to detect a 35% improvement (4.6 months* 6.2 months) Assessment by independent central review Response rate, overall survival, safety, and patient reported outcomes Secondary Endpoint *Motzer et al. JCO 2002;20:
 Assessment by independent central review. Response rate, overall survival, safety, and patient reported outcomes. Secondary Endpoint. *Motzer et al. JCO 2002;20:")
29
Study Treatment Repeated 6-week cycles Response and safety assessments
Arm A: Sunitinib 50 mg po daily on Schedule 4/ (4 weeks on/2 weeks off) Arm B: IFN- 3 MU TIW 1st week 6 MU TIW 2nd week 9 MU TIW 3rd week thereafter; SC Injection vs Repeated 6-week cycles Response and safety assessments Dose reduction for toxicity Treatment continued unless progression or intolerance
 Arm B: IFN- 3 MU TIW 1st week 6 MU TIW 2nd week 9 MU TIW 3rd week thereafter; SC Injection. vs. Repeated 6-week cycles. Response and safety assessments. Dose reduction for toxicity. Treatment continued unless progression or intolerance.")
30
Patient Disposition & Treatment Administered
Sunitinib (n=375) IFN- (n=375) Treatment ongoing (n) 248 126 Median duration of treatment (mos, range) 6 (<1–15+) 4 (<1–13+) Reason for discontinuation, n (%) Progressive disease 92 (25) 170 (45) Adverse event 30 (8) 47 (13) Consent withdrawn 4 (1) 31 (8)* Protocol violation 1 (<1) *15 pts (4%) randomized to IFN-α withdrew prior to starting treatment
 IFN- (n=375) Treatment ongoing (n) Median duration of treatment (mos, range) 6 (<1–15+) 4 (<1–13+) Reason for discontinuation, n (%) Progressive disease. 92 (25) 170 (45) Adverse event. 30 (8) 47 (13) Consent withdrawn. 4 (1) 31 (8)* Protocol violation. 1 (<1) *15 pts (4%) randomized to IFN-α withdrew prior to starting treatment.")
31
Best Response by RECIST
(Investigator Assessment) Response Sunitinib IFN- Pts with measurable disease at baseline (n) 374 373 Objective response* Complete response Partial response 137 (37%) 1 136 33 (9%) 0 33 Stable disease 176 (47%) 213 (57%) Progressive disease/Not evaluable 61 (16%) 127 (34%) *Sunitinib vs IFN-α: P <
 Response. Sunitinib. IFN- Pts with measurable disease at baseline (n) Objective response* Complete response Partial response. 137 (37%) (9%) Stable disease. 176 (47%) 213 (57%) Progressive disease/Not evaluable. 61 (16%) 127 (34%) *Sunitinib vs IFN-α: P <")
32
Best Response by RECIST
(Independent Central Review) Response Sunitinib IFN- Pts with measurable disease at baseline* (n) 335 327 Objective response** Complete response Partial response 103 (31%) 0 103 20 (6%) 0 20 Stable disease 160 (48%) 160 (49%) Progressive disease/Not evaluable 72 (21%) 147 (45%) **Sunitinib vs IFN-α: P < *88 patients not yet assessed by central review
 Response. Sunitinib. IFN- Pts with measurable disease at baseline* (n) Objective response** Complete response Partial response. 103 (31%) (6%) Stable disease. 160 (48%) 160 (49%) Progressive disease/Not evaluable. 72 (21%) 147 (45%) **Sunitinib vs IFN-α: P < *88 patients not yet assessed by central review.")
33
Supervivencia libre de progression
1 2 3 4 5 6 7 8 9 10 11 12 13 14 Tiempo (meses) 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0 Supervivencia libre de progresión Sunitinib Mediana: 11 meses (95% CI: 10–12) IFN- Mediana: 5 meses (95% CI: 4–6) Hazard Ratio = 0.415 (95% CI: 0.320–0.539) P < No. at Risk Sunitinib: No. at Risk IFN-:
 Supervivencia libre de progresión. Sunitinib. Mediana: 11 meses. (95% CI: 10–12) IFN- Mediana: 5 meses. (95% CI: 4–6) Hazard Ratio = (95% CI: 0.320–0.539) P < No. at Risk Sunitinib: No. at Risk IFN-:")
34
Hazard Ratios según categorías de riesgo MSKCC (Independent Central Review)
