Descargar la presentación
La descarga está en progreso. Por favor, espere

1
II JORNADAS INTERNACIONALES PROGRAMA DE INVESTIGACIÓN DE EXCELENCIA INTERDISCIPLINARIA EN ENVEJECIMIENTO SALUDABLE (PIEI-ES) Talca, Noviembre, 2014 Enfermedades neurodegenerativas y acumulación de hierro. Dr. Miguel Arredondo Olguín INTA, Universidad de Chile

2
IMPORTANCIA DEL HIERRO TRANSPORTE De OXIGENO Hb, Mb TRANSFERENCIA De e* Citocromos PROTEINA ENZIMAS. Fe-S Catalasa Peroxidasa Hidrolasa ALTA TOXICIDAD Fe 2+ + H 2 O 2 Fe 3+ + OH° + OH- Fe 3+ + NADH Fe 2+ + [NADH°+] ALTA REACTIVIDAD CAPACIDAD PARA CAPTAR e* -OH -, -COOH, NH 2, -SH Esencialidad vs Toxicidad

3
Esencialidad: Anemia por deficiencia de hierro Poblaciones susceptibles

4
HIERRO, VIDA Y EVOLUCIÓN Los seres vivos necesitan poco hierro El hierro abunda en la biosfera El hierro en atmósfera oxidante es poco soluble A pesar de la abundancia de hierro en la biosfera su bio-disponibilidad es muy baja. Los seres vivos han de ser capaces de “disolver” el hierro para poder asimilarlo. Primera paradoja: “ESCASEZ EN PLENA ABUNDANCIA”

5
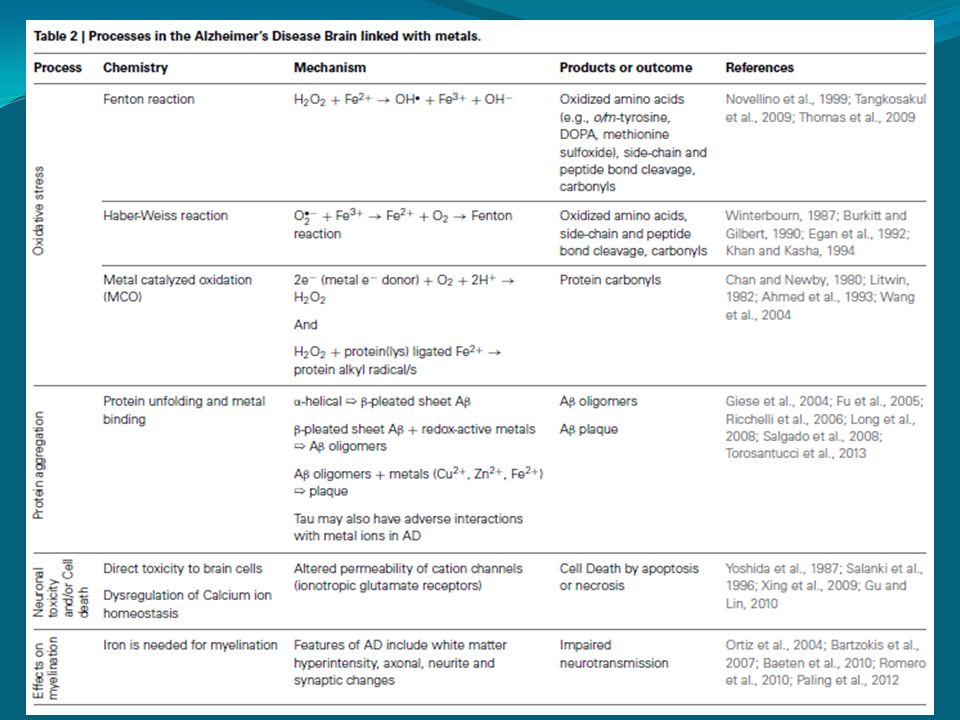
Segunda Paradoja: “El nutriente más tóxico”: “El estrés oxidativo” El Hierro es potencialmente tóxico en ambientes donde abunda el O 2. La concentración de hierro intracelular ha de estar controlada. Origen de la toxicidad del Fe: la reacción de Fenton: Fe (II) + H 2 O 2 ----> Fe (III) + OH - +.OH El hierro “libre” intracelular se relaciona directamente con el estrés oxidativo y sus consecuencias patológicas. La toxicidad del hierro en ambientes aerobios se manifiesta en todos los seres vivos. Los seres de vida aerobia disponen de mecanismos que atenúan efectos del estrés oxidativo. ¡Dos veces más potente que la lejía !
 + H 2 O > Fe (III) + OH - +.OH El hierro libre intracelular se relaciona directamente con el estrés oxidativo y sus consecuencias patológicas. La toxicidad del hierro en ambientes aerobios se manifiesta en todos los seres vivos. Los seres de vida aerobia disponen de mecanismos que atenúan efectos del estrés oxidativo. ¡Dos veces más potente que la lejía !.")
6
IMPORTANCIA DEL HIERRO HOMEOSTASIA DEL HIERRO TRANSPORTE DE OXIGENO Hb, Mb TRANSFERENCIA DE e* Citocromos PROTEINA ENZIMAS. Fe-S Catalasa Peroxidasa Hidrolasa ALTA TOXICIDAD Fe 2+ + H 2 O 2 Fe 3+ + OH° + OH- Fe 3+ + NADH Fe 2+ + [NADH°+] ALTA REACTIVIDAD CAPACIDAD PARA CAPTAR e* -OH -, -COOH, NH 2, -SH [Fe] Esencialidad vs Toxicidad Balance coordinado entre captación, utilización y almacenamiento intracelular

7
Metabolismo del Hierro Increased iron stores and inflammation induce hepcidin synthesis Suppression: hypoxia, anemia, increased and/or ineffective erythropoiesis in bone marrow. Hepcidin is induced under infection, decreasing the available host iron pool that is essential for survival of invading pathogens.

