Descargar la presentación
La descarga está en progreso. Por favor, espere

1
CANCER ESOFAGO

2
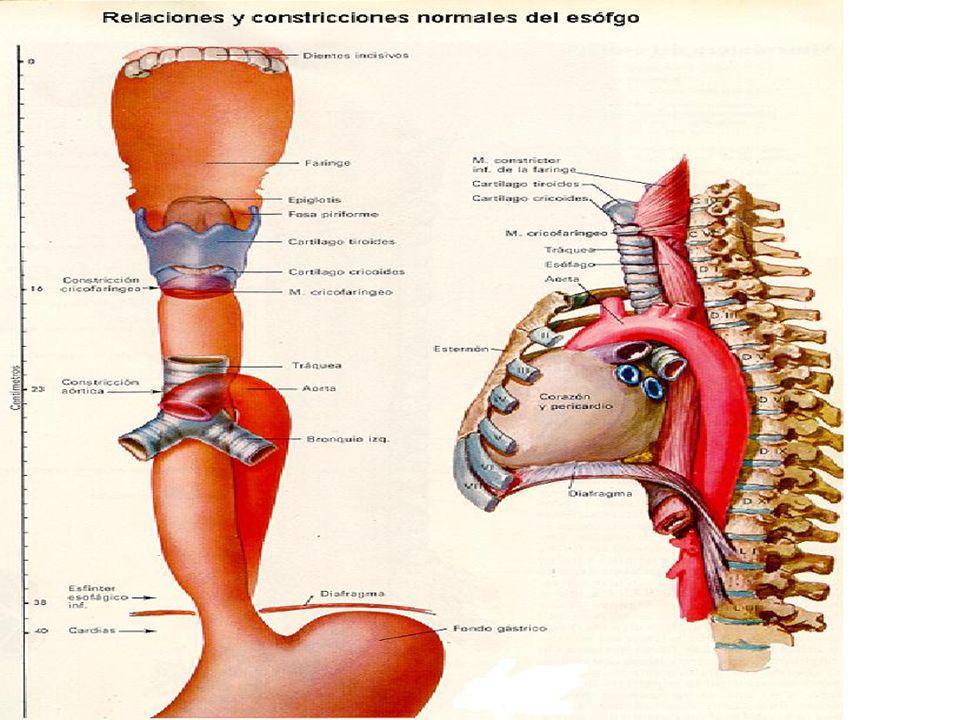
Esófago parte del tubo digestivo de los seres humanos formada por un tubo muscular de unos 20 centímetros. Se extiende desde la 6ª o 7ª vértebra cervical hasta la 11ª vértebra torácica y a través del mismo pasan los alimentos desde la faringe al estómago.

3
discurre por el cuello y mediastino posterior hasta introducirse en el abdomen superior, atravesando
el diafragma. Porción cervical Porción torácica Porción abdominal

4
En el recorrido ---improntas producidas por las estructuras vecinas en íntimo contacto :
El cartílago cricoides de la laringe. El cayado aórtico de la arteria aorta. La aurícula izquierda del corazón. El hiato diafragmático, que es el orificio del diafragma por el que pasa el esófago

6
Histologia El esófago presenta tres mucosas:
Esofágica torácica: epitelio plano estratificado no queratinizado. Esofágica de transición: epitelio de transición. Esofágica abdominal: epitelio tubárico glandular.

