Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Evaluación de la seguridad
Roberto Marín Gil FEA Farmacia Hospitalaria Hospital Universitario Virgen del Rocío

2
Novedades terapéuticas y seguridad
Relación beneficio-riesgo ¿Cómo medimos la seguridad? Toma de decisiones

3
Evaluación de la seguridad en los EECC
¿Cuál es el problema? La escasa información que nos dan los EECC en cuanto a seguridad. Los ensayos se diseñan para obtener significación estadística en la variable de eficacia, y se utiliza el tam de M mín para ello. La información de seguridad que nos dan es la que surge, que es muy muy poca Evaluación de la seguridad en los EECC

4
PRINCIPALES LIMITACIONES
RAMs baja frecuencia RAMs de exposición prolongada Exclusión de grupos de riesgo

6
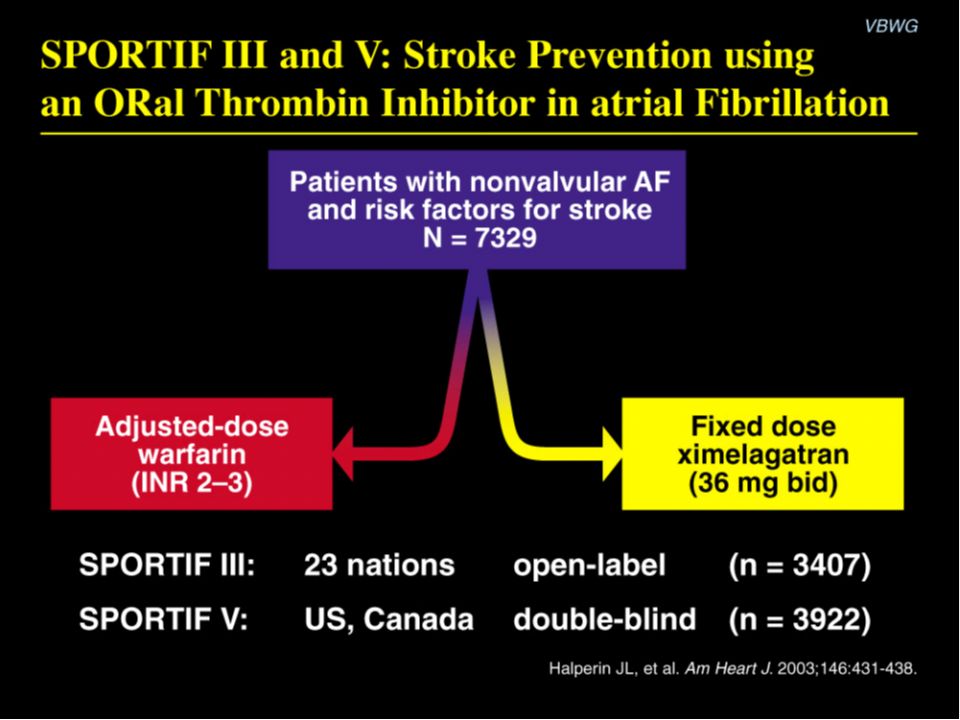
SPORTIF III: Primary outcome (stroke and systemic embolism)-Intention-to-treat analysis
Content Points: After a mean follow-up of 17.4 months, in intention-to-treat analysis the primary outcome occurred in 40 (1.6%/yr) ximelagatran patients and 56 (2.3%/yr) warfarin patients, a nonsignificant difference. The relative risk reduction was 29%.1 The absolute difference in the primary outcome rate was -0.7% per year (95% CI, -1.5 to 0.1; P = ). These CIs fell within the prespecified margins for establishing non-inferiority of ximelagatran. 1Executive Steering Committee on behalf of the SPORTIF Investigators. Stroke prevention with the oral direct thrombin inhibitor ximelagatran compared with warfarin in patients with non-valvular atrial fibrillation (SPORTIF III): Randomised controlled trial. Lancet. 2003;362:
 ximelagatran patients and 56 (2.3%/yr) warfarin patients, a nonsignificant difference. The relative risk reduction was 29%.1. The absolute difference in the primary outcome rate was -0.7% per year (95% CI, -1.5 to 0.1; P = ). These CIs fell within the prespecified margins for establishing non-inferiority of ximelagatran. 1Executive Steering Committee on behalf of the SPORTIF Investigators. Stroke prevention with the oral direct thrombin inhibitor ximelagatran compared with warfarin in patients with non-valvular atrial fibrillation (SPORTIF III): Randomised controlled trial. Lancet. 2003;362:")
7
SPORTIF III: Incidence of liver enzyme elevation Content Points:
Serum alanine aminotransferase (ALT) rose above 3x the upper limit of normal in 14 (0.8%) patients in the warfarin group and 107 (6.3%) patients in the ximelagatran group (P < 0.001).1 As shown, elevated ALT levels in ximelagatran patients typically occurred between 2 and 6 months after initiation of treatment and returned to baseline either spontaneously (59 patients) or after cessation of treatment (48 patients). 1Executive Steering Committee on behalf of the SPORTIF Investigators. Stroke prevention with the oral direct thrombin inhibitor ximelagatran compared with warfarin in patients with non-valvular atrial fibrillation (SPORTIF III): Randomised controlled trial. Lancet. 2003;362:
 rose above 3x the upper limit of normal in 14 (0.8%) patients in the warfarin group and 107 (6.3%) patients in the ximelagatran group (P < 0.001).1. As shown, elevated ALT levels in ximelagatran patients typically occurred between 2 and 6 months after initiation of treatment and returned to baseline either spontaneously (59 patients) or after cessation of treatment (48 patients). 1Executive Steering Committee on behalf of the SPORTIF Investigators. Stroke prevention with the oral direct thrombin inhibitor ximelagatran compared with warfarin in patients with non-valvular atrial fibrillation (SPORTIF III): Randomised controlled trial. Lancet. 2003;362:")
