Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Manejo del Paciente Hospitalizado Dra. Elizabeth Valinotti
Diabetes Mellitus Manejo del Paciente Hospitalizado Dra. Elizabeth Valinotti

8
El tratamiento de la diabetes en el hospital general, habitualmente se considera de importancia secundaria en comparación con la condición que origina la admisión hospitalaria.

9
Recientes estudios han centrado la atención sobre la posibilidad que la hiperglucemia en el hospital no es necesariamente una condición benigna y que tratamiento agresivo de la diabetes y la hiperglucemia resulta en la reducción de la mortalidad y la morbilidad. Umpierrez GE, Isaacs SD, Bazargan N, You X, Thaler LM, Kitabchi AE: Hyperglycemia: an independent marker of inhospital mortality in patients with undiagnosed diabetes. J Clin Endocrinol Metab 87:978–982, 2002 Van den Berghe G, Wouters P, Weekers F, VerWaest C, Bruyninckx F, Schetz M, Vlasselaers D, Ferdinande P, Lauwers P, Bouillon R: Intensive insulin therapy in critically ill patients. N Engl J Med 345:1359–1367, 2001

10
Cuál es la prevalencia de la Diabetes en pacientes hospitalizados?

11
Una encuesta reciente calcula que el 22% de los pacientes hospitalizados por día son diabéticos.
American Diabetes Association. Economic costs of diabetes in the U.S. in 2007. Diabetes Care 2008;31:596–615

12
Umpierrez et al. informó un 26% la prevalencia de diabetes conocida en pacientes hospitalizados en un hospital docente. 12% de los pacientes presentaron hiperglucemias durante su internación sin ser conocidos diabeticos. Umpierrez GE, Isaacs SD, Bazargan N, You X, Thaler LM, Kitabchi AE: Hyperglycemia: an independent marker of inhospital mortality in patients with undiagnosed diabetes. J Clin Endocrinol Metab 87:978–982, 2002

13
Norhammar et al. (7) estudió 181 pacientes con infarto agudo de miocardio (IAM), consecutivos ingresados la unidad coronaria de dos hospitales en Suecia. Pacientes sin diagnóstico de diabetes, y una de glucosa en la sangre de 200 mg / dl al ingreso. Una prueba de tolerancia a la glucosa standard se realizó al alta y otra vez 3 meses después. Los autores encontraron un 31% la prevalencia de la diabetes en el momento del alta hospitalaria y un 25% de prevalencia de diabetes 3 meses después del alta, en este grupo sin previo diagnóstico de la diabetes. Norhammar A, Tenerz A, Nilsson G, Hamsten A, Efendic S, Ryden L, Malmberg K: Glucose metabolism in patients with acute myocardial infarction and no previous diagnosis of diabetes mellitus: a prospective study. Lancet 359:2140– 2144, 2002

14
La atención hospitalaria representa la mitad de los 174 mil millones de dólares que EE.UU. gasta en cuidados médicos para pacintes con diabetes. American Diabetes Association. Economic costs of diabetes in the U.S. in 2007. Diabetes Care 2008;31:596–615

15
¿Cúal es el enlace entre la hiperglucemia y las complicaciones hospitalarias?

16
Hiperglucemia y sistema inmune
El principal problema ha sido identificado como disfunción fagocitaria de los leucocitos. Diversos estudios han informado de los defectos en la funcionalidad de los neutrófilos y monocitos en presencia de hiperglucemia, como por ejemplo, la adherencia, quimiotaxis, fagocitosis, muerte bacteriana, respiratorias y de ruptura. McManus L, Bloodworth R, Prihoda T, Blodgett J, Pinckard R: Agonist-dependent failure of neutrophil function in diabetes correlates with extent of hyperglycemia.J Leukocyte Biol 70:395–404, 2001

17
Hiperglucemia y sistema inmune
Se ha demostrado una mejora significativa en la adhesión de los granulocitos cuando la glucosa en sangre en ayunas se redujo de 293 ± 20 a 198 ± 29 mg / dl. Bagdade JD, Stewart M, Walters E: Impaired granulocyte adherence. A reversible defect in host defense in patients with poorly controlled diabetes. Diabetes 27:677–681, 1978

