Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Omega-3 y Riesgo Residual
Dr. Alonso Merchán V. Fundación (Clínica) A. Shaio Barranquilla, Septiembre 4 de 2010
 A. Shaio. Barranquilla, Septiembre 4 de")
2
Acido grasos esenciales
w-6 familia C18:3 w-3 w-3 familia A. a-Linolenico Nueces Aceite de linaza Aceite de canola Aceite de soya C20:5 w-3 Eicosapentaenoico EPA C22:6 w-3 Docosahexaenoico DHA Pescado Cápsulas de aceite de pescado H3C H3C COOH COOH C18:2 w-6 Acido Linoleico Aceite de maiz Aceite de girasol Aceite de algodón Mani Soya H3C COOH H3C COOH C20:4 w-6 Acido Araquidonico H3C COOH PROSTAGLANDINAS TROMBOXANOS LEUCOTRIENOS PGI3, TXA3, LTA5,B5,C5 Vs. PGE2, TXA2, LTB4,E4 ATEROSCLEROSIS, AGREGACION, PA, VISCOSIDAD, INMUNIDAD, INFLAMACION

3
Substancia que administrada interior o exteriormente
ACIDOS GRASOS OMEGA-3 FARMACO: Substancia que administrada interior o exteriormente a un organismo, previene, cura o alivia una enfermedad o repara las secuelas de esta enfermedad Fármaco: Concentración/pureza aprobado por FDA/Invima Dosis/Recomendaciones/Cuidado médico VERSUS Suplemento: No requiere aprobación por FDA. No recomendado para tratar o prevenir una enfermedad Brunton S. Current Medical Research and Opinions 2007;23:

7
Reducción Riesgo Relativo EVENTOS
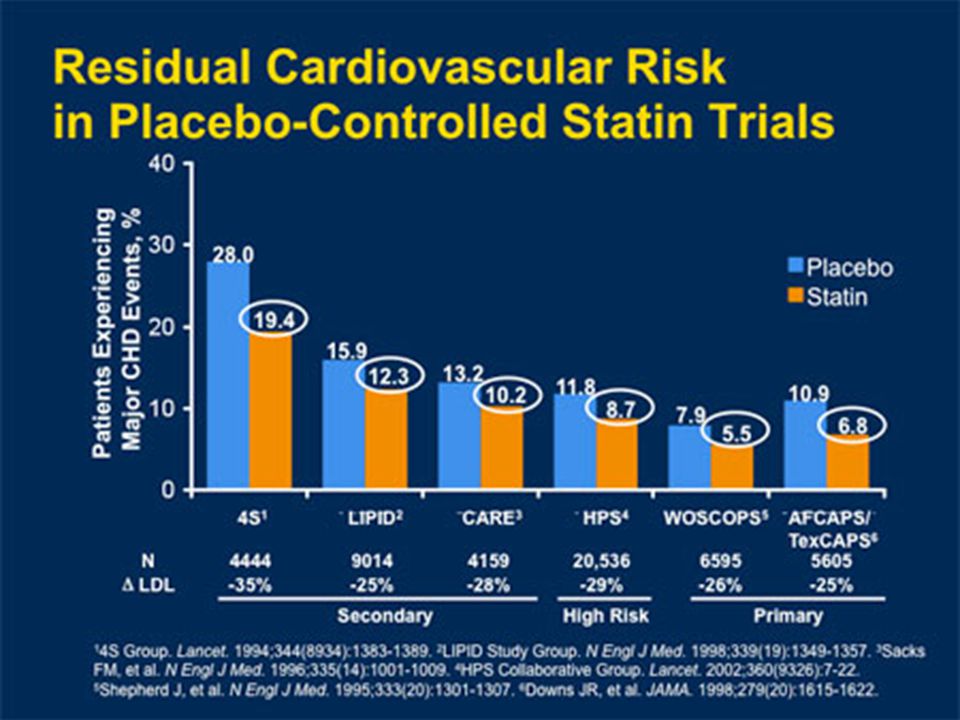
16 36 37 15 27 24 31 22 WOSCOPS ASCOT-LLA Reducción Riesgo Relativo EVENTOS 10 20 30 40 50 60 70 80 90 100 4S CARE LIPID AFCAPS HPS PROSPER CARDS TNT PROVE-IT IDEAL JUPITER RRR 30 % 44 Riesgo residual 70 % Enseñanza: La reducción de los niveles de C-LDL con tratamiento con estatinas reduce el riesgo de eventos cardiovasculares, pero aún permanece un riesgo residual sustancial. Las estatinas reducen el riesgo de eventos cardiovasculares en un amplio espectro de tipos de pacientes, principalmente a través de la reducción de los niveles de colesterol transportado por LDL, o C-LDL.1 En diversos estudios de resultados cardiovasculares, que difieren en diseño y composición de pacientes, la reducción de los niveles de C-LDL por medio del tratamiento con estatinas ha reducido el riesgo relativo de eventos cardiovasculares hasta en un 37%.1 El riesgo cardiovascular residual que persiste a pesar del tratamiento con estatinas, destaca la importancia de manejar los componentes lipídicos, además de C-LDL (por ejemplo el colesterol de lipoproteínas de alta densidad (C-HDL) y los triglicéridos) y otros factores de riesgo tales como la diabetes, tabaquismo, hipertensión y obesidad, mismos que contribuyen con el riesgo CV.1 Estudios posteriores usaron controles activos, de tal manera que en estos estudios la eficacia puede parecer disminuida en comparación con los resultados de los estudios controlados con placebo.2–4 Referencias: Chapman J. Beyond LDL-cholesterol reduction: the way ahead in managing dyslipidemia. Eur Heart J Suppl. 2005;7(suppl F):F56–F62. LaRosa JC, Grundy SM, Waters DD, y cols. Intensive lipid lowering with atorvastatin in patients with stable coronary disease. N Engl J Med. 2005;352:1425–1435. Cannon CP, Braunwald E, McCabe CH, y cols. Intensive versus moderate lipid lowering with statins after acute coronary syndromes. N Engl J Med. 2004;350:1495–1505. Pedersen TR, Faergeman O, Kastelein JJP, y cols. High dose atorvastatin vs usual-dose simvastin for secondary prevention after myocardial infarction: The IDEAL study: A randomized controlled trial. JAMA. 2005;294:2437–3092. Scandinavian Simvastatin Survival Study. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet. 1994;344:1383–1389. Sacks FM, Pfeffer MA, Lemuel AM, y cols. The effect of pravastatin on coronary events after myocardial infarction in patients with average cholesterol levels. Cholesterol and Recurrent Events Trial investigators. N Engl J Med. 1996;335:1001 –1009. Shepherd J, Cobbe SM, Ford I, y cols. Prevention of coronary heart disease with pravastatin in men with hypercholesterolemia. West of Scotland Coronary Prevention Study Group. N Engl J Med. 1995;333:1301– 1307. The Long-Term Intervention With Pravastatin in Ischaemic Disease (LIPID) Study Group. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N Engl J Med. 1998;339:1349–1357. Downs JR, Clearfield M, Weis S, y cols. Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels: results of AFCAPS/TexCAPS. Air Force/Texas Coronary Atherosclerosis Prevention Study. JAMA. 1998;279:1615–1622. Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in high-risk individuals: a randomised placebo controlled trial. Lancet. 2002;36:7–22. Shepherd J, Blauw GJ, Murphy MB, y cols. Pravastatin in elderly individuals at risk of vascular disease (PROSPER): a randomised controlled trial. Lancet. 2002;360:1623–1630. Colhoun HM, Betteridge DJ, Durrington PN, y cols. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): multicentre randomised placebo-controlled trial. Lancet. 2004;364:685–696. Sever PS, Björn Dahlöf, Neil R Poulter, y cols. Prevention of coronary and stroke events with atorvastatin in hypertensive patients who have average or lower-than-average cholesterol concentrations, in the Anglo-Scandinavian Cardiac Outcomes Trial--Lipid Lowering Arm (ASCOT-LLA): a multicentre randomised controlled trial. Lancet. 2003;361:1149–1158. 4S = Scandinavian Simvastatin Survival Study; CARE = Cholesterol And Recurrent Events; WOSCOPS = West of Scotland Coronary Prevention Study; LIPID= Long-term Intervention with Pravastatin in Ischemic Disease; AFCAPS = Air Force/Texas Coronary Atherosclerosis Prevention Study; HPS = Heart Protection Study; PROSPER = Prospective Study of Pravastatin in Elderly at Risk; CARDS = Collaborative Atorvastatin Diabetes Study; ASCOT-LLA = Anglo-Scandinavian Cardiac Outcomes Trial—Lipid-Lowering Arm; TNT = Treating to New Targets; PROVE-IT = PRavastatin Or atorVastatin Evaluation and Infection Therapy; IDEAL = Incremental Decrease in End points through Aggressive Lipid lowering; CV = cardiovascular. [4S Study Group]. Lancet. 1994;344:1383–1389; Sacks FM y cols. N Engl J Med. 1996;335:1001 –1009; Shepherd J y cols. N Engl J Med. 1995;333:1301– 1307; The Long-Term Intervention With Pravastatin in Ischaemic Disease (LIPID) Study Group. N Engl J Med. 1998;339:1349–1357; Downs JR y cols. JAMA. 1998;279:1615–1622; Heart Protection Study Collaborative Group. Lancet. 2002;36:7–22; Shepherd J y cols. Lancet. 2002;360:1623–1630; Colhoun HM y cols. Lancet. 2004;364:685–696; Sever PS y cols. Lancet. 2003;361:1149–1158; LaRosa JC y cols. N Engl J Med. 2005;352:1425–1435; Cannon CP y cols. N Engl J Med. 2004;350:1495–1505; Pedersen TR y cols. JAMA. 2005;294:2437–3092. Adaptado de Chapman J. Eur Heart J. 2005;7(suppl F):F56–F62.
