Descargar la presentación
La descarga está en progreso. Por favor, espere

2
Prognosis of Untreated Patients with Idiopathic Membranous Nephropathy Arrigo Schieppati, Lidia Mosconi, Annalisa Perna, Giuliano Mecca, Tullio Bertani, Silvio Garattini, and Giuseppe Remuzzi Volume 329:85-89 July 8, 1993Number 2

3
Probability of Adequate Renal Function in Untreated Patients with Idiopathic Membranous Nephropathy

4
Changes in the Clinical Status of Patients with Idiopathic Membranous Nephropathy.

5
Prognosis of Untreated Patients with Idiopathic Membranous Nephropathy Probability of Five-Year Kidney Survival According to the Degree of Proteinuria at Base Line..

6
Prognosis of Untreated Patients with Idiopathic Membranous Nephropathy Base-Line Clinical and Laboratory Data for 100 Patients with Idiopathic Membranous Nephropathy.

8
PONTICELLI TRIAL RESULTS: 10 YEAR RENAL SURVIVAL

9
PONTICELLI TRIAL RESULTS: PERCENT ACHIEVING REMISSION

14
TRATAMIENTO INMUNOSUPRESOR PARA LA NEFROPATÍA MEMBRANOSA IDIOPÁTICA EN ADULTOS CON SÍNDROME NEFRÓTICO (REVISIÓN COCHRANE TRADUCIDA) SCHIEPPATI A, PERNA A, ZAMORA J, GIULIANO GA, BRAUN N, REMUZZI G La nefropatía membranosa idiopática (NMI) es la forma más común de síndrome nefrótico en los adultos. La enfermedad tiene un curso benigno o indolente en la mayoría de los pacientes, con una alta tasa de remisión espontánea completa o parcial del síndrome nefrótico, del 30% o superior. A pesar de esto, del 30% al 40% de los pacientes progresan hacia la insuficiencia renal terminal (IRT) en el lapso de cinco a 15 años.
 en el lapso de cinco a 15 años..")
15
TRATAMIENTO INMUNOSUPRESOR PARA LA NEFROPATÍA MEMBRANOSA IDIOPÁTICA EN ADULTOS CON SÍNDROME NEFRÓTICO (REVISIÓN COCHRANE TRADUCIDA) Objetivos: Evaluar los beneficios y los daños del tratamiento inmunosupresor para la NMI en los adultos. Estrategia de búsqueda: Se realizaron búsquedas en el Registro Especializado del Grupo Cochrane de Riñón (Cochrane Renal Group) (diciembre de 2003), el Registro Cochrane Central de Ensayos Controlados (CENTRAL) (The Cochrane Central Register of Controlled Trials (CENTRAL)) (la Cochrane Library Número 4, 2003), MEDLINE y Pre- MEDLINE (1966 a diciembre de 2003), EMBASE (1980 a diciembre de 2003), las listas de referencias de los libros de texto de nefrología, artículos de revisión, registros de ensayos prospectivos, ensayos pertinentes y resúmenes de las reuniones científicas de nefrología y la Internet, sin restricción de idiomas. Se estableció contacto con los investigadores principales de los estudios controlados.
