Descargar la presentación
La descarga está en progreso. Por favor, espere

1
CALIDAD DE VIDA, ADHERENCIA Y SATISFACCIÓN DEL TRATAMIENTO DE LA HEPATITIS C
Isabel Moya Carmona Hospital Virgen de la Victoria. Málaga Mayo 2011

2
CALIDAD DE VIDA PACIENTE HEPATITIS C ADHERENCIA SATISFACCIÓN

3
ADHERENCIA Y CUMPLIMIENTO
Definición de adherencia y cumplimiento terapéutico: ADHERENCIA TERAPÉUTICA: grado de coincidencia entre la conducta del paciente (toma de medicación, seguir una dieta, cambios en estilo de vida) y las recomendaciones del médico(1). PARTICIPACIÓN ACTIVA DEL PACIENTE CUMPLIMIENTO TERAPÉUTICO: “obediencia” del paciente en relación a las pautas prescritas por su médico (toma de medicación, seguir una dieta, etc.)(2-3). PARTICIPACIÓN NO ACTIVA DEL PACIENTE 1. Haynes. John Hopkins University Press; Karoly. Hillsdale: LEA; 1993. 3. Basterra Gabarró. Pharmaceutical Care 1999. 3 3
 y las recomendaciones del médico(1). PARTICIPACIÓN ACTIVA DEL PACIENTE. CUMPLIMIENTO TERAPÉUTICO: obediencia del paciente en relación a las pautas prescritas por su médico (toma de medicación, seguir una dieta, etc.)(2-3). PARTICIPACIÓN NO ACTIVA DEL PACIENTE. 1. Haynes. John Hopkins University Press; Karoly. Hillsdale: LEA; Basterra Gabarró. Pharmaceutical Care")
4
“Las medicinas no funcionan
en los pacientes que no las toman” C. Everett Koop, M.D

5
Hepatitis C Adherencia terapéutica
Realización del tratamiento a dosis suficientes de interferón pegilado y ribavirina (> 80 %), durante el tiempo prescrito (1) No incluye la retirada del tratamiento por parte del facultativo, debida a ausencia de respuesta. 1. McHutchison JG, et al. Gastroenterology. 2002;123:
, durante el tiempo prescrito (1) No incluye la retirada del tratamiento por parte del facultativo, debida a ausencia de respuesta. 1. McHutchison JG, et al. Gastroenterology. 2002;123:")
6
Factores Predictores de Respuesta al tratamiento
Paciente Edad Sexo Raza Peso Resistencia a la insulina Hígado graso Salud Mental Hábitos tóxicos Cirrosis IL28B status HIV coinfección VHC Genotipo VHC RNA Tratamiento Adherencia a pegIFN/RBV Dosificación RBV ajustada por peso (genotipos 1/4) Mejorar las tasas de respuesta con IP (genotipo 1) PegIFN, peginterferon; RBV, ribavirin. Megan R. Mahoney, MD: Several other factors should be considered when estimating a patient’s likelihood of response to treatment, including older age, male sex, black race, high body mass index, or the presence of insulin resistance, liver disease, cirrhosis, or HIV infection, as these are all negative predictors of response. Dr. Dong, what are some other factors that have been shown to be predictive of response to HCV therapy? Betty J. Dong, PharmD, FASHP, FCCP, AAHIVE: Other patient factors that can have a negative impact on adherence—and therefore, treatment outcomes—include mental illness and substance abuse. Although these issues are not contraindications to standard-of-care therapy, they should be addressed before starting treatment to minimize their impact on outcomes. Another recently identified, powerful predictor of response is IL28B gene status. A genetic polymorphism near the IL28B gene, which encodes interferon 3, correlates with favorable response to HCV therapy. The CC genotype is associated with a 2-fold higher response rate, regardless of race.[1] Of interest, the CC genotype is less frequent in the black population than in the white population, which partly explains the difference in treatment response between these 2 groups. This test recently became commercially available and may be helpful in the management of black patients. Dr. Mahoney, how do genotype and HCV RNA levels affect response? As shown on the previous slide, genotype 2 or 3 HCV is associated with higher response rates compared with genotype 1. In addition, higher HCV RNA levels are associated with a poorer response to standard-of-care therapy. From a pharmacist’s point of view, regimen factors that improve treatment response include adherence, weight-based vs fixed-dose ribavirin dosing in patients with genotype 1 or 4 HCV infection, and the newer agents in development, particularly the HCV protease inhibitors for the treatment of patients with genotype 1 HCV. Other agents in the pipeline include polymerase inhibitors and cyclophilin inhibitors; it is hoped that these agents will continue to increase response rates. Reference 1. Ge E, Fellay J, Thompson AJ, et al. Genetic variation in IL28B predicts hepatitis C treatment-induced viral clearance. Nature. 2009;461: 6
 Mejorar las tasas de respuesta con IP (genotipo 1) PegIFN, peginterferon; RBV, ribavirin. Megan R. Mahoney, MD: Several other factors should be considered when estimating a patient’s likelihood of response to treatment, including older age, male sex, black race, high body mass index, or the presence of insulin resistance, liver disease, cirrhosis, or HIV infection, as these are all negative predictors of response. Dr. Dong, what are some other factors that have been shown to be predictive of response to HCV therapy Betty J. Dong, PharmD, FASHP, FCCP, AAHIVE: Other patient factors that can have a negative impact on adherence—and therefore, treatment outcomes—include mental illness and substance abuse. Although these issues are not contraindications to standard-of-care therapy, they should be addressed before starting treatment to minimize their impact on outcomes. Another recently identified, powerful predictor of response is IL28B gene status. A genetic polymorphism near the IL28B gene, which encodes interferon 3, correlates with favorable response to HCV therapy. The CC genotype is associated with a 2-fold higher response rate, regardless of race.[1] Of interest, the CC genotype is less frequent in the black population than in the white population, which partly explains the difference in treatment response between these 2 groups. This test recently became commercially available and may be helpful in the management of black patients. Dr. Mahoney, how do genotype and HCV RNA levels affect response As shown on the previous slide, genotype 2 or 3 HCV is associated with higher response rates compared with genotype 1. In addition, higher HCV RNA levels are associated with a poorer response to standard-of-care therapy. From a pharmacist’s point of view, regimen factors that improve treatment response include adherence, weight-based vs fixed-dose ribavirin dosing in patients with genotype 1 or 4 HCV infection, and the newer agents in development, particularly the HCV protease inhibitors for the treatment of patients with genotype 1 HCV. Other agents in the pipeline include polymerase inhibitors and cyclophilin inhibitors; it is hoped that these agents will continue to increase response rates. Reference. 1. Ge E, Fellay J, Thompson AJ, et al. Genetic variation in IL28B predicts hepatitis C treatment-induced viral clearance. Nature. 2009;461:")
7
Peg-IFN alfa 2a + Ribavirina Impacto de la Adherencia
EVR 86% (n=390) Week 12 (n=453) Full dose n=245 n=145 < Full dose SVR 75% (n=184) SVR 48% (n=69) SVR 67% (n=63) SVR 12% (n=6) Dose reduction Withdrawal or drop out n=94 n=51 Ferenci. AASLD Fried N Engl J Med
 Week 12. (n=453) Full dose. n=245. n=145. < Full dose. SVR 75% (n=184) SVR 48% (n=69) SVR 67% (n=63) SVR 12% (n=6) Dose. reduction. Withdrawal or drop out. n=94. n=51. Ferenci. AASLD Fried N Engl J Med")
8
La Adherencia al Tratamiento Mejora la Tasa de RVS en Pacientes VHC+
IFN + RBV (n = 1010) PegIFN + RBV (n = 511) 100 80 63 60 Sustained Response Rate (%) 54 53 52 43 38 40 HCV, hepatitis C virus; IFN, interferon; PegIFN, peginterferon; QoL, quality of life; SVR sustained virologic response. This slide shows how treatment adherence improves SVR rates in HCV‑infected patients. The blue bar depicts patients who received interferon plus ribavirin, and the orange bar shows those who received peginterferon plus ribavirin. As you can see, SVR rates improve with better adherence to therapy; therefore, providers and patients should strive to maintain the 80/80/80 rule, which aims for continued prescription of ≥ 80% of interferon doses and ≥ 80% of ribavirin doses for ≥ 80% of the planned treatment duration. 17 20 16 n = 58 35 68 24 111 72 142 75 631 305 10 30 50 70 90 Adherence (%) McHutchison JG, et al. Gastroenterology. 2002;123: 8
 PegIFN + RBV (n = 511) Sustained Response Rate (%) HCV, hepatitis C virus; IFN, interferon; PegIFN, peginterferon; QoL, quality of life; SVR sustained virologic response. This slide shows how treatment adherence improves SVR rates in HCV‑infected patients. The blue bar depicts patients who received interferon plus ribavirin, and the orange bar shows those who received peginterferon plus ribavirin. As you can see, SVR rates improve with better adherence to therapy; therefore, providers and patients should strive to maintain the 80/80/80 rule, which aims for continued prescription of ≥ 80% of interferon doses and ≥ 80% of ribavirin doses for ≥ 80% of the planned treatment duration n = Adherence (%) McHutchison JG, et al. Gastroenterology. 2002;123:")
9
Peg-IFN alfa 2b + RBV IFN alfa 2a + RBV 100 89 82 90 80 63 54 52 51 60
IT 42 > 80/80/80 34 40 < 80/80/80 20 Global G 1 G 2/3 MC Hutchison JG; Gastroenterology 2002 IFN alfa 2a + RBV 100 80 74 80 52 60 IT 44 39 Adherencia 31 33 40 No adherencia 20 8 Global G 1 G 2/3 Solà R et al; AIDS Res & Hum Retrov 2005