7
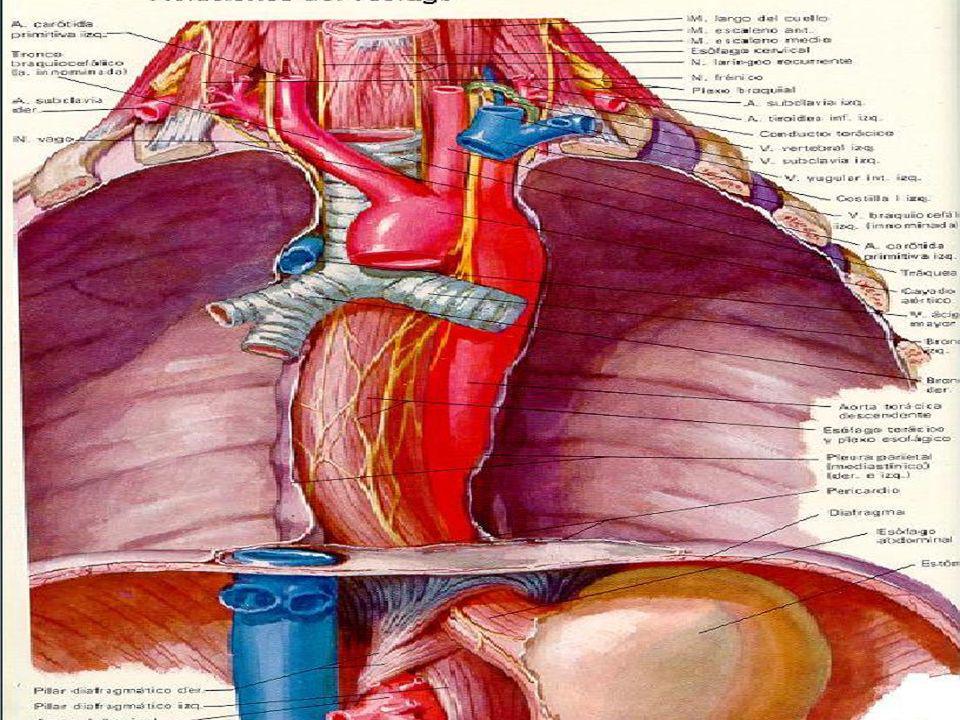
RELACIONES

9
Porción cervical: Anterior: tráquea (fibras de unión esófagotráquea)
Recurrentes del vago, tronco arterial braquiocefálico derecho. Posterior: espacio retroesofágico y columna vertebral. Lateral: * Derecha: cúpula del pulmón, paquete vasculonervioso cuello. * Izquierda: arteria subclavia izquierda.

10
Porción torácica: Retrotraqueales:
Anterior: tráquea (músculos anulares). Derecha: pulmones, vena ácigos, vena cava, recurrente y vago derecho. Izquierda: pulmón, vena subclavia izquierda, vena carótida izquierda, yugular interna, aorta descendente, cayado aórtico, conducto torácico, nervio vago y recurrente.
. Derecha: pulmones, vena ácigos, vena cava, recurrente y vago derecho. Izquierda: pulmón, vena subclavia izquierda, vena carótida izquierda, yugular interna, aorta descendente, cayado aórtico, conducto torácico, nervio vago y recurrente.")
11
Porción torácica: Retropericardiales:
Dorsal: espacio retroesofágico, músculos prevertebrales, músculos paravertebrales, columna vertebral, vago posterior. Derecha: vena ácigos. Izquierda: vena hemiácigos.

13
Porción abdominal: 2 cm. Nervios vagos: uno pasa por delante y el otro por detrás del esófago. Histología: la mucosa se transforma para poder resistir la acidez del estómago que por reflujo puede llegar hasta él.

14
Irrigacion En el cuello, está irrigado por arterias esofágicas superiores, ramas de la arteria tiroidea inferior que procede de la subclavia. En el tórax, por las arterias esofágicas medias, por arterias bronquiales y las intercostales, que son ramas directas de la aorta. En el abdomen, por las arterias esofágicas inferiores procedentes de las diafragmáticas inferiores de la arteria gástrica posterior.

15
venosa Porción cervical: vena esofágica de la subclavia
que drena en la cava superior. Porción torácica: venas intercostales esofágicas que se dirigen a la vena hemiácigos y ésta a la cava superior. Porción abdominal: vena esofágica gástrica izquierda que va a la vena porta, luego al hígado y de allí a la vena cava.

16
INERVACION Tanto la simpática como la parasimpática corre a cargo del nervio vago o décimo par craneal.

17
Concepto Es el desarrollo anárquico y permanente del tejido esofágico provocado por la falta de control del crecimiento, dando origen a serios trastornos por compresión de otras estructuras a medida que aumenta su tamaño, y que pueden llevar a la muerte por el compromiso de órganos vitales y por el estado de desnutrición que provocan en el paciente.

