Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Diferenciando asma de EPOC: Desde la mecánica respiratoria a los mecanismos inflamatorios. Perspectiva fisiopatológica. Juan José Rodríguez Moncalvo Hospital de Rehabilitación Respiratoria María Ferrer. Ciudad Autónoma de Buenos Aires

3
Diferenciando asma de EPOC: perspectiva fisiopatológica
D. Postma et al. Clin Chest Med 35(2014):
:")
4
ASMA EPOC P. Jeffery. Am J Respir Ctrit Care Med 2001;164:S28-S38

6
© 2014 Global Initiative for Chronic Obstructive Lung Disease
Global Strategy for Diagnosis, Management and Prevention of COPD Mechanisms Underlying Airflow Limitation in COPD Small Airways Disease Airway inflammation Airway fibrosis, luminal plugs Increased airway resistance Parenchymal Destruction Loss of alveolar attachments Decrease of elastic recoil AIRFLOW LIMITATION © 2014 Global Initiative for Chronic Obstructive Lung Disease

7
Diferenciando asma de EPOC: perspectiva fisiopatológica
Características fisiológicas de la obstrucción al flujo aéreo Hiperreactividad bronquial Reversibilidad y evolución del cuadro funcional obstructivo Mecánica respiratoria en reposo y en ejercicio Mecanismos limitantes para el intercambio gaseoso Evaluación funcional-bioquímica de la inflamación bronquial

8
Diferenciando asma de EPOC: perspectiva fisiopatológica
Curva flujo/volumen – espirometría BHR- Respuesta broncodilatadora Pletismografía DLco PECP FENO IOS-FOT Compliance

9
Diagnosis of asthma, COPD and asthma-COPD overlap syndrome (ACOS) A joint project of GINA and GOLD
 A joint project of GINA and GOLD")
10
Definitions Asthma COPD Asthma Asthma COPD
Asthma is a heterogeneous disease, usually characterized by chronic airway inflammation. It is defined by the history of respiratory symptoms such as wheeze, shortness of breath, chest tightness and cough that vary over time and in intensity, together with variable expiratory airflow limitation. [GINA 2014] COPD COPD is a common preventable and treatable disease, characterized by persistent airflow limitation that is usually progressive and associated with enhanced chronic inflammatory responses in the airways and the lungs to noxious particles or gases. Exacerbations and comorbidities contribute to the overall severity in individual patients. [GOLD 2014] Asthma Asthma is a heterogeneous disease, usually characterized by chronic airway inflammation. It is defined by the history of respiratory symptoms such as wheeze, shortness of breath, chest tightness and cough that vary over time and in intensity, together with variable expiratory airflow limitation. [GINA 2014] Asthma Asthma is a heterogeneous disease, usually characterized by chronic airway inflammation. It is defined by the history of respiratory symptoms such as wheeze, shortness of breath, chest tightness and cough that vary over time and in intensity, together with variable expiratory airflow limitation. [GINA 2014] COPD COPD is a common preventable and treatable disease, characterized by persistent airflow limitation that is usually progressive and associated with enhanced chronic inflammatory responses in the airways and the lungs to noxious particles or gases. Exacerbations and comorbidities contribute to the overall severity in individual patients. [GOLD 2014] Asthma-COPD overlap syndrome (ACOS) [a description] Asthma-COPD overlap syndrome (ACOS) is characterized by persistent airflow limitation with several features usually associated with asthma and several features usually associated with COPD. ACOS is therefore identified by the features that it shares with both asthma and COPD. GINA 2014, Box 5-1
 [a description] Asthma-COPD overlap syndrome (ACOS) is characterized by persistent airflow limitation with several features usually associated with asthma and several features usually associated with COPD. ACOS is therefore identified by the features that it shares with both asthma and COPD. GINA 2014, Box 5-1.")
11
Step 3 - Spirometry Essential if chronic airways disease is suspected
Confirms chronic airflow limitation More limited value in distinguishing between asthma with fixed airflow limitation, COPD and ACOS Measure at the initial visit or subsequent visit If possible measure before and after a trial of treatment Medications taken before testing may influence results Peak expiratory flow (PEF) Not a substitute for spirometry Normal PEF does not rule out asthma or COPD Repeated measurement may confirm excessive variability, found in asthma or in some patients with ACOS GINA 2014, Box 5-3
 Not a substitute for spirometry. Normal PEF does not rule out asthma or COPD. Repeated measurement may confirm excessive variability, found in asthma or in some patients with ACOS. GINA 2014, Box 5-3.")
12
Diferenciando asma de EPOC: perspectiva fisiopatológica
M. Mishima. Allergol Int. 2009;58:

13
Step 3 - Spirometry Spirometric variable Asthma COPD ACOS Normal FEV
1 /FVC pre - or post BD Compatible with asthma Not compatible with diagnosis (GOLD) Not compatible unless other evidence of chronic airflow limitation FEV =80% predicted (good control, or interval between symptoms) C ompatible with GOLD category A or B if post /FVC <0.7 Compatible with mild Post BD increase in >12% and 400mL from baseline High probability of asthma Unusual in COPD. Consider ACOS Compatible with diagnosis of ACOS Indicates airflow limitation; may improve Required for diagnosis by GOLD criteria Usual in ACOS >12% and 200mL from baseline (reversible airflow limitation) Usual at some time in course of asthma; not always present Common in COPD and more likely when FEV is low, but consider ACOS Common in ACOS, and low <80% predicted Compatible with asthma. A risk factor for exacerbations Indicates severity of airflow limitation and risk of exacerbations and mortality GINA 2014, Box 5-3
 Not compatible unless. other evidence of chronic. airflow limitation. FEV. =80% predicted. (good control, or interval. between symptoms) C. ompatible with GOLD. category A or B if post. /FVC <0.7. Compatible with mild. Post. BD increase in. >12% and 400mL. from baseline. High probability of asthma. Unusual in COPD. Consider ACOS. Compatible with. diagnosis of ACOS. Indicates. airflow. limitation; may improve. Required for diagnosis. by GOLD. criteria. Usual in ACOS. >12% and 200mL. from baseline (reversible. airflow limitation) Usual at some time in. course. of asthma; not. always present. Common in COPD and. more likely when FEV. is. low, but consider ACOS. Common in ACOS, and. low. <80% predicted. Compatible with asthma. A risk factor for. exacerbations. Indicates severity of. airflow limitation and risk. of exacerbations and. mortality. GINA 2014, Box 5-3.")
14
Diferenciando asma de EPOC: perspectiva fisiopatológica
M. Mishima. Allergol Int. 2009;58:

15
Curva F/V ASMA Curva F/V EPOC Pre BD Post BD Flujo (L/S) Flujo (L/S)
 Flujo (L/S)")
16
Diferenciando asma de EPOC: perspectiva fisiopatológica

17
Respuesta broncodilatadora en EPOC
Población: 52 pacientes (33 hombres); 59,2 ± 8,7 años (X±DS) Tabaquismo: 46 ± 33 paquetes/año FVC: 67 ± 17 % teórico FEV1: 40,4 ± 17 % teórico %FEV1/FVC: 46 ± 12 TLC ≥ 120% del teórico: 31% de los casos RV ≥ 130% del teórico: 65% de los casos Estadio GOLD 1. LEVE: 4% 2. MODERADO: 42% 3. SEVERO: 37% 4. MUY SEVERO: 17% Rodríguez Moncalvo y cols. Hospital María Ferrer.
; 59,2 ± 8,7 años (X±DS) Tabaquismo: 46 ± 33 paquetes/año. FVC: 67 ± 17 % teórico. FEV1: 40,4 ± 17 % teórico. %FEV1/FVC: 46 ± 12. TLC ≥ 120% del teórico: 31% de los casos. RV ≥ 130% del teórico: 65% de los casos. Estadio GOLD. 1. LEVE: 4% 2. MODERADO: 42% 3. SEVERO: 37% 4. MUY SEVERO: 17% Rodríguez Moncalvo y cols. Hospital María Ferrer.")
18
Respuesta broncodilatadora en EPOC
Rodríguez Moncalvo y cols. Hospital María Ferrer.