 (diciembre de 2003), el Registro Cochrane Central de Ensayos Controlados (CENTRAL) (The Cochrane Central Register of Controlled Trials (CENTRAL)) (la Cochrane Library Número 4, 2003), MEDLINE y Pre- MEDLINE (1966 a diciembre de 2003), EMBASE (1980 a diciembre de 2003), las listas de referencias de los libros de texto de nefrología, artículos de revisión, registros de ensayos prospectivos, ensayos pertinentes y resúmenes de las reuniones científicas de nefrología y la Internet, sin restricción de idiomas. Se estableció contacto con los investigadores principales de los estudios controlados..")
16
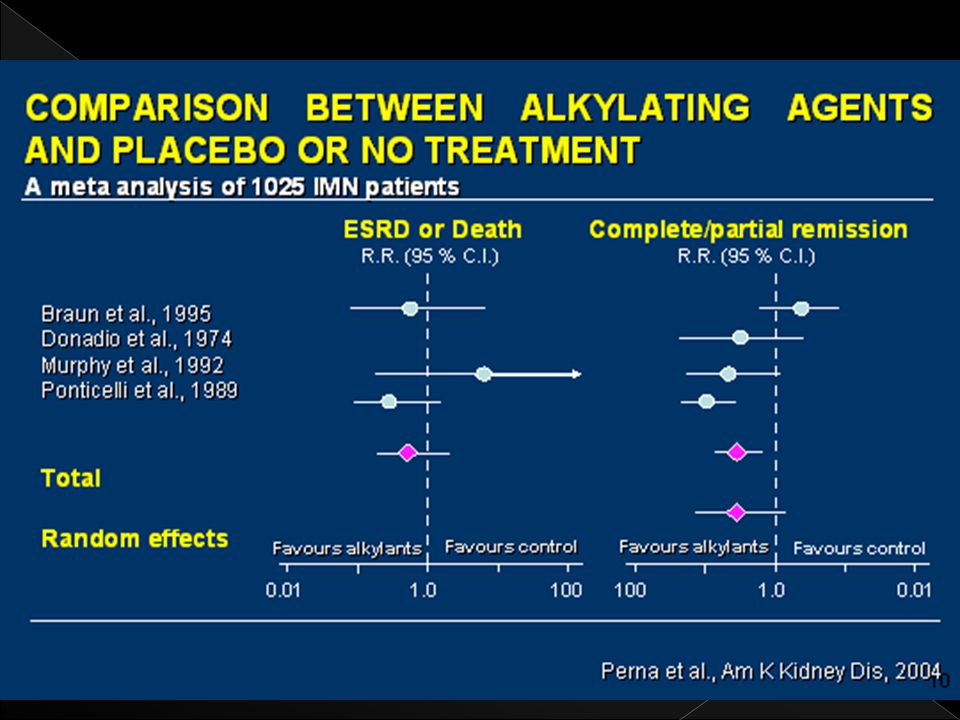
TRATAMIENTO INMUNOSUPRESOR PARA LA NEFROPATÍA MEMBRANOSA IDIOPÁTICA EN ADULTOS CON SÍNDROME NEFRÓTICO (REVISIÓN COCHRANE TRADUCIDA) Resultados principales: Se incluyó un total de 18 ensayos, con 1025 pacientes. No se encontraron diferencias cuando se combinaron los datos de todas las categorías de tratamiento como un grupo y se compararon con placebo o ningún tratamiento. Glucocorticosteroides orales: no se observaron efectos beneficiosos sobre las variables principales elegidas para evaluar la eficacia. Los agentes alquilantes mostraron un efecto beneficioso significativo sobre la remisión completa (RR 2,37; IC del 95%: 1,32 a 4,25; P=0,004) pero no sobre la remisión parcial (RR 1,22; IC del 95%: 0,63 a 2,35; P=0,56) o la remisión completa o parcial (RR 1,55; IC del 95%: 0,72 a 3,34; P=0,27). El tratamiento con ciclofosfamida resultó en una tasa significativamente inferior de interrupciones debidas a eventos adversos en comparación con el clorambucil (RR 2,34; IC del 95%: 1,25 a 4,39; P=0,008). No hubo pruebas de diferencias clínicamente pertinentes a favor de la ciclosporina y no hubo datos suficientes sobre los agentes antiproliferativos
 pero no sobre la remisión parcial (RR 1,22; IC del 95%: 0,63 a 2,35; P=0,56) o la remisión completa o parcial (RR 1,55; IC del 95%: 0,72 a 3,34; P=0,27). El tratamiento con ciclofosfamida resultó en una tasa significativamente inferior de interrupciones debidas a eventos adversos en comparación con el clorambucil (RR 2,34; IC del 95%: 1,25 a 4,39; P=0,008). No hubo pruebas de diferencias clínicamente pertinentes a favor de la ciclosporina y no hubo datos suficientes sobre los agentes antiproliferativos.")
17
TRATAMIENTO INMUNOSUPRESOR PARA LA NEFROPATÍA MEMBRANOSA IDIOPÁTICA EN ADULTOS CON SÍNDROME NEFRÓTICO (REVISIÓN COCHRANE TRADUCIDA) Conclusiones: Esta revisión no logró mostrar efectos a largo plazo del tratamiento inmunosupresor sobre la supervivencia de los pacientes o la supervivencia renal. Hubo un mayor número de interrupciones debidas a eventos adversos en los grupos con tratamiento inmunosupresor. Dentro de la clase de agentes alquilantes no hay pruebas sólidas que apoyen la eficacia de la ciclofosfamida en comparación con el clorambucil. Por otro lado, la ciclofosfamida presentó menos efectos secundarios que resultaban en el retiro del paciente en comparación con el clorambucil.

