Descargar la presentación
La descarga está en progreso. Por favor, espere

1
SISTEMAS CEREBRALES DE LA MEMORIA A LARGO PLAZO
Psicología del Aprendizaje Curso Prof. L.Aguado Facultad de Psicología Universidad Complutense de Madrid Tema 7 SISTEMAS CEREBRALES DE LA MEMORIA A LARGO PLAZO

2
Memoria explícita y memoria implícita
Evidencia empírica 1) Estudios neuropsicológicos -síndrome amnésico (amnesia de lóbulos temporales) 2) Disociaciones experimentales en sujetos normales -pruebas de memoria implícita (priming, condicionamiento, aprendizaje perceptivo…) -una misma variable afecta de distinto modo a distintas medidas de memoria
 Estudios neuropsicológicos. -síndrome amnésico (amnesia de lóbulos temporales) 2) Disociaciones experimentales en sujetos normales. -pruebas de memoria implícita (priming, condicionamiento, aprendizaje perceptivo…) -una misma variable afecta de distinto modo a distintas medidas de memoria.")
3
Memoria explícita y memoria implícita
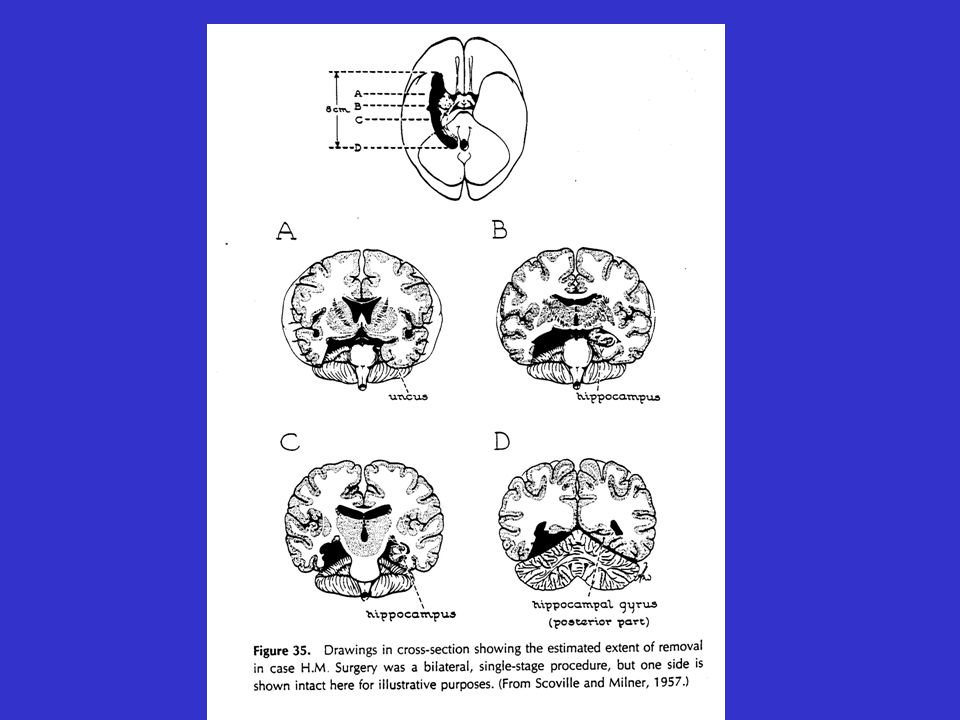
El caso HM (estudio original, Scoville & Milner, 1957) -epilepsia a consecuencia de un accidente de bicicleta -1933, 7 años de edad- (10 ataques leves diarios, uno grave semanal) -tratamiento anticonvulsivo ineficaz -operación de neurocirugía : -lóbulo temporal medial bilateral: hipocampo / amígdala (tejido en torno al tercer ventrículo) -reducción de frecuencia de ataques Artículo sobre H.M en WIKIPEDIA çHM (also known as "H.M." and "Henry M.," born 1926 in Connecticut) is an anonymous memory-impaired patient who has been widely studied since the late 1950s and has been very important in the development of theories that explain the link between brain function and memory, and in the development of cognitive neuropsychology, a branch of psychology that studies brain injury to infer normal psychological function. He is still alive today and resides in a care institute located in Hartford, Connecticut, where he remains in ongoing investigation.[1] Audio-recordings from the 1990s of him talking to scientists were released in early Recordings and Story of HM through NPR radio History HM suffered from intractable epilepsy that has been often—though inconclusively—attributed to a bicycle accident at the age of nine. He suffered from partial seizures for many years, and then several tonic-clonic seizures following his sixteenth birthday. In 1953, HM was referred to , a surgeon at Hartford Hospital, for treatment. Scoville localized HM's epilepsy to his medial temporal lobe (MTLs) and suggested surgical resection of the MTLs as a treatment. On September 1, 1953, Scoville removed parts of HM's medial temporal lobe on both sides of his brain. HM lost approximately two-thirds of his hippocampal formation, parahippocampal gyrus (all his entorhinal cortex was destroyed), and amygdala. His hippocampus appears entirely nonfunctional because the remaining 2 cm of hippocampal tissue appears atrophic and because the entire entorhinal (which forms the major sensory input to the hippocampus) was destroyed. Some of his anterolateral temporal cortex was also destroyed. After the surgery he suffered from severe anterograde amnesia: although his short-term memory was intact, he could not commit new events to long-term memory. According to some scientists (e.g., Schmolck, Kensinger, Corkin, & Squire, 2002), HM is impaired in his ability to form new semantic knowledge but researchers argue over the extent of this impairment. He also suffered moderate retrograde amnesia, and could not remember most events in the 3–4 -day period before surgery, and some events up to 11 years before, meaning that his amnesia was temporally graded. However, his ability to form long-term procedural memories was still intact; thus he could, as an example, learn new motor skills, despite not being able to remember learning them. The case was first reported in a paper by Scoville and Brenda Milner in 1957. [edit] Insights into memory formation HM has been important not only for the knowledge he has provided about memory impairment and amnesia, but also because his exact brain surgery has allowed a good understanding of how particular areas of the brain may be linked to specific processes hypothesized to occur in memory formation. In this way, he has provided vital information about brain pathology, and has helped form theories of normal memory function. Particularly, that he seems to be able to complete tasks that require recall from short-term memory and procedural memory but not long term episodic memory suggests that recall from these memory systems may be mediated, at least in part, by different areas of the brain. Similarly, that HM cannot create new long-term memories, but can recall long-term memories that existed well before his surgery suggests that encoding and retrieval of long-term memory information may also be mediated by distinct systems. [edit] HM's lifelong contribution to science The study of the patient HM has revolutionized our understanding of the organization of human memory. It has provided broad evidence for the rejection of old theories, as well as the formation of new theories on human memory, in particular about its processes and the underlying neural structures (cf. Kolb & Whishaw, 1996). In the following, some of the major insights are outlined. [edit] Surgery Most of HM's hippocampus was removed bilaterally. Since the age of 10, the patient HM suffered from increasing epileptic seizures. Eventually the seizures became so intense and frequent that by the age of 27 his doctors suggested removing parts of the brain that were thought to be responsible for his disorder. In 1953, the surgeon Scoville performed brain surgery on HM's medial temporal lobes. Regarding the exact areas of surgery, Scoville & Milner (1957) noted: “bilateral medial temporal lobe resection was carried out, extending posteriorly for a distance of 8 cm from the midpoints of the tips of the temporal lobes, with the temporal horns constituting the