18
Epidemiologia

19
9o lugar neoplasias malignas en el mundo y en paises en via de desarrollo ocupa el 5o.
4o en los tumores del tubo digestivo. alta incidencia en el cinturón asiático mayor en el sexo masculino 4:1 con mayor incidencia entre los 50 y 70 años México representa 1.3% de todas las neoplasias malignas El ADC se ha incrementado de 8 a 33%, el tercio inferior esofágico el mas afectado.

20
Factores predisponentes.
Síndrome de Plummer Winson Tylosis Esofagitis cáustica Esofagitis actínica Acalasia Hábitos tabáquico y alcohólico Reflujo gastroesofágico crónico (ERGE Divertículos esofágicos. Radioterapia Deficiencia nutricional (Vit. A y Riboflavina) Consumo carcinogenéticos genetica
 Consumo carcinogenéticos. genetica.")
21
CANCER DE ESÓFAGO VARIEDADES HISTOLÓGICAS Y VIAS DE DISEMINACIÓN

22
CA.ESÓFAGO:A.PATOLÓGICA
TIPOS HISTOLÓGICOS: CARCINOMA EPIDERMOIDE 70% Anaplásico 10 % ADENOCARCINOMA 20% OTROS

23
CA.ESÓFAGO:A.PATOLÓGICA
CARCINOMA EPIDERMOIDE FORMAS:-vegetante 60% -infiltrante 25% -ulcerado % - LOCALIZACIÓN: 20% TERCIO SUPERIOR 50% TERCIO MEDIO 30% TERCIO INFERIOR

24
CA.ESOFAGO.-A.PATOLOGICA
ADENOCARCINOMA 20% LOCALIZACIÓN: Tercio inferior OTROS: -CARCINOMA DE CELULAS FUSIFORMES -CARCINOMA MUCOEPIDERMOIDE -LEIOMIOSARCOMA -MELANOMA

25
DISEMINACION EXTENSIÓN DIRECTA EXTENSIÓN INTRAESOFAGICA DISEMINACION:
CRECIMIENTO SUBMUCOSO NÓDULOS SATÉLITES DISEMINACION: LINFÁTICA METAS GANGLIONARES EN EL 50% HEMATICA 45 % METAS : HEPÁTICAS,OSEAS,RIÑÓN, SUPRARRENALES.

26
DISEMINACIÓN: EXTENSIÓN DIRECTA
FIGURE Comparison of endoscopic ultrasonographic image with layers of gut wall. The first layer, hyperechoic, represents the interface between the endoscope and superficial mucosa. The second layer, hypoechoic, represents the lamina propria and muscularis mucosae. The third layer, hyperechoic, represents submucosa and the interface between submucosa and muscularis propria. The fourth layer, hypoechoic, represents the muscularis propria. The fifth layer, hyperechoic, represents the interface between serosa and surrounding tissues. (From Rice TW, Zuccaro G Jr: Endoscopic esophageal ultrasound. In Pearson FG, Cooper JD, Deslauriers J, et al [eds]: Esophageal Surgery, 2nd ed. Philadelphia, Churchill Livingstone, 2002, p 124.)
")
27
DISEMINACION EXTENSIÓN INTRAESOFAGICA CRECIMIENTO SUBMUCOSO
NÓDULOS SATÉLITES

28
DISEMINACION DISEMINACIÓN: HEMATICA 45 % DE LOS ENFERMOS,MUEREN CON
METAST. : HEPÁTICAS,OSEAS,RIÑÓN, SUPRARRENALES.

29
FIGURE 39-2. Arterial blood supply of the esophagus
FIGURE Arterial blood supply of the esophagus. (Adapted from Hagen JA, DeMeester TR: Anatomy of the esophagus. In Shields TW, LoCicero J III, Ponn RB [eds]: General Thoracic Surgery, 5th ed, vol 2. Philadelphia, Lippincott Williams & Wilkins, 2000, p 1599.)
")
30
FIGURE 39-3. Venous drainage of the esophagus
FIGURE Venous drainage of the esophagus. (Adapted from Hagen JA, DeMeester TR: Anatomy of the esophagus. In Shields TW, LoCicero J III, Ponn RB [eds]: General Thoracic Surgery, 5th ed, vol 2. Philadelphia, Lippincott Williams & Wilkins, 2000, p 1599.)
")
31
DISEMINACION DISEMINACION: LINFÁTICA METAS GANGLIONARES EN EL 50%