18
Hiperglucemia y sistema inmune
Las complicaciones microvasculares clásicas de la diabetes son causadas por alteraciones en la vía de las aldosa reductasa aldose, vía de las especies reactivas de oxígeno, y la víade la proteína C quinasa (PKC). Varias de estas vías puede contribuir a la disfunción inmune. Sheetz M, King G: Molecular understanding of hyperglycemia’s adverse effects for diabetic complications. JAMA 288:2579–2588, 2002
. Varias de estas vías puede contribuir a la disfunción inmune. Sheetz M, King G: Molecular understanding. of hyperglycemia’s adverse effects. for diabetic complications. JAMA. 288:2579–2588,")
19
Hiperglucemia y sistema cardiovascular
La Hiperglucemia aguda tiene numerosos efectos sobre el sistema cardiovascular. Hiperglucemia perjudica una precondición isquémica. El tamaño del infarto de miocardio aumenta en presencia de hiperglucemia. El flujo de las colaterales coronarias disminuye en presencia de hiperglucemia grave. La hiperglucemia aguda puede inducir apoptosis miocitos cardiacos. Ceriello A, Quagliaro L, D’Amico M, Di Filippo C, Marfella R, Nappo F, Berrino L, Rossi F, Giugliano D: Acute hyperglycemia induces nitrotyrosine formation and apoptosis in perfused heart from rat. Diabetes 51:1076–1082, 2002 Kersten J, Toller W, Tessmer J, Pagel P, Warltier D: Hyperglycemia reduces coronary collarteral blood flow through a nitric oxide-mediated mechanism. Am J Physiol 281:H2097–H2104, 2001

20
Hiperglucemia y sistema cardiovascular
Otras consecuencias vasculares de la hiperglucemia aguda hospitalaria son: cambios de la presión arterial, elevaciones de catecolaminas, las anomalías de la función plaquetaria Cambios electrolíticos

21
Hiperglucemia y trombosis
Estudios pacientes con diabetes tipo 2 han demostrado la hiperactividad plaquetaria que se demuestra por el aumento de la biosíntesis de tromboxano. Biosíntesis de tromboxano disminuye con la reducción en la sangre glucosa. Hiperglucemia induce elevaciones de la interleuquina (IL) -6, niveles elevados de la misma han sido vinculado a las altas concentraciones de fibrinógeno plasmático. Davi G, Catalano I, Averna M, Notarbartolo A, Strano A, Ciabattoni G, Patrono C: Thromboxane biosynthesis and platelet function in type II diabetes mellitus. N Engl J Med 322:1769–1774, 1990 Morohoshi M, Fujisawa K, Uchimura I, Numano F: Glucose-dependent interleukin 6 and tumor necrosis factor production by human peripheral blood monocytes in vitro. Diabetes 45:954– 959, 1996
 -6, niveles elevados de la misma han sido vinculado a las altas concentraciones de fibrinógeno plasmático. Davi G, Catalano I, Averna M, Notarbartolo. A, Strano A, Ciabattoni G, Patrono. C: Thromboxane biosynthesis and platelet. function in type II diabetes mellitus. N Engl J Med 322:1769–1774, Morohoshi M, Fujisawa K, Uchimura I, Numano F: Glucose-dependent interleukin. 6 and tumor necrosis factor production. by human peripheral blood. monocytes in vitro. Diabetes 45:954– 959,")
22
Hiperglucemia y trombosis
La Hiperglucemia también causa: aumento de las concentraciones plasmáticas del factor y el antígeno de von Willebrand 11 -- dehidro-tromboxano B2 (una medida de la producción de tromboxano A2). Estos los cambios no fueron vistos en el estado euglucemico.
. Estos los cambios no fueron vistos en el estado euglucemico.")
23
Hiperglucemia e Inflamación
En humanos, la elevación moderada de la glucosa a 270 mg/dl (15 mmol/l) ha sido asociada con un incremento marcado de IL-6, IL-18, and TNF. Esposito K, Nappo F, Marfella R, Giugliano G, Giugliano F, Ciotola M, Quagliaro L, Ceriello A, Giugliano D: Inflammatory cytokine concentrations are acutely increased by hyperglycemia in humans: role of oxidative stress. Circulation 106:2067–2072, 2002
 ha sido asociada con un incremento marcado de IL-6, IL-18, and TNF. Esposito K, Nappo F, Marfella R, Giugliano. G, Giugliano F, Ciotola M, Quagliaro. L, Ceriello A, Giugliano D: Inflammatory. cytokine concentrations are. acutely increased by hyperglycemia in. humans: role of oxidative stress. Circulation. 106:2067–2072,")
24
Hiperglucemia e Inflamación
En humanos, los niveles de TNF están elevados en el IAM y se correlacionan con la disfunción cardiaca. TNF tambien está relacionado con el daño que ocurre en la isquemia renal y en la insuficiencia carcdiaca congestiva. IL-18 ha sida propuesta como un desestabilizador de las placas ateroscleroticas, llevando a los sindromes isquemicos agudos. Meldrum DR, Dinarello CA, Shames BD, Cleveland JC, Jr., Cain BS, Banerjee A, Meng X, Harken AH: Ischemic preconditioning decreases postischemic myocardial tumor necrosis factor-alpha production: potential ultimate effector mechanism of preconditioning. Circulation 98:II214–II218; discussion II218– II219, 1998

25
Hiperglucemia y disfunción endotelial
En un estado saludable, el endotelio vascular mantiene a la vasculatera en un estado quiescente, relajado, antitrombótico, antioxidante y antiadhesivo. Marfella R, Quagliaro L, Nappo F, Ceriello A, Giugliano D: Acute hyperglycemia induces an oxidative stress in healthy subjects. J Clin Invest 108:635– 636, 2001