10
RVS y % Exposición al Fármaco (Genotype 1)
90 % Exposure: P = 0.259 P < 0.001 <80 80 72 70 65 64 59 57 60 56 57 100 49 SVR (%) 50 40 30 20 10 Cumulative Exposure to PEG-IFN alpha 2a Cumulative Exposure to RIBAVIRIN Exposure = related to dose & duration Reddy et al. EASL 2004
 Cumulative Exposure to PEG-IFN alpha 2a. Cumulative Exposure to RIBAVIRIN. Exposure = related to dose & duration. Reddy et al. EASL")
11
Métodos para medir la Adherencia
1. Directos Ventajas Inconvenientes Observación directa Muy preciso Pueden esconder comprimidos en la boca Imposible en práctica clínica Medición niveles (fármaco/metabolito) Objetivo Variaciones metabolismo Muy caro Medición marcador biológico Objetivo Puede ser útil para medir placebo Requiere análisis caro y extracción fluídos corporales Osterberg, Blaschke. Adherence to the medication. NEJM 2005
 Objetivo. Variaciones metabolismo. Muy caro. Medición marcador biológico. Objetivo. Puede ser útil para medir placebo. Requiere análisis caro y extracción fluídos corporales. Osterberg, Blaschke. Adherence to the medication. NEJM")
12
Métodos para medir la Adherencia
2. Indirectos (1) Ventajas Inconvenientes Cuestionarios autoadministrados/familiares o cuidadores Simple Económico Muy útil en clínica Susceptible de error que aumenta con el tiempo entre visitas Posibilidad de alteración Contaje de comprimidos Objetivo Cuantificable Fácil Posibilidad de alteración (tirar comp.) Diarios de pacientes Mejoran el posible olvido Posibilidad de alteración Osterberg, Blaschke. Adherence to the medication. NEJM 2005
 Ventajas. Inconvenientes. Cuestionarios autoadministrados/familiares o cuidadores. Simple. Económico. Muy útil en clínica. Susceptible de error que aumenta con el tiempo entre visitas. Posibilidad de alteración. Contaje de. comprimidos. Objetivo. Cuantificable. Fácil. Posibilidad de alteración (tirar comp.) Diarios de pacientes. Mejoran el posible olvido. Posibilidad de alteración. Osterberg, Blaschke. Adherence to the medication. NEJM")
13
Métodos para medir la Adherencia
2. Indirectos (2) Ventajas Inconvenientes Valoración de la respuesta clínica Simple Fácil La respuesta puede depender de otros factores Valoración de la respuesta clínica Simple Fácil La respuesta puede depender de otros factores Monitores electrónicos de medicación Preciso Cuantificable Permite control continuado Muy caro Requiere más visitas para control de los monitores Monitores electrónicos de medicación Preciso Cuantificable Permite control continuado Muy caro Requiere más visitas para control de los monitores Medición de marcadores fisiológicos (PE frecuencia cardíaca - beta bloqueantes) Puede ser fácil El marcador puede variar por otras razones (mayor metabolismo, falta de absorción, falta de respuesta) Osterberg, Blaschke. Adherence to the medication. NEJM 2005
 Ventajas. Inconvenientes. Valoración de la respuesta clínica. Simple. Fácil. La respuesta puede depender de otros factores. Valoración de la respuesta clínica. Simple. Fácil. La respuesta puede depender de otros factores. Monitores electrónicos de medicación. Preciso. Cuantificable. Permite control continuado. Muy caro. Requiere más visitas para control de los monitores. Monitores electrónicos de medicación. Preciso. Cuantificable. Permite control continuado. Muy caro. Requiere más visitas para control de los monitores. Medición de marcadores fisiológicos. (PE frecuencia cardíaca - beta bloqueantes) Puede ser fácil. El marcador puede variar por otras razones (mayor metabolismo, falta de absorción, falta de respuesta) Osterberg, Blaschke. Adherence to the medication. NEJM")
14
Cuestionario Adhepta Es importante detectar los pacientes no cumplidores con el tratamiento, ya que de esta forma se podría reducir el número de abandonos. Se estima que más del 25% de los pacientes no completan el tratamiento para la hepatitis C (1). Para medir la adherencia al tratamiento existen diversos cuestionarios (Morisky-Green, Haynes-Sackett, GEMMA, etc.) ninguno específico para pacientes con hepatitis C. Se ha desarrollado y se está actualmente validando un cuestionario de adherencia al tratamiento para pacientes con infección por VHC (4) :Morisky-Green(2) ‘gold estándar’(3). 1. Camma C Expert Opin Pharmacother 2005 2. Morisky et al. Med Care 1986. 3. Ros et al. REEMO 2002. 4. Solà et al. XX Congrés de la Societat Catalana de Digestologia Enero 2011 Abstract Ref.: T 14
. Para medir la adherencia al tratamiento existen diversos cuestionarios (Morisky-Green, Haynes-Sackett, GEMMA, etc.) ninguno específico para pacientes con hepatitis C. Se ha desarrollado y se está actualmente validando un cuestionario de adherencia al tratamiento para pacientes con infección por VHC (4) :Morisky-Green(2) ‘gold estándar’(3). 1. Camma C Expert Opin Pharmacother Morisky et al. Med Care Ros et al. REEMO Solà et al. XX Congrés de la Societat Catalana de Digestologia Enero 2011 Abstract Ref.: T. 14.")
17
Desarrollo y validación de un cuestionario de adherencia al tratamiento en pacientes con infección por Virus de la Hepatitis C Solà R1, Martín-Suárez JM2, Castellano G3, Tural C4, Pérez-Álvarez R5, de Cuenca B6, Castro MA7, Turnes-Vázquez J8, Molina E9, Ripolles V10, Alcántara R11, Diago M12, Hernández-Quero J13, Planas R14, en nombre de los investigadores del estudio ADHEPTA 1Hospital del Mar, IMIM, Barcelona, 2Hospital de Gran Canaria Dr. Negrín, Las Palmas de Gran Canaria, 3Hospital Universitario 12 de Octubre, Madrid, 4Hospital Germans Trias i Pujol, Barcelona, 5Hospital Universitario Central de Asturias, Oviedo, 6Hospital Infanta Cristina, Madrid, 7Hospital Universitario de A Coruña, A Coruña, 8Complejo Hospitalario de Pontevedra, Pontevedra, 9Hospital Clínico De Santiago, Santiago De Compostela, 10Hospital General de Castellón, Castellón de la Plana, 11Hospital Clínico Virgen de la Victoria, Málaga, 12Hospital General Universitario, Valencia, 13 Hospital Universitario San Cecilio, Granada, 14Hospital Germans Trias i Pujol, CIBEREHD, Barcelona 17 XX Congrés de la Societat Catalana de Digestologia (27-29 Enero 2011) Abstract Ref.: T
 Abstract Ref.: T.")
18
FASE I- Elaboración del cuestionario de adherencia
FASE II- Validación del cuestionario (estudio epidemiológico) Solà et al. XX Congrés de la Societat Catalana de Digestologia Enero 2011 Abstract Ref.: T
 Solà et al. XX Congrés de la Societat Catalana de Digestologia Enero 2011 Abstract Ref.: T.")
19
Fase I:Desarrollo del cuestionario de adherencia
Los objetivos de la fase de elaboración fueron: Obtener un cuestionario válido: - Que el cuestionario mida el grado de adherencia con el tratamiento en paciente con hepatitis C (validez de contenido) MONOINFECTADOS Y COINFECTADOS Obtener un cuestionario factible: - Cuestionario breve (pocos items) - Fácil interpretación de la puntuación Obtener un cuestionario con alta sensibilidad y especificidad Solà et al. XX Congrés de la Societat Catalana de Digestologia Enero 2011 Abstract Ref.: T 19
 MONOINFECTADOS Y COINFECTADOS. Obtener un cuestionario factible: - Cuestionario breve (pocos items) - Fácil interpretación de la puntuación. Obtener un cuestionario con alta sensibilidad y especificidad. Solà et al. XX Congrés de la Societat Catalana de Digestologia Enero 2011 Abstract Ref.: T. 19.")
20
Fase I: Desarrollo del cuestionario de adherencia
ETAPAS DE LA ELABORACIÓN ACCIONES RESULTADOS IDENTIFICACIÓN DE ATRIBUTOS REVISIÓN BIBLIOGRÁFICA LISTADO PRELIMINAR REUNIÓN GRUPO EXPERTOS ANALISIS Y SELECCIÓN DE ITEMS 1ª VERSION CUESTIONARIO ANALISIS CUALITATIVO 2ª VERSION/ CUESTIONARIO FINAL VALIDACIÓN PRELIMINAR Y COMPRENSIÓN CUESTIONARIO ESTUDIO PILOTO-VALIDEZ CONTENIDO con 18 pacientes Solà et al. XX Congrés de la Societat Catalana de Digestologia Enero 2011 Abstract Ref.: T 20

21
Desarrollo del cuestionario de adherencia
REVISIÓN BIBLIOGRÁFICA La revisión de la literatura realizada a través de diferentes bases de datos, como ‘Medline’ y ‘Índice Médico Español’. REUNIÓN GRUPO EXPERTOS ANALISIS CUALITATIVO ESTUDIO PILOTO-VALIDEZ CONTENIDO con 18 pacientes REVISIÓN BIBLIOGRÁFICA Identificación de los aspectos más importantes en relación a la adherencia con el tratamiento REUNIÓN GRUPO EXPERTOS ANALISIS CUALITATIVO ESTUDIO PILOTO-VALIDEZ CONTENIDO con 18 pacientes Supervisión del contenido del cuestionario. Reclutamiento/selección de pacientes que participen en el estudio piloto (18 pacientes). Solà et al. XX Congrés de la Societat Catalana de Digestologia Enero 2011 Abstract Ref.: T 21
. Solà et al. XX Congrés de la Societat Catalana de Digestologia Enero 2011 Abstract Ref.: T. 21.")
22
Desarrollo del cuestionario de adherencia
Motivos que afectan a la adherencia Cansancio o empeoramiento de la fatiga 2.Alteración del estado de ánimo (Ansiedad/ depresión/irritabilidad/tristeza/perdida de interés) 3.Percepción sobre la información recibida sobre el curso del tratamiento y sus posibles efectos secundarios (posibles respuestas al tratamiento) 4.Duración del tratamiento 5.Olvido tomar la medicación 6.Disponibilidad de acceso a los controles/recogida de medicación (horarios y días concretos de recogida) relacionado con la enfermedad 7.Grado de conocimiento que tiene el paciente sobre su enfermedad, sus consecuencias. 8. Conocimiento sobre el posible impacto del tratamiento de la Hep C sobre la eficacia del tratamiento anti VIH (SOLO COINFECTADOS) 9.Pérdida de peso durante el tratamiento para su enfermedad (SOLO CONINFECTADOS) 10.Impacto en la actividad laboral (perdida de días actividad laboral, ausencias laborales, retrasos horarios) 11.Percepción de sentirse cuidado y apoyado Solà et al. XX Congrés de la Societat Catalana de Digestologia Enero 2011 Abstract Ref.: T 22
 3.Percepción sobre la información recibida sobre el curso del tratamiento y sus posibles efectos secundarios (posibles respuestas al tratamiento) 4.Duración del tratamiento. 5.Olvido tomar la medicación. 6.Disponibilidad de acceso a los controles/recogida de medicación (horarios y días concretos de recogida) relacionado con la enfermedad. 7.Grado de conocimiento que tiene el paciente sobre su enfermedad, sus consecuencias. 8. Conocimiento sobre el posible impacto del tratamiento de la Hep C sobre la eficacia del tratamiento anti VIH (SOLO COINFECTADOS) 9.Pérdida de peso durante el tratamiento para su enfermedad (SOLO CONINFECTADOS) 10.Impacto en la actividad laboral (perdida de días actividad laboral, ausencias laborales, retrasos horarios) 11.Percepción de sentirse cuidado y apoyado. Solà et al. XX Congrés de la Societat Catalana de Digestologia Enero 2011 Abstract Ref.: T. 22.")
23
Desarrollo del cuestionario de adherencia
Diseño del formato del cuestionario: Establecimiento de los enunciados y formato visual del cuestionario. Diseño adaptado para que el cuestionario sea autoadministrado. Primera versión del cuestionario. REVISIÓN BIBLIOGRÁFICA REUNIÓN GRUPO EXPERTOS ANALISIS CUALITATIVO ESTUDIO PILOTO-VALIDEZ CONTENIDO con 18 pacientes REVISIÓN BIBLIOGRÁFICA Administración a una muestra de pacientes (Estudio Piloto): Administración de la primera versión del cuestionario a una muestra de 18 pacientes en tratamiento para la hepatitis C (8 coinfectados y 10 monoinfectados) en los que se evaluó: la comprensión de las preguntas y categorías de respuesta aplicabilidad de las preguntas opinión sobre el diseño del cuestionario. REUNIÓN GRUPO EXPERTOS ANALISIS CUALITATIVO ESTUDIO PILOTO-VALIDEZ CONTENIDO con 18 pacientes Solà et al. XX Congrés de la Societat Catalana de Digestologia Enero 2011 Abstract Ref.: T 23
: Administración de la primera versión del cuestionario a una muestra de 18 pacientes en tratamiento para la hepatitis C (8 coinfectados y 10 monoinfectados) en los que se evaluó: la comprensión de las preguntas y categorías de respuesta. aplicabilidad de las preguntas. opinión sobre el diseño del cuestionario. REUNIÓN GRUPO EXPERTOS. ANALISIS CUALITATIVO. ESTUDIO PILOTO-VALIDEZ CONTENIDO con 18 pacientes. Solà et al. XX Congrés de la Societat Catalana de Digestologia Enero 2011 Abstract Ref.: T. 23.")
24
Versión Final del Cuestionario
Módulo A: Preguntas directas sobre la adherencia a la medicación. Compuesto por dos preguntas: RBV, peg-IFN En relación con el tratamiento que recibe para la Hepatitis C, ¿cuántas inyecciones/tomas de comprimidos ha dejado de ponerse/tomar durante las últimas cuatro semanas/última semana? Ninguna Alguna vez Nº de veces ____________ Módulo B: Preguntas relacionadas con factores que influyen en la adherencia 1- He dejado de tomar la medicación porque me siento más cansado debido al tratamiento para la hepatitis C - Nunca dejo de tomar la medicación por este motivo - Alguna vez he dejado de tomar la medicación por este motivo 5-He dejado de tomar la medicación porque los horarios para recoger la medicación y de las visitas de control se adaptan poco a los horarios de mi vida diaria - He dejado de tomar la medicación porque pierdo peso desde que tomo la medicación para la Hepatitis C (sólo en coinfectados) Solà et al. XX Congrés de la Societat Catalana de Digestologia Enero 2011 Abstract Ref.: T
 Solà et al. XX Congrés de la Societat Catalana de Digestologia Enero 2011 Abstract Ref.: T.")
25
Fase II: Validación del Cuestionario
Metodología Diseño Estudio epidemiológico, prospectivo y multicéntrico, según la práctica clínica habitual Investigadores Participarán 120 investigadores que traten pacientes con VHC, incluyendo un total de pacientes: 800 pacientes monoinfectados 320 pacientes coinfectados Solà et al. XX Congrés de la Societat Catalana de Digestologia Enero 2011 Abstract Ref.: T 25

