Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Antiagregantes Plaquetarios en Síndrome Coronario Agudo
Carlos E Uribe Clinica Cardiovascular Santa Maria Medellin Colombia

2
Sindrome Coronario Agudo
Hamm Lancet 358:1533,2001 Discomfort Isquemico Presentacion Sindrome Coronario Agudo Dx de Trabajo Davies MJ Heart 83:361, 2000 ECG Sin Elevación ST Elevación ST NSTEMI Maracdores Bioquimicos Infarto del Miocardio Final Dx Angina Inestable NQMI Qw MI

3
Angina Inestable Ocurre con mucha mayor frecuencia que el Infarto del Miocardio En USA 1.3 millones de personas son admitidas con A. Inestable cada año personas son admitidas con I.A.M en USA.

4
Fisiopatología Evidencia
TROMBOSIS*: Trombos en las autopsias. Trombos en los especimenes de aterectomia. Marcadores de actividad plaquetaria (CD 40L) y Fibrina Evidencia clinica con la mejoria de la mortalidad y morbilidad con antiplaquetarios y antitromboticos (heparinas) Trombos evidenciados por angioscopia * Sullivan E, Kearney M, Isner JM, et al. J Thromb Thrombolysis 1:63–71, 1994.
 y Fibrina. Evidencia clinica con la mejoria de la mortalidad y morbilidad con antiplaquetarios y antitromboticos (heparinas) Trombos evidenciados por angioscopia. * Sullivan E, Kearney M, Isner JM, et al. J Thromb Thrombolysis 1:63–71,")
5
Estructura de el trombo Luego de la disrupción de la placa
Clinical manifestations of arterial thrombosis Plaque rupture leads to adhesion, activation, and aggregation of circulating platelets, resulting in formation of a platelet-rich thrombus and myocardial ischemia. The clinical manifestation of coronary thrombosis depends on the extent and duration of thrombotic occlusion. Unstable angina and non-Q-wave MI are characterized by mural, platelet-rich thrombi, which do not completely block coronary blood flow and therefore cause ischemia of relatively short duration. The aggregated platelets can serve as a substrate for further thrombus propagation, leading to formation of an occlusive red thrombus formed by entrapment of red blood cells within the fibrin mesh. This complete occlusion results in abrupt and persistent ischemia that clinically manifests as ST-segment elevation MI. Adapted from Davies MJ. Circulation. 1990; 82 (suppl II): 11-38—11-46.
: 11-38—")
6
Actividad Plaquetaria

7
Mecanismo de Acción

8
Mecanismo de acción Clase I: Inh. de la Cicloxigenasa (Aspirina, Sulfinpyrazone, otros AINES). Clase II: Inh. de la fosfodiesterasa y la ADA, AMPc y Adenosina. (Dipiridamol) Clase III: Tienopiridinas, Bloqueadores de los receptores de ADP (P2Y12) (Clopidogrel, Ticlopidina). Clase IV: Inh. de los receptores y anticuerpos IIb/IIIa (Abciximab, Eptifibatide, Tirofiban).
 Clase III: Tienopiridinas, Bloqueadores de los receptores de ADP (P2Y12) (Clopidogrel, Ticlopidina). Clase IV: Inh. de los receptores y anticuerpos IIb/IIIa (Abciximab, Eptifibatide, Tirofiban).")
9
Clase I Aspirina Triflusal Ridogrel

10
ASPIRINA

11
VA Cooperative Study Estudio Multicentrico, Randomizado, Doble ciego
1266 ptes con UA. por 12 semanas Aspirina (325 mgs) vs. Placebo incidencia de muerte y de IAM en un 50% No diferencia en efectos adversos GI. Mortalidad 43% mas baja despues de un año de seguimiento P= *Lewis HD Jr; Davis JW; Archibald DG. N Engl J Med 1983 Aug 18;309(7):
 vs. Placebo. incidencia de muerte y de IAM en un 50% No diferencia en efectos adversos GI. Mortalidad 43% mas baja despues de un año de seguimiento. P= *Lewis HD Jr; Davis JW; Archibald DG. N Engl J Med 1983 Aug 18;309(7):")
12
Canadian Multicenter Trial
Estudio Randomizado, doble ciego 555 pacientes con UA por 18 meses. ASA (325 mg/dia), Sulfinpyrazona (200 mgs/dia), Terapia combinacion, o Placebo. 71% en la mortalidad y 51% en el punto combinado de Muerte y IAM no fatal. No hubo beneficio observado con la sulfinpirazona. Cairns JA; Gent M; Singer J,. N Engl J Med 1985 Nov 28;313(22):
, Sulfinpyrazona (200 mgs/dia), Terapia combinacion, o Placebo. 71% en la mortalidad y 51% en el punto combinado de Muerte y IAM no fatal. No hubo beneficio observado con la sulfinpirazona. Cairns JA; Gent M; Singer J,. N Engl J Med 1985 Nov 28;313(22):")
13
RISC RCT doble ciego por 1 año en Suecia.
796 ptes con UA, con ASA (75 mgs/dia), Heparina (infusión intermitente por 5 días), o placebo. Todos los ptes eran < de 70 años. 48% de reducción en el punto combinado de muerte, y IAM no fatal. La heparina no mostró ser mejor sola que el asa. La adición ASA/heparina era mejor. ASA a BAJAS DOSIS 75 mg dia The RISC Group, Lancet Oct 6;336(8719):
, Heparina (infusión intermitente por 5 días), o placebo. Todos los ptes eran < de 70 años. 48% de reducción en el punto combinado de muerte, y IAM no fatal. La heparina no mostró ser mejor sola que el asa. La adición ASA/heparina era mejor. ASA a BAJAS DOSIS 75 mg dia. The RISC Group, Lancet 1990 Oct 6;336(8719):")
14
METANALISIS ANTITHROMBOTIC TRIALISTS COLLABORATION:
Revisión de 12 trabajos con mas de 5000 pacientes con UA. Terapia con ASA mostró una reducción del 46% significativa en el punto final combinado de muerte, IAM no fatal, ECV no fatal o muerte vascular de cualquier tipo Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ 2002 Jan 12;324(7329):71-86.
:")
15
Efectos Adversos GI (dispepsia, nausea, vomito): 40% vs. 30% placebo.
Sangrado GI: 5% por año, Melenas: 1% /año, Hematemesis: 0.1% /año. Complicaciones raras: Exacerbación de Gota Exacerbación Broncoespasmo, Asma.

16
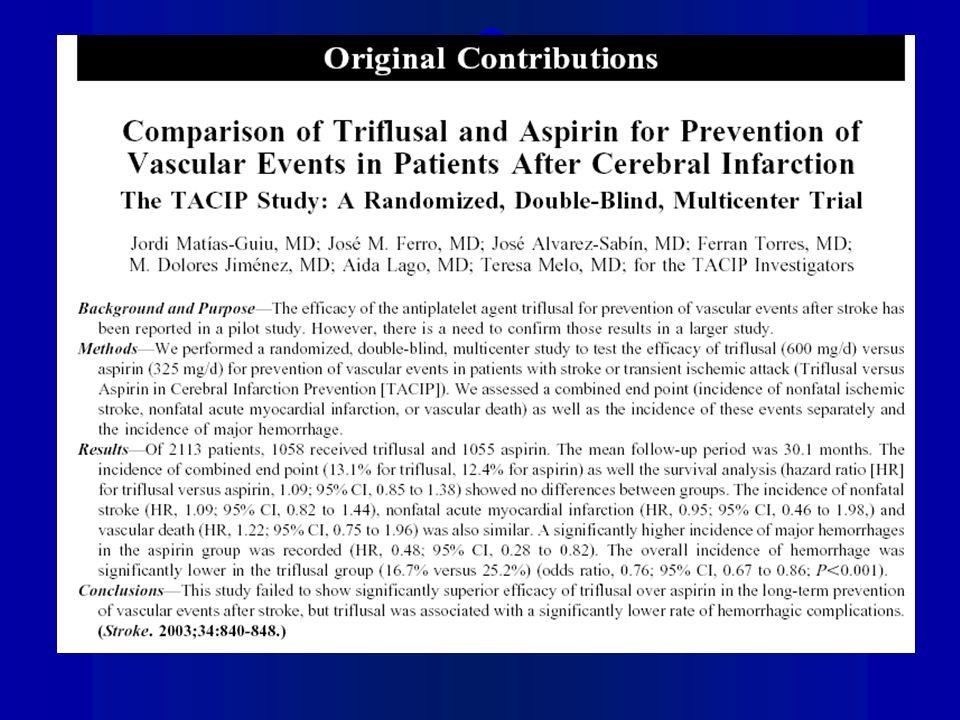
TRIFLUSAL No hay estudios en UA que comparen Triflusal vs. ASA.
Solo hay un estudio en IAM* Doble ciego, Multicentrico 2124 ptes. Triflusal 600 mg, ASA 300mg por 35 dias No hubo diferencias signifivativas en mortalidad, reinfarto no fatal o revascularizacion. Eventos cerebrovaculares hemorragicos fueron significativamente menos frecuentes en el grupo de triflusal. CONCLUSION: Triflusal tiene un perfil de seguridad mejor que la ASA. Cruz-Fernandez JM, Lopez-Bescos L.Department of Cardiology, Hospital Universitario Virgen de la Macarena, Sevilla, Spain. Eur Heart J Mar;21(6):457-65
:")
18
RIDOGREL Inhibidor de la Tromboxano sintetasa
Ventajas teóricas (No inhibe la Prostaciclina Sintetasa). Solo estudios en Fase II experimentales Malos resultados en Colitis Ulcerativa/Enfermedad de Crohn.
. Solo estudios en Fase II experimentales. Malos resultados en Colitis Ulcerativa/Enfermedad de Crohn.")
19
CLASE II Tienopiridinas: Ticlopidina Clopidogrel
Bloquea el receptor para el ADP plaquetario P2Y12