8
SPORTIF V: Primary outcome (stroke and systemic embolism)-Intention-to-treat analysis
Content Points: In intention-to-treat analysis, the primary outcome occurred in 51 patients (1.6%/yr) in the ximelagatran group and 37 (1.2%/yr) in the warfarin group. The absolute difference in the primary outcome rate was 0.45% (95% CI, to 1.03; P = 0.13). These CIs met the criteria for ximelagatran non-inferiority. 1Halperin JL. Stroke prevention using the direct oral thrombin inhibitor ximelagatran in patients with nonvalvular atrial fibrillation: SPORTIF V. Presented at: AHA Scientific Sessions 2003; Nov 11, 2003; Orlando, Fla.
 in the ximelagatran group and 37 (1.2%/yr) in the warfarin group. The absolute difference in the primary outcome rate was 0.45% (95% CI, to 1.03; P = 0.13). These CIs met the criteria for ximelagatran non-inferiority. 1Halperin JL. Stroke prevention using the direct oral thrombin inhibitor ximelagatran in patients with nonvalvular atrial fibrillation: SPORTIF V. Presented at: AHA Scientific Sessions 2003; Nov 11, 2003; Orlando, Fla.")
9
SPORTIF V: Incidence of liver enzyme elevation Content Points:
Serum ALT rose above 3x the upper limit of normal in 0.8% (14) of patients in the warfarin group and 6.0% (107) of patients in the ximelagatran group (P < 0.001).1 As shown, consistent with the SPORTIF III data, elevated ALT levels in ximelagatran patients typically occurred between 2 and 6 months after initiation of treatment and returned to baseline either spontaneously or after cessation of treatment. 1Halperin JL. Stroke prevention using the direct oral thrombin inhibitor ximelagatran in patients with nonvalvular atrial fibrillation: SPORTIF V. Presented at: AHA Scientific Sessions 2003; Nov 11, 2003; Orlando, Fla.
 of patients in the warfarin group and 6.0% (107) of patients in the ximelagatran group (P < 0.001).1. As shown, consistent with the SPORTIF III data, elevated ALT levels in ximelagatran patients typically occurred between 2 and 6 months after initiation of treatment and returned to baseline either spontaneously or after cessation of treatment. 1Halperin JL. Stroke prevention using the direct oral thrombin inhibitor ximelagatran in patients with nonvalvular atrial fibrillation: SPORTIF V. Presented at: AHA Scientific Sessions 2003; Nov 11, 2003; Orlando, Fla.")
10
Dudas que había en cuanto a hepatotoxicidad se han despejado
Dudas que había en cuanto a hepatotoxicidad se han despejado. El tratamiento a largo plazo es seguro y se realizarán controles de LFTs periódicamente, suspendiendo el ACo en pacientes con 3xULN

11
Rules of game: hepatotoxicity
The relationship of onset of liver injury with duration of drug exposure is not predictable. The hazard may be ‘frontloaded’, constant or develop after a threshold period of exposure. There are no measures that predict a priori whether injury will resolve or progress if a hepatotoxic drug is continued/discontinued. The tempo of injury is a characteristic both of individual drugs and patients. Rapid acceleration of liver injury in some individuals diminishes the value of periodic LFT monitoring.

