Descargar la presentación
La descarga está en progreso. Por favor, espere

1
<Pie de Página> Se edita por el menú Insertar, Número de Diapositiva... 1

2
SINDROME DE EMBOLIA GRASA

3
SINDROME DE EMBOLISMO GRASO
90% PACIENTES POLITRAUMATIZADOS GRASA EN LA CIRCULACION ASOCIADO CON 1 PATRON CLINICO DE SINTOMAS Y SIGNOS TRIADA – 72 HORAS INSUFICIENCIA RESPIRATORIA PROGRESIVA ALTERACIONES NEUROLOGICAS PETEQUIAS DIAGEl; en cambio, el síndrome de embolia grasa sóNOSTICO DE EXCLUSION

4
SINDROME DE EMBOLISMO GRASO
INCIDENCIA % 30 % FX PELVIS – FEMUR – TIBIA LA FRACTURA DE FEMUR ES LA MAS FRECUENTE MORTALIDAD % embolismo graso se produce en el 90% de los pacientes politraumáticos

5
SEG ETIOLOGIA OTRAS QUEMADURAS PANCREATITIS DISRUPCION MECANICA
DE LA BONE MARROW TRAUMA BX - TRASPLANTE MO SEG GRASA EXOGENA NUTRICION PARENTERAL TOTAL INFUSION DE PROPOFOL DISRUPCION MECANICA DE LOS ADIPOSITOS LIPOSUCCION TRAUMA DE TEJIDOS BLANDOS

6
FACTORES DE RIESGO 65 mm Hg in man n patients with fractured femurs,
elevations of intramedullary pressure between 140 and 830 mm Hg have been observed [6 The increase in intramedullary pressur ]. Efforts such as different reamer head designs, venting during nailing, and the unreamed nailing technique have been used to minimize intramedullary pressure changes [40, over the optimal method of nail inser- tion [45, 46] that centers on the systemic effects of intramedullary reaming. evidence that instrumentation of the femoral medullary canal causes intravasation of bone mar- row fat. NAIL CLAVO RIMADO O NO RIMADO CUAL ES PEOR In addition, careful surgical technique can limit the medullary canal pressurization associated with reaming.