lateral edges of resection” (p. 107). HM recovered from the operation, which eased his epileptic seizures to a manageable degree. However, the surgery had induced serious side-effects, which were first described by Scoville & Milner (1957) as “a complete loss of memory for events [...], together with a partial retrograde amnesia for the three years leading up to his operation” (p. 108). Furthermore, they found that “early memories are seemingly normal and there is no impairment of personality or general intelligence” (p. 108). [edit] Amnesia HM's general condition has been described as heavy anterograde amnesia, as well as temporally graded retrograde amnesia (Smith & Kosslyn, 2007). HM is highly unable to form new long-term memories of new events or new semantic knowledge – he basically lives in the past (Corkin, 2002). Since HM did not show any memory impairment before the surgery, the removal of the medial temporal lobes can be held responsible for his memory disorder. Consequently, the medial temporal lobes can be assumed to be a major component involved in the formation of semantic and episodic long-term memories (cf. medial temporal lobes described as a convergence zone for episodic encoding in Smith & Kosslyn, 2007). Further evidence for this assumption has been gained by studies of other patients with lesions of their medial temporal lobe structures (cf. Kolb & Whishaw, 1996; Scoville & Milner, 1957). Despite of his amnesic symptoms, HM performs quite normally in tests of intellectual ability and shows largely-intact language abilities indicating that some memory functions (e.g., short-term stores, stores for words, phonemes etc.) were not impaired by the surgery (Smith & Kosslyn, 2007; Corkin, 2002). HM is able to remember information over short intervals of time. This has been tested in a working memory experiment involving the recall of previously presented numbers; in fact, his performance is no worse than that of control subjects (Smith & Kosslyn, 2007). This finding provides evidence that working memory does not rely on . It further supports the general distinction between short-term and long-term stores of memory (Kolb & Whishaw, 1996). HM's largely intact language abilities provide evidence that language production and comprehension, as well as lexical memory, are independent of the medial temporal structures (Corkin, 2002). [edit] Motor skill learning In addition to his intact working memory and intellectual abilities, studies of HM's ability to acquire new motor skills demonstrated preserved motor learning (Corkin, 2002). In a study conducted by Milner in the early 1960s, HM acquired the new skill of drawing a figure by looking at its reflection in a mirror (Corkin, 2002). Further evidence for intact motor learning was provided in a study carried out by Corkin (1968). In this study, HM was tested on three different motor learning tasks and HM demonstrated full motor learning abilities in all three tasks. HM's ability to learn certain problem-solving procedures has also been shown with the Tower of Hanoi task (Kolb & Whishaw, 1996). Experiments involving repetition priming underscored HM's ability to acquire implicit (non-conscious) memories, in contrast to his inability to acquire new explicit semantic and episodic memories (Corkin, 2002). These findings provide evidence that memory of skills and repetition priming rely on different neural structures than memories of episodes and facts; whereas procedural memory and repetition priming do not rely on the medial temporal structures removed in HM, semantic and episodic memory do (cf. Corkin, 1984). The dissociation of HM's implicit and explicit learning abilities along their underlying neural structures has served as an important contribution to our understanding of human memory: Long-term memories are not unitary and can be differentiated as being either declarative and non-declarative (Smith & Kosslyn, 2007). [edit] Spatial memory According to Corkin (2002), studies of HM's memory abilities have also provided insights regarding the neural structures responsible for spatial memory and processing of spatial information. Despite his general inability to form new episodic or factual long-term memories, as well as his heavy impairment on certain spatial memory tests, HM was able to draw a quite detailed map of the topographical layout of his residence. This finding is remarkable since HM had moved to the house five years after his surgery and hence, given his severe anterograde amnesia and insights from other cases, the common expectation was that the acquisition of topographical memories would have been impaired as well. Corkin (2002) hypothesized that HM “was able to construct a cognitive map of the spatial layout of his house as the result of daily locomotion from room to room” (p. 156). Regarding the underlying neural structures, Corkin (2002) argues that HM's ability to acquire the floor plan is due to partly intact structures of his spatial processing network (e.g. the posterior part of his parahippocampal gyrus). In addition to his , HM showed some learning in a picture memorization-recognition task, as well as in a famous faces recognition test, but in the latter only when he was provided with a phonemic cue. HM's positive performance in the picture recognition task might be due to spared parts of his . Furthermore, Corkin (2002) argues that despite HM's general inability to form new declarative memories, he seems to be able to acquire small and impoverished pieces of information regarding public life (e.g., cued retrieval of celebrities names). These findings underscore the importance of HM's spared extrahippocampal sites in semantic and recognition memory and enhance our understanding of the interrelations between the different medial temporal lobe structures. HM's heavy impairment in certain spatial tasks provides further evidence for the association of the hippocampus with spatial memory (Kolb & Whishaw, 