13
Case 1 - Fatal Liver Injury
28 January 2005 FDA/CDER-AASLD-PhRMA HepTox Steering Group

14
Edad, comorbilidades… Lo que me faltaba ya... Conocer la patología...

15
16 EECC (n = 45276) vs 299 pacientes 34% en alguno de los 16 EECC (8–71%).
 vs 299 pacientes 34% en alguno de los 16 EECC (8–71%).")
17
RELY ROCKET AF Dabigatran 110 mg Dabigatran 150 mg Warfarin
CHADS2 Mean 0-1 (%) (%) 3+ (%) 2.1 32.6 34.7 32.7 2.2 32.2 35.2 30.9 37.0 32.1 ROCKET AF Rivaroxaban Warfarin CHADS2 Mean 2 (%) 3 (%) 4 (%) 5 (%) 6 (%) 3.5 13 43 29 2 44 28 12 87% Patel MR et al, NEJM 2011; Connolly SJ, et al. N Engl J Med. 2009;361: ; Granger C et al, NEJM; 2011
 2 (%) 3+ (%) ROCKET AF. Rivaroxaban. Warfarin. CHADS2 Mean. 2 (%) 3 (%) 4 (%) 5 (%) 6 (%) % Patel MR et al, NEJM 2011; Connolly SJ, et al. N Engl J Med. 2009;361: ; Granger C et al, NEJM;")
18
Falacias sobre seguridad de nuevos medicamentos
Falacia: razonamiento no válido o incorrecto pero con apariencia de razonamiento correcto. Es un razonamiento engañoso o erróneo , pero que pretende ser convincente o persuasivo. Falacias sobre seguridad de nuevos medicamentos

19
Promocional Científica Institucional Sociocultural
Cultural: ¿fármaco más moderno=mejor, más seguro, mas caro? Autorización: el aval del registro Promocional: punto de vista de la industria Mediática/Científica: editoriales ó revisiones del nuevo fármaco Promocional Científica Institucional Sociocultural

20
Promocional

21
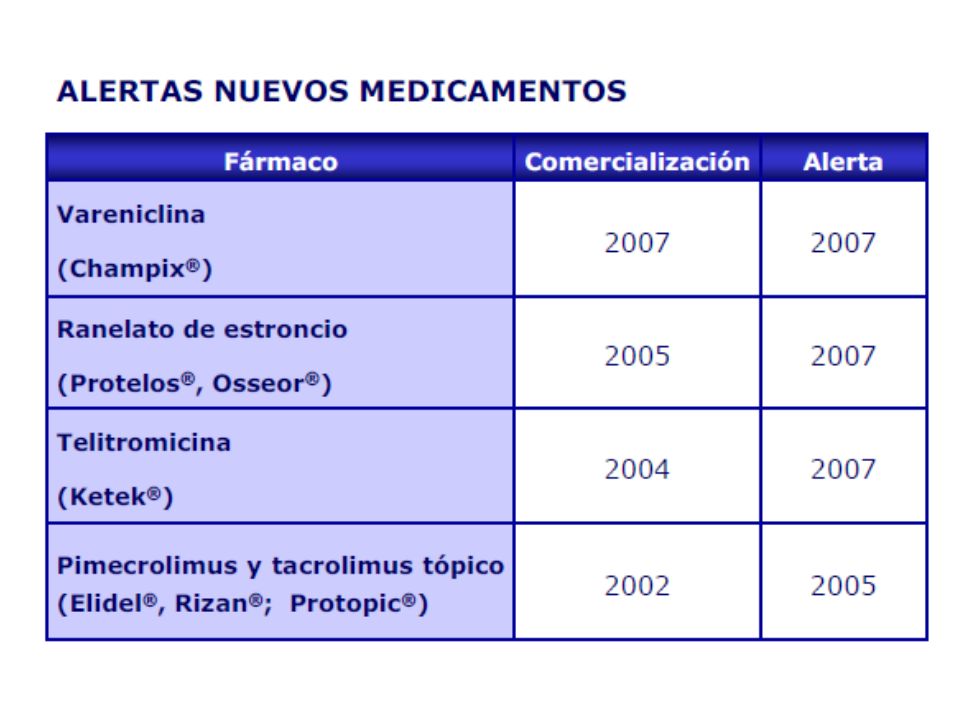
Durante el período postcomercialización, se han notificado casos de depresión, ideación y comportamiento suicida e intento de suicidio en pacientes sometidos a deshabituación tabáquica con Champix. Se debe interrumpir inmediatamente el tratamiento con Champix si el paciente desarrollara una ideación o comportamiento suicida