20
TICLOPIDINA

21
STAIG trial Estudio multicentrico, randomizado. 652 Ptes. con UA
Ticlopidina 250 mg/BID vs. Placebo. NO la compararon contra ASA. Reducción en IAM no fatales, muerte y revascularización en un 46% a los 6 meses. No hay estudios que comparen ASA Vs. Ticlopidina. Balsano F; Rizzon P; Violi F; Circulation Jul;82(1):17-26
:")
22
Efectos Adversos ticlopidina
Neutropenia: 1% Durante las 1eras 12 semanas de tratamiento (por supresión medular) Rash: 2% Diarrea: 3% PTT/HUS: raro 1 en 1600 ptes. Ocurre en las 1eras 12 semanas de tratamiento TTo: Plasmaferesis Otros raros: Disfuncion hepatica, BOOP
 Rash: 2% Diarrea: 3% PTT/HUS: raro 1 en 1600 ptes. Ocurre en las 1eras 12 semanas de tratamiento. TTo: Plasmaferesis. Otros raros: Disfuncion hepatica, BOOP.")
23
CLOPIDOGREL

24
CURE Estudio randomizado multicentrico llevado a cabo en 48 paises.
ptes con UA/NSTEMI ASA vs. ASA + Clopidogrel La mayoría de los pacientes tenían UA de alto riesgo Se evaluaron: Punto final primario: Muerte cardiovascular, IAM, o Stroke. Punto secunadario: Lo anterior + revascularizacion Eventos adversos 9 meses de seguimiento promedio The CURE Trial Investigators. N Engl J Med. 2001;345:

25
Punto Final Primario - IAM/Stroke/MuerteCV
CURE Punto Final Primario - IAM/Stroke/MuerteCV 11.4% Placebo + ASA* 9.3% Clopidogrel + ASA* Clopidogrel provided a 20% relative risk reduction in the composite outcome of MI, stroke or CV death (95% CI , P < 0.001). Overall there were 719 (11.4%) first events in the placebo group and 582 (9.3%) in the clopidogrel group. The hazard rate curves began to separate within the first few hours after therapy initiation and continued to diverge over the remainder of the trial. 20% RRR P < 0.001 N = 12,562 3 6 9 12 Months of Follow-Up * In combination with standard therapy The CURE Trial Investigators. N Engl J Med. 2001;345:
. Overall there were 719 (11.4%) first events in the placebo group and 582 (9.3%) in the clopidogrel group. The hazard rate curves began to separate within the first few hours after therapy initiation and continued to diverge over the remainder of the trial. 20% RRR. P < N = 12, Months of Follow-Up. * In combination with standard therapy. The CURE Trial Investigators. N Engl J Med. 2001;345:")
26
MI/Stroke/CV Death within 30 Days
CURE MI/Stroke/CV Death within 30 Days Placebo + ASA* Clopidogrel + ASA* Clopidogrel provided a 21% relative risk reduction in the primary end point of MI, stroke or CV death within 30 days (95% CI , P = 0.003). Beneficial effects were reported within a few hours, with the rate of cardiovascular death, nonfatal stroke, or refractory or severe ischemia significantly reduced by 24 hours in the clopidogrel treated group vs the placebo group (1.4% vs 2.1%, RRR 34% 95% CI of 0.51 to 0.86). 21% RRR P = 0.003 N = 12,562 10 20 30 Days of Follow-Up * In combination with standard therapy The CURE Trial Investigators. N Engl J Med. 2001;345:
. Beneficial effects were reported within a few hours, with the rate of cardiovascular death, nonfatal stroke, or refractory or severe ischemia significantly reduced by 24 hours in the clopidogrel treated group vs the placebo group (1.4% vs 2.1%, RRR 34% 95% CI of 0.51 to 0.86). 21% RRR. P = N = 12, Days of Follow-Up. * In combination with standard therapy. The CURE Trial Investigators. N Engl J Med. 2001;345:")
27
Resultados Sangrado CURE Placebo + ASA* N = 6303
Clopidogrel + ASA* N = 6259 End Point Major bleeding 2.7% 3.7%** Life-threatening bleeding 1.8% 2.2% † Non-life-threatening bleeding 0.9% 1.5% ‡ Minor bleeding 2.4% 5.1% § NEJM There was a significant difference in major and minor bleeding between the clopidogrel and aspirin group compared to the aspirin group alone. However, there was no statistically significant difference in life-threatening bleeding between the two treatment arms, which included fatal bleeding, drop in hemoglobin of at least 5 g/dL, significant hypotension requiring IV inotropes, bleeds requiring surgical interventions, intracranial hemorrhage, or transfusion of 4 or more units of blood. Major bleeds were increased both early (< 30 days) and late (> 30 days). The principal sites for major bleeding included gastrointestinal and at arterial puncture sites. There was a statistically significant difference in minor bleeding in the clopidogrel plus aspirin group (2.4% vs 5.1%, P < 0.001). The number of patients receiving transfusions of 2 or more units of blood was higher in the clopidogrel plus aspirin group (2.8% vs 2.2%, P = 0.02). Overall, there was no significant excess in major bleeds after coronary bypass graft surgery with clopidogrel plus aspirin vs aspirin. However, in most patients scheduled for CABG, study medication were discontinued prior to procedure (median time of stopping before procedure was 5 days). * In combination with standard therapy ** P = 0.001; † P = NS; ‡ P = 0.002; § P < The CURE Trial Investigators. N Engl J Med. 2001;345:
 and late (> 30 days). The principal sites for major bleeding included gastrointestinal and at arterial puncture sites. There was a statistically significant difference in minor bleeding in the clopidogrel plus aspirin group (2.4% vs 5.1%, P < 0.001). The number of patients receiving transfusions of 2 or more units of blood was higher in the clopidogrel plus aspirin group (2.8% vs 2.2%, P = 0.02). Overall, there was no significant excess in major bleeds after coronary bypass graft surgery with clopidogrel plus aspirin vs aspirin. However, in most patients scheduled for CABG, study medication were discontinued prior to procedure (median time of stopping before procedure was 5 days). * In combination with standard therapy. ** P = 0.001; † P = NS; ‡ P = 0.002; § P < The CURE Trial Investigators. N Engl J Med. 2001;345:")
28
PCI-CURE 2658 ptes dentro del estudio CURE con UA de alto riesgo, sometidos a intervencionismo.(seguimiento de 1 año) ASA vs. ASA+CLOPIDOGREL por 4 semanas luego de PCI Punto Primario: Muerte cardiovascular, infarto del miocardio, revascularización urgente a los 30 dias de la PTCA. Limitaciones: El pretratamiento con Clopidogrel fue en promedio 6 dias antes de la PTCA y no en las primeras 24 hrs. (CREDO). Gp IIb/IIIa unicamente se les dio al 21% de los pacientes (TARGET). Complicaciones: Un subgrupo de pacientes (aquellos que se sometieron a CABG) presentaron mas sangrado si se suspendía el clopidogrel < de 5 dias de la cirugia. (3.3% de incremento en el sangrado absoluto y 10x mas de riesgo de reoperación por sangrado) El estudio credo permitio demostrar antes de 6 dias el otcome con clopidogrel Un analisis post hoc del estudio TARGET (topol) demostro que aun con IIb/IIIa el grupo de clopidogrel les iba mejor (menos IAM, Menos mortalidad) Mehta, SR. et al for the CURE Trial Investigators. N Engl J Med. 2001;345:
. Gp IIb/IIIa unicamente se les dio al 21% de los pacientes (TARGET). Complicaciones: Un subgrupo de pacientes (aquellos que se sometieron a CABG) presentaron mas sangrado si se suspendía el clopidogrel < de 5 dias de la cirugia. (3.3% de incremento en el sangrado absoluto y 10x mas de riesgo de reoperación por sangrado) El estudio credo permitio demostrar antes de 6 dias el otcome con clopidogrel. Un analisis post hoc del estudio TARGET (topol) demostro que aun con IIb/IIIa el grupo de clopidogrel les iba mejor (menos IAM, Menos mortalidad) Mehta, SR. et al for the CURE Trial Investigators. N Engl J Med. 2001;345:")
29
Eficacia, Desenlaces Placebo + ASA* N = 1345
PCI-CURE Eficacia, Desenlaces Placebo + ASA* N = 1345 Clopidogrel + ASA* N = 1313 From PCI to 30 days MI, urgent revascularization or CV death 6.4% 4.5% % From PCI to follow-up CV death or MI 8.0% 6.0% % RRR P value NEJM Clopidogrel provided a 25% relative risk reduction in the composite outcome of MI or CV death at follow-up (8.0% vs 6.0%, P = 0.047), with a 29% reduction in MI (6.4% vs 4.5%, P = 0.03). Cardiovascular death was similar between the two groups at follow-up. Within 30 days there was also a 30% relative risk reduction in the primary outcome of MI, target vessel revascularization or CV death (6.4% vs 4.5%, P = 0.03), with a significant reduction in MI (3.8% vs 2.1%, RRR 44%) and urgent revascularization (2.8% vs 1.9%, RRR 33%). The rate of CV death was similar between the two groups. The reduction in the primary end point was seen within 48 hours following PCI, with increasing benefit at 7 and 14 days which continued throughout the 30 days. The benefits seen with early and long-term clopidogrel in addition to aspirin and other standard therapy, illustrates the need for early and continued antiplatelet protection in these high-risk patients. * In combination with standard therapy Mehta, SR. et al for the CURE Trial Investigators. Lancet. August 2001;21:
, with a 29% reduction in MI (6.4% vs 4.5%, P = 0.03). Cardiovascular death was similar between the two groups at follow-up. Within 30 days there was also a 30% relative risk reduction in the primary outcome of MI, target vessel revascularization or CV death (6.4% vs 4.5%, P = 0.03), with a significant reduction in MI (3.8% vs 2.1%, RRR 44%) and urgent revascularization (2.8% vs 1.9%, RRR 33%). The rate of CV death was similar between the two groups. The reduction in the primary end point was seen within 48 hours following PCI, with increasing benefit at 7 and 14 days which continued throughout the 30 days. The benefits seen with early and long-term clopidogrel in addition to aspirin and other standard therapy, illustrates the need for early and continued antiplatelet protection in these high-risk patients. * In combination with standard therapy. Mehta, SR. et al for the CURE Trial Investigators. Lancet. August 2001;21:")
30
Resultados Generales a Largo Plazo
PCI-CURE Resultados Generales a Largo Plazo Composite of cardiovascular death or MI from randomization to end of follow-up 0.15 12.6% Placebo + ASA* 0.10 8.8% Clopidogrel + ASA* Cumulative Hazard Rate 0.05 31% RRR P = N = 2658 For the end point of MI or cardiovascular death from time of randomization to end of follow-up, treatment with clopidogrel in addition to aspirin and other standard therapy resulted in a 31% RRR (8.8% clopidogrel vs. 12.6% placebo, P = 0.002). The curves diverged early and continued to separate over the course of 12 months. This end point included events that were prevented prior to PCI, in addition to those following the procedure. There were consistent reductions in MI or cardiovascular death in almost every subgroup examined 0.0 100 200 300 400 Days of follow-up * In combination with standard therapy Mehta, SR. et al for the CURE Trial Investigators. Lancet. August 2001.
. The curves diverged early and continued to separate over the course of 12 months. This end point included events that were prevented prior to PCI, in addition to those following the procedure. There were consistent reductions in MI or cardiovascular death in almost every subgroup examined Days of follow-up. * In combination with standard therapy. Mehta, SR. et al for the CURE Trial Investigators. Lancet. August")
31
Resultados a 30 Dias PCI-CURE
Composite of cardiovascular death, MI, or urgent revascularization 0.08 Placebo + ASA* 6.4% 0.06 4.5% Cumulative Hazard Rate 0.04 Clopidogrel + ASA* 0.02 30% RRR P = 0.03 N = 2658 Treatment with clopidogrel in addition to aspirin and other standard therapy resulted in a RRR of 30% (P = 0.03) compared with aspirin and standard therapy alone for the endpoint of cardiovascular death, MI, or urgent revascularization at 30 days post-PCI. The event curves separated early and continued to separate up to 30 days and beyond. A reduction in this endpoint was observed within 2 days, with continuing benefit throughout the study period (up to 1 year). The majority of patients (> 80% in both groups) received open-label ADP-receptor antagonist following PCI, suggesting the early benefit was mainly due to clopidogrel pre-treatment. An “on-treatment” analysis which excluded those patients that received open-label ADP-receptor antagonist prior to PCI (~25% in both groups) demonstrated a 42% RRR (P = 0.005) in this endpoint. 0.0 5 10 15 20 25 30 Days of follow-up * In combination with standard therapy Mehta, SR. et al for the CURE Trial Investigators. Lancet. August 2001;21:
 compared with aspirin and standard therapy alone for the endpoint of cardiovascular death, MI, or urgent revascularization at 30 days post-PCI. The event curves separated early and continued to separate up to 30 days and beyond. A reduction in this endpoint was observed within 2 days, with continuing benefit throughout the study period (up to 1 year). The majority of patients (> 80% in both groups) received open-label ADP-receptor antagonist following PCI, suggesting the early benefit was mainly due to clopidogrel pre-treatment. An on-treatment analysis which excluded those patients that received open-label ADP-receptor antagonist prior to PCI (~25% in both groups) demonstrated a 42% RRR (P = 0.005) in this endpoint Days of follow-up. * In combination with standard therapy. Mehta, SR. et al for the CURE Trial Investigators. Lancet. August 2001;21:")
32
Sangrado PCI-CURE Placebo + ASA* Clopidogrel + ASA*
From PCI to 30 days Major 1.4% % † Life threatening 0.7% 0.7% † Minor 0.7% 1.0% † From PCI to end of follow-up Major 2.5% 2.7% † Life threatening 1.3% 1.2% † Minor 2.1% 3.5% ‡ NEJM There was no significant difference in major bleeding at 30 days or at end of follow-up (2.5% vs 2.7%, RR 1.12, P = 0.64). Similarly, there was no significant difference in life-threatening bleeding at 30 days (0.7% vs 0.7%) or at follow-up (1.3% vs. 1.2%). Minor bleeding was slightly increased in the clopidogrel group at 30 days (0.7% vs. 1.0%) and significantly increased at follow-up (2.1% vs. 3.5%, RR 1.68, P = 0.03). Mehta, SR. et al for the CURE Trial Investigators. Lancet. August 2001;21: * In combination with standard therapy † P = NS, ‡ P = 0.03
. Similarly, there was no significant difference in life-threatening bleeding at 30 days (0.7% vs 0.7%) or at follow-up (1.3% vs. 1.2%). Minor bleeding was slightly increased in the clopidogrel group at 30 days (0.7% vs. 1.0%) and significantly increased at follow-up (2.1% vs. 3.5%, RR 1.68, P = 0.03). Mehta, SR. et al for the CURE Trial Investigators. Lancet. August 2001;21: * In combination with standard therapy. † P = NS, ‡ P =")
33
CREDO Estudio multicentrico (99 centros) randomizado doble ciego.
2116 pacientes con UA quienes fueron sometidos a PCI electiva. Clopidogrel dosis de carga y mantenimiento vs. Placebo (tto. estándar) a 12 meses. 1 grupo con clopidogrel a largo plazo y otro grupo con clopidogrel a corto plazo.(sin dosis bolo antes de PCI). Punto Final a los 28 dias: Muerte, AMI, Revascularizacion urgente. Punto Final 1 año: Muerte, ECV, AMI. Steinhubl S, Berger P, Tift Mann III J et al. JAMA. 2002;Vol 288,No 19:
 a 12 meses. 1 grupo con clopidogrel a largo plazo y otro grupo con clopidogrel a corto plazo.(sin dosis bolo antes de PCI). Punto Final a los 28 dias: Muerte, AMI, Revascularizacion urgente. Punto Final 1 año: Muerte, ECV, AMI. Steinhubl S, Berger P, Tift Mann III J et al. JAMA. 2002;Vol 288,No 19:")
34
Diseño General del Estudio CREDO
PCI* 28 Days 12 Months Pre-treatment 3-24 h before PCI Clopidogrel Arm Clopidogrel 300 mg + ASA† (325 mg) Clopidogrel 75 mg QD + ASA† 325 mg QD Clopidogrel 75 mg QD + ASA† ( mg) QD R Clopidogrel 75 mg QD + ASA† 325 mg QD Placebo QD + ASA† ( mg) QD Following randomization, patients entered in CREDO received either a 300 mg loading dose of clopidogrel, or matching placebo, 3-24 hours prior to PCI. In addition, all patients also received a 325 mg dose of ASA at this point. Both arms then received clopidogrel 75 mg daily from the time of PCI up to 28 days, on top of standard therapy including a daily dose of 325 mg ASA. Thus, at the end of 28 days, the only difference between the two groups was the use of a 300 mg loading dose of clopidogrel before the PCI. From day 29 to 1 year, the group initially randomized to pre-treatment with clopidogrel received a 75 mg daily dose of clopidogrel, whilst the no-pre-treatment arm received a matching placebo. Both groups continued to receive ASA (81 mg to 325 mg daily dose, left at the investigator’s discretion) and other standard therapy until the end of the 1 year period. The medications that encompassed post-randomized concomitant therapy were left to the discretion of the investigator with the exception of ASA, which was mandated by the protocol for every patient. Reference: Steinhubl S, Berger P, Tift Mann III J, et al. JAMA. 2002;Vol 288,No 19: Placebo Arm Placebo + ASA† (325 mg) † Plus other standard therapies * Both groups received clopidogrel 75 mg + ASA 325 mg at time of procedure Steinhubl S, Berger P, Tift Mann III J et al. JAMA. 2002;Vol 288,No 19:
 Clopidogrel 75 mg QD + ASA† 325 mg QD. Clopidogrel 75 mg QD + ASA† ( mg) QD. R. Clopidogrel 75 mg QD + ASA† 325 mg QD. Placebo QD + ASA† ( mg) QD. Following randomization, patients entered in CREDO received either a 300 mg loading dose of clopidogrel, or matching placebo, 3-24 hours prior to PCI. In addition, all patients also received a 325 mg dose of ASA at this point. Both arms then received clopidogrel 75 mg daily from the time of PCI up to 28 days, on top of standard therapy including a daily dose of 325 mg ASA. Thus, at the end of 28 days, the only difference between the two groups was the use of a 300 mg loading dose of clopidogrel before the PCI. From day 29 to 1 year, the group initially randomized to pre-treatment with clopidogrel received a 75 mg daily dose of clopidogrel, whilst the no-pre-treatment arm received a matching placebo. Both groups continued to receive ASA (81 mg to 325 mg daily dose, left at the investigator’s discretion) and other standard therapy until the end of the 1 year period. The medications that encompassed post-randomized concomitant therapy were left to the discretion of the investigator with the exception of ASA, which was mandated by the protocol for every patient. Reference: Steinhubl S, Berger P, Tift Mann III J, et al. JAMA. 2002;Vol 288,No 19: Placebo. Arm. Placebo + ASA† (325 mg) † Plus other standard therapies. * Both groups received clopidogrel 75 mg + ASA 325 mg at time of procedure. Steinhubl S, Berger P, Tift Mann III J et al. JAMA. 2002;Vol 288,No 19:")
35
Efectos Tempranos de el Pre-tratamiento con Clopidogrel – Resultados a los 28 días CREDO
Death, MI, UTVR- PP Population 10 9 8.3% 8 18.5% RRR P=0.23 7 6.8% 6 Combined Endpoint Occurrence (%) 5 4 Looking at the per protocol population of those patients who underwent a PCI, pre-treatment with a 300 mg loading dose of clopidogrel, plus ASA (325 mg) and other standard therapy, led to an 18.5% relative reduction in the risk of the combined endpoint of death, MI, and urgent target vessel revascularization at 28 days that did not achieve statistical significance (6.8% clopidogrel pre-treatment vs. 8.3% no clopidogrel pre-treatment, 95% CI, -14.2, -41.8, p=0.23).1 The relative risk reduction for the other PP endpoints (MI, death, TVR or MI, death) also showed similar risk reductions. The inability to reach a statistically significant RRR for the primary endpoints has been attributed primarily to a much lower than expected overall event rate in the trial (8.3% actual vs. 13.4% planned) due to good standard of care in the overall study population. Reference: 1Steinhubl S, Berger P, Tift Mann III J, et al. JAMA. 2002;Vol 288,No 19: 2Steinhubl S, Ellis S, Wolski K et al. Circulation. 2001;103:1403. 3 No-PT - Placebo* PT- Clopidogrel* 2 1 7 14 21 28 Days From Randomization PT = Pre-treatment *Plus ASA and other standard therapies Steinhubl S, Berger P, Tift Mann III J et al. JAMA. 2002;Vol 288,No 19:
 Looking at the per protocol population of those patients who underwent a PCI, pre-treatment with a 300 mg loading dose of clopidogrel, plus ASA (325 mg) and other standard therapy, led to an 18.5% relative reduction in the risk of the combined endpoint of death, MI, and urgent target vessel revascularization at 28 days that did not achieve statistical significance (6.8% clopidogrel pre-treatment vs. 8.3% no clopidogrel pre-treatment, 95% CI, -14.2, -41.8, p=0.23).1. The relative risk reduction for the other PP endpoints (MI, death, TVR or MI, death) also showed similar risk reductions. The inability to reach a statistically significant RRR for the primary endpoints has been attributed primarily to a much lower than expected overall event rate in the trial (8.3% actual vs. 13.4% planned) due to good standard of care in the overall study population. Reference: 1Steinhubl S, Berger P, Tift Mann III J, et al. JAMA. 2002;Vol 288,No 19: Steinhubl S, Ellis S, Wolski K et al. Circulation. 2001;103: No-PT - Placebo* PT- Clopidogrel* Days From Randomization. PT = Pre-treatment. *Plus ASA and other standard therapies. Steinhubl S, Berger P, Tift Mann III J et al. JAMA. 2002;Vol 288,No 19:")
36
Combined Endpoint Occurrence (%)
Beneficios a Largo Plazo (1 año) del Clopidogrel en Pacientes PCI CREDO MI, Stroke, or Death – ITT Population Combined Endpoint Occurrence (%) Months From Randomization 27% RRR P=0.02 Placebo* Clopidogrel* 5 10 15 8.5% 11.5% 3 6 9 12 The CREDO results demonstrate the benefits of long-term (1 year) administration of clopidogrel plus ASA and other standard therapies in patients undergoing PCI, with or without stent. For the entire study population, long-term clopidogrel treatment was associated with a 27% reduction in the relative risk of the combined endpoint of death, MI, and stroke at 1 year. This result was statistically significant (8.5% clopidogrel vs. 11.5% placebo, 95% CI, , p=0.02). Reference: Steinhubl S, Berger P, Tift Mann III J, et al. JAMA. 2002;Vol 288,No 19: * Plus ASA and other standard therapies Steinhubl S, Berger P, Tift Mann III J et al. JAMA. 2002;Vol 288,No 19:
 del Clopidogrel en Pacientes PCI CREDO. MI, Stroke, or Death – ITT Population. Combined Endpoint Occurrence (%) Months From Randomization. 27% RRR. P=0.02. Placebo* Clopidogrel* % 11.5% The CREDO results demonstrate the benefits of long-term (1 year) administration of clopidogrel plus ASA and other standard therapies in patients undergoing PCI, with or without stent. For the entire study population, long-term clopidogrel treatment was associated with a 27% reduction in the relative risk of the combined endpoint of death, MI, and stroke at 1 year. This result was statistically significant (8.5% clopidogrel vs. 11.5% placebo, 95% CI, , p=0.02). Reference: Steinhubl S, Berger P, Tift Mann III J, et al. JAMA. 2002;Vol 288,No 19: * Plus ASA and other standard therapies. Steinhubl S, Berger P, Tift Mann III J et al. JAMA. 2002;Vol 288,No 19:")
37
Sangrado Mayores a 1 año Resultados: CREDO
Major Bleeding Clopidogrel* (n=1,053) Placebo* (n=1,063) P-value Any 93 (8.8%) 71 (6.7%) 0.07 Non-procedural 13 (1.2%) 8 (0.8%) 0.28 Procedural 81 (7.7%)† 63 (5.9%)‡ 0.12 CABG 64 55 Non-CABG 17 8 P= NS Steinhubl S, Berger P, Tift Mann III J et al. JAMA. 2002;Vol 288,No 19:
 Placebo* (n=1,063) P-value. Any. 93 (8.8%) 71 (6.7%) Non-procedural. 13 (1.2%) 8 (0.8%) Procedural. 81 (7.7%)† 63 (5.9%)‡ CABG Non-CABG P= NS. Steinhubl S, Berger P, Tift Mann III J et al. JAMA. 2002;Vol 288,No 19:")
38
CAPRIE Steering Committee. Lancet.1996; 348:1329-1339
ptes ASA vs. Clopidogrel Seguimiento a 3 años Pacientes con enfermedad ateroesclerotica: ECV isquemico reciente IAM reciente Enfermedad arterial periferica CAPRIE Steering Committee. Lancet.1996; 348:

39
CAPRIE Study Reducción del Riesgo in IAM (Fatal and Nonfatal MI)
Relative Risk Reduction 19.2% Aspirin 5 Aspirin1 3.6% Clopidogrel 4 (P = 0.008)2* Event Rate for MI (%) (fatal or nonfatal) 3 2.9% Clopidogrel1 2 1 3 6 9 12 15 18 21 24 27 30 33 36 Months of Follow-Up * Based on post hoc analysis of individual outcome events (N=19,185). 1 Data on file, Sanofi Pharmaceuticals, Inc. 2 Gent M. Circulation. 1997;96(suppl):I-467. Abstract 2608.
2* Event Rate for MI (%) (fatal or nonfatal) % Clopidogrel Months of Follow-Up. * Based on post hoc analysis of individual outcome events (N=19,185). 1 Data on file, Sanofi Pharmaceuticals, Inc. 2 Gent M. Circulation. 1997;96(suppl):I-467. Abstract")
40
CAPRIE Study MI Paradox: Subgroups vs. Outcomes
Relative Risk Reduction* by Qualifying Subgroup1 Relative Risk Reduction of Individual Outcomes in Total Population 7.3% 5.2% 2 IS MI PAD Total Aspirin better Clopidogrel better IS (fatal or non-fatal) MI (fatal or non-fatal) Vascular death Total Aspirin better Clopidogrel better -3.7% 19.2% 3‡ 23.8% 7.6%1 8.7%1† 8.7%1† References on slide *Cluster of IS, MI, or vascular death † p= ‡ p=0.008 1 CAPRIE Steering Committee. Lancet.1996; 348: 2 Easton JD. Neurology July; P Abstract. 3 Gent M. Circulation. 1997; 96(8 supple): I-467 Abstract.
 MI. (fatal or non-fatal) Vascular death. Total. Aspirin better Clopidogrel better. -3.7% 19.2% 3‡ 23.8% 7.6%1. 8.7%1† 8.7%1† References on slide *Cluster of IS, MI, or vascular death † p=0.043 ‡ p= CAPRIE Steering Committee. Lancet.1996; 348: Easton JD. Neurology July; P Abstract. 3 Gent M. Circulation. 1997; 96(8 supple): I-467 Abstract.")
41
19.2% Relative Risk Reduction (P=0.008)2*
CAPRIE Study Reducción del Riesgo en Eventos Desenlace IAM (Fatal and Nonfatal MI) 19.2% Event Rate for MI (fatal or nonfatal) Relative Risk Reduction (P=0.008)2* Aspirin1 3.6% PLAVIX1 2.9% * Based on post hoc analysis of individual outcome events (N=19,185). 1 Data on file, Sanofi Pharmaceuticals, Inc. 2 Gent M. Circulation. 1997; 96 (suppl): I-467. Abstract 2608.
 19.2% Event Rate for MI. (fatal or nonfatal) Relative. Risk. Reduction. (P=0.008)2* Aspirin1. 3.6% PLAVIX1. 2.9% * Based on post hoc analysis of individual outcome events (N=19,185). 1 Data on file, Sanofi Pharmaceuticals, Inc. 2 Gent M. Circulation. 1997; 96 (suppl): I-467. Abstract")
42
Costo Efectividad ASA vs. Clopidogrel ???