 y los triglicéridos) y otros factores de riesgo tales como la diabetes, tabaquismo, hipertensión y obesidad, mismos que contribuyen con el riesgo CV.1. Estudios posteriores usaron controles activos, de tal manera que en estos estudios la eficacia puede parecer disminuida en comparación con los resultados de los estudios controlados con placebo.2–4. Referencias: Chapman J. Beyond LDL-cholesterol reduction: the way ahead in managing dyslipidemia. Eur Heart J Suppl. 2005;7(suppl F):F56–F62. LaRosa JC, Grundy SM, Waters DD, y cols. Intensive lipid lowering with atorvastatin in patients with stable coronary disease. N Engl J Med. 2005;352:1425–1435. Cannon CP, Braunwald E, McCabe CH, y cols. Intensive versus moderate lipid lowering with statins after acute coronary syndromes. N Engl J Med. 2004;350:1495–1505. Pedersen TR, Faergeman O, Kastelein JJP, y cols. High dose atorvastatin vs usual-dose simvastin for secondary prevention after myocardial infarction: The IDEAL study: A randomized controlled trial. JAMA. 2005;294:2437–3092. Scandinavian Simvastatin Survival Study. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet. 1994;344:1383–1389. Sacks FM, Pfeffer MA, Lemuel AM, y cols. The effect of pravastatin on coronary events after myocardial infarction in patients with average cholesterol levels. Cholesterol and Recurrent Events Trial investigators. N Engl J Med. 1996;335:1001 –1009. Shepherd J, Cobbe SM, Ford I, y cols. Prevention of coronary heart disease with pravastatin in men with hypercholesterolemia. West of Scotland Coronary Prevention Study Group. N Engl J Med. 1995;333:1301– The Long-Term Intervention With Pravastatin in Ischaemic Disease (LIPID) Study Group. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N Engl J Med. 1998;339:1349–1357. Downs JR, Clearfield M, Weis S, y cols. Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels: results of AFCAPS/TexCAPS. Air Force/Texas Coronary Atherosclerosis Prevention Study. JAMA. 1998;279:1615–1622. Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in high-risk individuals: a randomised placebo controlled trial. Lancet. 2002;36:7–22. Shepherd J, Blauw GJ, Murphy MB, y cols. Pravastatin in elderly individuals at risk of vascular disease (PROSPER): a randomised controlled trial. Lancet. 2002;360:1623–1630. Colhoun HM, Betteridge DJ, Durrington PN, y cols. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): multicentre randomised placebo-controlled trial. Lancet. 2004;364:685–696. Sever PS, Björn Dahlöf, Neil R Poulter, y cols. Prevention of coronary and stroke events with atorvastatin in hypertensive patients who have average or lower-than-average cholesterol concentrations, in the Anglo-Scandinavian Cardiac Outcomes Trial--Lipid Lowering Arm (ASCOT-LLA): a multicentre randomised controlled trial. Lancet. 2003;361:1149– S = Scandinavian Simvastatin Survival Study; CARE = Cholesterol And Recurrent Events; WOSCOPS = West of Scotland Coronary Prevention Study; LIPID= Long-term Intervention with Pravastatin in Ischemic Disease; AFCAPS = Air Force/Texas Coronary Atherosclerosis Prevention Study; HPS = Heart Protection Study; PROSPER = Prospective Study of Pravastatin in Elderly at Risk; CARDS = Collaborative Atorvastatin Diabetes Study; ASCOT-LLA = Anglo-Scandinavian Cardiac Outcomes Trial—Lipid-Lowering Arm; TNT = Treating to New Targets; PROVE-IT = PRavastatin Or atorVastatin Evaluation and Infection Therapy; IDEAL = Incremental Decrease in End points through Aggressive Lipid lowering; CV = cardiovascular. [4S Study Group]. Lancet. 1994;344:1383–1389; Sacks FM y cols. N Engl J Med. 1996;335:1001 –1009; Shepherd J y cols. N Engl J Med. 1995;333:1301– 1307; The Long-Term Intervention With Pravastatin in Ischaemic Disease (LIPID) Study Group. N Engl J Med. 1998;339:1349–1357; Downs JR y cols. JAMA. 1998;279:1615–1622; Heart Protection Study Collaborative Group. Lancet. 2002;36:7–22; Shepherd J y cols. Lancet. 2002;360:1623–1630; Colhoun HM y cols. Lancet. 2004;364:685–696; Sever PS y cols. Lancet. 2003;361:1149–1158; LaRosa JC y cols. N Engl J Med. 2005;352:1425–1435; Cannon CP y cols. N Engl J Med. 2004;350:1495–1505; Pedersen TR y cols. JAMA. 2005;294:2437–3092. Adaptado de Chapman J. Eur Heart J. 2005;7(suppl F):F56–F62.")