7
FISIOPATOLOGIA MECANICA OBSTRUCCION DE MICROVASCULATURA
PULMON - CEREBRO – PIEL – OJOS BIOQUMICA HIDRÓLISIS X LIPASA RADICALES LIBRES REACCION INFLAMATORIA SEVERA LESION NEUMOCITOS - SURFACTANTE LLEVANDO A HIPOXEMIA SEVERA Fat droplets that gain access to the circulation at the injury site cause direct mechanical obstruction of the pulmonary microvasculature (D) Immunochemical staining showing marked iNOS in alveolar macrophages (arrows). (E) H&E staining showing fat droplets (white colour). Fat staining with Oil Red (F microvasculature; free fatty acids, which are byproducts of hydrolyzed neutral fat, act locally to increase permeability of the capillary bed, destroy the alveolar architecture, and damage lung surfactant; and platelet aggregation stimulated by fat globules causes local release of serotonin, histamine, and various other agents that can cause edema, hemorrhage, and vessel disruption (6,7,11). Although the precise mechanism of FES is still to be determined, the radiographic features are presumed to be manifestations of increased pulmonary capillary permeability and edema or ARDS
 Immunochemical staining showing marked iNOS in alveolar macrophages (arrows). (E) H&E staining showing fat droplets (white. colour). Fat staining with Oil Red (F. microvasculature; free fatty acids, which are byproducts of hydrolyzed neutral fat, act locally to increase permeability of the capillary bed, destroy the alveolar architecture, and damage lung surfactant; and platelet aggregation stimulated by fat globules causes local release of serotonin, histamine, and various other agents that can cause edema, hemorrhage, and vessel disruption (6,7,11). Although the precise mechanism of FES is still to be determined, the radiographic features are presumed to be manifestations of increased pulmonary capillary permeability and edema or ARDS.")
8
FISIOPATOLOGIA BIOQUIMICA HIDRÓLISIS X LIPASA RADICALES LIBRES
REACCION INFLAMATORIA SEVERA LESION NEUMOCITOS - SURFACTANTE DESTRUCCION ARQUITECTURA ALVEOLAR > PERMEABILIDAD CAPILAR - EDEMA - HEMORRAGIA HIPOXEMIA SEVERA (D) Immunochemical staining showing marked iNOS in alveolar macrophages (arrows). (E) H&E staining showing fat droplets (white colour). Fat staining with Oil Red (F microvasculature; free fatty acids, which are byproducts of hydrolyzed neutral fat, act locally to increase permeability of the capillary bed, destroy the alveolar architecture, and damage lung surfactant; and platelet aggregation stimulated by fat globules causes local release of serotonin, histamine, and various other agents that can cause edema, hemorrhage, and vessel disruption (6,7,11). Although the precise mechanism of FES is still to be determined, the radiographic features are presumed to be manifestations of increased pulmonary capillary permeability and edema or ARDS
 Immunochemical staining showing marked iNOS in alveolar macrophages (arrows). (E) H&E staining showing fat droplets (white. colour). Fat staining with Oil Red (F. microvasculature; free fatty acids, which are byproducts of hydrolyzed neutral fat, act locally to increase permeability of the capillary bed, destroy the alveolar architecture, and damage lung surfactant; and platelet aggregation stimulated by fat globules causes local release of serotonin, histamine, and various other agents that can cause edema, hemorrhage, and vessel disruption (6,7,11). Although the precise mechanism of FES is still to be determined, the radiographic features are presumed to be manifestations of increased pulmonary capillary permeability and edema or ARDS.")
9
FALLA DEL VENTRICULO DERECHA OBSTRUCCION 60% COR PULMONAR DISMINUCION DEL GASTO CARDIACO
INESTABILIDAD HEMODINAMICA CIDAdhesión de plaquetas. Secreción de serotonina y formación de coagulación intravascular, con subsecuente lesión vascular.. Cardiovascular changes after pulmonary fat embolization are characterized by an INCREASE IN PULMONARY ARTERY PRESSURE, SYSTEMIC ARTERIAL HYPOTENSION, A DECREASE IN CARDIAC OUTPUT, AND ARRHYTHMIAS. THE CARDIOVASCULAR DETERIORATION IS OFTEN TRANSIENT BUT MAY BE FULMINANT, RESULTING IN FULL-BLOWN CARDIAC FAILURE, CARDIAC ARREST, AND EVEN death. 4 The increase in pulmonary artery pressure that occurs due to fat embolism is due not only to a mechanical blockage of the pulmonary artery, but may be the result Respiratory failure from FES is characterized as permeability edema with decreased compliance similar to oleic acid lung injury [15]. Gas ex- change abnormalities include shunt AND INCREASED DEAD SPACE FROM ATELECTASIS and alveolar flooding comparable to ALI and ARDS from other causes [45 47]. La fisiopatología de la disfunción neurológica se describe mediante la presencia DE FORAMEN OVAL PERMEABLE, SHUNTS AV INTRAPULMONARES Y AL MOLDEAMIENTO DEL ÉMBOLO A TRAVÉS DEL CAPILAR PULMONAR.

