Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Clínica Los Yoses Dr. Luis Carlos Ramírez Z.
Endocrinología Universidad de Costa Rica; Southwestern Medical School , Dallas, Texas Tel: ,

2
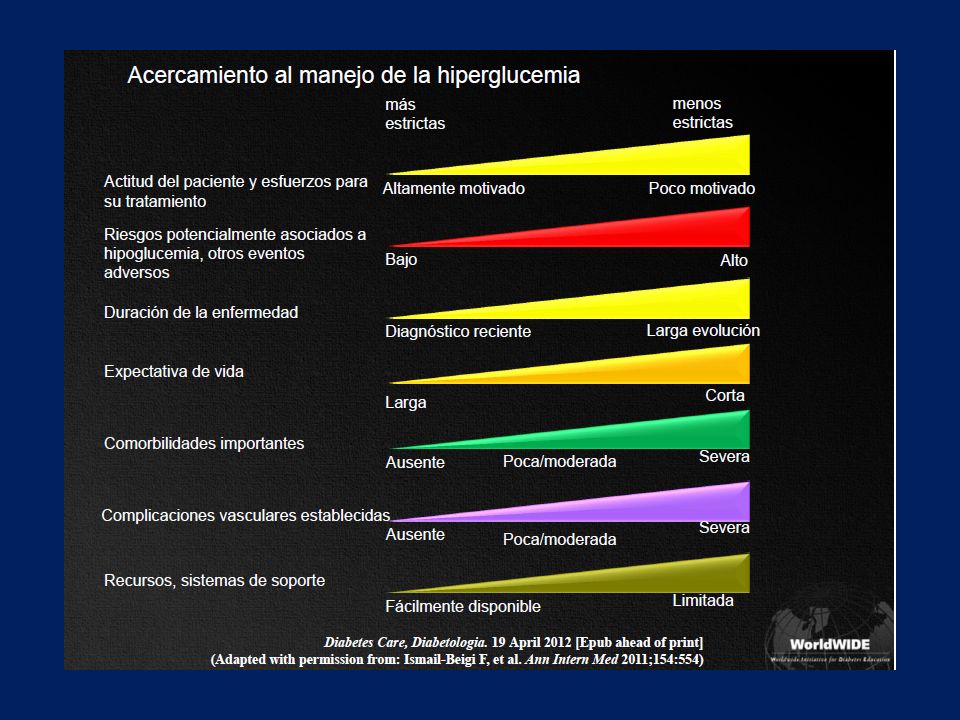
Objetivos HbA1c en la Tercera Edad
American Diabetes Association American Geriatics Society Department of Veterans Affairs A1c < 7.0 % < 7.0 % en adultos en buen estado de salud 8.0 % en pacientes enfermos o con EV < 5 años < 7.0 % si EV > 15 a ( sin comorbilidad mayor) 8 % si EV 5 – 15 a (comorbilidad moderada) 9 % si EV < 5 a ( comorbilidad mayor) Cleveland Clinic Journal of Medicine Volume 75:1 Jan 2008
 8 % si EV 5 – 15 a (comorbilidad moderada) 9 % si EV < 5 a ( comorbilidad mayor) Cleveland Clinic Journal of Medicine Volume 75:1 Jan")
4
Insulina basal: Ajuste de dosis por el paciente
Incrementar 3 unidades Glucosa de ayunas >90 mg/dl Glucosa de ayunas >110 mg/dl Glucosa de ayunas 70-90mg/dl Mantener Dosis mg/dl Disminuir 3 unidades Glucosa de ayunas <70 mg/dl Glucosa de ayunas <80 mg/dl 244 pacientes con DM 2 con falla a orales que iniciaban insulina detemir La titiulación de dosis es fundamental para lograr llegar a las metas con una insulina basal. Este es uno de los errores comunes con el uso de insulinas basales. Los metanálisis indican que la dosis final promedio de insulina basal es de aproximaddamente 0.5 u/kg de peso real. Ajuste cada 3 días según el promedio de la glucosa de ayuno Diabetes Obes Metab. Jun 2009;11(6):
:")
6
Tratamiento farmacológico y quirúrgico de la obesidad Un plan nacional de lucha contra la obesidad