19
BAJO RIESGO PROTEINURIA < 4g/DIA FUNCION RENAL NORMAL RIESGO MODERADO PROTEINURIA 4 – 8 g/DIA FUNCION RENAL NORMAL BAJO RIESGO PROTEINURIA > 8g/DIA FUNCION RENAL ALTERADA RESTRICCION PROTEINAS DIETA IECA O ARA POR HTA O PROTEINURIA ESTATINAS SI DISLIPIDEMIA RESTRICCION PROTEINAS DIETA IECA O ARA POR HTA O PROTEINURIA ESTATINAS SI DISLIPIDEMIA CONTROL EN 6 MESES RESTRICCION PROTEINAS DIETA IECA O ARA POR HTA O PROTEINURIA ESTATINAS SI DISLIPIDEMIA CORTICOIDES + AGENTES CITOTOXICOS PROTEINURIA DE RANGO NEFROTICO PERSISTENTE + PRESENCIA DE FACTORES DE POBRE PRONOSTICO ESTEROIDES ALTERNANDO CON DROGAS CITOTOXICAS FUNCION RENAL DETERIORADA PROTEINURIA DE RANGO NEFROTICO PERSISTENTE DETERIORO FUNCION RENAL CsAMMFFK506

20
LES DROGAS: aines, sales oro, penicilamina, captopril INFECCIONES: Hep B, C, HIV, otras, Exposiciones crónicas solventes. CANCER: pulmón, colon, estomago, riñón, próstata, ovario, vejiga, linfoma, otros. LES DROGAS: aines, sales oro, penicilamina, captopril INFECCIONES: Hep B, C, HIV, otras, Exposiciones crónicas solventes. CANCER: pulmón, colon, estomago, riñón, próstata, ovario, vejiga, linfoma, otros.

21
Creatinina >=1.2 en mujeres y >= 1.4 en hombres con proteinuria rango nefrótico. Proteinuria >8 g/24 h por mas 6 meses. Biopsia renal con 10% fibrosis intersticial y proteinuria rango nefrótico. Otros: masculino, hipertensión, edad > 50 años. Creatinina >=1.2 en mujeres y >= 1.4 en hombres con proteinuria rango nefrótico. Proteinuria >8 g/24 h por mas 6 meses. Biopsia renal con 10% fibrosis intersticial y proteinuria rango nefrótico. Otros: masculino, hipertensión, edad > 50 años.

22
PRESENCIA FACTORES PROGRESION NO TERAPIA CONSERVADORA SI TERAPIA CONSERVADORA INMUNOSUPRESION

23
CONTROL DE PRESION ARTERIAL: pas 120 O MENOS. IECA AUN SI HAY NORMOTENSION, ARA O BLOQUEADORES CALCIO NO DIHIDROPIRIDINICOS. RESTRICCION EN DIETA: › PROTEINAS 0,7 – 0,8 g/K/dia. › ADICIONAR: 1 g PROTEINAS POR CADA g/PROTEINURIA > 3g/DIA. › SAL : 100 – 120 mEq /DIA.