8
MECANISMOS DE REGULACIÓN

9
Iron and hepcidin: a story of recycling and balance Clara Camaschella. Hematology 2013 Hepcidin

10
Absorción de Fe hem

11
Figure 2. Effect of age on body iron. All values for body iron are positive and indicate the amount of storage iron. Data are based on a convenience sample of 2057 specimens collected in NHANES III. Shaded areas represent the mean 1 SEM for each 5-year interval. Figure 3. Cumulative frequency distributions of body iron calculated from the ratio of the serum transferrin receptor to serum ferritin. The clear area and positive values indicate storage iron, and the shaded area and negative values indicate tissue iron deficiency. Data are shown for pregnant Jamaican women aged 16-35 years, US women aged 20-45 years, and US men aged 20-65 years.

12
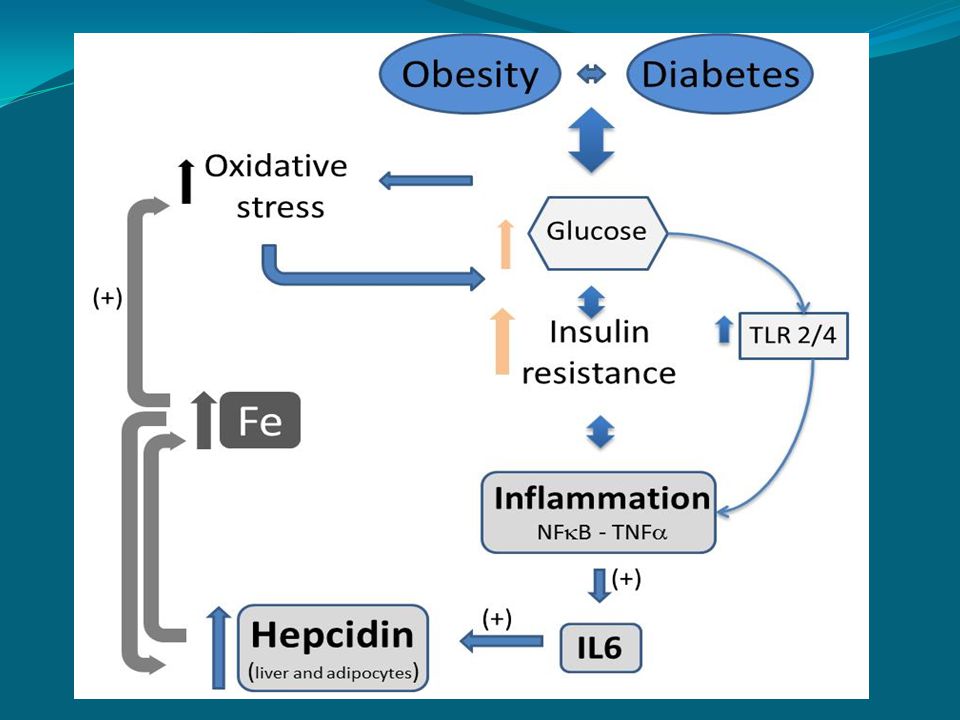
RNAm Ferritina Ferritina Fe+2 Fe libre Insulina Internalización de Insulina y Acciones Biológicas Transferrina Glicación de proteínas Estrés oxidativo Hiperinsulinemia Insulino resistencia RTf - + + Intracelular Extracelular + + Reactividad Vascular anormal Daño celular y tisular ¿Cuál es la relación entre metabolismo de Fe y Sindróme Metabólico y diabetes?