1996). [edit] Memory consolidation Another contribution of HM to our understanding of human memory regards the neural structures of the memory consolidation process, which is responsible for forming stable long-term memories (Eysenck & Keane, 2005). HM displayed a temporally graded retrograde amnesia in the way that he “could still recall childhood memories, but he had difficulty remembering events that happened during the years immediately preceding the surgery” (Smith & Kosslyn, 2007, p. 214). His old memories were not impaired, whereas the ones relatively close to the surgery were. This is evidence that the older childhood memories do not rely on the medial temporal lobe, whereas the younger long-term memories seem to do so (Smith & Kosslyn, 2007). The medial temporal structures, which were removed in the surgery, are hypothesized to be involved in the consolidation of memories in the way that “interactions between the medial temporal lobe and various lateral cortical regions are thought to store memories outside the medial temporal lobes by slowly forming direct links between the cortical representations of the experience” (Smith & Kosslyn, 2007, p. 214).
 -epilepsia a consecuencia de un accidente de bicicleta -1933, 7 años de edad- (10 ataques leves diarios, uno grave semanal) -tratamiento anticonvulsivo ineficaz. -operación de neurocirugía : -lóbulo temporal medial bilateral: hipocampo / amígdala (tejido en torno al tercer ventrículo) -reducción de frecuencia de ataques. Artículo sobre H.M en WIKIPEDIA. çHM (also known as H.M. and Henry M., born 1926 in Connecticut) is an anonymous memory-impaired patient who has been widely studied since the late 1950s and has been very important in the development of theories that explain the link between brain function and memory, and in the development of cognitive neuropsychology, a branch of psychology that studies brain injury to infer normal psychological function. He is still alive today and resides in a care institute located in Hartford, Connecticut, where he remains in ongoing investigation.[1] Audio-recordings from the 1990s of him talking to scientists were released in early Recordings and Story of HM through NPR radio. History. HM suffered from intractable epilepsy that has been often—though inconclusively—attributed to a bicycle accident at the age of nine. He suffered from partial seizures for many years, and then several tonic-clonic seizures following his sixteenth birthday. In 1953, HM was referred to , a surgeon at Hartford Hospital, for treatment. Scoville localized HM s epilepsy to his medial temporal lobe (MTLs) and suggested surgical resection of the MTLs as a treatment. On September 1, 1953, Scoville removed parts of HM s medial temporal lobe on both sides of his brain. HM lost approximately two-thirds of his hippocampal formation, parahippocampal gyrus (all his entorhinal cortex was destroyed), and amygdala. His hippocampus appears entirely nonfunctional because the remaining 2 cm of hippocampal tissue appears atrophic and because the entire entorhinal (which forms the major sensory input to the hippocampus) was destroyed. Some of his anterolateral temporal cortex was also destroyed. After the surgery he suffered from severe anterograde amnesia: although his short-term memory was intact, he could not commit new events to long-term memory. According to some scientists (e.g., Schmolck, Kensinger, Corkin, & Squire, 2002), HM is impaired in his ability to form new semantic knowledge but researchers argue over the extent of this impairment. He also suffered moderate retrograde amnesia, and could not remember most events in the 3–4 -day period before surgery, and some events up to 11 years before, meaning that his amnesia was temporally graded. However, his ability to form long-term procedural memories was still intact; thus he could, as an example, learn new motor skills, despite not being able to remember learning them. The case was first reported in a paper by Scoville and Brenda Milner in [edit] Insights into memory formation. HM has been important not only for the knowledge he has provided about memory impairment and amnesia, but also because his exact brain surgery has allowed a good understanding of how particular areas of the brain may be linked to specific processes hypothesized to occur in memory formation. In this way, he has provided vital information about brain pathology, and has helped form theories of normal memory function. Particularly, that he seems to be able to complete tasks that require recall from short-term memory and procedural memory but not long term episodic memory suggests that recall from these memory systems may be mediated, at least in part, by different areas of the brain. Similarly, that HM cannot create new long-term memories, but can recall long-term memories that existed well before his surgery suggests that encoding and retrieval of long-term memory information may also be mediated by distinct systems. [edit] HM s lifelong contribution to science. The study of the patient HM has revolutionized our understanding of the organization of human memory. It has provided broad evidence for the rejection of old theories, as well as the formation of new theories on human memory, in particular about its processes and the underlying neural structures (cf. Kolb & Whishaw, 1996). In the following, some of the major insights are outlined. [edit] Surgery. Most of HM s hippocampus was removed bilaterally. Since the age of 10, the patient HM suffered from increasing epileptic seizures. Eventually the seizures became so intense and frequent that by the age of 27 his doctors suggested removing parts of the brain that were thought to be responsible for his disorder. In 1953, the surgeon Scoville performed brain surgery on HM s medial temporal lobes. Regarding the exact areas of surgery, Scoville & Milner (1957) noted: bilateral medial temporal lobe resection was carried out, extending posteriorly for a distance