22
Cabazitaxel 1 Ensayo clínico 110 artículos 41 revisiones Lancet
en pubmed 41 revisiones ¿seguridad…? Científica

24
Resultados seguridad ROCKET AF
Variable RIVAR N (7.111)Ϯ WARF N (7.125) Ϯ RAR (IC95%) NNT (IC95%) Hemorragia mayor Hemorragia mayor intracraneal Hemorragia GI 395 (5,6%) 55 (0,8%) 224 (3,2%) 386 (5,5%) 84 (1,2%) 154 (2,2%) NS 0,4% (0,1-0,7%) -1,0% (-0,5 -1,5%) NA 246 ( ) NNH = 100 (65-214)
Ϯ. WARF. N (7.125) Ϯ. RAR (IC95%) NNT (IC95%) Hemorragia mayor. Hemorragia mayor intracraneal. Hemorragia GI. 395 (5,6%) 55 (0,8%) 224 (3,2%) 386 (5,5%) 84 (1,2%) 154 (2,2%) NS. 0,4% (0,1-0,7%) -1,0% (-0,5 -1,5%) NA ( ) NNH = 100 (65-214)")
25
Institucional

27
56 (10. 2%) acquired a new black box warning or were withdrawn
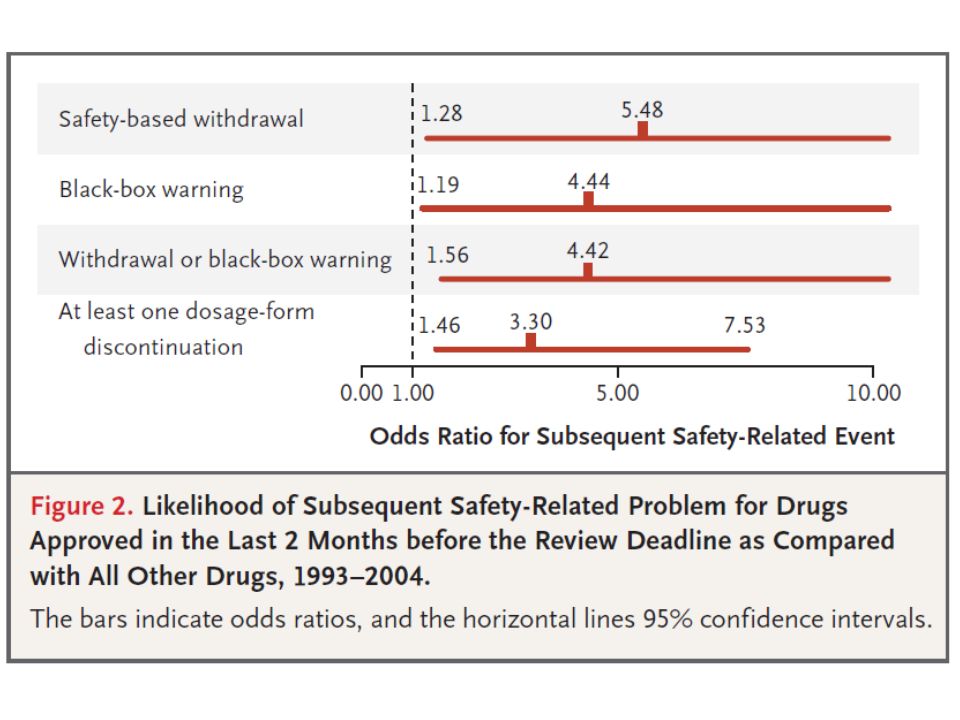
56 (10.2%) acquired a new black box warning or were withdrawn. In Kaplan- Meier analyses, half of these changes occurred within 7 years of drug introduction; half of the withdrawals occurred within 2 years
 acquired a new black box warning or were withdrawn. In Kaplan- Meier analyses, half of these changes occurred within 7 years of drug introduction; half of the withdrawals occurred within 2 years.")
31
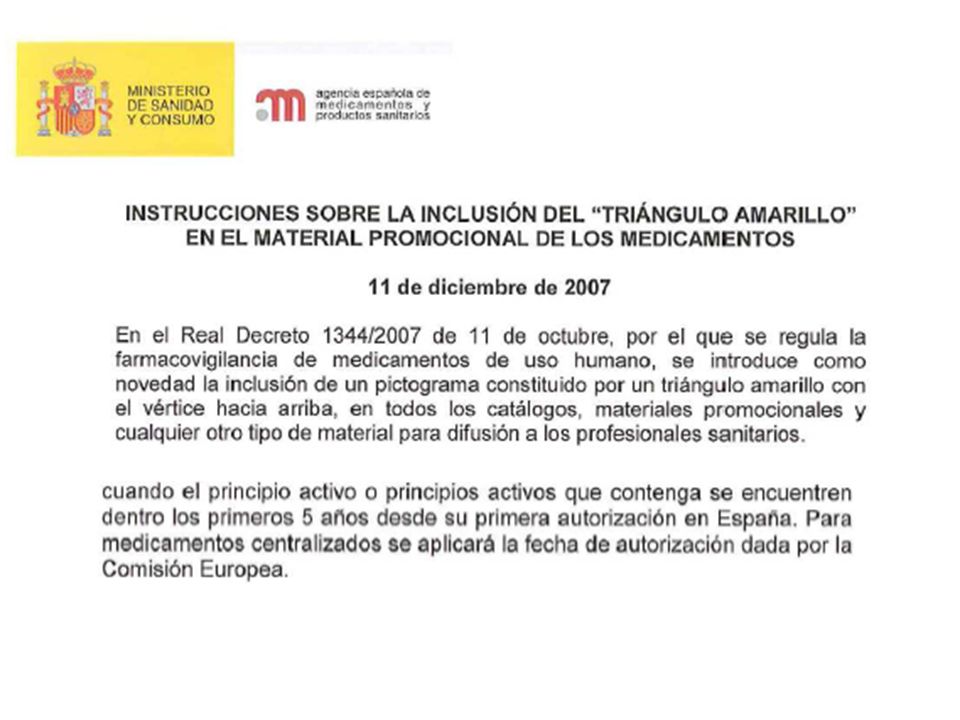
23/09/2010 European Medicines Agency recommends suspension of Avandia, Avandamet and Avaglim Anti-diabetes medication to be taken off the market The current review of rosiglitazone by the Agency’s Committee for Medicinal Products for Human Use (CHMP) was initiated on 9 July 2010 following the availability of new studies questioning the cardiovascular safety of the medicine. Since its first authorisation, rosiglitazone has been recognised to be associated with fluid retention and increased risk of heart failure and its cardiovascular safety has always been kept under close review. Consequently, the use of rosiglitazone was restricted to a second-line treatment and contra-indicated in patients with heart failure or a history of heart failure when it was first granted a marketing authorisation as Avandia in 2000. Data from clinical trials, observational studies and meta-analyses of existing studies that have become available over the last three years have suggested a possibly increased risk of ischaemic heart