43
Clase IV Inhibidores de la Glicoproteinas IIb/IIIa. Abciximab
Tirofiban Eptifibatide Lamifiban Fradafiban

44
Inhibidores Parenterales de la GP IIb-IIIa
Anticuerpos abciximab (ReoPro, Centocor/Lilly) Peptido Cíclico eptifibatide (INTEGRILIN®, COR/Key) Parenteral inhibitors of GP IIb-IIIa Several parenteral GP IIb-IIIa inhibitors are in various stages of clinical development. To date, three parenteral agents have been approved for clinical use. Abciximab (ReoPro®/Centocor & Lilly) is an Fab fragment of a chimeric human-mouse antibody directed against GP IIb-IIIa. Eptifibatide (INTEGRILIN®/COR & Key) is a cyclic heptapeptide based on the structure of a larger peptide, barbourin, which was isolated from the venom of the southeastern pigmy rattlesnake, and which binds with high specificity to the platelet receptor GP IIb-IIIa. Tirofiban HCl (Aggrastat®/Merck) is a nonpeptide synthetic molecule (peptidomimetic) with a molecular structure that mimics the GP IIb-IIIa binding sequences of natural ligands. No-peptídicos tirofiban HCI (Aggrastat, Merck)
 Peptido Cíclico. eptifibatide. (INTEGRILIN®, COR/Key) Parenteral inhibitors of GP IIb-IIIa. Several parenteral GP IIb-IIIa inhibitors are in various stages of clinical development. To date, three parenteral agents have been approved for clinical use. Abciximab (ReoPro®/Centocor & Lilly) is an Fab fragment of a chimeric human-mouse antibody directed against GP IIb-IIIa. Eptifibatide (INTEGRILIN®/COR & Key) is a cyclic heptapeptide based on the structure of a larger peptide, barbourin, which was isolated from the venom of the southeastern pigmy rattlesnake, and which binds with high specificity to the platelet receptor GP IIb-IIIa. Tirofiban HCl (Aggrastat®/Merck) is a nonpeptide synthetic molecule (peptidomimetic) with a molecular structure that mimics the GP IIb-IIIa binding sequences of natural ligands. No-peptídicos. tirofiban HCI. (Aggrastat, Merck)")
45
Propiedades de los inhibidores GP IIb-IIIa
Specificidad por GP IIb-IIIa; no interfiere con las funciones biologicas de otros receptores Rapida restauracion de la actividad plaquetaria (<50% inhibition) dentro de las 4 horas de descontinuar la infusion Evidencia de antigenicidad Eptifibatide1 SI No Abciximab2 No SI Tirofiban HCI3 SI No Properties of GP IIb-IIIa inhibitors In preclinical and clinical studies, parenteral inhibitors of GP IIb-IIIa have exhibited distinct pharmacological properties. Small molecule inhibitors, eptifibatide and tirofiban HCl, bind to GP IIb-IIIa with high specificity and do not cross-react with structurally related integrins, avoiding interference with the normal physiologic roles of other receptors. Abciximab, on the other hand, can bind to at least two other integrins — the broadly distributed vitronectin receptor and the leukocyte integrin Mac-1. Abciximab also has a relatively long biological half-life, and can profoundly affect platelet function for hours after termination of infusion. The small molecule inhibitors have a relatively short biological half-life, so that the platelet function is restored toward baseline (<50% inhibition) within 4 hours after termination of infusion, which may be important if a patient needs to undergo an emergency surgery or develops a bleeding complication. Abciximab also has been demonstrated to elicit antibodies in up to 6.5 percent of patients receiving it for the first time. This percentage increases with repeat usage. Although diminished efficacy or anaphylaxis have not been reported with repeat abciximab use, severe profound thrombocytopenia has been shown to increase with repeat exposure to abciximab. 1. Full prescribing information. Physicians’ Desk Reference. 1999; 53: Full prescribing information. Physicians’ Desk Reference. 1999; 53: Full prescribing information. Physicians’ Desk Reference. 1999; 53:
 dentro de las 4 horas de descontinuar la infusion. Evidencia de antigenicidad. Eptifibatide1. SI. No. Abciximab2. No. SI. Tirofiban HCI3. SI. No. Properties of GP IIb-IIIa inhibitors. In preclinical and clinical studies, parenteral inhibitors of GP IIb-IIIa have exhibited distinct pharmacological properties. Small molecule inhibitors, eptifibatide and tirofiban HCl, bind to GP IIb-IIIa with high specificity and do not cross-react with structurally related integrins, avoiding interference with the normal physiologic roles of other receptors. Abciximab, on the other hand, can bind to at least two other integrins — the broadly distributed vitronectin receptor and the leukocyte integrin Mac-1. Abciximab also has a relatively long biological half-life, and can profoundly affect platelet function for hours after termination of infusion. The small molecule inhibitors have a relatively short biological half-life, so that the platelet function is restored toward baseline (<50% inhibition) within 4 hours after termination of infusion, which may be important if a patient needs to undergo an emergency surgery or develops a bleeding complication. Abciximab also has been demonstrated to elicit antibodies in up to 6.5 percent of patients receiving it for the first time. This percentage increases with repeat usage. Although diminished efficacy or anaphylaxis have not been reported with repeat abciximab use, severe profound thrombocytopenia has been shown to increase with repeat exposure to abciximab. 1. Full prescribing information. Physicians’ Desk Reference. 1999; 53: Full prescribing information. Physicians’ Desk Reference. 1999; 53: Full prescribing information. Physicians’ Desk Reference. 1999; 53:")
46
INHIBIDORES GP IIB/IIIA

47
ABCIXIMAB Fragmentos de fraciones Fab de anticuerpos murinos-humanos quimericos monoclonales Acción inhibitoria mas rapida. (80% a las 2 hrs) Sangrado menor mas frecuente, No diferencia estadistica en el sangrado mayor (EPILOG). EPIC CAPTURE GUSTO 4-ACS EPILOG RAPPORT ADMIRAL CADILLAC EPISTENT ISAR-2 ERASER GRAPE
. EPIC. CAPTURE. GUSTO 4-ACS. EPILOG. RAPPORT. ADMIRAL. CADILLAC. EPISTENT. ISAR-2. ERASER. GRAPE.")
48
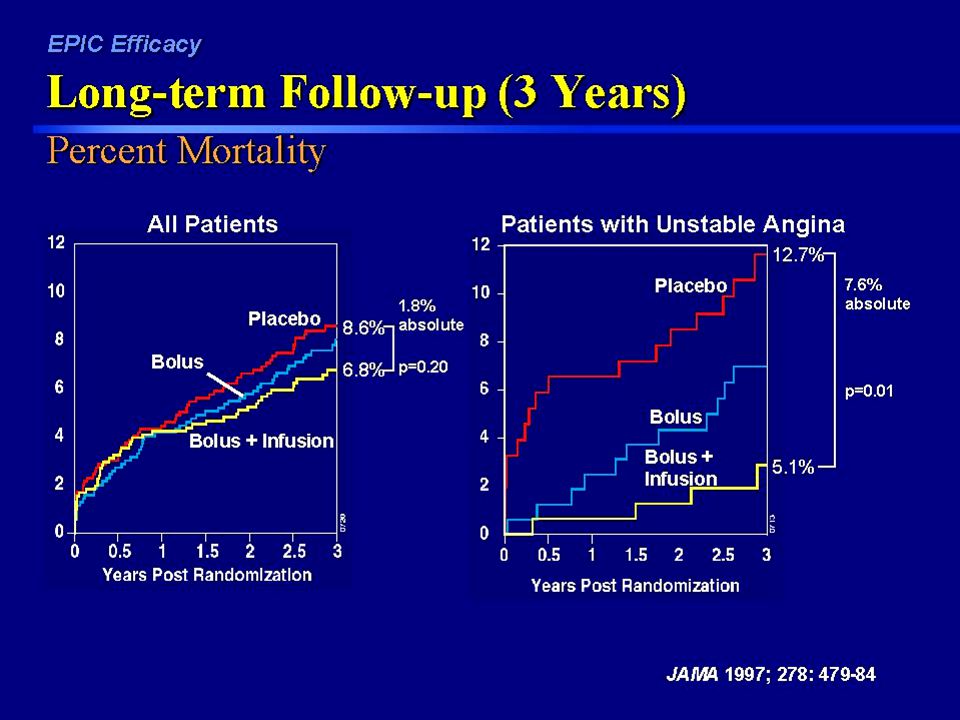
EPIC 2099 pacientes con UA de alto riesgo Antes de PTCA, 3 brazos:
Abciximab bolo vs. Abciximab bolo + mantenimiento vs. Placebo Beneficio mantenido hasta por 3 años luego del procedimiento

