Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Estrategias intraoperatorias de ventilación unipulmonar

2
VENTILACION UNIPULMONAR
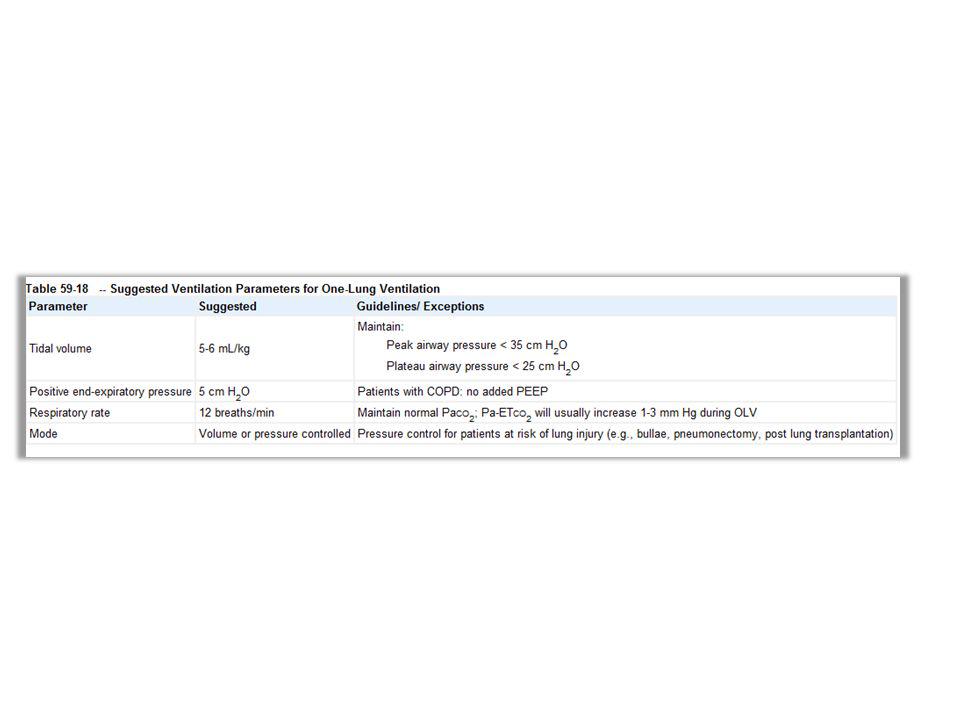
VOLUMEN CORRIENTE PEEP FIO2 HIPERCAPNIA RELACION I:E PRESION PICO Y PLATEU MODO VENTILATORIO

3
VOLUMEN TIDAL VOLUMEN TIDAL 4-6 ML/K
This form of lung injury results in diffuse alveolar damage, increased permeability, pulmonary oedema, cell contraction and cytokine production OLV traditionally has been performed with tidal volumes that are equal to those being used on TLV [4,61]. This practice was recommended, because large tidal volumes were shown to improve oxygenation and decrease shunt fraction during TLV [62] and OLV, irrespective of PEEP applied [63]. Improved oxygenation was thought to occur because of end-inspiratory alveolar recruitment. Excessive tidal volumes (eg, 15 mL/kg) on the other hand were shown to worsen oxygenation, likely because of elevations in PVR resulting in increased shunt flow [64]. However, OLV with high tidal volumes (referring to 10 to 12 mL/kg) has been pervasive for decades, and as such has an established safety record which investigated 32 patients undergoing OLV for thoracotomy. Minute ventilation and PEEP were identical between groups, and only tidal volumes were altered. Patients received OLV with 10 mL/kg or 5 mL/kg, both without PEEP. OLV was associated with cytokine elevations (tumor necrosis factor a [TNF-a], sICAM-1), but to a lesser degree with low tidal volume ventilation.
 on the other hand. were shown to worsen oxygenation, likely because of elevations in PVR resulting. in increased shunt flow [64]. However, OLV with high tidal volumes. (referring to 10 to 12 mL/kg) has been pervasive for decades, and as such. has an established safety record. which investigated 32 patients. undergoing OLV for thoracotomy. Minute ventilation and PEEP were. identical between groups, and only tidal volumes were altered. Patients. received OLV with 10 mL/kg or 5 mL/kg, both without PEEP. OLV was. associated with cytokine elevations (tumor necrosis factor a [TNF-a], sICAM-1), but to a lesser degree with low tidal volume ventilation.")
4
PEEP