10
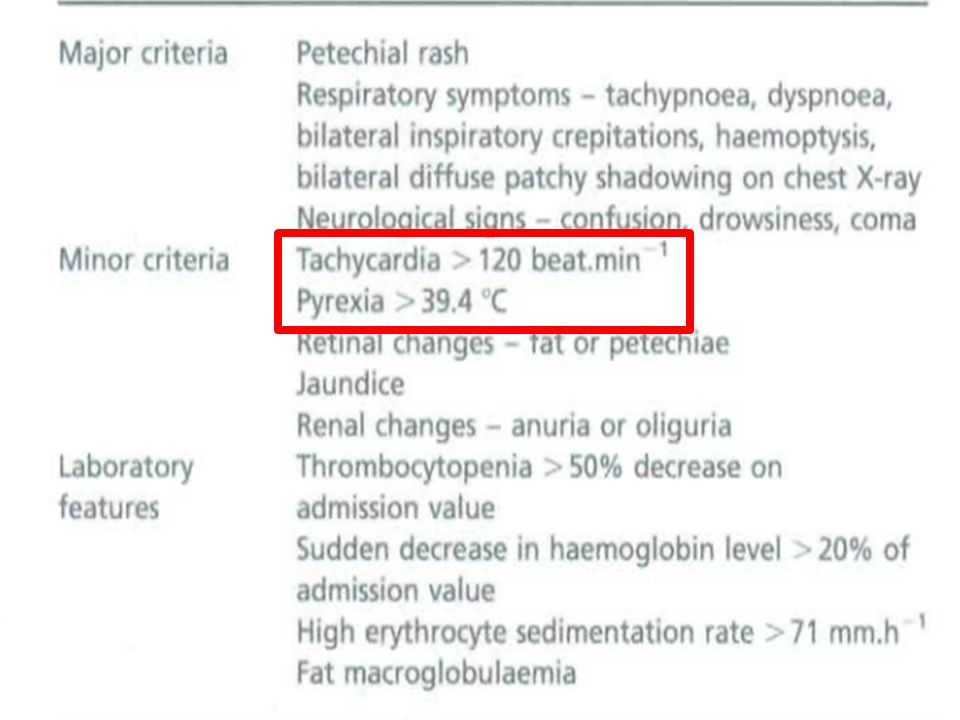
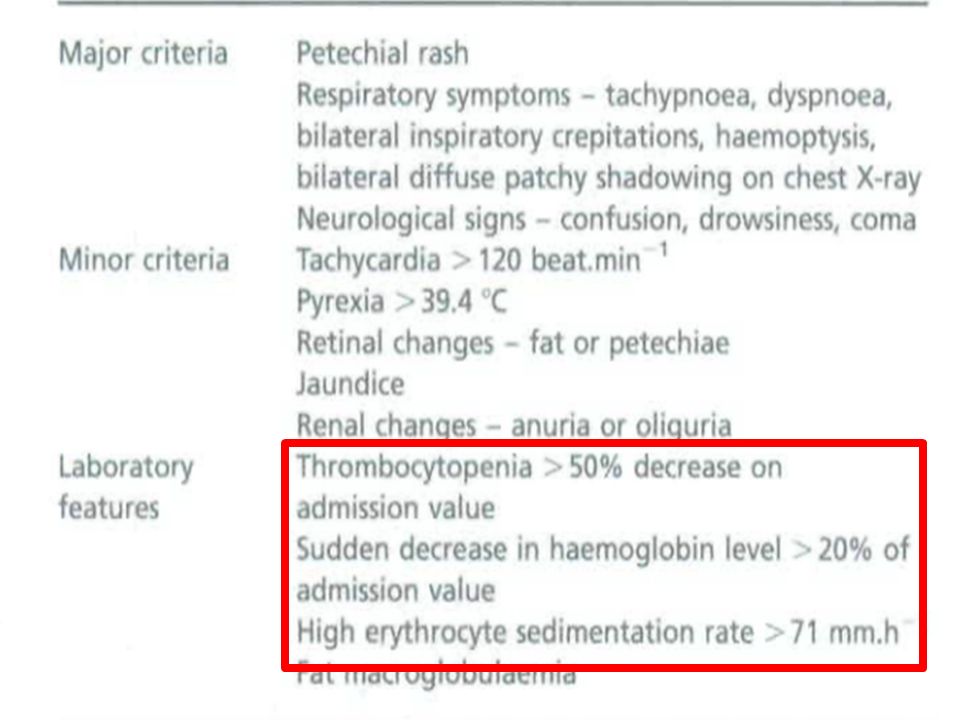
TAQUICARDIA 385 TEMPERATURA 39.4 RESPIRATORIA TAQUIPNEA DISNEA CREPITOS HEMOPTISIS RX DIFUSOS BILATERALES NEUROLOGICO CONFUSION COMA DISMINUCION HB SU TROMBOCITOPENIA > 50 % DE VALOR DE ADMISION HB > 20% DEL VALOR DE ADMISION VSG > 71 MACROBLOBULINEMIA GRASA