26
Fase II: Objetivos del estudio
Objetivo principal Validar un cuestionario de adherencia al tratamiento para pacientes con infección por el VHC. Objetivos secundarios Describir la adherencia al tratamiento en pacientes con VHC a lo largo del tiempo (regla del 80/80/80) Establecer la relación entre la adherencia y la Respuesta Viral (RV) y Respuesta Viral Sostenida (RVS). Identificar aquellos factores relacionados con la baja adherencia en pacientes monoinfectados y en pacientes co-infectados. Evaluar la evolución de la CVRS de pacientes con VHC monoinfectados y de pacientes co-infectados Solà et al. XX Congrés de la Societat Catalana de Digestologia Enero 2011 Abstract Ref.: T 26
 Establecer la relación entre la adherencia y la Respuesta Viral (RV) y Respuesta Viral Sostenida (RVS). Identificar aquellos factores relacionados con la baja adherencia en pacientes monoinfectados y en pacientes co-infectados. Evaluar la evolución de la CVRS de pacientes con VHC monoinfectados y de pacientes co-infectados. Solà et al. XX Congrés de la Societat Catalana de Digestologia Enero 2011 Abstract Ref.: T. 26.")
27
Objetivos y diseño del estudio
Esquema del estudio Basal 1 mes 2 meses 3 meses 6 meses Visitas cada 6 meses durante el tratamiento Ultima visita a las 24 semanas después de finalizar el tratamiento visita opcional El periodo de inclusión de pacientes será de 9 meses Solà et al. XX Congrés de la Societat Catalana de Digestologia Enero 2011 Abstract Ref.: T 27

28
Adherencia: Factores Dependientes
CUMPLIMIENTO TERAPÉUTICO PACIENTE PROFESIONAL SANITARIO FÁRMACO TIPO Y DOSIS DEL FÁRMACO VÍA DE ADMINISTRACIÓN DURACIÓN DEL TRATAMIENTO EFECTOS SECUNDARIOS MOTIVACIÓN EDUCACIÓN E INFORMACIÓN DEL ENFERMO RELACIÓN PACIENTE-PROFESIONAL SANITARIO CALIDAD DE LA INFORMACIÓN RECIBIDA ACCESIBILIDAD DEL PROFESIONAL SANITARIO

29
Factores Predictores de Baja Adherencia al tratamiento
Relacionados con el paciente y el tratamiento Tratamiento de enfermedad asintomática Problemas psicológicos: depresion Falta de confianza en el beneficio del tratamiento Complejidad del tratamiento Efectos adversos Otros Mala relación profesional/paciente Seguimiento o continuidad asistencial inadecuada No asistencia a consulta Coste del tratamiento, copago This slide shows the major predictors of poor adherence to medication and gives an idea of how we can intervene early in treatment. Patient and treatment factors to be aware of are treatment of asymptomatic disease; the presence of psychological problems, particularly depression; a patient’s lack of belief in the benefit of treatment; the complexity of the treatment; and adverse events. Other factors that perhaps are harder to quantify are a poor provider‑patient relationship, inadequate follow‑up or discharge planning, missed appointments, and the cost of medication, copayment, or both. Osterberg L, et al. N Engl J Med. 2005;353: 29 29

30
Estrategias de Mejora de la Adherencia al Tratamiento
IDENTIFICAR PRECOZMENTE FACTORES DE RIESGO DE BAJA ADHERENCIA EDUCACIÓN E INFORMACIÓN Hacer especial hincapié al paciente en la importancia del tratamiento Instrucciones claras y sencillas, intentando simplificar el tratamiento Adaptar el tratamiento al estilo de vida del paciente Soporte adecuado para familiares y amigos MANEJO Y CONTROL DE LOS EFECTOS ADVERSOS MOTIVACIÓN Pt, patient. Improving adherence can be achieved by identifying some of these risk factors early and intervening accordingly. The provider can emphasize the value of the regimen and the potential results that can be achieved. In addition, providing comprehensive, clear instructions, and reinforcing them when necessary can help adherence. The use of medication dispensing packaging should be encouraged where available, and customizing a regimen to a patient’s lifestyle should be done when possible. Support from the patient’s family and community should always be encouraged. Finally, medications that have fewer adverse events should be prescribed when possible, such as medications that have longer half‑lives, as we noted with the change from 3-times-weekly interferon to peginterferon and those that have a sustained release formulation. Osterberg L, et al. N Engl J Med. 2005;353: 30 30

31
Información al paciente
ORAL ESCRITA Al paciente Al entorno Asegurar buena accesibilidad 31

32
Información al Paciente
Qué es el virus C, genotipos Epidemiología, formas de contagio Historia natural Sistemas de diagnóstico Tratamiento, expectativas de curación Efectos secundarios Importancia del cumplimiento Hábitos de vida Recomendaciones a familiares y amigos ATENCIÓN MÉDICA Y FARMACEÚTICA 32

33
Manejo de Efectos Adversos
ANTICIPACIÓN: Un correcto conocimiento y manejo de los EA evita retiradas o reducciones de dosis Impacto negativo en el objetivo del tratamiento y en QoL El manejo de los EA debe comenzar en el inicio del tratamiento, e incluso antes: INFORMACIÓN AL PACIENTE Son comunes: aparecen en la mayoría de los pacientes 10%-14% de los pacientes interrumpen el tratamiento a causa de EA La gravedad y naturaleza de los efectos adversos es muy variable pegIFN, peginterferon; RBV, ribavirin. Betty J. Dong, PharmD, FASHP, FCCP, AAHIVE: This slide summarizes some of the key adverse effect management principles that we use in our clinic. Adverse effects of HCV therapy are common and will occur in nearly all patients; therefore, the issue is not whether these events will occur but what to expect when they do occur and how to manage them. The type and severity of the toxicity is highly variable, but it will negatively affect treatment outcome and quality of life. During therapy with peginterferon and ribavirin, approximately 10% to 14% of patients will discontinue treatment because of adverse effects. It is essential that patients understand that these events will occur and that adverse effect management begins before treatment begins. 1. Seeff LB, et al. Semin Liver Dis. 2010;30: 33

34
M. Varela. Proyecto Irys.Jornadas Ghevi 2010

35
Efectos Adversos PEG-IFN
AE Occurring in > 20% of Pts, % PegIFN alfa-2a/RBV (n = 1035) PegIFN alfa-2b/RBV (n = 1019) Fatigue/insomnia 64/41 67/38 Headache 41 50 Nausea 34 40 Anemia 35 Rash 29 Neutropenia 31 26 Irritability/depression 25/20 25/25 Chills 23 39 Injection-site reactions Myalgia/arthralgia 22/22 27/21 Dyspnea 22 21 Pyrexia Anorexia Alopecia 17 AE, adverse event; pegIFN, peginterferon; RBV, ribavirin. Megan R. Mahoney, MD: This slide lists the adverse events associated with peginterferon use. 35
 PegIFN alfa-2b/RBV. (n = 1019) Fatigue/insomnia. 64/41. 67/38. Headache Nausea Anemia. 35. Rash. 29. Neutropenia Irritability/depression. 25/20. 25/25. Chills Injection-site reactions. Myalgia/arthralgia. 22/22. 27/21. Dyspnea Pyrexia. Anorexia. Alopecia. 17. AE, adverse event; pegIFN, peginterferon; RBV, ribavirin. Megan R. Mahoney, MD: This slide lists the adverse events associated with peginterferon use. 35.")
36
Trastornos Psiquiátricos
Causa más habitual de interrupción del tratamiento (1) No es una contraindicación absoluta Atención Multidisciplinar Detección precoz (cuestionarios riesgo: PHQ) Control psicólogo-psiquiatra en casos positivos Antidepresivos ISRS Discontinuar tratamiento en casos graves Dieperink E. Am J Psychiatry 2000; 157:867-76 36
 No es una contraindicación absoluta. Atención Multidisciplinar. Detección precoz (cuestionarios riesgo: PHQ) Control psicólogo-psiquiatra en casos positivos. Antidepresivos ISRS. Discontinuar tratamiento en casos graves. Dieperink E. Am J Psychiatry 2000; 157:")
37
Efectos Adversos RBV Graves Frecuentes y leves
AE Occurring in > 15% of Pts, % Graves Anemia Hemolítica 15-25% Teratogenicidad - Frecuentes y leves Hiperuricemia 20% Molestias GI leves 15% Tos 17% Rash Prurito 12% Insomnio AE, adverse event; pegIFN, peginterferon; RBV, ribavirin. Megan R. Mahoney, MD: This slide lists the adverse events associated with peginterferon use. 37