7
Spectrum of Obesity Treatment
Pharmacotherapy With co-morbidity + With co-morbidity Surgery + Overweight (Mild) (BMI 25 to 26.9) Overweight (Severe) (BMI 27 to 29.9) Obese (Class I) (BMI 30 to 34.9) Obese (Class II) (BMI 35 to 39.9 ) Extremely Obese (Class III) (BMI ≥40) TREATMENT + + + + Lifestyle modification With co-morbidity The official recommendations are to consider bariatric surgery for patients with a BMI greater than 35 with co-morbidities or greater than 40 without co-morbidities. Furthermore, you should inform your patients if they are a candidate. However, surgery is obviously not for everyone, even if they meet the recommended guidelines for referral. They must also generally demonstrate that they are unable to achieve and maintain a healthier body weight with non-surgical approaches understands how surgery works and is willing to make necessary lifestyle changes have a strong social support system have no significant mental health problems that would preclude post-operative compliance or that may worsen after surgery For may people, approval by insurance companies is also a critical factor for obvious economic reasons. ************************************************* So based on these recommendations, our sample patient meets criteria for surgery because his BMI is greater than or equal to 40. He also has numerous co-morbidities, at least one of which, his BP, is poorly controlled despite multiple medication. You should tell him that he is a candidate for surgery and suggest that he attend an information session offered by the local bariatric group. Even if he is not interested in surgery at the moment in may provided extra motivation for lifestyle changes, which you should also recommend. Most programs and insurance companies require a trial of lifestyle management regardless, so candidacy for surgery is not a reason to omit this. Nevertheless, given his degree of obesity (class III), he is not likely to achieve clinically significant weight loss with medical management alone so there is no point of waiting another 6 months to start thinking about surgery. Surgery BMI > 30 with co-morbid conditions OR BMI>40 Unable to achieve and maintain a healthier body weight with non-surgical approaches Understands how surgery works and is willing to make necessary lifestyle changes Has a strong social support system No significant mental health problems that would preclude post-operative comliance or may worsen after surgery NIH/NHLBI Clinical Guidelines on the identification, evaluation, and treatment of overweight and obesity in adults. NIH Publication , September (Slide adapted from Dr. Anita Courcoulos).
 (BMI 25 to 26.9) Overweight (Severe) (BMI 27 to 29.9) Obese. (Class I) (BMI 30 to 34.9) Obese. (Class II) (BMI 35 to 39.9 ) Extremely Obese. (Class III) (BMI ≥40) TREATMENT Lifestyle. modification. With. co-morbidity. The official recommendations are to consider bariatric surgery for patients with a BMI greater than 35 with co-morbidities or greater than 40 without co-morbidities. Furthermore, you should inform your patients if they are a candidate. However, surgery is obviously not for everyone, even if they meet the recommended guidelines for referral. They must also generally demonstrate that they. are unable to achieve and maintain a healthier body weight with non-surgical approaches. understands how surgery works and is willing to make necessary lifestyle changes. have a strong social support system. have no significant mental health problems that would preclude post-operative compliance or that may worsen after surgery. For may people, approval by insurance companies is also a critical factor for obvious economic reasons. ************************************************* So based on these recommendations, our sample patient meets criteria for surgery because his BMI is greater than or equal to 40. He also has numerous co-morbidities, at least one of which, his BP, is poorly controlled despite multiple medication. You should tell him that he is a candidate for surgery and suggest that he attend an information session offered by the local bariatric group. Even if he is not interested in surgery at the moment in may provided extra motivation for lifestyle changes, which you should also recommend. Most programs and insurance companies require a trial of lifestyle management regardless, so candidacy for surgery is not a reason to omit this. Nevertheless, given his degree of obesity (class III), he is not likely to achieve clinically significant weight loss with medical management alone so there is no point of waiting another 6 months to start thinking about surgery. Surgery. BMI > 30 with co-morbid conditions OR BMI>40. Unable to achieve and maintain a healthier body weight with non-surgical approaches. Understands how surgery works and is willing to make necessary lifestyle changes. Has a strong social support system. No significant mental health problems that would preclude post-operative comliance or may worsen after surgery. NIH/NHLBI Clinical Guidelines on the identification, evaluation, and treatment of overweight and obesity in adults. NIH Publication , September (Slide adapted from Dr. Anita Courcoulos).")
8
Temario Tratamiento Farmacológico Cirugía Bariátrica
Medicamentos prohibidos Medicamentos permitidos Medicamentos en investigación Cirugía Bariátrica Definición y modalidades Indicaciones Resultadosn Un Plan Nacional de lucha contra la Obesidad