11
2 MAYORES O 1 MAYOR 3 MENORES en adapted by other authors who
stated that one of the following combinations of major and minor features was needed to make the diagnosis: two major [12 15]; one major and three minor [16, 17]; two major and two minor [16]; or one major and two minor [18] features

12
variada desde déficits focales hasta cuadros confusionales y
crisis comiciales. Su

15
CRITERIOS DE LINDEQUE ion has been criticized for excluding an objective assessment of hypoxemia documented by arterial blood gas, which precedes other clinical symp- toms and signs. Lindeque and colleague

16
INDICE SCHONFELD

17
and axillae. The rash tends to be tran-
sient and disappears within 24 hours. rior torso, and is also evident on oral mucous membranes, conjunctiva, skin folds of the neck, and axillae. The EXANTEMA PETEQUIAL: LA ZONA PREDOMINANTE ES CABEZA, CUELLO, TORAX ANTERIOR, AXILA Y CONJUNTIVA

18
CONJUNTIVA

19
Alteraciones visuales: En un 50% de los casos se afecta la retina por depósito
graso en la microcirculación

20
DIAGNOSTICO DIFERENCIAL
CONTUSION PULMONAR BRONCOASPIRACION EDEMA PULMONAR SDRA TROMBOEMBOLISMO PULMONAR TRALI El diagnóstico de embolia grasa es complicado en todo paciente politraumático debido a la multitud de entidades que pueden asociarse a éste y solaparse con la sintomatología respiratoria subclínica del embolismo graso. TRALI o DISTRESS RESPIRATORIO ASOCIADO A LA TRANSFUSIÓN

21
DIAGNOSTICO DIFERENCIAL
DE EXCLUSION CONTUSION PULMONAR BRONCOASPIRACION EDEMA PULMONAR SDRA TROMBOEMBOLISMO PULMONAR TRALI El diagnóstico de embolia grasa es complicado en todo paciente politraumático debido a la multitud de entidades que pueden asociarse a éste y solaparse con la sintomatología respiratoria subclínica del embolismo graso.

22
CONTUSION PULMONAR BRONCOASPIRACION EDEMA PULMONAR SDRA TROMBOEMBOLISMO PULMONAR TRALI

23
RADIOGRAFIA DE TORAX atients with FES 30% to 50% o
RADIOLOGIA: En la gran mayoría de pacientes suele ser normal.En un pequeño porcentaje puede objetivarse aumento de densidad difuso o parcheado períférico o basal.Es is nonspecific and variable (6,12,13). The chest radiograph remains normal in milder cases; Chest radiographs on admission (A) and at 1 h (B) and 2 h (C) after On admission, the lungs were clear, whereas pulmonary infiltration (arrows) was observed at 1 and 2 h after admission.
. The chest radiograph remains normal in milder cases; Chest radiographs on admission (A) and at 1 h (B) and 2 h (C) after. On admission, the lungs were clear, whereas pulmonary infiltration (arrows) was observed at 1 and 2 h after admission.")
24
RADIOGRAFIA DE TORAX failure shows diffuse bilateral consolidation and ground-glass opacities. The abnormalities were predominant in the right lung