of 8 cm from the midpoints of the tips of the temporal lobes, with the temporal horns constituting the lateral edges of resection (p. 107). HM recovered from the operation, which eased his epileptic seizures to a manageable degree. However, the surgery had induced serious side-effects, which were first described by Scoville & Milner (1957) as a complete loss of memory for events [...], together with a partial retrograde amnesia for the three years leading up to his operation (p. 108). Furthermore, they found that early memories are seemingly normal and there is no impairment of personality or general intelligence (p. 108). [edit] Amnesia. HM s general condition has been described as heavy anterograde amnesia, as well as temporally graded retrograde amnesia (Smith & Kosslyn, 2007). HM is highly unable to form new long-term memories of new events or new semantic knowledge – he basically lives in the past (Corkin, 2002). Since HM did not show any memory impairment before the surgery, the removal of the medial temporal lobes can be held responsible for his memory disorder. Consequently, the medial temporal lobes can be assumed to be a major component involved in the formation of semantic and episodic long-term memories (cf. medial temporal lobes described as a convergence zone for episodic encoding in Smith & Kosslyn, 2007). Further evidence for this assumption has been gained by studies of other patients with lesions of their medial temporal lobe structures (cf. Kolb & Whishaw, 1996; Scoville & Milner, 1957). Despite of his amnesic symptoms, HM performs quite normally in tests of intellectual ability and shows largely-intact language abilities indicating that some memory functions (e.g., short-term stores, stores for words, phonemes etc.) were not impaired by the surgery (Smith & Kosslyn, 2007; Corkin, 2002). HM is able to remember information over short intervals of time. This has been tested in a working memory experiment involving the recall of previously presented numbers; in fact, his performance is no worse than that of control subjects (Smith & Kosslyn, 2007). This finding provides evidence that working memory does not rely on . It further supports the general distinction between short-term and long-term stores of memory (Kolb & Whishaw, 1996). HM s largely intact language abilities provide evidence that language production and comprehension, as well as lexical memory, are independent of the medial temporal structures (Corkin, 2002). [edit] Motor skill learning. In addition to his intact working memory and intellectual abilities, studies of HM s ability to acquire new motor skills demonstrated preserved motor learning (Corkin, 2002). In a study conducted by Milner in the early 1960s, HM acquired the new skill of drawing a figure by looking at its reflection in a mirror (Corkin, 2002). Further evidence for intact motor learning was provided in a study carried out by Corkin (1968). In this study, HM was tested on three different motor learning tasks and HM demonstrated full motor learning abilities in all three tasks. HM s ability to learn certain problem-solving procedures has also been shown with the Tower of Hanoi task (Kolb & Whishaw, 1996). Experiments involving repetition priming underscored HM s ability to acquire implicit (non-conscious) memories, in contrast to his inability to acquire new explicit semantic and episodic memories (Corkin, 2002). These findings provide evidence that memory of skills and repetition priming rely on different neural structures than memories of episodes and facts; whereas procedural memory and repetition priming do not rely on the medial temporal structures removed in HM, semantic and episodic memory do (cf. Corkin, 1984). The dissociation of HM s implicit and explicit learning abilities along their underlying neural structures has served as an important contribution to our understanding of human memory: Long-term memories are not unitary and can be differentiated as being either declarative and non-declarative (Smith & Kosslyn, 2007). [edit] Spatial memory. According to Corkin (2002), studies of HM s memory abilities have also provided insights regarding the neural structures responsible for spatial memory and processing of spatial information. Despite his general inability to form new episodic or factual long-term memories, as well as his heavy impairment on certain spatial memory tests, HM was able to draw a quite detailed map of the topographical layout of his residence. This finding is remarkable since HM had moved to the house five years after his surgery and hence, given his severe anterograde amnesia and insights from other cases, the common expectation was that the acquisition of topographical memories would have been impaired as well. Corkin (2002) hypothesized that HM was able to construct a cognitive map of the spatial layout of his house as the result of daily locomotion from room to room (p. 156). Regarding the underlying neural structures, Corkin (2002) argues that HM s ability to acquire the floor plan is due to partly intact structures of his spatial processing network (e.g. the posterior part of his parahippocampal gyrus). In addition to his , HM showed some learning in a picture memorization-recognition task, as well as in a famous faces recognition test, but in the latter only when he was provided with a phonemic cue. HM s positive performance in the picture recognition task might be due to spared parts of his . Furthermore, Corkin (2002) argues that despite HM s general inability to form new declarative memories, he seems to be able to acquire small and impoverished pieces of information regarding public life (e.g., cued retrieval of celebrities names). These findings underscore the importance of HM s spared extrahippocampal sites in semantic and recognition memory and enhance our understanding of the interrelations between the different medial temporal lobe structures. HM s heavy impairment in certain spatial tasks provides