9
FARMACOTERAPIA

10
Farmacoterapia de la Obesidad Medicamentos Prohibidos
“ Primun non nocere ” La historia reciente de la farmacoterapia de la obesidad está llena de drogas prohibidas y abusos terapéuticos

11
Medicamentos Prohibidos
Levotiroxina Hipertiroidismo Anfetaminas Abuso, crisis adrenérgicas Dinitrofenol Cataratas y neuropatía Rainbow pills Arritmias y trastornos hidroelectrolíticos Aminorex Hipertensión pulmonar D – fenfluramina Hipertensión pulmonar y valvulopatías Sibutramina aumento de riesgo cardiovascular

12
Pharmacotherapy: Older Obesity Medications
Drug Name Mechanism ∆Weight Pros Cons Orlistat Pancreatic lipase inhibitor ~3% OTC Safe qAC dosing Cost Fecal fat/bloating Sibutramine Central 5HT/NE re-uptake inhibitor ~5% Most weight loss qD dosing Scheduled ↑ BP & HR, HA, insomnia Phentermine (others)* Sympatho-mimetic (↑ NE) ~4% Lowest cost Short-term Addictive So what medications are FDA-approved for weight loss. Currently these are the FDA-approved medications: Orlistat which inhibits absorption of fat from the gut by inhibiting fat breakdown by pancreatic lipase Sibutramine which reduced appetite by inhibiting reuptake of serotonin/NE in the central nervous system And Phentermine as well as other comparable “amphetamine-like” sympathomimetics that primarily reduce appetite. Studies have shown that these medication are effective in producing average weight reductions of 3-5% when used alone, however these effects can double or even triple when used in combination with lifestyle modification. I suspect that many of you are familiar with these medications, since they have been around for while. In fact, no new medications have been approved for weight loss in the US in over a decade. So breifly, what are the pros and cons of each? Orlistat is over the counter and is relative safe (although a multivitamin is recommended). However, it needs to be taken multiple times per day with meals, costs about ~$90/month, and has gastrointestinal side effects. Sibutrimine usually promotes the most weight loss and is taking once day. Most insurance companies do cover it now but it can cost up to around ~$110/months. It is scheduled and side effects including potentially increasing cardiovascular events as we will talk about. Phentermine is the most commonly prescribed drug for weight loss because it has been around for ever and is relatively cheap, but it is only approved for short-term use, is schedule and has addictive potential, and can increase BP as well as other side effects. *Also other similar sympathomimetics (diethlpropion, phendimetrazine,benzphetamine) Eckel BH. NEJM 358(18):
* Sympatho-mimetic (↑ NE) ~4% Lowest cost. Short-term. Addictive. So what medications are FDA-approved for weight loss. Currently these are the FDA-approved medications: Orlistat which inhibits absorption of fat from the gut by inhibiting fat breakdown by pancreatic lipase. Sibutramine which reduced appetite by inhibiting reuptake of serotonin/NE in the central nervous system. And Phentermine as well as other comparable amphetamine-like sympathomimetics that primarily reduce appetite. Studies have shown that these medication are effective in producing average weight reductions of 3-5% when used alone, however these effects can double or even triple when used in combination with lifestyle modification. I suspect that many of you are familiar with these medications, since they have been around for while. In fact, no new medications have been approved for weight loss in the US in over a decade. So breifly, what are the pros and cons of each Orlistat is over the counter and is relative safe (although a multivitamin is recommended). However, it needs to be taken multiple times per day with meals, costs about ~$90/month, and has gastrointestinal side effects. Sibutrimine usually promotes the most weight loss and is taking once day. Most insurance companies do cover it now but it can cost up to around ~$110/months. It is scheduled and side effects including potentially increasing cardiovascular events as we will talk about. Phentermine is the most commonly prescribed drug for weight loss because it has been around for ever and is relatively cheap, but it is only approved for short-term use, is schedule and has addictive potential, and can increase BP as well as other side effects. *Also other similar sympathomimetics (diethlpropion, phendimetrazine,benzphetamine) Eckel BH. NEJM 358(18):")
13
On October 8, 2010, the U.S. Food and Drug Administration (FDA) asked Abbott Laboratories to voluntarily withdraw from the U.S. market, its weight loss drug Meridia (sibutramine) because of clinical trial data indicating an increased risk of cardiovascular adverse events, including heart attack and stroke, in the studied population. Abbott has agreed to voluntarily stop marketing of Meridia in the United States.
14
Sibutramina: ( Raductil®, Betagen®, Vintix®, Lowex® )
")
15
Anorexígenos Productos simpaticomiméticos que aumentan tasa de metabolismo basal e inducen hiporexia : Fentermina ( Duromine ® ), Dietilpropion ( Tenuate Dos Pan ® , Neobes ® ), Mazindol ( Solucaps ® ) Deben ser usadas con seguimiento médico y nutricional y tx ansiolítico PRN Recomendados por no más de 3 meses
, Dietilpropion ( Tenuate Dos Pan ® , Neobes ® ), Mazindol ( Solucaps ® ) Deben ser usadas con seguimiento médico y nutricional y tx ansiolítico PRN. Recomendados por no más de 3 meses.")
16
Efectos adversos de los anorexígenos
Boca seca Nerviosismo, ansiedad, insomnio Palpitaciones Arritmias Constipación y/o diarrea Cefaleas Disminución de la libido