26
Hiperglucemia y disfunción endotelial
En estudios in vivo en Humanos utilizando estos parametros confirman que la hiperglucemia aguda en niveles comumente observados en los hospitales (142–300 mg/dl) causan disfunción endotelial. Beckman J, Goldfine A, Gordon M, Creager M: Ascorbate restores endothelium- dependent vasodilation impaired by acute hyperglycemia in humans. Circulation 103:1618–1623, 2001
 causan disfunción endotelial. Beckman J, Goldfine A, Gordon M, Creager M: Ascorbate restores endothelium- dependent vasodilation impaired. by acute hyperglycemia in humans. Circulation. 103:1618–1623,")
27
Hiperglucemia y disfunción endotelial
La hiperglucemia puede afectar directamente la función celular endotelial mediante la inactivación química del óxido nítrico. Otros mecanismos incluyen la activación de la producción de especias reactivas de oxigeno (ROS). Brodsky SV, Morrishow AM, Dharia N, Gross SS, Goligorsky MS: Glucose scavenging of nitric oxide. Am J Physiol Renal Physiol 280:F480–F486, 2001
. Brodsky SV, Morrishow AM, Dharia N, Gross SS, Goligorsky MS: Glucose scavenging. of nitric oxide. Am J Physiol Renal. Physiol 280:F480–F486,")
28
Hiperglucemia y cerebro
En Humanos, Parsons et al. ha demostrado que la relación lactato colina (ratio) determinada por RM por espectroscopia de protones tiene valor prediciendo los resultados clínicos y el tamaño final de un infato agudo (stroke). Tambien se ha demostrado que existe correlación positiva entre la elevación de la glucemia y la producción de lactato. A traves de este mecanismo parece que la hiperglucemia cause un riesgo de hipoperfusión en el tejido y una progresión del infarto. Parsons M, Barber P, Desmond P, Baird T, Darby D, Byrnes G, Tress B, Davis S: Acute hyperglycemia adversely affects stroke outcome: a magnetic resonance imaging and spectroscopy study. Ann Neurol 52:20–28, 2002 Parsons MW, Li T, Barber PA, Yang Q, Darby DG, Desmond PM, Gerraty RP, Tress BM, Davis SM: Combined (1)H MR spectroscopy and diffusion-weighted MRI improves the prediction of stroke outcome. Neurology 55:498–505, 2000
 determinada por RM por espectroscopia de protones tiene valor prediciendo los resultados clínicos y el tamaño final de un infato agudo (stroke). Tambien se ha demostrado que existe correlación positiva entre la elevación de la glucemia y la producción de lactato. A traves de este mecanismo parece que la hiperglucemia cause un riesgo de hipoperfusión en el tejido y una progresión del infarto. Parsons M, Barber P, Desmond P, Baird. T, Darby D, Byrnes G, Tress B, Davis S: Acute hyperglycemia adversely affects. stroke outcome: a magnetic resonance. imaging and spectroscopy study. Ann. Neurol 52:20–28, Parsons MW, Li T, Barber PA, Yang Q, Darby DG, Desmond PM, Gerraty RP, Tress BM, Davis SM: Combined (1)H MR. spectroscopy and diffusion-weighted. MRI improves the prediction of stroke. outcome. Neurology 55:498–505,")
29
Potential relationships between metabolic stress, hyperglycemia, hypoinsulinemia, and poor hospital outcomes