8
Reducción Riesgo Relativo EVENTOS
16 36 37 15 27 24 31 22 WOSCOPS ASCOT-LLA Reducción Riesgo Relativo EVENTOS 10 20 30 40 50 60 70 80 90 100 4S CARE LIPID AFCAPS HPS PROSPER CARDS TNT PROVE-IT IDEAL JUPITER RRR 30 % 44 M/Factorial en metas TG (colesterol no-HDL) c-HDL ??? c-LDL, TG, c-HDL Triada lipidica Dislipidemia mixta D. Aterogenica R. Residual 70 % Enseñanza: La reducción de los niveles de C-LDL con tratamiento con estatinas reduce el riesgo de eventos cardiovasculares, pero aún permanece un riesgo residual sustancial. Las estatinas reducen el riesgo de eventos cardiovasculares en un amplio espectro de tipos de pacientes, principalmente a través de la reducción de los niveles de colesterol transportado por LDL, o C-LDL.1 En diversos estudios de resultados cardiovasculares, que difieren en diseño y composición de pacientes, la reducción de los niveles de C-LDL por medio del tratamiento con estatinas ha reducido el riesgo relativo de eventos cardiovasculares hasta en un 37%.1 El riesgo cardiovascular residual que persiste a pesar del tratamiento con estatinas, destaca la importancia de manejar los componentes lipídicos, además de C-LDL (por ejemplo el colesterol de lipoproteínas de alta densidad (C-HDL) y los triglicéridos) y otros factores de riesgo tales como la diabetes, tabaquismo, hipertensión y obesidad, mismos que contribuyen con el riesgo CV.1 Estudios posteriores usaron controles activos, de tal manera que en estos estudios la eficacia puede parecer disminuida en comparación con los resultados de los estudios controlados con placebo.2–4 Referencias: Chapman J. Beyond LDL-cholesterol reduction: the way ahead in managing dyslipidemia. Eur Heart J Suppl. 2005;7(suppl F):F56–F62. LaRosa JC, Grundy SM, Waters DD, y cols. Intensive lipid lowering with atorvastatin in patients with stable coronary disease. N Engl J Med. 2005;352:1425–1435. Cannon CP, Braunwald E, McCabe CH, y cols. Intensive versus moderate lipid lowering with statins after acute coronary syndromes. N Engl J Med. 2004;350:1495–1505. Pedersen TR, Faergeman O, Kastelein JJP, y cols. High dose atorvastatin vs usual-dose simvastin for secondary prevention after myocardial infarction: The IDEAL study: A randomized controlled trial. JAMA. 2005;294:2437–3092. Scandinavian Simvastatin Survival Study. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet. 1994;344:1383–1389. Sacks FM, Pfeffer MA, Lemuel AM, y cols. The effect of pravastatin on coronary events after myocardial infarction in patients with average cholesterol levels. Cholesterol and Recurrent Events Trial investigators. N Engl J Med. 1996;335:1001 –1009. Shepherd J, Cobbe SM, Ford I, y cols. Prevention of coronary heart disease with pravastatin in men with hypercholesterolemia. West of Scotland Coronary Prevention Study Group. N Engl J Med. 1995;333:1301– 1307. The Long-Term Intervention With Pravastatin in Ischaemic Disease (LIPID) Study Group. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N Engl J Med. 1998;339:1349–1357. Downs JR, Clearfield M, Weis S, y cols. Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels: results of AFCAPS/TexCAPS. Air Force/Texas Coronary Atherosclerosis Prevention Study. JAMA. 1998;279:1615–1622. Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in high-risk individuals: a randomised placebo controlled trial. Lancet. 2002;36:7–22. Shepherd J, Blauw GJ, Murphy MB, y cols. Pravastatin in elderly individuals at risk of vascular disease (PROSPER): a randomised controlled trial. Lancet. 2002;360:1623–1630. Colhoun HM, Betteridge DJ, Durrington PN, y cols. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): multicentre randomised placebo-controlled trial. Lancet. 2004;364:685–696. Sever PS, Björn Dahlöf, Neil R Poulter, y cols. Prevention of coronary and stroke events with atorvastatin in hypertensive patients who have average or lower-than-average cholesterol concentrations, in the Anglo-Scandinavian Cardiac Outcomes Trial--Lipid Lowering Arm (ASCOT-LLA): a multicentre randomised controlled trial. Lancet. 2003;361:1149–1158. 4S = Scandinavian Simvastatin Survival Study; CARE = Cholesterol And Recurrent Events; WOSCOPS = West of Scotland Coronary Prevention Study; LIPID= Long-term Intervention with Pravastatin in Ischemic Disease; AFCAPS = Air Force/Texas Coronary Atherosclerosis Prevention Study; HPS = Heart Protection Study; PROSPER = Prospective Study of Pravastatin in Elderly at Risk; CARDS = Collaborative Atorvastatin Diabetes Study; ASCOT-LLA = Anglo-Scandinavian Cardiac Outcomes Trial—Lipid-Lowering Arm; TNT = Treating to New Targets; PROVE-IT = PRavastatin Or atorVastatin Evaluation and Infection Therapy; IDEAL = Incremental Decrease in End points through Aggressive Lipid lowering; CV = cardiovascular. [4S Study Group]. Lancet. 1994;344:1383–1389; Sacks FM y cols. N Engl J Med. 1996;335:1001 –1009; Shepherd J y cols. N Engl J Med. 1995;333:1301– 1307; The Long-Term Intervention With Pravastatin in Ischaemic Disease (LIPID) Study Group. N Engl J Med. 1998;339:1349–1357; Downs JR y cols. JAMA. 1998;279:1615–1622; Heart Protection Study Collaborative Group. Lancet. 2002;36:7–22; Shepherd J y cols. Lancet. 2002;360:1623–1630; Colhoun HM y cols. Lancet. 2004;364:685–696; Sever PS y cols. Lancet. 2003;361:1149–1158; LaRosa JC y cols. N Engl J Med. 2005;352:1425–1435; Cannon CP y cols. N Engl J Med. 2004;350:1495–1505; Pedersen TR y cols. JAMA. 2005;294:2437–3092. Adaptado de Chapman J. Eur Heart J. 2005;7(suppl F):F56–F62.
 c-HDL. c-LDL, TG, c-HDL. Triada lipidica. Dislipidemia mixta. D. Aterogenica. R. Residual. 70 % Enseñanza: La reducción de los niveles de C-LDL con tratamiento con estatinas reduce el riesgo de eventos cardiovasculares, pero aún permanece un riesgo residual sustancial. Las estatinas reducen el riesgo de eventos cardiovasculares en un amplio espectro de tipos de pacientes, principalmente a través de la reducción de los niveles de colesterol transportado por LDL, o C-LDL.1. En diversos estudios de resultados cardiovasculares, que difieren en diseño y composición de pacientes, la reducción de los niveles de C-LDL por medio del tratamiento con estatinas ha reducido el riesgo relativo de eventos cardiovasculares hasta en un 37%.1. El riesgo cardiovascular residual que persiste a pesar del tratamiento con estatinas, destaca la importancia de manejar los componentes lipídicos, además de C-LDL (por ejemplo el colesterol de lipoproteínas de alta densidad (C-HDL) y los triglicéridos) y otros factores de riesgo tales como la diabetes, tabaquismo, hipertensión y obesidad, mismos que contribuyen con el riesgo CV.1. Estudios posteriores usaron controles activos, de tal manera que en estos estudios la eficacia puede parecer disminuida en comparación con los resultados de los estudios controlados con placebo.2–4. Referencias: Chapman J. Beyond LDL-cholesterol reduction: the way ahead in managing dyslipidemia. Eur Heart J Suppl. 2005;7(suppl F):F56–F62. LaRosa JC, Grundy SM, Waters DD, y cols. Intensive lipid lowering with atorvastatin in patients with stable coronary disease. N Engl J Med. 2005;352:1425–1435. Cannon CP, Braunwald E, McCabe CH, y cols. Intensive versus moderate lipid lowering with statins after acute coronary syndromes. N Engl J Med. 2004;350:1495–1505. Pedersen TR, Faergeman O, Kastelein JJP, y cols. High dose atorvastatin vs usual-dose simvastin for secondary prevention after myocardial infarction: The IDEAL study: A randomized controlled trial. JAMA. 2005;294:2437–3092. Scandinavian Simvastatin Survival Study. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet. 1994;344:1383–1389. Sacks FM, Pfeffer MA, Lemuel AM, y cols. The effect of pravastatin on coronary events after myocardial infarction in patients with average cholesterol levels. Cholesterol and Recurrent Events Trial investigators. N Engl J Med. 1996;335:1001 –1009. Shepherd J, Cobbe SM, Ford I, y cols. Prevention of coronary heart disease with pravastatin in men with hypercholesterolemia. West of Scotland Coronary Prevention Study Group. N Engl J Med. 1995;333:1301– The Long-Term Intervention With Pravastatin in Ischaemic Disease (LIPID) Study Group. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N Engl J Med. 1998;339:1349–1357. Downs JR, Clearfield M, Weis S, y cols. Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels: results of AFCAPS/TexCAPS. Air Force/Texas Coronary Atherosclerosis Prevention Study. JAMA. 1998;279:1615–1622. Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in high-risk individuals: a randomised placebo controlled trial. Lancet. 2002;36:7–22. Shepherd J, Blauw GJ, Murphy MB, y cols. Pravastatin in elderly individuals at risk of vascular disease (PROSPER): a randomised controlled trial. Lancet. 2002;360:1623–1630. Colhoun HM, Betteridge DJ, Durrington PN, y cols. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): multicentre randomised placebo-controlled trial. Lancet. 2004;364:685–696. Sever PS, Björn Dahlöf, Neil R Poulter, y cols. Prevention of coronary and stroke events with atorvastatin in hypertensive patients who have average or lower-than-average cholesterol concentrations, in the Anglo-Scandinavian Cardiac Outcomes Trial--Lipid Lowering Arm (ASCOT-LLA): a multicentre randomised controlled trial. Lancet. 2003;361:1149– S = Scandinavian Simvastatin Survival Study; CARE = Cholesterol And Recurrent Events; WOSCOPS = West of Scotland Coronary Prevention Study; LIPID= Long-term Intervention with Pravastatin in Ischemic Disease; AFCAPS = Air Force/Texas Coronary Atherosclerosis Prevention Study; HPS = Heart Protection Study; PROSPER = Prospective Study of Pravastatin in Elderly at Risk; CARDS = Collaborative Atorvastatin Diabetes Study; ASCOT-LLA = Anglo-Scandinavian Cardiac Outcomes Trial—Lipid-Lowering Arm; TNT = Treating to New Targets; PROVE-IT = PRavastatin Or atorVastatin Evaluation and Infection Therapy; IDEAL = Incremental Decrease in End points through Aggressive Lipid lowering; CV = cardiovascular. [4S Study Group]. Lancet. 1994;344:1383–1389; Sacks FM y cols. N Engl J Med. 1996;335:1001 –1009; Shepherd J y cols. N Engl J Med. 1995;333:1301– 1307; The Long-Term Intervention With Pravastatin in Ischaemic Disease (LIPID) Study Group. N Engl J Med. 1998;339:1349–1357; Downs JR y cols. JAMA. 1998;279:1615–1622; Heart Protection Study Collaborative Group. Lancet. 2002;36:7–22; Shepherd J y cols. Lancet. 2002;360:1623–1630; Colhoun HM y cols. Lancet. 2004;364:685–696; Sever PS y cols. Lancet. 2003;361:1149–1158; LaRosa JC y cols. N Engl J Med. 2005;352:1425–1435; Cannon CP y cols. N Engl J Med. 2004;350:1495–1505; Pedersen TR y cols. JAMA. 2005;294:2437–3092. Adaptado de Chapman J. Eur Heart J. 2005;7(suppl F):F56–F62.")