25
TAC HALLAZGOS RADIOLOGICOS
OPACIDADES EN VIDRIO DESLUSTRADO CONSOLIDACION FOCAL - DIFUSA NODULOS DE VARIOS TAMAÑOS < 10 MM DISTRIBUCION PERIFERICA - PERIHILIAR DIÁMETRO DE BRONQUIOS Y ARTERIAS TThe different distributions reported in the literature may be due to differences in the severity of the syndrome hese abnormal shadows may be distributed in the peripheral lung zones (13), or they may predominate in the perihilar areas, simulating a pulmonary edema pattern (12) degrees ranging from localized alveolar opacities to mixed diffuse confluent nodules and consolidation, and most cases showed a mild degree of HEMORRAGIAA ALVEOLAR DIFUSA – INTERSTICIAL EDEMA - NEUMONITIS QUIMICA Common CT findings of pulmonary FES include focal or diffuse areas of CONSOLIDATION, FOCAL OR DIFFUSE AREAS OF GROUND-GLASS OPACITIES, and small nodules of various sizes ss than 10 mm. 6Y8 These findings are thought to represent interstitial hemorrhage, diffuse alveolar hemorrhage, edema, and chemical pneumonitis. 9,10
, or they may predominate in the perihilar areas, simulating a pulmonary edema pattern (12) degrees ranging from localized alveolar opacities to mixed diffuse confluent nodules and consolidation, and most cases showed a mild degree of. HEMORRAGIAA ALVEOLAR DIFUSA – INTERSTICIAL. EDEMA - NEUMONITIS QUIMICA. Common CT findings of pulmonary FES include focal. or diffuse areas of CONSOLIDATION, FOCAL OR DIFFUSE AREAS OF. GROUND-GLASS OPACITIES, and small nodules of various sizes. ss than 10 mm. 6Y8. These findings are thought to represent. interstitial hemorrhage, diffuse alveolar hemorrhage, edema, and chemical pneumonitis. 9,10.")
26
OPACIDADES VIDRIO ESMERILADO
ENGROSAMIENTO SEPTAL PREDOMINANTE MENTE PERIFERICOS GROUND GLAS ASOCIADOS CON NODULOS Y ENGROSAMIENTO SEPTAÑ

27
DISTRIBUCIÓN PARCHEADA-GEOGRÁFICA
OPAIDADES GRONUN GLAS AMBOS LOBULOS AREAS NORMALES ANORMALES ( APARIENCIA GENOGRAFIA ENGROSAMIENTO SEPTAL DIAMETROS ARTERIAS BRONQUIOS SON NORMALES

28
NODULOS DE VARIOS TAMAÑOS < 10 MM
CONSOLIDACION FOCAL DIFUSA AREAS DIFUSAS DE NODULOS DE VARIOS TAMAÑOS < 10 MM HEORRAFIA ALVEOLAR DIFUSA – INTERSTICIAL EDEMA - NEUMONITIS QUIMICA . 9,10

29
CONSOLIDACION - DERRAME PLEURAL
Olgunun toraks tomografisinde parankimal konsoli- dasyon ve minimal plevral effüzyon.

30
In the right lung, mixed diffuse consolidation and ground-glass opacity are noted. I
n the left lung, multifocal areas of ground-glass opacity, small well-defined nodules, and reticular density are noted. C: CT scan at a more caudal level shows bilateral pleural effusion

31
NODULOS CENTROLOBULILLARES
NODULOS SUBPLEURALES large ill-defined centrilobular airspace nodules (white arrow) and subpleural nodules (black arrow). The nodules are predominantly of ground-glass opacity with some areas of soft tissue attenuation obscuring the edges of the vessels.
 and subpleural nodules (black arrow). The nodules are. predominantly of ground-glass opacity with some areas of soft. tissue attenuation obscuring the edges of the vessels.")
32
PATRON NODULAR 1 2 MM

33
PATRON NODULAR

34
CAMBIOS RADIOLOGICOS EL INICIO DE LA APARICIÓN DE LAS IMÁGENES
1 - 3 DIAS LA RESOLUCIÓN ENTRE LOS DIAS eural.El inicio de la aparición de las imágenes suele ser entre el 1- 3 dias y la resolución entre los 7-25 dias tras el accidente.