30
RECOMMENDATIONS

31
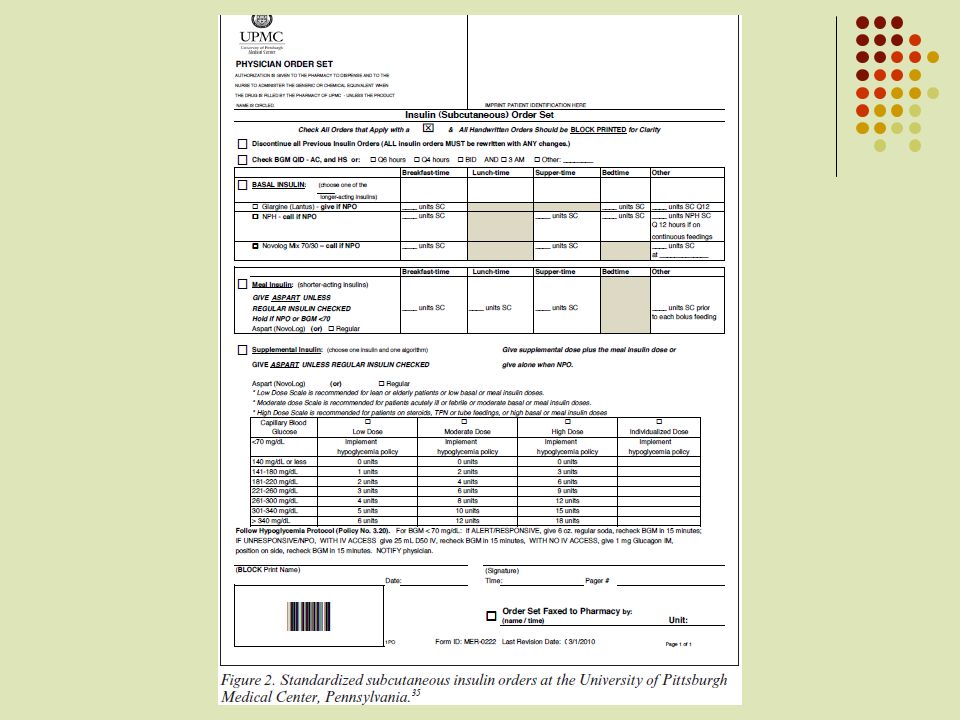
SSI A topic that deserves particular attention is the persistent overuse of what has been branded as sliding scale insulin (SSI) for management of hyperglycemia. The term “correction insulin,” which refers to the use of additional short- or rapidactinginsulin in conjunction with scheduled insulin doses to treat BG levels above desired targets, is preferred . Prolonged therapy with SSI as the sole regimen is ineffective in the majority of patients (and potentially dangerous in those with type 1 diabetes). Umpierrez GE, Smiley D, Zisman A, et al. Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes (RABBIT 2 trial). Diabetes Care 2007;30: 2181–2186 Umpierrez GE, Palacio A, Smiley D. Sliding scale insulin use: myth or insanity? Am J Med 2007;120:563–567
 for management of hyperglycemia. The term correction insulin, which refers to the use of additional short- or rapidactinginsulin in conjunction with scheduled insulin doses to treat BG levels above desired targets, is preferred . Prolonged therapy with SSI as the sole regimen is ineffective in the majority of patients (and potentially dangerous in those with type 1 diabetes). Umpierrez GE, Smiley D, Zisman A, et. al. Randomized study of basal-bolus insulin. therapy in the inpatient management. of patients with type 2 diabetes. (RABBIT 2 trial). Diabetes Care 2007;30: 2181–2186. Umpierrez GE, Palacio A, Smiley D. Sliding scale insulin use: myth or insanity Am J Med 2007;120:563–567.")
32
Critically ill patients
Insulin therapy should be initiated for treatment of persistent hyperglycemia, starting at a threshold of no greater than180 mg/dl. Once insulin therapy has been started,a glucose range of 140 –180 mg/dl is recommended for the majority of critically ill patients.

33
Critically ill patients
Intravenous insulin infusions are thepreferred method for achieving and maintaining glycemic control in critically ill patients. Validated insulin infusion protocols with demonstrated safety and efficacy, and with low rates of occurrence of hypoglycemia, are recommended. With IV insulin therapy, frequent glucose monitoring is essential to minimize the occurrence of hypoglycemia and to achieve optimal glucose control.

34
Noncritically ill patients
For the majority of noncritically ill patients treated with insulin, the premeal BG target should generally be 140 mg/dl in conjunction with random BG values 180 mg/dl, provided these targets can be safely achieved. More stringent targets may be appropriate in stable patients with previous tight glycemic control. Less stringent targets may be appropriate in terminally ill patients or in patients with severe comorbidities.

35
Scheduled subcutaneous administration of insulin, with basal, nutritional, and correction components, is the preferred method for achieving and maintaining glucos control. Prolonged therapy with SSI as the sole regimen is discouraged. Noninsulin antihyperglycemic agents are not appropriate in most hospitalized patients who require therapy for hyperglycemia.

36
Safety issues Overtreatment and undertreatment of hyperglycemia represent major safety concerns. Education of hospital personnel is essential in engaging the support of those involved in the care of inpatients with hyperglycemia. Caution is required in interpreting results of POC glucose meters in patients with anemia, polycythemia, hypoperfusion, or use of some medications. Buy-in and financial support from hospital administration are required for promoting a rational systems approach to inpatient glycemic management

37
Discharge planning Preparation for transition to the outpatient setting should begin at the time of hospital admission. Discharge planning, patient education, and clear communication with outpatient providers are critical for ensuring a safe and successful transition to outpatient`glycemic management.

39
The importance of glycemic control onoutco me is not limited to patients in critical care areas but also applies to patients admitted to general surgical and medical wards. In such patients, the presence of hyperglycemia has been associated with prolonged hospital stay, infection, disability after hospital discharge, and death

40
In general surgery patients, the relative risk for serious postoperative infections (sepsis, pneumonia, and wound infection) increased 5.7-fold when any postoperative day 1 blood glucose was 220 mg/dl Goldberg PA, Siegel MD, Sherwin RS, Halickman JI, Lee M, Bailey VA, Lee SL, Dziura JD, Inzucchi SE: Implementation of a safe and effective insulin infusion protocol in a medical intensive care unit. Diabetes Care 27:461– 467, 2004

41
OBJECTIVE Study the optimal management of hyperglycemia in non– intensive care unit patients with type 2 diabetes, as few studies thus far have focused on the subject.