13
Hiperglicemia GLICOLISIS Glucosa Fructosa-6P Gliceraldehido 3-P 1,3 Difodfoglicerato Piruvato Formación de AGEs Glicación de Proteínas AGEsAGEs RAGERAGE Glicación de SOD y Catalasa ( ↑ H2O2) Glicación de SOD y Catalasa ( ↑ H2O2) Glicación de Transferrina Glicación de Transferrina Glicación de SOD y Catalasa ( ↑ H2O2) Glicación de SOD y Catalasa ( ↑ H2O2) Glicación de Transferrina Glicación de Transferrina Activación de NADPH oxidasa ( ↑ O 2.- ) Activación de Nf-κB ( ↑ NOS, NO, ONOO - ) Activación de NADPH oxidasa ( ↑ O 2.- ) Activación de Nf-κB ( ↑ NOS, NO, ONOO - ) Cadena Transportadora de electrones en la Mitocondria.
 Glicación de SOD y Catalasa ( ↑ H2O2) Glicación de Transferrina Glicación de Transferrina Glicación de SOD y Catalasa ( ↑ H2O2) Glicación de SOD y Catalasa ( ↑ H2O2) Glicación de Transferrina Glicación de Transferrina Activación de NADPH oxidasa ( ↑ O 2.- ) Activación de Nf-κB ( ↑ NOS, NO, ONOO - ) Activación de NADPH oxidasa ( ↑ O 2.- ) Activación de Nf-κB ( ↑ NOS, NO, ONOO - ) Cadena Transportadora de electrones en la Mitocondria.")
14
Fe y Diabetes (Arredondo et al., AJCN, 2007) No solo altos niveles de Fe se han asociado a DM2 HEM Fe + CO 2 + Biliverdina HO-1HO-1 Polimorfismo en el promotor de la HO-1 de repeticiones (GT) n Pacientes DM2 portadores de repeticiones cortas > niveles de Ferritina > actividad de HO-1 complicaciones por estrés oxidativo > niveles de Ferritina > actividad de HO-1 complicaciones por estrés oxidativo
 No solo altos niveles de Fe se han asociado a DM2 HEM Fe + CO 2 + Biliverdina HO-1HO-1 Polimorfismo en el promotor de la HO-1 de repeticiones (GT) n Pacientes DM2 portadores de repeticiones cortas > niveles de Ferritina > actividad de HO-1 complicaciones por estrés oxidativo > niveles de Ferritina > actividad de HO-1 complicaciones por estrés oxidativo")
15
Hb (g/dL) 14,0±1,4 NS Fe (mg/dL) 128,3±52,8 <0,002 FS (µg/L) & <0,001 HO& <0,001 (nmoles bilirrubina/mg proteína/hr) DM2 SM C 61 (35-107) # # : Diferencia estadística entre Mujeres/grupos &: Promedio geométrico + rango A: Diferencia estadística entre DM2 y C 0,7 (0,3-2,0) # Parámetros hematológicos: niveles de Fe RTf (mg/L) & 5,5 ±2,0 14,2±1,4 126,5± 44,5 52 (27-100) # 0,6 (0,2-1,7) # 6,3 ±1,7 13,8±1,5 108,2±37,5 34 (15-76) # 0,3 (0,1-0,7) # 6,8 ±2,7 <0,001 A
 14,0±1,4 NS Fe (mg/dL) 128,3±52,8 <0,002 FS (µg/L) & <0,001 HO& <0,001 (nmoles bilirrubina/mg proteína/hr) DM2 SM C 61 (35-107) # # : Diferencia estadística entre Mujeres/grupos &: Promedio geométrico + rango A: Diferencia estadística entre DM2 y C 0,7 (0,3-2,0) # Parámetros hematológicos: niveles de Fe RTf (mg/L) & 5,5 ±2,0 14,2±1,4 126,5± 44,5 52 (27-100) # 0,6 (0,2-1,7) # 6,3 ±1,7 13,8±1,5 108,2±37,5 34 (15-76) # 0,3 (0,1-0,7) # 6,8 ±2,7 <0,001 A")
16
Control n=146 OB n=132 T2D n=60 T2DOB n=106 Hemoglobin (g/dl)15.7±1.316.2±1.2 a 14.7±1.8 c 15.3±1.6 Serum Ferritin (µg/L) 1 56.5 (33.7-90.9) 75.5 c (50.0-111.0) 70.3 b (42.2-118.1) 82.3 c (53.9-125.7) Serum Fe (µg/dl)107.5±37.4100.2±35.1124.2±88.2107.9±50.7 Transferrin Saturation (%)32.7±12.030.5±9.035.6±15.927.9±9.7 a Transferrin Receptor (µg/mL) 1 2.8 (1.2-6.4) 3.9 (1.3-6.6) 3.6 (1.8-7.4) 3.6 (1.9-6.5) TBI (mg/kg)8.5±3.29.7±3.3 a 9.1±3.79.6±2.7 a Hepcidin (ng/mL)19.0±8.725.0±11.5 a 23.4±10.6 a 25.2±10.8 b RBP4 (µg/mL)26.1±8.433.6±7.3 a 31.7±9.6 a 32.7±9.3 a hsCRP (µg/dl) 1 0.8 (0.2-4.4) 1.8 (0.5-6.8) 1.9 b (0.4-7.8) 2.0 b (0.4-9.0) HO-1 (nmole bilirubin/mg protein/h) 1 2.6 (0.9-7.1) 4.2 a (1.7-10.1) 4.6 c (1.7-12.4) 3.4 (0.4-9.0) TBARS (nmoles/mL) 1 0.99 (0.4-2.4) 1.4 a (0.7-2.7) 1.7 b (1.0-3.1) 2.1 c (1.2-3.5) Iron Nutrition and oxidative stress parameters in studied subjects TBI: Total body iron; RBP4: Retinol Binding protein 4; hsCRP: high-sensitivity C reactive protein; HO-1: heme oxygenase-1; TBARS: Thiobarbituric Acid Reactive Species. Values are mean ± SD; 1 Values are geometric mean±(Range) One way ANOVA, post hoc Dunnett`s a p<0.05; b p<0.01; c p<0.001
 One way ANOVA, post hoc Dunnett`s a p<0.05; b p<0.01; c p<")
17
OR without to adjust CIpOR adjusted * CIP Ferritin Q1: <50 μg/L1.000 Ferritin Q2: 50-100 μg/L1.0210.42-1.71 0.121.1010.87-1.57 0.66 Ferritin Q3: 100-150 μg/L1.3020.45-1.91 0.091.1330.66-1.83 0.08 Ferritin Q4: 150-200 μg/L1.3770.97-2.19 0.071.7821.61-1.92<0.01 TBARS1.9801.91-2.28<0.052.2501.89-3.25<0.05 Table 3 Risk of developing type 2 diabetes (OR) according to ferritin quartiles and TBARS concentration. * Adjusted to age, BMI and hsCRP OR were estimated through logistic regression