disease associated with the use of rosiglitazone. Further restrictions on the use of these medicines in patients with ischaemic heart disease were introduced. The availability of recent studies has added to the knowledge about rosiglitazone and overall, the accumulated data support an increased cardiovascular risk of rosiglitazone. In view of the restrictions already in place on the use of rosiglitazone, the Committee could not identify additional measures that would reduce the cardiovascular risk. The Committee therefore concluded that the benefits of rosiglitazone no longer outweigh its risks and recommended the suspension of the marketing authorisation of the medicines
 was initiated on 9 July 2010 following the availability of new studies questioning the cardiovascular safety of the medicine. Since its first authorisation, rosiglitazone has been recognised to be associated with fluid retention and increased risk of heart failure and its cardiovascular safety has always been kept under close review. Consequently, the use of rosiglitazone was restricted to a second-line treatment and contra-indicated in patients with heart failure or a history of heart failure when it was first granted a marketing authorisation as Avandia in Data from clinical trials, observational studies and meta-analyses of existing studies that have become available over the last three years have suggested a possibly increased risk of ischaemic heart disease associated with the use of rosiglitazone. Further restrictions on the use of these medicines in patients with ischaemic heart disease were introduced. The availability of recent studies has added to the knowledge about rosiglitazone and overall, the accumulated data support an increased cardiovascular risk of rosiglitazone. In view of the restrictions already in place on the use of rosiglitazone, the Committee could not identify additional measures that would reduce the cardiovascular risk. The Committee therefore concluded that the benefits of rosiglitazone no longer outweigh its risks and recommended the suspension of the marketing authorisation of the medicines.")
32
Estructura química o mecanismo de acción más seguro: incremento otras RAMs. Fcos “mejorados en seguridad” Sociocultural