35
TAC CON CONTRASTE VENTANA PARA MEDIASTINO
CONTRAST-ENHANCED MULTIDETECTOR ROW SPIRAL CT SHOWING fiLLING DEFECTS (WHITE ARROWS) AT THE SEGMENTAL LEVEL OF THE RIGHT AND LEFT PULMONARY ARTERIES (A). Region of interest measurements showed negative mean attenuation values of the fillingDEFECTS, SUGGESTING THE PRESENCE OF FAT TISSUE (mean attenuation values of the emboli at the segmental level of the right and left pulmonary artery were j54 and j42 Hounsfield units, respectively). Coronal (B) and sagittal (C) reformations of the filling defect at the segmental level of the right pulmonary artery. UNIDADES DESDE MENOS – AIRE 0 AGUA MAS 100 METALICA ABOSORCION DE LOS RAYOS S DENSIDAD NEGATIVA COMPATIBLE ON GRASA
 AT THE SEGMENTAL LEVEL OF THE RIGHT AND LEFT PULMONARY ARTERIES (A). Region of interest measurements showed negative mean attenuation values of the fillingDEFECTS, SUGGESTING THE PRESENCE OF FAT TISSUE (mean attenuation values of the emboli at the segmental level of the right and left. pulmonary artery were j54 and j42 Hounsfield units, respectively). Coronal (B) and sagittal (C) reformations of the filling defect. at the segmental level of the right pulmonary artery. UNIDADES DESDE MENOS – 1000 AIRE 0 AGUA MAS 100 METALICA ABOSORCION DE LOS RAYOS S. DENSIDAD NEGATIVA COMPATIBLE ON GRASA.")
36
TAC CON CONTRASTE VENTANA PARA MEDIASTINO
CONTRAST-ENHANCED MULTIDETECTOR ROW SPIRAL CT SHOWING fiLLING DEFECTS (WHITE ARROWS) AT THE SEGMENTAL LEVEL OF THE RIGHT AND LEFT PULMONARY ARTERIES (A). Region of interest measurements showed negative mean attenuation values of the fillingDEFECTS, SUGGESTING THE PRESENCE OF FAT TISSUE (mean attenuation values of the emboli at the segmental level of the right and left pulmonary artery were j54 and j42 Hounsfield units, respectively). Coronal (B) and sagittal (C) reformations of the filling defect at the segmental level of the right pulmonary artery. UNIDADES DESDE MENOS – AIRE 0 AGUA MAS 100 METALICA ABOSORCION DE LOS RAYOS S DENSIDAD NEGATIVA COMPATIBLE ON GRASA
 AT THE SEGMENTAL LEVEL OF THE RIGHT AND LEFT PULMONARY ARTERIES (A). Region of interest measurements showed negative mean attenuation values of the fillingDEFECTS, SUGGESTING THE PRESENCE OF FAT TISSUE (mean attenuation values of the emboli at the segmental level of the right and left. pulmonary artery were j54 and j42 Hounsfield units, respectively). Coronal (B) and sagittal (C) reformations of the filling defect. at the segmental level of the right pulmonary artery. UNIDADES DESDE MENOS – 1000 AIRE 0 AGUA MAS 100 METALICA ABOSORCION DE LOS RAYOS S. DENSIDAD NEGATIVA COMPATIBLE ON GRASA.")
37
RESONANCIA MAGNETICA Diffusion-weighted magnetic resonance images (D and E) and T2-weighted magnetic resonance images (1.5 T) (G and H) obtained when the patient was initially seen demonstrate punctuate lesions in the white matter and basal ganglia. Magnetic resonance images (3 T) obtained at follow-up demonstrate resolution of these lesions (F an
 and T2-weighted magnetic resonance images (1.5 T) (G and H) obtained when the. patient was initially seen demonstrate punctuate lesions in the white matter and basal ganglia. Magnetic resonance images (3 T) obtained at follow-up. demonstrate resolution of these lesions (F an.")
38
RESONANCIA MAGNETICA ig. 1. RM cerebral. Corte coronal. (Técnica FLAIR). Las flechas señalan imágenes hiperintensas localizadas en la sustancia blanca periventricular (a) y en ambos hemisferios cerebelosos (b). 2 mediante la cual la grasa es objetivada como señal hiperintensa.
 y en ambos hemisferios cerebelosos (b). 2 mediante la cual la grasa es objetivada como señal hiperintensa.")
39
FIG. 2. Brain MRI, T2 image showing multiple hypersignalling le-
sions. Cerebral MRI examination showing multiple focal lesions of the white matter. Such lesions were widespread in the different areas of the brain.