38
Anemia Inducida por RBV
Reversible y Autolimitada Dosis-Dependiente: Reducción dosis RBV (1) Influye negativamente en la calidad de vida y adherencia al tratamiento La disminución media máxima de Hb de g/dL aparece en las primeras 2-4 semanas Ficha técnica: Reducir dosis 200 mg/dia si Hb<10g/dL Si Hb<8,5g/dL: Suspender ¿USO DE ERITROPOYETINA? CV, cardiovascular; Hb, hemoglobin; RBV, ribavirin; RVR, rapid virologic response; SOB, shortness of breath; SVR, sustained virologic response. Megan R. Mahoney, MD: Ribavirin-induced anemia during the first 4-8 weeks of therapy correlates with an increased probability of achieving an RVR or an SVR. For this reason, anemia is considered a somewhat favorable event when treating HCV infection. However, complications associated with anemia, such as fatigue, shortness of breath, cardiovascular disease, or a decrease in quality of life, can lead to dose reduction or discontinuation of treatment. Betty J. Dong, PharmD, FASHP, FCCP, AAHIVE: Although drug toxicity is an unfavorable outcome, in this setting, anemia provides an indication that the drug is working. In our clinic, we generally counsel patients on the relationship between anemia and response so that they are often pleased to receive laboratory results indicating the presence of anemia. For more information, go online to: 1. Rapatopoulou et al. J Viral Hepat 2005;12:91-95 38
 Influye negativamente en la calidad de vida y adherencia al tratamiento. La disminución media máxima de Hb de g/dL aparece en las primeras 2-4 semanas. Ficha técnica: Reducir dosis 200 mg/dia si Hb<10g/dL. Si Hb<8,5g/dL: Suspender. ¿USO DE ERITROPOYETINA CV, cardiovascular; Hb, hemoglobin; RBV, ribavirin; RVR, rapid virologic response; SOB, shortness of breath; SVR, sustained virologic response. Megan R. Mahoney, MD: Ribavirin-induced anemia during the first 4-8 weeks of therapy correlates with an increased probability of achieving an RVR or an SVR. For this reason, anemia is considered a somewhat favorable event when treating HCV infection. However, complications associated with anemia, such as fatigue, shortness of breath, cardiovascular disease, or a decrease in quality of life, can lead to dose reduction or discontinuation of treatment. Betty J. Dong, PharmD, FASHP, FCCP, AAHIVE: Although drug toxicity is an unfavorable outcome, in this setting, anemia provides an indication that the drug is working. In our clinic, we generally counsel patients on the relationship between anemia and response so that they are often pleased to receive laboratory results indicating the presence of anemia. For more information, go online to: 1. Rapatopoulou et al. J Viral Hepat 2005;12:")
39
M. Varela. Proyecto Irys.Jornadas Ghevi 2010

40
EA Reportados con TVR y BOC
Telaprevir[1] Boceprevir[2] Adverse Event, % TVR-Containing Arms (n = 727) PegIFN/RBV Arm (n = 361) Pruritus 45-50 36 Nausea 40-43 31 Rash 35-37 24 Anemia 37-39 19 Diarrhea 28-32 22 BOC, boceprevir; pegIFN, peginterferon; RBV, ribavirin; TVR, telaprevir. Megan R. Mahoney, MD: How do the protease inhibitors contribute to the adverse events that are reported when used in HCV treatment? In general, adverse effects are reported more frequently with telaprevir- and boceprevir-containing regimens. Telaprevir has been shown to be associated with higher rates of pruritus, nausea, rash, anemia, and diarrhea relative to peginterferon/ribavirin alone, and boceprevir has been reported to be associated with higher rates of anemia and dysgeusia, which is a bad taste in the mouth and is a common adverse effect of interferon therapy. For more information, go online to: For more information, go online to: Adverse Event, % BOC-Containing Arms (n = 734) PegIFN/RBV Arm (n = 363) Anemia 49 29 Dysgeusia 37-43 18 1. Jacobson IM, et al. AASLD Abstract Poordad F, et al. AASLD Abstract LB4. 40
 PegIFN/RBV Arm (n = 361) Pruritus Nausea Rash Anemia Diarrhea BOC, boceprevir; pegIFN, peginterferon; RBV, ribavirin; TVR, telaprevir. Megan R. Mahoney, MD: How do the protease inhibitors contribute to the adverse events that are reported when used in HCV treatment In general, adverse effects are reported more frequently with telaprevir- and boceprevir-containing regimens. Telaprevir has been shown to be associated with higher rates of pruritus, nausea, rash, anemia, and diarrhea relative to peginterferon/ribavirin alone, and boceprevir has been reported to be associated with higher rates of anemia and dysgeusia, which is a bad taste in the mouth and is a common adverse effect of interferon therapy. For more information, go online to: For more information, go online to: Adverse Event, % BOC-Containing Arms. (n = 734) PegIFN/RBV Arm (n = 363) Anemia Dysgeusia Jacobson IM, et al. AASLD Abstract Poordad F, et al. AASLD Abstract LB")
41
¿Cómo modificará la aprobación de TVR y BOC al manejo de EA?
La aparición de nuevos efectos adversos requerirá ofrecer información adicional pre-tratamiento y mayor control y manejo durante el tratamiento Anemia Reducción de dosis de RBV? EPO? Rash Antihistamínicos, esteroides tópicos Control estrecho de aparición de reacciones cutáneas Disgeusia Mejorar la higiene oral Colutorios antibacterianos Chicles/caramelos sin azúcar AE, adverse event; BOC, boceprevir; RBV, ribavirin; TVR, telaprevir. Betty J. Dong, PharmD, FASHP, FCCP, AAHIVE: How will adverse effect management change with the approval of telaprevir and boceprevir? The incidence of adverse effects is expected to increase, requiring additional pretreatment counseling, on-treatment monitoring, and event management. For the patient, this increase translates to additional clinic visits and possibly additional laboratory testing. As noted, the incidence of anemia increases with both HCV protease inhibitors, suggesting that there might be a greater need for ribavirin dose reduction as well as increased use of epoetin alfa. These changes may also increase treatment costs. A relatively high incidence of rash has been reported with telaprevir, and severe cutaneous reactions can also occur. Therefore, patients will require closer monitoring and antihistamines, topical steroids, or systemic steroids may be required. Finally, dysgeusia or bad taste is a frequent adverse effect with boceprevir therapy. The etiology of this effect is unknown, but supportive measures including improving oral hygiene, using antibacterial mouth rinses, and using sugarless gums and mints may make patients more comfortable. 41

42
La Educación al Paciente Influye en la Adherencia al Tratamiento VHC
Estudio observacional en la práctica real de las tasas de adherencia a los 6 meses en pacientes genotipo 2/3 RVS :77% de pacientes con educación terapéutica vs % de pacientes sin educación terapéutica (p= .05) Adherence Rate, % Therapeutic Education (n = 208) No Therapeutic Education (n = 175) P Value PegIFN alfa-2b/RBV 61 47 .01 PegIFN alfa-2b 78 69 .06 RBV 70 56 .006 HCV, hepatitis C virus; pegIFN, peginterferon; RBV, ribavirin; SVR, sustained virologic response. Betty J. Dong, PharmD, FASHP, FCCP, AAHIVE: Patient education can influence adherence to HCV treatment. In this univariate analysis of adherence rates at 6 months from a French cohort of patients with genotype 2/3 HCV infection, therapeutic education for the first 3 months was associated with significantly higher adherence rates to peginterferon alfa-2b/ribavirin relative to no therapeutic education (P = .01), particularly for the ribavirin component (P = .006). Other studies have reported higher adherence to peginterferon than ribavirin.[1] In this study, 77% of patients with therapeutic education achieved SVR vs 70% of patients without therapeutic education. A multivariate analysis showed that after adjustment for various baseline factors, therapeutic education increased the probability of adherence at 6 months by approximately 58%, reflecting a significant benefit (P = .04). These findings emphasize the importance of educating patients on what to expect when they receive HCV therapies. Reference 1. Lo Re V 3rd, Amorosa VK, Localio AR, et al. Adherence to hepatitis C virus therapy and early virologic outcomes. Clin Infect Dis. 2009;48: Cacoub P, et al. World J Gastroenterol. 2008;14: 42
 Adherence Rate, % Therapeutic Education (n = 208) No Therapeutic Education (n = 175) P Value. PegIFN alfa-2b/RBV PegIFN alfa-2b RBV HCV, hepatitis C virus; pegIFN, peginterferon; RBV, ribavirin; SVR, sustained virologic response. Betty J. Dong, PharmD, FASHP, FCCP, AAHIVE: Patient education can influence adherence to HCV treatment. In this univariate analysis of adherence rates at 6 months from a French cohort of patients with genotype 2/3 HCV infection, therapeutic education for the first 3 months was associated with significantly higher adherence rates to peginterferon alfa-2b/ribavirin relative to no therapeutic education (P = .01), particularly for the ribavirin component (P = .006). Other studies have reported higher adherence to peginterferon than ribavirin.[1] In this study, 77% of patients with therapeutic education achieved SVR vs 70% of patients without therapeutic education. A multivariate analysis showed that after adjustment for various baseline factors, therapeutic education increased the probability of adherence at 6 months by approximately 58%, reflecting a significant benefit (P = .04). These findings emphasize the importance of educating patients on what to expect when they receive HCV therapies. Reference. 1. Lo Re V 3rd, Amorosa VK, Localio AR, et al. Adherence to hepatitis C virus therapy and early virologic outcomes. Clin Infect Dis. 2009;48: Cacoub P, et al. World J Gastroenterol. 2008;14:")
43
% RVS con o sin Programas de Soporte Multidisciplinar
Con Soporte Sin Soporte p Collin E et al, AASLD 2008 (mono y coinfectados) 65,7% 40,4% p=0.01 Garcia-Retortillo M et al, AASLD 2008 (monoinfectados naive) 77,1% 61,9% p=0.006
 65,7% 40,4% p=0.01. Garcia-Retortillo M et al, AASLD 2008 (monoinfectados naive) 77,1% 61,9% p=")
44
Intervención Farmacéutica Mejora la Adherencia al Tratamiento VHC
Estudio abierto prospectivo para evaluar el impacto de la intervención farmacéutica en la adherencia Tras la visita de inicio al Hepatólogo, los pacientes acudían al Servicio de Farmacia: El farmacéutico ofrecía información oral, escrita y gráfica del plan de tratamiento, administración del fármaco, importancia de la adherencia, manejo de efectos adversos, beneficios del tratamiento Se realizó una entrevista educacional en cada visita con el objetivo de motivar al paciente Se obtuvo una elevada tasa de adherencia mediante recuento de medicación 85.7% total de los pacientes (n = 50) 95.5% en el subgrupo de pacientes que consiguieron RVS EVR, early virologic response; HCV, hepatitis C virus; SVR, sustained virologic response. Betty J. Dong, PharmD, FASHP, FCCP, AAHIVE: The study shown on this slide demonstrated that pharmacist intervention can improve adherence to HCV therapy. This prospective, open-label study conducted in Spain investigated the role of pharmacists in optimizing HCV treatment adherence rates. Following the initial visit to a hepatologist for evaluation of liver disease severity, patients were directed to the pharmacy for consultation. The pharmacist provided education on the therapeutic plan, drug administration methods, the importance of adherence, the management of adverse drug effects if they occurred, and how to handle missed doses. They also discussed medication storage and dietary recommendations. Adherence was monitored at each visit by inspecting pill boxes. The pharmacist and the hepatologist alternated visits, but the pharmacist provided patient support after business hours and on holidays and weekends. The pharmacist counseled patients who achieved an EVR that they had an excellent chance of achieving an SVR, thereby providing motivation to continue therapy. This approach yielded very high adherence rates: 85.7% overall and 95.5% among patients achieving SVR. This clinic’s operation is very similar to how our clinic operates. Using this approach, we have also achieved very high adherence rates and successful SVR for all our treated patients to date, which is quite amazing. Marino EL, et al. J Manag Care Pharm. 2009;15: 44 44
 95.5% en el subgrupo de pacientes que consiguieron RVS. EVR, early virologic response; HCV, hepatitis C virus; SVR, sustained virologic response. Betty J. Dong, PharmD, FASHP, FCCP, AAHIVE: The study shown on this slide demonstrated that pharmacist intervention can improve adherence to HCV therapy. This prospective, open-label study conducted in Spain investigated the role of pharmacists in optimizing HCV treatment adherence rates. Following the initial visit to a hepatologist for evaluation of liver disease severity, patients were directed to the pharmacy for consultation. The pharmacist provided education on the therapeutic plan, drug administration methods, the importance of adherence, the management of adverse drug effects if they occurred, and how to handle missed doses. They also discussed medication storage and dietary recommendations. Adherence was monitored at each visit by inspecting pill boxes. The pharmacist and the hepatologist alternated visits, but the pharmacist provided patient support after business hours and on holidays and weekends. The pharmacist counseled patients who achieved an EVR that they had an excellent chance of achieving an SVR, thereby providing motivation to continue therapy. This approach yielded very high adherence rates: 85.7% overall and 95.5% among patients achieving SVR. This clinic’s operation is very similar to how our clinic operates. Using this approach, we have also achieved very high adherence rates and successful SVR for all our treated patients to date, which is quite amazing. Marino EL, et al. J Manag Care Pharm. 2009;15:")
45
¿Cómo afectará la aprobación de TVR y BOC a la adherencia?
Ambos fármacos se administran tres veces al día Mayor número de comprimidos Aumenta la incidencia de efectos adversos Aumenta la toma de fármacos frente a EA Posible aparición de resistencias a los Inhibidores de la Proteasa debido a la falta de adherencia BOC, boceprevir; HCV, hepatitis C virus; TVR, telaprevir. Betty J. Dong, PharmD, FASHP, FCCP, AAHIVE: How will adherence management change with the anticipated approval of telaprevir and boceprevir? Adherence will likely become more challenging as a result of the potentially increased incidence of adverse effects, 3-times-daily dosing schedules, and the higher pill burden. Dietary requirements may also be needed. In addition, treatment providers will have to update the discussion regarding the importance of adherence to include the potential for the development of resistance to the new protease inhibitors if patients do not adhere to therapy. This discussion should also include concerns regarding the potential for cross-resistance to other HCV protease inhibitors in the setting of resistance to 1 agent. For example, viral resistance to telaprevir may be associated with cross-resistance to boceprevir and vice versa. Megan R. Mahoney, MD: Assistance from the pharmacist will be essential for encouraging adherence to these new agents, particularly when considering the potential for drug resistance and the critical role of adherence in reducing the risk of resistance development. ¿DISMINUCIÓN DELA ADHERENCIA? 45