17
Orlistat Inhibe el 33 % de la actividad de la lipasa pancreática
Contraindicado en pacientes con enfermedades del colon Estudios de doble ciego muestran eficacia en obesidad, obesidad y diabetes, obesidad en adolescentes y en prevención de diabetes Dosis : 120 mg tid

18
33 % Lumen intestinal Cell mucosa Linfáticos Inhibidor lipasa Micela
TG Inhibidor lipasa FA FA MG Micela MG 33 % Acidos biliares

19
Orlistat Efectos adversos
Diarrea Esteatorrea Flatulencia “ Oily ” spotting Incontinencia fecal episódica ( posible ante la ingesta de una comida fuertemente grasosa )
")
20
Pérdida de peso con orlistat, después de 1 año
Pérdida de peso media (%) PLA ORL -1 -2 -3 p<0.0001 -4 -5 -6 -2 12 24 36 52 Semana Análisis ITT preliminar, M37048
 PLA. ORL p< Semana. Análisis ITT preliminar, M")
21
Prospectivo, randomizado doble ciego, DM2 con HGO´s
Orlistat-Estudio Latinoamericano (Brasil, Argentina, México, Colombia y Costa Rica) Prospectivo, randomizado doble ciego, DM2 con HGO´s Edades 18-70, IMC > 27kg/m2 24 semanas Orlistat 120mg tid vs placebo Diabetes, Obesity and Metabolism, 5: , 2003
 Prospectivo, randomizado doble ciego, DM2 con HGO´s. Edades 18-70, IMC > 27kg/m2. 24 semanas. Orlistat 120mg tid vs placebo. Diabetes, Obesity and Metabolism, 5: ,")
22
Orlistat-Estudio Latinoamericano (Brasil, Argentina, México, Colombia y Costa Rica)
Resultados Orlistat % del peso inicial; Placebo % (p=0.0003) ≥ 5% del peso inicial : Orlistat 30%, placebo 17% (p=0.003) Orlistat A1c, glicemia en ayunas, glicemia postprandial y lípidos ( mejoría marginal ) Eventos adversos gastrointestinales 65.1%
 ≥ 5% del peso inicial : Orlistat 30%, placebo 17% (p=0.003) Orlistat A1c, glicemia en ayunas, glicemia postprandial y lípidos ( mejoría marginal ) Eventos adversos gastrointestinales 65.1%")
23
Recent Additions to Obesity Pharmacotherapy
Agents Action Approval/Phase Phentermine/ Topiramate ER (Qsymia®) Sympathomimetic Anticonvulsant (GABA receptor modulation, carbonic anhydrase inhibition, glutamate antagonism) Approved, Summer 2012 Lorcaserin (Belviq®) 5-HT2C serotonin agonist: Little affinity for other serotonergic receptors Bupropion/ Naltrexone Dopamine/noradrenaline reuptake inhibitor Opioid receptor antagonist NDA