24
CONTROL LIPIDOS: EVITAR ESTROGENOS. DEJAR DE FUMAR. NO AINES. AAS. ACIDO FOLICO. ANTIOXIDANTES : VIT C 200 mg/DIA. EVITAR SOBREINGESTA HIDRICA.

25
CICLOFOSFAMIDA + PREDNISONA. CLORAMBUCIL + PREDNISONA. AZATHIOPRINA + PREDNISONA. CICLOSPORINA + PREDNISONA?. MICOFENOLATO + PREDNISONA?.

28
Prognosis of Untreated Patients with Idiopathic Membranous Nephropathy Results Twenty-four (65 percent) of the 37 patients followed for at least five years had complete or partial remission of proteinuria; in 6 others (16 percent), end-stage renal disease developed, and they required dialysis. As calculated by the Kaplan-Meier method, the estimated probability (±the standard error of the estimate) of retaining adequate kidney function was 88 ±5 percent after five years and 73 ±7 percent after eight years. The prognosis was poorer in men and in patients over 50 years of age, but not in patients with the nephrotic syndrome, hypertension, or hypercholesterolemia. Conclusions Most untreated patients with idiopathic membranous nephropathy maintain renal function for prolonged periods and are likely to have spontaneous remission. These results do not support the use of glucocorticoids and immunosuppressive drugs in patients with idiopathic membranous nephropathy.
 of retaining adequate kidney function was 88 ±5 percent after five years and 73 ±7 percent after eight years. The prognosis was poorer in men and in patients over 50 years of age, but not in patients with the nephrotic syndrome, hypertension, or hypercholesterolemia. Conclusions Most untreated patients with idiopathic membranous nephropathy maintain renal function for prolonged periods and are likely to have spontaneous remission. These results do not support the use of glucocorticoids and immunosuppressive drugs in patients with idiopathic membranous nephropathy..")
29
METHYLPREDNISOLONE PLUS CHLORAMBUCIL AS COMPARED WITH METHYLPREDNISOLONE ALONE FOR THE TREATMENT OF IDIOPATHIC MEMBRANOUS NEPHROPATHY Author(s): PONTICELLI C, ZUCCHELLI P, PASSERINI P, CESANA B Source: NEW ENGLAND JOURNAL OF MEDICINE Volume: 327 Issue: 9 Pages: 599-603 Published: AUG 27 1992 Background and Methods. Treatment with methylprednisolone and chlorambucil may protect renal function and increase the chance of remission of the nephrotic syndrome in patients with idiopathic membranous nephropathy. To determine whether similar results might be obtained with methylprednisolone alone, we compared the effects of methylprednisolone and chlorambucil with those of methylprednisolone alone in 92 patients with the nephrotic syndrome caused by idiopathic membranous nephropathy. The patients were randomly assigned to receive either alternating one- month courses of methylprednisolone and then chlorambucil for a total of six months (group 1) or methylprednisolone alone for six months at the same cumulative dosage (group 2).
 or methylprednisolone alone for six months at the same cumulative dosage (group 2)..")
30
METHYLPREDNISOLONE PLUS CHLORAMBUCIL AS COMPARED WITH METHYLPREDNISOLONE ALONE FOR THE TREATMENT OF IDIOPATHIC MEMBRANOUS NEPHROPATHY Author(s): PONTICELLI C, ZUCCHELLI P, PASSERINI P, CESANA B Source: NEW ENGLAND JOURNAL OF MEDICINE Volume: 327 Issue: 9 Pages: 599-603 Published: AUG 27 1992 Results. Four of the 45 patients in group 1 (9 percent) and 1 of the 47 in group 2 (2 percent) stopped treatment because of side effects. At one, two, and three years, the percentage of patients who did not have the nephrotic syndrome was significantly higher