further evidence for the association of the hippocampus with spatial memory (Kolb & Whishaw, 1996). [edit] Memory consolidation. Another contribution of HM to our understanding of human memory regards the neural structures of the memory consolidation process, which is responsible for forming stable long-term memories (Eysenck & Keane, 2005). HM displayed a temporally graded retrograde amnesia in the way that he could still recall childhood memories, but he had difficulty remembering events that happened during the years immediately preceding the surgery (Smith & Kosslyn, 2007, p. 214). His old memories were not impaired, whereas the ones relatively close to the surgery were. This is evidence that the older childhood memories do not rely on the medial temporal lobe, whereas the younger long-term memories seem to do so (Smith & Kosslyn, 2007). The medial temporal structures, which were removed in the surgery, are hypothesized to be involved in the consolidation of memories in the way that interactions between the medial temporal lobe and various lateral cortical regions are thought to store memories outside the medial temporal lobes by slowly forming direct links between the cortical representations of the experience (Smith & Kosslyn, 2007, p. 214).")
6
Resultados de los estudios con HM
(estudio original, Scoville & Milner, 1957) * conservación de funciones perceptivas y cognitivas -lenguaje, percepción y razonamiento normales -memoria inmediata normal -amplitud de MCP normal * déficit de memoria de largo plazo: -amnesia retrógrada graduada temporalmente -amnesia anterógrada: dificultades de aprendizaje * disociación memoria implícita / explícita Does H.M. have a sense of self? (tomado del artículo: What’s new with the amnesic patient H.M.?, de Suzanne Coirkin, Nature Reviews Neuroscience, 2002). Philosophers, psychologists and neuroscientists have proposed that,without memory, a person lacks an identity — a sense of self. By this view, H.M. should not have a sense of who he is. The following observations are worthy of consideration in this regard. Amnesia is not an all-or-nothing condition, and even H.M., from time to time, has meagre conscious recollections of information encountered postoperatively6. In addition, he has memories of his childhood, which include vacations with his parents and information about a number of relatives, although these memories seem to be semanticized65. For example, in trying to elicit an autobiographical memory, I asked him, “What is your favourite memory that you have of your mother?”“Well I, that she’s just my mother.” “But can you remember any particular event that was special — like a holiday, Christmas, birthday, Easter?”“There I have an argument with myself about Christmas time.”“What about Christmas?” “Well, ’cause my daddy was from the South, and they didn’t celebrate down there like they do up here — in the North. Like they don’t have the trees or anything like that. And uh, but he came North even though he was born down Louisiana. And I know the name of the town he was born in.”H.M. was unable to supply an episodic memory of his mother or his father — he could not narrate even one event that occurred at a specific time and place. In view of the lively disagreement about the participation of the hippocampus in memory consolidation and storage, it would be useful to know the status of H.M.’s premorbid semantic memory relative to his premorbid episodic memory. The ‘standard’ model of consolidation66–69 predicts that remote episodic and semantic memory should be equivalent. By contrast, the multiple-trace theory65,70–73 predicts a dissociation within remote memory such that autobiographical memory is the most severely affected by MTL lesions, whereas memory for personal semantics, public events and famous people is less severely affected. Although our preliminary results favour the latter view, a definitive answer awaits the results of more rigorous experiments that are now underway with H.M. and other amnesic patients. Although H.M.’s remote memories do not contain as much detail as those of control participants, they do provide some fodder for his self-concept. Furthermore, beyond those fragmentary memories, he has beliefs, desires and values that are always present. For example, he believes that doing crossword puzzles helps him to remember words and is fun.He is altruistic: when I asked him to tell me about Dr Scoville (with whom H.M. had several appointments before his operation) he said, “He did medical research on people — all kinds of people.What he learned about me helped others too, and I’m glad about that.” His social behaviour is appropriate and courteous. Years ago, when he and I were walking from the MIT Clinical Research Center to the Psychology Department, he would cup my elbow with his hand to guide me down the sidewalk. He has high moral standards with respect to right and wrong in his personal conduct, which is consistent with the preservation of his orbitofrontal cortex74. He has a conscience. For example, when explaining why he could not fulfil his dream of being a neurosurgeon, he cites the fact that he wears glasses, and that blood might spurt up onto his glasses, creating an obstacle to his vision and causing him to miss his target in the patient’s brain, thereby causing the patient harm. In addition, he has good insight into his memory disorder. When I asked him, “What do you do to try to remember?” he replied, “Well, that I don’t know ’cause I don’t remember (laugh) what I tried.” He has a sense of humour, and often makes jokes. Another aspect of a sense of self is knowledge of one’s appearance and physical state. H.M. describes himself as ‘thin but heavy.’He does not know his age, or whether he has grey hair. On one occasion when I showed him an old photograph of himself and his mother, he replied that the man looked like his father, but that it could not be his father because his father does not wear glasses. His ability