submitted, FDA requested CV outcomes study ─ The Light Study Liraglutide GLP-1 agonist Phase 3 (High dose for obesity) FC: Phentermine and topiramate extended-release [package insert]. Mountain View, CA : Vivus; Lorcaserin hydrochloride [package insert]. Woodcliff Lake, NJ: Eisai Inc.; Clinicaltrials.gov. Cardiovascular Outcomes Study of Naltrexone SR/Bupropion SR in Overweight and Obese Subjects With Cardiovascular Risk Factors (The Light Study) Clinicaltrials.gov. Effect of Liraglutide on Body Weight in Non-diabetic Obese Subjects or Overweight Subjects With Co-morbidities: SCALE™ - Obesity and Pre-diabetes 23 23
 Sympathomimetic. Anticonvulsant (GABA receptor modulation, carbonic anhydrase inhibition, glutamate antagonism) Approved, Summer Lorcaserin. (Belviq®) 5-HT2C serotonin agonist: Little affinity for other serotonergic receptors. Bupropion/ Naltrexone. Dopamine/noradrenaline reuptake inhibitor. Opioid receptor antagonist. NDA submitted, FDA requested CV outcomes study ─ The Light Study. Liraglutide. GLP-1 agonist. Phase 3 (High dose for obesity) FC: Phentermine and topiramate extended-release [package insert]. Mountain View, CA : Vivus; Lorcaserin hydrochloride [package insert]. Woodcliff Lake, NJ: Eisai Inc.; Clinicaltrials.gov. Cardiovascular Outcomes Study of Naltrexone SR/Bupropion SR in Overweight and Obese Subjects With Cardiovascular Risk Factors (The Light Study) Clinicaltrials.gov. Effect of Liraglutide on Body Weight in Non-diabetic Obese Subjects or Overweight Subjects With Co-morbidities: SCALE™ - Obesity and Pre-diabetes")
24
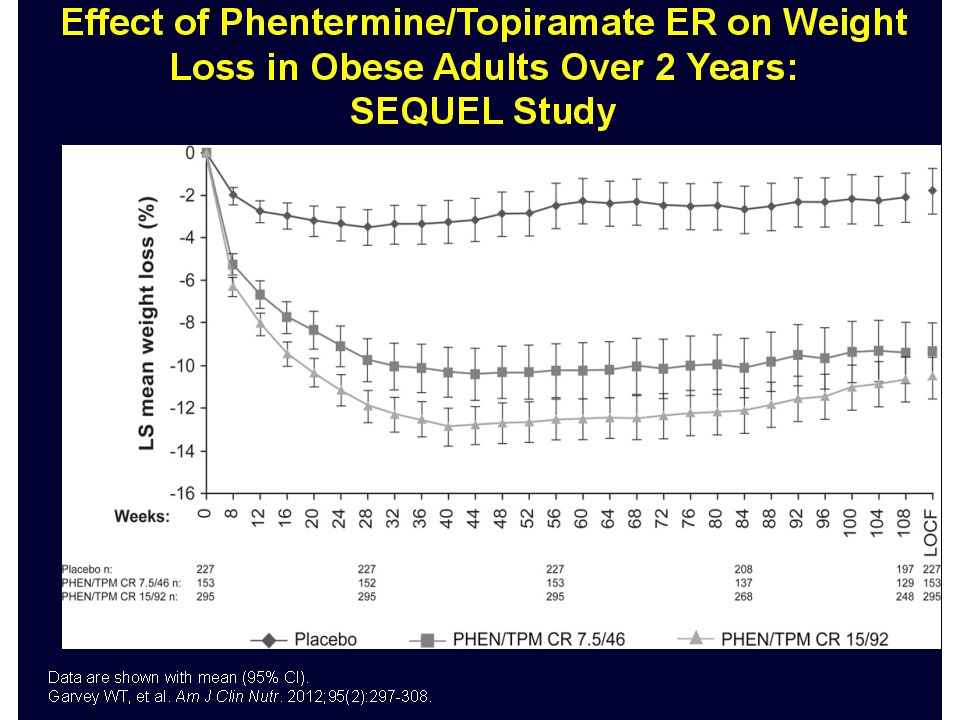
Phentermine/Topiramate ER
Mechanism of Action Indications and Dose Contraindications and Warnings Approved by FDA, July 2012, schedule IV Contraindications: Phentermine: Pregnancy, glaucoma, hyperthyroidism, MAOIs Sympathomimetic amine, NE release Indication: Weight loss in patients with BMI ≥30 kg/m2 or BMI ≥27 kg/m2 with weight-related co- morbid condition(s) Blunts appetite Warnings: Topiramate: Fetal toxicity Increases GABA Increased heart rate activity, antagonize Suicide and mood and sleep disorders Treatment dose daily: phentermine 7.5 mg topiramate ER 46 mg AMPA/ kainate Acute myopia and glaucoma glutamate receptor, carbonic Max dose daily: phentermine 15 mg topiramate ER 92 mg Cognitive impairment anhydrase inhibitor Metabolic acidosis Prolongs satiety Creatinine elevations Hypoglycemia with diabetes meds v v Phentermine and topiramate extended-release [package insert]. Mountain View, CA : Vivus; 2012.