50
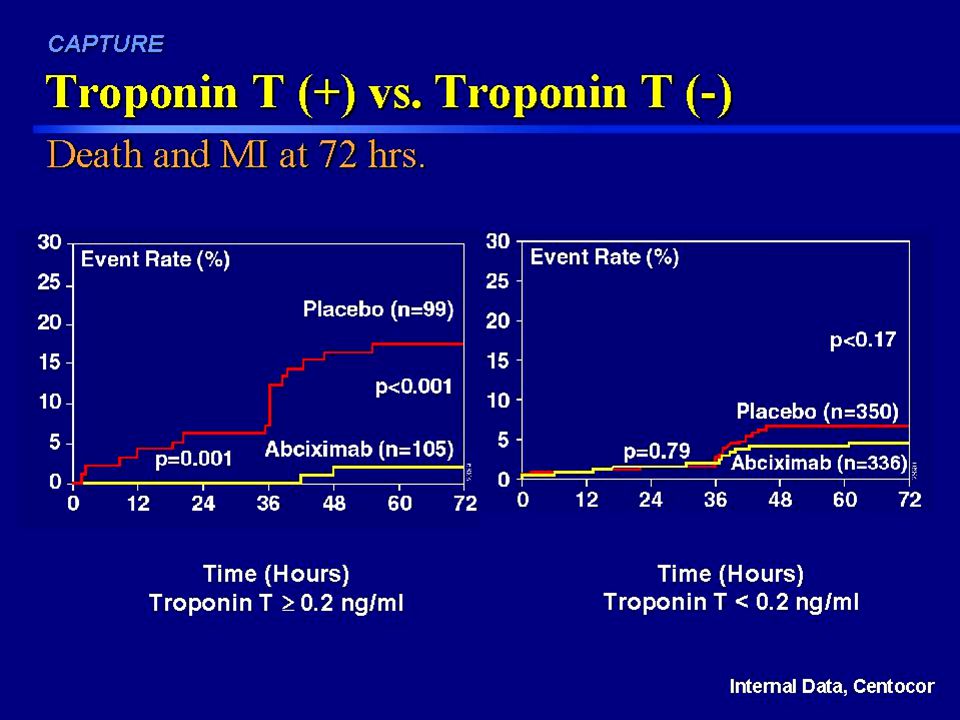
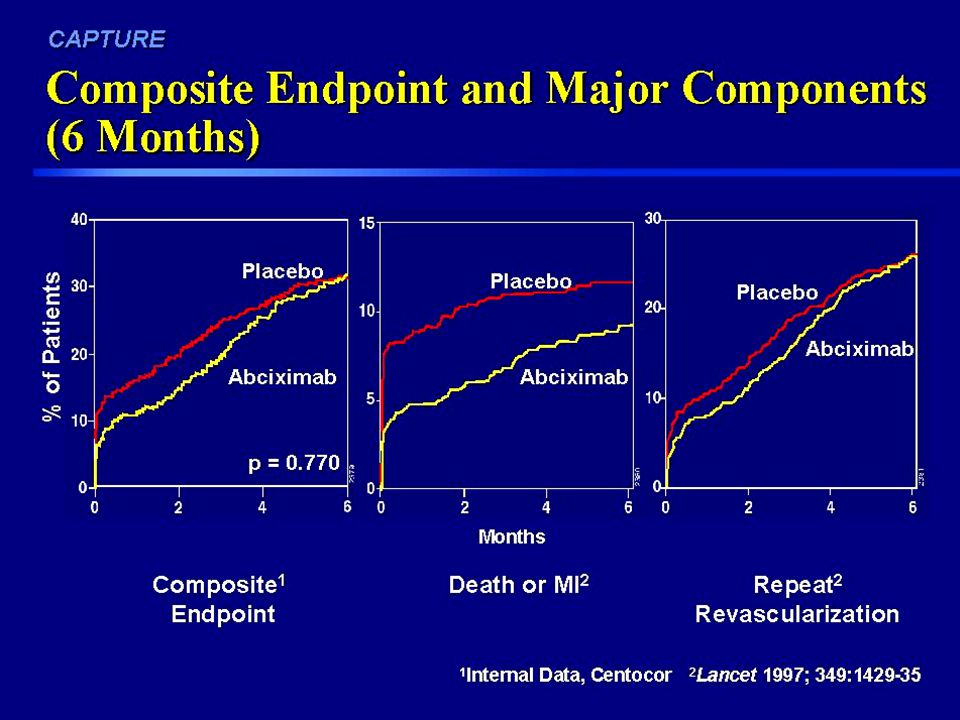
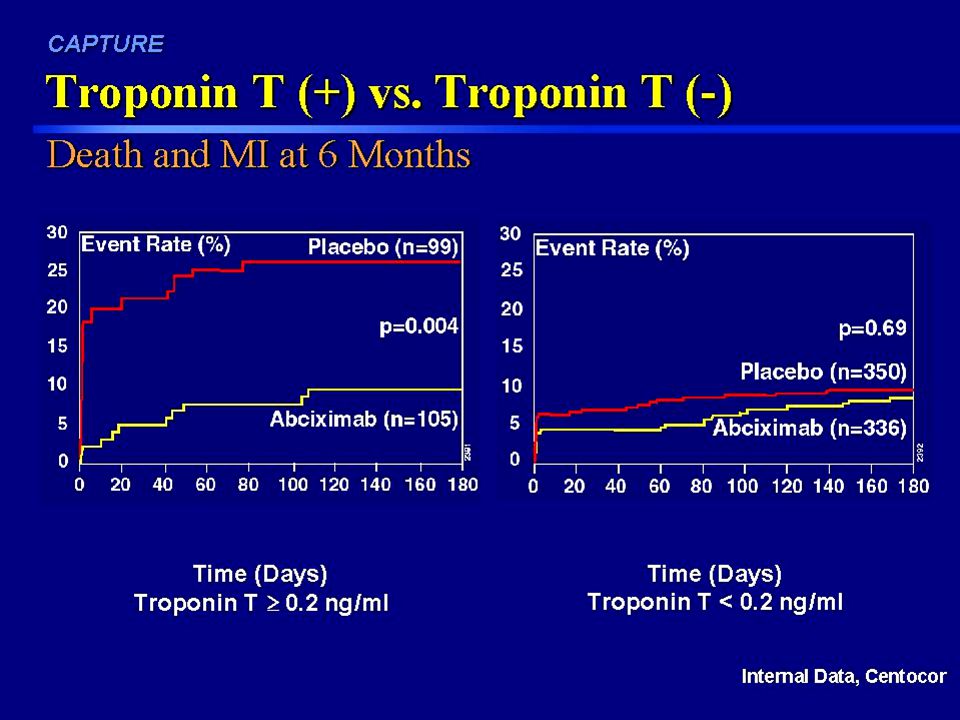
CAPTURE 1265 ptes con UA de alto riesgo, refractarios a tto medico convencional. Abciximab bolo + sostenimiento (1 hr despues de la PTCA UNICAMENTE) vs Placebo Se suspendió prematuramente por resultados benéficos (eficacia significativa). Mayor beneficio en aquellos con Troponina T elevada NO hubo beneficio en aquellos con Troponina T normal Lancet 1997; 349:
 vs Placebo. Se suspendió prematuramente por resultados benéficos (eficacia significativa). Mayor beneficio en aquellos con Troponina T elevada. NO hubo beneficio en aquellos con Troponina T normal. Lancet 1997; 349:")
51
CAPTURE: Infarto del Miocardio
Medical Therapy Pre-Intervention Incidencia Antes y Despues de PTCA Lancet 1997; 349: CAPTURE: Myocardial Infarction The graph shows the incidence of MI by treatment arm in patients before, during, and after coronary intervention. Myocardial infarction in this case was defined as new Q waves or an increase of 3-fold or greater in serum CK-MB/CK enzyme levels. The incidence of myocardial infarction in the placebo arm before coronary intervention was 2.0%, and was reduced to 0.6% in the abciximab bolus and 24 hour infusion arm. This translated into a relative reduction of 70%, an absolute reduction of 1.4%, and was statistically significant (p= 0.029). Consistent with the hypothesis that intervention itself can cause complications, there is a marked increase in the incidence of MI immediately following the intervention. The incidence of MI post intervention is reduced more than 50% (p=0.009) with abciximab, a rate which is consistent with previous trials, EPIC, EPILOG and EPISTENT. In the CAPTURE trial, there was also a doubling of thrombus resolution with abciximab therapy pre-intervention, from 20.5% to 41.9% (EHJ 1997; 18 supplement: 243), a 51% reduction in angiographic failure, from 10.8% to 5.7% (EHJ 1997; 18 supplement: 621) and a trend in reduction in the need for urgent intervention, from 2.2% to 1.4%; p>0.1 (Lancet 1997; 349: ). Data not shown. A reduction in each major pre-PTCA parameter evaluated in the CAPTURE trial strongly suggests that abciximab stabilizes patients in preparation for undergoing PTCA.
. Consistent with the hypothesis that intervention itself can cause complications, there is a marked increase in the incidence of MI immediately following the intervention. The incidence of MI post intervention is reduced more than 50% (p=0.009) with abciximab, a rate which is consistent with previous trials, EPIC, EPILOG and EPISTENT. In the CAPTURE trial, there was also a doubling of thrombus resolution with abciximab therapy pre-intervention, from 20.5% to 41.9% (EHJ 1997; 18 supplement: 243), a 51% reduction in angiographic failure, from 10.8% to 5.7% (EHJ 1997; 18 supplement: 621) and a trend in reduction in the need for urgent intervention, from 2.2% to 1.4%; p>0.1 (Lancet 1997; 349: ). Data not shown. A reduction in each major pre-PTCA parameter evaluated in the CAPTURE trial strongly suggests that abciximab stabilizes patients in preparation for undergoing PTCA.")
55
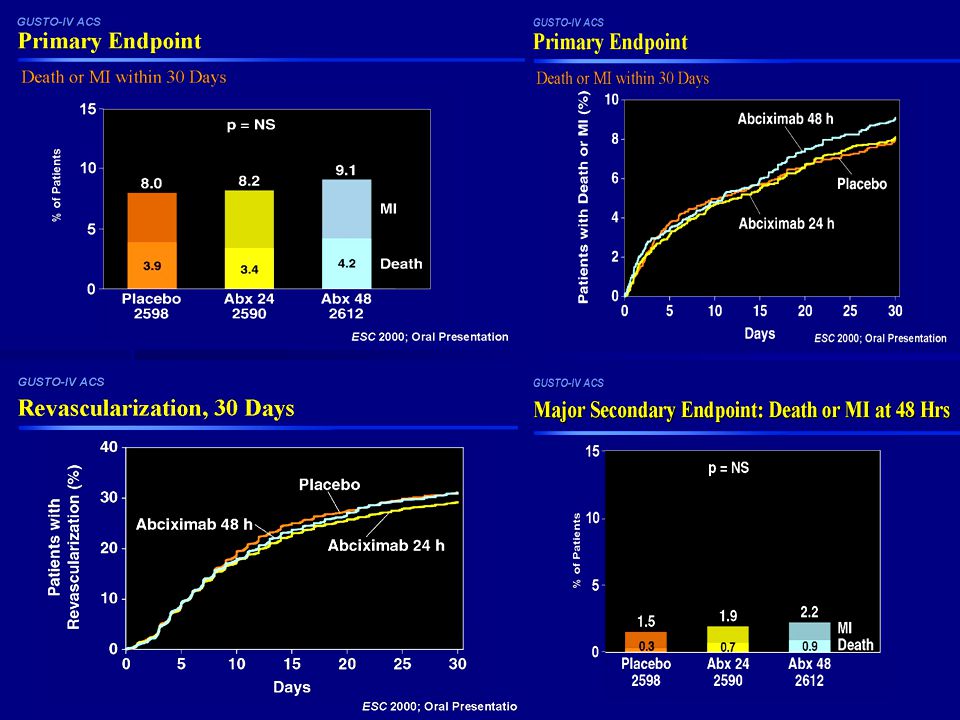
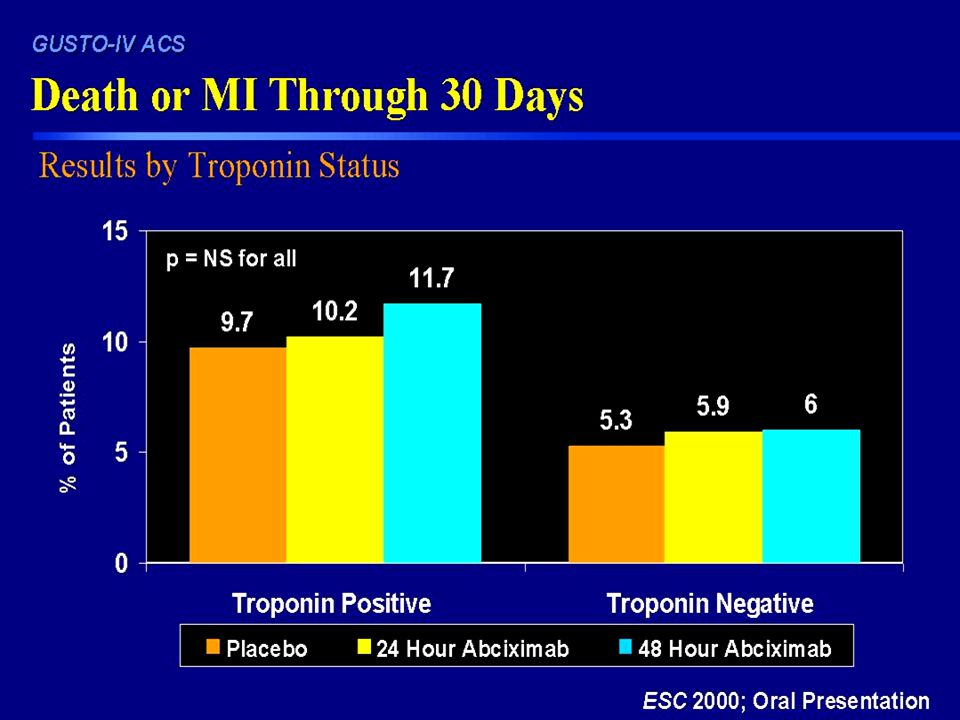
GUSTO 4-ACS 7800 ptes. Con UA de alto riesgo quienes no fueron sometidos a PTCA (Tratamiento medico) Resultados desalentadores