5
AUTO-PEEP PEEP 5-10 NORMAL PEEP 3 -8 EPOC

6
FIO2 Fio2 necesaria para saturar >90% Tiempo Isquemia reperfusion
Stress oxidativo REEXPANSION CON FIO2 BAJAS Fio2 necesaria para saturar >90%

7
Hipercapnia

8
Paco mmHg sanos Y niveles mayores en ptes con severa obstrucción y trasplantes

9
RELACION I:E obstructivo Aumentar tiempo expiratorio Disminuir FR
Minimiza riesgo de autopeep restrictivo Igualar tiempo inspiratorio Aumentar FR Maximiza tiempo inspiratorio

10
Presión Pico y PLateu Riesgo de ali
Presion pico no mas de 35 – 40 cm H2O Presion plateu no mas de 25 cm H2O Riesgo de ali

11
Modo ventilatorio No diferencias en oxigenación con VCV o PCV, el ultimo disminuye riesgo de barotrauma

12
Reclutamiento Atelectasia Reexpansion Fio2 altas Falta de PEEP
Compresion extrinseca por visceras abdominales o mediastino Lento y progresivo Fio2 bajas Ojo con edema pulmonar por re expansion.

13
Tiempo

16
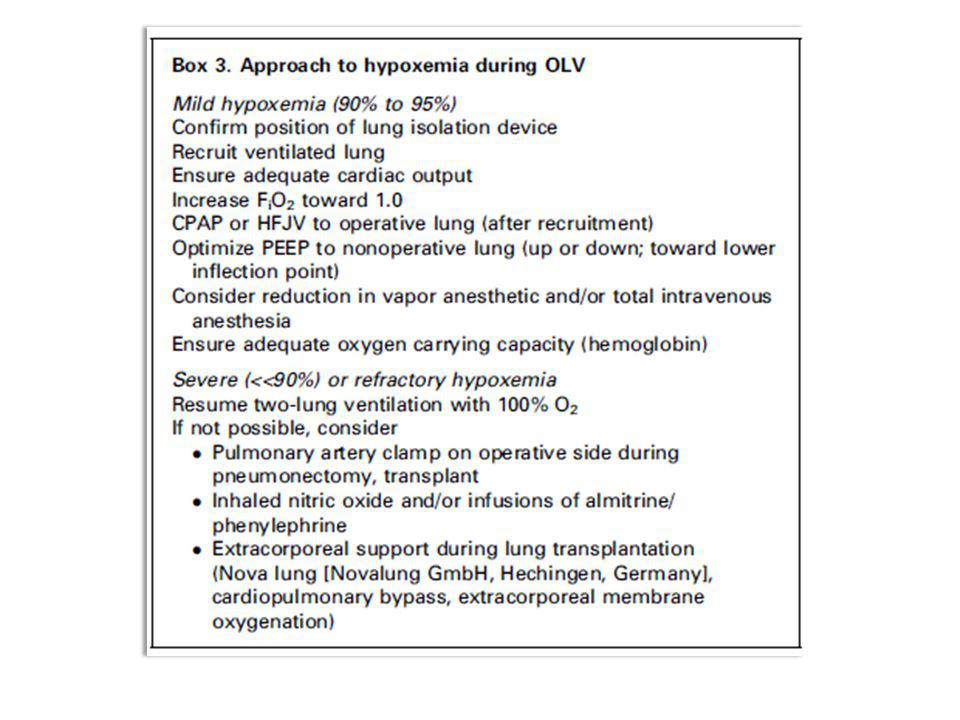
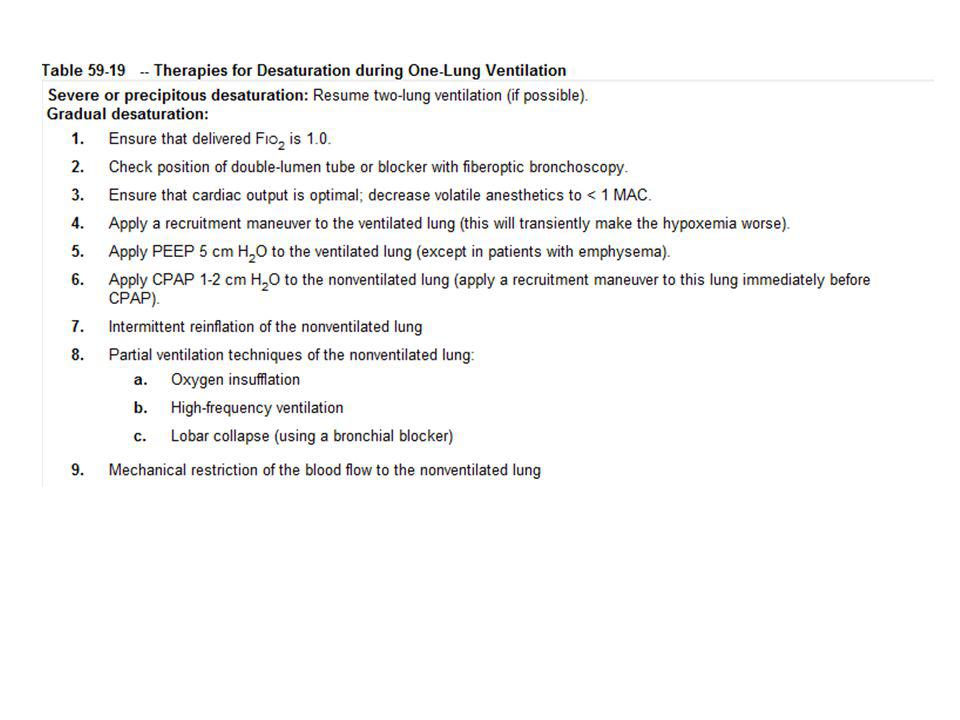
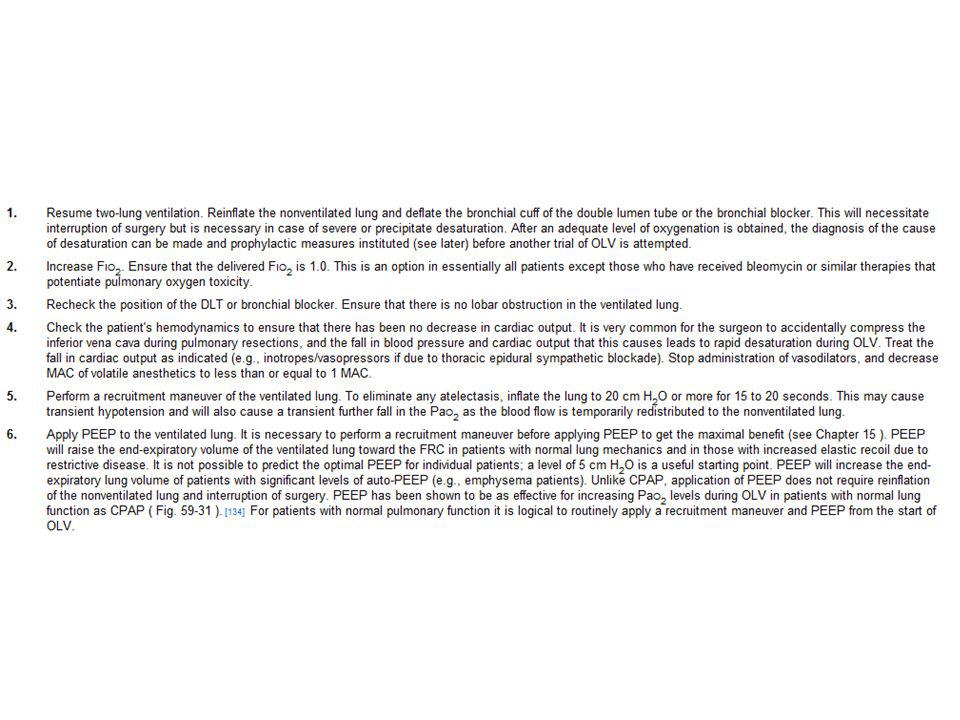
Hipoxemia intraoperatoria

17
INCIDENCIA ACTUAL >1%
SIEMPRE DESCARTAR ETIOLOGIA CARDIOVASCULAR!!!

Presentaciones similares