32
FIGURE 39-4. Innervation of the esophagus
FIGURE Innervation of the esophagus. (Adapted from Hagen JA, DeMeester TR: Anatomy of the esophagus. In Shields TW, LoCicero J III, Ponn RB [eds]: General Thoracic Surgery, 5th ed, vol 2. Philadelphia, Lippincott Williams & Wilkins, 2000, p 1599.)
")
33
FIGURE 39-34. Concept of lymphatic pathways
FIGURE Concept of lymphatic pathways. Owing to the embryonic development of the lymphatic pathways from two sources, the branchiogenic and the body mesenchyme, lymph drains toward two different directions. There is bidirectional flow at the tracheal bifurcation, which is the area of embryologic tissue transition. This feature is consistent with clinical observations. The knowledge of lymph flow and the corresponding lymph node distribution is essential in understanding potential spread of malignancy. (From Liebermann-Meffert D: Anatomy, embryology, and histology. In Pearson FG, Cooper JD, Deslauriers J, et al [eds]: Esophageal Surgery, 2nd ed. Philadelphia, Churchill Livingstone, 2002, p 17.

34
CANCER DE ESÓFAGO ESTADIFICACIÓN EXTENSIÓN LOCALIZACIÓN DEL TUMOR
INVASIÓN LOCAL AFECTACIÓN ORGANOS VECINOS ADENOPATÍAS EXTENSIÓN METÁSTASIS A DISTANCIA

35
CA.ESÓFAGO: TNM T 1 : INVASIÓN MUCOSA Y SUBMUCOSA
T 2 : INVASIÓN MUSCULAR T 3 : AFECTACIÓN DE TODA LA PARED N O : SIN AFECTACIÓN GANGLIOS N 1 : AFECTA. GANGLIOS UNILATERALES N 2 : GANGLIOS BILATERALES N3 : GANGLIOS A DISTANCIA M 0 : SIN METAS A DISTANCIA M 1 : CON METAS A DISTANCIA

36
ESTADIFICACIÓN FIGURE Primary tumor status (T) is defined by depth of tumor invasion. Regional lymph node (N) status is defined by the absence (N0) or presence (N1) of regional nodal metastases. HGD, high-grade dysplasia. (From Rice TW: Esophageal carcinoma: Diagnosis and staging of esophageal carcinoma. In Pearson FG, Cooper JD, Deslauriers J, et al [eds]: Esophageal Surgery, 2nd ed. Philadelphia, Churchill Livingstone, 2002, p 687.)
 is defined by depth of tumor invasion. Regional lymph node (N) status is defined by the absence (N0) or presence (N1) of regional nodal metastases. HGD, high-grade dysplasia. (From Rice TW: Esophageal carcinoma: Diagnosis and staging of esophageal carcinoma. In Pearson FG, Cooper JD, Deslauriers J, et al [eds]: Esophageal Surgery, 2nd ed. Philadelphia, Churchill Livingstone, 2002, p 687.)")
37
CANCER DE ESÓFAGO CUADRO CLINICO

38
CA. ESOFAGO : CLINICA DISFAGIA : lógica SIALORREA PERDIDA DE PESO
DOLOR RETROESTERNAL HEMORRAGIA : Hematemesis y melenas COMPLICACIONES: FISTULA TRAQEOESOFAGICA DISFONÍA.- TOS.-RONQUERA.- NEUMONIAS POR ASPIRACIÓN

39
CANCER DE ESÓFAGO ESTRATEGIA DIAGNÓSTICA

40
CA. ESÓFAGO.DIAGNÓSTICO
DIAGNÓSTICO DE LA NEOPLASIA RADIOGRAFIAS POR TRÁNSITO ENDOSCOPIA Y BIOPSIA ESTADIFICACIÓN ECO ENDOSCOPIA, TAC Y RNM EVALUACIÓN ESTADO GENERAL VALORACION CARDIACA VALORACION RESPIRATORIA VALORACION RENAL, HEPATICA, ESTADO NUTRICIONA

41
ENDOSCOPIA: ESOFAGOSCOPIA
FIGURE Adenocarcinoma of the esophagogastric junction. (From Rice TW, Zuccaro G Jr: Flexible esophagoscopy. In Pearson FG, Cooper JD, Deslauriers J, et al [eds]: Esophageal Surgery, 2nd ed. Philadelphia, Churchill Livingstone, 2002, p 153.)
")
42
ECOGRAFÍA ENDOLUMINAL
FIGURE Use of endoscopic ultrasound allows real-time imaging of lymph nodes within 5 cm of the esophagus, including subcarinal nodes, providing direct access for fine-needle aspiration.