58
TIROFIBAN Inhibidor no peptidico RESTORE PRISM PRISM-PLUS

59
Programa Clinico para AGGRASTAT ® (tirofiban HCl) en UA/NSTEMI
Terapia Medica 3232 ptes. Estabilizacion Medica CABG ± Angiografía Presentación PTCA PRISM RESTORE PRISM-PLUS The PRISM Study Investigators. N Engl J Med. 1998;338: The PRISM-PLUS Study Investigators. N Engl J Med. 1998;338: The RESTORE Investigators. Circulation. 1997;96:

60
PRISM-PLUS: Reducciones de Eventos a los 7 Dias
RR=32% P=0.004 Heparin (n=797) AGGRASTAT® (tirofiban HCl) + Heparin (n=773) RR=30% P=0.02 RR=47% P=0.006 RR=43% P=0.006 % Patients P=0.99 Slide 13 PRISM-PLUS: Event Reductions at 7 Days At 7 days, the AGGRASTAT-plus-heparin group in PRISM-PLUS attained significant reductions compared to heparin alone in the composite endpoint (32%, P=0.004), in refractory ischemia (30%, P=0.02), in MI (47%, P=0.006), and in the combination of MI and death (43%, P=0.006). The incidence of death at 7 days was comparable between the two treatment groups.13 Composite Endpoint Refractory Ischemia MI Death MI/Death The PRISM-PLUS Study Investigators. N Engl J Med. 1998;338: 13 The Platelet Receptor Inhibition for Ischemic Syndrome Management in Patients Limited by Unstable Signs and Symptoms (PRISM-PLUS) Study Investigators. Inhibition of the platelet glycoprotein IIb/IIIa receptor with tirofiban in unstable angina and non–Q-wave myocardial infarction. N Engl J Med. 1998;338:
 AGGRASTAT® (tirofiban HCl) + Heparin (n=773) RR=30% P=0.02. RR=47% P= RR=43% P= % Patients. P=0.99. Slide 13 PRISM-PLUS: Event Reductions at 7 Days. At 7 days, the AGGRASTAT-plus-heparin group in PRISM-PLUS attained significant reductions compared to heparin alone in the composite endpoint (32%, P=0.004), in refractory ischemia (30%, P=0.02), in MI (47%, P=0.006), and in the combination of MI and death (43%, P=0.006). The incidence of death at 7 days was comparable between the two treatment groups.13. Composite Endpoint. Refractory Ischemia. MI. Death. MI/Death. The PRISM-PLUS Study Investigators. N Engl J Med. 1998;338: The Platelet Receptor Inhibition for Ischemic Syndrome Management in Patients Limited by Unstable Signs and Symptoms (PRISM-PLUS) Study Investigators. Inhibition of the platelet glycoprotein IIb/IIIa receptor with tirofiban in unstable angina and non–Q-wave myocardial infarction. N Engl J Med. 1998;338:")
61
PRISM-PLUS: Punto Final Combinado (180 Dias)
= -4.4%, RR=19%, P=0.02 35 Heparin 30 25 AGGRASTAT® (tirofiban HCl) + Heparin 20 % With Endpoint 15 = -3.8%, RR=22%, P=0.029 10 = -5.0%, RR=32%, P=0.004 5 30 60 90 120 150 180 7 Day The PRISM-PLUS Study Investigators. N Engl J Med. 1998;338:
 + Heparin. 20. % With Endpoint. 15. = -3.8%, RR=22%, P= = -5.0%, RR=32%, P= Day. The PRISM-PLUS Study Investigators. N Engl J Med. 1998;338:")
62
PRISM-PLUS: Punto Final Compuesto a los 30 Dias in Pacientes Tratados Medicamente
RR=13% 20 16.8% 14.8% 15 Heparin (n=375) AGGRASTAT® (tirofiban HCl) + Heparin (n=344) 10 10 % Patients 5 The PRISM-PLUS Study Investigators. N Engl J Med. 1998;338:
 AGGRASTAT® (tirofiban HCl) + Heparin (n=344) % Patients. 5. The PRISM-PLUS Study Investigators. N Engl J Med. 1998;338:")
63
EPTIFIBATIDE Heptapeptido cíclico derivado de la barbourina un veneno de la serpiente cascabel del suroeste. Uno de los inhibidores mas rapidos, 80% de inh. A los 15 minutos. PURSUIT IMPACT-II ESPRIT IMPACT-AMI

64
PURSUIT Estudio multicentrico con ptes. UA de alto riesgo, o NSTEMI Menos eficacia en mujeres.

65
PURSUIT Diseño del Estudio
10,948 patients with unstable angina or non-Q-wave MI at 726 centers in 27 countries Heparin (at physician discretion) + aspirin Placebo Eptifibatide (180/1.3) 180 µg/kg bolus+ 1.3 µg/kg/min infusion Eptifibatide (180/2) 180 µg/kg bolus+ 2 µg/kg/min infusion Discontinued due to acceptable safety at higher dose Infusion up to hospital discharge or CABG surgery, up to 72 hours (96 hours in patients undergoing PCI late during course of infusion) Harrington RA. Am J Cardiol. 1997;80:34B-38B.
 + aspirin. Placebo. Eptifibatide (180/1.3) 180 µg/kg bolus+ 1.3 µg/kg/min infusion. Eptifibatide (180/2) 180 µg/kg bolus+ 2 µg/kg/min infusion. Discontinued due to acceptable safety at higher dose. Infusion up to hospital discharge or CABG surgery, up to 72 hours (96 hours in patients undergoing PCI late during course of infusion) Harrington RA. Am J Cardiol. 1997;80:34B-38B.")
66
PURSUIT Muerte o IAM puntos combinados
72 hours 1.7% (P = 0.001) 7 days 1.5% (P = 0.002) 30 days 1.5% (P = 0.042) % Patients with composite events 15.7% 14.2% 11.6% 10.1% 7.6% 5.9%
 7 days. 1.5% (P = 0.002) 30 days. 1.5% (P = 0.042) % Patients with composite events. 15.7% 14.2% 11.6% 10.1% 7.6% 5.9%")
67
PURSUIT Muerte o IAM a los 6 meses combinados
% Patients with composite events 13.6% 12.1% PURSUIT – Investigator-reported death or MI composite within 6 months The six-month endpoint in PURSUIT measured the combined incidence of death or MI as reported by the investigators. At 6 months after randomization, the incidence of the composite endpoint as reported by study investigators was still significantly lower among patients treated with eptifibatide 180/2. Therefore, the very early benefit obtained with a relatively short duration of therapy could still be observed after 6 months.