in group 1 than in group 2. It was 58, 54, and 66 percent, respectively, in group 1, as compared with 26, 32, and 40 percent in group 2 (P = 0.002, 0.029, and 0.011). By year 4, the difference was no longer statistically significant: 62 percent of the patients in group 1 and 42 percent of those in group 2 did not have the nephrotic syndrome (P = 0.102). The patients in group 1 were in remission longer than those in group 2 (P = 0.008). Conclusions. In patients with the nephrotic syndrome caused by idiopathic membranous nephropathy, treatment with methylprednisolone and chlorambucil for six months induces an earlier remission of the nephrotic syndrome than methylprednisolone alone, but the difference may diminish with time.
 and 1 of the 47 in group 2 (2 percent) stopped treatment because of side effects. At one, two, and three years, the percentage of patients who did not have the nephrotic syndrome was significantly higher in group 1 than in group 2. It was 58, 54, and 66 percent, respectively, in group 1, as compared with 26, 32, and 40 percent in group 2 (P = 0.002, 0.029, and 0.011). By year 4, the difference was no longer statistically significant: 62 percent of the patients in group 1 and 42 percent of those in group 2 did not have the nephrotic syndrome (P = 0.102). The patients in group 1 were in remission longer than those in group 2 (P = 0.008). Conclusions. In patients with the nephrotic syndrome caused by idiopathic membranous nephropathy, treatment with methylprednisolone and chlorambucil for six months induces an earlier remission of the nephrotic syndrome than methylprednisolone alone, but the difference may diminish with time..")
32
CHARACTERISTICGROUP 1GROUP 2P No. of cases4647 Age (yr)37.2 ± 12.438.0 ± 13.60.77 range16 to 6618 to 64 Gender ratio27:1930:170.67 Disease duration (mo)11.7 ± 6.210.8 ± 7.90.48 Serum creatinine (mg/dl) 1.17 ± 0.221.21 ± 0.310.48 MDRD GFR (ml/min)84 ± 2289 ± 260.32 Serum albumin (g/dl)2.42 ± 0.812.34 ± 0.580.58 Serum cholesterol (mg/dl) 306.4 ± 88.2336.7 ± 99.60.12 Proteinuria (g/d)5.91 ± 2.26.11 ± 2.50.68
37.2 ± ± range16 to 6618 to 64 Gender ratio27:1930: Disease duration (mo)11.7 ± ± Serum creatinine (mg/dl) 1.17 ± ± MDRD GFR (ml/min)84 ± 2289 ± Serum albumin (g/dl)2.42 ± ± Serum cholesterol (mg/dl) ± ± Proteinuria (g/d)5.91 ± ±")
33
Kaplan-Meier plots showing probabilities of dialysis-free survival (A), survival without reaching either end point (B), complete remission (C), and complete or partial remission (D). Solid line, group 1; dashed line, group 2.

34
The course of proteinuria (A) and the Modification of Diet in Renal Disease (MDRD) estimated GFR (eGFR; B) during the follow up-period., group 1,, group 2. *P < 0.05; # P < 0.01; **P < 0.0001.

35
In conclusion: Untreated IMN with nephrotic syndrome is associated with a high risk for deterioration of renal function. A 6-mo regimen of cyclophosphamide and steroids induces remissions in a high proportion, arrests progression of renal insufficiency, and improves quality of life.

Presentaciones similares













>")

 BUENOS AIRES-ARGENTINA AÑO 2009 INTRODUCCION : Resumen: Título: Presentación.>")


![La eficacia de la condroitina en el tratamiento de la artrosis es dudosa AP al día [ ] Reichenbach.](/12/3380941/big_thumb.jpg "La eficacia de la condroitina en el tratamiento de la artrosis es dudosa AP al día [ ] Reichenbach.>")

 developed ischemia with exercise. During a mean follow-up of 4.5 3.4 years, 313 patients died, and 183 patients had.>")