to interpret and report internal states is diminished75. Specifically, he has an impaired ability to identify and respond to painful stimuli, and shows no difference in his ratings of hunger and thirst made before and after a meal. A suggestion as to the neural substrate of self comes from Miller and colleagues76. They posit that the self comprises three cognitive domains (semantic knowledge, autobiographical memories and will), and that the first two are mediated by frontal lobe processes. Although knowledge of self is stored outside the frontal lobes, these structures are specialized for accessing, integrating and maintaining this information. Because H.M.’s frontal lobes are intact18, he has the substrate for organizing his meagre remote memories, perhaps to maintain a sense of self.Whether H.M. in fact has a sense of self is a matter for the reader to ponder. When H.M. looks in the mirror Students, scientists and lay people are fascinated by H.M.’s case history. When they hear about his condition, an abundance of questions follows. The most commonly asked question is: what happens when H.M. looks in the mirror? You could imagine that he might express shock and incredulity at the sight of an old man, because he does not remember that decades have elapsed since 1953 when his memory was last intact. I can report the following anecdotal evidence: when he looks at himself in a mirror, he shows no change in facial expression, his conversation is matter-offact, and he does not seem to be at all upset. On one occasion he was asked, “What do you think about how you look?”He replied, “I’m not a boy.” This response reveals his sense of humour and his acceptance of the image he sees in the mirror. Although H.M.’s lack of concern might stem from his having had a bilateral amygdalectomy, it could be the case that he actually perceives his face as familiar. This sense of familiarity would be the result of repeated daily exposure to his face year after year. The neural representation of his face is updated daily, probably in his intact fusiform face area, and perhaps through interactions with the posterior parahippocampal cortex (perirhinal cortex), which is believed to support familiarity discrimination29,60.
 * conservación de funciones perceptivas y cognitivas. -lenguaje, percepción y razonamiento normales. -memoria inmediata normal. -amplitud de MCP normal. * déficit de memoria de largo plazo: -amnesia retrógrada graduada temporalmente. -amnesia anterógrada: dificultades de aprendizaje. * disociación memoria implícita / explícita. Does H.M. have a sense of self (tomado del artículo: What’s new with the amnesic. patient H.M. , de Suzanne Coirkin, Nature Reviews Neuroscience, 2002). Philosophers, psychologists and neuroscientists have proposed that,without memory, a. person lacks an identity — a sense of self. By. this view, H.M. should not have a sense of. who he is. The following observations are. worthy of consideration in this regard. Amnesia is not an all-or-nothing condition, and even H.M., from time to time, has. meagre conscious recollections of information. encountered postoperatively6. In addition, he has memories of his childhood, which include vacations with his parents and. information about a number of relatives, although these memories seem to be semanticized65. For example, in trying to elicit an. autobiographical memory, I asked him, What is your favourite memory that you. have of your mother Well I, that she’s just. my mother. But can you remember any. particular event that was special — like a. holiday, Christmas, birthday, Easter There. I have an argument with myself about. Christmas time. What about Christmas Well, ’cause my daddy was from the South, and they didn’t celebrate down there like. they do up here — in the North. Like they. don’t have the trees or anything like that. And uh, but he came North even though he. was born down Louisiana. And I know the. name of the town he was born in. H.M. was. unable to supply an episodic memory of his. mother or his father — he could not narrate. even one event that occurred at a specific. time and place. In view of the lively disagreement. about the participation of the hippocampus. in memory consolidation and. storage, it would be useful to know the status. of H.M.’s premorbid semantic memory relative. to his premorbid episodic memory. The. ‘standard’ model of consolidation66–69 predicts. that remote episodic and semantic. memory should be equivalent. By contrast, the multiple-trace theory65,70–73 predicts a. dissociation within remote memory such. that autobiographical memory is the most. severely affected by MTL lesions, whereas. memory for personal semantics, public. events and famous people is less severely. affected. Although our preliminary results. favour the latter view, a definitive answer. awaits the results of more rigorous experiments. that are now underway with H.M. and other amnesic patients. Although H.M.’s remote memories do. not contain as much detail as those of control. participants, they do provide some fodder. for his self-concept. Furthermore, beyond those fragmentary memories, he. has beliefs, desires and values that are. always present. For example, he believes. that doing crossword puzzles helps him to. remember words and is fun.He is altruistic: when I asked him to tell me about Dr Scoville. (with whom H.M. had several appointments. before his operation) he said, He. did medical research on people — all kinds. of people.What he learned about me helped. others too, and I’m glad about that. His. social behaviour is appropriate and courteous. Years ago, when he and I were walking. from the MIT Clinical Research Center to. the Psychology Department, he would cup. my elbow with his hand to guide me down. the sidewalk. He has high moral standards. with respect to right and wrong in his personal. conduct, which is consistent with the. preservation of his orbitofrontal cortex74. He has a conscience. For