42
RESEARCH DESIGN AND METHODS
a prospective, multicenter, randomized trial to compare the efficacy and safety of a basal-bolus insulin regimen with that of sliding-scale regular insulin (SSI) in patients with type 2 diabetes.
 in patients with type 2 diabetes.")
43
RESEARCH DESIGN AND METHODS

44
RESEARCH DESIGN AND METHODS

45
RESEARCH DESIGN AND METHODS

46
RESEARCH DESIGN AND METHODS
The primary end point was to determine differences in glycemic control between treatment groups as measured by the mean daily blood glucose concentration. Secondary outcomes include differences between treatment groups in number of hypoglycemic events, number of episodes of severe hyperglycemia, length of hospital stay, and mortality rate.

47
Results

48
Results The most common admitting illnesses included a variety of cardiovascular (40%), infectious (20%), pulmonary (18%), renal (4%), and gastrointestinal (12%) disorders.
, infectious (20%), pulmonary (18%), renal (4%), and gastrointestinal (12%) disorders.")
49
Results The mean hospital length of stay was 5.3 ± 6 days in patients treated with basal-bolus and 5.1± 4 days in the SSItreated group (P NS)
")
50
Results Only one death was reported in a patient in the basalbolus treatment group who was admitted with shortness of breath and later developed respiratory failure secondary to a pulmonary embolism.

51
Results

52
Results The mean admission blood glucose for study patients was 227 ± 65 mg/dl and the mean A1C 8.8 ± 2%.

53
Results The percentage of patients within the mean glucose target (140 mg/dl) was 66% in patients treated with glargine and glulisine versus 38% in those treated with SSI
 was 66% in patients treated with glargine and glulisine versus 38% in those treated with SSI.")
54
Results Nine (14%) patients treated with SSI remained with blood glucose 240 mg/dl despite increasing the SSI dose to the maximal or insulin-resistant scale. Glycemic control rapidly improved in all of the SSI failure subjects after they were switched to the basal-bolus insulin regimen.
 patients treated with SSI remained with blood glucose 240 mg/dl despite increasing the SSI dose to the maximal or insulin-resistant scale. Glycemic control rapidly improved in all of the SSI failure subjects after they were switched to the basal-bolus insulin regimen.")
55
Results The meandaily dose of insulin glargine was
22 ±2units, and the daily dose of insulin glulisine was 20± 1 units. A total of 26 patients had the lantus dose adjusted, and 44 patients required supplemental glulisine insulin during the hospital stay. Patients treated with SSI received a mean daily dose of units regular insulin/ day, with approximately one-half of patients receiving 10 units/day.

56
Results Hypoglycemia (defined as blood glucose 60 mg/dl) occurred in two patients in each treatment group.
 occurred in two patients in each treatment group.")
57
Conclusions We observed that treatment with insulin glargine and glulisine results in a significant improvement in glycemic control compared with that resulting from the sole use of SSI. The mean daily glucose difference between groups ranged from 23 to 58 mg/dl during days 2–6 of therapy.

58
Conclusions Differences in glycemic control between treatment groups can be explained by the fact that an SSI regimen treats hyperglycemia after it has already occurred instead of preventing the occurrence of hyperglycemia.

60
objetivo Studies comparing the use of basal bolus with insulin analogs vs. split-mixed regimens with human insulins in hospitalized patients with type 2 diabetes are lacking.

61
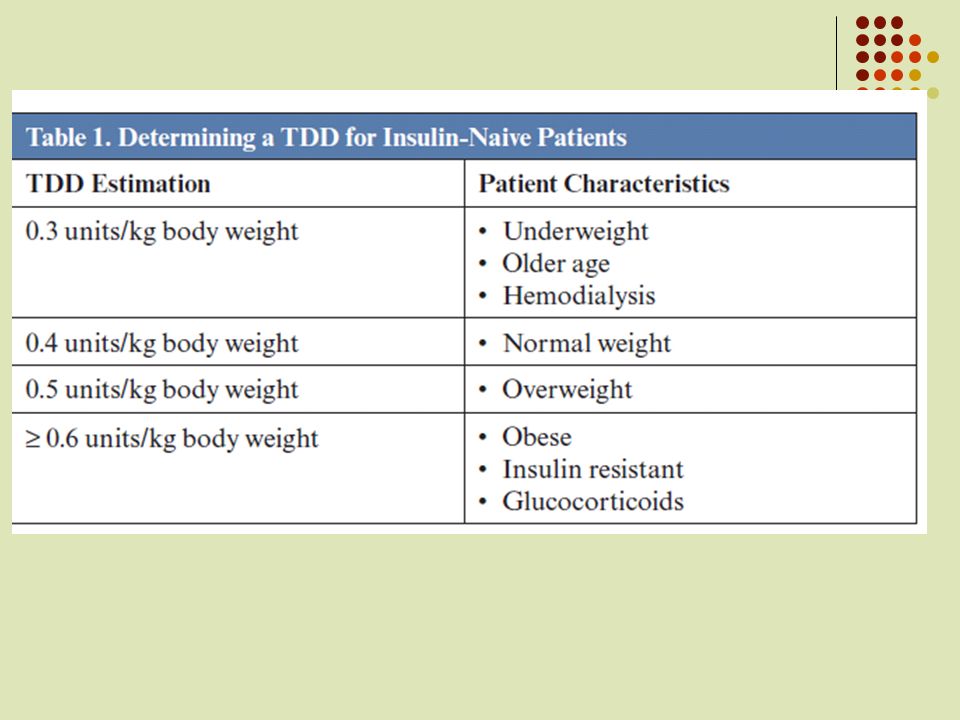
a controlled multicenter trial, we randomized 130 nonsurgical patients with blood glucose (BG) between 140 and 400 mg/dl to receive detemir once daily and aspart before meals (n 67) or neutral protamine Hagedorn (NPH) and regular insulin twice daily (n 63). Insulin dose was started at 0.4 U/kg d for BG between 140 and 200 mg/dl or 0.5 U/kg d for BG mg/dl.