18
ORCIpOR Adjusted * CIp Hepcidin Q11.000 Hepcidin Q21.4831.11-1.980.0071.3000.95-1.110.470 Hepcidin Q31.9800.89-4.370.0912.1200.89-5.030.087 Hepcidin Q43.2911.39-7.750.0064.3701.67-11.420.003 Table 4: Risk of developing type 2 diabetes (OR) according to hepcidin expression quartiles * Adjusted to age, BMI and hsCRP OR were estimated through logistic regression.
 according to hepcidin expression quartiles * Adjusted to age, BMI and hsCRP OR were estimated through logistic regression.")
19
HO 5` 3` GT n 19202122232425262728293031323334353637383940 20 40 60 80 100 120 Nº Individuals GT Repetitions Frecuencia alélica(%) Hardy-Weinberg Equilibrium S = < 27 (GT) n M = 27-32 (GT) n L = >32 (GT) n Micro-polimorfismo SML C6.29.64.2 MS8.010.91.1 OB7.98.93.1 DM7.68.73.7 DMO B 8.38.03.7 SMSLMLMMSSLL C7.82.30.85.51.32.7 MS13.70.41.26.02.80.6 OB12.31.11.92.82.12.0 DM10.82.11.62.61.21.9 DMOB7.51.81.30.7 0.8 GENOTIPO (%) C175 MS210 OB189 DM172 DMOB109 Total 855
 Hardy-Weinberg Equilibrium S = < 27 (GT) n M = (GT) n L = >32 (GT) n Micro-polimorfismo SML C MS OB DM DMO B SMSLMLMMSSLL C MS OB DM DMOB GENOTIPO (%) C175 MS210 OB189 DM172 DMOB109 Total 855")
20
Figure 1: Relative abundance of genes related to inflammation in OB, T2DOB, T2D and Cn subjects. A)Hepcidin; B)IL6; C)NF- B; D)TLR-2; E)TLR-4; F)TNF- . Values are mean ± SEM. Data were analyzed using the Kruskal-Wallis test. *p<0.05; **p<0.01; ***p<0.001.
Hepcidin; B)IL6; C)NF- B; D)TLR-2; E)TLR-4; F)TNF- . Values are mean ± SEM. Data were analyzed using the Kruskal-Wallis test. *p<0.05; **p<0.01; ***p<")
22
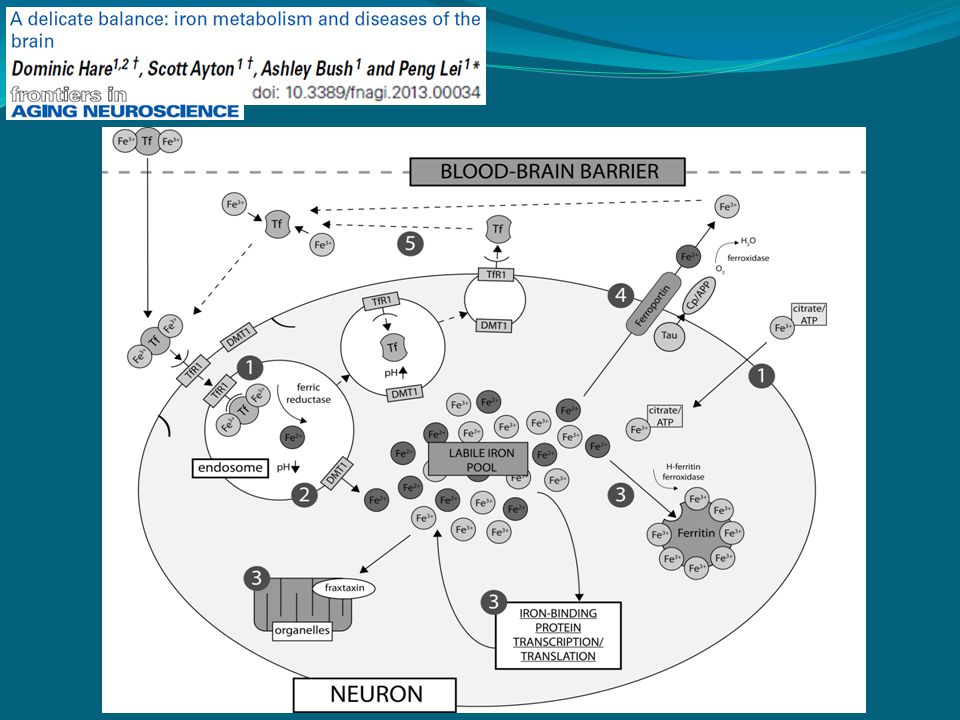
Hierro y cerebro. Es importante para la función neuronal. Funciones: Es un componente esencial del citocromo a, b y c oxidasa. Componente del complejo hierro – sulfuro de la cadena oxidativa. Es un cofactor para la tirosina, triptófano hidroxilasa, ribonucleótido reductasa, succinato deshidrogenasa y aconitasa. Es esencial para síntesis de lípidos, colesterol y un rol en el sistema GABA.