 Blunts appetite. Warnings: Topiramate: Fetal toxicity. Increases GABA. Increased heart rate. activity, antagonize. Suicide and mood and sleep disorders. Treatment dose daily: phentermine 7.5 mg topiramate ER 46 mg. AMPA/ kainate. Acute myopia and glaucoma. glutamate. receptor, carbonic. Max dose daily: phentermine 15 mg topiramate ER 92 mg. Cognitive impairment. anhydrase inhibitor. Metabolic acidosis. Prolongs satiety. Creatinine elevations. Hypoglycemia with diabetes meds. v. v. Phentermine and topiramate extended-release [package insert]. Mountain View, CA : Vivus;")
26
Contraindications and Warnings
Lorcaserin Mechanism of Action Indications and Dose Contraindications and Warnings Approved by FDA June 2012 Contraindications: Selective 5-HT2C receptor agonist Pregnancy Indication: Weight loss in patients with BMI ≥30 kg/m2 or BMI ≥27 kg/m2 with weight-related co-morbid condition(s) Warnings: Stimulates α-MSH production from POMC neurons resulting in activation of MC4R Coadministration with other serotonergic or antidopaminergic agents 10 mg po bid, schedule pending (IV) Valvular heart disease Discontinue if 5% weight loss is not achieved in 12 wks Cognitive impairment Increases satiety Psychiatric disorders (euphoria, suicidal thoughts, depression) Priapism Risk of hypoglycemia with diabetes meds v v Lorcaserin hydrochloride [package insert]. Woodcliff Lake, NJ: Eisai Inc.; 2012.
 Warnings: Stimulates α-MSH production from POMC neurons resulting in activation of MC4R. Coadministration with other serotonergic or antidopaminergic agents. 10 mg po bid, schedule pending (IV) Valvular heart disease. Discontinue if 5% weight loss is not achieved in 12 wks. Cognitive impairment. Increases satiety. Psychiatric disorders (euphoria, suicidal thoughts, depression) Priapism. Risk of hypoglycemia with diabetes meds. v. v. Lorcaserin hydrochloride [package insert]. Woodcliff Lake, NJ: Eisai Inc.;")
27
27