40
ECOCARDIOGRAMA TRANSESOFAGICO
PARTICULAS DE GRASA EN EL CORAZON DERECHO HIPERTENSION PULMONAR ANOMALIDAS MOTILIDAD DEL VENTRICULO, DILATA, DESPLAZA EL TABIQUE A LA IZQUIERDA ECOCARDIOGRAMA INESTABLE EMBOLO VALVULA TAPONADO ENDOCARDITIS, DISEC¨CION AORTICAThe use of intraoperative transesophageal echocardiography (TEE) has also shown intravasation of fat into the lung vasculature TEE can be extremely helpful in excluding significant pulmonary thromboembolism and regional wall motion abnormalities suggestive of myocardial ischemia, and ruling out other causes of intraoperative hemo- dynamic instability.
 has also. shown intravasation of fat into the lung vasculature. TEE can be extremely helpful in excluding. significant pulmonary thromboembolism and regional wall motion abnormalities. suggestive of myocardial ischemia, and ruling out other causes of intraoperative hemo- dynamic instability.")
41
LAVADO BRONCOALVEOLAR
for the diagnosis of FES. 84,85 Quantification of cells containing fat droplets in bronchial alveolar lavage (BAL) fluid within the first 24 hours after trauma have also been shown to correlate with clinical fat embolism in some studies. 86–89 In the absence of a high load of exogenously delivered fat, BAL fluid that contains more than 30% macrophages laden with lipid inclusions is very suggestive of FES. However, it may not be possible to obtain an adequate number of macrophages for analysis; 90 obtaining BAL is resource intensive (requires bronchoscopy) and is not specific for FES. 8 However, these methods are not yet widely accepted clinically, and their validity is still to be determined Recently, several authors have reported the usefulness of bronchoalveolar lavage fluid analysis (18) and microvascular cytology from Swan-Ganz catheters (19) Figure 3: BAl fluid (Oil-red-O-staining) showing abundantly present lipid inclusions in alveolar macrophages, magnification 400 X. On day 5, a broncho-alveolar lavage was performed to elucidate the cause of the rapidly progressive ArdS. microscopic inspection of the lavage fluid showed fat inclusions (Oil-red-O-staining), present in more than 70 % of the alveolar macrophages (Figure 3). > 30 % MACROFAGOS ALVEOLARES INCLUSIONES LIPIDICAS EN LAS PRIMERAS 24 HORAS
 fluid within the first. 24 hours after trauma have also been shown to correlate with clinical fat embolism. in some studies. 86–89. In the absence of a high load of exogenously delivered fat, BAL fluid that contains more than 30% macrophages laden with lipid inclusions is. very suggestive of FES. However, it may not be possible to obtain an adequate. number of macrophages for analysis; 90. obtaining BAL is resource intensive (requires. bronchoscopy) and is not specific for FES. 8. However, these methods are not yet widely accepted clinically, and their validity is still to be determined. Recently, several authors have reported the usefulness of bronchoalveolar lavage fluid analysis (18) and microvascular cytology from Swan-Ganz catheters (19) Figure 3: BAl fluid (Oil-red-O-staining) showing abundantly. present lipid inclusions in alveolar macrophages, magnification X. On day 5, a broncho-alveolar lavage was performed to. elucidate the cause of the rapidly progressive ArdS. microscopic inspection of the lavage fluid showed. fat inclusions (Oil-red-O-staining), present in more. than 70 % of the alveolar macrophages (Figure 3). > 30 % MACROFAGOS ALVEOLARES. INCLUSIONES LIPIDICAS. EN LAS PRIMERAS 24 HORAS.")
42
MANEJO TRATAMIENTO ES PREVENCION Y DE SOPORTE SOPORTE VENTILATORIO
MANEJO DEL SHOCK ESTABILIDAD HEMODINAMICA ALBUMINA G LIGA 100 MG ACIDOS GRASOS CHOQUE OBSTRUCTIVO - FALLA VENTRICULO DERECHO SOPORTE CON DOBUTAMINA EXAMEN NEUROLOGICO EDEMA CEREBRAL