23
Existen altas concentraciones en globo pálido, sustancia nigra, núcleo dentado y corteza motora. Las neuronas lo almacenan como Ferritina de cadena liviana o pesadas. La alteración de Ferritina (por inserción de adenosina) produce la “neuroferritinopatía”. Existen múltiples vías de regulación para el metabolismo del hierro
 produce la neuroferritinopatía . Existen múltiples vías de regulación para el metabolismo del hierro.")
24
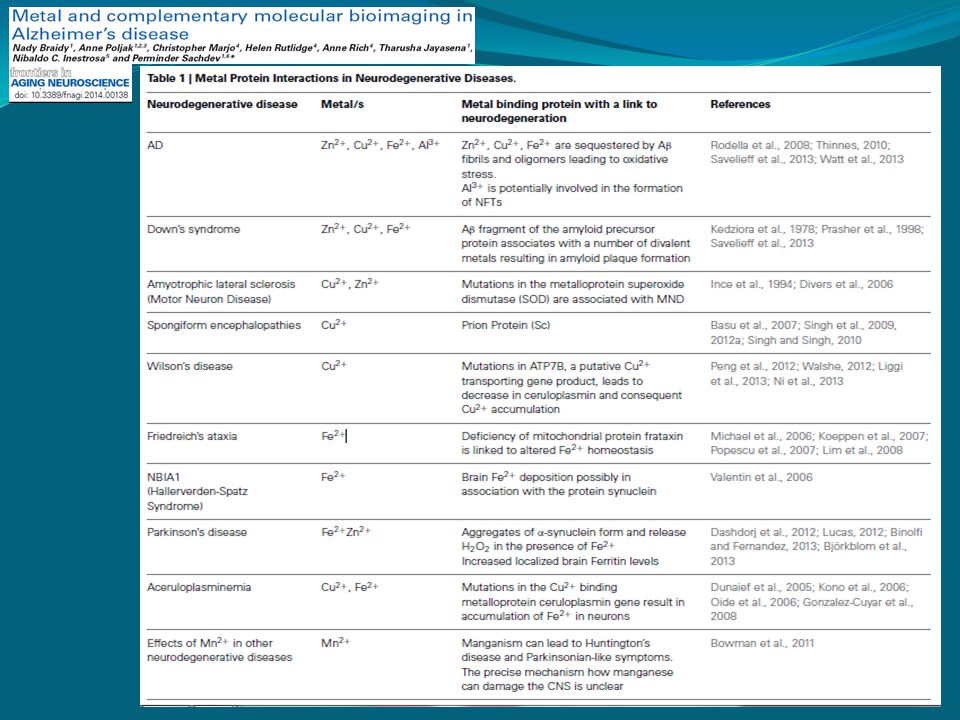
Lista de enfermedades neurodegenerativas Enfermedad de Alzheimer Demencia con cuerpos de Lewy Demencia frontotemporal Demencia mixta (multi-infarto y E. de Alzheimer) Enfermedad de Parkinson Atrofia Multisistémica Parálisis supranuclear progresiva Degeneración córticobasal Esclerosis lateral amiotrófica. Enfermedad de Creutzfeldt-Jacob.
 Enfermedad de Parkinson Atrofia Multisistémica Parálisis supranuclear progresiva Degeneración córticobasal Esclerosis lateral amiotrófica. Enfermedad de Creutzfeldt-Jacob..")
25
Desordenes asociados con neurodegeneración y anormalidades en la regulación del hierro que resultan depósitos de hierro en el cerebro. Desordenes asociados a depósitos de hierro primarios con anormalidades genéticas en las vías metabólicas del hierro. Neuro-degeneración asociada a la pantotenato kinasa (PKAN) Hipo-prebetalipoproteinemia, acantosis y retinitis pigmentosa con degeneración del pallidal (HARP) Neuro-degeneración con acumulación de hierro en cerebro (NBIA) Neuro-ferritinopatía Aceruloplasminemia Hemocromatosis Desordenes con cambios secundarios en las vias regulatorias del metabolismo de hierro Enfermedad de Huntington Enfermedad de Parkinson Friedreich´s ataxia.
 Hipo-prebetalipoproteinemia, acantosis y retinitis pigmentosa con degeneración del pallidal (HARP) Neuro-degeneración con acumulación de hierro en cerebro (NBIA) Neuro-ferritinopatía Aceruloplasminemia Hemocromatosis Desordenes con cambios secundarios en las vias regulatorias del metabolismo de hierro Enfermedad de Huntington Enfermedad de Parkinson Friedreich´s ataxia..")
29
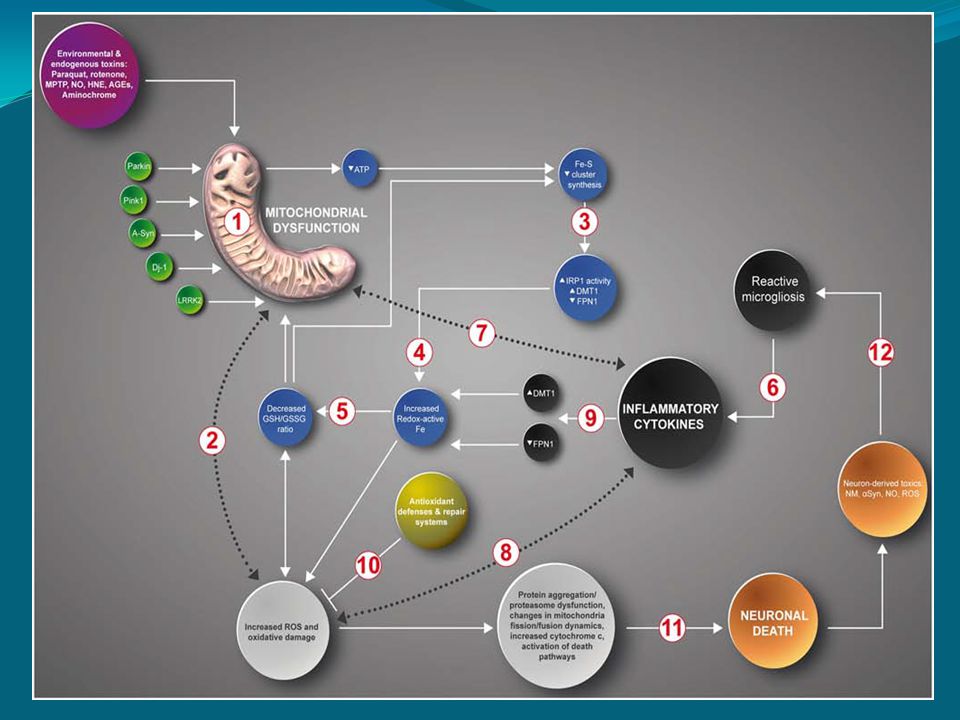
FIGURE 1 | Inflammation causes ROS/RNS production, mitochondrial dysfunction, and iron accumulation. Inflammation, oxidative damage, and mitochondrial dysfunction are common features of neurodegenerative diseases. A complex net of relationships connect these features, which through feedback mechanisms contribute to the evolvement of neuronal death. Inflammation NF B activation Infl cytokines