Sunitinib benefit IFN- benefit Sunitinib vs. IFN- treatment effect without adjusting for risk factors Prior nephrectomy (yes vs no) ECOG score (0 vs 1) LDH (≤1.5 vs >1.5 x ULN) Time since diagnosis (≥1 yr vs <1 yr) Hemoglobin (≥LLN vs <LLN) Corrected calcium (≤10 vs >10 mg/dL) LLN = lower limit of normal ULN = upper limit of normal * Cox proportional hazards analysis; Motzer et al. JCO 1999;17: ; Motzer et al. JCO 2002;20:
 ECOG score (0 vs 1) LDH (≤1.5 vs >1.5 x ULN) Time since diagnosis (≥1 yr vs <1 yr) Hemoglobin (≥LLN vs <LLN) Corrected calcium (≤10 vs >10 mg/dL) LLN = lower limit of normal ULN = upper limit of normal. * Cox proportional hazards analysis; Motzer et al. JCO 1999;17: ; Motzer et al. JCO 2002;20:")
35
Supervivencia libre de progresion según categoría de riesgo MSKCC
(Independent Central Review) MSKCC Risk Factors: 0 (Favorable) MSKCC risk factors: 1-2 (Intermediate) 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Time (Months) 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0 Progression Free Survival Probability Sunitinib (n=143) Median not been reached IFN- (n=121) Median: 8 months (95% CI: 7–NA) Hazard Ratio = 0.371 (95% CI: 0.214–0.643) Sunitinib (n=209) Median: 11 months (95% CI: 11–11) IFN- (n=212) Median: 4 months (95% CI: 3–4) Hazard Ratio = 0.388 (95% CI: 0.281–0.537) *Motzer et al. JCO 2002;20: ; Excludes 17 pts from IFN- with missing data
 MSKCC Risk Factors: 0. (Favorable) MSKCC risk factors: 1-2 (Intermediate) Time (Months) Progression Free Survival Probability. Sunitinib (n=143) Median not been reached. IFN- (n=121) Median: 8 months. (95% CI: 7–NA) Hazard Ratio = (95% CI: 0.214–0.643) Sunitinib (n=209) Median: 11 months. (95% CI: 11–11) IFN- (n=212) Median: 4 months. (95% CI: 3–4) Hazard Ratio = (95% CI: 0.281–0.537) *Motzer et al. JCO 2002;20: ; Excludes 17 pts from IFN- with missing data.")
36
Treatment-Related Adverse Events
Sunitinib (%) IFN- (%) All grade Grade 3/4 Fatigue 51 7 11/<1* Diarrhea 53 5* 13 Nausea 44 3 33 1 Stomatitis 25 2 <1 Hypertension 24 8* Hand-foot syndrome 20 Ejection fraction decline 10 Pyrexia 34 Chills 6 29 Myalgia 5 16 Flu-like symptoms 8 * Greater frequency, P <0.05
 IFN- (%) All grade. Grade 3/4. Fatigue /<1* Diarrhea * 13. Nausea Stomatitis <1. Hypertension * Hand-foot syndrome. 20. Ejection fraction decline. 10. Pyrexia. 34. Chills Myalgia Flu-like symptoms. 8. * Greater frequency, P <0.05.")
37
Supervivencia global Sunitinib (n=375) Median not reached
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Time (Months) 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0 Overall Survival Probability Sunitinib (n=375) Median not reached IFN- (N=375) Hazard Ratio = 0.65 (95% CI: 0.449–0.942) P = * No. at Risk Sunitinib: No. at Risk IFN-: *The observed p-value did not meet the pre-specified level of significance for this interim analysis
 Overall Survival Probability. Sunitinib (n=375) Median not reached. IFN- (N=375) Hazard Ratio = (95% CI: 0.449–0.942) P = * No. at Risk Sunitinib: No. at Risk IFN-: *The observed p-value did not meet the pre-specified level of significance for this interim analysis.")
38
*Sunitinib vs IFN-: P <0.000001
Outcome Summary Sunitinib IFN- Median Progression-free Survival*, mos (95% CI) Independent Review Investigator 11 (10-12) 11 (8-14) 5 (4-6) 4 (4-5) Objective response*, % (95% CI) 31 (26-36) 37 (32-42) 6 (4-9) 9 (6-12) Safety Acceptable — Patient-reported Outcomes Superior *Sunitinib vs IFN-: P <
 Independent Review Investigator. 11 (10-12) 11 (8-14) 5 (4-6) 4 (4-5) Objective response*, % (95% CI) 31 (26-36) 37 (32-42) 6 (4-9) 9 (6-12) Safety. Acceptable. — Patient-reported Outcomes. Superior. *Sunitinib vs IFN-: P <")