28
LiraglutiferLi

29
Obesidad Nadando contra corriente…
Tx farmacológico puede inducir aproximadamente un % de pp Control nutricional puede inducir un 3 % de pp El 20 % de pacientes exitosos logran mantener una pp > 10 % Am J. Clin Nutr 2005 ¿ Y el 80 % restante ?

30
Cirugía Bariátrica ¿ Logrará este paciente bajar de peso de forma significativa y duradera con dieta ?

31
Updated: 4/27/2017 2:17 PM Mean Percent Weight Change during a 15-Year Period According to the Method of Bariatric Surgery Very poor results of non-surgical treatments Maximal Weight loss Sjostrom L et al (SOS) N Engl J Med 2007;357:741
 N Engl J Med 2007;357:741.")
32
OBESIDAD y Cirugía En práctica desde hace 60 años
IMC > 40 ( hasta hace 3 años; ya no ) IMC > 35 con comorbilidades IMC entre 30 – 35 bajo investigación Diferentes técnicas Depende de la experiencia y destreza del equipo quirúrgico Puede estar indicada en adolescentes y > 55 a. Buenos resultados
 IMC > 35 con comorbilidades. IMC entre 30 – 35 bajo investigación. Diferentes técnicas. Depende de la experiencia y destreza del equipo quirúrgico. Puede estar indicada en adolescentes y > 55 a. Buenos resultados.")
33
Cirugía Bariátrica Variaciones
Procedimientos restrictivos: Gastroplastías , LAGB Procedimientos mixtos: RYGB Derivaciones biliopancreáticas

34
Modalidades de Cx. bariátrica

35
Enfasis en trabajo en equipo
Cirugía Bariátrica Enfasis en trabajo en equipo Internista Cirujano Psicóloga Otros Nutricionista

36
Seguimiento post quirúrgico
Suplementar vitaminas liposolubles PRN Suplementar hierro PRN Suplementar alimentos proteicos PRN ¡ Colelitiasis ! % Control nutricional J Clin Gastroenterology 2006 ; 40 :

37
Cirugía Bariátrica Resultados
Ashley y cols, 1993 : 114 pacientes 60 % perdieron más de 50 % del exceso de peso IMC al año Flickinger y cols, 1984 : 210 pacientes Pérdida de peso de 51 kg en 18 meses Sugerman y cols, 1992 : pérdida de 50 % del exceso de peso a los 9 años

38
Resultados Cirugía Bariátrica
Pérdida de peso del % del exceso de peso en los primeros dos años de la cirugía Disminución del riesgo relativo de muerte de 89 % en los próximos 5 años en relación con el grupo control (p < ) ASA 2004
 ASA")
39
…Resultados Cirugía Bariátrica
DM 2 : normalización % IGT : normalización % HTA : normalización %

40
RESULTADOS ESPERADOS A LARGO PLAZO DE CIRUGÍA GÁSTRICA RESTRICTIVA
Condición Comórbida Mejoría o Resolución (%) Diabetes 100 Enfermedad Coronaria Hipercolesterolemia 96 Reflujo gastroesofágico Apnea del sueño 93 Hipertensión 88 Osteoartritis Hipertrigliceridemia 86 Depresión 55 Ann Surg 232: , 2000
 Diabetes Enfermedad Coronaria. Hipercolesterolemia. 96. Reflujo gastroesofágico. Apnea del sueño. 93. Hipertensión. 88. Osteoartritis. Hipertrigliceridemia. 86. Depresión. 55. Ann Surg 232: ,")
41
Riesgo de mortalidad con la cirugía : 0.68 %
Riesgo de mortalidad sin la cirugía: %

42
Updated: 4/27/2017 2:17 PM Mean Percent Weight Change during a 15-Year Period According to the Method of Bariatric Surgery Very poor results of non-surgical treatments Maximal Weight loss Sjostrom L et al (SOS) N Engl J Med 2007;357:741
 N Engl J Med 2007;357:741.")
43
Bariatric Surgery vs intensive Medical Therapy in Obese patients with Diabetes NEJM March 26, 2012
Estudio aleatorizado de 12 m. en 150 pacientes con DM , IMC A1c 9. 2 % Edad 49 años Duración de la diabetes 8. 2 años Punto final A1c < 6 % Resultados : Tx médico PP k ( - 12 % ) Roux en Y PP k ( - 42 %) Sleeve gastrectomy PP k ( - 37 % ) A1c < 6 % sin tx farmacológico : Tx médico 0 % , R en Y 42 % , SG 27 %
 Roux en Y PP 29.4 k ( - 42 %) Sleeve gastrectomy PP k ( - 37 % ) A1c < 6 % sin tx farmacológico : Tx médico 0 % , R en Y 42 % , SG 27 %")
44
Bariatric Surgery vs Conventional Medical Therapy for Type 2 Diabetes NEJM March 26, 2012
Estudio aleatorizado, de 2 a., 60 pacientes con DM , IMC > 35. X 45 . A1c > % ; promedio % Edades a. Duración de la diabetes > 5 años Punto final : remisión : < 6. 5 % sin tx farmacológico Resultados : Tx médico A1c < %, 0 ; A1c promedio % R en Y : A1c < 6. 5 %, 75 % ; A1c promedio % Desviación bilio pancreática : A1c < 6. 5 %, 95 % , A1c promedio %