46
Calidad de Vida “Calidad de Vida” (QoL)
Percepción del individuo de su posición en la vida, en el contexto cultural y el sistema de valores en que vive, en relación con sus metas, objetivos, expectativas, valores y preocupaciones “SALUD” (WHO) Completo estado de bienestar físico, mental y social, no sólo la ausencia de enfermedad “Calidad de Vida Relacionada con la Salud” Percepción subjetiva, influenciada por el estado de salud actual, de la capacidad para realizar aquellas actividades importantes para el individuo Schumaker y Naughton HRQL, health-related quality of life; WHO, World Health Organization Quality of life emerged as a concept in the United States after World War II in an attempt to describe the effect of the acquisition of material goods on people’s lives. Around this same time, the term was also redefined by the World Health Organization (WHO); instead of defining quality of life as merely the absence of disease, the new definition also incorporated people’s perception of their own complete physical, mental, and social well‑being. The term “health‑related quality of life” includes an assessment of the effect of health on well‑being using environmental and economic features of a study population. Outcome measures may vary, but they often include patient‑reported levels of pain and emotional and psychological statuses as well as levels of functioning. 46
 Completo estado de bienestar físico, mental y social, no sólo la ausencia de enfermedad. Calidad de Vida Relacionada con la Salud Percepción subjetiva, influenciada por el estado de salud actual, de la capacidad para realizar aquellas actividades importantes para el individuo. Schumaker y Naughton. HRQL, health-related quality of life; WHO, World Health Organization. Quality of life emerged as a concept in the United States after World War II in an attempt to describe the effect of the acquisition of material goods on people’s lives. Around this same time, the term was also redefined by the World Health Organization (WHO); instead of defining quality of life as merely the absence of disease, the new definition also incorporated people’s perception of their own complete physical, mental, and social well‑being. The term health‑related quality of life includes an assessment of the effect of health on well‑being using environmental and economic features of a study population. Outcome measures may vary, but they often include patient‑reported levels of pain and emotional and psychological statuses as well as levels of functioning. 46.")
47
Percepción Subjetiva de Calidad de Vida
Cada individuo tiene un punto de vista subjetivo sobre qué mejora su calidad de vida Individuos con idénticos escenarios clínicos pueden tener distintas calidades de vida en función de sus distintas expectativas, valores, objetivos… En las Ciencias de la Salud, es indispensable aplicar la Calidad de Vida a la evaluación de las distintas intervenciones Un EA puede ser aceptable si la calidad de vida se ve significativamente mejorada La calidad de vida es una consideración a tener en cuenta para el inicio de tratamiento VHC HCV, hepatitis C virus. The perception of quality of life varies across individuals and across cultures. Every person has a unique standard of what is important to them, what has value, and what makes their particular life worthwhile. Individuals with identical clinical scenarios may report very different qualities of life based on different expectations that they may hold. With the evolution of health sciences, the need to assess and justify available interventions became evident. It became apparent that a clinical adverse event may be acceptable if the overall quality of life is improved. Therefore, quality of life was determined to be an important consideration in patient screening for initiation of hepatitis C treatment and other chronic conditions. 47

48
Factores que afectan a la Calidad de Vida
Salud física y mental Relaciones Familiares Relaciones sociales Calidad de Vida Capacidad cognitiva As depicted on this slide, many factors can affect quality of life. Although physical and mental health may be more obvious factors, living arrangements, the ability to think, religious beliefs and spirituality, cultural values, social relationships, and economic and financial circumstances have all been shown to impact a patient’s quality of life. Aspectos Culturales Creencias religiosas Circunstancias económicas 48

49
Cuestionarios de Medida de Calidad de Vida
Cuestionarios genéricos Muestran diferentes aspectos del estado de salud Permite comparar diferentes poblaciones o patologías aunque con algunas limitaciones No permite estudiar aspectos específicos de la patología Cuestionarios específicos Clínicamente sensibles Valor limitado en intervenciones poblacionales QoL, quality of life. How does one measure quality of life? Various instruments are now available for this assessment. Generic instruments can be universally applied and, with limitations, allow comparisons of different diseases or populations. However, since these generic instruments do not necessarily allow disease‑specific aspects to be studied, specific disease instruments have been developed and are more comprehensive. Several instruments can be used in the setting of hepatitis C. 49

50
Cuestionarios Genéricos
Utilizados en la práctica clínica diaria Rápidos EECC, estudios coste-efectividad, estudios epidemiológicos QoL Questionnaires Administered by Short-Form 36 (SF-36) Self Sickness Impact Profile Observer Beck Depression Inventory Hamilton Depression Rating Scale Center for Epidemiological Studies of Depression Hamilton Anxiety Scale Fatigue Severity Scale QoL, quality of life; SF-36, Short-Form 36. Generic instruments for assessing quality of life are shown on this slide. Many treaters may be familiar with the Short-Form (SF) 36, a questionnaire that can be self-administered by the patient. The other forms and questionnaires shown on this slide can be administered either by physicians, nurses, healthcare professionals, or the patient themselves. A major advantage of these questionnaires is that they are quick to administer, and many of them have now been incorporated into ongoing clinical trials. 50
 Self. Sickness Impact Profile. Observer. Beck Depression Inventory. Hamilton Depression Rating Scale. Center for Epidemiological Studies of Depression. Hamilton Anxiety Scale. Fatigue Severity Scale. QoL, quality of life; SF-36, Short-Form 36. Generic instruments for assessing quality of life are shown on this slide. Many treaters may be familiar with the Short-Form (SF) 36, a questionnaire that can be self-administered by the patient. The other forms and questionnaires shown on this slide can be administered either by physicians, nurses, healthcare professionals, or the patient themselves. A major advantage of these questionnaires is that they are quick to administer, and many of them have now been incorporated into ongoing clinical trials. 50.")
51
Cuestionario de Salud SF-36
Ofrece una perspectiva general del estado de salud de la persona Fácil y rápido de rellenar (15`) Excelente herramienta para investigación relacionada con la salud Mide 8 dimensiones Funcionalidad física Limitaciones por problemas físicos Dolor Corporal Salud general Vitalidad Funcionalidad social Limitaciones por problemas emocionales Salud Mental QoL, quality of life; SF-36, Short-Form 36. The SF‑36 is commonly used to assess quality of life. There are 8 domains within this questionnaire: physical function, role limitations due to physical health problems, bodily pain, general health, vitality, social function, role limitations due to emotional problems, and mental health. 51
 Excelente herramienta para investigación relacionada con la salud. Mide 8 dimensiones. Funcionalidad física. Limitaciones por problemas físicos. Dolor Corporal. Salud general. Vitalidad. Funcionalidad social. Limitaciones por problemas emocionales. Salud Mental. QoL, quality of life; SF-36, Short-Form 36. The SF‑36 is commonly used to assess quality of life. There are 8 domains within this questionnaire: physical function, role limitations due to physical health problems, bodily pain, general health, vitality, social function, role limitations due to emotional problems, and mental health. 51.")
52
Cuestionarios Específicos de Calidad de Vida en Enfermedad Hepática
SF-36 específico VHC Se añaden algunos items para hacer el SF-36 más específico para el VHC (1) Cuestionario de Enfermedad Hepática Crónica Cuestionario de Calidad de Vida en Enfermedad Hepática Cuestionario de Calidad de Vida en Hepatitis Cuestionario de Calidad de Vida en Enfermedad GI HCV, hepatitis C virus; QoL, quality of life; SF-36, Short-Form 36. This slide shows liver disease–specific instruments that have been developed for assessing quality of life. To make the SF‑36 questionnaire more specific to hepatitis C, it was modified slightly to include a mental component score and a physical component score. Other instruments include the Chronic Liver Disease Questionnaire, the Liver Disease Quality of Life Questionnaire, the Viral Hepatitis Quality of Life Questionnaire, and the Gastrointestinal Quality of Life Instrument. 1. Ware JE Jr, et al. Hepatology. 1999;30: 52
 Cuestionario de Enfermedad Hepática Crónica. Cuestionario de Calidad de Vida en Enfermedad Hepática. Cuestionario de Calidad de Vida en Hepatitis. Cuestionario de Calidad de Vida en Enfermedad GI. HCV, hepatitis C virus; QoL, quality of life; SF-36, Short-Form 36. This slide shows liver disease–specific instruments that have been developed for assessing quality of life. To make the SF‑36 questionnaire more specific to hepatitis C, it was modified slightly to include a mental component score and a physical component score. Other instruments include the Chronic Liver Disease Questionnaire, the Liver Disease Quality of Life Questionnaire, the Viral Hepatitis Quality of Life Questionnaire, and the Gastrointestinal Quality of Life Instrument. 1. Ware JE Jr, et al. Hepatology. 1999;30:")
53
Importancia de la Calidad de Vida para el Tratamiento de VHC
La Calidad de Vida es una importante medida dél éxito terapéutico en el tratamiento VHC VHC y su tratamiento afecta a la calidad de vida, que afecta a su vez a: Adherencia Probabilidad finalización del tratamiento RVS RVS mejora la calidad de vida HCV, hepatitis C virus; QoL, quality of life; SVR, sustained virologic response. In summary, it is important to note that quality of life is subjective, and yet it is being recognized as one of the measures of therapeutic success. We have reviewed a variety of standard measures, some of which have been customized for hepatitis C. Hepatitis C and its treatment impact quality of life, which in turn may affect adherence, treatment completion rates, and SVR. Attaining SVR has been shown to improve quality of life. 53

54
RVS + RVS: Respuesta viral sostenida CVRS: Calidad de vida relacionada con la salud HCC: Hepatitis crónica C + CVRS - - HCC Peg-INF+ RBV Diagrama de Percepción de Calidad de Vida. Younossi et al. Hepatology 2007 54

55
Cómo afecta el VHC a la Calidad de Vida
HCV, hepatitis C virus. Now, how does hepatitis C impact quality of life? 55 55