9
Frecuencia acumulativa
100 – 80 – 60 – 40 – 20 – 0 – LDL grande y sobrenadante LDL pequeña y densa Frecuencia acumulativa TG y HDL-c Inversamente proporcional TG e IDL Directamente proporcional Nivel de triglicéridos (mg/dL) Fenotipo LDL A: lipoproteina grande, sobrenadante Fenotipo LDL B: lipoproteina pequeña y densa Austin MA, et al. Circulation 1990 ; 82 : 495
 Fenotipo LDL A: lipoproteina grande, sobrenadante. Fenotipo LDL B: lipoproteina pequeña y densa. Austin MA, et al. Circulation 1990 ; 82 : 495.")
10
“Triada Lipidica” : Mayor Riesgo Coronario Vs c-LDL aisladamente alto
Scandinavian Simvastatin Survival Study (4S) Placebo Arm 40 35.9 35 c-LDL elevado aisladamente c-LDL + TG altos y c-HDL bajo 30 25 20.9 Event rate (%) 20 15 12.2 The clinical impact of the “lipid triad” of HDL-C combined with elevated triglycerides in the presence of elevated LDL-C was evident in 5-year CHD-event data from the placebo arm of the Scandinavian Simvastatin Survival Study (4S). Patients enrolled into this study had a history of CHD and had total cholesterol levels of 5.5 to 8.0 mmol/L (210 to 310 mg/dL).1 The analysis shown here provides rates of major coronary events, on the left, and coronary mortality, on the right, for 2 distinct subgroups of patients: those with isolated LDL-C elevations who were in the highest quartile for HDL-C and lowest quartile for triglycerides, represented by the orange bars; and, those with the “lipid triad” who had elevated LDL-C and were in the lowest quartile for HDL-C and highest quartile for triglycerides, and are represented by the yellow bars. At baseline, patients with the lipid triad had a mean LDL-C of 4.91 mmol/L (190 mg/dL), mean HDL-C of 0.85 mmol/L (33 mg/dL), and a mean triglyceride level of 2.23 mmol/L (198 mg/dL). Patients with isolated LDL-C elevation had a mean LDL-C level of 4.67 mmol/L (181 mg/dL) at baseline, with mean values of 1.62 mmol/L (63 mg/dL) and 0.89 mmol/L (79 mg/dL) for HDL-C and triglycerides, respectively.1 The 5-year rate of major coronary events was higher among patients with the lipid triad (35.9%) versus patients with only elevation of LDL-C (20.9%).1 These events included coronary death, definite or probable hospital-verified nonfatal acute myocardial infarction, resuscitated cardiac arrest, and definite silent myocardial infarction, as verified by electrocardiogram.1 The 5-year rate of CHD death was also markedly higher among patients with the lipid triad at baseline (12.2%) versus patients with isolated elevation of LDL-C (8.5%).1 These findings support the conclusion that the lipid triad of the lowest levels of HDL-C and the highest levels of triglycerides in the presence of elevated LDL-C places patients at very high risk for CHD events compared with isolated LDL-C elevations.1 10 8.5 5 (n=284) (n=237) (n=284) (n=237) Eventos coronarios mayores Mortalidad Coronaria Adapted from Ballantyne CM et al. Circulation. 2001;104:3046–3051. Reference Ballantyne CM, Olsson AG, Cook TJ, et al. Influence of low high-density lipoprotein cholesterol and elevated triglyceride on coronary heart disease events and response to simvastatin therapy in 4S. Circulation. 2001;104:3046–3051.
 Placebo Arm c-LDL elevado aisladamente. c-LDL + TG altos y c-HDL bajo Event rate (%) The clinical impact of the lipid triad of HDL-C combined with elevated triglycerides in the presence of elevated LDL-C was evident in 5-year CHD-event data from the placebo arm of the Scandinavian Simvastatin Survival Study (4S). Patients enrolled into this study had a history of CHD and had total cholesterol levels of 5.5 to 8.0 mmol/L (210 to 310 mg/dL).1 The analysis shown here provides rates of major coronary events, on the left, and coronary mortality, on the right, for 2 distinct subgroups of patients: those with isolated LDL-C elevations who were in the highest quartile for HDL-C and lowest quartile for triglycerides, represented by the orange bars; and, those with the lipid triad who had elevated LDL-C and were in the lowest quartile for HDL-C and highest quartile for triglycerides, and are represented by the yellow bars. At baseline, patients with the lipid triad had a mean LDL-C of 4.91 mmol/L (190 mg/dL), mean HDL-C of 0.85 mmol/L (33 mg/dL), and a mean triglyceride level of 2.23 mmol/L (198 mg/dL). Patients with isolated LDL-C elevation had a mean LDL-C level of 4.67 mmol/L (181 mg/dL) at baseline, with mean values of 1.62 mmol/L (63 mg/dL) and 0.89 mmol/L (79 mg/dL) for HDL-C and triglycerides, respectively.1. The 5-year rate of major coronary events was higher among patients with the lipid triad (35.9%) versus patients with only elevation of LDL-C (20.9%).1 These events included coronary death, definite or probable hospital-verified nonfatal acute myocardial infarction, resuscitated cardiac arrest, and definite silent myocardial infarction, as verified by electrocardiogram.1. The 5-year rate of CHD death was also markedly higher among patients with the lipid triad at baseline (12.2%) versus patients with isolated elevation of LDL-C (8.5%).1. These findings support the conclusion that the lipid triad of the lowest levels of HDL-C and the highest levels of triglycerides in the presence of elevated LDL-C places patients at very high risk for CHD events compared with isolated LDL-C elevations (n=284) (n=237) (n=284) (n=237) Eventos coronarios mayores. Mortalidad Coronaria. Adapted from Ballantyne CM et al. Circulation. 2001;104:3046–3051. Reference. Ballantyne CM, Olsson AG, Cook TJ, et al. Influence of low high-density lipoprotein cholesterol and elevated triglyceride on coronary heart disease events and response to simvastatin therapy in 4S. Circulation. 2001;104:3046–3051.")
11
c-LDL en meta (de acuerdo al riesgo)
Objetivo Primario: c-LDL (I A) Objetivo Secundario: col no-HDL (TG) y c-HDL (IIa B en Alto y Muy Alto Riesgo) NCEP-ATPIII (2001 Y 2004) c-LDL en meta (de acuerdo al riesgo) TG < : META > : FIBRATO, NIACINA, ESTATINA, OMEGA-3 : CALCULE no-HDL y así decide TTO c-HDL > 40 en Hombres > 50 en Mujeres
 Objetivo Secundario: col no-HDL (TG) y c-HDL. (IIa B en Alto y Muy Alto Riesgo) NCEP-ATPIII (2001 Y 2004) c-LDL en meta (de acuerdo al riesgo) TG < 150 : META. > 500 : FIBRATO, NIACINA, ESTATINA, OMEGA : CALCULE no-HDL y así decide TTO. c-HDL > 40 en Hombres. > 50 en Mujeres.")