33
NOVEDADES TERAPEUTICAS Y SEGURIDAD

34
Cambio en el perfil de RA!!!

35
Falacias Alertas Incertidumbre Toxicidad inesperada RA fatales
Limitaciones RA fatales Alertas Incertidumbre Toxicidad inesperada

36
Cry wolf syndrome

37
Novedades terapéuticas y seguridad
Relación beneficio-riesgo ¿Cómo medimos la seguridad? Toma de decisiones

38
Gravedad de las RAMs Incidencia de las RAMs Fármaco

39
No se midió calidad de vida en los pacientes, lo cual hubiera sido deseable dado el perfil de toxicidad del fármaco. La gravedad de los efectos secundarios sería aceptable en una enfermedad cuyo objetivo sea la curación…

40
Pronóstico de la patología
Grado de esencialidad Pronóstico de la patología Contexto del tratamiento

41
Novedades terapéuticas y seguridad
Relación beneficio-riesgo ¿Cómo medimos la seguridad? Toma de decisiones

42
Número necesario para dañar ó lesionar (NND, NNH)
1 NND = x100 (% eventos en población intervención) - (% eventos en población control) Aumento absoluto del riesgo (AAR) Se utiliza para medir EA de la intervención Nº de pacientes para producir/evitar un EA adicional Sólo eventos estadísticamente significativos
 - (% eventos en población control) Aumento absoluto del riesgo (AAR) Se utiliza para medir EA de la intervención. Nº de pacientes para producir/evitar un EA adicional. Sólo eventos estadísticamente significativos.")
43
¿Cuántos pacientes debo tratar?

44
1 más sufra daño

45
Resultados seguridad ROCKET AF
Variable RIVAR N (7.111)Ϯ WARF N (7.125) Ϯ RAR (IC95%) NNT (IC95%) Hemorragia mayor Hemorragia mayor intracraneal Hemorragia GI 395 (5,6%) 55 (0,8%) 224 (3,2%) 386 (5,5%) 84 (1,2%) 154 (2,2%) NS 0,4% (0,1-0,7%) -1,0% (-0,5 -1,5%) NA 246 ( ) NNH = 100 (65-214)
Ϯ. WARF. N (7.125) Ϯ. RAR (IC95%) NNT (IC95%) Hemorragia mayor. Hemorragia mayor intracraneal. Hemorragia GI. 395 (5,6%) 55 (0,8%) 224 (3,2%) 386 (5,5%) 84 (1,2%) 154 (2,2%) NS. 0,4% (0,1-0,7%) -1,0% (-0,5 -1,5%) NA ( ) NNH = 100 (65-214)")
46
Probabilidad de ayudar a un paciente vs dañarlo (LHH)
1/NNT (RAR) LHH = x /NNH (AAR) LHH>1 mas probabilidad de ayudar que de dañar LHH<1 mas probabilidad de dañar que de ayudar
 LHH = x100 1/NNH (AAR) LHH>1 mas probabilidad de ayudar que de dañar. LHH<1 mas probabilidad de dañar que de ayudar.")
47
El resultado se inclina a favor del interferón:
Interferón en EM NNT=9: para evitar una complicación de parálisis por EM NNH=12: por cada 12 pacientes que trato aparece un efecto adverso mayor El resultado se inclina a favor del interferón: 1/9 / 1/12 =1,321