56
QoL en Pacientes Conscientes de Serostatus VHC+ vs Control
98 pacientes VHC+ ADVP a los que se le realizò SF-36 76% conscientes de serología VHC+ Pacientes VHC+ conscientes de su diagnóstico tienen peor QoL scores que aquellos no conocedores Todos los pacientes tenían peor puntuación que la población general HCV serostatus unknown HCV serostatus known P = .04 P = .01 SF-36 Scores 60 20 80 40 Physical Function Role, Physical Bodily Pain General Health Vitality Social Function Role, Emotional Mental Health 100 HCV, hepatitis C virus; QoL, quality of life; SF-36, Short-Form 36. It seems that lower quality-of-life scores are noted in patients who are aware of having hepatitis C vs those who are unaware of their serostatus. In this particular study, 98 HCV‑infected injection drug users underwent SF‑36 testing; 76% were aware of their serostatus whereas 24% were not. The results showed that those aware of their HCV infection had a worse quality of life than those who were unaware of their HCV status. As you can see from the graph where the blue bars represent patients unaware of their serostatus and the orange bars represent those aware of their HCV serostatus, the SF-36 scores were significantly lower in the physical role categories and in the general health and vitality categories when the serostatus was known. There were also insignificant differences in the other domains of bodily pain, social function, emotional role, and mental health. As expected, all subjects scored worse than the general population. Health-Related Quality of Life in Active Injecting Drug Users With and Without Chronic Hepatitis C Virus Infection, Dalgard AJ, et al. Hepatology. 2004;39:74-80 56

57
Weighted Mean Change in SF-36 Score
Calidad de Vida en Pacientes VHC+ Sin Enfermedad Hepática Significativa Revisión sistemática de 15 estudios que comparan Calidad de Vida en pacientes con VHC con Enfermedad Hepática Compensada vs controles sanos VHC disminuye QoL en ausencia de Enfermedad Hepática clínicamente significativa a través de síntomas y desórdenes extrahepáticos o disfunciones cognitivas Physical Function Role, Physical Bodily Pain General Health Social Function Role, Emotional Mental Health Vitality 5 Weighted Mean Change in SF-36 Score -7.0 -7.2 10 -9.0 -10.1 -11.9 15 -12.6 -13.0 HCV, hepatitis C virus; Pts, patients; QoL, quality of life; SF-36, Short-Form 36. This slide addresses the previous question and shows that the reduced quality of life seen in HCV-infected patients is not just a function of the liver disease because quality-of-life reductions are seen in HCV‑infected patients without significant liver disease. In this systematic review of 15 studies by Spiegel and colleagues, quality-of-life scores in patients with compensated hepatitis C were compared with healthy controls. The results showed that hepatitis C patients have greater SF‑36 score decreases than healthy controls, most significantly in the physical and emotional role categories. Based on these results, it is thought that hepatitis C may diminish quality of life in the absence of clinically significant liver disease through extrahepatic somatic symptoms such as fatigue, extrahepatic disorders such as some of the arthralgias and other associated disorders, and cognitive dysfunction. -15.8 20 25 Spiegel BMR, et al. Hepatology. 2005;41: 57

58
QoL en HCV/HIV-Pacientes coinfectados vs HIV-Monoinfectados
QoL, depresión, y fatiga: 105 HCV/HIV-coinfectados vs 379 pacientes VIH Menor QoL, mayor incidencia de depresión y fatiga en pacientes coinfectados Análisis multivariante: atribuible a factores sociodemográficos Pacientes coinfectados : sexo femenino, ADVP, desempleados, sin vivienda fija Parameter, % HCV/HIV Coinfected (n = 105) HIV Monoinfected (n = 379) P Value Female sex 18 3 < .001 Injection drug user 79 5 Unemployed 91 49 Living in unstable housing 19 1 HCV, hepatitis C virus; QoL, quality of life According to a study by Brainstein and colleagues, a worse quality of life can be seen in patients coinfected with HCV and HIV vs HIV-monoinfected patients. This study showed that quality of life was worse among 105 coinfected patients vs 379 monoinfected patients. This lower quality of life was mainly explained by a higher incidence of depression and fatigue in coinfected patients, although sociodemographic factors likely also played a role. Indeed, coinfected patients were more likely to be female, injection drug users, homeless, and unemployed. Braitstein P, et al. AIDS Care. 2005;17: 58
 HIV Monoinfected (n = 379) P Value. Female sex < Injection drug user Unemployed Living in unstable housing HCV, hepatitis C virus; QoL, quality of life. According to a study by Brainstein and colleagues, a worse quality of life can be seen in patients coinfected with HCV and HIV vs HIV-monoinfected patients. This study showed that quality of life was worse among 105 coinfected patients vs 379 monoinfected patients. This lower quality of life was mainly explained by a higher incidence of depression and fatigue in coinfected patients, although sociodemographic factors likely also played a role. Indeed, coinfected patients were more likely to be female, injection drug users, homeless, and unemployed. Braitstein P, et al. AIDS Care. 2005;17:")
59
QoL Pacientes VHC+ vs Pacientes VHB+ en tratamiento con PegIFN alfa-2a
Datos obtenidos de 5 estudios de monoterapia con pegIFN alfa-2a en VHC comparada con 2 estudios en infección crónica VHB Menor incidencia de efectos adversos relacionados con IFN y de depresión en pacientes VHB Mayores reducciones de QoL medidas mediante SF-36 en pacientes VHC vs VHB Las puntuaciones volvieron a los valores basales después de 24 semanas de seguimiento en ambos grupos AE, adverse events; BL, baseline; HBV, hepatitis B virus; HCV, hepatitis C virus; IFN, interferon; PegIFN, peginterferon; Pts, patients; QoL, quality of life; SF-36, Short-Form 36. This slide shows that greater quality-of-life reductions are noted in hepatitis C vs hepatitis B patients receiving therapy. In a pooled analysis of 5 studies looking at peginterferon alfa‑2a monotherapy in hepatitis C and 2 studies in chronic hepatitis B, the authors found a lower incidence of interferon‑related adverse events and a significantly lower incidence of depression in hepatitis B patients. Greater quality-of-life reductions, as assessed with the SF‑36 questionnaire, were noted in the hepatitis C patients and reached statistical significance in the physical component score. Mean Reductions in On-Treatment SF-36 Composite Scores From BL to Wk 48 HBV (n = 448) HCV (n = 791) P Value Physical component score -1.1 -2.5 < .001 Mental component score -1.7 -2.4 NS Marcellin P, et al. Liver International. 2008;28: 59
 HCV (n = 791) P Value. Physical component score < Mental component score NS. Marcellin P, et al. Liver International. 2008;28:")
60
Cómo afecta el tratamiento VHC a la Calidad de Vida
HCV, hepatitis C virus. Now, we will discuss quality of life and hepatitis C patient management. 60 60

61
Calidad de Vida con IFN + RBV vs PegIFN
Estudio abierto en 412 pacientes VHC+ randomizados a recibir tratamiento pegIFN alfa-2a sin RBV vs IFN alfa-2b + RBV Standard IFN alfa-2b + RBV PegIFN alfa-2a Mental Component Score Physical Component Score Week 4 Week 12 Week 4 Week 12 2 HCV, hepatitis C virus; IFN, interferon; PegIFN, peginterferon; Pts, patients; QoL, quality of life; RBV, ribavirin; SF-36, Short-Form 36. In this trial that we mentioned earlier by Perrillo and colleagues, 412 patients with HCV were randomized to either peginterferon alfa‑2a without ribavirin (orange bars) or interferon alfa‑2b plus ribavirin (blue bars). As you can see from the graph, treatment with standard interferon and ribavirin was associated with a worse quality of life vs peginterferon alone. Indeed, a statistically significant difference in the mental and physical component scores of the SF-36 at both Weeks 4 and 12 can be seen between the 2 arms of the study. Although the arms are not completely comparable because ribavirin was used with standard interferon alfa but not with peginterferon, this slide is added to demonstrate how the evolution of therapy has impacted quality of life. -1.5 2 -2.4 Change in SF-36 Score From Baseline Change in SF-36 Score From Baseline -3.1 4 4 -3.5 -3.9 -5.1 6 6 -5.9 P ≤ .01 -6.2 P ≤ .05 8 8 P ≤ .05 P ≤ .01 10 10 Comparison of quality of life, work productivity and medical resource utilization of peginterferon alpha 2a vs the combination of interferon alpha 2b plus ribavirin as initial treatment in patients with chronic hepatitis C, Perrillo R, et al. J Viral Hepat. 2004;11: 61
 or interferon alfa‑2b plus ribavirin (blue bars). As you can see from the graph, treatment with standard interferon and ribavirin was associated with a worse quality of life vs peginterferon alone. Indeed, a statistically significant difference in the mental and physical component scores of the SF-36 at both Weeks 4 and 12 can be seen between the 2 arms of the study. Although the arms are not completely comparable because ribavirin was used with standard interferon alfa but not with peginterferon, this slide is added to demonstrate how the evolution of therapy has impacted quality of life Change in SF-36 Score From Baseline. Change in SF-36 Score From Baseline P ≤ P ≤ P ≤ .05. P ≤ Comparison of quality of life, work productivity and medical resource utilization of peginterferon alpha 2a vs the combination of interferon alpha 2b plus ribavirin as initial treatment in patients with chronic hepatitis C, Perrillo R, et al. J Viral Hepat. 2004;11:")
62
Aumento de Calidad de Vida en Pacientes post-Tratamiento VHC
Estudio abierto 412 pacientes VHC+ randomizados a recibir tratamiento con pegIFN alfa-2a vs IFN alfa-2b + RBV PF BP VT RE RP GH SF MH Standard IFN alfa + RBV PegIFN alfa-2a Treatment Posttreatment Treatment Posttreatment 90 90 SF-36 Domain Score 60 SF-36 Domain Score 60 BP, bodily pain; GH, general healthy; IFN, interferon; HCV, hepatitis C virus; MH, mental health; PegIFN, peginterferon; PF, physical function; QoL, quality of life; RBV, ribavirin; RE, role emotional; RP, role physical; SF, social function; VT, vitality. This slide shows how quality-of-life scores decline in patients receiving HCV therapy. In this study by Perrillo and colleagues, 412 patients with hepatitis C were randomized to open‑label treatment with peginterferon alfa‑2a vs interferon alfa‑2b plus ribavirin. One can see from these graphs that all SF‑36 domains decreased while on treatment, although the declines were less in the peginterferon alfa‑2a without ribavirin arm. I do not think it is necessary to belabor this point to all the people in the audience who have treated hepatitis C, as we have all probably noted these declines in our practices. 30 30 BL 4 12 24 48 60 72 BL 4 12 24 48 60 72 Week Week Comparison of quality of life, work productivity and medical resource utilization of peginterferon alpha 2a vs the combination of interferon alpha 2b plus ribavirin as initial treatment in patients with chronic hepatitis C, Perrillo R, et al. J Viral Hepat. 2004;11: 62