12
c-Total = c-HDL + c-VLDL + c-LDL + c-IDL + c-Lp(a)
Apo A Apo B c-LDL, c-IDL, c-Lp(a) = c-LDL Colesterol no-HDL c-Total - c-HDL c-LDL = c-Total – (c-HDL + TG/5) META c-LDL/Riesgo + 30 mg/dl Riesgo global a 10 años (IM, muerte coronaria) c-LDL Colesterol no-HDL > 20%: Aterosclerosis, DM-2, FR/Framingham, HFH >> 20 %: Aterosclerosis + DM/SM/FR no controlados < 100 < 70 < 130 10-20%: DM-1, SM, FR/Framingham < 160 < 10%: Factores de riesgo < 160 < 190
 = c-LDL. Colesterol no-HDL. c-Total - c-HDL. c-LDL = c-Total – (c-HDL + TG/5) META. c-LDL/Riesgo + 30 mg/dl. Riesgo global a 10 años (IM, muerte coronaria) c-LDL. Colesterol no-HDL. > 20%: Aterosclerosis, DM-2, FR/Framingham, HFH. >> 20 %: Aterosclerosis + DM/SM/FR no controlados. < 100. < 70. < %: DM-1, SM, FR/Framingham. < 160. < 10%: Factores de riesgo. < 160. < 190.")
13
c-LDL = c-Total - (c-HDL + TG/5)
c-Total = c-LDL + c-HDL + c-VLDL (TG/5) c-LDL = c-Total - (c-HDL + TG/5) - Válida con TG < 400 mg/dl - 8 horas de ayuno c-Total = c-HDL + c-VLDL + c-LDL + c-IDL + c-Lp(a) c-Total = 200 mg/dl c-HDL = 40 c-LDL = 130 TG = 150 no-HDL = 160 c-Total = 200 mg/dl c-HDL = 40 c-LDL = 100 TG = 300 no-HDL = 160 Fridewald WT. Clin Chem 1972;18:
 c-LDL = c-Total - (c-HDL + TG/5) - Válida con TG < 400 mg/dl. - 8 horas de ayuno. c-Total = c-HDL + c-VLDL + c-LDL + c-IDL + c-Lp(a) c-Total = 200 mg/dl. c-HDL = 40. c-LDL = 130. TG = 150. no-HDL = 160. c-Total = 200 mg/dl. c-HDL = 40. c-LDL = 100. TG = 300. no-HDL = 160. Fridewald WT. Clin Chem 1972;18:")
14
Basado en Framingham Heart Study
Am J Cardiol 2006;98:

15
Cual es el mejor predictor de eventos coronarios ?
c-LDL, colesterol no-HDL, ApoB, ApoB/Apo A ? AÑO/REF ESTUDIO c-LDL c-no HDL Apo B ApoB/ ApoA COMENTARIOS 1996 (1) Quebec X HOMBRES 2001 (2) Amoris SIN E. CORONARIA PREVIA 2001 (3) LRCP E. CORONARIA CONOCIDA 2002 (4) BARI 2003 (5) Strong Heart DM-2 2005 (6) 4 estudios 2005 (7) Women’s Health MUJERES “SANAS” 2005 (8) Health Proffessio HOMBRES “SANOS” 2006 (9) Framingham Coh 2007 (10) 2008 (11) TNT - IDEAL 2009 (12) ISIS–Reino Unido 3510 IAM Vs controles 2010 (13) EPIC-Europa 21448 sin DM/EC, a 12 años Adaptada por: Dr. Alonso Merchán V
 Quebec. X. HOMBRES (2) Amoris. SIN E. CORONARIA PREVIA (3) LRCP. E. CORONARIA CONOCIDA (4) BARI (5) Strong Heart. DM (6) 4 estudios (7) Women’s Health. MUJERES SANAS 2005 (8) Health Proffessio. HOMBRES SANOS 2006 (9) Framingham Coh (10) 2008 (11) TNT - IDEAL (12) ISIS–Reino Unido IAM Vs controles (13) EPIC-Europa sin DM/EC, a 12 años. Adaptada por: Dr. Alonso Merchán V.")
16
Cual es el mejor predictor de eventos coronarios ?
c-LDL, colesterol no-HDL, ApoB, ApoB/Apo A ? Referencias bibliograficas Lamarceh B, et al. Circulation 1996;94:23-28 Waldis G, et al. Lancet 2001;358: Cui Y, et al. Arch Inter Med 2001;161: Bittner B, et al. Circulation 2002, 106: Lu W, et al. Diabetes Care 2003;26:16-23 Liu J, et al. Diabetes Care 2005;28: Ridker PM, et al. JAMA 2005;294:326-33 Pischon T, et al. Circualtion 2005;112: Liu J, et al. Am J Cardiol 2006;98: Ingelsson E, et al. JAMA 2007;298:776-85 Kastelein J, et al. Circualtion 2008;117: Parish S, et al. Eur Heart J 2009;30: Arsenault B, et al. JACC 2010;55:35-41

17
Niveles de TG como factor de riesgo para E
Niveles de TG como factor de riesgo para E. Coronaria Metanálisis de 29 estudios. Grupos Casos de E.Cor RR 1.72 N = 262,525 10158 eventos Duración del Seguimiento ≥10 años <10 años Sexo Hombres Mujeres Estado de ayuno Ayuno No ayuno Ajustada por el HDL Triglyceride Level Is Significant CVD Risk Fact: Recent Meta-Analysis of 29 Studies. A recent meta-analysis by Sarwar et al1 included 29 prospective studies and was the largest and most comprehensive epidemiological assessment of the association between triglyceride values and CHD risk in Western populations ( participants; 10,158 CHD cases). A combined analysis of the 29 studies yielded an adjusted odds ratio of 1.72 (95% CI, ) in a comparison of extreme thirds of usual triglyceride values (ie, individuals with usual log-triglyceride values in the top third of the population compared with those in the bottom third). This odds ratio was adjusted in all but one study for at least age, sex, smoking status, lipid concentrations, and most studies also adjusted for blood pressure. The above figure shows the CHD risk ratio adjusted for several established risk factors and grouped according to several study characteristics (ie, duration of follow-up, sex, fasting status, and adjusted for HDL-cholesterol). The data indicate that the impact of triglycerides on CHD risk is similar in women and men and also regardless of duration of follow up. The data suggest no important differences in the strength of associations between triglycerides and CHD in studies of fasting participants compared with studies of nonfasting participants. Finally, adjustment for HDL-cholesterol attenuated the magnitude of the association between triglyceride level and CHD risk. The conclusion of the study is that there is a strong and highly significant association between triglyceride value and CHD risk. Reference 1. Sarwar N, et al. Circulation. 2007;115: Si No 1.72 ( ) 1 2 Riesgo de ECV * (95% CI) TG > 178 mg/dl Vs. < 115 mg/dl. Sarwar N, et al. Circulation. 2007;115: 17
. A combined analysis of the 29 studies yielded an adjusted odds ratio of 1.72 (95% CI, ) in a comparison of extreme thirds of usual triglyceride values (ie, individuals with usual log-triglyceride values in the top third of the population compared with those in the bottom third). This odds ratio was adjusted in all but one study for at least age, sex, smoking status, lipid concentrations, and most studies also adjusted for blood pressure. The above figure shows the CHD risk ratio adjusted for several established risk factors and grouped according to several study characteristics (ie, duration of follow-up, sex, fasting status, and adjusted for HDL-cholesterol). The data indicate that the impact of triglycerides on CHD risk is similar in women and men and also regardless of duration of follow up. The data suggest no important differences in the strength of associations between triglycerides and CHD in studies of fasting participants compared with studies of nonfasting participants. Finally, adjustment for HDL-cholesterol attenuated the magnitude of the association between triglyceride level and CHD risk. The conclusion of the study is that there is a strong and highly significant association between triglyceride value and CHD risk. Reference. 1. Sarwar N, et al. Circulation. 2007;115: Si No ( ) Riesgo de ECV * (95% CI) TG > 178 mg/dl Vs. < 115 mg/dl. Sarwar N, et al. Circulation. 2007;115:")
18
53 estudios/16,802 pacientes fibratos Vs. placebo
Efecto de los Fibratos sobre Enfermedad Coronaria: Resultado de un Meta-analisis 53 estudios/16,802 pacientes fibratos Vs. placebo Ref 1, p187, C1, ¶2, L5-7, L21-23; p192, T4, L3, L12, L18, L24, L30 P<0.001 P=NS P=NS Ref 1, p187, C1, ¶2, L 5-7, L21-23 P=NS Ref 1, p189, C1, ¶cont, L 9-12 P=NS Ref 1, p189, C1, ¶cont, L 12-18 Takeaway: Treatment with fibrates significantly reduced the risk of major coronary events by 25%, but not coronary deaths. A meta-analysis of 53 trials using fibrates or placebo was conducted.1 Statistically significant reductions in major coronary events (P<0.001) were shown only in the VA-HIT Trial and the Helsinki Heart Study.1 Other long-term trials (ie, Bezafibrate Coronary Atherosclerosis Intervention Trial [BECAIT], Bezafibrate Infarction Prevention Study, and the Bezafibrate Treatment in Lower Extremity Arterial Disease Event Reduction trial) showed tendencies toward significance in reduction in major coronary events (P=0.07).1 Pooled studies with the fibrates indicated a significant reduction in coronary events but no statistically significant reductions in mortality due to coronary cause or all cause.1 Ref 1, p189, C1, ¶cont, L 5-7 NS=No Significativo; CV=cardiovascular Birjmohun RS et al. J Am Coll Cardiol. 2005;45:185–197. Reference: 1. Birjmohun RS, Hutten BA, Kastelein JJ, et al. Efficacy and safety of high-density lipoprotein cholesterol-increasing compounds: a meta-analysis of randomized controlled trials. J Am Coll Cardiol. 2005;45:185–197.