20
EPOC: Atrapamiento aéreo e hiperinsuflación
O´Donell D. Chest 2000;117:42S-47S Shuterland E. N Engl J Med 2004;350:

22
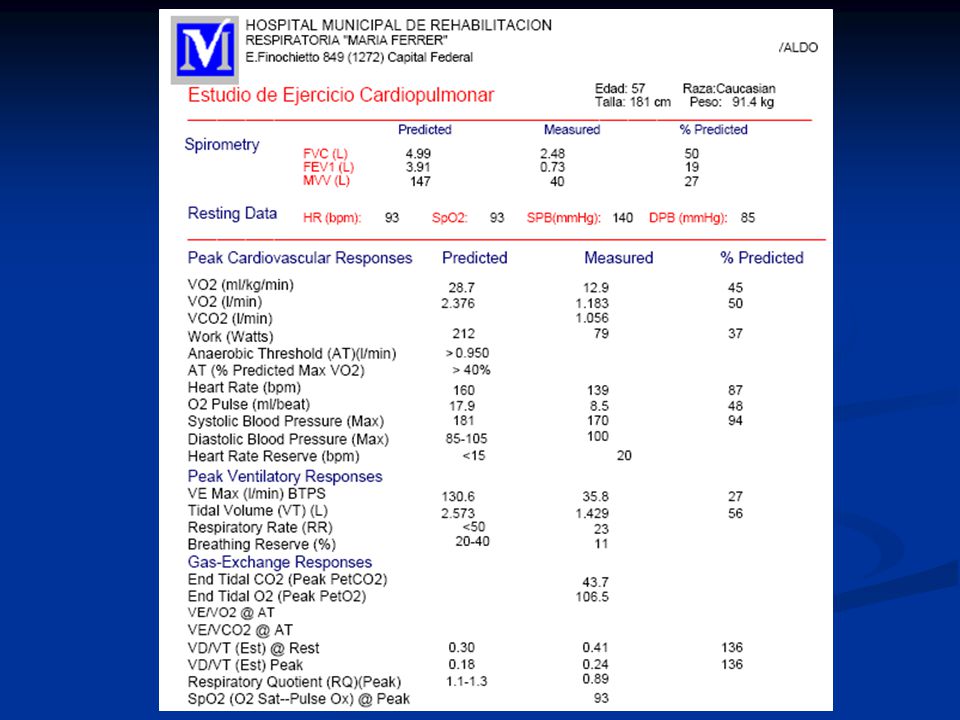
P.C. EPOC. 12/05/04

25
Diferenciando asma de EPOC:
oscilación forzada y oscilometría de impulso

27
Diferenciando asma de EPOC: oscilometría de impulso

28
Diferenciando asma de EPOC: oscilometría de impulso
M. Mishima. Allergol Int. 2009;58:

34
J.,Donohue et. al.

35
Diferenciando asma de EPOC: perspectiva fisiopatológica
Espirometría, curva F/V, respuesta BD y manifestaciones de HRB, son útiles para diferenciar las características de la obstrucción al flujo aéreo en asma y EPOC La mecánica respiratoria pletismográfica y en ejercicio puede aportar datos orientadores respecto de los mecanismos fisiopatológicos involucrados en la obstrucción crónica al flujo aéreo DLco debe ser examinada en contexto con otros datos clínicos y funcionales debido a su limitada especificidad La evaluación funcional-celular-bioquímica incluyendo FENO puede ser útil para estudiar y diferenciar los mecanismos obstructivos de origen inflamatorio a nivel bronquial

