Descargar la presentación
La descarga está en progreso. Por favor, espere

1
ARTRITIS Hospital Ramón y Cajal Cristina Abad Nacho Gallego
José Acosta Isabel García

2
CONTEXTO CLINICO ♂ 64 años Artritis larga evolución.
Ciatalgia + RM lumbar sin causa del dolor AHORA: ↑ dolor + paralisis sensitivo-motora. EMG: neuropatía nervio tibial posterior

3
¿De qué tipo de artritis se trata?
Artritis reumatoide Artritis infecciosa Artritis gotosa Artritis por PFC

5
¿PODEMOS DETERMINAR LA CAUSA DE LA CLINICA DEL PACIENTE?
Si, se debe a compresión nerviosa por el quiste de Baker Si, se debe a compresión nerviosa por ocupación del arco soleo. Si, se debe a una lesión traumática por los tofos. No, debemos extender el estudio al resto del MI.

6
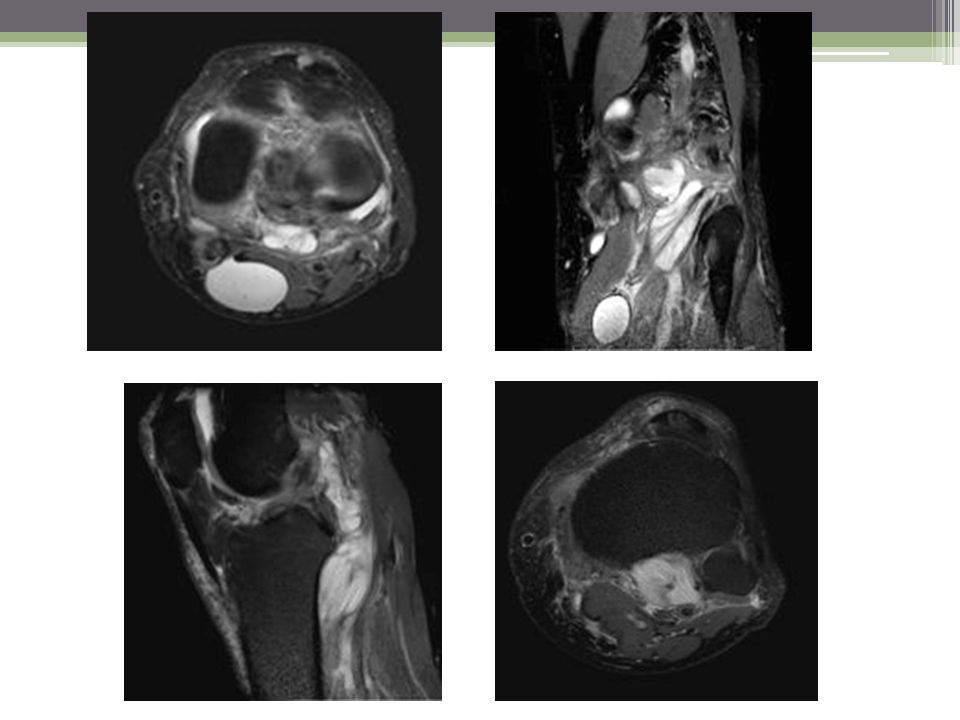
CONCLUSIÓN Artritis gotosa: Formación de quistes articulares
Espacio articular normal Cartílago conservado Tofos y erosiones óseas Formación de quistes articulares Rotura de ganglión y miositis del m.poplíteo Compresión de terbio tibial por aumento de tamaño del m. poplíteo. ARTRITIS GOTOSA QUISTE DE BAKER Y GANGLIONES ROTURA GANGLION MIOSITIS MUSCULO POPLITEO NEURITIS COMPRESIVA NERVIO TIBIAL

7
BIBLIOGRAFIA Girish G, Glazebrook KN, Jacobson JA. Advanced imaging in gout. AJR Am J Roentgenol Sep;201(3): Su H, Li X, Zhao N, Zou H, Jiang L, Zhou Y. Comparing the usefulness of four imaging techniques in the same gouty arthritis patient. Int J Rheum Dis Oct;15(5):e Dalbeth N, Doyle AJ. Imaging of gout: an overview. Best Pract Res Clin Rheumatol Dec;26(6):
:e Dalbeth N, Doyle AJ. Imaging of gout: an overview. Best Pract Res Clin Rheumatol Dec;26(6):")
Presentaciones similares