 were shown only in the VA-HIT Trial and the Helsinki Heart Study.1. Other long-term trials (ie, Bezafibrate Coronary Atherosclerosis Intervention Trial [BECAIT], Bezafibrate Infarction Prevention Study, and the Bezafibrate Treatment in Lower Extremity Arterial Disease Event Reduction trial) showed tendencies toward significance in reduction in major coronary events (P=0.07).1. Pooled studies with the fibrates indicated a significant reduction in coronary events but no statistically significant reductions in mortality due to coronary cause or all cause.1. Ref 1, p189, C1, ¶cont, L 5-7. NS=No Significativo; CV=cardiovascular. Birjmohun RS et al. J Am Coll Cardiol. 2005;45:185–197. Reference: 1. Birjmohun RS, Hutten BA, Kastelein JJ, et al. Efficacy and safety of high-density lipoprotein cholesterol-increasing compounds: a meta-analysis of randomized controlled trials. J Am Coll Cardiol. 2005;45:185–197.")
20
Atorvastatina 80 Vs. Pravastatina 40 mg/día
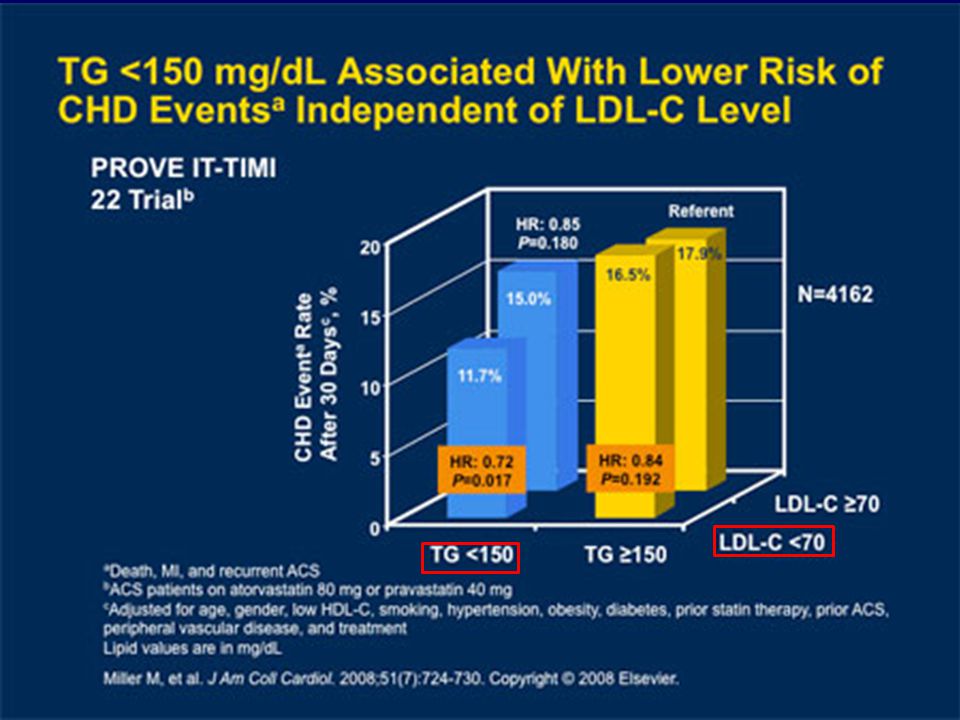
J Am Coll Cardiol 2008;51: 4162 personas con SCA Atorvastatina 80 Vs. Pravastatina 40 mg/día

21
No debe utilizarse cuando los triglicéridos son superiores a 400 mg/dl
Cálculo del colesterol LDL CT = cHDL + cLDL CT CT = cHDL + cLDL + cVLDL CT = cHDL VLDL Fosfolípidos y Proteínas 28% No debe utilizarse cuando los triglicéridos son superiores a 400 mg/dl Colesterol 12% Triglicéridos 60 % Triglicéridos 5 Colesterol 1 Fórmula de Friedewald 5 Triglicéridos cLDL cLDL = CT – (cHDL + cVLDL) 12-05-VYT CANDEAN-1310-SS
 VYT CANDEAN-1310-SS.")
22
c-LDL < 70 < 100 < = 130 TG < 150 c-HDL
Perfil lipìdico posterior a enfermedad coronaria. Recibe estatina c-Total mg/dl c-LDL 100 mg/dl (colesterol total – cHDL) = 190 – 30 = 160 c- HDL mg/dl TG mg/dl Variable (mg/dl) Muy alto riesgo Alto riesgo Otros riesgos c-LDL < 70 < 100 < = 130 TG < 150 c-HDL > 40 (H) > 50 (M) Col. no HDL < 130 < 160 c-Total/c-HDL < 3.5 (< 140/40) < 4.0 (170/40) < 5.0 (200/40) c-LDL/c-HDL < 1.5 (70/40) < 2.5 (100/40) < 3.5 (130/40) Apo B < 80 < 90 ApoB/ApoA < 0.5 (80/160) < 0.6 (90/160) < 0.6 TTO: aumento CTEV o ESTATINA o ESTATINA más efectiva o asociar: EZETIMIBE, NIACINA, FIBRATO, OMEGA-3
 = 190 – 30 = 160. c- HDL 30 mg/dl TG 300 mg/dl. Variable (mg/dl) Muy alto riesgo. Alto riesgo. Otros riesgos. c-LDL. < 70. < 100. < = 130. TG. < 150. c-HDL. > 40 (H) > 50 (M) Col. no HDL. < 130. < 160. c-Total/c-HDL. < 3.5 (< 140/40) < 4.0 (170/40) < 5.0 (200/40) c-LDL/c-HDL. < 1.5 (70/40) < 2.5 (100/40) < 3.5 (130/40) Apo B. < 80. < 90. ApoB/ApoA. < 0.5 (80/160) < 0.6 (90/160) < 0.6. TTO: aumento CTEV o ESTATINA o ESTATINA más efectiva. o asociar: EZETIMIBE, NIACINA, FIBRATO, OMEGA-3.")
23
Ezetimibe/simvastati
PROPUESTA PARA ESCOGENCIA DE HIPOLIPEMIANTE, DE ACUERDO AL LDL-c % LDL–c Disminuir Ezetimibe/simvastati 10/ / /40 Simvastatina Atorvastatina Rosuvastatina Pravastatina Lovastatina < 30% X 35 % 40 % 45% 50% >55% 6 % Eze/Sim 10/10 = 45% 10/20 = 50% 10/40 = 55% c-HDL aumenta % TG reduce % STELLAR : Am J Cardiol 2003 ; 9 : 11c – 19c Adaptada por Dr. A. Merchán V.

24
Hipolipemiantes y perfil lipídico Fibratos
Terapia A. nicotinico Estatinas Fibratos Omega-3 Ezetimibe HDL-C 15–35% 5–10% 5–15% 2-4% LDL-C 5–25% 18–55% 0–15% O TG 20–40% 7–30% 30–50% Lp(a)/Fibrin Nicotinic acid and other lipid-modifying agents: typical effects on lipoproteins Clinical experience with lipid-modifying agents shows that nicotinic acid is the most effective agent we have available today for raising HDL-C. In addition, nicotinic acid provides clinically useful improvements in other components of the lipid profile. The following slides describe in detail the extensive clinical experience gained with Niaspan® to date. National Cholesterol Education Program. NIH Publication No September 2002 20-40 5 % 18% 10-20%
/Fibrin. Nicotinic acid and other lipid-modifying agents: typical effects on lipoproteins. Clinical experience with lipid-modifying agents shows that nicotinic acid is the most effective agent we have available today for raising HDL-C. In addition, nicotinic acid provides clinically useful improvements in other components of the lipid profile. The following slides describe in detail the extensive clinical experience gained with Niaspan® to date. National Cholesterol Education Program. NIH Publication No September % 18% 10-20%")
25
Rabdiomiolisis por millón de prescripciones asociando Estatinas
Basado en el Sistema de Reporte de Eventos Adversos de la FDA. Am J Cardiol 2005;95: Rabdiomiolisis por millón de prescripciones asociando Estatinas (no cerivastatina) y Fenofibrato o Gemfibrozil
 y Fenofibrato o Gemfibrozil.")