62
Insulin treatment protocols

63
Insulin treatment protocols

64
Insulin treatment protocols

65
The goal of insulin therapy was to maintain premeal and bedtime BG levels lower than 140 mg/dl while avoiding hypoglycemia.

66
The primary outcome of the study was to determine differences in glycemic control between treatment groups as measured by mean daily BG concentration during the hospital stay. Secondary outcomes include differences between treatment groups in premeal and bedtime glucose levels, number of hypoglycemic events, length of hospital stay, and mortality rate.

67
Results A total of 130 subjects with type 2 diabetes were recruited. After randomization, 67 patients received insulin detemir once daily and insulin aspart before meals, and 63 patients received splitmixed regimen with NPH and regular insulin twice daily.

68
Results

69
Results Admitting illnesses included a variety of cardiovascular (35%), infectious (15%), pulmonary (12%), and gastrointestinal (14%) conditions. The mean hospital length of stay was d in patients treated with detemir plus aspart and d in the NPHplus regular group Pnot significant (NS). There was no mortality reported in this trial.
. There was no mortality reported in this trial.")
70
Results The mean admission glucose levels in the detemir/aspart and NPH/regular insulin treatment groups were 230±102 and 231±145 mg/dl, respectively (P: NS).
.")
71
Results

72
Results Nineteen patients (28.4%) in the detemir/aspart group had a BGbetween 40 and 59 mg/dl, and three patients (4.5%) had a BG below 40 mg/dl. Fifteen patients in the NPH/regular group (23.8%) had a BG of 40–59 mg/dl, and one patient (1.6%) hada BG below 40 mg/dl (P0.20 vs. detemir/aspart group).
 had a BG of 40–59 mg/dl, and one patient (1.6%) hada BG below 40 mg/dl (P0.20 vs. detemir/aspart group).")
73
Discussion BG target below 140 mg/dl before meals was achieved in less than half of patients in both treatment regimens, and approximately 30% of patients experienced one or more episodes of hypoglycemia during the hospital stay. These results indicate that the basal/bolus regimen with detemir once daily and aspart before meals results in equivalent glycemic control with no significant differences in the frequency of hypoglycemia compared with a twice daily split-mixed human insulin regimen with NPH and regular insulin in patients with type 2 diabetes.

74
Discussion The American Diabetes Association recently recommended a level below 70 mg/dl to define hypoglycemia.Using this definition, we observed that 24 patients (38%) in the NPH/regular insulin group and 29 patients (43%) in the detemir/aspart group had at least one episode of hypoglycemia (P 0.67) during the hospital stay.
 in the NPH/regular insulin group and 29 patients (43%) in the detemir/aspart group had at least one episode of hypoglycemia (P 0.67) during the hospital stay.")
75
Discussion A BGtarget below 140 mg/dl was achieved in 66%of patients in the glargine plus glulisine group and 38% in the sliding-scale group. Only two patients (3%) in the glargine/glulisine group and in the sliding-scale regimen developed a BG below 60 mg/dl, and no patients had a BG below 40 mg/dl during the hospital stay.
 in the glargine/glulisine group and in the sliding-scale regimen developed a BG below 60 mg/dl, and no patients had a BG below 40 mg/dl during the hospital stay.")
76
Discussion In this study, the frequency of hypoglycemiawith detemir/aspart and NPH/regular insulin was higher than that reported with the use of glargineandglulisine in the Rabbit-2 trial.

77
Discussion In this study, less than half of patients in either treatment group achieved a target BG below 140 mg/dl before meals.