38
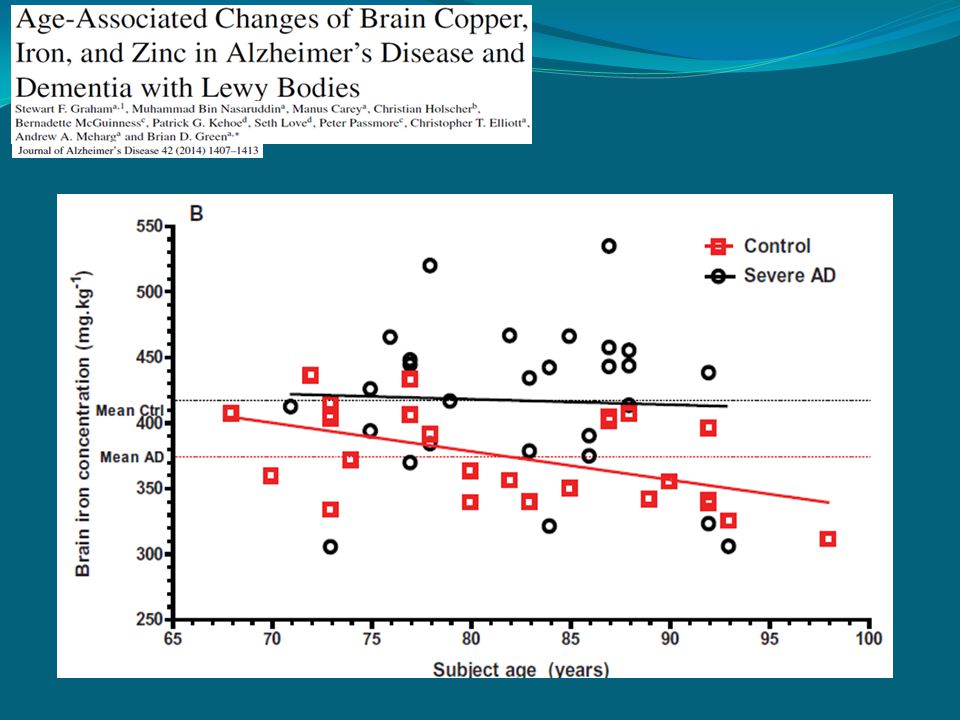
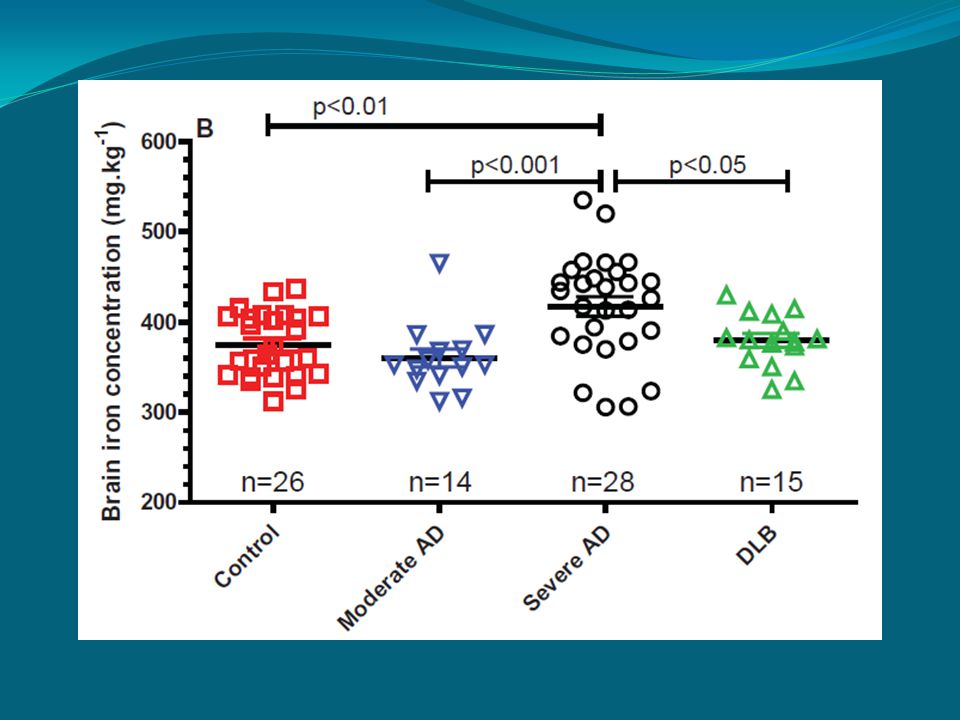
Dementia with Lewy bodies (DLB)
")
40
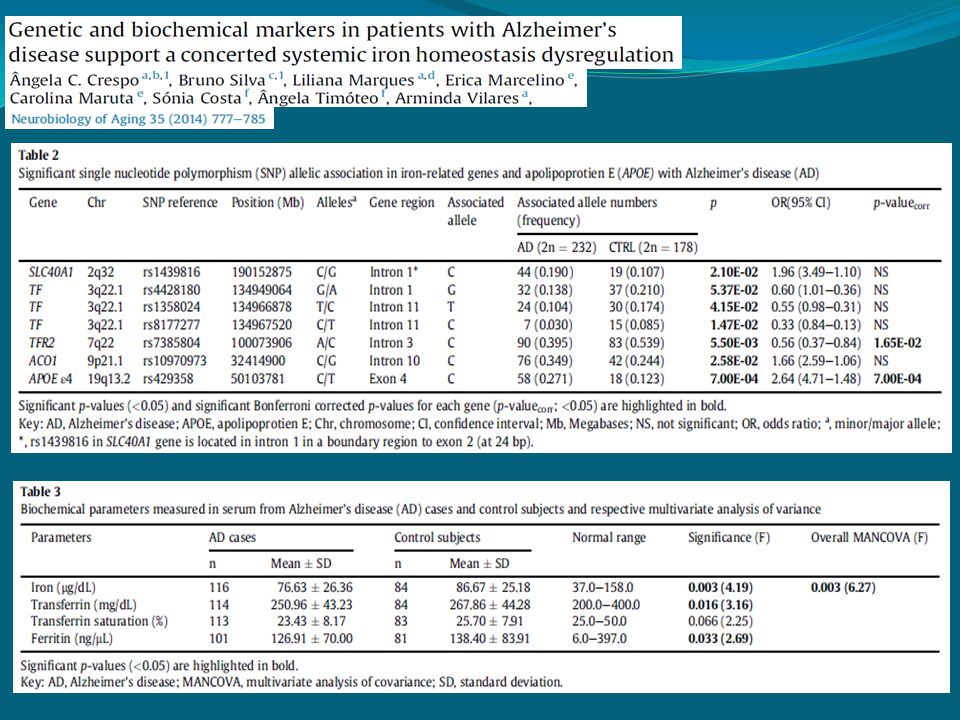
Fig. 1. Expression levels of several iron metabolism genes in patients with AD compared with controls. The distribution of the expression levels of (A) TFRC (B) TFR2 (C) SLC40A1 (D) HAMP and (E) SLC11A2 of patients with AD and control subjects are represented by the box-plots. The quantification was performed by normalizing the sample to a pool of individuals and using HPRT1 as a housekeeping gene. Dots represent the mild outliers. The number of individuals analyzed is indicated in brackets. p-values were obtained by covariance analysis.
 TFRC (B) TFR2 (C) SLC40A1 (D) HAMP and (E) SLC11A2 of patients with AD and control subjects are represented by the box-plots. The quantification was performed by normalizing the sample to a pool of individuals and using HPRT1 as a housekeeping gene. Dots represent the mild outliers. The number of individuals analyzed is indicated in brackets. p-values were obtained by covariance analysis..")