68
30-Day Death, MI, Urgent Revascularization %
RESUMEN 30-Day Death, MI, Urgent Revascularization % Odds Ratio Trial N Agent IIb/IIIa Control (95% CI) EPIC 2099 Abciximab EPILOG 2792 Abciximab EPISTENT 1603 Abciximab (stent arms only) IMPACT-II 4010 Eptifibatide ESPRIT 2064 Eptifibatide RESTORE 2141 Tirofiban 0.0 0.5 1.0 2.0 Presented at AHA Scientific Sessions Nov. 15, 2000
 EPIC 2099 Abciximab EPILOG 2792 Abciximab EPISTENT 1603 Abciximab (stent arms only) IMPACT-II 4010 Eptifibatide ESPRIT 2064 Eptifibatide RESTORE 2141 Tirofiban Presented at AHA Scientific Sessions Nov. 15,")
69
CUAL ES EL MEJOR DE TODOS Y EL IDEAL ??

70
Cual es mejor?? No hay estudios que puedan compararlos por igual.
Tirofibán produce menos grado de inhibición plaquetaria en los 15 a 60 minutos CRUCIALES luego de la PCI. Solo hay 1 trabajo: TARGET Comparo Abciximab vs. Tirofiban 4809 ptes. Topol EJ; Moliterno DJ; Herrmann HC; Powers ER; Grines C, N Engl J Med 2001 Jun 21;344(25):
:")
71
Punto Final Primario TARGET trial
30 day Death, MI, Urgent TVR RR = 1.26 Non-inferiority boundary Upper bound of 95% confidence interval = 1.51 p=0.038 RR = 1.26 1.47 10.0% 9.0% 7.6% Abciximab better 8.0% 6.0% 7.0% 30 day Death, MI, Urgent TVR (%) 6.0% 1.00 5.0% 4.0% Tirofiban better 3.0% 2.0% 1.0% 0.0% Tirofiban Abciximab N Engl J Med 2001;344:
 6.0% % 4.0% Tirofiban. better. 3.0% 2.0% 1.0% 0.0% Tirofiban. Abciximab. N Engl J Med 2001;344:")
72
6-Meses, Eventos Combinados (Muerte/IAM/TVR)
TARGET trial 0.20 Tirofiban, N=2398 P=0.591 HR 1.04 95% CI: 0.90,1.21 Abciximab, N=2411 14.8% 0.15 14.3% Composite Event Rate 0.10 0.05 0.00 30 60 90 120 150 180 Days Topol EJ; Moliterno DJ; Herrmann HC; Powers ER; Grines C, N Engl J Med 2001 Jun 21;344(25):
:")
73
CONCLUSION (Metanalisis)
Meta-analisis con 6 trabajos. pacientes Los Inh. GP IIb/IIIa, son de beneficio substancial en pacientes con UA/NSTEMI, quienes van a ser sometidos a intervencionismo.(justo antes del intervencionismo) Nivel de Evidencia I El beneficio principal es visto en pacientes de alto riesgo (Troponina alta, TIMI risk score > 4, ptes con isquemia recurrente, cambios eléctricos) Evidencia IIa Son de beneficio QUESTIONABLE en quienes NO van a ser sometidos a PCI. Nivel de evidencia IIb-III con abciximab. *Boersma E; Harrington RA; Moliterno DJ; A meta-analysis of all major randomised clinical trials. Lancet 2002 Jan 19;359(9302):
 Nivel de Evidencia I. El beneficio principal es visto en pacientes de alto riesgo (Troponina alta, TIMI risk score > 4, ptes con isquemia recurrente, cambios eléctricos) Evidencia IIa. Son de beneficio QUESTIONABLE en quienes NO van a ser sometidos a PCI. Nivel de evidencia IIb-III con abciximab. *Boersma E; Harrington RA; Moliterno DJ; A meta-analysis of all major randomised clinical trials. Lancet 2002 Jan 19;359(9302):")
74
Y... QUE PASA EN EL MUNDO REAL..???

75
CRUSADE: A National Quality Improvement Initiative
Can Rapid Risk Stratification of Unstable Angina Patients Suppress ADverse Outcomes with Early Implementation of the ACC/AHA Guidelines

76
Objetivos Determinar la adherencia de los centros hospitalarios Americanos a las guias de tratamiento de la ACC de UA/NSTEMI. Implementar un Control de Calidad de los centros ante la iniciativa de las guias de tratamiento de la ACC.

77
Site Locations as of 8/23/02 WA (9) VT (0) ME (2) MT (0) ND (1) MI
NH (2) MN (5) OR (2) NY (40) MA (13) SD (1) WI (5) ID (1) MI (21) RI (0) WY (0) PA (41) CT (5) IA (4) NJ (12) NE (1) OH (37) DE (3) NV (1) IL (15) IN (7) WV (5) VA (13) MD (14) UT (2) CO (2) KS (5) MO (9) KY (10) DC (2) CA (30) NC (14) TN (13) OK (4) SC (7) AZ (9) AR (5) NM (3) AL (10) GA (13) MS (8) LA (5) TX (20) FL (42) AK (0) HI (3)
 MN. (5) OR. (2) NY. (40) MA (13) SD. (1) WI. (5) ID. (1) MI. (21) RI (0) WY. (0) PA. (41) CT (5) IA. (4) NJ (12) NE (1) OH. (37) DE (3) NV. (1) IL. (15) IN. (7) WV. (5) VA. (13) MD (14) UT. (2) CO. (2) KS. (5) MO. (9) KY. (10) DC (2) CA. (30) NC. (14) TN (13) OK. (4) SC. (7) AZ. (9) AR. (5) NM. (3) AL. (10) GA. (13) MS. (8) LA. (5) TX. (20) FL. (42) AK. (0) HI (3)")
78
Uso de Medicación Aguda (En las 1eras 24 hours)
100% 90% 83% 76% 80% 60% 31% 40% 35% 20% 0% ASA Beta Blockers Heparin (LMW + UFH) GP IIb-IIIa Inhibitors Clopidogrel
 GP IIb-IIIa. Inhibitors. Clopidogrel.")
79
Uso de GP IIb-IIIa Inhibidores
100% 84% 80% 61% 60% 40% 26% 20% 0% Any Use for Patients Undergoing PCI Any Use for Patients Undergoing Diagnostic Cath Use Before Diagnostic Catheterization

80
Rata de Mortalidad temprana
In-hospital mortality rate 4.9% 7-day mortality rate 1.8% 1.9% 1.8% PURSUIT1 (n = 9,461) PRISM-PLUS2 (n = 1,915) GUSTO IV-ACS3 (n = 7,800) CRUSADE (n = 18,937) 1.The PURSUIT Trial Investigators. N Engl J Med 1998 2.The PRISM-PLUS Study Investigators. N Engl J Med 1998 3.The GUSTO IV-ACS Investigators. Lancet 2001
 PRISM-PLUS2 (n = 1,915) GUSTO IV-ACS3 (n = 7,800) CRUSADE (n = 18,937) 1.The PURSUIT Trial Investigators. N Engl J Med The PRISM-PLUS Study Investigators. N Engl J Med The GUSTO IV-ACS Investigators. Lancet")
81
Uso de Medicaciones al Alta
100% 88% 80% 77% 80% 59% 60% 49% 40% 20% 0% ASA Beta Blockers ACE- Lipid Lowering Agent # Clopidogrel Inhibitors * * LVEF < 40%, CHF, DM, HTN # Known hyperlipidemia, TC, LDL

82
CONCLUSIONES Los resultados en la practica son PEORES que en los estudios Clínicos. La Mortalidad en el CRUSADE fue de ~5%: esto es, 3 veces mas alto que los reportados en los estudios Aquellos pacintes con UA/NSTEMI de alto riesgo tuvieron una mortalidad/IAM combinadas del ~12%. Al alta: 40% de los ptes con FdeE baja, HTA o DM2, no se les formuló IECAS. 23% de los pacientes con Hiperlipidemia no se les recetó hipolipemiantes 10% de los ptes. No recibieron ASA 42% de los fumadores no recibieron ayuda para dejar de fumar.

Presentaciones similares



en Ateroesclerosis. Seguridad y Eficacia Presentado en el.>")








 developed ischemia with exercise. During a mean follow-up of 4.5 3.4 years, 313 patients died, and 183 patients had.>")