78
Discussion The relatively low rate of BG readings within target could be the result of a relatively high rate of hypoglycemic events, or in the case of detemir because the algorithm did not include an option for twice daily dosing of insulin detemir. Based on the reported pharmacodynamic profile of detemir (about 16-h duration, and a peak from 4–8 h), the use of detemir twice daily may have facilitated a more rapid insulin dose titration resulting in further improvements in glycemic control.
, the use of detemir twice daily may have facilitated a more rapid insulin dose titration resulting in further improvements in glycemic control.")
80
IDENTIFICACIÓN CLARA DE LOS PACIENTES CON DIABETES

81
CONTROL DE GLUCEMIA A TODOS LOS PACIENTES QUE INGRESAN AL HOSPITAL

82
Glucemia ≥ 140 mg/dl sin historia de Diabetes, MONITORIZAR POR 24 A 48 HS Y TRATAR SI FUERA NECESARIO

83
Si es ≥ requiere seguir con los controles e instaurar terapeútica
Paciente con CORTICOIDES U OCTREOTIDE, NUTRICIÓN ENTERAL O PARENTERAL , deben ser monitorizados por 24 a 48 hs despues el inicio del tto. Si es ≥ requiere seguir con los controles e instaurar terapeútica

84
Pacientes con DM o hiperglucemia (mayor ≥

86
GLUCEMIA CAPILAR COMO GUÍA DEL MANEJO INDIVIDUAL DE LOS PACIENTES

87
GLUCOMETROS QUE SEAN CONFIABLES

88
CONTROLES DE GLUCEMIA CAPILAR PRE PRANDIALES Y ANTES DE DORMIR EN LOS QUE SE ALIMENTAN.
CONTROLES DE GLUCEMIA EN PCTES QUE NO SE ALIMENTEN CONTROLES DE GLUCEMIA CAPILAR CADA 4-6 HS

90
PACINTES NO CRÍTICOS HOSPITALIZADOS
OBJETIVO PRE PRANDIAL: < 140 mg/dl AL AZAR: < 180 mg/dl PACINTES NO CRÍTICOS HOSPITALIZADOS

91
GLUCEMIA < 200 mg/dl en Pacientes con: Enfermedad terminal
Expectativa de Vida Pequeña Riesgo de hipoglucemia

92
MODIFICACION NECESARIA SI LA GLUCEMIA <70 MG/DL
PARA EVITAR HIPOGLUCEMIAS, REEVALUAR LA TERAPIA CUANDO LAS GLUCEMIAS SEAN < 100 MG/DL MODIFICACION NECESARIA SI LA GLUCEMIA <70 MG/DL

94
NECESITAMOS NUTRICIONISTAS EN LA INTERNACIÓN

95
Las comidas del hospital deben contener una cantidad consistente de carbohidratos en cada comida que sea util para coordinar la dosis de la insulina de acción rápida

96
LA INSULINA ES LA TERAPIA PREFERIDA COMO METODO PARA ALCANZAR LOS CONTROLES GLUCEMICOS EN PACIENTES HOSPITALIZADOS

97
DISCONTINUAR LOS ANTIDIABETICOS ORALES E INICIAR INSULINA EN LOS DM2 INTERNADOS POR UNA ENFERMEDAD AGUDA

98
EVALUAR Y CAMBIAR LA DOSIS DE INSULINA QUE YA RECIBIA EL PACIENTE EN SU CASA A FIN DE DISMINUIR EL RIESGO DE HIPOGLUCEMIAS

99
LOS QUE YA RECIBIAN INSULINA EN SU CASA DEBEN SEGUIR RECIBIENDO INSULINA SUBCUTÁNEA EN EL HOSPITAL

100
NO USAR LA ESCALA MOVIL DE INSULINA COMO TERAPIA UNICA PARA ALCANZAR EL CONTROL GLUCEMICO DURANTE LA INTERNACION EN PACIENTES CON DIABETES

101
IMPLEMENTAR: INSULINA BASAL (1 O 2 VECES) + INSULINA RÁPIDA O ULTRARRÁPIDA PRE PRANDIALES
 + INSULINA RÁPIDA O ULTRARRÁPIDA PRE PRANDIALES")
102
LAS CORRECCIONES CON INSULINA DEBEN SER INCLUIDAS EN EL ESQUEMA INSULINICO

106
RESTITUIR EL ESQUEMA PRE INTERNACIÓN EN PACIENTES CON CONTROL ACEPTABLE EN LA PRE ADMISIÓN SIN CONTRAINDICACIONES PARA LA CONTINUACIÓN DEL ESQUEMA ANTERIOR

107
Se sugiere que la insulina se instaure al menos un día antes del alta para parmitir evaluar la eficacia y la seguridad de esta transición

108
Entregar INDICACION ESCRITA Y EXPLICAR VERBALMENTE, todo lo referente al manejo glucémico.
LA INDICACIÓN DEBE ESTAR ESCRITA DE MANERA ENTENDIBLE PARA LA PERSONA QUE VA A ADMINISTRAR LA MEDICACIÓN

110
EN PACIENTES QUE RECIBIAN INFUSIÓN CONTINUA DE INSULINA, INICIAR EL ESQUEMA SUCRUTANEO 1 – 2 HS ANTES DE LA DISCONTINUACIÓN DEL GOTEO