42
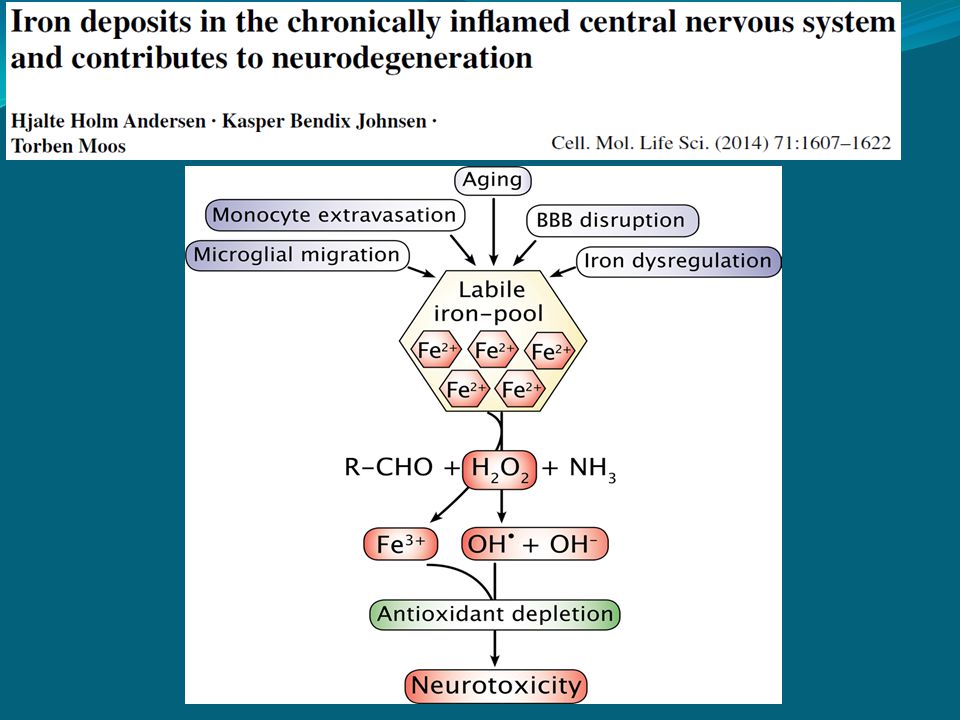
Fig. 2 Macrophages migrating into the brain release nitric oxide radicals (NO), a process that involves the catalytic oxidation of ferrous iron. NO is capable of diffusing pass the cellular membranes and into neurons where it can react with superoxide (O2−) and promote formation of the highly reactive and toxic peroxynitrite (ONOO−)
, a process that involves the catalytic oxidation of ferrous iron. NO is capable of diffusing pass the cellular membranes and into neurons where it can react with superoxide (O2−) and promote formation of the highly reactive and toxic peroxynitrite (ONOO−).")
44
Fig. 4 Extravasated macrophages phagocytose and degrade damaged neurons and subsequently die to terminate their function, which leads to the release of iron into the extracellular space of the CNS on a low molecular weight form