43
U.S. ENDOLUMINAL CAPA MUSCULAR PROPIA
FIGURE A T2 esophageal carcinoma. Top, A T2 tumor as seen by endoscopic ultrasound. The hypoechoic (black) tumor invades the hypoechoic (black) fourth ultrasound layer (muscularis propria) but does not breach the boundary between fourth and fifth ultrasound layers (arrows). Bottom, A T2 tumor invades but does not breach the muscularis propria. (From Rice TW, Zuccaro G Jr: Endoscopic esophageal ultrasound. In Pearson FG, Cooper JD, Deslauriers J, et al [eds]: Esophageal Surgery, 2nd ed. Philadelphia, Churchill Livingstone, 2002, p 688.) CAPA MUSCULAR PROPIA
 tumor invades the hypoechoic (black) fourth ultrasound layer (muscularis propria) but does not breach the boundary between fourth and fifth ultrasound layers (arrows). Bottom, A T2 tumor invades but does not breach the muscularis propria. (From Rice TW, Zuccaro G Jr: Endoscopic esophageal ultrasound. In Pearson FG, Cooper JD, Deslauriers J, et al [eds]: Esophageal Surgery, 2nd ed. Philadelphia, Churchill Livingstone, 2002, p 688.) CAPA MUSCULAR. PROPIA.")
44
PRONÓSTICO PROFUNDIDAD PENETRACION PARED AFECTACIÓN GANGLIONAR
T 3, T 4 , PEOR QUE: T 1, T 2 AFECTACIÓN GANGLIONAR > 4 GANGLIOS , PEOR QUE < PÉRDIDA DE PESO > 10 % peor pronóstico EDAD ESTADO NUTRICIONAL

45
CA. ESÓFAGO: INOPERABILIDAD
METÁSTASIS A DISTANCIA PARÁLISIS DE CUERDAS INFILTRACIÓN TRAQUEOBRONQUIAL > 5-9 cm EN 1/3 superior y medio FUNCIÓN PULMONAR < 50 % CARDIOPATÍAS VALVULARES ANGOR SINTOMÁTICO EDAD ? > 70 a.

46
CANCER DE ESÓFAGO TRATAMIENTO

47
CANCER DE ESÓFAGO ALTERNATIVAS TERAPEÚTICAS CIRUGÍA RADICAL
CIRUGÍA PALIATIVA RT QX OTROS

48
CA. ESÓFAGO: TRATAMIENTO
CIRUGÍA = TRATAMIENTO ESTÁNDAR T 1, T 2 RESECCIÓN “CURATIVA” = 50 % MEDIANA DE SUPERVIVENCIA 11 meses MORTALIDAD QUIRURGICA < 10 %