39
SUNITINIB (Sutent, SU 11248)
Primera demostración beneficio sobre inmunoterapia en estudio fase III en primera línea. Nuevo estándar en tto de cancer renal avanzado Fase II Sunitinib en mRCC refractarios a Bevacizumab (Rini) Al menos 4 dosis Avastin previas Objetivo: ORR N=61 Sutent 50 mg v.o. 4 sem cada 6 sem RECIST Evaluación cada 2 ciclos RP 23 % SD 57% SLP 29.7 sem Ef adversos: astenia, diarrea, mucositis, disgeusia, HTA
 Al menos 4 dosis Avastin previas. Objetivo: ORR. N=61 Sutent 50 mg v.o. 4 sem cada 6 sem. RECIST Evaluación cada 2 ciclos. RP 23 % SD 57% SLP 29.7 sem. Ef adversos: astenia, diarrea, mucositis, disgeusia, HTA.")
40
FASE III Tensirolimus vs IFNα vs combinación ambos (Hudes)
TEMSR (CCI-779) mTOR(-) Fase II en pacientes mal pronóstico (n111) TTP 5.8 m OS 15 m Sinérgico con IFN 15 mg iv + 6mU sc x 3 Fase III n 626 julio 03 1ª linea RCC m1 >o= 3-6 fact riesgo tres ramas: IFN 18 mU sc TIW TEMSR 25 mg iv sem TEMSR 15 mg iv sem + IFN 6mU sc TIW
 mTOR(-) Fase II en pacientes mal pronóstico (n111) TTP 5.8 m OS 15 m. Sinérgico con IFN 15 mg iv + 6mU sc x 3. Fase III n 626 julio 03 1ª linea RCC m1 >o= 3-6 fact riesgo tres ramas: IFN 18 mU sc TIW. TEMSR 25 mg iv sem. TEMSR 15 mg iv sem + IFN 6mU sc TIW.")
41
FASE III Tensirolimus vs IFNα vs combinación ambos (Hudes)
Pacientes: RECIST, 1ª linea m1, colesterol <350, TG <400, pobre pronóstico (IK 60%, LDH >1.5, Hb, Ca >10, dco < 1 a, m1 múltiples órganos) Objetivo primario: OS mejoría 40 % “ secundarios: PFS, TTF, OR, beneficio clínico Resultados: 49 % aumento OS TEMSR frente IFN. 15% aumento OS de la combinación frente IFN
 Objetivo primario: OS mejoría 40 % secundarios: PFS, TTF, OR, beneficio clínico. Resultados: 49 % aumento OS TEMSR frente IFN. 15% aumento OS de la combinación frente IFN.")
42
FASE III Tensirolimus vs IFNα vs combinación ambos (Hudes)
OS TEMSR 10.9 m vs 7.3 m IFN vs 8.4 m combinación PFS similar 2 ramas TEMSR 3.7 m vs 1.9 m IFN monoterapia (p ) Ef adversos: astenia, anemia, nausea , disnea y rash TEMSR mejor tolerancia TEMSR 16% reducción proporción pacientes tox G3-4 Frecuencia G3-4: 69% TEMSR, 85% IFN, 87% combinación (p < 0.001)
 Ef adversos: astenia, anemia, nausea , disnea y rash TEMSR. mejor tolerancia TEMSR 16% reducción proporción pacientes tox G3-4. Frecuencia G3-4: 69% TEMSR, 85% IFN, 87% combinación (p < 0.001)")
43
FASE III Tensirolimus vs IFNα vs combinación ambos (Hudes)
TEMSR 25 mg IV mejora OS y PFS en pacientes mal pco TEMSR combinado con IFN no mejora OS comparado con IFN Nuevo estandar pacientes RCC avanzado de mal pronóstico

44
¿Deben integrarse ya las nuevas dianas al tratamiento del cáncer renal avanzado en primera línea?

45
TRATAMIENTO DEL CA RENAL AVANZADO EN 1ª LÍNEA
SLP correlación con OS SLP en 1ª línea de cáncer renal IL-2 3 meses IFN 4.7 meses Sorafenib 5.7 meses Avastin 8.5 meses Sunitinib 11 meses Datos excepcionales, pero definitivos?? (análisis de SG no planeado)
")
46
TRATAMIENTO DEL CA RENAL AVANZADO
Queda pendiente definir el esquema óptimo Necesitamos predictores de respuesta ¿Qué hacer en histologías no cél claras? Papel de la nefrectomía citorreductiva integrada a las nuevas terapias Tasas de RC realmente anecdóticas. NECESITAMOS CURAR!! La inhibición de angiogénesis debe ser continuada Toxicidades de uso crónico: sd nefrótico Problema de resistencias tardías Estudios de adyuvancia en marcha

Presentaciones similares









 Noviembre de 2004.>")




 Tacrolimus en combinación con dos dosis diferentes de sirolimus versus un.>")



en Ateroesclerosis. Seguridad y Eficacia Presentado en el.>")