63
Calidad de Vida y Productividad: RVS vs No Respondedores
Estudio 235 pacientes práctica clínica tras finalizar el tto (3,7 años) Cuestionarios: SF-36 , HQLQ, TTO, HUI2/3 Días de ausencia del trabajo, tareas domésticas últimos 3 meses SF-36 NR RVS p Función física 68 80.7 P<0.001 Rol físico 58.3 75.6 Dolor Corporal 56.9 72 P<0.0001 Salud general 45.5 64.7 Vitalidad 42.3 55 Función social 60.5 74.4 Rol emocional 63.6 77.5 Salud Mental 62.3 71.6 Componente físico 42.5 49.2 Componente Mental 40.5 46.1 P<0.01 SF-36 NR RVS p Limitaciones específicas de la Hepatitis 61.3 85 P<0.0001 Problemas de salud específicos de la Hepatitis 59.3 82.8 Productividad: 44% NR vs 9% VRS p<0.001 El incremento en la Calidad de Vida en los Respondedores se mantiene en el tiempo. Ava A. John_Baptiste et al. Am J Gastroenterol 2009;104:
 Cuestionarios: SF-36 , HQLQ, TTO, HUI2/3. Días de ausencia del trabajo, tareas domésticas últimos 3 meses. SF-36. NR. RVS. p. Función física P< Rol físico Dolor Corporal P< Salud general Vitalidad Función social Rol emocional Salud Mental Componente físico Componente Mental P<0.01. SF-36. NR. RVS. p. Limitaciones específicas de la Hepatitis P< Problemas de salud específicos de la Hepatitis Productividad: 44% NR vs 9% VRS p< El incremento en la Calidad de Vida en los Respondedores se mantiene en el tiempo. Ava A. John_Baptiste et al. Am J Gastroenterol 2009;104:")
64
Calidad de Vida: RVS vs Pacientes no Tratados y No Respondedores
912 pacientes randomizados a recibir IFN alfa-2b + RBV 24 o 48 semanas o placebo Se midió la calidad de vida (SF-36 mod) y la productividad laboral (días perdidos), antes, durante y tras el tratamiento En el periodo basal, todos los pacientes puntuaron menos que la población general en 5/8 dimensiones Al final del seguimiento, los pacientes que consiguieron RVS puntuaron de forma similar en todos las dimensiones que la población general Excepto dimensión Salud General (P < .05) La calidad de vida no mejoró en los no respondedores ni en los no tratados BL, baseline; HCV, hepatitis C virus; IFN, interferon; Pts, patients; QoL, quality of life; RBV, ribavirin; SVR, sustained virologic response. A study by McHutchinson and colleagues showed that hepatitis C patients achieving SVR experience an improved quality of life vs untreated patients. In this study, 912 patients were randomized to interferon alfa‑2b plus ribavirin for 24 or 48 weeks or to placebo. Quality-of-life scores were analyzed from the subset of patients who achieved SVR (n = 184). At baseline, patients scored lower in 5 of 8 categories vs the general population, but at the end of follow‑up, the patients achieving SVR scored similarly in almost all categories vs the general population. Their general health domain unfortunately remained lower. McHutchison JG, et al. J Hepatology. 2001;34: 64
 y la productividad laboral (días perdidos), antes, durante y tras el tratamiento. En el periodo basal, todos los pacientes puntuaron menos que la población general en 5/8 dimensiones. Al final del seguimiento, los pacientes que consiguieron RVS puntuaron de forma similar en todos las dimensiones que la población general. Excepto dimensión Salud General (P < .05) La calidad de vida no mejoró en los no respondedores ni en los no tratados. BL, baseline; HCV, hepatitis C virus; IFN, interferon; Pts, patients; QoL, quality of life; RBV, ribavirin; SVR, sustained virologic response. A study by McHutchinson and colleagues showed that hepatitis C patients achieving SVR experience an improved quality of life vs untreated patients. In this study, 912 patients were randomized to interferon alfa‑2b plus ribavirin for 24 or 48 weeks or to placebo. Quality-of-life scores were analyzed from the subset of patients who achieved SVR (n = 184). At baseline, patients scored lower in 5 of 8 categories vs the general population, but at the end of follow‑up, the patients achieving SVR scored similarly in almost all categories vs the general population. Their general health domain unfortunately remained lower. McHutchison JG, et al. J Hepatology. 2001;34:")
65
Calidad de Vida:No Respondedores vs No Tratados y Recidivantes
Estudio Italiano para determinar si el resultado del tratamiento afecta a QoL 264 pts: 163 No tratados, 43 recidivantes, 58 No Respondedores a estándar IFN SF-36, Cuestionario de Enfermedad Hepática Crónica, y WHO QoL Todos los pacientes mostraron menor QoL comparados con los controles sanos No Respondedores tuvieron menor QoL vs No tratados y recidivantes Posiblemente debido a desmotivación y miedo a la progresión de la enfermedad Los pacientes No tratados y los Recidivantes tuvieron niveles comparables de Calidad de Vida HCV, hepatitis C virus; Pts, patients; QoL, quality of life; WHO, World Health Organization. This slide shows that nonresponders to HCV treatment have a worse quality of life vs untreated patients and relapsers. In this Italian study conducted to determine if the treatment history affected quality of life in hepatitis C–infected patients, 264 patients were interviewed; 163 were treatment naive, 43 were relapsers, and 58 were nonresponders to standard interferon. Several instruments were used to assess quality of life, including the SF‑36 questionnaire, the Chronic Liver Disease Questionnaire, and the WHO Quality of Life Assessment. Not surprisingly, all patients displayed lower quality of life compared with healthy controls, but nonresponders were shown to have a poorer quality of life vs untreated patients and relapsers. Their concomitant physical comorbidity probably worsened their quality of life. Notably, untreated patients and relapsers had comparable levels of quality of life. Taliani GJ, et al. J Viral Hepat. 2007;14: 65

66
VHC, Trasplante Hepático y QoL
La evidencia científica sugiere que QoL mejora tras trasplante ortotópico de hígado[1-2] Aunque mejora el componente físico de la enfermedad, el componente emocional se ve comprometido[3] Pacientes experimentan mayores episodios de ansiedad y depresión Puede afectar al cumplimiento del tratamiento postransplante Los pacientes VHC+ sometidos a trasplante hepático tienen peor calidad de vida que aquellos sometidos a otro tipo de trasplantes[4] Debido posiblemente a una pobre funcionalidad física, mayores tasas de depresión y elevada incidencia de fatiga HCV, hepatitis C virus; QoL, quality of life. Liver transplantation is another arena where quality of life can have an impact. The published literature would suggest that quality of life improves after liver transplantation. Despite improved physical health, however, the psychological well‑being of patients may remain compromised, which may in turn impact treatment compliance posttransplantation. Indeed, these patients generally experience more anxiety and depression. In addition, worse quality-of-life outcomes in hepatitis C–infected patients undergoing liver transplantation are noted vs other transplantation recipients, possibly because of recurrent disease, poorer physical functioning, higher rates of depression, and greater fatigue. 1. De Bona M, et al. J Hepatol. 2000;33: Levy MF, et al. Transplantation. 1995;59: Nickel R, et al. Liver Transplantation. 2002;8: Bravata DM, et al. Liver Transplantation Surgery. 1999;5: 66

67
Relación entre Calidad de Vida y Adherencia Tratamiento
Estudio multicéntrico, randomizado y abierto que compara eficacia y seguridad de pegIFN alfa-2a vs IFN alfa-2a en 1441 pacientes VHC+ 141 (10%) de pacientes discontinuaron el tratamiento La Disminución en Calidad de Vida es predictora de la Disminución de Adherencia al tratamiento Predictor of Tx Discontinuation Odds Ratio (95% CI) P Value CI, confidence interval; HCV, hepatitis C virus; IFN, interferon; PegIFN, peginterferon; QoL, quality of life; SF-36, Short-Form 36; Tx, treatment. To help illustrate this, we will review the results of a trial conducted by Bernstein and colleagues. In this multicenter, open‑label, randomized trial looking at the efficacy of peginterferon alfa‑2a vs interferon alfa‑2a in 1441 patients with hepatitis C, quality-of-life scores were significantly associated with treatment adherence. Indeed, predictors of premature discontinuation were greater physical and mental component declines on the SF‑36 questionnaire. As you can see, the odds ratio for discontinuation increased by nearly one third in patients displaying declines in either the physical or mental component scores, and these differences were statistically significant. Caída de escala SF-36 physical component 1.35 < .001 Caída de escala SF-36 mental component 1.28 < .001 0.1 1.0 2.0 Bernstein D, et al. Hepatology. 2002;35: 67
 de pacientes discontinuaron el tratamiento. La Disminución en Calidad de Vida es predictora de la Disminución de Adherencia al tratamiento. Predictor of Tx Discontinuation. Odds Ratio (95% CI) P Value. CI, confidence interval; HCV, hepatitis C virus; IFN, interferon; PegIFN, peginterferon; QoL, quality of life; SF-36, Short-Form 36; Tx, treatment. To help illustrate this, we will review the results of a trial conducted by Bernstein and colleagues. In this multicenter, open‑label, randomized trial looking at the efficacy of peginterferon alfa‑2a vs interferon alfa‑2a in 1441 patients with hepatitis C, quality-of-life scores were significantly associated with treatment adherence. Indeed, predictors of premature discontinuation were greater physical and mental component declines on the SF‑36 questionnaire. As you can see, the odds ratio for discontinuation increased by nearly one third in patients displaying declines in either the physical or mental component scores, and these differences were statistically significant. Caída de escala SF-36 physical component < Caída de escala SF-36 mental component < Bernstein D, et al. Hepatology. 2002;35:")
68
QoL y Adherencia mejoran al disminuir la complejidad del tratamiento
Se evaluó Calidad de vida, adherencia, y preferencias del paciente : Pacientes pretradados con RBV estándar, utilizando kit comprimidos RBV Pacientes naive que cambiaron de RBV estándar a kit comprimidos RBV en la semana 12 Adherencia: Pretratados: 27 pacientes olvidaron tomar los comprimidos de RBV estándar vs 3 pacientes con kit deRBV Naïve: 11 pacientes olvidaron tomar los comprimidos de RBV estándar vs ningún paciente en el grupo con kit RBV Exp, experienced; QoL, quality of life; RBV, ribavirin; Pts, patients; SVR, sustained virologic response; Tx, treatment. This slide shows that quality-of-life scores and adherence are improved when pill burden is reduced. Data has shown that fewer higher dose ribavirin tablets (400 or 600 mg) are required vs standard ribavirin (200 mg). In this recent article by Palmer and colleagues, quality-of-life scores, adherence, and regimen preference were assessed in treatment‑experienced patients receiving higher dose ribavirin vs previous ribavirin treatment and in treatment‑naive patients who switched from standard to higher dose ribavirin at Week 12. Twenty‑seven patients missed pills in the treatment‑experienced group receiving standard ribavirin vs only 3 receiving the higher dose of ribavirin. Eleven patients missed pills in the treatment‑naive group receiving standard ribavirin vs 0 in the treatment‑naive group receiving the higher dose of ribavirin, speaking to the impact of reducing the pill burden. As you can see in the orange bars on the right, patients clearly preferred the higher-dose ribavirin. Improved QoL Scores With Higher-Dose RBV Drug Preference With Higher-Dose RBV 63.6 75.5 20 40 60 80 100 Tx Exp Tx Naive Patients (%) 14 37 n = 68.2 81.6 15 Palmer M, et al. Pract Gastroenterol. 2008;32:31-42. 68
 are required vs standard ribavirin (200 mg). In this recent article by Palmer and colleagues, quality-of-life scores, adherence, and regimen preference were assessed in treatment‑experienced patients receiving higher dose ribavirin vs previous ribavirin treatment and in treatment‑naive patients who switched from standard to higher dose ribavirin at Week 12. Twenty‑seven patients missed pills in the treatment‑experienced group receiving standard ribavirin vs only 3 receiving the higher dose of ribavirin. Eleven patients missed pills in the treatment‑naive group receiving standard ribavirin vs 0 in the treatment‑naive group receiving the higher dose of ribavirin, speaking to the impact of reducing the pill burden. As you can see in the orange bars on the right, patients clearly preferred the higher-dose ribavirin. Improved QoL Scores With Higher-Dose RBV. Drug Preference With Higher-Dose RBV Tx Exp. Tx Naive. Patients (%) n = Palmer M, et al. Pract Gastroenterol. 2008;32:")
69
Estrategias para simplificar la complejidad del tratamiento
Es posible mejorar la Adherencia, la Calidad de Vida y la Satisfacción del paciente mediante simplificación de la terapia y control de la misma Reducción del número de comprimidos/inyecciones[1,2] Envases que favorezcan el cumplimiento y sistemas dispensadores[1,3,4] Terapia directamente observada para pacientes con baja adherencia al tratamiento[5,6] As mentioned, strategies to simplify the treatment complexity can help maintain adherence. The reduction of pill and injection burden is something that we will see more of in the future. There are various formulations now available to diminish the number of ribavirin capsules that a patient has to take, and methods of reducing the frequency of interferon injections are being investigated. In addition, some of you may be familiar with compliance packaging and dispensing systems that are being studied in clinical trials. Finally, although it is difficult in hepatitis C, directly observed therapy (for interferon in particular) may become necessary for difficult-to-treat patients, such as prisoners. 1. Palmer M, et al. Pract Gastroenterol. 2008;32: Pianko S, et al. DDW Abstract S Janisch HD et al. AASLD Abstract Dzyublyk I, et al. AASLD Abstract LB Flanigan TP, et al. Clin Infect Dis. 2005;40(suppl 5):S346-S Grebely, J, et al. J Gastro Hepatol. 2007;22: 69 69
 may become necessary for difficult-to-treat patients, such as prisoners. 1. Palmer M, et al. Pract Gastroenterol. 2008;32: Pianko S, et al. DDW Abstract S Janisch HD et al. AASLD Abstract Dzyublyk I, et al. AASLD Abstract LB Flanigan TP, et al. Clin Infect Dis. 2005;40(suppl 5):S346-S Grebely, J, et al. J Gastro Hepatol. 2007;22:")
70
Satisfacción SATISFACCIÓN DEL PACIENTE
Medida del resultado de la interacción entre el profesional de la salud y el paciente (Koos y Donabedian) Concepto complejo, multidimensional y subjetivo El fracaso en la identificación de las preocupaciones principales del paciente lleva a una menor adherencia al tratamiento Tener en cuenta inquietudes y afectos: PREFERENCIAS Interacciones sociales: relación PROFESIONAL DE LA SALUD-PACIENTE
 Concepto complejo, multidimensional y subjetivo. El fracaso en la identificación de las preocupaciones principales del paciente lleva a una menor adherencia al tratamiento. Tener en cuenta inquietudes y afectos: PREFERENCIAS. Interacciones sociales: relación PROFESIONAL DE LA SALUD-PACIENTE.")
71
Motivos de Insatisfacción entre los Pacientes
Diagnóstico y Tratamiento Problemas en el diagnóstico Problemas con el tratamiento Aparición Efectos adversos Demoras de las pruebas diagnósticas Altas prematuras Sensación de no progreso Comunicación Profesional de la Salud-Paciente Inadecuada información o ausencia de la misma Informaciones incongruentes por parte de distintos profesionales No respeto a la confidencialidad o intimidad del paciente Relación Profesional de la Salud- Paciente Falta de cortesía-trato rudo Percepción de maltrato por parte del paciente Accesibilidad y Disponibilidad Dificultades de accesibilidad al profesional Cambios injustificados de cita No atención a necesidades del paciente No mantener la continuidad asistencial Pitcherd et Al.Journal of Quality improvement 1998;24:

72
Relación Profesional de la Salud- Paciente
Interacción que se establece entre el profesional de la salud y el paciente durante la enfermedad. Esta relación influye en el curso de la enfermedad y en la eficacia del tratamiento Satisfacción Adherencia Eficacia Va a estar influenciada por las Motivaciones tanto del Profesional de la Salud como del Paciente Habilidades de Comunicación

73
¿Cómo perciben los pacientes con VHC crónica al personal sanitario?
Estudio realizado en EEUU con 332 pacientes 41% refirió dificultades de comunicación 28% observó que su médico tenía pocas habilidades de comunicación 16 % se sintió ignorado o incomprendido 23% refirió percibir incompetencia en el manejo de su enfermedad. 9% se sintió estigmatizado por su médico Zickmund S, et al Hepatitis C virus-infected patients report communication problems with physicians. Hepatology 2004; 39: 73

74
Preferencias del Paciente y su Impacto en la Adherencia
Determinar las preferencias de los pacientes en las características del tratamiento de la Hepatitis C Evaluar la valoración de los pacientes de la importancia de las distintas características en la adherencia al tratamiento Flu Mean Lower Upper Days Bound Bound Importancia Relativa Adherencia Relativa en función de los días de sintomas gripales Eficacia Depresión Flu days Días trabajo perd Alopecia Dispositivo Brett et al. Patient preferences and assesment of likely adherencie to hepatitis C virus treatment. Journal of Viral Hepatitis. 2010

75
Preferencias del Paciente en el Tratamiento de la Hepatitis C
El objetivo del estudio fue determinar las preferencias de los pacientes en relación al tratamiento de la Hepatitis C Subjects preferring treatment n=72 Subjects non preferring treatment n=68 Characteristic P value Age (23–64) (26–70) HCV-related quality of life 28 (0–77) (0–84) Expectation of cirrhosis (0–100) (0–100) <0.0004 Social support (5–100) (12–100) Trust in physician (36–68) (34–68) Decisional conflict (0–58) (0–73) Fraenkel et al. Med Decis Making ; 30(1): 45–57.
 53 (26–70) 0.1. HCV-related quality of life 28 (0–77) 14 (0–84) Expectation of cirrhosis 50 (0–100) 33 (0–100) < Social support 62 (5–100) 63 (12–100) 0.7. Trust in physician 57 (36–68) 55 (34–68) 0.2. Decisional conflict 25 (0–58) 34 (0–73) Fraenkel et al. Med Decis Making ; 30(1): 45–57.")
76
Impacto Relativo de las características del tratamiento en las preferencias de los pacientes
Pacientes con Fibrosis Severa dan mayor importancia al esperado beneficio del tratamiento y menos al riesgo de toxicidad comparado con los pacientes sin fibrosis Relative Impact** Characteristic Mild/No Fibrosis Moderate Fibrosis Severe Fibrosis Benefit ± ± 25* ± 16* Monitor ± ± ± 7 Flu ± ± 11* ± 7* Fatigue ± ± 10* ± 7* Depression ± ± ± 8* * p<0.05 compared to Mild/None (least square means adjusted for multiple comparisons using Tukey’s procedure). ** The relative impact reflect the impact that each characteristic has on subjects’ preferences. The values are proportions that sum to 100. Fraenkel et al. Med Decis Making ; 30(1): 45–57.
. ** The relative impact reflect the impact that each characteristic has on subjects’ preferences. The values are proportions that sum to 100. Fraenkel et al. Med Decis Making ; 30(1): 45–57.")
77
CALIDAD DE VIDA PACIENTE HEPATITIS C ADHERENCIA SATISFACCIÓN

78
MUCHAS GRACIAS

Presentaciones similares
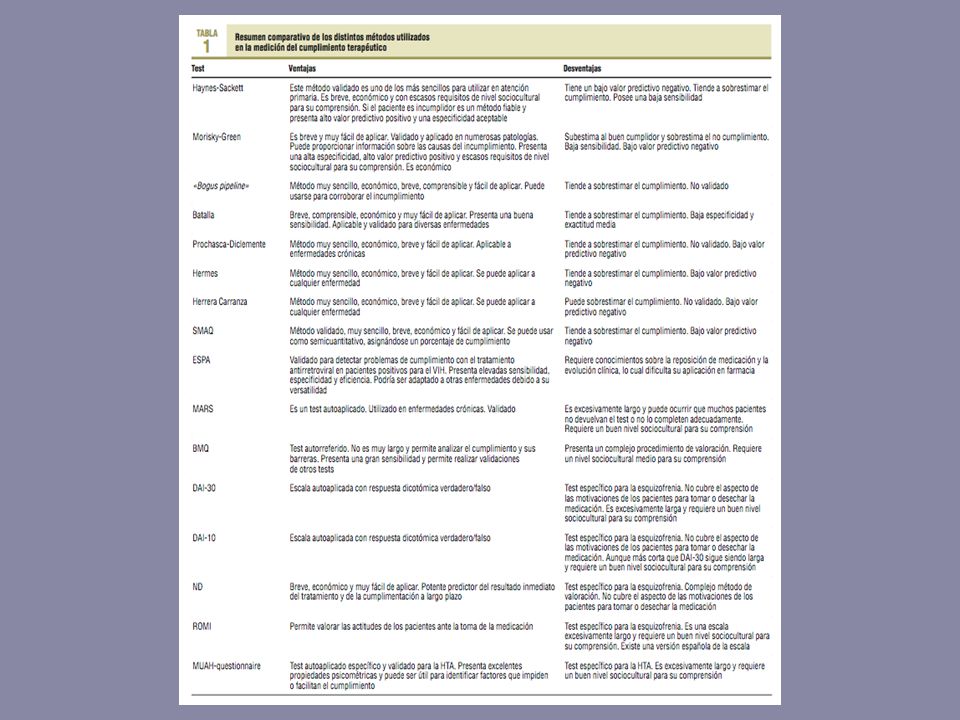
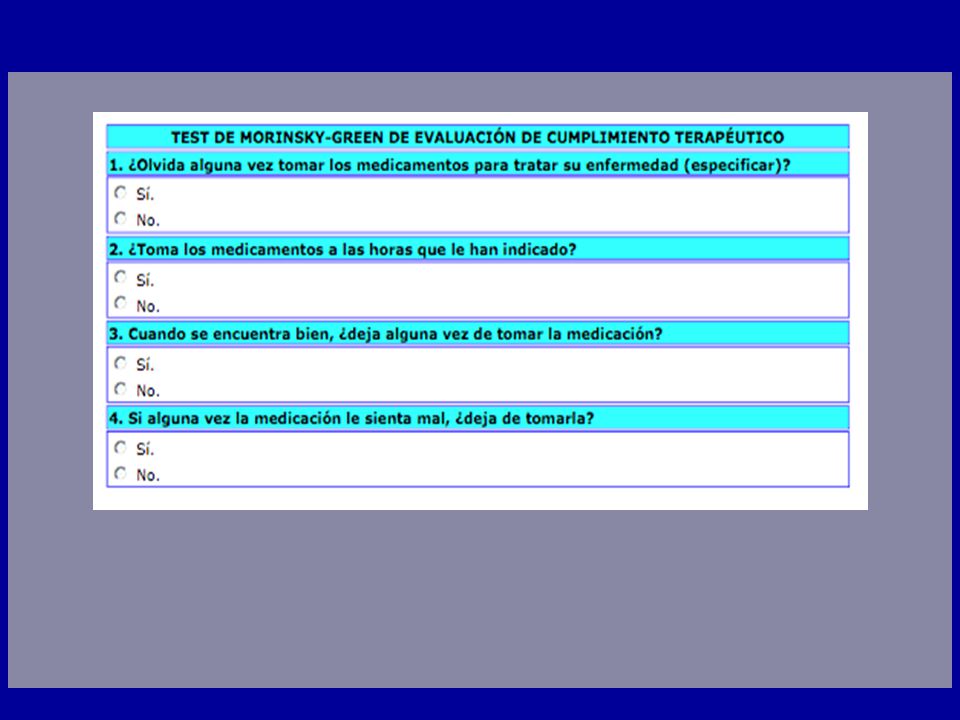
















>")