48
Novedades terapéuticas y seguridad
Relación beneficio-riesgo ¿Cómo medimos la seguridad? Toma de decisiones

49
PRASUGREL (Efient®) En profilaxis antitrombótica en pacientes con SCA sometidos a ICP Informe del grupo GÉNESIS de la SEFH 20/10/2010 PRASUGREL (Efient®) En profilaxis antitrombótica en pacientes con SCA sometidos a ICP Informe del grupo GÉNESIS de la SEFH 20/10/2010
 En profilaxis antitrombótica en pacientes con SCA sometidos a ICP Informe del grupo GÉNESIS de la SEFH 20/10/2010.")
50
Tabla 4. Resultados de seguridad.
Referencia: Informe EPAR EMEA15 y estudio TRITON-TIMI 38, Wiviot et al12 Reacciones adversas y muertes Variable de seguridad evaluada en el estudio Prasugrel N=6813 Clopidogrel N=6795 AAR (IC 95%) P NNH o NND (IC 95%)* EA EA hemorrágicos EA no hemorrágicos Abandonos por EA 80,34% 29,7% 77,33% 7,15% 80,02% 22,04% 77,86% 6,02% 0,3% (-1,7 a 1,0) 7,66% - Ns <0,001 13 EACS* Muertes globales Muerte cardiovascular Muerte no cardiovascular 5,34% 2,76% 1,95% 0,81% 5,0% 2,90% 2,21% 0,69% 0,4% (-0,4 a 1,1) -0,1%(-0,7 a 0,4) -0,3%(-0,7 a 0,2) 0,1%(-0,2 a 0,4) EA: Efecto adverso EACS: Efecto adverso clínicamente significativo (excluyendo las hemorragias) entre los que se incluyeron trombocitopenia, púrpura trombocitopénica trombótica, neutropenia, leucopenia, pancitopenia, torsades de pointes/prolongación del segmento ST, reacciones alérgicas o alteraciones de la función hepática. Ns: no significativo
 P. NNH o NND. (IC 95%)* EA. EA hemorrágicos. EA no hemorrágicos. Abandonos por EA. 80,34% 29,7% 77,33% 7,15% 80,02% 22,04% 77,86% 6,02% 0,3% (-1,7 a 1,0) 7,66% - Ns. <0, EACS* Muertes globales. Muerte cardiovascular. Muerte no cardiovascular. 5,34% 2,76% 1,95% 0,81% 5,0% 2,90% 2,21% 0,69% 0,4% (-0,4 a 1,1) -0,1%(-0,7 a 0,4) -0,3%(-0,7 a 0,2) 0,1%(-0,2 a 0,4) EA: Efecto adverso. EACS: Efecto adverso clínicamente significativo (excluyendo las hemorragias) entre los que se incluyeron trombocitopenia, púrpura trombocitopénica trombótica, neutropenia, leucopenia, pancitopenia, torsades de pointes/prolongación del segmento ST, reacciones alérgicas o alteraciones de la función hepática. Ns: no significativo.")
51
Tabla 5. Resultados del ensayo TRITON-TIMI 38
Referencia: Wiviott SD et al. N Engl J Med 2007; 357: ; Wiviott SD et al. Am Heart J 2006; 152: Resultados de seguridad Variable evaluada en el estudio Prasugrel N = 6.741 Clopidogrel N = 6.716 HR (IC 95%) p NNH Sangrado mayor no relacionado con CBAC 146 (2,4%) 111 (1,8%) 1,32 (1,03-1,68) 0,03 176* ( ) 197**( ) Sangrado que compromete la vida no relacionado con CBAC Hemorragias fatales 85 (1,4%) 21 (0,4%) 56 (0,9%) 5 (0,1%) 1,52 (1,08-2,13) 4,19 (1,58-11,11) 0,01 0,002 215*( ) 236**( ) 314*( ) 426**( ) Sangrado mayor o menor 303 (5%) 231 (3,8%) 1,31 (1,11-1,56) 87*(48-244) 96**(59-251) Sangrado que requiere transfusión 244 (4%) 182(3,0%) 1,34 (1,11-1,63) <0,001 110 (67-333) Neoplasia de colon 13 (0,2%) 4 (0,1%) RR 3,24 (1,06-9,94) 758** *Calculado a partir de HR **Calculado a partir de RAR
 p. NNH. Sangrado mayor no relacionado con CBAC. 146 (2,4%) 111 (1,8%) 1,32. (1,03-1,68) 0, * ( ) 197**( ) Sangrado que compromete la vida no relacionado con CBAC. Hemorragias fatales. 85 (1,4%) 21 (0,4%) 56 (0,9%) 5 (0,1%) 1,52. (1,08-2,13) 4,19. (1,58-11,11) 0,01. 0, *( ) 236**( ) 314*( ) 426**( ) Sangrado mayor o menor. 303 (5%) 231 (3,8%) 1,31. (1,11-1,56) 87*(48-244) 96**(59-251) Sangrado que requiere transfusión. 244 (4%) 182(3,0%) 1,34. (1,11-1,63) <0, (67-333) Neoplasia de colon. 13 (0,2%) 4 (0,1%) RR 3,24. (1,06-9,94) 758** *Calculado a partir de HR. **Calculado a partir de RAR.")
52
Sangrado que compromete la vida (no CBAC)
Sangrado que requiere transfusión Hemorragias fatales