49
CA.ESÓFAGO. RECONSTRUCCIÓN
ESTÓMAGO : en el 80 % de los casos Una sola anastomosis

50
FIGURE A to C, Overview of transhiatal esophagectomy with gastric mobilization and gastric pull-up for cervical-esophagogastric anastomosis. (A to C, Adapted from Ellis FH Jr: Esophagogastrectomy for carcinoma: Technical considerations based on anatomic location of lesion. Surg Clin North Am 60:275, 1980.)
.")
51
FIGURE Overview of left thoracotomy (A) and esophageal mobilization with gastric pull-up (B) for intrathoracic anastomosis (C). D, The completed low intrathoracic esophagogastric anastomosis is shown. The remaining distal stomach has been mobilized into the chest through the diaphragmatic hiatus and the stomach suspended from the prevertebral fascia with several sutures. The anastomosis is constructed away from the suture line of the gastric transection. The edge of the diaphragmatic hiatus has been sutured to the stomach to prevent herniation of abdominal viscera. The diaphragmatic incision is closed with everting horizontal mattress sutures followed by a running whipstitch of nonabsorbable suture. (A to C, Adapted from Ellis FH Jr, Shahian DM: Tumors of the esophagus. In Glenn WWL, Baue AE, Geha AS, et al [eds]: Thoracic and Cardiovascular Surgery, 4th ed. Norwalk, CT, Appleton & Lange, 1983, p 566, with permission of the McGraw-Hill Companies. D, Adapted from Orringer MB: Surgical options for esophageal resection and reconstruction with stomach. In Baue AE, Geha AS, Hammond GL [eds]: Glenn’s Thoracic and Cardiovascular Surgery, 5th ed. Norwalk, CT, Appleton & Lange, 1991, p 793, with permission of the McGraw-Hill Companies.)
 and esophageal mobilization with gastric pull-up (B) for intrathoracic anastomosis (C). D, The completed low intrathoracic esophagogastric anastomosis is shown. The remaining distal stomach has been mobilized into the chest through the diaphragmatic hiatus and the stomach suspended from the prevertebral fascia with several sutures. The anastomosis is constructed away from the suture line of the gastric transection. The edge of the diaphragmatic hiatus has been sutured to the stomach to prevent herniation of abdominal viscera. The diaphragmatic incision is closed with everting horizontal mattress sutures followed by a running whipstitch of nonabsorbable suture. (A to C, Adapted from Ellis FH Jr, Shahian DM: Tumors of the esophagus. In Glenn WWL, Baue AE, Geha AS, et al [eds]: Thoracic and Cardiovascular Surgery, 4th ed. Norwalk, CT, Appleton & Lange, 1983, p 566, with permission of the McGraw-Hill Companies. D, Adapted from Orringer MB: Surgical options for esophageal resection and reconstruction with stomach. In Baue AE, Geha AS, Hammond GL [eds]: Glenn’s Thoracic and Cardiovascular Surgery, 5th ed. Norwalk, CT, Appleton & Lange, 1991, p 793, with permission of the McGraw-Hill Companies.).")
52
FIGURE After completing the transhiatal esophagectomy for a localized distal third carcinoma, the surgical stapler is used to fashion a gastric tube from the greater curvature, resecting as much stomach as possible distal to gross tumor. The remaining stomach is then positioned in the posterior mediastinum in the original esophageal bed and is anastomosed to the cervical esophagus. (Adapted from Orringer MB, Sloan H: Esophageal replacement after blunt esophagectomy. In Nyhus LM, Baker RJ [eds]: Mastery of Surgery. Boston, Little, Brown, 1984.)
.")
53
CA.ESÓFAGO RECONSTRUCCIÓN
OTRAS ANASTOMOSIS: COLON YEYUNO

54
FIGURE Esophagectomy with interposition of antiperistaltic segment of left colon. A, Incisions used in performance of esophagectomy, cervical esophagostomy, pyloromyotomy, and gastrostomy. B, Extent of esophageal resection (shaded area). C, Preparation of segment of left colon (shaded area) for interposition based on middle colic artery (note sites of vascular interruption, which maintain the integrity of the vascular arcade). D, Completed operation. (A to D, Adapted from Ellis FH Jr: Esophagogastrectomy for carcinoma: Technical considerations based on anatomic location of lesion. Surg Clin North Am 60: , 1980.)
. C, Preparation of segment of left colon (shaded area) for interposition based on middle colic artery (note sites of vascular interruption, which maintain the integrity of the vascular arcade). D, Completed operation. (A to D, Adapted from Ellis FH Jr: Esophagogastrectomy for carcinoma: Technical considerations based on anatomic location of lesion. Surg Clin North Am 60: , 1980.).")
55
CA. ESÓFAGO : TÉCNICAS PALIATIVAS
RESECCIONES PALIATIVAS CITORREDUCCION EVITAR LA AFAGIA TÉCNICAS DE BY-PASS GASTROSTOMIA Ó ENTEROSTOMÍA DE ALIMENTACIÓN INTUBACIÓN TRANSTUMORAL TRATAMIENTO CON LASER

Presentaciones similares








 ( 8-12 ) ESTERNÓN ESCOTADURA YUGULAR MANUBRIO>")