45
Bariatric Surgery vs. Medical Therapy for T2DM: Italian Study
7.7±0.6% 6.4±1.4% 5.0±0.5% 93% retention rate at 2 years. Average baseline A1C was 8.65±1.45%. Avg diabetes duration 6 years Avg age 43.45±7.27 Pts with biliopancreatic diversion had shorter time to remission likely due to the substantial fat malabsorption that occurs. N=60 Mingrone et al. N Engl J Med 2012;366:1577

47
Temario Tratamiento Farmacológico Cirugía Bariátrica
Medicamentos prohibidos Medicamentos permitidos Medicamentos en investigación Cirugía Bariátrica Definición y modalidades Indicaciones Resultadosn Un Plan Nacional de lucha contra la Obesidad

48
"In the end, as First Lady, this isn’t just a policy issue for me
"In the end, as First Lady, this isn’t just a policy issue for me. This is a passion. This is my mission. I am determined to work with folks across this country to change the way a generation of kids thinks about food nutrition and phsyical activity.“ Michelle Obama

49
Los cinco pilares de la iniciativa «Lets Move»
1. Crear un “arranque” saludable en los niños 2. Empoderar a los padres y maestros 3. Proveer comida saludable en las escuelas 4. Mejorar el acceso y el precio de la comida saludable 5. Aumentar la actividad física

50
EPODE Ensemble, prévenon l´obesité des enfants
Nestlé 1992, Francia : plan piloto comunal que logró suprimir el crecimiento de la obesidad en niños; grupo no intervenido 2x 2003 : EPODE en Francia , 10 ciudades, luego 167 más incluyendo 30 en España, 8 en Bélgica y se sumarán Grecia, Australia y Canadá Apoyado por la Fundación Carrefour y la Nestlé.

51
Sugerencia para atacar la obesidad “Community approach”
El plan es involucrar a profesores, dueños de restaurantes, la comunidad, el gobierno, los médicos, las asociaciones deportivas, etc.... Es la lucha de la sociedad entera contra la obesidad EPODE ( Ensemble, prévenons l´obesité des enfants) N ENGL J MED 360; 9 February 26, 2009
 N ENGL J MED 360; 9 February 26,")
52
La experiencia australiana Geelong, Australia, 2010
Estudio de seguimiento de niños y adolescentes Financiado por el Ministerio de Salud 3 años de seguimiento Mejores resultados en niños < de 5 años, intermedios en escolares y pobres en adolescentes Niños 1 kilo de peso menos que el grupo control ; prevalencia de obesidad no aumentó Psychology and Sociology, July 13, 2010

53
Esfuerzo en Costa Rica Reciente logro del Ministerio de Educación para limitar la venta de ciertos productos perjudiciales en escuelas

54
Una política nacional contra la epidemia de la obesidad…
Casa Presidencial y el gobierno Ministerio de Salud CCSS Ministerio de Educación Pública Prensa Empresas, Iglesias Municipalidades y barrios Y Ud.

55
Muchas gracias

56
Ajustando las dosis de insulina en la Diabetes tipo 2 Reglas generales
Primero llegar al objetivo en ayunas con insulinas basales Dejar dosis estable si glicemia en ayunas y A1c alcanzan objetivo Si glicemia en ayunas alcanza objetivo pero A1c no, agregar insulina prandial con desayuno o comida más fuerte ( 4-8 u ) En debut diabético, suspender insulina ( basal ) cuando se alcanzan las metas con dosis menores de u/d.
 En debut diabético, suspender insulina ( basal ) cuando se alcanzan las metas con dosis menores de u/d.")
Presentaciones similares