53
Evaluar cuantitativamente la relación riesgo/beneficio para prasugrel
Evaluar cuantitativamente la relación riesgo/beneficio para prasugrel. Por cada 1000 pacientes tratados con prasugrel en lugar de con clopidogrel se evitarán 22 IM no fatales, pero se producirán 5 sangrados con compromiso vital, de los que 3 fallecerán.

54
Evaluar cuantitativamente la relación riesgo/beneficio para prasugrel LHH = (1/NNT)/(1/NNH) = (1/46)/(1/176) = 4, Por cada 4 pacientes que obtuvieran un resultado primario de eficacia (muerte de origen cardiovascular + IM no fatal + ACV no fatal) 1 paciente sufriría un sangrado mayor
/(1/NNH) = (1/46)/(1/176) = 4, Por cada 4 pacientes que obtuvieran un resultado primario de eficacia (muerte de origen cardiovascular + IM no fatal + ACV no fatal) 1 paciente sufriría un sangrado mayor")
55
Subgrupos

56
Discordancia Eficacia / Seguridad
Beneficio Neto* HR (IC95%) P Historia de AIT/ Ictus 1,54 (1,02 a 2.32) 0.04 Pacientes ≥ 75 años 0.99 (0.81 a 1.21) 0.92 Pacientes < 60 kg 1.03 (0.69 a 1.53) 0.89 *Beneficio neto: muerte, IM no fatal, Ictus no fatal, hemorragia mayor no-CBAC.
 P. Historia de AIT/ Ictus. 1,54. (1,02 a 2.32) Pacientes ≥ 75 años (0.81 a 1.21) Pacientes < 60 kg (0.69 a 1.53) *Beneficio neto: muerte, IM no fatal, Ictus no fatal, hemorragia mayor no-CBAC.")
57
Edad < 75 años Peso ≥60 Kg No AIT/Ictus previo PRA + ASA CLO HR (IC95%) p Variable principal Hemorragia mayor no-CBAC Beneficio neto 8,3% 2% 10,2% 11% 1.5% 12,5% 0,74 (0.66, 0.84) 1.24 (0.91, 1.69) 0.80 (0.71, 0.89) <0,01 0,17
 1.24 (0.91, 1.69) 0.80 (0.71, 0.89) <0,01. 0,17.")
58
Platelet Inhibition Related to the Risk of Ischemic and Bleeding Events
High risk of ischemic events High risk of bleeding events “Sweet spot” Risk of Any Event Risk of Any Event – Inhibition of platelet aggregation + Ischemic risk Bleeding risk Ferreiro JL et al. Thromb Haemost. 2010;103:1-8. 1. The CURE Trial Investigators. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N Engl J Med. 2001;345: 2. Plavix® (clopidogrel bisulfate) Prescribing Information. 58
 Prescribing Information. 58.")
59
MUCHAS GRACIAS

Presentaciones similares




>")