36
Muchas gracias

37
Step 5 – Refer for specialized investigations if needed
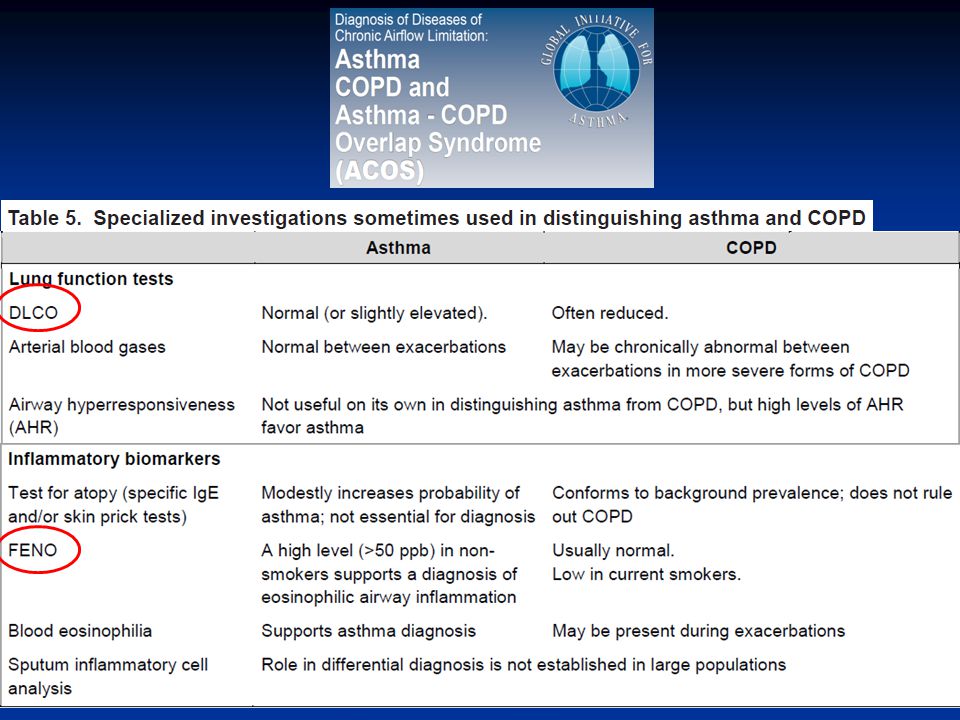
Asthma COPD DLCO Normal or slightly elevated Often reduced Arterial blood gases Normal between exacerbations In severe COPD, may be abnormal between exacerbations Airway hyperresponsiveness Not useful on its own in distinguishing asthma and COPD. High levels favor asthma High resolution CT scan Usually normal; may show air trapping and increased airway wall thickness Air trapping or emphysema; may show bronchial wall thickening and features of pulmonary hypertension Tests for atopy (sIgE and/or skin prick tests) Not essential for diagnosis; increases probability of asthma Conforms to background prevalence; does not rule out COPD FENO If high (>50ppb) supports eosinophilic inflammation Usually normal. Low in current smokers Blood eosinophilia Supports asthma diagnosis May be found during exacerbations Sputum inflammatory cell analysis Role in differential diagnosis not established in large populations GINA 2014, Box 5-5
 Not essential for diagnosis; increases probability of asthma. Conforms to background prevalence; does not rule out COPD. FENO. If high (>50ppb) supports eosinophilic inflammation. Usually normal. Low in current smokers. Blood eosinophilia. Supports asthma diagnosis. May be found during exacerbations. Sputum inflammatory cell analysis. Role in differential diagnosis not established in large populations. GINA 2014, Box 5-5.")
40
Respuesta broncodilatadora en EPOC
Δ % FVC 0,49 21,7 % FEV1 0,25 22,4 % VC 0,45 17 % IC 0,33 18,5 % TLC - 0,20 - 2,98 % RV - 0,65 - 16,5 % FRC - 0,52 - 11,07 % Rodríguez Moncalvo y cols. Hospital María Ferrer.

Presentaciones similares




















 Knowledge Management tools Knowledge management tools.>")