example, when. explaining why he could not fulfil his. dream of being a neurosurgeon, he cites the. fact that he wears glasses, and that blood. might spurt up onto his glasses, creating an. obstacle to his vision and causing him to. miss his target in the patient’s brain, thereby. causing the patient harm. In addition, he. has good insight into his memory disorder. When I asked him, What do you do to try. to remember he replied, Well, that I don’t. know ’cause I don’t remember (laugh) what. I tried. He has a sense of humour, and. often makes jokes. Another aspect of a sense of self is knowledge. of one’s appearance and physical state. H.M. describes himself as ‘thin but heavy.’He. does not know his age, or whether he has grey. hair. On one occasion when I showed him an. old photograph of himself and his mother, he. replied that the man looked like his father, but. that it could not be his father because his. father does not wear glasses. His ability to. interpret and report internal states is diminished75. Specifically, he has an impaired ability. to identify and respond to painful stimuli, and. shows no difference in his ratings of hunger. and thirst made before and after a meal. A suggestion as to the neural substrate of. self comes from Miller and colleagues76. They. posit that the self comprises three cognitive. domains (semantic knowledge, autobiographical. memories and will), and that the. first two are mediated by frontal lobe. processes. Although knowledge of self is. stored outside the frontal lobes, these structures. are specialized for accessing, integrating. and maintaining this information. Because. H.M.’s frontal lobes are intact18, he has the. substrate for organizing his meagre remote. memories, perhaps to maintain a sense of. self.Whether H.M. in fact has a sense of self. is a matter for the reader to ponder. When H.M. looks in the mirror. Students, scientists and lay people are fascinated. by H.M.’s case history. When they. hear about his condition, an abundance of. questions follows. The most commonly. asked question is: what happens when. H.M. looks in the mirror You could imagine. that he might express shock and. incredulity at the sight of an old man, because he does not remember that decades. have elapsed since 1953 when his memory. was last intact. I can report the following. anecdotal evidence: when he looks at himself. in a mirror, he shows no change in facial. expression, his conversation is matter-offact, and he does not seem to be at all upset. On one occasion he was asked, What do. you think about how you look He replied, I’m not a boy. This response reveals his. sense of humour and his acceptance of the. image he sees in the mirror. Although. H.M.’s lack of concern might stem from his. having had a bilateral amygdalectomy, it. could be the case that he actually perceives. his face as familiar. This sense of familiarity. would be the result of repeated daily exposure. to his face year after year. The neural. representation of his face is updated daily, probably in his intact fusiform face area, and perhaps through interactions with the. posterior parahippocampal cortex (perirhinal. cortex), which is believed to support. familiarity discrimination29,60.")
7
Conservación MCP en amnesia de lóbulos temporales

8
Amnesia retrógrada gradual

9
Capacidades de memoria conservadas en amnesia de lóbulos temporales (“síndrome amnésico”)
* adquisición de destrezas percepto-motoras * efectos de exposición perceptiva * Efectos de “priming” perceptivo * condicionamiento pavloviano simple * adquisición de destrezas cognitivas Característica común * disociación entre uso del conocimiento adquirido (memoria implícita) y recuerdo/conciencia del aprendizaje (memoria explícita)
 y recuerdo/conciencia del aprendizaje (memoria explícita)")
10
HM: adquisición de habilidades percepto-motoras
LECTURA EN ESPEJO Día 1 Día 2 Dia 3 Día 94 Día 1 Día 2 Dia 3 Día 94

11
HM: adquisición de habilidades percepto-motoras
(dibujo en espejo)
")
12
Aprendizaje perceptivo: efectos de exposición

13
Aprendizaje perceptivo: efectos de exposición
Procedimiento 1) entrenamiento -20 ítems (5 tarjetas x ítem /1-5/) -presentación sucesiva por bloques -repetición hasta aprendizaje 2) prueba de recuerdo
 entrenamiento. -20 ítems (5 tarjetas x ítem /1-5/) -presentación sucesiva por bloques. -repetición hasta aprendizaje. 2) prueba de recuerdo.")
14
Efectos de “priming”: completamiento de palabras
estudio test

15
adquisición de habilidades cognitivas: gramáticas artificiales
Adquisición de gramáticas artificiales 1) entrenamiento -23 casos positivos 2) prueba -reconocimiento (23 familiares / 23 nuevos) -clasificación (23 positivos / 23 negativos)
 entrenamiento. -23 casos positivos. 2) prueba. -reconocimiento (23 familiares / 23 nuevos) -clasificación (23 positivos / 23 negativos)")
16
Cerebelo Amígdala Cerebro y condicionamiento
(condicionamiento de RCs motoras) Amígdala (condicionamiento de RCs emocionales)
 Amígdala. (condicionamiento de RCs emocionales)")
17
(1) Lesión amigdalar (enfermedad de Urbach-Whiete)
PAPEL DE LA AMÍGDALA Y EL HIPOCAMPO EN EL CONDICIONAMIENTO EMOCIONAL (Bechara y cols., 1995) Sujetos (1) Lesión amigdalar (enfermedad de Urbach-Whiete) (2) Atrofia hipocampal (hipoxia/isquemia por paradas cardiacas múltiples) (3) Lesión bilateral amígdala/hipocampo (encefalitis) (4) Controles normales No condicionamiento emocional No conocimiento explícito No condicionamiento emocional Conocimiento Explícito Condicionamiento emocional Conocimiento explícito HIPOCAMPO normal lesión AMÍGDALA
 Sujetos. (1) Lesión amigdalar (enfermedad de Urbach-Whiete) (2) Atrofia hipocampal (hipoxia/isquemia por paradas cardiacas múltiples) (3) Lesión bilateral amígdala/hipocampo (encefalitis) (4) Controles normales. No condicionamiento emocional. No conocimiento explícito. No condicionamiento. emocional. Conocimiento. Explícito. Condicionamiento emocional. Conocimiento explícito. HIPOCAMPO. normal. lesión. AMÍGDALA.")