111
USAR UN ESQUEMA DE INSULINA SUB CUTÁNEA EN PACIENTES QUE RECIBEN INFUSIÓN CONTÍNUA DE INSULINA SIN HISTORIA PREVIA DE DIABETES PERO QUE HAYAN REQUERIDO MÁS DE 2 UI/HORA

112
CONTROLES DE GLUCEMIA CAPILAR LUEGO DE LA DISCONTINUADCIÓN DE LA INFUSIÓN CONTINUA DE INSULINA

113
CONTROLAR LA GLUCEMIA CAPILAR EN PACIENTES QUE RECIBEN NUTRICION PARENTERAL O ENTERAL

115
DISCONTINUAR LAS GLUCEMIAS CAPILARES EN LOS PACIENTES CON DM QUE PRESENTAN VALORES MENORES A 140 MG/DL SIN TERAPIA INSULINICA POR 24 – 48 HS DESPUES DE HABER ALCANZADO AL INGESTA CALORICA DESEADA ?

116
INICIAR INSULINA EN PACIENTES DIABETICOS CONOCIDOS Y EN AQUELLOS QUE NO SE CONOCEN PERO CON GLUCEMIAS > 140 MG/DL, QUE DEMOSTRARON UN REQUERIMIENTO PERSISTENTE (> HS ) DE CORRECCIONES CON INSULINA.
 DE CORRECCIONES CON INSULINA.")
117
TODOS LOS PACIENTES CON DM1 QUE SERÁN SOMETIDOS A UN PROCEDIMIENTO QUIRURGICO (MAYOR O MENOR) DEBEN RECIBIR INFUSIÓN O INSULINA SC BASA CON BOLOS PARA PREVENIR LA HIPERGLUCEMIA EN EL PERIODO PERIOPERATORIO
 DEBEN RECIBIR INFUSIÓN O INSULINA SC BASA CON BOLOS PARA PREVENIR LA HIPERGLUCEMIA EN EL PERIODO PERIOPERATORIO")
118
DISCONTINUAR LA TERAPIA ANTIDIABÉTICA NO INSULINICA ANTES DE LA CIRUGIA CON INICIO DE INSULINA EN LOS QUE DESARROLLAN HIPERGLUCEMIA DURANTE EL PERIODO PERIOPERATORIO

119
CUANDO SE INSTITUYE LA TERAPIA SC CON INSULINA EN EL POST OPERATORIO.
USAR INSULINA BASAL (PARA LOS PACIENTES NPO) o BASAL BOLUS (para paciente que comen).
 o BASAL BOLUS (para paciente que comen).")
120
CONTROL DE GLUCEMIA CAPILAR EN PACIENTES QUE RECIBEN CORTICOIDES.
CON O SIN HISTORIA DE DIABETES

121
DISCONTINUAR EL CONTROL DE GLUCEMIA CAPILAR SI ESPUES DE 24 – 48 HS NO EXISTIERA HIPERGLUCEMIA (GLUCEMIAS MENORES A 140 MG/DL)
")
122
INICIAR INSULINA EN LOS PACIENTES CON HIPERGLUCEMIA PERSISTENTE QUE RECIBEN TERAPIA CON GLUCOCORTICOIDES

123
USAR INFUSIÓN CONTÍNUA COMO ALTERNATIVA A LA INSULINA SC EN LOS PACIENTES CON GLUCEMIA CAPILAR ELEVADA A PESAR DE UN ESQUEMA BASAL BOLUS SC

124
PREPARAR PROTOCOLOS CON DIRECCIONES ESPECÍFICAS PARA EVITAR Y MANEJAR LAS HIPOGLUCEMIAS EN EL HOSPITAL

125
IMPLEMENTAR UN PROTOCOLO QUE DEBE SER INICIADO POR ENFERMERIA INMEDIATAMENTE UNA VEZ RECONOCIDA UNA HIPOGLUCEMIA (DEFINIDA COM GLUCEMIA POR DEBAJO DE 70 MG/DL)
")
126
INSTAURAR UN PLAN DE BUSQUEDA DE LA FRECUENCIA DE EVENTOS HIPOGLUCEMICOS CON ANALISIS DE SUS CAUSAS Y LOS EVENTOS ASOCIADOS CON EL DAÑO POTENCIAL AL PACIENTE

127
IMPLEMENTAR UN COMITE INTERDISCIPLINARIO PARA MEJORAR EL CUIDADO DE PACIENTES CON DIABETES

129
CADA INSTITUCIÓN DEBERÍA TENER UN METODO DE COLECCIÓN Y EVALUACIÓN DE LAS GLUCEMIAS CAPILARES Y LA INSULINA Y UTILIZAR ESA INFORMACIÓN COMO MANERA DE MONITORIZAR LA SEGURIDAD Y EFICACIA DEL CONTROL GLUCÉMICO

130
LAS INSTITUCIONES DEBEN PROVEER GLUCOMETROS EFICACES Y EXACTOS

132
Muchas Gracias

Presentaciones similares




























 developed ischemia with exercise. During a mean follow-up of 4.5 3.4 years, 313 patients died, and 183 patients had.>")