43
CORTICOIDES PREVENCION DE SEG PTE FX HUESO LARGO 6 ADECUADOS ANALISIS
REDUCEN EL RIESGO 77 % IC 40 – 91 7 PACIENTES TRATADOS PARA PREVENIR 1 CASO NO ENCONTRARON DIFERENCIAS EN MORTALIDAD – INFECCION – CONSOLIDACION > 1970 POLITRAUMATIZADOS EXCLUIDOS There is no evidence be avoided. It is also important to emphasize that the effect demonstrated does not apply to polytraumatized patients, since these were excluded from the clinical trials that, after a diagnosis of FES has been established, specific therapy provides any benefit. epidemiologic characteristics (age bracket) and clinical characteristics (area of fracture, type of trauma, and number of fractures) to evaluate the risk of developing FES. he effect of corticosteroids on FES might be related to the stabilization of the alveolar- capillary membrane/complement system, reduction of interstitial edema, and inhibition of the inflam- matory response, as well as to delayed platelet aggregation. ALI induced by fat embolism. 118 High-dose methylprednisone (90 mg/kg over 4 days) or a lower dose prophylactically (6 mg/kg over 2 days) has shown some clinical efficacy in improving outcomes. 119 Steroids are thought to limit the increase of FFAs, stabilize the membranes, and inhibit complement-mediated leuko- cyte aggregation. However, high-dose methylprednisolone can also have significant side effects. Therefore, the use or methylprednisolone has not been proved by any large-scale prospective trials and its routine use cannot be advocated.
 and clinical characteristics (area of fracture, type of. trauma, and number of fractures) to evaluate the. risk of developing FES. he effect of corticosteroids on FES. might be related to the stabilization of the alveolar- capillary membrane/complement system, reduction. of interstitial edema, and inhibition of the inflam- matory response, as well as to delayed platelet. aggregation. ALI induced by fat embolism High-dose methylprednisone (90 mg/kg. over 4 days) or a lower dose prophylactically (6 mg/kg over 2 days) has shown. some clinical efficacy in improving outcomes Steroids are thought to limit the. increase of FFAs, stabilize the membranes, and inhibit complement-mediated leuko- cyte aggregation. However, high-dose methylprednisolone can also have significant. side effects. Therefore, the use or methylprednisolone has not been proved by any. large-scale prospective trials and its routine use cannot be advocated.")
44
La inmovilización precoz de la fractura reduce claramente el riesgo de desarrollar una
SEG.La profilaxis del SEG habría de empezar ya en el sitio del accidente evitando la hipovolemia y fijando el foco de fractura. dosis más recomendada de metilprednisolona es de 1.5 mgr/ kg/8h durante 48 h. Se suelen evitar dosis mayores por predisposición a padecer infecciones, sobretodo en pacientes con fracturas abiertas. Un aspecto crucial a considerar, entre otros, en la profilaxis del embolismo graso seria el momento de la fijación quirúrgica. Esta idea está basada en el concepto del damage control16. Básicamente habría que tener en cuanta el estado basal del paciente, si presenta TCE, traumatismo torácico, estabilidad hemodinámica y la presencia o no de foramen oval permeable para su valoración en conjunto y decidir de una forma multidisciplinar cuándo y de qué forma se realiza la fijación quirúrgica precoz y/o tardía de las diferentes fracturas y/o lesiones del paciente.( V

45
PREVENCION .. DESDE EL TRASLADO
FIJACION TEMPRANA DE LA FRACTURA < 24 HORAS REDUCE LA LIBERACION DE GRASA MOVILIDAD REDUCCION 70 % DE COMPLICACIONES PULMONARES FIJACION EXTERNA INICIAL INMOVILIZACION CON ENTABLILLADO

46
PREVENCION CIRUGIA DE CONTROL DE DAÑOS
TECNICAS INTRAMEDULARES > RIESGO SEG CLAVOS NO FRESADOS EMBOLIZAN MENOS VENTILAR EL CANAL ANTES DE CEMENTAR CEMENTO PREPARADO AL VACIO LAVADO DEL CANAL MEDULAR

47
INSUFICIENCIA RESPIRATORIA PROGRESIVA
PARA RECORDAR COMPLICACION DEL POLITRAUMATIZADO CON FX DE HUESOS LARGOS INSUFICIENCIA RESPIRATORIA TRIADA ALTERACIONES NEUROLOGICAS PETEQUIAS INSUFICIENCIA RESPIRATORIA PROGRESIVA ALTERACIONES NEUROLOGICAS PETEQUIAS SINTOMAS USUALMENTE INICIAN < 72 HORAS LA FIJACION TEMPRANA DE LA FRACTURA < RIESGO TRATAMIENTO ES DE SOPORTE

Presentaciones similares











>")