45
Fig. 5 The macrophages, like monocytes and microglia, are capable of secreting hepcidin into the brain extracellular space. Hepatic hepcidin is synthesized in response to inflammatory signals and secreted into blood plasma from where it can diffuse into the brain in areas with a compromised blood–brain barrier. The hepcidin is capable of binding and inhibiting ferroportin needed for export of iron from neurons, which may result in neuronal iron accumulation and increased the likelihood of neuronal damage via Fenton chemistry

46
Fig. 6 Potential pharmacological intervention points to inhibit the impact of migrating macrophages on their deposition of iron in the brain. a)Inhibition of monocytes migration into the brain via transfer through the brain capillaries. b)Inhibition of the functioning of the brain macrophages for phagocytosis and nitric oxide (NO) release. c)Extracellular chelation of low molecular weight iron released from dying macrophages. d)Intracellular chelation of iron in neurons subsequent to their uptake of low molecular weight iron from the extracellular space
Inhibition of monocytes migration into the brain via transfer through the brain capillaries. b)Inhibition of the functioning of the brain macrophages for phagocytosis and nitric oxide (NO) release. c)Extracellular chelation of low molecular weight iron released from dying macrophages. d)Intracellular chelation of iron in neurons subsequent to their uptake of low molecular weight iron from the extracellular space.")
47
Fig. 6. A hypothetical scheme for the pharmacologic mechanisms of Huperzine A (HupA) in the treatment of Alzheimer’s disease. In addition to acting as an acetylcholinesterase inhibitor, Huperzine A (HupA) has the ability to inhibit transferring receptor 1 (TfR1) expression and then reduce transferrin-bound iron (TBI) uptake by the neurons or other brain cells which has TfR1 expression on the membrane. This will lead to progressive reduction in iron contents in the brain and thus protecting neurons and other brain cells from damage and apoptosis probably by inhibiting the iron-associated oxidative stress. “Reducing iron in the brain” is a novel pharmacologic mechanism of HupA in the treatment of Alzheimer’s disease. Abbreviations: HupA, Huperzine A; TBI, transferrin-bound iron; TfR1, transferring receptor 1. REDUCING IRON IN THE BRAIN: A NOVEL PHARMACOLOGIC MECHANISM OF HUPERZINE A IN THE TREATMENT OF ALZHEIMER’S DISEASE. Xiao-Tian Huang. Neurobiology of Aging 35 (2014) 1045
 in the treatment of Alzheimer’s disease. In addition to acting as an acetylcholinesterase inhibitor, Huperzine A (HupA) has the ability to inhibit transferring receptor 1 (TfR1) expression and then reduce transferrin-bound iron (TBI) uptake by the neurons or other brain cells which has TfR1 expression on the membrane. This will lead to progressive reduction in iron contents in the brain and thus protecting neurons and other brain cells from damage and apoptosis probably by inhibiting the iron-associated oxidative stress. Reducing iron in the brain is a novel pharmacologic mechanism of HupA in the treatment of Alzheimer’s disease. Abbreviations: HupA, Huperzine A; TBI, transferrin-bound iron; TfR1, transferring receptor 1. REDUCING IRON IN THE BRAIN: A NOVEL PHARMACOLOGIC MECHANISM OF HUPERZINE A IN THE TREATMENT OF ALZHEIMER’S DISEASE. Xiao-Tian Huang. Neurobiology of Aging 35 (2014)")
48
Low-copper diet as a preventive strategy for Alzheimer’s disease Rosanna Squitti, Mariacristina Siotto, Renato Polimanti Neurobiology of Aging DOI: 10.1016/j.neurobiolaging.2014.02.031

49
Low-copper diet as a preventive strategy for Alzheimer’s disease Rosanna Squitti, Mariacristina Siotto, Renato Polimanti Neurobiology of Aging DOI: 10.1016/j.neurobiolaging.2014.02.031

50
Fig. 1. Biochemical basis of the theoretical model of copper toxicity in AD. b-APP binds and reduces copper from Cu(II) to Cu(I), which modulatescopper-induced toxicity based on redox reactions through the production of H2O2,triggering chain reactions of oxidative stress and lipid peroxidation. A and metalsare packed together in plaques, and it has been postulated that A plaques disturbneuronal physiology, entrapping metals within the plaques, while cell-associatedcopper could be decreased. On this basis it could be assumed that decopper-ing agents, as for example zinc therapy, can reduce systemic Non-Cp copper andstop the feeding of noxious copper entering redox cycles with A, thus halting theprogression of A plaques and promoting their solubilization. Additionally, metalionophores can improve neuroregenerative processes, restoring the physiologicaluptake of metals in neurons, which would suffer because of the copper entrappedwithin the extracellular A plaques. Copper subtype of Alzheimer’s disease (AD): Meta-analyses, geneticstudies and predictive value of non-ceruloplasmim copper in mildcognitive impairment conversion to full AD Rosanna Squitti, JTEMB, 2014
 to Cu(I), which modulatescopper-induced toxicity based on redox reactions through the production of H2O2,triggering chain reactions of oxidative stress and lipid peroxidation. A and metalsare packed together in plaques, and it has been postulated that A plaques disturbneuronal physiology, entrapping metals within the plaques, while cell-associatedcopper could be decreased. On this basis it could be assumed that decopper-ing agents, as for example zinc therapy, can reduce systemic Non-Cp copper andstop the feeding of noxious copper entering redox cycles with A, thus halting theprogression of A plaques and promoting their solubilization. Additionally, metalionophores can improve neuroregenerative processes, restoring the physiologicaluptake of metals in neurons, which would suffer because of the copper entrappedwithin the extracellular A plaques. Copper subtype of Alzheimer’s disease (AD): Meta-analyses, geneticstudies and predictive value of non-ceruloplasmim copper in mildcognitive impairment conversion to full AD Rosanna Squitti, JTEMB,")
51
En resumen……. 1) Existe asociación entre el metabolismo del hierro y Enfermedades neurodegenerativas 2) Elemento común desencadenador: Eje Inflamación – Hepcidina 3) Elemento mediador: Estrés Oxidativo 4) Consecuencia final: Muerte Celular
 Existe asociación entre el metabolismo del hierro y Enfermedades neurodegenerativas 2) Elemento común desencadenador: Eje Inflamación – Hepcidina 3) Elemento mediador: Estrés Oxidativo 4) Consecuencia final: Muerte Celular.")
52
Mónica Andrews, PhD (INTA) Valeria Candia, MSc (INTA) Dr. Manuel Olivares (INTA) Dr. Néstor Soto (Hospital Arriarán) Solange Le Blanc, PhDc (Suiza) Alejandra Espinoza, PhDc Marcela Fuentes, PhD (PUC) “Muchas gracias por su atención”
 Dr. Néstor Soto (Hospital Arriarán) Solange Le Blanc, PhDc (Suiza) Alejandra Espinoza, PhDc Marcela Fuentes, PhD (PUC) Muchas gracias por su atención .")
Presentaciones similares













 y electrones (citocromos)>")


: Autótrofos: A partir de la materia inorgánica y del CO2 de la atmósfera.>")