26
In Diabetes (FIELD). 975 personas con DM-2
Analisis post-hoc del estudio Fenofibrate Intervention and Event Lowering In Diabetes (FIELD). 975 personas con DM-2 Eventos C/V: IM, ACV, Muerte C/V, Revascularizacion Scott R, et al. (FIELD). Circulation 2007;116:II-838 (abstract)
. 975 personas con DM-2. Eventos C/V: IM, ACV, Muerte C/V, Revascularizacion. Scott R, et al. (FIELD). Circulation 2007;116:II-838 (abstract)")
27
Pacientes con DM-2 alto riesgo Simvastatina + Fenofibrato
N Engl J Med Marzo 2010; Pacientes con DM-2 alto riesgo Simvastatina + Fenofibrato Simvastatina + Placebo Eventos C/Vasculares fatales IM no fatal ACV no fatal - Seguimiento 4.7 años c-LDL no cambió c-HDL aumentó 8% TG disminuyó 21% 2.4% suspendieron

28
Hipolipemiantes y perfil lipídico Niacina/Laropiprant
Terapia Niacina Estatinas Fibratos Omega-3 Ezetimibe HDL-C 15–35% 5–10% 2 - 4 LDL-C 5–25% 18–55% 0–15% O TG 20–40% 7–30% 30–50% Lp(a)/Fibrin Nicotinic acid and other lipid-modifying agents: typical effects on lipoproteins Clinical experience with lipid-modifying agents shows that nicotinic acid is the most effective agent we have available today for raising HDL-C. In addition, nicotinic acid provides clinically useful improvements in other components of the lipid profile. The following slides describe in detail the extensive clinical experience gained with Niaspan® to date. National Cholesterol Education Program. NIH Publication No September 2002 20-40 5 % 18% 10-20%
/Fibrin. Nicotinic acid and other lipid-modifying agents: typical effects on lipoproteins. Clinical experience with lipid-modifying agents shows that nicotinic acid is the most effective agent we have available today for raising HDL-C. In addition, nicotinic acid provides clinically useful improvements in other components of the lipid profile. The following slides describe in detail the extensive clinical experience gained with Niaspan® to date. National Cholesterol Education Program. NIH Publication No September % 18% 10-20%")
29
ESTUDIOS EN CURSO CON FARMACOS QUE MODIFICAN
LA TRIADA LIPIDICA (c-LDL, c-HDL, TG) ESTUDIO FARMACOS NUMERO TOTAL/ SEGUIMIENTO PUBLICACION ACCORD FENOFIBRATO + ESTATINA VS. ESTATINA 5900/5.6 AÑOS 2009 AIM – HIGH NIACINA + SIMVASTATINA VS. SIMVASTATINA 3300/4.0 AÑOS 2010 HPS - THRIVE NIACINA/LAROPIPRANT + VS. SIMVASTATINA 20000/4.0 AÑOS 2012
 ESTUDIO. FARMACOS. NUMERO TOTAL/ SEGUIMIENTO. PUBLICACION. ACCORD. FENOFIBRATO + ESTATINA VS. ESTATINA. 5900/5.6 AÑOS AIM – HIGH. NIACINA + SIMVASTATINA VS. SIMVASTATINA. 3300/4.0 AÑOS HPS - THRIVE. NIACINA/LAROPIPRANT + VS. SIMVASTATINA /4.0 AÑOS")
30
Hipolipemiantes y perfil lipídico Omega-3 (2 a 4 gs/día)
Terapia A. nicotinico Estatinas Fibratos Omega-3 Ezetimibe HDL-C 15–35% 5–10% 5–15% 2-4% LDL-C 5–25% 18–55% 0–15% O TG 20–40% 7–30% 30–50% Lp(a)/Fibrin Nicotinic acid and other lipid-modifying agents: typical effects on lipoproteins Clinical experience with lipid-modifying agents shows that nicotinic acid is the most effective agent we have available today for raising HDL-C. In addition, nicotinic acid provides clinically useful improvements in other components of the lipid profile. The following slides describe in detail the extensive clinical experience gained with Niaspan® to date. National Cholesterol Education Program. NIH Publication No September 2002 20-40 5 % 18% 10-20%
/Fibrin. Nicotinic acid and other lipid-modifying agents: typical effects on lipoproteins. Clinical experience with lipid-modifying agents shows that nicotinic acid is the most effective agent we have available today for raising HDL-C. In addition, nicotinic acid provides clinically useful improvements in other components of the lipid profile. The following slides describe in detail the extensive clinical experience gained with Niaspan® to date. National Cholesterol Education Program. NIH Publication No September % 18% 10-20%")
31
Reducción aprox. de TG plasmáticos en %
1.0 2.0 3.0 4.0 5.0 6.0 40% 32% 27% 20% 15% 10% Reducción aprox. de TG plasmáticos en % Dosis de EPA + DHA (g/día) - 27 estudios que midieron TG: A > TG basales > efectividad LDL-c aumento en 10 mg/dl y HDL-c en 3.5 mg/dl Mínimos efectos secundarios y de laboratorio Balk E et al. Agency for Healthcare Research and Quality. March AHRQ publication No 04-E010-2
 - 27 estudios que midieron TG: A > TG basales > efectividad. LDL-c aumento en 10 mg/dl y HDL-c en 3.5 mg/dl. Mínimos efectos secundarios y de laboratorio. Balk E et al. Agency for Healthcare Research and Quality. March AHRQ publication No 04-E")
32
Estudios aleatorizados para el tratamiento de la hipertrigliceridemia con OMEGA-3
Cambio desde basal (%) Ref Población Diseño N Duración (semanas) TG basales (mg/dl) TG C-LDL C-HDL 3 Hiperlipidemia combinada EAC: DC paralelo 57 12 356 -28 Sin datos NS 4 Revascularización miocárdica quirúrgica EAC: 2x2 factorial 610 52 178 -19 +10 5 HTG severa EAC: DC, paralelo 42 16 926 -45 +31 +13 6 40 500-2,000 -26 +14 7 EAC: paralelo 27 > 28 876 -47 8 801 -39 +17 9 Angioplastia coronaria 500 2 antes + 24 después 196 -27 10 Hiperlipidemia familiar combinada EAC: DC, cruzado 14 251 +21 11 Paralelo 1,210 -40 +46 HTG primaria 28 872 -37 +30 +11 13 HTG persistente en tratamiento con simvastatina 59 24 409 -30 EAC: DC cruzado 378 -44 +25 17 HTG persistente en Tto. con simvastatina 254 -29.5 +3.4
 Ref. Población. Diseño. N. Duración (semanas) TG basales (mg/dl) TG. C-LDL. C-HDL. 3. Hiperlipidemia combinada. EAC: DC paralelo Sin datos. NS. 4. Revascularización miocárdica quirúrgica. EAC: 2x2 factorial HTG severa. EAC: DC, paralelo , EAC: paralelo. 27. > Angioplastia coronaria antes + 24 después Hiperlipidemia familiar combinada. EAC: DC, cruzado Paralelo. 1, HTG primaria HTG persistente en tratamiento con simvastatina EAC: DC cruzado HTG persistente en Tto. con simvastatina")
33
Estudios con omega-3 e hipertrigliceridemia
CARACTERISTICAS n +/ DOSIS: 2 a 4 gramos al día. Estudios aleatorizados NUMERO DE ESTUDIOS Hipertrigliceridemia severa 6 Hiperlipidemia combinada 3 Hipertrigliceridemia persistente a pesar de estatinas 2 Combinados con estatinas y fibratos Combinados con Ezetimibe/Simvastatina y Niacina 1 Otros (angioplastia, revascularización) Estudios de efectividad; en general de corta duración (6-8 sem) Reducciones en TG entre el 30 y 40 %; promedio 27.5 % La reducción en TG depende de su valor basal La reducción en el colesterol no-HDL es menor Efecto no significatico en c-HDL; puede elevar el c-LDL % No hay estudios que demuestren efecto sobre eventos clínicos Tomado de Guías Colombianas de Cardiología. 2009;16:1-27
 Estudios de efectividad; en general de corta duración (6-8 sem) Reducciones en TG entre el 30 y 40 %; promedio 27.5 % La reducción en TG depende de su valor basal. La reducción en el colesterol no-HDL es menor. Efecto no significatico en c-HDL; puede elevar el c-LDL % No hay estudios que demuestren efecto sobre eventos clínicos. Tomado de Guías Colombianas de Cardiología. 2009;16:1-27.")