18
Adquisición de destrezas y sistema estriado
Ganglios basales Sistema estriado -Sistema subcorticcal formado por el Núcleo caudado y el Putamen -forma parte de los ganglios basales -inputs y outputs: corteza motora y pre-motora -implicado en control motor amígdala caudado putamen

19
1. Ventriculus lateralis
Imagen PET de putamen y estriado 1. Ventriculus lateralis 2. Gyrus cinguli 3. Corpus callosum 4. Capsula interna 5. Putamen 6. Capsula extrema 7. Insula 8. Capsula externa 9. Globus pallidus 10. Commissura anterior 11. Nucleus accumbens 12. Claustrum 13. Columna fornicis 14. Nucleus caudatus 15. Lobus temporalis 16. Lobus frontalis

20
Adquisición de destrezas y sistema estriado
Disfunciones en sistema estriado -enfermedad de Parkinson (muerte celular y déficit de dopamina) -corea de Huntington (degeneración neuronal en estriado) -déficits en aprendizaje motor (aprendizaje de hábitos) # Rotor de persecución # tiempo de reacción serial (TRS) (aprendizaje implícito de secuencias) Estudios de neuroimagen -activación de estriado en tareas motoras (ej. TRS)
 -corea de Huntington (degeneración neuronal en estriado) -déficits en aprendizaje motor (aprendizaje de hábitos) # Rotor de persecución. # tiempo de reacción serial (TRS) (aprendizaje implícito de secuencias) Estudios de neuroimagen. -activación de estriado en tareas motoras (ej. TRS)")
21
D A C B E F D A C B E F … (entrenamiento)
Aprendizaje de secuencias: Tiempo de reacción serial Mean RT (ms) (Datos de A.Cleeremans) 500 Transferencia 480 A B C D E F 460 440 420 400 380 360 340 RSI 320 no RSI 300 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Training blocks D A C B E F D A C B E F … (entrenamiento) F B E A C B F B E A C B … (transferencia)
 (Datos de A.Cleeremans) 500. Transferencia A B C D E F RSI no RSI Training blocks. D A C B E F D A C B E F … (entrenamiento) F B E A C B F B E A C B … (transferencia)")
22
Efectos de la experiencia perceptiva
1) modificación de mapas somatosensoriales -estudios en animales -estudios en expertos humanos 2) efectos compensatorios -lectura Braille en ciegos
 modificación de mapas somatosensoriales. -estudios en animales. -estudios en expertos humanos. 2) efectos compensatorios. -lectura Braille en ciegos.")
23
* * * * * *

25
Aprendizaje y memoria implícita: sistemas cerebrales
1) condicionamiento lesiones amigdalares y condicionamiento emocional lesiones cerebelares y condicionamiento de RC motoras 2) aprendizaje perceptivo alteraciones en respuestas corticales a los estímulos reorganización de mapas sensoriales 3) destrezas motoras sistema estriado
 condicionamiento. lesiones amigdalares y condicionamiento emocional. lesiones cerebelares y condicionamiento de RC motoras. 2) aprendizaje perceptivo. alteraciones en respuestas corticales a los estímulos. reorganización de mapas sensoriales. 3) destrezas motoras. sistema estriado.")
26
SISTEMAS DE MEMORIA DE LARGO PLAZO
Memoria implícita (no dependiente del hipocampo) Memoria explícita (dependiente del hipocampo) Condicionamiento Memoria episódica Destrezas cognitivas Memoria semántica Priming y aprendizaje perceptivo Destrezas motoras
 Memoria explícita. (dependiente del hipocampo) Condicionamiento. Memoria episódica. Destrezas cognitivas. Memoria semántica. Priming y aprendizaje perceptivo. Destrezas motoras.")
27
Priming y aprendizaje perceptivo
SISTEMAS DE MEMORIA IMPLÍCITA Amígdala (cond. Emocional) Cerebelo (RC motoras) Condicionamiento Corteza sensorial Cerebelo Ganglios basales (estriado) Destrezas motoras Priming y aprendizaje perceptivo Corteza sensorial Destrezas cognitivas Ganglios basales (???)
 Cerebelo (RC motoras) Condicionamiento. Corteza sensorial. Cerebelo. Ganglios basales (estriado) Destrezas motoras. Priming y aprendizaje perceptivo. Corteza sensorial. Destrezas cognitivas. Ganglios basales ( )")
Presentaciones similares



>")









>")