34
Reducción adicional en TG
Asociación estatinas - ácidos omega-3 (aceite de pescado) y efecto sobre trigliceridos Estatina mg/día Omega 3 (EPA+DHA) g/día Reducción adicional en TG Pravastatina 40 3 24 % Simvastatina 20 4 28% Simvastatina 40 35% Atorvastatina 10 2 No cambio Atorvastatina 40 40% No cambio en LDL, HDL-c con la asociación. Segura, tolerada Tomado de Nambi et al. Am J Cardiol 2006;98(suppl):34i
 y efecto sobre trigliceridos. Estatina. mg/día. Omega 3 (EPA+DHA) g/día. Reducción adicional en TG. Pravastatina % Simvastatina % Simvastatina % Atorvastatina No cambio. Atorvastatina % No cambio en LDL, HDL-c con la asociación. Segura, tolerada. Tomado de Nambi et al. Am J Cardiol 2006;98(suppl):34i.")
35
Prevención Secundaria
Posterior a IAM II b (B) Arritmias ventriculares y fibrilaciòn auricular II b (B) Trigliceridos (coadyuvante) II a (B) Fàrmaco OMEGA – 3 (EPA + DHA) Falla Cardiaca II a (A) Prevención primaria II b (C) RESUMEN INDICACIONES OMEGA-3 AL 2010
 Arritmias ventriculares. y fibrilaciòn auricular. II b (B) Trigliceridos. (coadyuvante) II a (B) Fàrmaco. OMEGA – 3. (EPA + DHA) Falla Cardiaca. II a (A) Prevención primaria. II b (C) RESUMEN INDICACIONES OMEGA-3 AL")
36
AHA/ACC Guías para prevención secundaria de enfermedad cardiovascular
Circulation 2006;113: Circulation 2006;113: Utilidad y eficacia menos bien establecida. Puede considerarse

37
Circulation 2007;116:

38
Clase IIb: Utilidad y eficacia menos bien establecida.
Puede ser considerado.

40
Futuros estudios clínicos con aceite de pescado (omega-3) (EPA-DHA)
INCLUSION DOSIS g/d TERMINA Autonomic Balance in Heart Failure ICC 0.8 2006 – Italia Post Cardio Surgery Atrial Fibrilation Puentes A-C. Valvul 1.6 2008 –Italia OPACH Hemodialisis 2006 –Dinamarc T-Wave Alternans Post IM, FEVI baja OMEGA (3800 pacientes) IAM 1 2007-Alemania GISSI-HF (GISSI-V) (7000 pacientes) 1 + Rosuvastati 2008 – Italia ASCEND ( pacientes) DM Asa 2008 – G. Bretaña SU.FOL.OM3 E. Coronaria/ACV 600 Vs B6+B12 Europa ORIGIN ( pacientes) DM, GAA, ITG Glargina USA Tomado de: Jacobson TA. Am J Cardiol 2006;98 (suppl):61i Tavazzi L. Eur J Heart Fail 2004;6:635 Schacky C. Curr Opin Nutr Metab Care 2007;10:129-35
 IAM Alemania. GISSI-HF (GISSI-V) (7000 pacientes) 1 + Rosuvastati – Italia. ASCEND ( pacientes) DM. Asa – G. Bretaña. SU.FOL.OM3. E. Coronaria/ACV. 600 Vs B6+B Europa. ORIGIN ( pacientes) DM, GAA, ITG Glargina USA. Tomado de: Jacobson TA. Am J Cardiol 2006;98 (suppl):61i. Tavazzi L. Eur J Heart Fail 2004;6:635. Schacky C. Curr Opin Nutr Metab Care 2007;10:")
42
INDICACIONES OMEGA-3 Enfermedad Coronaria Arritmias ventriculares
Dr. Fernan Mendoza Carlos Luengas Camilo Arana Edison García Juan M. senior Arritmias ventriculares y fibrilaciòn auricular Dr. Carlos Morillo Mauricio Duque Alberto Negrette Ignacio Malabeth Dislipidemias Dr. Sebastian Velez Adalberto Quintero Alfonso Muñoz Alonso Merchán Fàrmaco OMEGA – 3 (EPA + DHA) Prevención primaria Dr. Gregorio Sanchez Dora I. Molina Rafael Roca Alvaro Fortich Jairo Acuña Falla Cardiaca Dr. Efrain Gómez Solón Navarrete Maria e. Casanova Nicolas Jaramillo INDICACIONES OMEGA-3
 Prevención primaria. Dr. Gregorio Sanchez. Dora I. Molina. Rafael Roca. Alvaro Fortich. Jairo Acuña. Falla Cardiaca. Dr. Efrain Gómez. Solón Navarrete. Maria e. Casanova. Nicolas Jaramillo. INDICACIONES OMEGA-3.")
43
c-LDL en meta (de acuerdo al riesgo)
Objetivo Primario: c-LDL (I A) Objetivo Secundario: col no-HDL (TG) y c-HDL (IIa B en Alto y Muy Alto Riesgo) NCEP-ATPIII (2001 Y 2004) c-LDL en meta (de acuerdo al riesgo) TG < : META > : FIBRATO, NIACINA, ESTATINA, OMEGA-3 : CALCULE no-HDL y así decide TTO c-HDL > 40 en Hombres > 50 en Mujeres
 Objetivo Secundario: col no-HDL (TG) y c-HDL. (IIa B en Alto y Muy Alto Riesgo) NCEP-ATPIII (2001 Y 2004) c-LDL en meta (de acuerdo al riesgo) TG < 150 : META. > 500 : FIBRATO, NIACINA, ESTATINA, OMEGA : CALCULE no-HDL y así decide TTO. c-HDL > 40 en Hombres. > 50 en Mujeres.")
44
c-Total = c-HDL + c-VLDL + c-LDL + c-IDL + c-Lp(a)
Apo A Apo B c-Total = c-HDL + c-VLDL + c-LDL + c-IDL + c-Lp(a) c-LDL, c-IDL, c-Lp(a) = c-LDL c-LDL c-LDL + TG/5 c-LDL + c-VLDL Colesterol no-HDL c-Total - c-HDL META c-LDL/Riesgo + 30 mg/dl Colesterol no-HDL Predice más eventos coronarios que el c-LDL pero menos que apoB/apoA Simultáneamente debe llegarse a la meta del c-LDL y no-HDL Estatinas o combinaciones con: ezetimibe, niacina, fibratos, omega-3 Conclusiones
 c-LDL, c-IDL, c-Lp(a) = c-LDL. c-LDL. c-LDL + TG/5. c-LDL + c-VLDL. Colesterol no-HDL. c-Total - c-HDL. META. c-LDL/Riesgo + 30 mg/dl. Colesterol no-HDL. Predice más eventos coronarios que el c-LDL pero menos que apoB/apoA. Simultáneamente debe llegarse a la meta del c-LDL y no-HDL. Estatinas o combinaciones con: ezetimibe, niacina, fibratos, omega-3. Conclusiones.")
45
Cuál es el c-LDL Optimo. ARIC. Sharret AR et al
Cuál es el c-LDL Optimo ? ARIC. Sharret AR et al. Circulation 2001;104: Ajustado para edad, etnia 12-a seguimiento; N=12,339 Women Men Relative Risk for Incident CHD LDL-C Quintiles mg/dl (median) 95 120 137 156 185 88 113 131 152 187 Muy poco Muy tarde TG (no-HDL) c-HDL F. R. Insuficiente c-LDL
 Muy poco. Muy tarde. TG (no-HDL) c-HDL. F. R. Insuficiente. c-LDL.")
Presentaciones similares




. Panel de expertos en detección, evaluación y tratamiento del colesterol alto.>")









>")




